CLINICAL 42 Vol. XXVI/No. One/2000 b Re film USE OF THE MANDIBULAR RAMUS AS A DONOR SITE FOR ONLAY BONE GRAFTING Craig M. Misch, DDS, MDS KEY WORDS Bone grafting Mandibular ramus Autologous bone Donor site Craig M. Misch, DDS, MDS, is an Assistant Professor, Department of Surgical Sciences, University of Pittsburgh School of Dental Medicine, Pittsburgh, Pa. He is in private practice and specializes in Oral and Maxillofacial Surgery and Prosthodontics in Sarasota, Fla. Cortical bone grafts harvested from the posterior mandible offer several advantages for bone augmentation prior to implant placement. These grafts maintain their dense quality and exhibit minimal resorption upon incorporation. Considerable amounts of bone can be harvested from this area for use as an onlay graft. In addition, the ramus area has some inherent advantages over other donor sites. This article describes the indications and surgical technique for harvesting bone from the ramus region. INTRODUCTION T he ability to predictably al- ter bone volume for im- plant placement has dra- matically changed the prac- tice of implant dentistry. Clinicians are able to offer a greater number of patients implant services and can also treat more diffi- cult cases with consistent results. Al- though many osseous augmentation techniques have been developed, autol- ogous bone grafting remains the gold standard in maxillofacial reconstruc- tion. 1–5 The use of autologous bone grafts with osseointegrated implants is a well-accepted procedure in oral re- habilitation. 6 Various donor sites throughout the skeleton have been investigated and de- scribed for bone harvest. Local grafts from the oral and facial region offer a convenient source of bone and have re- vealed several benefits in the repair of alveolar defects. 7–16 Mandibular bone grafts, which are primarily cortical bone, exhibit little volume loss and show ex- cellent incorporation at short healing times. 8,11,12,16–20 Another obvious advan- tage of local grafts is that donor and re- cipient sites are in the same operating field, so surgical and anesthesia times are reduced. 15,16,19,21 These procedures are ideal for outpatient surgery delivered in the office environment. In addition, these areas may offer a decreased morbidity from graft harvest compared to extraoral donor sites. 8,11,13,15,19 Block-type grafts may be harvested from the mandibular symphysis, body, or ramus regions. However, the unique anatomy of these different regions results in various graft sizes, shapes, and morphologies. 16 Many clinicians have concluded that the ramus area offers several advantages over other donor sites and augmentation tech- niques. This article describes the use of the mandibular ramus as a donor site for onlay grafting prior to implant place- ment. Ramus donor site Indications for the mandibular ramus as a donor site include localized mod- erate to severe alveolar atrophy or a bone defect involving a one- to four- tooth edentulous span (Table 1). The bone harvested from this area is well suited for use as a veneer graft to gain
Transcript
CLINICAL
42 Vol. XXVI/No. One/2000
b Refilm
USE OF THE MANDIBULAR RAMUS AS A DONORSITE FOR ONLAY BONE GRAFTING
Craig M. Misch, DDS, MDS
KEY WORDS
Bone graftingMandibular ramusAutologous boneDonor site
Craig M. Misch, DDS, MDS, is an AssistantProfessor, Department of Surgical Sciences,University of Pittsburgh School of DentalMedicine, Pittsburgh, Pa. He is in privatepractice and specializes in Oral andMaxillofacial Surgery and Prosthodontics inSarasota, Fla.
Cortical bone grafts harvested from the posterior mandible offer several advantages forbone augmentation prior to implant placement. These grafts maintain their dense qualityand exhibit minimal resorption upon incorporation. Considerable amounts of bone can beharvested from this area for use as an onlay graft. In addition, the ramus area has someinherent advantages over other donor sites. This article describes the indications andsurgical technique for harvesting bone from the ramus region.
