Using the BRAVO Risk Engine toPredict Cardiovascular Outcomesin Clinical Trials With Sodium–Glucose Transporter 2 InhibitorsDiabetes Care 2020;43:1530–1536 | https://doi.org/10.2337/dc20-0227
OBJECTIVE
This study evaluated the ability of the Building, Relating, Assessing, and ValidatingOutcomes (BRAVO) risk engine to accurately project cardiovascular outcomes in threemajor clinical trialsdBI 10773 (Empagliflozin) Cardiovascular Outcome Event Trial inType2DiabetesMellitusPatients (EMPA-REGOUTCOME),CanagliflozinCardiovascularAssessment Study (CANVAS), and Dapagliflozin Effect on Cardiovascular Events–Thrombolysis in Myocardial Infarction (DECLARE-TIMI 58) trialdon sodium–glucosecotransporter 2 inhibitors (SGLT2is) to treat patients with type 2 diabetes.
RESEARCH DESIGN AND METHODS
Baseline data from the publications of the three trials were obtained and enteredinto the BRAVO model to predict cardiovascular outcomes. Projected benefits ofreducing risk factors of interest (A1C, systolic blood pressure [SBP], LDL, or BMI) oncardiovascular events were evaluated, and simulated outcomes were comparedwith those observed in each trial.
RESULTS
BRAVO achieved the best prediction accuracy when simulating outcomes of theCANVASandDECLARE-TIMI58 trials. For EMPA-REGOUTCOME, amildbiaswasobserved(∼20%) in the prediction of mortality and angina. The effect of risk reduction onoutcomes in treatment versus placebo groups predicted by the BRAVOmodel stronglycorrelatedwiththeobservedeffectof riskreductiononthetrialoutcomesaspublished.Finally, the BRAVO engine revealed that most of the clinical benefits associated withSGLT2i treatment are through A1C control, although reductions in SBP and BMIexplain a proportion of the observed decline in cardiovascular events.
CONCLUSIONS
The BRAVO risk engine was effective in predicting the benefits of SGLT2is oncardiovascular health through improvements in commonly measured risk factors,including A1C, SBP, and BMI. Since these benefits are individually small, the use ofthe complex, dynamic BRAVOmodel is ideal to explain the cardiovascular outcometrial results.
Over the last few years, much interest has been placed on cardiovascular outcometrials (CVOTs) in diabetes, particularly those investigating sodium–glucose cotrans-porter 2 inhibitors (SGLT2is), because of their tremendous success in reducingcardiovascular events (1–6). The most striking reductions have been observed in the
1Department of Pharmaceutical Outcomes andPolicy, University of Florida College of Pharmacy,Gainesville, FL2Tulane University School of Public Health andTropical Medicine, New Orleans, LA3Tulane University School of Medicine, NewOrleans, LA
number of hospitalizations for conges-tive heart failure (CHF), mortality, anddecline in kidney function. Less impres-sivebut still positive hasbeen themodestdecline in myocardial infarction (MI) andother atherosclerotic events. The fact thatthese drugs may be associated with asmall increase in the incidence of strokeand amputations has led to questionsabout whether SGLT2is may have lessof an effect on the atherosclerotic pro-cess, implicating that other mechanismsmay underlie the positive results on theheart.SGLT2is block reabsorption of glucose
in the proximal tubule of the kidney,leading to reduced glucose reabsorptionfrom urine into the blood, subsequentcalorie and fluid loss through glycosuria,and sodium depletion in the urine (7).Overall, the reduction in each of theseparameters is modest, yet they yield asignificant drop in blood pressure (BP)and body weight. It is therefore possiblethat, collectively, the weakening of theseknown risk factors jointly leads to some ofthe benefits seen with SGLT2 inhibition.Most patients enrolled in the three
main SGLT2is cardiovascular outcometrialsdBI 10773 (Empagliflozin) Cardio-vascular Outcome Event Trial in Type 2Diabetes Mellitus Patients (EMPA-REGOUTCOME), Canagliflozin CardiovascularAssessment Study (CANVAS), and Dapa-gliflozin Effect on Cardiovascular Events–Thrombolysis in Myocardial Infarction(DECLARE-TIMI 58)dhad high A1C levelsatbaseline ($7%)andwerealreadytakingmetformin as first-line therapy (1,3,4).Whether initiating an SGLT2i before met-formin leads to cardiovascular risk reduc-tion is unknown, as is the efficacy of thisdrug classon reducing risk in patientswithtype 2 diabetes (T2D) and A1C ,7%.Moreover, intensive glycemic control inthe placebo groups of these trials (e.g.,through combination therapy with met-formin and sulfonylureas) may havecaused hypoglycemia and weight gain,further increasing the risk of cardiovas-cular events and mortality. Given thelack of no true equipoise to establish adirect effect of SGLT2is, it has beenchallenging to quantify, evaluate, andexplain the mechanisms responsible forimproved cardiovascular outcomes inSGLT2i-treated patients with T2D.Our previous analysis of data from
