119
USMLE EXAM SLIDES!!! Tarek Hassouna
| Date post: | 26-Nov-2014 |
| Category: |
Documents |
| Upload: | tarek-hassouna |
| View: | 201 times |
| Download: | 24 times |
USMLE EXAM SLIDES!!!
Tarek Hassouna

47,XYYPaternal cause @ meiosis II-gamete receiving both copies of one homolog (in this case YY)
Prophase=> crossover
4 chromosomes2 types
2 chromosomes 2 types – All x 2
1 chromosomes 1 types – All x 4

Brachial PlexusBiceps brachialisBiceps brachi
Deltoids
Can not flex elbow!
Cannot ABduct! arm
Cannot extend wrist
Claw hand – lesioned by tauma to heel of hand-fracture of hook of hammate

Nerve innervations of arm
Dr CuMaRadial nerve injury = wrist dropUlnar nerve injury = claw hand Median nerve injury = Ape hand
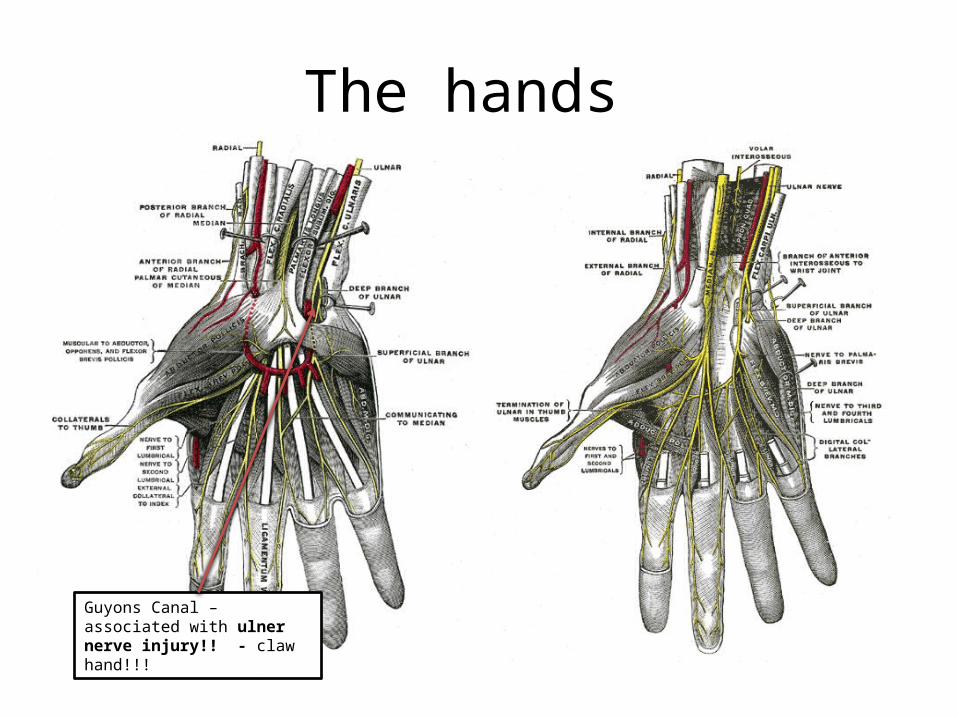
The hands
Guyons Canal – associated with ulner nerve injury!! - claw hand!!!
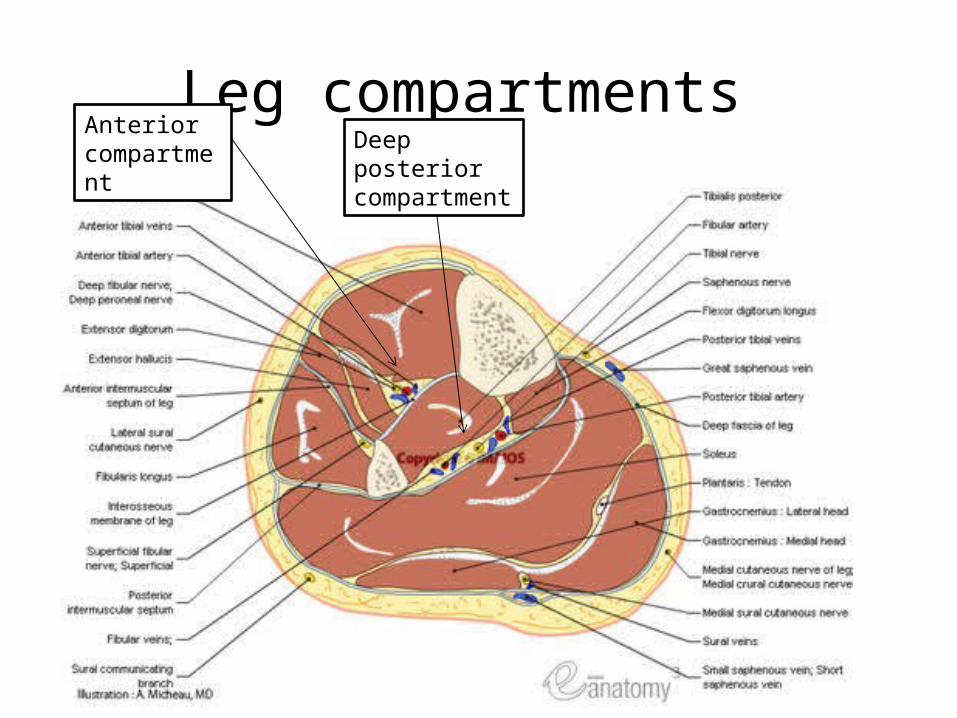
Leg compartments Deep posteriorcompartment
Anterior compartment

Unhappy triad
Medial collateral ligament
Lateral Meniscus
Anterior cruciate ligament
A blow from the lateral side of the knee causes a tearing of the medial coll lig. – occurs among foot players
This occurs because of attachment of the lateral meniscus which tears Medial meniscus is associated with the ACL – so that also tears Thus, you get the unhappy triad…
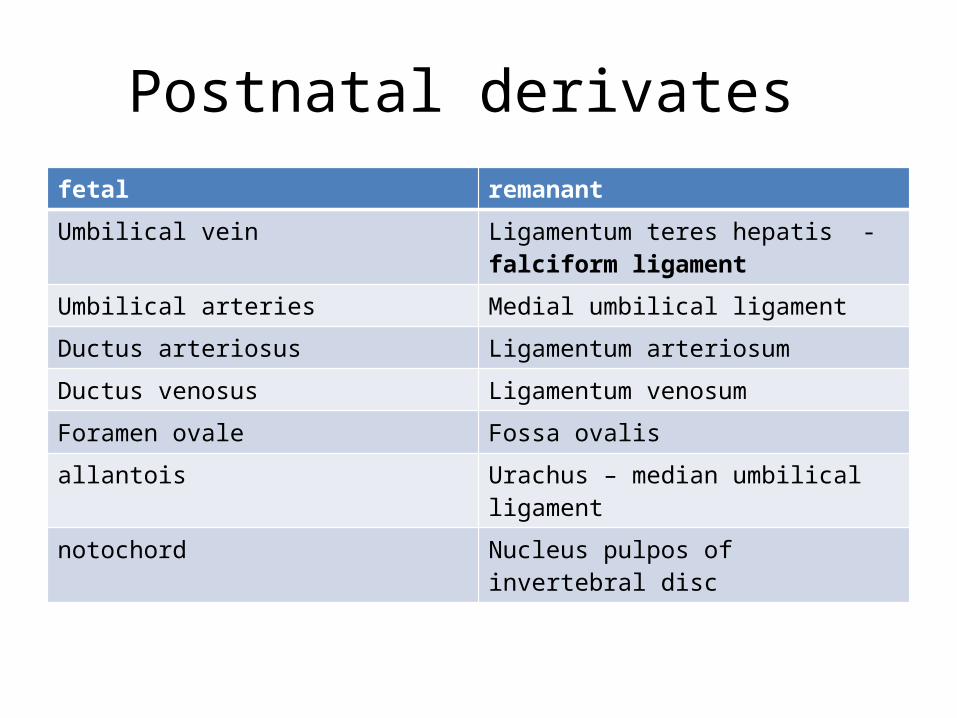
Postnatal derivates fetal remanant
Umbilical vein Ligamentum teres hepatis - falciform ligament
Umbilical arteries Medial umbilical ligament
Ductus arteriosus Ligamentum arteriosum
Ductus venosus Ligamentum venosum
Foramen ovale Fossa ovalis
allantois Urachus – median umbilical ligament
notochord Nucleus pulpos of invertebral disc
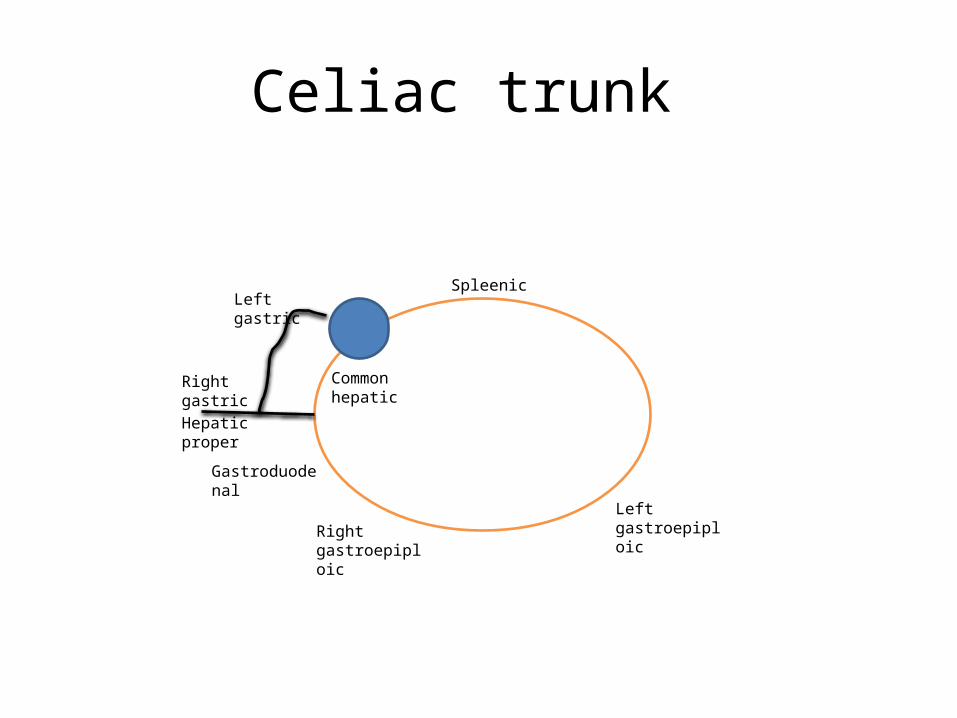
Celiac trunk
Common hepatic
Hepatic proper
Right gastric
Spleenic
Left gastroepiploicRight
gastroepiploic
Gastroduodenal
Left gastric

Hesselbach Triangle indirect hernia-internal deep ring-into the scrotum – compresses sperm chord-infants
Direct hernia -hasselbech triangle -medial to epigastric artery-external ring!!!
Rectus abdominis muscle (medially)Inferior epigastric vessels (superior and laterally).Inguinal ligament, sometimes referred to as Poupart's ligament (inferiorly)

Bilateral hemiparisisContralateral proprioception deficitIpsilateral paralysis of hypoglossyl
Contralateral loss of pain + tempIpsilateral-dysphagia-hoarsness -decreased gag reflex-facial pain + temp-trigeminal nucleus -ataxia
Ipsilateral-faical paralysis-cochlear paralysis-Vestibular -facial pain + temp-dystaxia
Contralateral -homonymous hemianiopia with macular sparing-visual changes
Contralateral-face + arm paralysis + sensory loss-aphasia (dominant)-left sided neglect
Medial surface of brain-leg+ foot area -sensory cortices
Most common site of CoW aneurysm!!-visual field defects
Most common site of aneurysm!!-CNIII palsy
Locked in syndrome- CNIII is intact

