1 Using Anti-Depressants in the IBS Patient Philip Schoenfeld, MD, MSEd, MSc (Epi) Associate Professor of Medicine Director, Training Program in GI Epidemiology U. of Michigan School of Medicine
Transcript
1
Using Anti-Depressants
in the IBS Patient
Philip Schoenfeld, MD, MSEd, MSc (Epi)
Associate Professor of Medicine
Director, Training Program in GI Epidemiology
U. of Michigan School of Medicine
2
• Abdominal cramping/bloating & frequent loose,
watery stools with urgency or
hard, pellet-like stools with straining
• Associated nausea/dyspepsia/gerd sxs
are commonly present
• Has had multiple diagnostic tests-all normal
• Has tried fiber, lactose-free diet, elimination of
some foods
• Tried anti-spasmodic agents in low doses (e.g., Bentyl®
10 mg bid),laxative (Miralax® 17gm/day) or anti-
diarrheal (Imodium®) prescribed to use “as needed”
My “Average” Severe IBS Patient
3
Is this patient a candidate for
anti-depressant therapy?
What medication should be used?
4
• TCAs and SSRIs are more effective than placebo at
relieving global IBS symptoms, and appear to reduce
abdominal pain
• There are limited data on the safety and tolerability of
these agents in patients with IBS
• For IBS-D, use TCAs
• For IBS-C, use SSRIs
Antidepressants: ACG Recommendations
Brandt LJ et al. Am J Gastroenterol. 2009;104 Suppl 1:S1-35.
5
0
20
40
60
80
100
ITT n=201
Desipramine Placebo
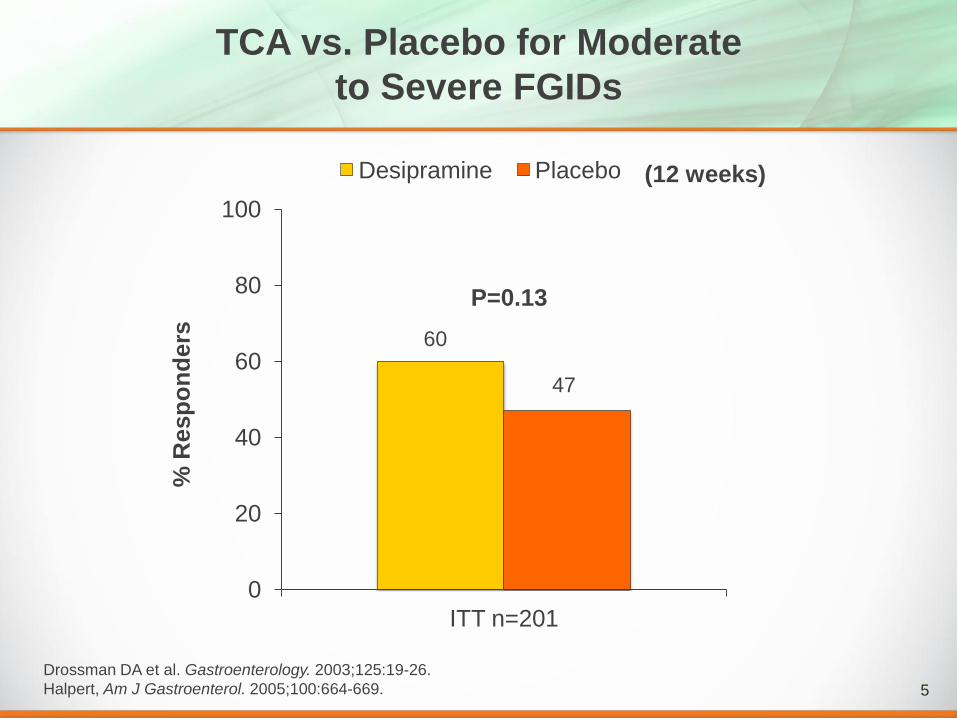
TCA vs. Placebo for Moderate
to Severe FGIDs
Drossman DA et al. Gastroenterology. 2003;125:19-26.