large cohorts in clinical practice demon-strated that improved control over three
commonly tested risk factorsdglucose,lipids, and BPdleads to better outcomesand fewer cardiovascular events thansingle or dual risk factor control (8).Although amultiple risk factor reductionstrategy has never been tested in largeclinical trials, a relatively small study(Steno-2) revealed that tight control ofglucose, lipids, and BP among patientswith T2D results in a sustained reductionof cardiovascular events and mortality(9,10). Alongside the limited samplesize, however, all patients enrolled inthe Steno-2 study were Danish and ofEuropean descent, making it difficult togeneralize the trial’s findings to moreheterogenous populations. It is there-fore critical to evaluate the impact ofmultiple risk factor reduction in clin-ical trials with SGLT2is compared withplacebo groups to determine whetherSGLT2 inhibition alone can explain theimproved cardiovascular outcomes seenin patients with T2D.
Recently, our group developed theBuilding, Relating, Assessing, and Vali-dating Outcomes (BRAVO) risk engine(11) based on data from the Action toControl Cardiovascular Risk in Diabetes(ACCORD) trialdone of the largest stud-ies of adults with T2D in the U.S. (12).BRAVO is a patient-level, discrete-time,microsimulation model capable of pre-dicting the onset of diabetes complica-tions over an individual’s life span. Wehave extensively validated the BRAVOriskengine against 18 international trialsand developed a globalization moduleto address region-specific differences.The risk engine is different from othersthat are frequently used (13) in that itaccounts for changes in treatment and isalso based on data from a more diversepatient population.
The current study used BRAVO to pro-ject (3) improvements in cardiovascularoutcomes in clinical trials with SGLT2isbased on collective and individual riskfactor reduction in patients with T2D.
RESEARCH DESIGN AND METHODS
Study FlowThe overview of the study flow is pre-sented in Fig. 1. Themodel validationwasexecuted by comparing the primary andsecondary end points observed in one ofeach SGLT2 trial with the correspondingpredicted end points simulated by theBRAVO model. To facilitate the simula-tion, theBRAVOmodel takes thebaseline
characteristics of each trial to generatethe cumulative incidence of end pointsusing the same length of follow-up forthe corresponding trial. We conductedthe validation for the intervention groupand the control group for each trial. Weevaluated the model’s prediction accu-racy from two aspects: whether themodel can correctly predict the absoluteincidence of each end point, and whetherthe predicted risk reduction (i.e., hazardratio) on each end point matches theobserved risk reduction as a result ofusing SGLT2 inhibition.
The BRAVO Diabetes ModelThe BRAVO diabetes model is a discrete-time patient-level microsimulationmodelat anannual cycle. In each year, themodeluses the BRAVO risk equations tocalculate the risk of a series of end pointsbased on the patient’s baseline character-istics and treatment regimen. These endpoints include macrovascular complica-tions (MI, congestive heart failure [CHF],stroke, revascularization surgery, and an-gina), microvascular complications, andadverse events (end-stage renal disease,blindness, severe pressure sensation loss,and severe hypoglycemia), and all-causeand cardiovascular-related mortality. Pa-rameters of each risk equation are re-ported in great detail in the original study(11). After the risk of each end point iscalculated, the model uses a “randomdraw” technique to decide whether thesimulation patient encounters any ofthe end points based on the calculatedrisks and whether the encounter leadsto a death. The simulation continues toexecute year-by-year until it reachesthe prespecified length of study or afatal event occurs.