Nortrptyiline DesipramineImipramine
ClomipramineAmitriptyline
MoA:
Block the presynaptic reuptake of 5HT + NE + DA-increased levels!!!
Treatment /DOC:
Neuropathic pain
Adverse effects!!
Anticholinergic effects!!Orthostatic HypoTNDry mouth + confusion + sedation
Cardiac tox!!
Things to know!!
Impramine – eneuresisNortryptiline – least orthostatic!!Clomipramine – most serotonergic TCA!!
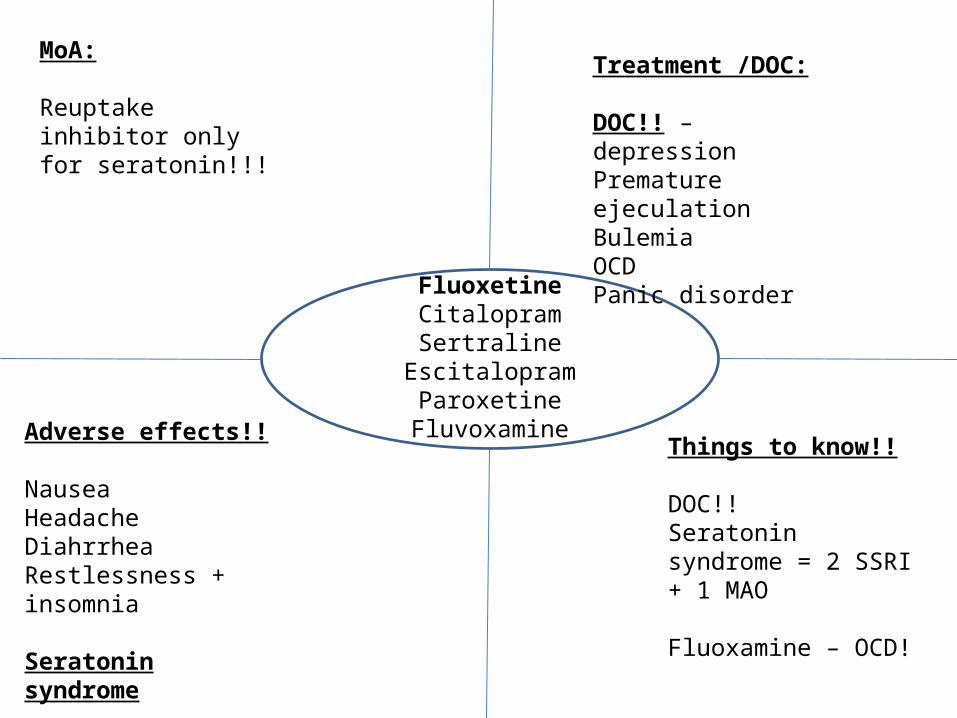
FluoxetineCitalopramSertraline
EscitalopramParoxetine
Fluvoxamine
MoA:
Reuptake inhibitor only for seratonin!!!
Treatment /DOC:
DOC!! – depressionPremature ejeculationBulemiaOCDPanic disorder
Adverse effects!!
NauseaHeadacheDiahrrheaRestlessness + insomnia
Seratonin syndrome
Things to know!!
DOC!!Seratonin syndrome = 2 SSRI + 1 MAO
Fluoxamine – OCD!
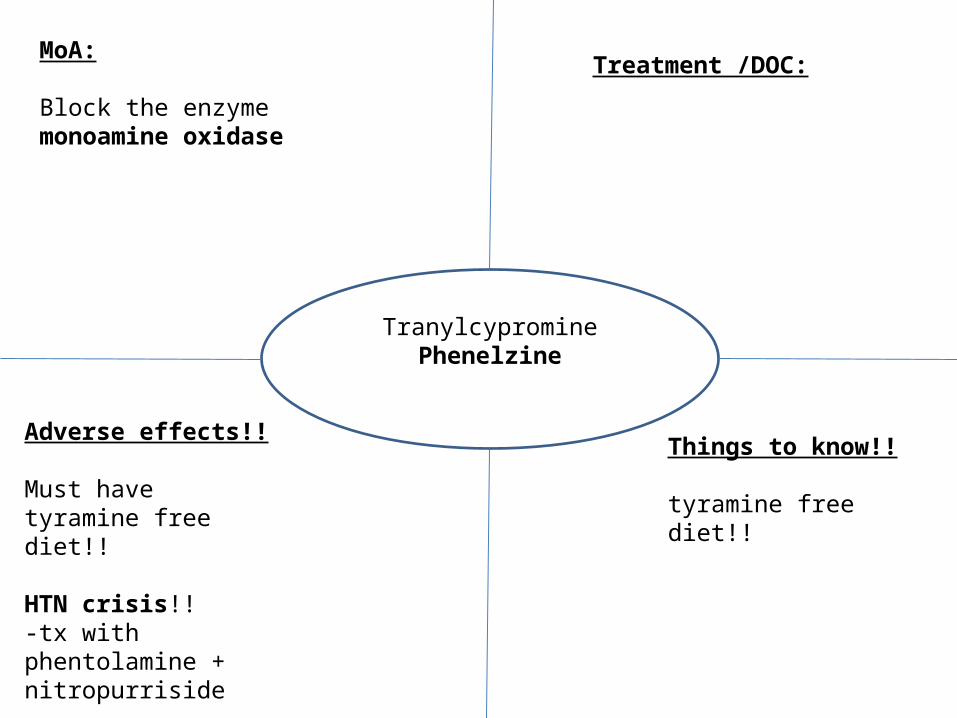
TranylcyprominePhenelzine
MoA:
Block the enzyme monoamine oxidase
Treatment /DOC:
Adverse effects!!
Must have tyramine free diet!!
HTN crisis!!-tx with phentolamine + nitropurriside
Things to know!!
tyramine free diet!!

Calculating + interpreting RiskRisk Equation Interpretation
Odds ratio (a/b)/(c/d) = ad/bc Odds of having disease in exposed group vs. unexposed
Relative Risk a/(a+b) / c/(c+d) getting the disease exposed vs. unexposed
Attributable risk (a/a+b)/(c/c+d) DifferenceExposed vs. unexposed
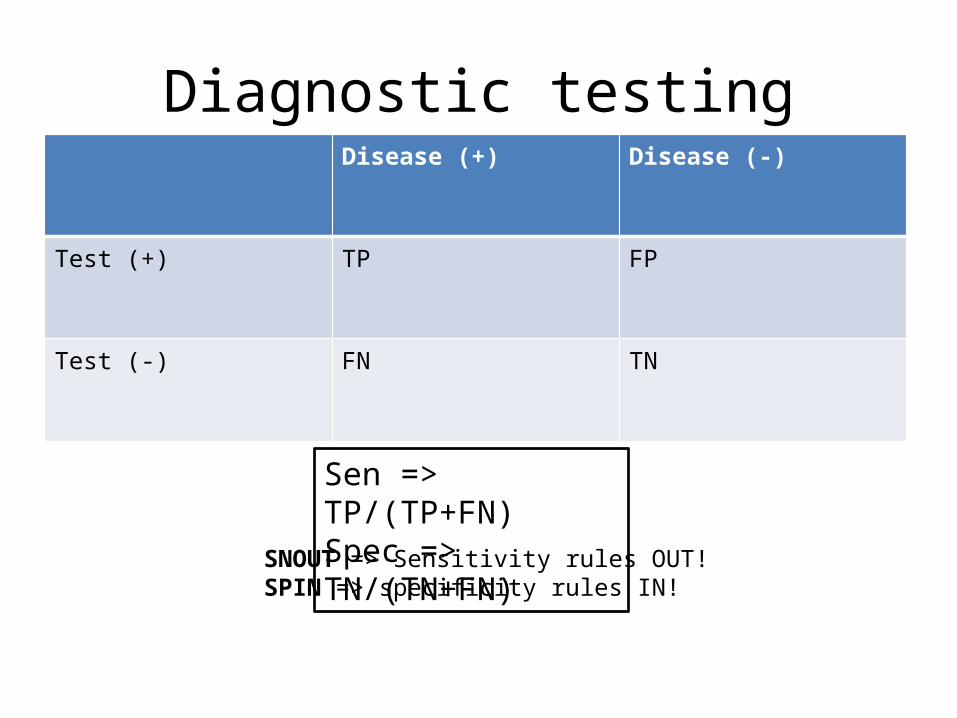
Diagnostic testingDisease (+) Disease (-)
Test (+) TP FP
Test (-) FN TN
Sen => TP/(TP+FN)Spec => TN/(TN+FN)
SNOUT => Sensitivity rules OUT!SPIN => specificity rules IN!

SleepSleep stages description EEG readings
awake Awake + alertActive + mental concentration - Beta waves
Awake but eyes closed - Alpha waves
1 Light sleep
2 Deeper sleep- bruxism
3-4 Deepest non REM sleeepSleepwalking Night terrorBed wetting
REM Dreaming loss of motor toneerections
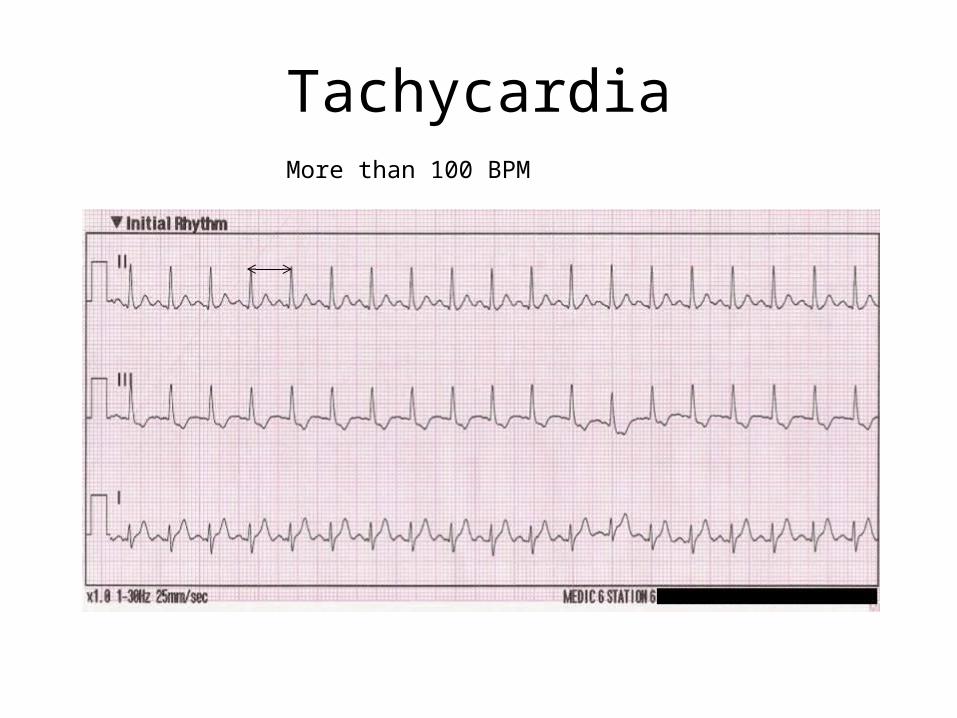
TachycardiaMore than 100 BPM
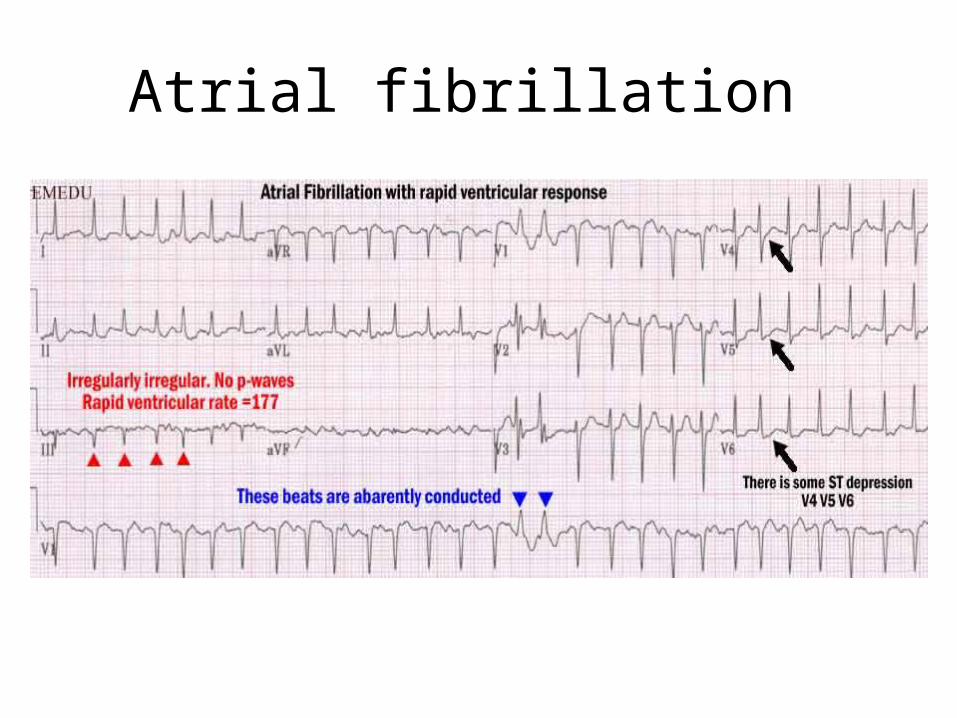
Atrial fibrillation