INTRODUCTION
The ability to predictably al-ter bone volume for im-plant placement has dra-matically changed the prac-tice of implant dentistry.Clinicians are able to offer
a greater number of patients implantservices and can also treat more diffi-cult cases with consistent results. Al-though many osseous augmentationtechniques have been developed, autol-ogous bone grafting remains the goldstandard in maxillofacial reconstruc-tion.1–5 The use of autologous bonegrafts with osseointegrated implants isa well-accepted procedure in oral re-habilitation.6
Various donor sites throughout theskeleton have been investigated and de-scribed for bone harvest. Local graftsfrom the oral and facial region offer aconvenient source of bone and have re-vealed several benefits in the repair ofalveolar defects.7–16 Mandibular bonegrafts, which are primarily cortical bone,exhibit little volume loss and show ex-cellent incorporation at short healingtimes.8,11,12,16–20 Another obvious advan-tage of local grafts is that donor and re-
cipient sites are in the same operatingfield, so surgical and anesthesia timesare reduced.15,16,19,21 These procedures areideal for outpatient surgery delivered inthe office environment. In addition, theseareas may offer a decreased morbidityfrom graft harvest compared to extraoraldonor sites.8,11,13,15,19 Block-type graftsmay be harvested from the mandibularsymphysis, body, or ramus regions.However, the unique anatomy of thesedifferent regions results in various graftsizes, shapes, and morphologies.16 Manyclinicians have concluded that the ramusarea offers several advantages over otherdonor sites and augmentation tech-niques. This article describes the use ofthe mandibular ramus as a donor site foronlay grafting prior to implant place-ment.
Ramus donor site
Indications for the mandibular ramusas a donor site include localized mod-erate to severe alveolar atrophy or abone defect involving a one- to four-tooth edentulous span (Table 1). Thebone harvested from this area is wellsuited for use as a veneer graft to gain
Craig M. Misch
Journal of Oral Implantology 43
TABLE 1
Ramus graft indications
Localized moderate to severe atro-phy/defect
One- to four-tooth edentulous span(unilateral ramus harvest)
Donor site combinations (chin, tu-berosity, and tibia)
Inadequate available bone for sym-physis harvest
Craniofacial augmentation/repair
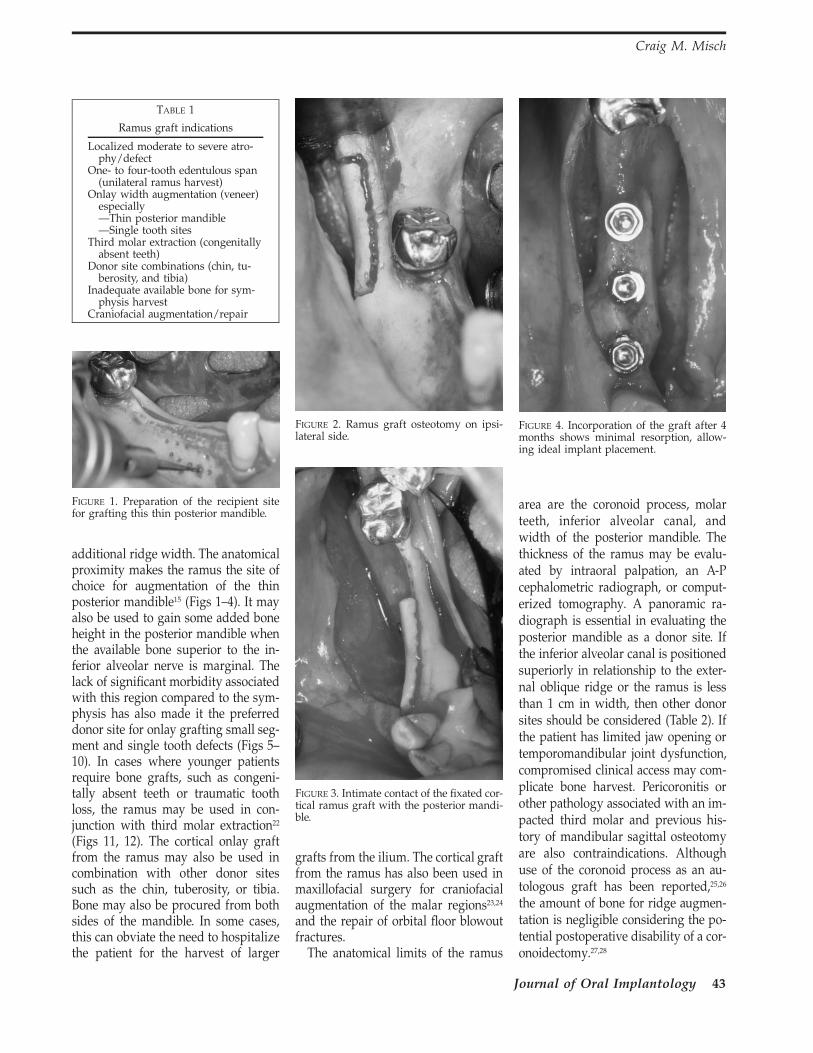
FIGURE 1. Preparation of the recipient sitefor grafting this thin posterior mandible.