After the simulation is completed forall of the patients in the target popula-tion, the simulation results are summa-rized toproduce thepredicted cumulativeincidence of each end point and the pre-dicted risk reduction for SGLT2 inhibitioncompared with the placebo group. Thevalidation was conducted exclusivelyon end points reported by each trial.The simulation flow for the BRAVOmodel is presented in greater detail inthe Supplementary Appendix.
Data ExtractionWe obtained baseline data for each trialarm from the publications of threelarge CVOTsdEMPA-REG OUTCOME (14),
care.diabetesjournals.org Shao, Shi, and Fonseca 1531
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/43/7/1530/630376/dc200227.pdf by guest on 16 January 2022
CANVAS (4), and DECLARE-TIMI 58 (3)dand entered these data into the BRAVOmodel to predict outcomes of interest.Details are summarized in SupplementaryTable2. Incidence rates foreachof theendpoints were extracted from both the pla-cebo and treatment groups of these threetrials. We also pooled clinical efficacyresults of the three active treatmentgroups to simulate the impact of empagli-flozin, canagliflozin, and dapagliflozinindividually and then collectively exam-ine the overall effect of SGLT2 inhibition.Details on the treatment effects are sum-marized in Supplementary Table 3. TheMount Hood Network’s Checklist for re-porting model input was used to ensurethe transparency of this simulation ex-periment (15).Values for each risk factor were de-
termined via a sensitivity analysis on theinfluence of lowering A1C, systolic BP(SBP), LDL, or BMI on cardiovascularevents. We then evaluated projectedbenefits of reducing these risk factorsin all three trials and compared thesimulated outcomes to those observedin each trial.
RESULTS
Figure 2 shows correlations betweenpredictions made by the BRAVO modelon the incidence of trial outcomes and theobserved incidence of trial outcomes aspublished. The x-axis of each figure showsthe observed incidence of outcomes per1,000person-years, and they-axispresentsthe predicted incidence of outcomes per1,000 person-years. The 45° diagonal lineindicates 100% prediction accuracy, anddots falling near this line indicate goodprediction accuracy. The BRAVO model
achieved the best prediction accuracywhen simulating the CANVAS andDECLARE-TIMI 58 trials, with most of thedots falling directly on the 100% accuracyline. When simulating the EMPA-REGOUTCOME trial, the BRAVO model wasstill able to predict most of the outcomescorrectly, except for the prediction of mor-tality and angina, where a mild bias wasobserved (;20%).
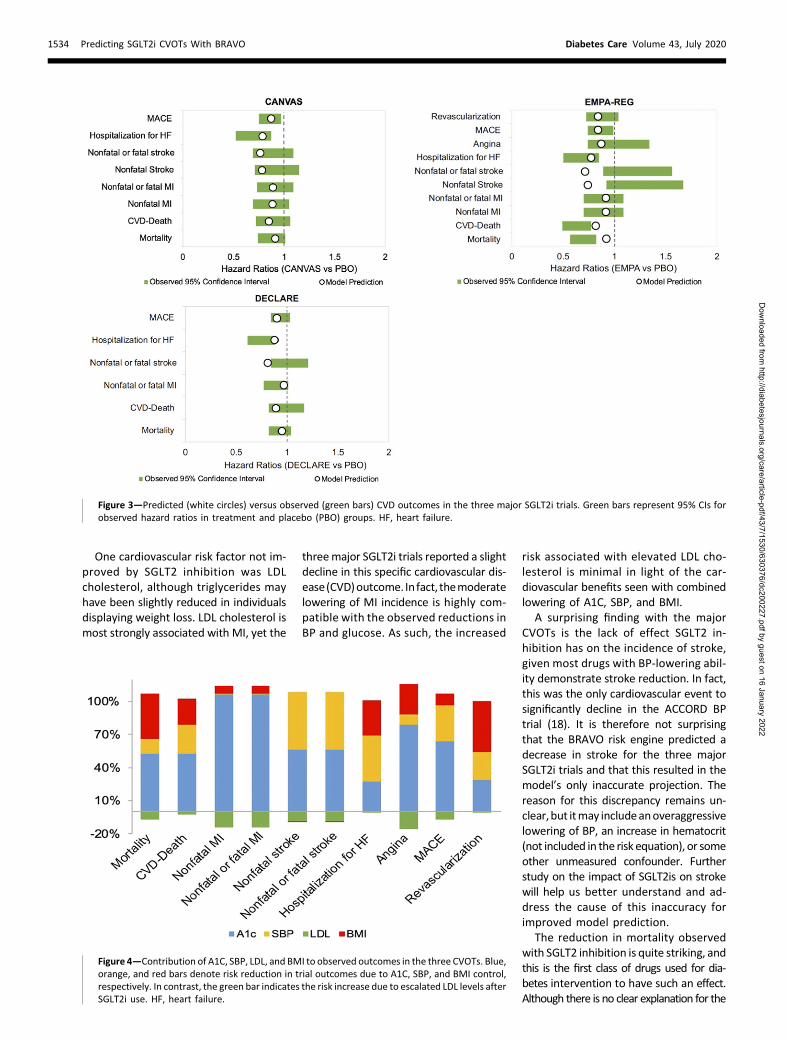