Halpert, Am J Gastroenterol. 2005;100:664-669.
P=0.13
(12 weeks) %
Resp
on
ders
60
47
6
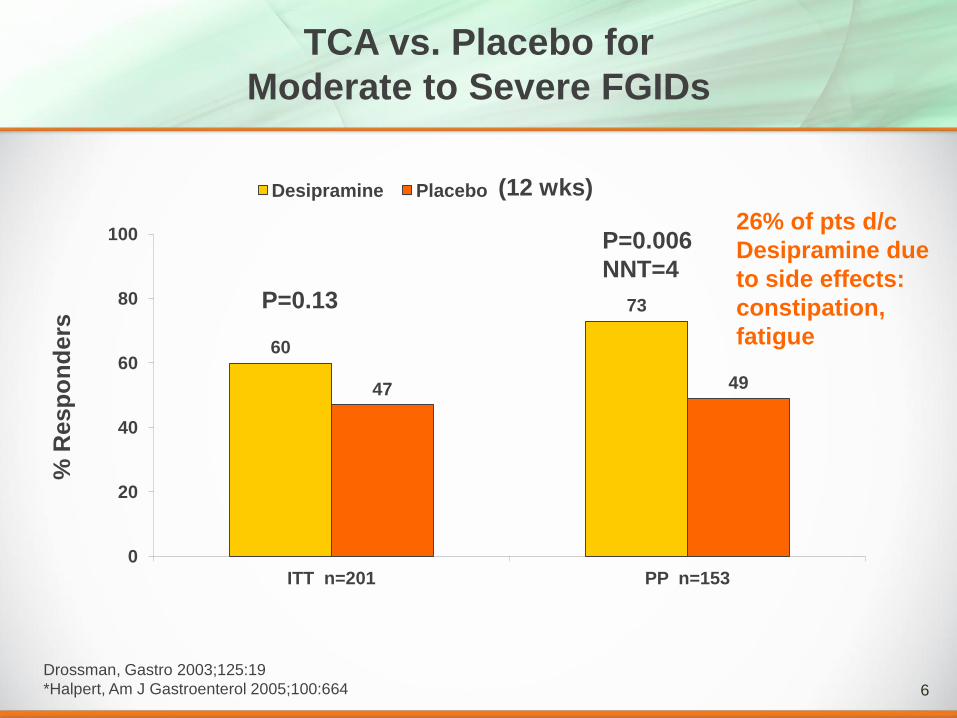
TCA vs. Placebo for
Moderate to Severe FGIDs
Drossman, Gastro 2003;125:19
*Halpert, Am J Gastroenterol 2005;100:664
60
73
47 49
0
20
40
60
80
100
ITT n=201 PP n=153
Desipramine Placebo
P=0.13
P=0.006
NNT=4
26% of pts d/c
Desipramine due
to side effects:
constipation,
fatigue
% R
esp
on
ders
(12 wks)
7
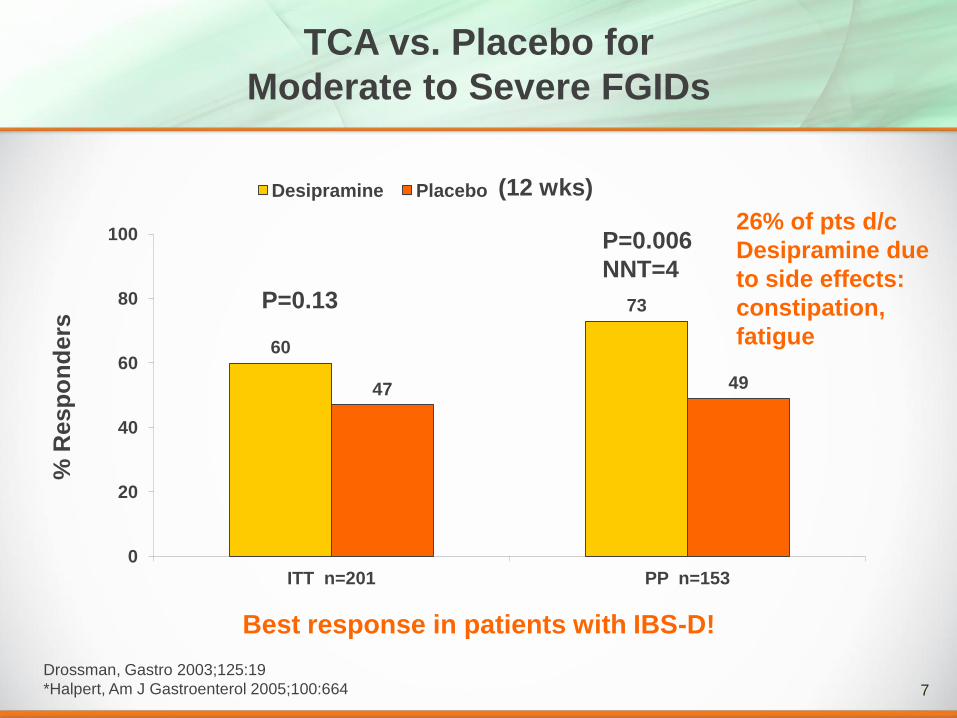
TCA vs. Placebo for
Moderate to Severe FGIDs
Drossman, Gastro 2003;125:19