FIGURE 2. Ramus graft osteotomy on ipsi-lateral side.
FIGURE 3. Intimate contact of the fixated cor-tical ramus graft with the posterior mandi-ble.
FIGURE 4. Incorporation of the graft after 4months shows minimal resorption, allow-ing ideal implant placement.
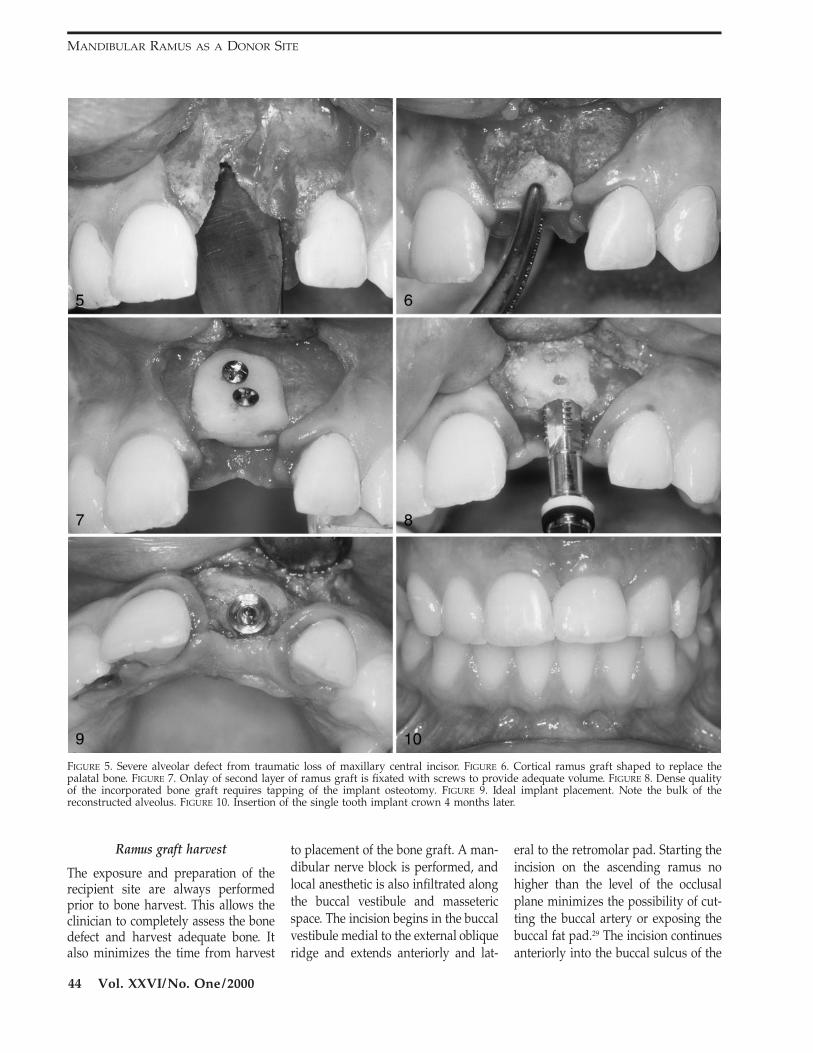
additional ridge width. The anatomicalproximity makes the ramus the site ofchoice for augmentation of the thinposterior mandible15 (Figs 1–4). It mayalso be used to gain some added boneheight in the posterior mandible whenthe available bone superior to the in-ferior alveolar nerve is marginal. Thelack of significant morbidity associatedwith this region compared to the sym-physis has also made it the preferreddonor site for onlay grafting small seg-ment and single tooth defects (Figs 5–10). In cases where younger patientsrequire bone grafts, such as congeni-tally absent teeth or traumatic toothloss, the ramus may be used in con-junction with third molar extraction22
(Figs 11, 12). The cortical onlay graftfrom the ramus may also be used incombination with other donor sitessuch as the chin, tuberosity, or tibia.Bone may also be procured from bothsides of the mandible. In some cases,this can obviate the need to hospitalizethe patient for the harvest of larger
grafts from the ilium. The cortical graftfrom the ramus has also been used inmaxillofacial surgery for craniofacialaugmentation of the malar regions23,24
and the repair of orbital floor blowoutfractures.