Figure 3 shows correlations betweenthe effect of risk reduction on outcomesin treatment versus placebo groups pre-dicted by the BRAVO model and the ob-served effect of risk reduction on the trialoutcomes as published. Green bars denoteCIs of the observed hazard ratios for eachtrial outcome, and the white dots showpredicted hazard ratios from the BRAVOmodel. With the exception of stroke, pre-dictionsmadeby theBRAVO risk engine fellwithin the confidence limits of the oddsratios for individual outcomes (Fig. 3) for allthree trials. BRAVOpredicted a reduction instroke incidence for each of the three trials;however, no significant change in strokewas observed in the CVOTs.
Figure 4 shows the proportion of ob-served risk reduction explained by eachrisk factor in theCVOTs.Blue,orange, andred bars denote risk reduction in trialoutcomes due to A1C, SBP, and BMIcontrol, respectively. In contrast, greenbars indicate the risk increase due toescalated LDL levels after SGLT2i use.As shown in Fig. 4, most of the clinicalbenefit associated with SGLT2i treat-ment was achieved through A1C con-trol: mortality (50%), MI (100%), stroke(50%), CHF (25%), and major adversecardiac events (MACE; 60%). SGLT2iswere also found to reduce moderately
elevated levels of SBP, explaining aproportion of the observed clinicalbenefit in mortality (15%), stroke (40%),CHF (40%), and MACE (25%), as well aspatient body weight, explaining a propor-tion of the observed risk reduction inmortality (40%) and CHF (30%).
CONCLUSIONS
Using the BRAVO risk engine, we deter-mined that beneficial effects of SGLT2ison commonly measured risk factors(e.g., glycemic index and BP) collectivelyexplain improved outcomes (e.g., re-duced CHF and mortality) seen in theEMPA-REG OUTCOME, CANVAS, andDECLARE-TIMI 58 studies,making it unlikelythat specific reduction of any one factoris directly responsible for the positiveresults observed in these trials.
We and others have previously de-scribed the efficacy of risk factor controlin reducing major cardiovascular eventsand improving survival in patients withT2D (8,10,16). Specifically, attempting tocontrol multiple risk factors simulta-neously appears to have greater po-tential to reduce cardiovascular eventsthan controlling just one factor alone,however well that is done. This is illus-trated by the various arms of the ACCORDtrial, which failed to show benefits of veryrobustly decreasing any single risk factor(17,18). In contrast, despite the fact thatrisk factorcontrol in theSteno-2trial failedto reach target levels in many patients,modest reductions in multiple risk factorsled to significant lowering of cardiovas-cular events and mortality (10). Thesepositive outcomes are reminiscent ofthose observed in the three major SGLT2itrials, which reported significant loweringof A1C in addition to moderate declinesin SBP and BMI.