What to know:-uncoordinated-irregularly irregular -upper chambers quiver – bag of worms appearance
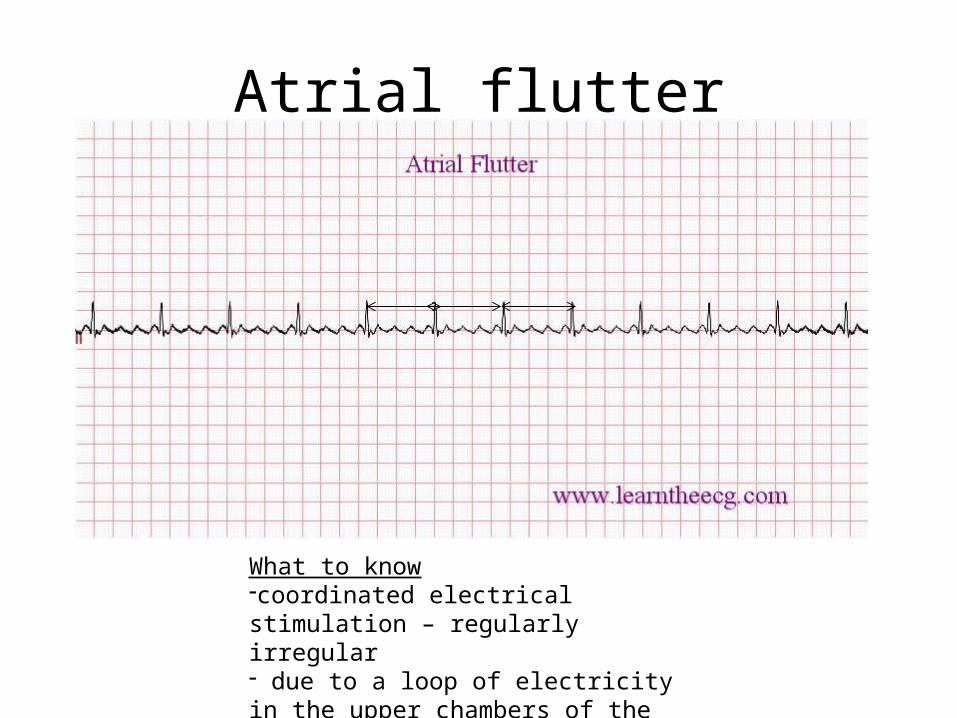
Atrial flutter
What to know-coordinated electrical stimulation – regularly irregular- due to a loop of electricity in the upper chambers of the heart.

Supraventricular tachycardia
What to know:-repeated periods of very fast heartbeats begin and end suddenly-Same as paroxysmal SVT

Wolf-Parkinson White
What do you need to know: - extra (accessory) connection- most common causes of fast heart rate disorders (tachyarrhymthmias) in infants and children

Perfusion vs. Diffusion vs. Airway problemsproblem PaO2 PaCO2 pH RR Clincal
presentation
Restrictive – Perfusion defect
FungusProtozoatesCancer Neuromuscular diseases
Decrease-causes pul HTN!!
decrease increase increases SOB!!Pul HTNNarrow S2Loud S2RV hypertrophyS4 sound – increases on inspiration
Inpiratory crackles + alveolar infilitrates – hyaline disease
Obstructive –airwayBacterial!!
Decreased Increases-CO2 retainer!!! – pneumotactic center stimulated!!
decrease increases TachypneaSOB!!
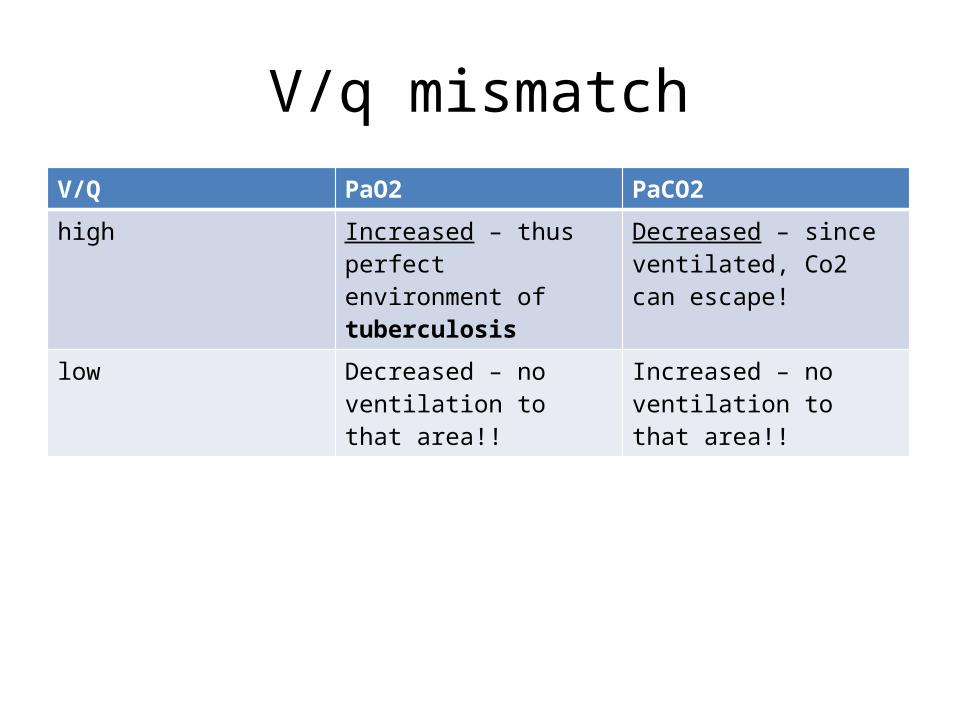
V/q mismatchV/Q PaO2 PaCO2
high Increased – thus perfect environment of tuberculosis
Decreased – since ventilated, Co2 can escape!
low Decreased – no ventilation to that area!!
Increased – no ventilation to that area!!