The anatomical limits of the ramus
area are the coronoid process, molarteeth, inferior alveolar canal, andwidth of the posterior mandible. Thethickness of the ramus may be evalu-ated by intraoral palpation, an A-Pcephalometric radiograph, or comput-erized tomography. A panoramic ra-diograph is essential in evaluating theposterior mandible as a donor site. Ifthe inferior alveolar canal is positionedsuperiorly in relationship to the exter-nal oblique ridge or the ramus is lessthan 1 cm in width, then other donorsites should be considered (Table 2). Ifthe patient has limited jaw opening ortemporomandibular joint dysfunction,compromised clinical access may com-plicate bone harvest. Pericoronitis orother pathology associated with an im-pacted third molar and previous his-tory of mandibular sagittal osteotomyare also contraindications. Althoughuse of the coronoid process as an au-tologous graft has been reported,25,26
the amount of bone for ridge augmen-tation is negligible considering the po-tential postoperative disability of a cor-onoidectomy.27,28
MANDIBULAR RAMUS AS A DONOR SITE
44 Vol. XXVI/No. One/2000
FIGURE 5. Severe alveolar defect from traumatic loss of maxillary central incisor. FIGURE 6. Cortical ramus graft shaped to replace thepalatal bone. FIGURE 7. Onlay of second layer of ramus graft is fixated with screws to provide adequate volume. FIGURE 8. Dense qualityof the incorporated bone graft requires tapping of the implant osteotomy. FIGURE 9. Ideal implant placement. Note the bulk of thereconstructed alveolus. FIGURE 10. Insertion of the single tooth implant crown 4 months later.
Ramus graft harvest
The exposure and preparation of therecipient site are always performedprior to bone harvest. This allows theclinician to completely assess the bonedefect and harvest adequate bone. Italso minimizes the time from harvest
to placement of the bone graft. A man-dibular nerve block is performed, andlocal anesthetic is also infiltrated alongthe buccal vestibule and massetericspace. The incision begins in the buccalvestibule medial to the external obliqueridge and extends anteriorly and lat-
eral to the retromolar pad. Starting theincision on the ascending ramus nohigher than the level of the occlusalplane minimizes the possibility of cut-ting the buccal artery or exposing thebuccal fat pad.29 The incision continuesanteriorly into the buccal sulcus of the
FIGURE 13. Modified notched ramus retrac-tor improves buccal flap retraction and vis-ibility of ramus area for the osteotomies.
FIGURE 14. The four osteotomies for ramusbone harvest.
molar teeth or posterior ridge area. Ifthe posterior mandible is the recipientsite for the graft, the incision shouldbisect the keratinized mucosa on theresidual ridge crest. A mucoperiostealflap is elevated from the mandibularbody, and the masseter muscle is re-flected, exposing the lateral aspect ofthe ramus. The flap is elevated supe-riorly along the external oblique ridgewith a notched ramus retractor to thebase of the coronoid process. Fibersfrom the temporalis muscle insertionmay need to be reflected to gain ac-cess. A modified notched ramus re-tractor has been developed that has abuccal extension for improved flap re-traction during the graft osteotomies
(Ace Surgical Supply, Brockton, Mass)(Fig 13). A surgical headlight is usefulto illuminate the field.