SGLT2is are known to improve hyper-glycemia and did so in all three CVOTsincluded in this study. In theCANVAS trial(4), for example, a difference of 0.6% inA1C was observed within a few weeks ofrandomization, and the treated groupremained lower than the placebo groupfor the duration of the trial. The con-tribution of hyperglycemia to the dys-function of cardiac muscle, which in itsextreme status has been called “diabeticcardiomyopathy” (19), has been well de-scribed, and multiple studies have dem-onstrated an association between highA1C and hospitalization for CHF (20–26).However, until now, interventions to
Figure 1—Simulation and validation flowchart.
1532 Predicting SGLT2i CVOTs With BRAVO Diabetes Care Volume 43, July 2020
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/43/7/1530/630376/dc200227.pdf by guest on 16 January 2022
reduce hyperglycemia alone have not ledto a reduction in CHF hospitalization. Thisis partly explainedby the fact that someofthe drugs used to treat diabetes, such asthiazolidinediones, may themselves causefluid retention,decline in cardiac function,and hospitalization for heart failure (27).Hypertension remains one of the lead-
ing precursors to the development ofCHF, such that evenmodest reductions inBP are associated with decreased hospi-talizations for heart failure (28). This isparticularly true when the mechanismfor BP reduction includes loss of sodiumand water, as seen with diuretic therapy.In the SGLT2i CVOTs, the consistent re-duction of SBP persisted for the duration
of the trials. Moreover, the reduction inhospitalization for heart failure withSGLT2is to some extent mimics thatseen when a second diuretic is addedto treat patients with known CHF (29). Adecrease in proteinuria and slowing inprogression of chronic kidney diseasecould also be explained by the moderatereductions in BP and glucose. Theseresults very closely resemble the benefitsseen with drugs that block the renin-angiotensin system, such as those re-portedby theHeartOutcomesPreventionEvaluation (HOPE) study, where slight low-ering of BP led to a significant reduction inthe progression of kidney disease (30,31).Other potential actions of SGLT2 inhibition
in the kidney may alternatively lead to theobserved benefits (5,7,32).
In all three CVOTs, hypoglycemia andweight gain were more common in theplacebo group relative to the SGLT2i treat-ment group. In the CANVAS program,body weight fell 3 kg, and the differencebetween groups was maintained throughthe duration of trial (4). Drugs used toimproveglycemiccontrol inT2D(e.g., insulinand sulfonylureas) often lead toweight gain,which itself is associated with heart failure(21), as well as hypoglycemia, which islinked to increased mortality (33,34). It istherefore possible that the weight lossseen with SGLT2is may have been ad-ditive to other risk factor reduction.
Figure 2—Validation plots comparing the predicted incidence of CVD outcomes with the observed incidence of CVD outcomes in placebo (blue) andtreatment (white) groups of the threemajor SGLT2i trials. The y-axis represents the predicted incidence of CVD outcomes per 1,000 person-years, andthe x-axis denotes the actual observed incidence of CVD outcomes. Data points falling on the 45° diagonal lines indicate 100% prediction accuracy. HF,heart failure.
care.diabetesjournals.org Shao, Shi, and Fonseca 1533
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/43/7/1530/630376/dc200227.pdf by guest on 16 January 2022
One cardiovascular risk factor not im-proved by SGLT2 inhibition was LDLcholesterol, although triglycerides mayhave been slightly reduced in individualsdisplaying weight loss. LDL cholesterol ismost strongly associated with MI, yet the
threemajor SGLT2i trials reported a slightdecline in this specific cardiovascular dis-ease(CVD)outcome. Infact, themoderatelowering of MI incidence is highly com-patible with the observed reductions inBP and glucose. As such, the increased
risk associated with elevated LDL cho-lesterol is minimal in light of the car-diovascular benefits seen with combinedlowering of A1C, SBP, and BMI.
A surprising finding with the majorCVOTs is the lack of effect SGLT2 in-hibition has on the incidence of stroke,given most drugs with BP-lowering abil-ity demonstrate stroke reduction. In fact,this was the only cardiovascular event tosignificantly decline in the ACCORD BPtrial (18). It is therefore not surprisingthat the BRAVO risk engine predicted adecrease in stroke for the three majorSGLT2i trials and that this resulted in themodel’s only inaccurate projection. Thereason for this discrepancy remains un-clear,but itmay includeanoveraggressivelowering of BP, an increase in hematocrit(not included in the risk equation), or someother unmeasured confounder. Furtherstudy on the impact of SGLT2is on strokewill help us better understand and ad-dress the cause of this inaccuracy forimproved model prediction.