Antiarrythmics in kids

Ventilatory and ABG patterns in ComaBreathing Pattern
Metabolic Pattern
pH, PaCO2, HCO3
Specific Conditions
HyperventilationHypocapnia => vasoconstriction => decreased CSF formation
CompMetabolic acidosis
pH < 7.3PaCO2 < 40HCO3 < 17
Uremia, DKA, lactic acidosis, acute sepsis, salicylates, methanol, ethylene glycol
HyperventilationHypocapnia => vasoconstriction => decreased CSF formation
Respiratory alkalosis
pH > 7.45PaCO2 < 40HCO3 > 17
Hepatic failure, acute salicylate intoxication, pychogenic causes, sudden onset dyspnea
Hypoventilation Respiratory acidosis
pH < 7.3PaCO2 < 90HCO3 > 17
Respiratory failure from CNS or PNS disease, chest conditions or deformities
Hypoventilation UncompMetabolic alkalosis
pH > 7.45PaCO2 > 45HCO3 > 30
Alkali ingestion. Usually no impairment of consciousness; suspect psychogenicLow volume state!
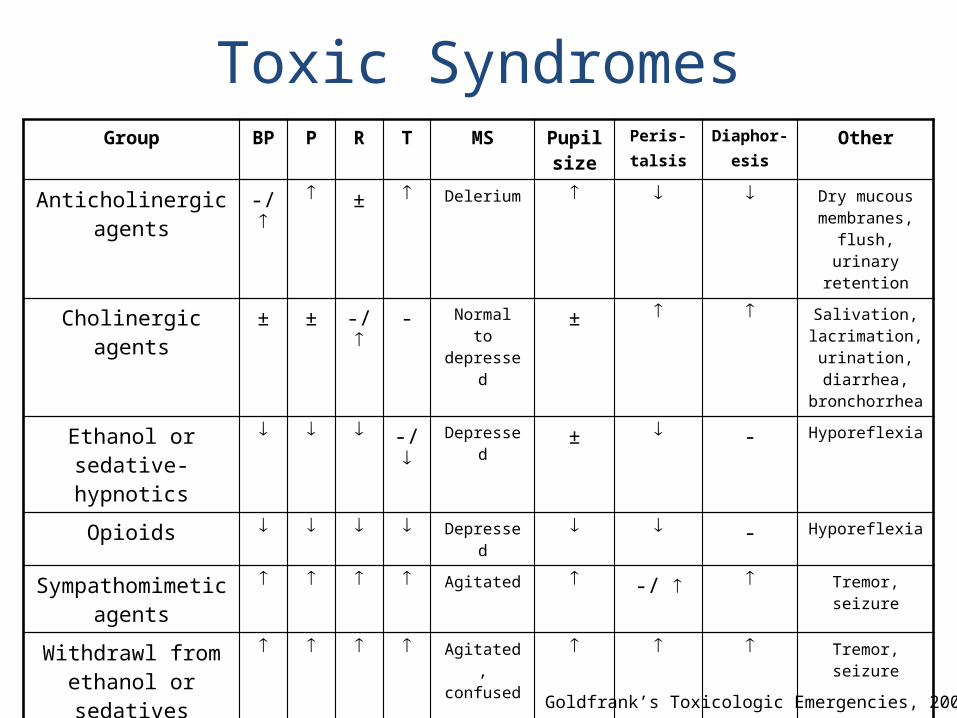
Toxic SyndromesGroup BP P R T MS Pupil
sizePeris-talsis
Diaphor-esis
Other
Anticholinergic agents
-/ ± Delerium Dry mucous membranes, flush, urinary
retention
Cholinergic agents ± ± -/ - Normal to depressed
± Salivation, lacrimation, urination, diarrhea,
bronchorrhea
Ethanol or sedative-hypnotics
-/ Depressed ± - Hyporeflexia
Opioids Depressed - Hyporeflexia
Sympathomimetic agents
Agitated -/ Tremor, seizure
Withdrawl from ethanol or sedatives
Agitated, confused
Tremor, seizure
Withdrawl from opioids
- - Normal, anxious
Vomiting, rhinorrhea,
piloerection, diarrhea
Goldfrank’s Toxicologic Emergencies, 2006
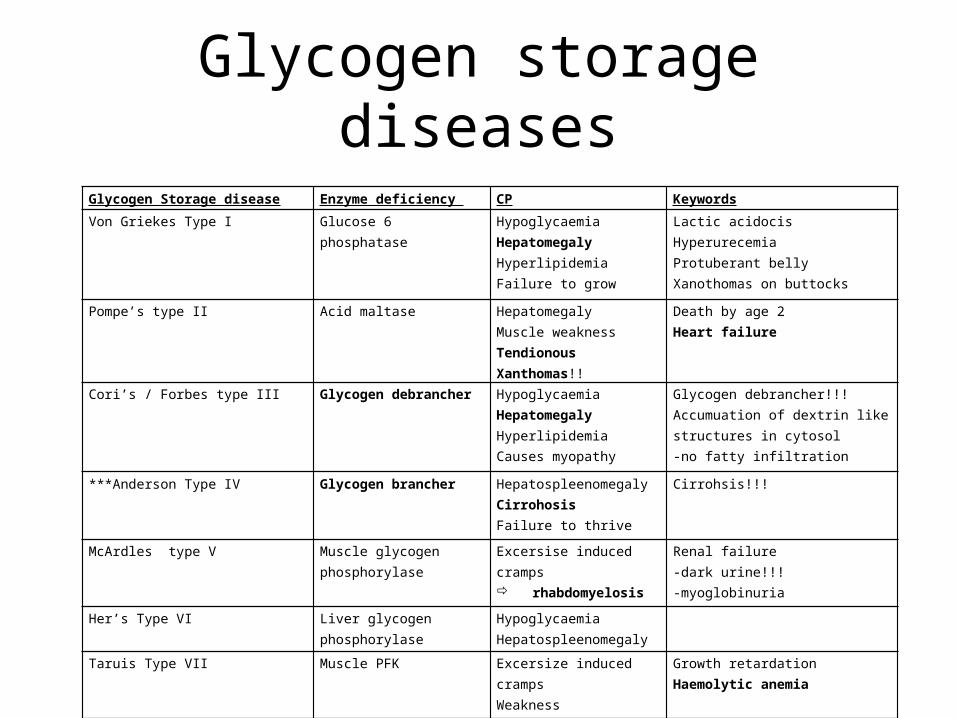
Glycogen storage diseasesGlycogen Storage disease Enzyme deficiency CP Keywords
Von Griekes Type I Glucose 6 phosphatase Hypoglycaemia Hepatomegaly Hyperlipidemia Failure to grow
Lactic acidocis Hyperurecemia Protuberant bellyXanothomas on buttocks
Pompe’s type II Acid maltase Hepatomegaly Muscle weakness Tendionous Xanthomas!!
Death by age 2Heart failure
Cori’s / Forbes type III Glycogen debrancher Hypoglycaemia Hepatomegaly Hyperlipidemia Causes myopathy
Glycogen debrancher!!!Accumuation of dextrin like structures in cytosol-no fatty infiltration
***Anderson Type IV Glycogen brancher Hepatospleenomegaly Cirrohosis Failure to thrive
Cirrohsis!!!
McArdles type V Muscle glycogen phosphorylase
Excersise induced cramps rhabdomyelosis
Renal failure-dark urine!!!-myoglobinuria
Her’s Type VI Liver glycogen phosphorylase HypoglycaemiaHepatospleenomegaly
Taruis Type VII Muscle PFK Excersize induced cramps Weakness
Growth retardation Haemolytic anemia
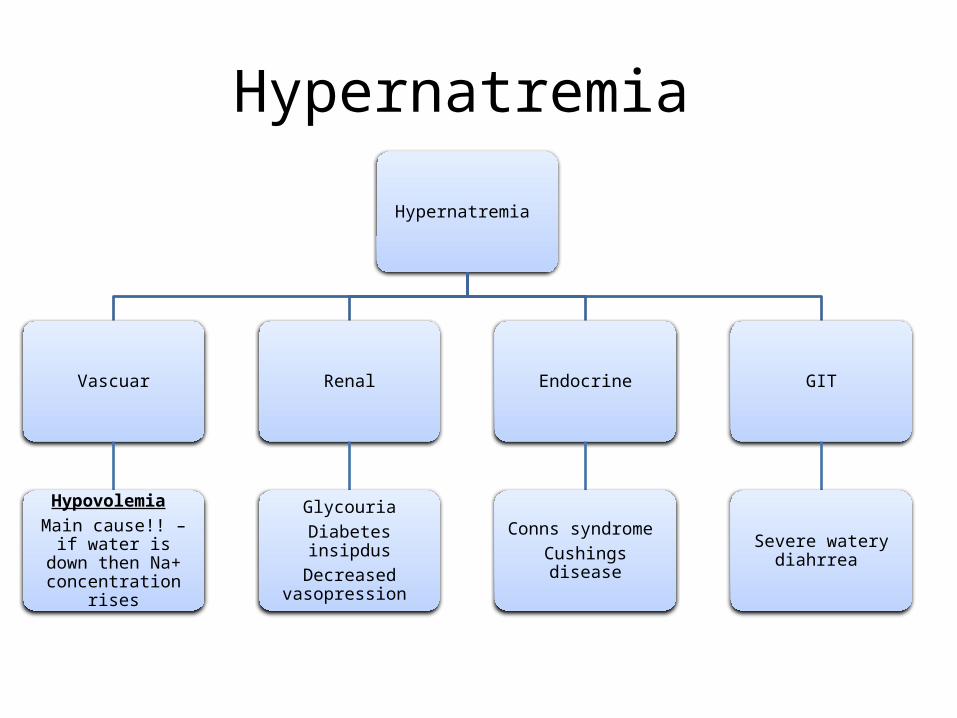
Hypernatremia
Hypernatremia
Vascuar
Hypovolemia Main cause!! – if water
is down then Na+ concentration rises
Renal
GlycouriaDiabetes insipdus
Decreased vasopression
Endocrine
Conns syndrome Cushings disease
GIT
Severe watery diahrrea
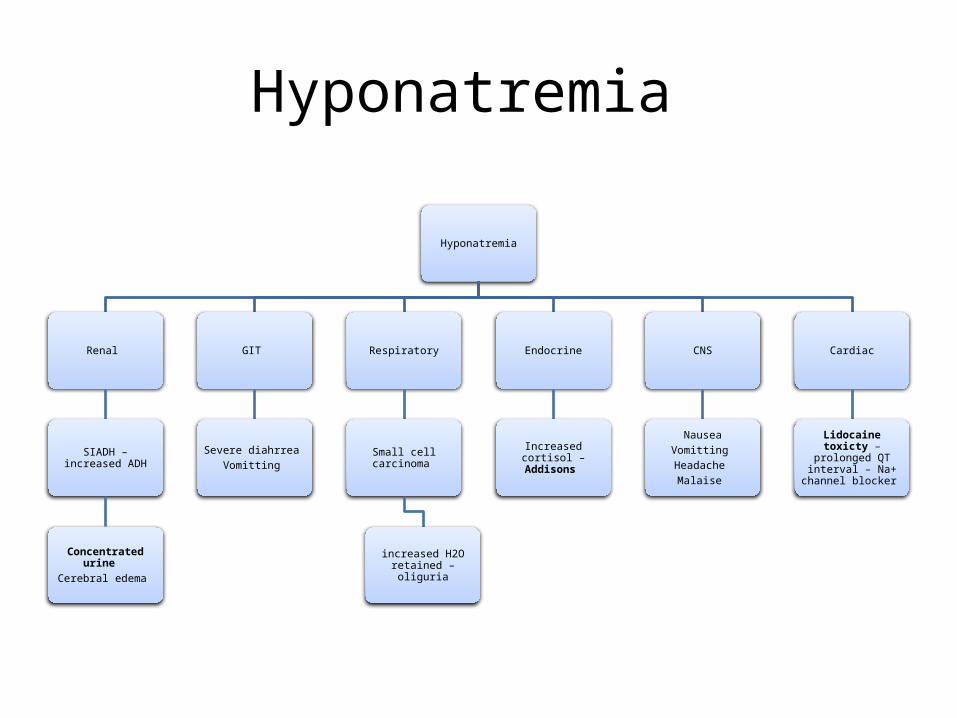
Hyponatremia
Hyponatremia
Renal
SIADH – increased ADH
Concentrated urine Cerebral edema
GIT
Severe diahrrea Vomitting
Respiratory
Small cell carcinoma
increased H2O retained – oliguria
Endocrine
Increased cortisol – Addisons
CNS
NauseaVomitting Headache Malaise
Cardiac
Lidocaine toxicty – prolonged QT interval –
Na+ channel blocker
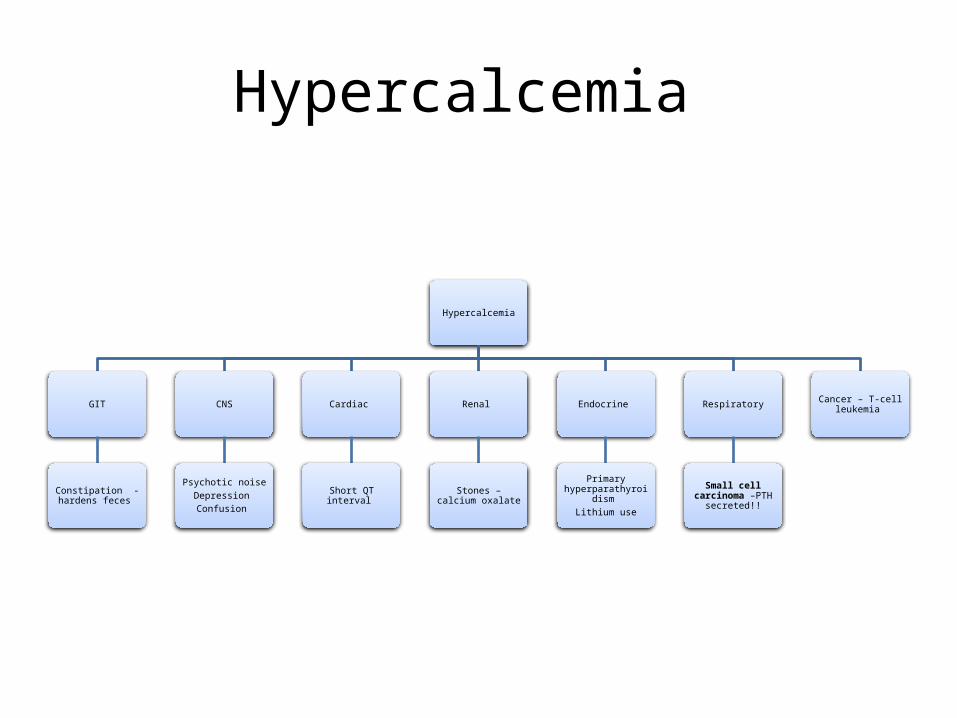
Hypercalcemia
Hypercalcemia
GIT
Constipation - hardens feces
CNS
Psychotic noiseDepression Confusion
Cardiac
Short QT interval
Renal
Stones – calcium oxalate
Endocrine
Primary hyperparathyroidism
Lithium use
Respiratory
Small cell carcinoma –PTH secreted!!
Cancer – T-cell leukemia
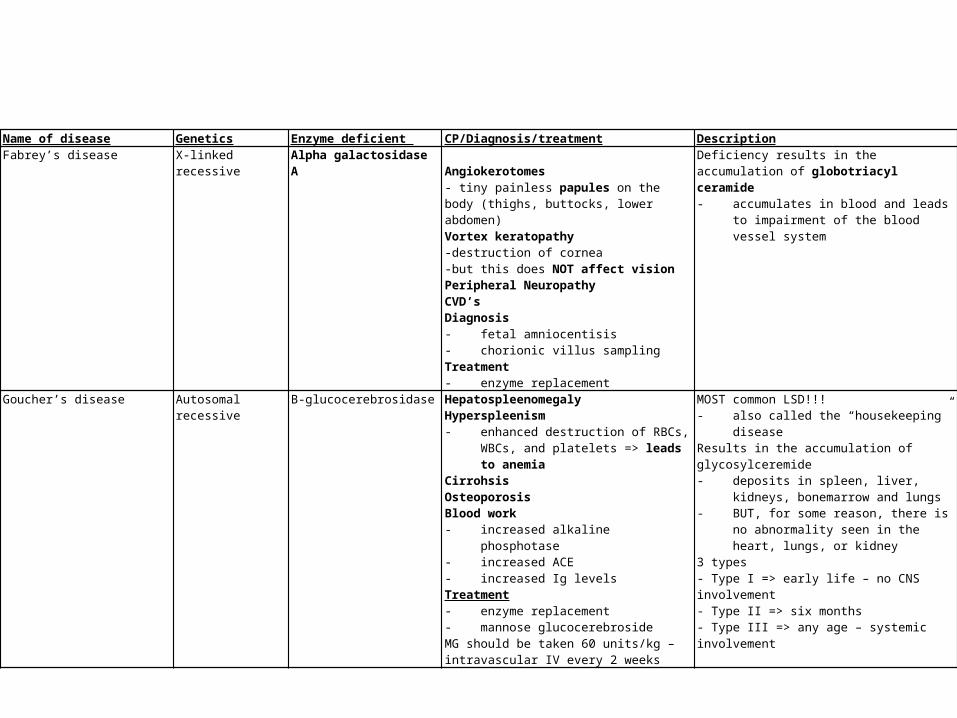
Name of disease Genetics Enzyme deficient CP/Diagnosis/treatment DescriptionFabrey’s disease X-linked recessive Alpha galactosidase A
Angiokerotomes- tiny painless papules on the body (thighs, buttocks, lower abdomen)Vortex keratopathy -destruction of cornea -but this does NOT affect visionPeripheral NeuropathyCVD’s Diagnosis - fetal amniocentisis- chorionic villus sampling Treatment - enzyme replacement
Deficiency results in the accumulation of globotriacyl ceramide - accumulates in blood and leads to impairment
of the blood vessel system
Goucher’s disease Autosomal recessive B-glucocerebrosidase Hepatospleenomegaly Hyperspleenism- enhanced destruction of RBCs, WBCs, and
platelets => leads to anemiaCirrohsisOsteoporosisBlood work- increased alkaline phosphotase- increased ACE- increased Ig levels Treatment- enzyme replacement- mannose glucocerebrosideMG should be taken 60 units/kg – intravascular IV every 2 weeks
MOST common LSD!!!- also called the “housekeeping” diseaseResults in the accumulation of glycosylceremide - deposits in spleen, liver, kidneys,
bonemarrow and lungs - BUT, for some reason, there is no
abnormality seen in the heart, lungs, or kidney
3 types- Type I => early life – no CNS involvement - Type II => six months- Type III => any age – systemic involvement
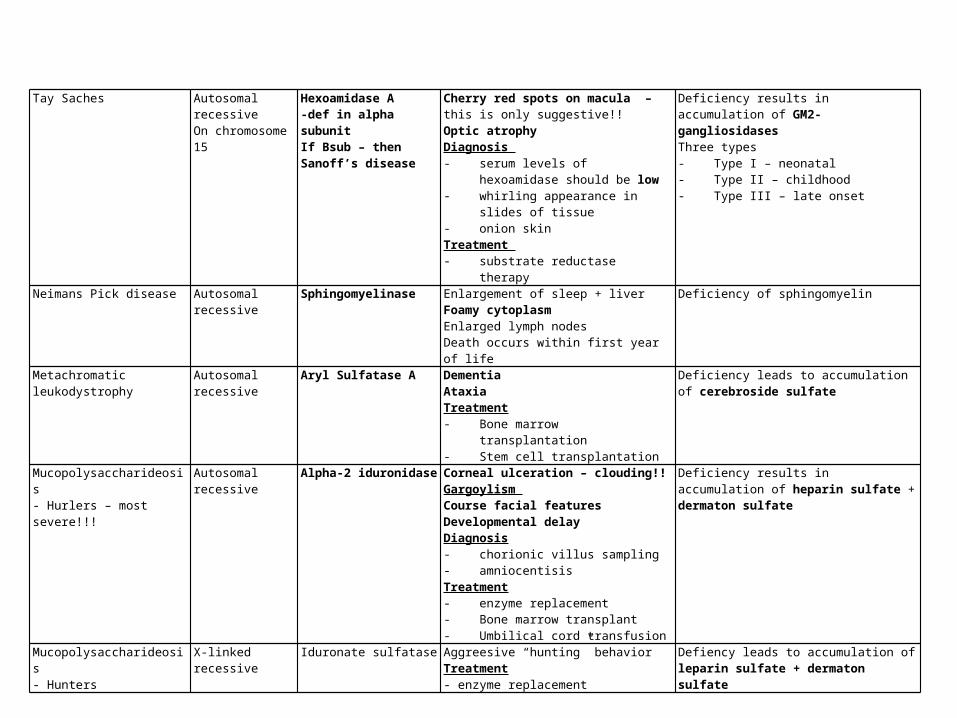
Tay Saches Autosomal recessive On chromosome 15
Hexoamidase A-def in alpha subunitIf Bsub – then Sanoff’s disease
Cherry red spots on macula – this is only suggestive!!Optic atrophy Diagnosis - serum levels of hexoamidase should be
low- whirling appearance in slides of tissue- onion skin Treatment - substrate reductase therapy
Deficiency results in accumulation of GM2-gangliosidases Three types- Type I – neonatal- Type II – childhood- Type III – late onset
Neimans Pick disease Autosomal recessive Sphingomyelinase Enlargement of sleep + liverFoamy cytoplasmEnlarged lymph nodesDeath occurs within first year of life
Deficiency of sphingomyelin
Metachromatic leukodystrophy Autosomal recessive Aryl Sulfatase A DementiaAtaxiaTreatment- Bone marrow transplantation- Stem cell transplantation
Deficiency leads to accumulation of cerebroside sulfate
Mucopolysaccharideosis- Hurlers – most severe!!!
Autosomal recessive Alpha-2 iduronidase Corneal ulceration – clouding!!Gargoylism Course facial featuresDevelopmental delayDiagnosis- chorionic villus sampling- amniocentisis Treatment- enzyme replacement- Bone marrow transplant- Umbilical cord transfusion
Deficiency results in accumulation of heparin sulfate + dermaton sulfate
Mucopolysaccharideosis- Hunters
X-linked recessive Iduronate sulfatase Aggreesive “hunting” behaviorTreatment- enzyme replacement
Defiency leads to accumulation of leparin sulfate + dermaton sulfate