*Halpert, Am J Gastroenterol 2005;100:664
Best response in patients with IBS-D!
60
73
47 49
0
20
40
60
80
100
ITT n=201 PP n=153
Desipramine Placebo
P=0.13
P=0.006
NNT=4
26% of pts d/c
Desipramine due
to side effects:
constipation,
fatigue
% R
esp
on
ders
(12 wks)
8
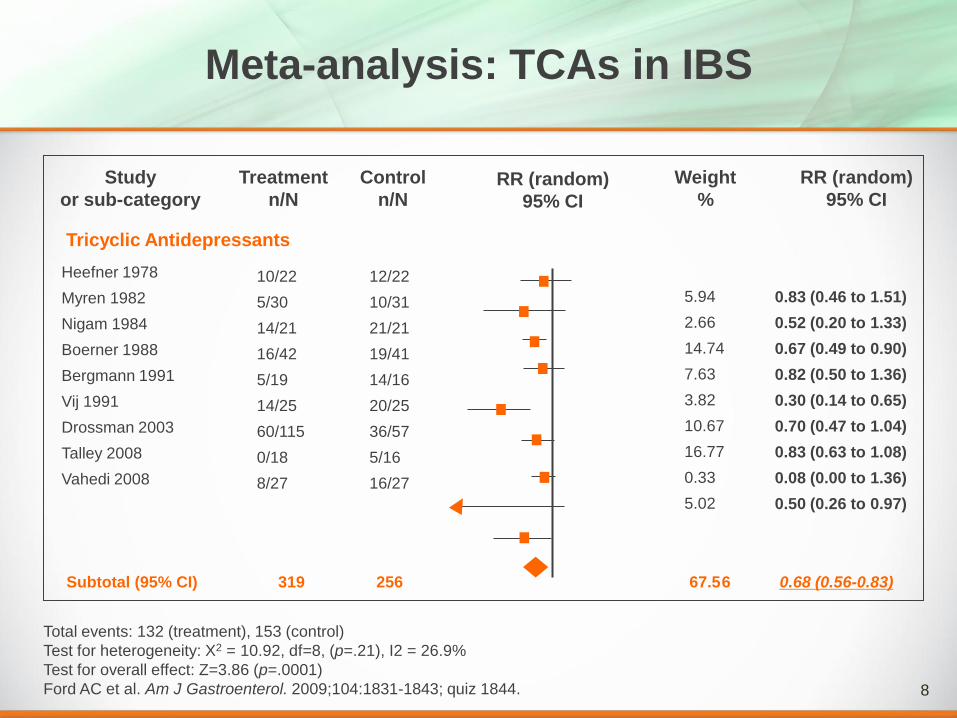
Meta-analysis: TCAs in IBS
Total events: 132 (treatment), 153 (control)
Test for heterogeneity: X2 = 10.92, df=8, (p=.21), I2 = 26.9%
Test for overall effect: Z=3.86 (p=.0001)
Ford AC et al. Am J Gastroenterol. 2009;104:1831-1843; quiz 1844.