The reduction in mortality observedwith SGLT2 inhibition is quite striking, andthis is the first class of drugs used for dia-betes intervention to have such an effect.Although there is no clear explanation for the
Figure 3—Predicted (white circles) versus observed (green bars) CVD outcomes in the three major SGLT2i trials. Green bars represent 95% CIs forobserved hazard ratios in treatment and placebo (PBO) groups. HF, heart failure.
Figure 4—Contribution of A1C, SBP, LDL, and BMI to observed outcomes in the three CVOTs. Blue,orange, and red bars denote risk reduction in trial outcomes due to A1C, SBP, and BMI control,respectively. In contrast, the green bar indicates the risk increase due to escalated LDL levels afterSGLT2i use. HF, heart failure.
1534 Predicting SGLT2i CVOTs With BRAVO Diabetes Care Volume 43, July 2020
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/43/7/1530/630376/dc200227.pdf by guest on 16 January 2022
underlying mechanism, it is well recog-nized that elevated glucose levels, BP, andBMI are all associated with increasedmortality and that even modest improve-ments to these parameters can exacer-bate this risk. Our use of the BRAVO riskengine to predict cardiovascular eventssuggests that most of the SGLT2i-relatedbenefits seen in the EMPA-REG OUT-COME, CANVAS, and DECLARE-TIMI 58trials can be explained by improvementsin commonly measured risk factors suchas A1C, BP, and BMI. Since these ben-efits are individually small, a complex,dynamicmodel withmultiple risk factorevaluation is needed to explain the out-come results. The BRAVO risk engine ap-pears to be ideal in this respect.This validation experiment was con-
ductedagainst cardiovascular trials,whichinclude patients exclusively at escalatedCVD risk compared with regular patients inreal-world settings. Whether the BRAVOmodel can achieve a similar predictionaccuracy in real-world settings is morerelevant to the clinical practice; thus, fur-ther examination is strongly encouraged.One challenge is to evaluate the actual“treatment effect” from real-world settingswith sufficient adjustment for confounders,so that validation can be performed tocompare against this effect.With the exception of the preventive
effect of empagliflozin on CHF, which theBRAVO model could not capture throughbiomarkers, use of the BRAVO risk engine inthe current study predicted that the cardio-vascular benefits of SGLT2is relate to actionson traditional biomarkers. This result chal-lenges the belief that SGLT2is act via path-ways unrelated to biomarker control toimprove cardiovascular health. By compar-ing predicted outcomes from the BRAVOmodel and observed outcomes from recentmajor CVOTs, we conclude that the BRAVOmodel can predict benefits of the SGLT2idrug class with high accuracy. This provesthat a novel risk engine developed fromclinical trials (i.e., the BRAVO model) is ca-pable of capturing and explaining the ben-efit of newer classes of antidiabetic drugs.The beneficial effects of SGLT2is on
commonly measured risk factors (e.g.,glycemic index and BP) collectively,rather than single measured or unmea-sured factors, explain improved outcomes(e.g., reduced CHF and mortality) observedin clinical trials with these drugs.
Acknowledgments. The authors thank KathrynCarzoli (Department of Research, Tulane Univer-sity School of Medicine, New Orleans, LA) forassistance in preparation of this manuscript andfor reviewing/editing the manuscript.Funding. V.A.F. is supported in part by theTullis-Tulane Alumni Chair in Diabetes.Duality of Interest. All authors codevelopedthe BRAVO risk engine and have ownershipinterest in BRAVO4Health, a private companythat aims to incorporate such risk assessmentin clinical practice. V.A.F. has received researchgrants (to Tulane) from Bayer, Janssen, andBoehringer Ingelheim and honoraria for consul-tation work from Novo Nordisk, Sanofi, Eli Lilly,and AstraZeneca. No other potential conflicts ofinterest relevant to this article were reported.Author Contributions. H.S. conducted theinitial model analysis. All authors researchedthe data and wrote the manuscript. V.A.F. isthe guarantor of this work and, as such, had fullaccess to all the data in the study and takesresponsibility for the integrity of the data andthe accuracy of the data analysis.