Acid base disorders pH = 6.1 log ([HCO3-]/(0.0301)PCO2
pH can be decreased by decreasing HCO3 or by increasing PCO2 pH can be increased by increasing HCO3 or by decreasing PCO2
pH HCO3 PCO2 compensation
Respiratory alkalosis
increased Decreased – by compensation
Decreased Renal-increased excretion of HCO3
Respiratory acidosis
decreased Increased – by compensation
increased Renal-increased NH4 use!
Metabolic alkalosis
Increased Increased Increased – by compensation
Lungs – keep CO2 – hypoventiliation
Hypokalemia Metabolic acidosis
decreased decreased decerased Lungs – eliminate CO2 – hyperventilation
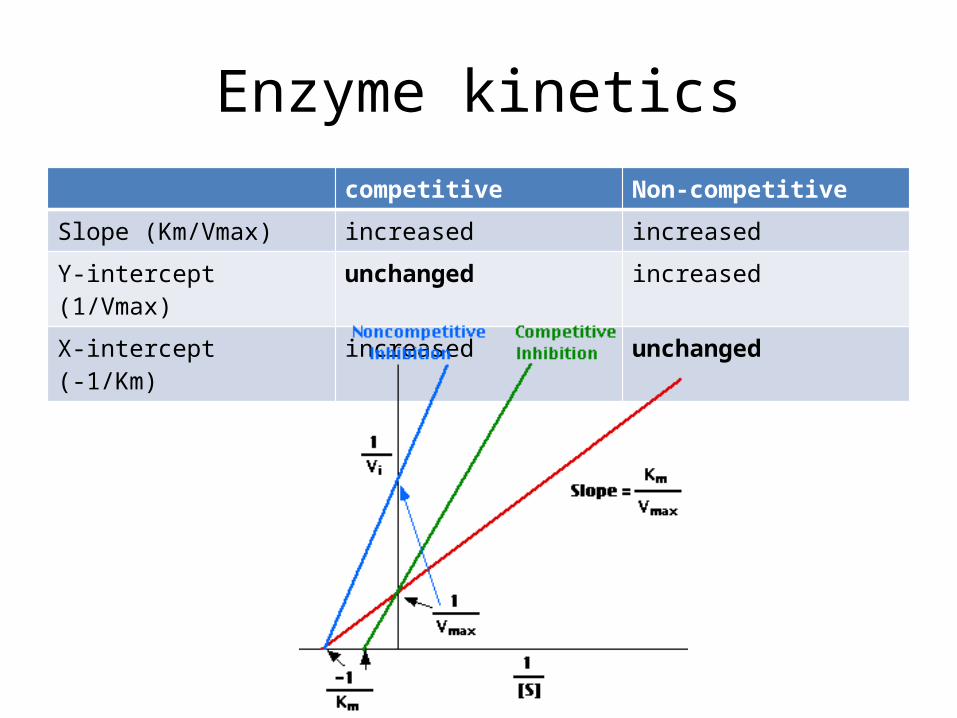
Enzyme kineticscompetitive Non-competitive
Slope (Km/Vmax) increased increased
Y-intercept (1/Vmax) unchanged increased
X-intercept (-1/Km) increased unchanged