Study
or sub-category
Treatment
n/N
Control
n/N RR (random)
95% CI
Weight
%
RR (random)
95% CI
Heefner 1978
Myren 1982
Nigam 1984
Boerner 1988
Bergmann 1991
Vij 1991
Drossman 2003
Talley 2008
Vahedi 2008
10/22
5/30
14/21
16/42
5/19
14/25
60/115
0/18
8/27
12/22
10/31
21/21
19/41
14/16
20/25
36/57
5/16
16/27
Subtotal (95% CI) 319 256 67.56 0.68 (0.56-0.83)
5.94
2.66
14.74
7.63
3.82
10.67
16.77
0.33
5.02
0.83 (0.46 to 1.51)
0.52 (0.20 to 1.33)
0.67 (0.49 to 0.90)
0.82 (0.50 to 1.36)
0.30 (0.14 to 0.65)
0.70 (0.47 to 1.04)
0.83 (0.63 to 1.08)
0.08 (0.00 to 1.36)
0.50 (0.26 to 0.97)
Tricyclic Antidepressants
9
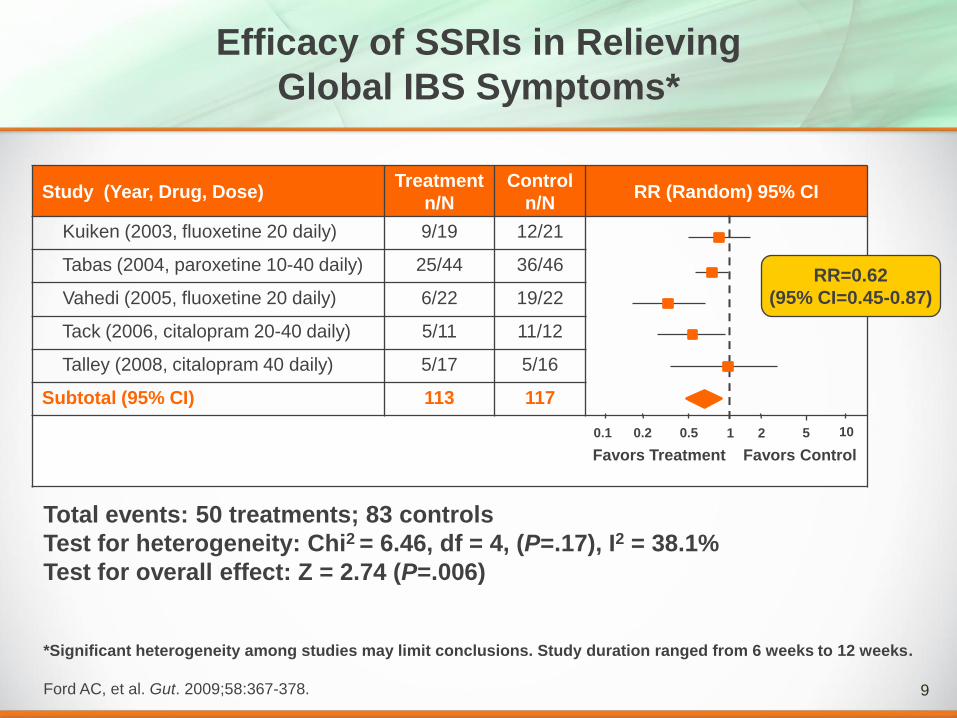
Efficacy of SSRIs in Relieving
Global IBS Symptoms*
*Significant heterogeneity among studies may limit conclusions. Study duration ranged from 6 weeks to 12 weeks.
