22
Use of Structured Judgement Casenote Review Tool in NHS Highland 8 th May 2017 Dr Rod Harvey, Board Medical Director Rachel Hill, Clinical Governance Manager

Use of Structured Judgement Casenote Review Tool in NHS
Highland
8th May 2017
Dr Rod Harvey, Board Medical DirectorRachel Hill, Clinical Governance Manager
H
H
H
H

OVERVIEW OF MORTALITY REVIEW PROCESS USING STRUCTURED JUDGEMENT REVIEW (SJR)
• Approached by HIS to be Scottish pilot site for Royal College of Physicians National Mortality Case Record Review (NMCRR) Programme
• Method used is SJR Tool
• 32 people trained in the use of SJR tool in sessions in July and September 2016
• Now completed and reported on 76 mortality reviews using SJR. Use is ongoing and forms part of our standard way of mortality (and other) reviews

https://www.rcplondon.ac.uk/projects/national-mortality-case-record-review-programme
SJR toolConsideration of phases of care –numeric score and narrative structured judgement• Admission and initial management• Ongoing care• Care during a procedure• Perioperative care• End of life/discharge care• Overall assessment• Quality of recording

“Numerical measures…don’t give clinicians enough detail to let them know what parts of the clinical pathway might be causing concerns…
…Research has shown that the best way to learn from hospital deaths is by experienced clinicians using a standardised, structured qualitative approach linked to quality improvement work”
From RCP FAQs

Example of completed SJR

PROCESS IN PRACTICE
• Reviews undertaken of deceased cases in three hospitals– Hospital A: all deceased cases Jan to Mar 2016 (34 reviews)– Hospital B: deceased cases Jan to Mar 2016 (15 reviews)– Hospital C: sample of deceased cases Apr 2015 to Sept 2016
(27 reviews)
• Reviewers were asked to prioritise this work into busy schedules
• Time pressures resulted in further ‘mini’ training session delivered to expand the team of reviewers to complete reviews within timeframe

PROCESS IN PRACTICE
• Majority of reviews undertaken by reviewers external to the hospital in which patient received care
• Completed SJRs returned to central Clinical Governance Team for collation, analysis and reporting
• Hospital-based reports produced summarising findings and themes
• Reports and completed SJRs sent to relevant hospital leads for consideration and action planning
• Themes built into hospital improvement plans and informed prioritised improvement work

REVIEW FINDINGS
Findings presented by score for stage of care (1-5)
1 2 3 4 5
Admission and initial managementOngoing careCare during a procedurePerioperative careEnd of life/discharge careOverall assessmentQuality of recording

REVIEW FINDINGS
Narrative comments by stage of care, for example:
Overall care
“There was ... evidence of a delay in initial senior review, a delay in obtaining and collating the initial objective investigations, a delay in instituting rescue therapy following deterioration and a failure to follow through on a consultant management and monitoring plan over a weekend. Taken together this represents poor practice”
Score = 2

Overall care
“The failure to consider VTE prophylaxis in an immobile patient under active investigation is a significant omission. Local consultant input was very limited over the first five days of the admission with almost all management and external liaison devolved to the FY2 doctor. This represents inadequate supervision and support although there is no evidence that this resulted in patient harm.”

Overall care
“Overall this patient was appropriately investigated and a diagnosis established in consultation with off site specialists. There was a good standard of end of life care, although the possibility of discharge to home did not appear to be seriously entertained”
Score = 3

KEY THEMES IDENTIFIED FROM INITIAL REVIEWS
• Documentation• Treatment escalation planning• Structured sepsis care (sepsis 6)• Diagnostic testing• Diagnostic follow-up• VTE assessment • Timeliness of senior medical review• Medicines reconciliation

OVERALL ASSESSMENT: POSITIVES
• Reviewers like it!
“Very easy, intuitive for a clinician”
“The best mortality assessment tool I have seen”
• Useful findings yielded which would not have been identified by previous method (3x2 matrix)
“Good at capturing the whole patient experience and did allow for quality failings to be exposed”
“It did allow an accurate reflection of the quality of care provided”