O2 binding curve
This occurs at 100% saturation of O2
- When fully saturated, each gram of Hb contains 1.39 mL of O2
This upward spike is due to the fact that the combination of the first heme in Hb and O2 increases affinity for the second, then the third, then the fourth!!
O2 affinity deccreases!!
O2 affinity increases!!
In any case of chronic blood loss – there is less Hb avalible!! – function of it is still normal!!
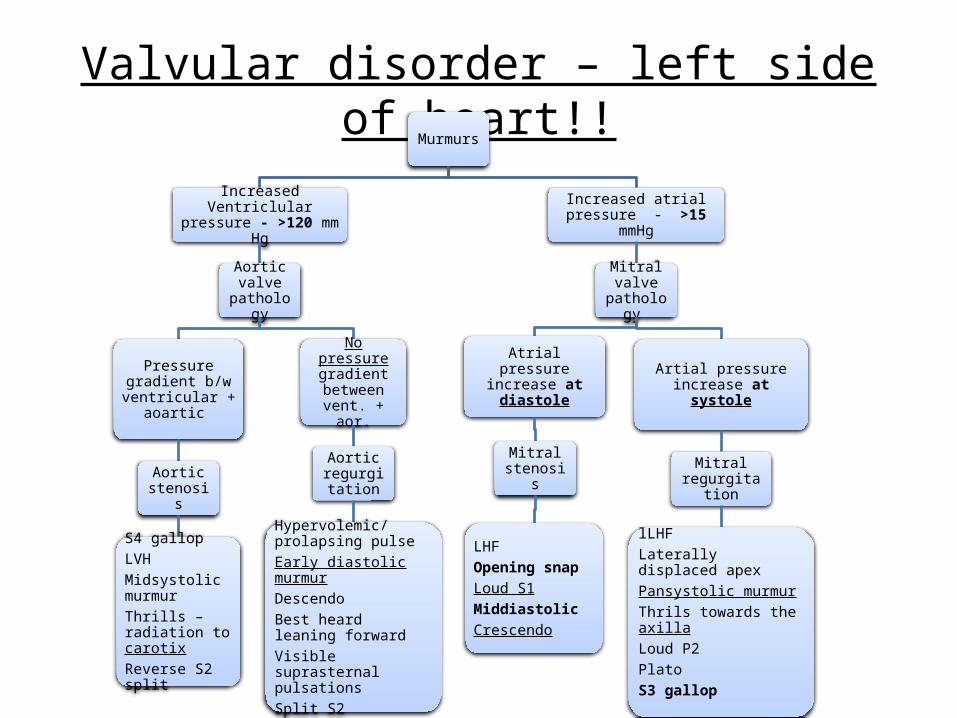
Valvular disorder – left side of heart!!Murmurs
Increased Ventriclular pressure - >120 mm Hg
Aortic valve
pathology
Pressure gradient b/w ventricular +
aoartic
Aortic stenosis
S4 gallopLVHMidsystolic murmurThrills – radiation to carotixReverse S2 split
No pressure gradient
between vent. + aor.
Aortic regurgitati
on
Hypervolemic/prolapsing pulseEarly diastolic murmurDescendoBest heard leaning forwardVisible suprasternal pulsationsSplit S2
Increased atrial pressure - >15 mmHg
Mitral valve
pathology
Atrial pressure increase at diastole
Mitral stenosis
LHFOpening snapLoud S1Middiastolic Crescendo
Artial pressure increase at systole
Mitral regurgitation
lLHFLaterally displaced apexPansystolic murmurThrils towards the axilla Loud P2PlatoS3 gallop
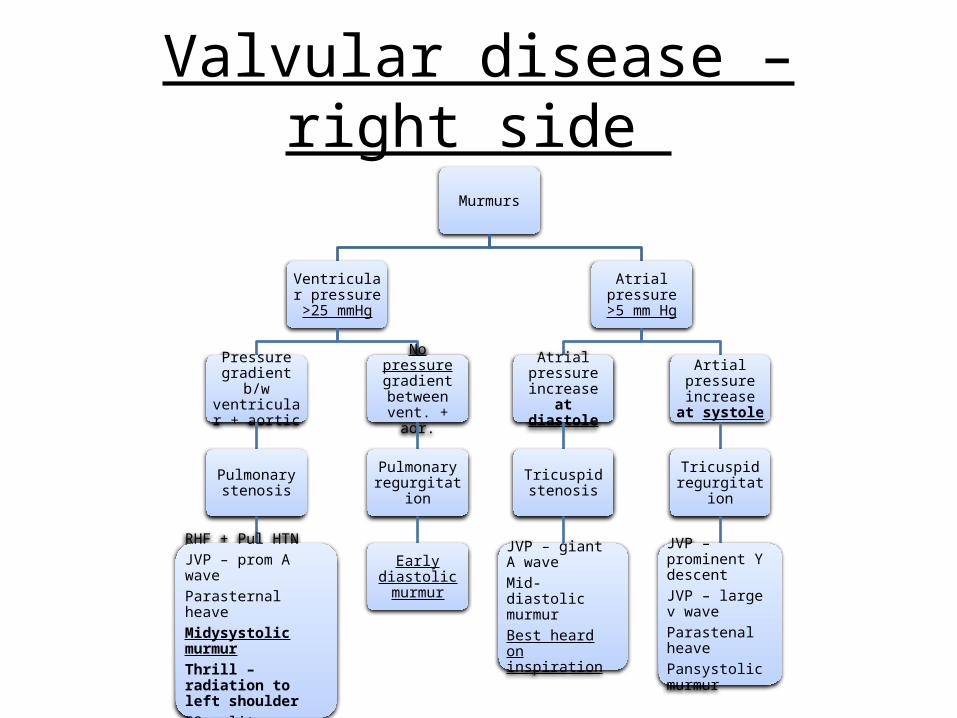
Valvular disease – right side
Murmurs
Ventricular pressure >25
mmHg
Pressure gradient b/w ventricular +
aortic
Pulmonary stenosis
RHF + Pul HTNJVP – prom A waveParasternal heaveMidysystolic murmurThrill – radiation to left shoulderS2 split
No pressure gradient
between vent. + aor.
Pulmonary regurgitation
Early diastolic murmur
Atrial pressure >5 mm Hg
Atrial pressure increase at
diastole
Tricuspid stenosis
JVP – giant A waveMid-diastolic murmurBest heard on inspiration
Artial pressure increase at
systole
Tricuspid regurgitation
JVP – prominent Y descent JVP – large v waveParastenal heavePansystolic murmur
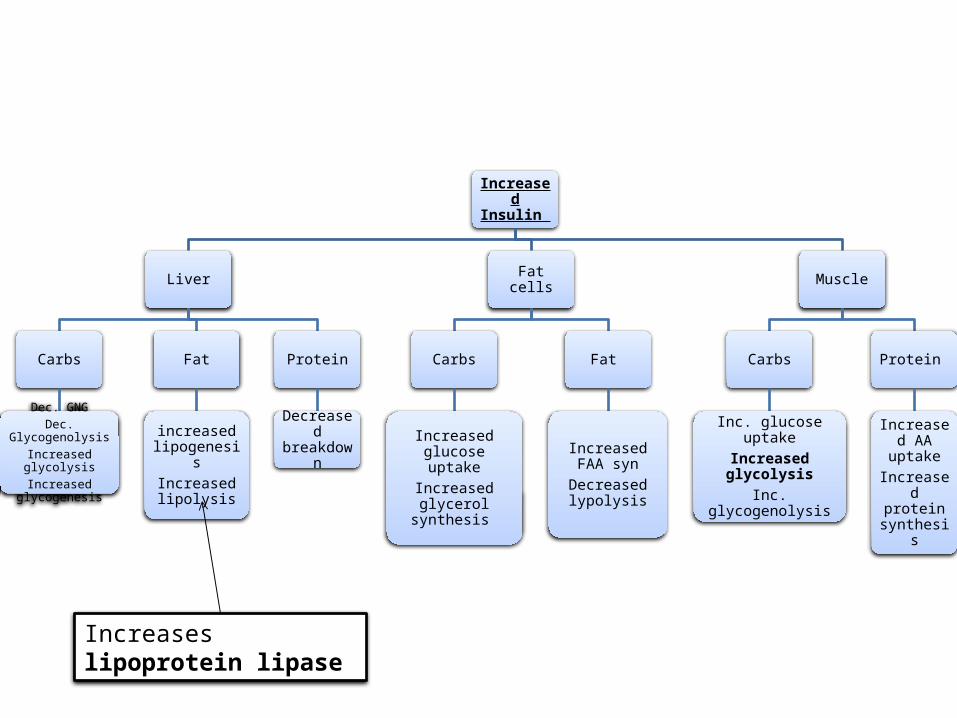
Increased Insulin
Liver
Carbs
Dec. GNGDec. GlycogenolysisIncreased glycolysis
Increased glycogenesis
Fat
increased lipogenesisIncreased lipolysis
Protein
Decreased breakdown
Fat cells
Carbs
Increased glucose uptake
Increased glycerol synthesis
Fat
Increased FAA syn
Decreased lypolysis
Muscle
Carbs
Inc. glucose uptakeIncreased glycolysisInc. glycogenolysis
Protein
Increased AA uptakeIncreased
protein synthesis
Increases lipoprotein lipase

GlycolysisGlucose
G6P
F6P
F16-BP
F26-BP
Glyceraldehyde-3P
DHAP
Glycerol 3P
1,3 BPG
23-BPG
3PG
2 PG
PEP
Pyruvate
Hexokinase+ GIT
PFK 1PFK II
G6P Isomerase
ATP -> ADP + Pi-ATP, Citrate, Glucogon inhibit PFK1 in high amounts
Aldolase
TriosphosphateIsomerase
G3P dehydrogenaseNAD -> NADH
ATP -> ADP + Pi
Phosphoglyceratekinase
ADP + Pi -> ATP >
Phosphoglyceratemutase
PhosphoenolpyruvateEnolase+ H2O
Deficiency is an autosomal recessive disorder•it affects survival of RBCs because RBCs can only rely on glycolysis and nothing else- treatment – spleenectomy and blood transfusion
Lactate
Lactate dehydrogenase
NADH -> NAD + H+
GalactoseGal-1PGlu-1P
GalactokinaseUridyl transferasePhosphogluco mutase
CP: - vomiting, jaundice, hyperbilremia, hyperglycemia, lethargy, cirrohsisTreatment – eat/drink milk products
FructoseF1P
FructokinaseFructose 1P uridyl transferase
Deficiency in FK-fructoseuria – a hereditary condition CP – vomiting, diahrea, apathy, liver damage leading to jaundice•if it reaches the kidney, you get Fanconi syndrome!•Failure of resorption of fructoseThink of expired drugs – adverse reactions cause this syndromeCP: hypophosphatenemia, renal glycosuria, hypourecimia
HemolyticAnemia
Rate limiting Enzymes!!+ Rate limiting step in Glycolysis
Pyruvate Kinase
ADP + Pi -> ATP >
Deficiency leads to galatosemia + galatosuria •causes cataracts and mental retardation at young ages