Three osteotomies are made throughthe outer cortical bone to harvest theramus graft. They are described as theexternal oblique cut, the superior ra-mus cut, and the anterior body cut. Afourth partial thickness osteotomy isalso made inferiorly to facilitate frac-ture of the cortical graft from the man-dible (Fig 14). The external oblique os-teotomy is started anterior to the cor-onoid process at a point where ade-
quate thickness develops (7–8 mm). Asmall fissure bur in a straight hand-piece is used to make a cut completelythrough the outer cortex along the an-terior border of the ramus. This oste-otomy is made approximately 3–5 mmmedial to the external oblique ridge.Pilot holes may be first drilled throughthe cortex along the planned osteoto-my and connected using the bur or re-ciprocating saw blade. The externaloblique osteotomy may be extendedanteriorly into the body of the mandi-ble as far as the distal aspect of the firstmolar area. The length of this cut is de-termined by the size of the recipientsite defect. It is typically 15 mm longfor single tooth defects and up to 40mm long for areas where multiple im-plants will be placed. The superior ra-mus cut is made next, starting at thesuperior point of the external obliqueosteotomy. The superior ramus oste-otomy should be perpendicular to theexternal oblique ridge and extend ontothe lateral aspect of the ramus throughthe outer cortex. The anterior body cutis made in the mandibular body ex-tending inferiorly from the second orfirst molar region. The length of thiscut is dependent on the size require-ments of the graft and the position ofthe inferior alveolar canal. The cut isprogressively deepened until bleedingfrom the underlying cancellous bone isvisible to prevent injury to the under-lying neurovascular bundle. The par-tial thickness inferior osteotomy con-necting the superior ramus and ante-rior body cuts may be performed with3-mm round carbide bur in a straighthandpiece or an oscillating saw. As ac-cess and visibility are limited whenmaking the inferior osteotomy, a moreshallow cut is made into the cortexonly to create a line of fracture (Fig 15).Although this inferior cut is ideallyabove the mandibular canal, it may bemade carefully below the nerve whengraft dimensions require a larger pieceof bone, and the clinician has more ex-perience with procuring bone from thisregion. A thin chisel may be gentlymalletted along the entire length of the
MANDIBULAR RAMUS AS A DONOR SITE
46 Vol. XXVI/No. One/2000
FIGURE 15. Use of a round carbide bur in astraight handpiece for preparation of thepartial thickness inferior ramus cut.
FIGURE 16. A Potts elevator is used to pryand fracture off the ramus graft.
external oblique osteotomy, taking careto parallel the lateral surface of the ra-mus so as to avoid inadvertent injuryto the inferior alveolar nerve. A widerwedge chisel or Potts elevator maythen be inserted and levered to pry thebuccal segment free and complete thesplitting of the graft from the ramus(Fig 16). Following graft harvest, atten-tion should immediately be directed toadapting the block graft to the recipi-ent site. The graft may be stored insterile saline if necessary. No attemptshould be made at harvesting addition-al cancellous bone from the donor site.Any sharp edges around the ramus aresmoothed with a bur or file. A hemo-static dressing (collagen, gelatinsponge, oxidized regenerated cellulose)can be placed into the donor area ifneeded. Closure of the site may becompleted following fixation of thegraft and suturing of the recipient site.The donor site is typically closed witha 3–0 chromic gut continuous lockingsuture.
DISCUSSION
A rectangular piece of cortical boneapproximately 3–5 mm in thickness
may be harvested from the ramus. Thismorphology conforms especially wellas a veneer graft to gain additionalridge width. The size of the block graftshould ideally completely restore thedefect dimensions. The length of therectangular graft may approach 4 cm,but the height usually is not muchgreater than 1–1½ cm.16 These dimen-sions accommodate bone deficienciesinvolving a span of three to four toothsites. Although the symphysis donorsite can offer a thicker bone graft, bonemay be harvested from the ramus ar-eas bilaterally to produce a greater vol-ume of available bone.16 The corticalgraft may also be sectioned, and thesegments may be layered upon eachother to produce a thicker graft (Figs6, 7). This bone can also be particulat-ed in a bone mill and used in sinusgrafting.25,30,31 Smaller bone blocks ortrephine cores may be procured fromthe retromolar region between the in-ternal and external oblique lines(Crawford, personal communication).14
Compared to the symphysis region,the ramus donor site is associated withfewer postoperative complications.16
Patients have also shown less cosmeticconcern with bone removal from the
ramus area, and augmentation of thisdonor site has been unnecessary. Post-operative radiographs have revealedbone repair along the external obliqueridge. Wound dehiscence of the vestib-ular incision has occurred with chingrafts but has not been found withposterior donor sites. The alternative ofa sulcular incision for chin harvest canresult in gingival recession around thelower teeth. Patients are less able todiscern sensory disturbances in theposterior buccal soft tissues comparedto the lower lip and chin.16,32 In contrastto the complaints of altered sensationof the lower anterior teeth associatedwith the symphysis donor area, pa-tients have reported no changes intheir molar teeth.16 Subjective observa-tions have been made that indicate thatthe ramus donor site seems to be as-sociated with less postoperative dis-comfort compared to the chin. Thepain associated with the symphysismay be due to irritation from the ac-tion of the perioral musculature duringspeaking and eating. Some patientsmay experience trismus after ramusgraft harvest. A loading dose and post-operative course of anti-inflammatorymedications is recommended to mini-mize edema.