Ford AC, et al. Gut. 2009;58:367-378.
Study (Year, Drug, Dose) Treatment
n/N
Control
n/N RR (Random) 95% CI
Kuiken (2003, fluoxetine 20 daily) 9/19 12/21
Tabas (2004, paroxetine 10-40 daily) 25/44 36/46
Vahedi (2005, fluoxetine 20 daily) 6/22 19/22
Tack (2006, citalopram 20-40 daily) 5/11 11/12
Talley (2008, citalopram 40 daily) 5/17 5/16
Subtotal (95% CI) 113 117
RR=0.62
(95% CI=0.45-0.87)
0.2 0.5 1 2 5
Favors Treatment Favors Control
0.1 10
Total events: 50 treatments; 83 controls
Test for heterogeneity: Chi2 = 6.46, df = 4, (P=.17), I2 = 38.1%
Test for overall effect: Z = 2.74 (P=.006)
10
If I prescribe anti-depressants, then
am I implying that the patient is simply
depressed or anxious and that her IBS
symptoms are “just in her head”?
11
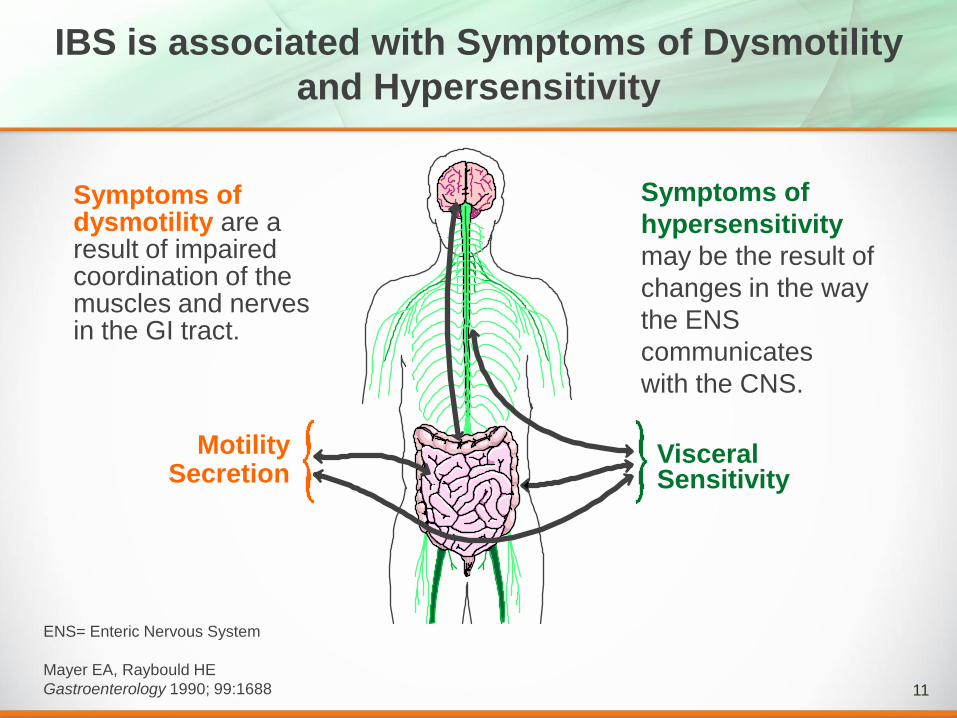
IBS is associated with Symptoms of Dysmotility
and Hypersensitivity
Symptoms of
hypersensitivity
may be the result of
changes in the way
the ENS
communicates
with the CNS.
Symptoms of dysmotility are a result of impaired coordination of the muscles and nerves in the GI tract.