AlanineAlanine aminotransferase
Deficiency of alpha 1-4 glucosidase •type II Pompes•type III Cori’s •type IV Anderson’s
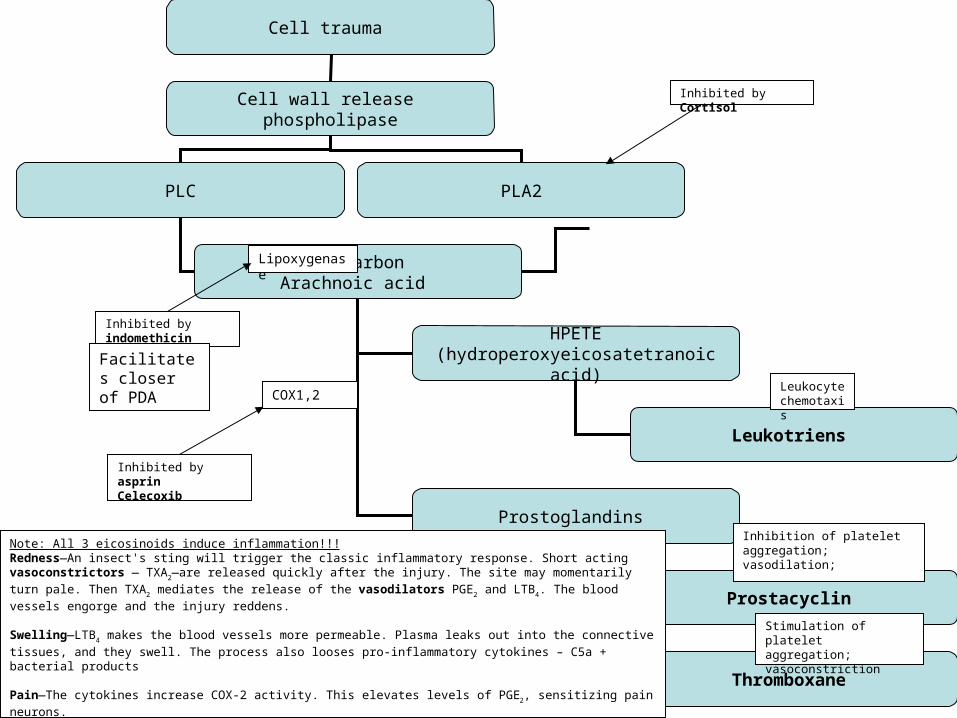
Cell trauma
Cell wall release phospholipase
PLC PLA2
20 carbonArachnoic acid
HPETE (hydroperoxyeicosatetranoic acid)
Prostoglandins
Leukotriens
Prostacyclin
Thromboxane
Lipoxygenase
COX1,2
Inhibition of platelet aggregation;vasodilation;
Inhibited by indomethicin
Inhibited by asprinCelecoxib
Inhibited by Cortisol
Leukocyte chemotaxis
Facilitates closer of PDA
Stimulation of plateletaggregation; vasoconstriction
Note: All 3 eicosinoids induce inflammation!!!Redness—An insect's sting will trigger the classic inflammatory response. Short acting vasoconstrictors — TXA2—are released quickly after the injury. The site may momentarily turn pale. Then TXA2 mediates the release of the vasodilators PGE2 and LTB4. The blood vessels engorge and the injury reddens.
Swelling—LTB4 makes the blood vessels more permeable. Plasma leaks out into the connective tissues, and they swell. The process also looses pro-inflammatory cytokines – C5a + bacterial products
Pain—The cytokines increase COX-2 activity. This elevates levels of PGE2, sensitizing pain neurons.
Heat—PGE2 is also a potent pyretic agent. Aspirin and NSAIDS—drugs that block the COX pathways and stop prostanoid synthesis—limit fever or the heat of localized inflammation.
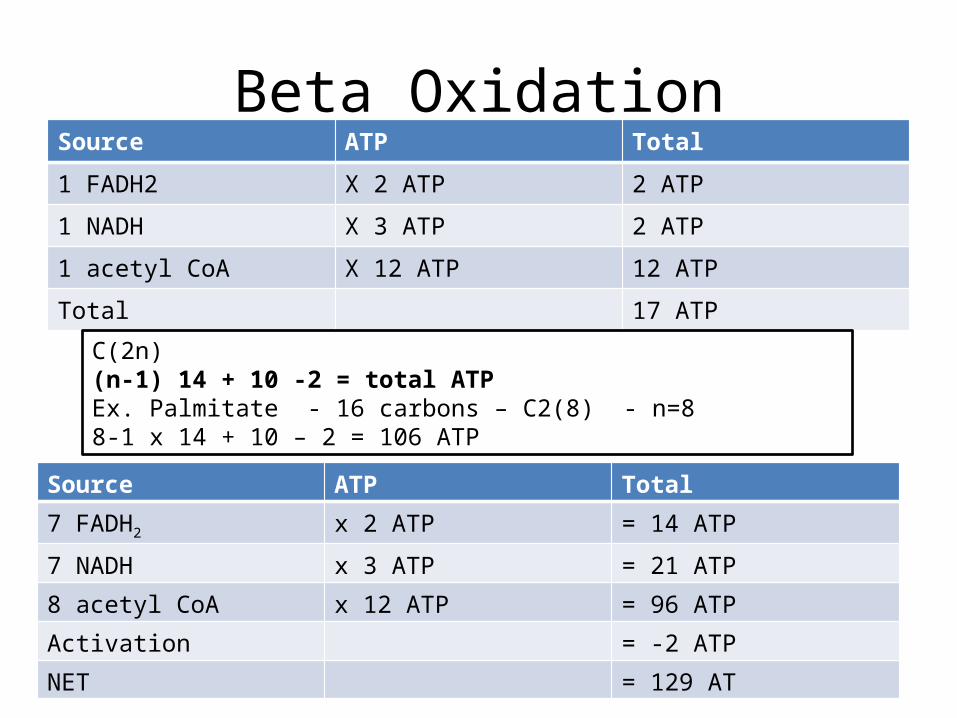
Beta OxidationSource ATP Total
1 FADH2 X 2 ATP 2 ATP
1 NADH X 3 ATP 2 ATP
1 acetyl CoA X 12 ATP 12 ATP
Total 17 ATP
C(2n)(n-1) 14 + 10 -2 = total ATPEx. Palmitate - 16 carbons – C2(8) - n=88-1 x 14 + 10 – 2 = 106 ATP
Source ATP Total
7 FADH2 x 2 ATP = 14 ATP
7 NADH x 3 ATP = 21 ATP
8 acetyl CoA x 12 ATP = 96 ATP
Activation = -2 ATP
NET = 129 AT
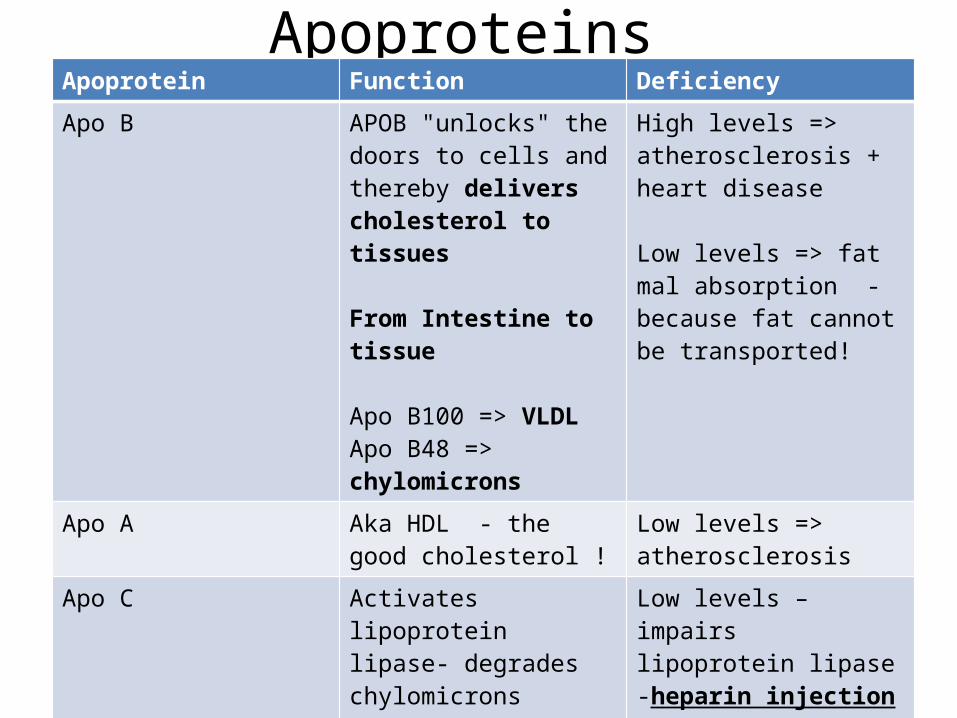
Apoproteins Apoprotein Function Deficiency
Apo B APOB "unlocks" the doors to cells and thereby delivers cholesterol to tissues
From Intestine to tissue
Apo B100 => VLDLApo B48 => chylomicrons
High levels => atherosclerosis + heart disease
Low levels => fat mal absorption - because fat cannot be transported!
Apo A Aka HDL - the good cholesterol !
Low levels => atherosclerosis
Apo C Activates lipoprotein lipase- degrades chylomicrons
Low levels – impairs lipoprotein lipase-heparin injection test
Abdominal pain => pancreatitis
Apo E Allows for liver for chylomicrons + IDL to be taken in by liver
triglyceride and cholesterol levels in blood if deficient

Glomerular filtration rateAfferent Efferent
Assessing-RBF-GFR-Creatinine -Inulin
Assessing-RPF-PAH-BUNPrerenal pathologies – results in afferent constriction!!!
-decreased RBF-decreased GFR-increased Creatinine in plasma!!! – why? Because bowmens oncotic pressure is decreased – thus, “sucking power” is decreased!!!
In response -renin -> ang II constricts efferent arterioles-decreased RPF-decreased PAH-decreased BUN in blood
BUT then...turns into renal!!!
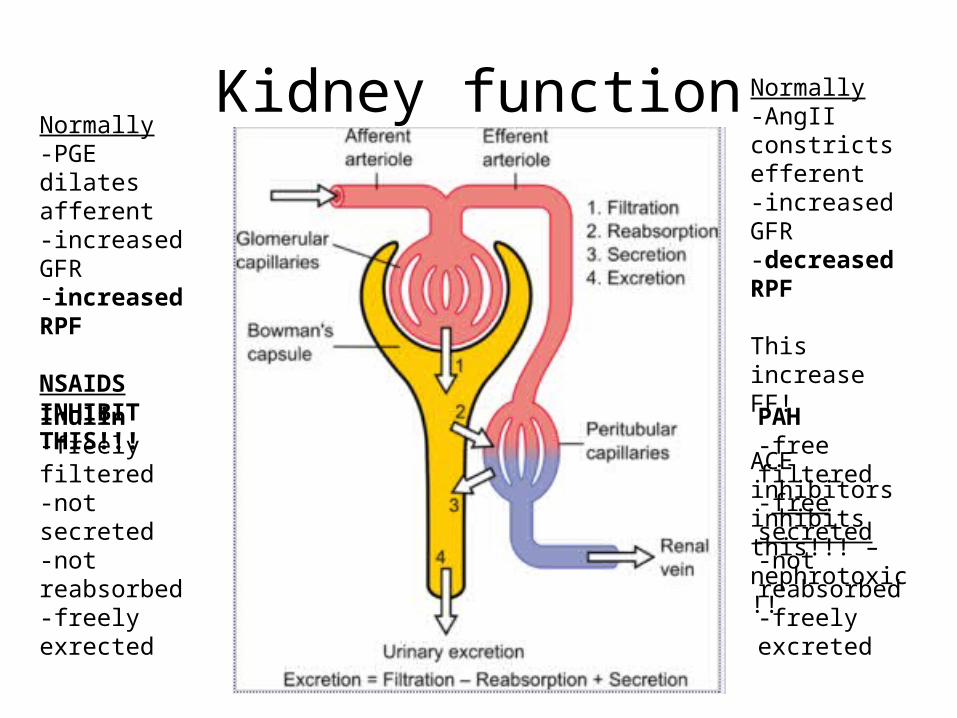
Kidney function
Inulin -freely filtered-not secreted -not reabsorbed -freely exrected
PAH-free filtered-free secreted-not reabsorbed-freely excreted
Normally-PGE dilates afferent-increased GFR-increased RPF
NSAIDS INHIBIT THIS!!!
Normally-AngII constricts efferent-increased GFR-decreased RPF
This increase FF!
ACE inhibitors inhibits this!!! – nephrotoxic!!
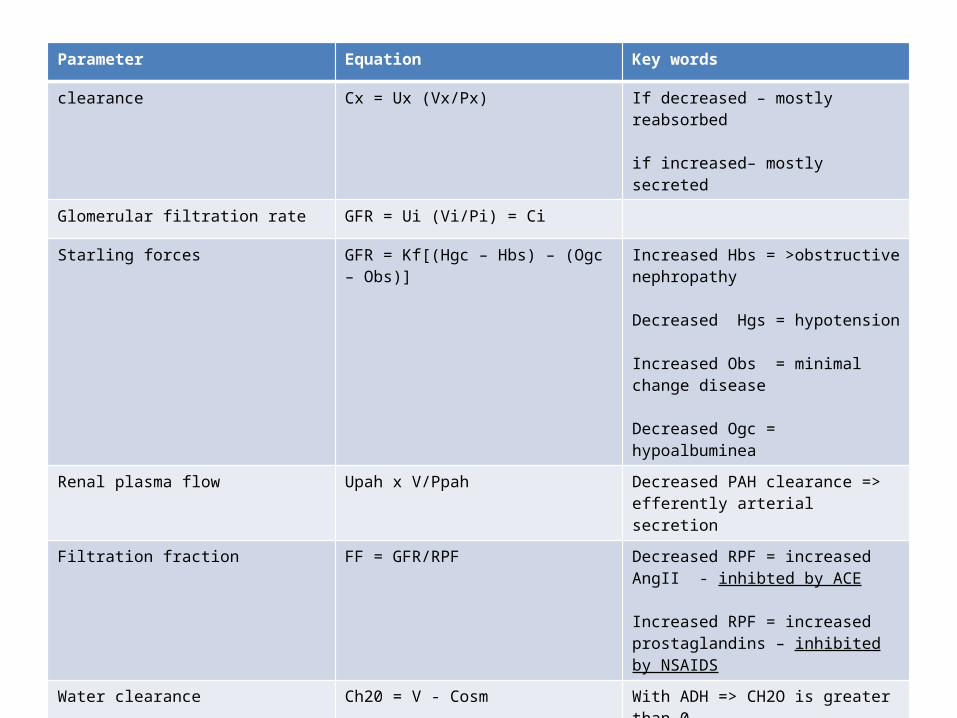
Renal EquationsParameter Equation Key words
clearance Cx = Ux (Vx/Px) If decreased – mostly reabsorbed
if increased– mostly secreted
Glomerular filtration rate GFR = Ui (Vi/Pi) = Ci
Starling forces GFR = Kf[(Hgc – Hbs) – (Ogc – Obs)] Increased Hbs = >obstructive nephropathy
Decreased Hgs = hypotension
Increased Obs = minimal change disease
Decreased Ogc = hypoalbuminea
Renal plasma flow Upah x V/Ppah Decreased PAH clearance => efferently arterial secretion
Filtration fraction FF = GFR/RPF Decreased RPF = increased AngII - inhibted by ACE
Increased RPF = increased prostaglandins – inhibited by NSAIDS
Water clearance Ch20 = V - Cosm With ADH => CH2O is greater than 0
Without ADH => CH2O is less than 0
Filtered load GFR X Px GFR = Ui (Vi/Pi) = Ci
GFR = exretion rate / Pi = Ci
Excretion rate V X Ux
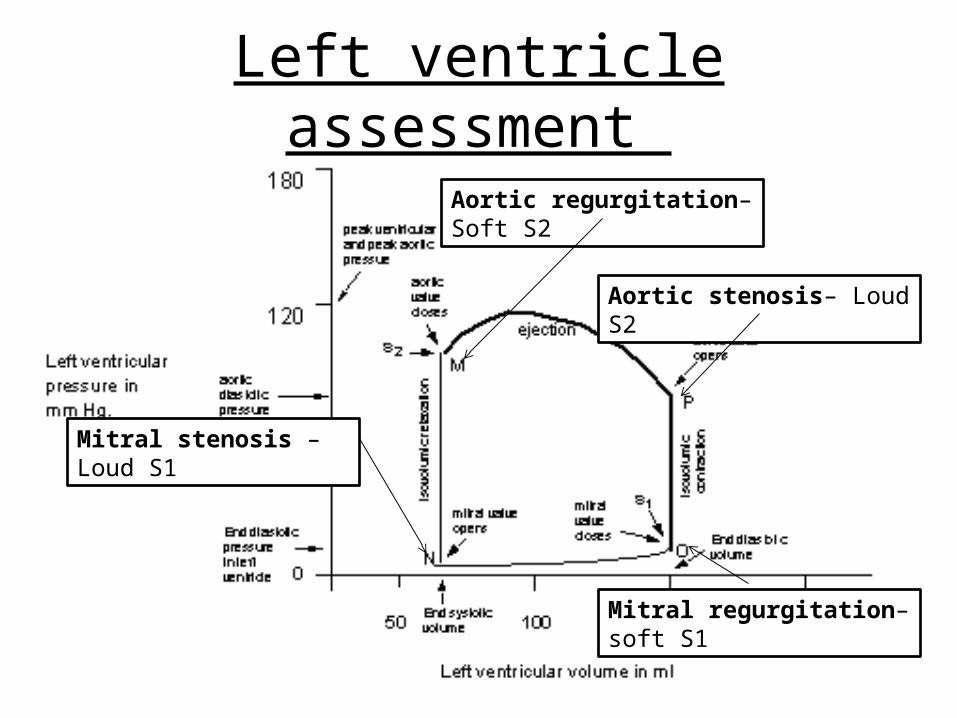
Left ventricle assessment
Aortic regurgitation– Soft S2
Mitral stenosis – Loud S1
Aortic stenosis– Loud S2
Mitral regurgitation– soft S1