Harvesting bone from the ramus re-quires knowledge of the mandibularcanal anatomy to prevent nerve injury.The mean anteroposterior width of theramus is approximately 30 mm, withthe mandibular foramen usually locat-ed about two-thirds from the anteriorborder.33 Although the buccolingualposition of the mandibular canal is var-iable, the distance from the canal to theinner aspect of the buccal cortex (med-ullary bone thickness) was found to begreatest at the distal half of the firstmolar34 (Fig 17). Therefore, when largergrafts are planned, the anterior bodycut should be made in this area. Thebone cuts are progressively deepeneduntil bleeding from the underlyingcancellous bone is visible.29,33 The buc-cal cortex is typically 3–4 mm thick inthis region33 (Fig 17). Damage to theneurovascular bundle could also occur
Craig M. Misch
Journal of Oral Implantology 47
FIGURE 17. Cross-section of the posteriormandible in the first molar area. The med-ullary bone thickness lateral to the canal isgreatest in this region.
FIGURE 18. Preoperative view of anteriormaxillary bone defect from bicycle accident.
FIGURE 19. Simulated reconstruction of the bone defect using the CT scan with prosthetictemplate (SIM/Plant Software, Columbia Scientific Inc, Columbia, Md).
FIGURE 20. Three-dimensional model milledfrom the CT scan. The maxillary defect isreconstructed with acrylic for use as a sur-gical template.
during sectioning of the graft. Bonechisels should parallel the lateral sur-face of the ramus. If the inferior ramuscut is below the level of the inferior al-veolar canal, graft separation shouldnot be completed until it can be en-sured that the neurovascular bundle isnot entrapped within the graft. Insome cases, the inferior alveolar nervemay even be exposed following boneremoval. Although no permanent in-jury to the inferior alveolar nerve hasoccurred, patients should be aware ofthe risk.
The main limitation of intraoral bonegrafts is the limited supply of autoge-
nous bone. The most common treat-ment planning error is to overestimatethe available bone for harvest from themandible.35 A comprehensive evalua-tion is necessary for the planning ofany reconstructive surgery. In estheticareas, an emphasis must be placed onnot only providing adequate osseousvolume but on developing alveolar
contours as well. Computerized to-mography may be very useful in pre-operative planning36 (Figs 18, 19).Mounted casts and a diagnostic wax-ing of the reconstructed ridge and re-stored dentition are useful in deter-mining the graft size requirements andanalyzing the occlusion. This is alsoused for the fabrication of templates forcomputerized tomography, graft posi-tioning, and implant surgery13,15,35–38
(Figs 20–22).The most common and detrimental
complication associated with onlaybone grafts is wound dehiscence andexposure of the bone during healing.6,35
This is most often due to inadequateflap manipulation and lack of tension-free soft tissue closure. Cortical onlaygrafts must be well fixated and remainunloaded during healing. Block intra-oral grafts are allowed to heal for a
MANDIBULAR RAMUS AS A DONOR SITE
48 Vol. XXVI/No. One/2000
FIGURE 21. Intraoral bone grafts harvestedusing the acrylic templates. The ramus graftis the larger block on the right.
FIGURE 22. Bone grafts shaped and fit intopremaxilla defect. Note the similarity be-tween the reconstructed model and the pa-tient.