OVERALL ASSESSMENT: NEGATIVES
• The SJR Tool
“The electronic form could be more user friendly”
“Easy to use, except for the specific questions at the end of the sheet”
“More structure to statements. Within each domain a chance to record multiple free text statements which are preceded or followed by a drop down selection "this was good/poor/very poor etc care, because". This would encourage reviewers to make clear judgements with an explanatory justification”
CHALLENGES
• Adequate number of trained reviewers
• Ensuring reviewers have adequate time to conduct review – 1 hour per case
• Ensuring consistency
• Quality assurance of reviews
• Ensuring reviewers make a JUDGEMENT rather than purely descriptive narrative

CHALLENGES
• Analysing large amount of freetext comments and undertaking meaningful, systematic thematic analysis
• Balancing ‘independent’ vs ‘team-based’ review
• Incorporating output into governance structure and ensuring findings acted upon
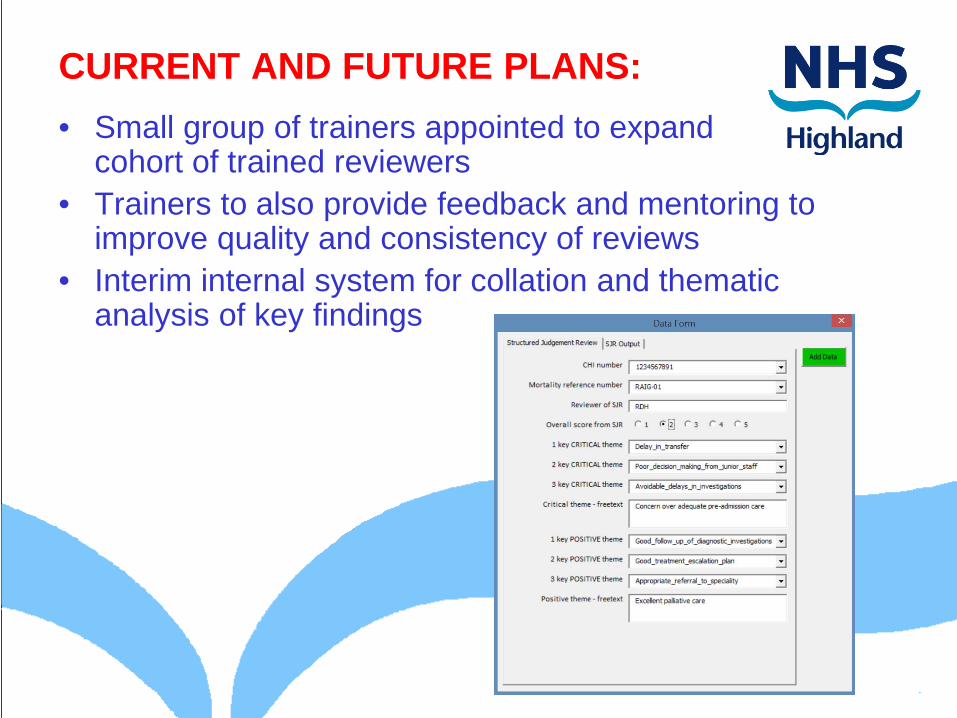
CURRENT AND FUTURE PLANS: • Small group of trainers appointed to expand
cohort of trained reviewers• Trainers to also provide feedback and mentoring to
improve quality and consistency of reviews• Interim internal system for collation and thematic
analysis of key findings


CURRENT AND FUTURE PLANS:
• Output reviewed in hospital Quality & Patient Safety Groups– Thematic analysis– Develop and monitor action plans– Feed back to treating clinicians– Report to Board Clinical Governance Committee
• Awaiting outputs from national team re system to collate, analyse and report (datix planned)
• To further enhance root cause analysis and action planning from findings
• To review process in light of recommendations from HIS Draft Practice Guide for M&M meetings

Systematic mortality review: • Every inpatient death reviewed by level 1 (initial)
reviewer within ~48 hours of death• Record minimum dataset in purpose-built database• Level 2 (SJR) review triggered if evidence of;
– Moderate to severe harm (F to I Global Trigger Tool)– Post procedure complication– New onset medical problem unrelated to disease
process on admission– Defect in care that had potential to cause significant
harm (near miss)• All cases that trigger for Level 2 review also screened
for need for adverse event review

