References1. Zinman B, Wanner C, Lachin JM, et al.; EMPA-REG OUTCOME Investigators. Empagliflozin, car-diovascular outcomes, and mortality in type 2diabetes. N Engl J Med 2015;373:2117–21282. McMurray JJV, SolomonSD, Inzucchi SE, et al.;DAPA-HF Trial Committees and Investigators.Dapagliflozin in patients with heart failure andreduced ejection fraction. N Engl J Med 2019;381:1995–20083. Wiviott SD, Raz I, Bonaca MP, et al. Dapagli-flozin and cardiovascular outcomes in type 2diabetes. N Engl J Med 2019;380:347–3574. Neal B, Perkovic V, Mahaffey KW, et al.;CANVAS Program Collaborative Group. Canagli-flozin and cardiovascular and renal events in type2 diabetes. N Engl J Med 2017;377:644–6575. HeerspinkHJL,KosiborodM, InzucchiSE,CherneyDZI. Renoprotective effects of sodium-glucose co-transporter-2 inhibitors. Kidney Int 2018;94:26–396. Kluger AY, Tecson KM, Barbin CM, et al. Car-diorenal outcomes in the CANVAS, DECLARE-TIMI58, and EMPA-REGOUTCOME trials: a systematicreview. Rev Cardiovasc Med 2018;19:41–497. Bakris GL, Fonseca VA, Sharma K, Wright EM.Renal sodium-glucose transport: role in diabetesmellitus and potential clinical implications. Kid-ney Int 2009;75:1272–12778. ShiQ, Liu S, Krousel-WoodM, ShaoH, FonsecaV, Shi L. Long-term outcomes associated withtriple-goal achievement in patients with type 2diabetesmellitus (T2DM).DiabetesResClinPract2018;140:45–549. Gaede P, Lund-Andersen H, Parving HH,Pedersen O. Effect of a multifactorial interven-tion onmortality in type 2 diabetes. N Engl JMed2008;358:580–59110. Gaede P, Vedel P, Larsen N, Jensen GV,Parving HH, Pedersen O. Multifactorial inter-vention and cardiovascular disease in patientswith type 2 diabetes. N Engl J Med 2003;348:383–39311. Shao H, Fonseca V, Stoecker C, Liu S, Shi L.Novel risk engine for diabetes progression andmortality in USA: Building, Relating, Assessing,and Validating Outcomes (BRAVO). Pharmacoe-conomics 2018;36:1125–1134
12. Buse JB, Bigger JT, Byington RP, et al.; ACCORDStudy Group. Action to Control Cardiovascular Riskin Diabetes (ACCORD) trial: design and methods.Am J Cardiol 2007;99:21i–33i13. Stevens RJ, Kothari V, Adler AI, Stratton IM.The UKPDS risk engine: a model for the risk ofcoronary heart disease in type II diabetes (UKPDS56). Clin Sci (Lond) 2001;101:671–67914. Zinman B, Lachin JM, Inzucchi SE. Empagli-flozin, cardiovascular outcomes, andmortality intype 2 diabetes. N Engl J Med 2016;374:109415. Palmer AJ, Si L, Tew M, et al. Computermodeling of diabetes and its transparency: a re-port on the eighthMount Hood challenge. ValueHealth 2018;21:724–73116. Bittner V, Bertolet M, Barraza Felix R, et al.;BARI 2D Study Group. Comprehensive cardiovas-cular risk factor control improves survival: theBARI 2D trial. J AmColl Cardiol 2015;66:765–77317. Ginsberg HN, Elam MB, Lovato LC, et al.;ACCORD Study Group. Effects of combinationlipid therapy in type 2 diabetes mellitus. N Engl JMed 2010;362:1563–157418. CushmanWC, Evans GW, Byington RP, et al.;ACCORDStudy Group. Effects of intensive blood-pressure control in type 2 diabetes mellitus.N Engl J Med 2010;362:1575–158519. Jia G, Whaley-Connell A, Sowers JR. Diabeticcardiomyopathy: a hyperglycaemia- and insulin-resistance-induced heart disease. Diabetologia2018;61:21–2820. AronowWS,AhnC. Incidenceof heart failurein 2,737 older personswith andwithout diabetesmellitus. Chest 1999;115:867–86821. Bahrami H, Bluemke DA, Kronmal R, et al.Novel metabolic risk factors