minimum of 4 months for maxillary re-cipient sites and 4–6 months for man-dibular sites.35 As these grafts exhibitminimal resorption, predictable gainsin bone volume allow implant place-ment in most planned sites.13,16,20 Astaged treatment plan with implantplacement following graft healing isthe preferred method of reconstruc-tion.35 The density of healed blockmandibular bone grafts has beenfound to be D-1 to D-2 regardless ofthe original quality of the recipientsite.11,13,16,20 An appropriate drilling se-quence for dense bone and tappingmay be necessary for atraumatic im-plant placement. Implant healing timesare based on the healed quality of thegrafted site, which usually results in a4-month healing phase.35 Additionalgraft resorption following implant in-sertion has not been noted radiograph-ically on loaded cases (Hall, ab-stract).8,13,20,39
CONCLUSION
Autogenous bone grafts harvestedfrom the mandible offer several advan-
tages in the reconstruction of alveolarridges for implant placement. Thesegrafts require a short healing periodand exhibit minimal resorption whilemaintaining their dense quality. Theramus area has some advantages overthe mandibular symphysis as a donorsite. They include minimal patient con-cern for altered facial contour, lower in-cidence of incision dehiscence, de-creased complaints of postoperativesensory disturbances of the face andteeth, and proximity to posterior man-dible recipient sites. However, the sur-gical access can be more difficult, andthere are limitations to the size andshape of the graft.
REFERENCES
1. Hammack BL, Enneking WF.Comparative vascularization of autog-enous and homogenous bone trans-plants. J Bone Joint Surg. 1960;42A:811.
2. Male AJ, Gasser J, Fonseca RJ, etal. Comparison of onlay autologousand allogenic bone grafts to the max-illa in primates. J Oral Maxillofac Surg.1983;42:487–499.
3. Boyne PJ. Performance of bonegrafts in reconstructive surgery. In:Williams EF, ed. Biocompatibility of Tis-sue Analogs, Volume II. Boca Raton, Fl:CRC Press, Inc; 1985:1–29.
4. Burchardt H. Biology of bonetransplantation. Orthop Clin North Am.1987;18:187–195.
5. Marx RE. The science of recon-struction. In: Bell WH, ed. Modern Prac-tice in Orthognathic and ReconstructiveSurgery. Philadelphia, Pa: WB SaundersCo; 1992:1449–1452.
6. Tolman DE. Reconstructive pro-cedures with endosseous implants ingrafted bone: a review of the literature.Int J Oral Maxillofac Implants. 1995;10:275–294.
7. Collins TA. Onlay bone graftingin combination with Branemark im-plants. Oral Maxillofac Surg Clin NorthAm. 1991;3:893–902.
8. Jensen J, Sindet-Pedersen S. Au-togenous mandibular bone grafts andosseointegrated implants for recon-struction of the severely atrophied
maxilla: a preliminary report. J OralMaxillofac Surg. 1991;49:1277–1287.
9. Misch CM. Enhance maxillaryimplant sites through symphysis bonegraft. Dent Implantol Update. 1991;2:101–104.
10. ten Bruggenkate CM, Kraaijen-hagen HA, van der Kwast WAM, et al.Autogenous maxillary bone grafts inconjunction with placement of I.T.I. en-dosseous implants. A preliminary re-port. Int J Oral Maxillofac Surg. 1992;21:81–84.
11. Misch CM, Misch CE, Resnik R,et al. Reconstruction of maxillary alve-olar defects with mandibular symphy-sis grafts for dental implants: a prelim-inary procedural report. Int J Oral Max-illofac Implants. 1992;7:360–366.
12. Jensen J, Sindet-Pedersen S, Oli-ver AJ. Varying treatment strategies forreconstruction of maxillary atrophywith implants: results in 98 patients. JOral Maxillofac Surg. 1994;52:210–216.
13. Misch CM, Misch CE. The repairof localized severe ridge defects for im-plant placement using mandibularbone grafts. Implant Dent. 1995;4:261–267.
14. Buser D, Dula K, Belser UC, et al.Localized ridge augmentation usingguided bone regeneration. II. Surgicalprocedure in the mandible. Int J Perio-dont Rest Dent. 1995;15:11–29.
15. Misch CM. Ridge augmentationusing mandibular ramus bone graftsfor the placement of dental implants:presentation of a technique. Pract Per-iodont Aesthetic Dent. 1996;8:127–135.
16. Misch CM. Comparison of intra-oral donor sites for onlay grafting priorto implant placement. Int J Oral Max-illofac Implants. 1997;12:767–776.
17. Koole R, Bosker H, Noormanvan der Dussen F. Secondary autoge-nous bone grafting in cleft patientscomparing mandibular (ectomesenchy-mal) and iliac crest (mesenchymal)grafts. J Cranio-Max-Fac Surg. 1989;17;28–30.