for incident heartfailure and their relationship with obesity: theMESA (Multi-Ethnic Study of Atherosclerosis)study. J Am Coll Cardiol 2008;51:1775–178322. Lindman BR, Davila-Roman VG, Mann DL,et al. Cardiovascular phenotype in HFpEF pa-tients with or without diabetes: a RELAX trialancillary study. J Am Coll Cardiol 2014;64:541–54923. Zhao W, Katzmarzyk PT, Horswell R, et al.Blood pressure and heart failure risk among di-abetic patients. Int J Cardiol 2014;176:125–13224. ZhaoW, Katzmarzyk PT, Horswell R,Wang Y,Johnson J, Hu G. HbA1c and heart failure riskamong diabetic patients. J Clin EndocrinolMetab2014;99:E263–E26725. Erqou S, Lee CT, Suffoletto M, et al. Asso-ciation between glycated haemoglobin and therisk of congestive heart failure in diabetes mel-litus: systematic review and meta-analysis. Eur JHeart Fail 2013;15:185–19326. Gerstein HC, Swedberg K, Carlsson J, et al.;CHARM Program Investigators. The hemoglobinA1c level as a progressive risk factor for cardio-vascular death, hospitalization for heart failure,or death in patientswith chronic heart failure: ananalysis of the Candesartan in Heart failure: As-sessment of Reduction in Mortality and Morbidity(CHARM) program. Arch Intern Med 2008;168:1699–170427. Dormandy JA, Charbonnel B, Eckland DJ,et al.; PROactive Investigators. Secondary pre-vention of macrovascular events in patients withtype 2 diabetes in the PROactive Study (PRO-spective pioglitAzone Clinical Trial In macroVas-cular Events): a randomised controlled trial.Lancet 2005;366:1279–1289
care.diabetesjournals.org Shao, Shi, and Fonseca 1535
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/43/7/1530/630376/dc200227.pdf by guest on 16 January 2022
28. Kannan A, Janardhanan R. Hypertension as arisk factor for heart failure. Curr Hypertens Rep2014;16:44729. Pitt B, Remme W, Zannad F, et al.; Epler-enone Post-Acute Myocardial Infarction HeartFailure Efficacy and Survival Study Investigators.Eplerenone, a selective aldosterone blocker, inpatients with left ventricular dysfunction aftermyocardial infarction. N Engl J Med 2003;348:1309–132130. Heart Outcomes Prevention EvaluationStudy Investigators. Effects of ramipril on car-diovascular and microvascular outcomes in
people with diabetes mellitus: results of theHOPE study and MICRO-HOPE substudy [pub-lished correction appears in Lancet 2000;356:860]. Lancet 2000;355:253–25931. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R,Dagenais G; Heart Outcomes Prevention Evalu-ation Study Investigators. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, oncardiovascularevents in high-risk patients. N Engl J Med 2000;342:145–15332. Woods TC, Satou R, Miyata K, et al. Canagli-flozin prevents intrarenal angiotensinogenaugmentation and mitigates kidney injury
and hypertension in mouse model of type 2diabetes mellitus. Am J Nephrol 2019;49:331–34233. Svensson AM, McGuire DK, Abrahamsson P,Dellborg M. Association between hyper- andhypoglycaemia and 2 year all-cause mortalityrisk in diabetic patients with acute coronaryevents. Eur Heart J 2005;26:1255–126134. ZhaoY,CampbellCR, FonsecaV, Shi L. Impactof hypoglycemia associated with antihypergly-cemic medications on vascular risks in veteranswith type 2 diabetes. Diabetes Care 2012;35:1126–1132
1536 Predicting SGLT2i CVOTs With BRAVO Diabetes Care Volume 43, July 2020
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/43/7/1530/630376/dc200227.pdf by guest on 16 January 2022