18. Borstlap WA, HeidbuchelKLWM, Freihofer HPM, et al. Early sec-ondary bone grafting of alveolar cleftdefects: a comparison between chin
Craig M. Misch
Journal of Oral Implantology 49
and rib grafts. J Cranio-Max-Fac Surg.1990;18:201–205.
19. Sindet-Pedersen S, Enemark H.Reconstruction of alveolar clefts withmandibular or iliac crest bone grafts: acomparative study. J Oral MaxillofacSurg. 1990;48:554–558.
20. Williamson RA. Rehabilitation ofthe resorbed maxilla and mandible us-ing autogenous bone grafts and os-seointegrated implants. Int J Oral Max-illofac Implants. 1996;11:476–488.
21. Braun TW, Sotereanos GC. Au-togenous regional bone grafting as anadjunct in orthognathic surgery. J OralMaxillofac Surg. 1984;42:43–48.
22. Misch CM. The harvest of ramusbone in conjunction with third molarremoval for onlay grafting beforeplacement of dental implants. J OralMaxillofac Surg. 1999;57:1376–1379.
23. Heggie AAC. The use of man-dibular buccal cortical grafts in bimax-illary surgery. J Oral Maxillofac Surg.1993;51:1282–1283.
24. Jensen J, Reiche-Fischel O, Sindet-Pedersen S. Autogenous mandibularbone grafts for malar augmentation. JOral Maxillofac Surg. 1995;53:88–90.
25. Wood RM, Moore DL. Graftingof the maxillary sinus with intraorallyharvested autogenous bone prior toimplant placement. Int J Oral MaxillofacImplants. 1988;3:209–214.
26. Berry RL, Edwards RC, PaxtonMC. Nasal augmentation using the
mandibular coronoid as an autogenousgraft: report of case. J Oral MaxillofacSurg. 1994;52:633–638.
27. McLoughlin PM, Hopper C,Bowley NB. Hyperplasia of the man-dibular coronoid process: an analysisof 31 cases and a review of the litera-ture. J Oral Maxillofac Surg. 1995;53:250–255.
29. Hall HD. Intraoral surgery. In:Bell WH, ed. Modern Practice in Orthog-nathic and Reconstructive Surgery. Phil-adelphia, Pa: WB Saunders Co; 1992:2111–2139.
30. Wheeler S, Holmes RE, CalhounCJ. Six-year clinical and histologicstudy of sinus-lift grafts. Int J OralMaxillofac Implants. 1996;11:26–34.
31. Lundgren S, Moy P, Johansson C,et al. Augmentation of the maxillary si-nus floor with particulated mandible: ahistologic and histomorphometricstudy. Int J Oral Maxillofac Implants.1996;11:760–766.
32. Hendy CW, Smith KG, RobinsonPP. Surgical anatomy of the buccalnerve. Br J Oral Maxillofac Surg. 1996;34:457–460.
33. Smith BR, Rajchel JL. II. Ana-tomic considerations in mandibular ra-
mus osteotomies. In: Bell WH, ed.Modern Practice in Orthognathic and Re-constructive Surgery. Philadelphia, Pa:WB Saunders Co; 1992:2347–2360.
34. Rajchel J, Ellis E, Fonseca RJ. Theanatomical location of the mandibularcanal: its relationship to the sagittal ra-mus osteotomy. Int J Adult Orthod Or-thognath Surg. 1986;1:37.
35. Misch CM, Misch CE. Intraoralautogenous donor bone grafts for im-plant dentistry. In: Misch CE, ed. Con-temporary Implant Dentistry. St. Louis:Mosby Year-Book Inc; 1998:497–508.
36. Rosenfeld AL, Mecall RA. Theuse of interactive computed tomogra-phy to predict the esthetic and func-tional demands of implant-supportedprostheses. Compend Contin Educ Dent.1996;17:1125–1144.
37. Collins TA, Nunn W. Autoge-nous veneer grafting for improved es-thetics with dental implants. CompendContin Educ Dent. 1994;15:370–376.
38. Misch CM. The use of a templatefor autologous bone grafting alveolardefects prior to implant placement. JProsthodont. 1999;8:47–52.
39. Schliephake H, Neukam FW,Scheller H, et al. Local ridge augmen-tation using bone grafts and osseoin-tegrated implants in the rehabilitationof partial edentulism: preliminary re-sults. Int J Oral Maxillofac Implants.1994;9:557–564.