Prerenal vs. Renal problem Etiology Initially after BUN /Cr ratio
Prerenal Renal artery stenosisCHFLow volume state!
Afferent Decreased GFRDecreased RBFIncreased serum Cr
Efferent Decreased RPFIncreased serum BUN
AngII restablishes GFR!
Afferent Increased GFRDecreased RBFdecreased serum Cr
Efferent Decreased RPFIncreased serum BUN
>20
Renal glomerulonephritis, acute tubular necrosis acute interstitial nephritisVancomycin tox!!
Afferent Decreased GFRIncreased serum Cr
Efferent increased RPFDecreased serum BUN
AngII restablishes GFR!
Afferent Decreased GFRIncreased serum Cr
Efferent Decreased RPFIncreased serum BUN
<20
Post renal Urinary tract obstructionBPHKidney stones

Nephrotic syndromeSuspect kidney
disease
Nephrotic syndrome
Proteinuria - >3.5 g/dayHypoalbuminea
Edema Hyperlipideamia
Proliferative
Mesangial proliferative
Lupus + IgA nephro
Endocapillary prlif
Parvo B-19
Membranoprolif
Tram-tracking appearance
Immune complex in mesangium!!
Non-proliferative
Minimal change
Diffuse loss of podocyte foot processes =>
fusion!!
Focal segmental
Only some glomeruli + only
part of it!
Membranous
Immune complex in BM!
Spike + domeSubepithelial

Nephritic syndromeNephritic syndrome
Proteinuria – under 3.5 g/dayHematuria AzostomiaRBC casts
Oliguria – less than 400 mL/day
Type I rapidly progressive
Type II HS
Goodpastures
Linear IF - antiBMPoor prognosisHemoptyisis +
oliguria
Type II rapidly
progressive
Type II HS
Post strep
Lumpy-bumpy
Subepithelial Ics – C3
Children
Diffuse proliferative GN
Wiring loopSubendothelial Anti-DNA Ics in
mesagnium URTI
Acute gastritis
IgA nephro/berge
rs
IC deposits in mesagnium
Type III rapidly
progressive
Wegners granulomato
sis
C-ANCASaddle nose deformitiyPulmonary infections
Microscopic polyangitis
pANCA
Ass. With anti-neutrophil antibodies
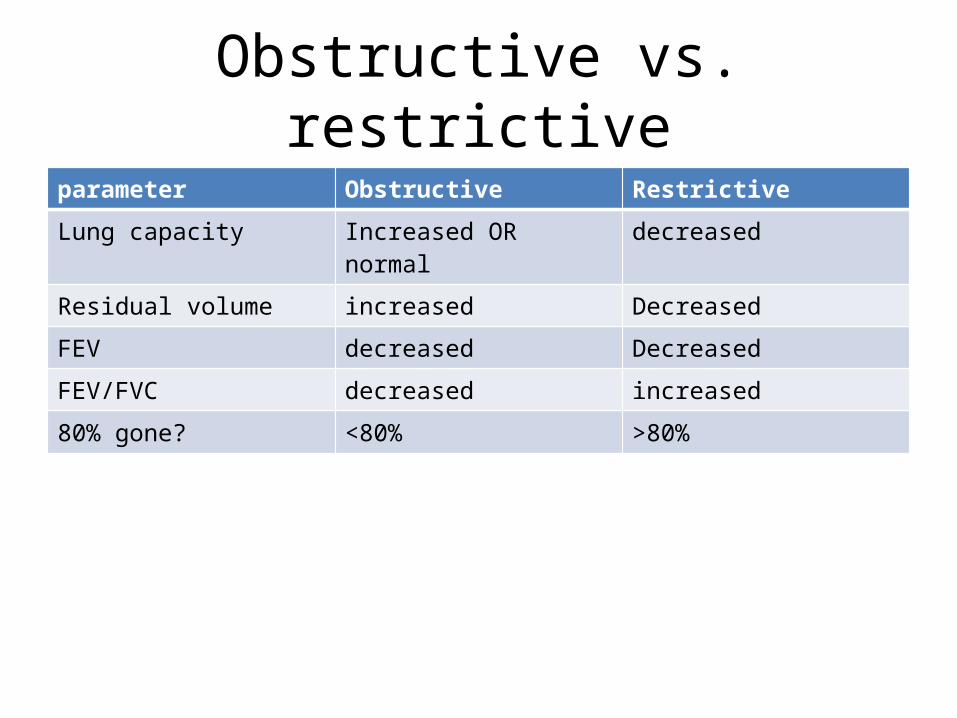
Obstructive vs. restrictiveparameter Obstructive Restrictive
Lung capacity Increased OR normal decreased
Residual volume increased Decreased
FEV decreased Decreased
FEV/FVC decreased increased
80% gone? <80% >80%
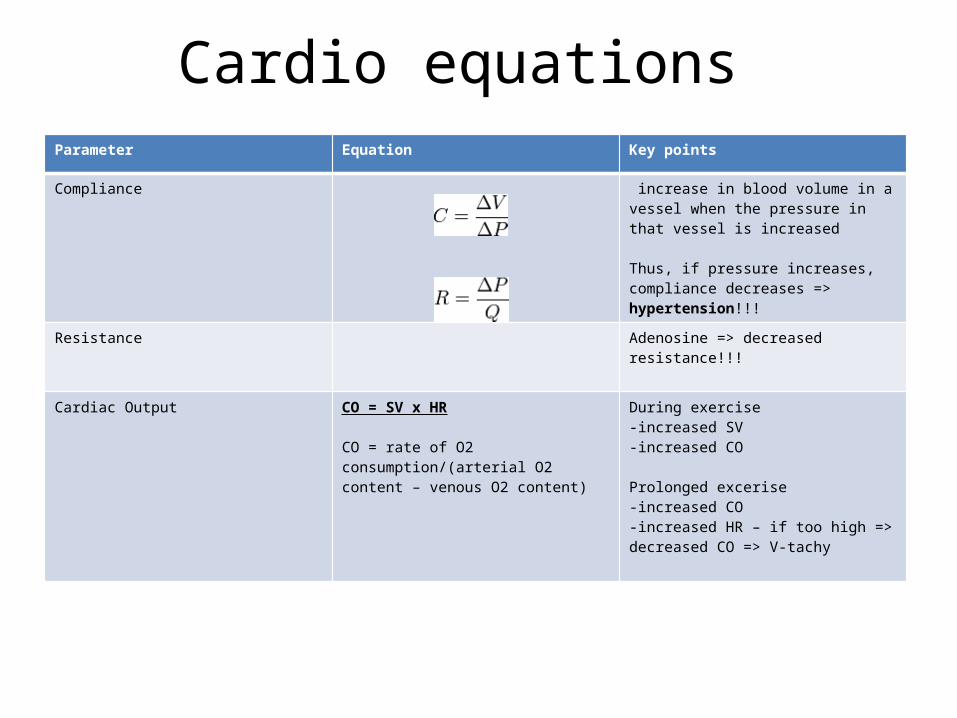
Cardio equations Parameter Equation Key points
Compliance increase in blood volume in a vessel when the pressure in that vessel is increased
Thus, if pressure increases, compliance decreases => hypertension!!!
Resistance Adenosine => decreased resistance!!!
Cardiac Output CO = SV x HR
CO = rate of O2 consumption/(arterial O2 content – venous O2 content)
During exercise -increased SV-increased CO
Prolonged excerise -increased CO-increased HR – if too high => decreased CO => V-tachy
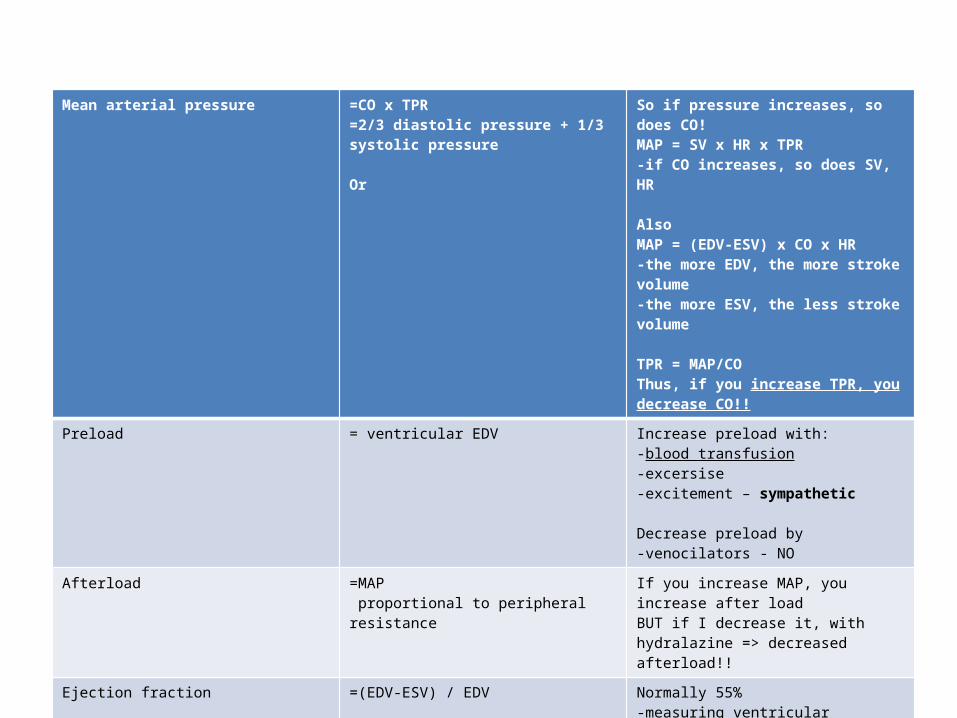
Mean arterial pressure =CO x TPR=2/3 diastolic pressure + 1/3 systolic pressure
Or
So if pressure increases, so does CO!MAP = SV x HR x TPR-if CO increases, so does SV, HR
AlsoMAP = (EDV-ESV) x CO x HR-the more EDV, the more stroke volume-the more ESV, the less stroke volume
TPR = MAP/COThus, if you increase TPR, you decrease CO!!
Preload = ventricular EDV Increase preload with:-blood transfusion-excersise -excitement – sympathetic
Decrease preload by-venocilators - NO
Afterload =MAP proportional to peripheral resistance
If you increase MAP, you increase after load BUT if I decrease it, with hydralazine => decreased afterload!!
Ejection fraction =(EDV-ESV) / EDV Normally 55%-measuring ventricular contractility – so how much blood is ejected from the ventricle
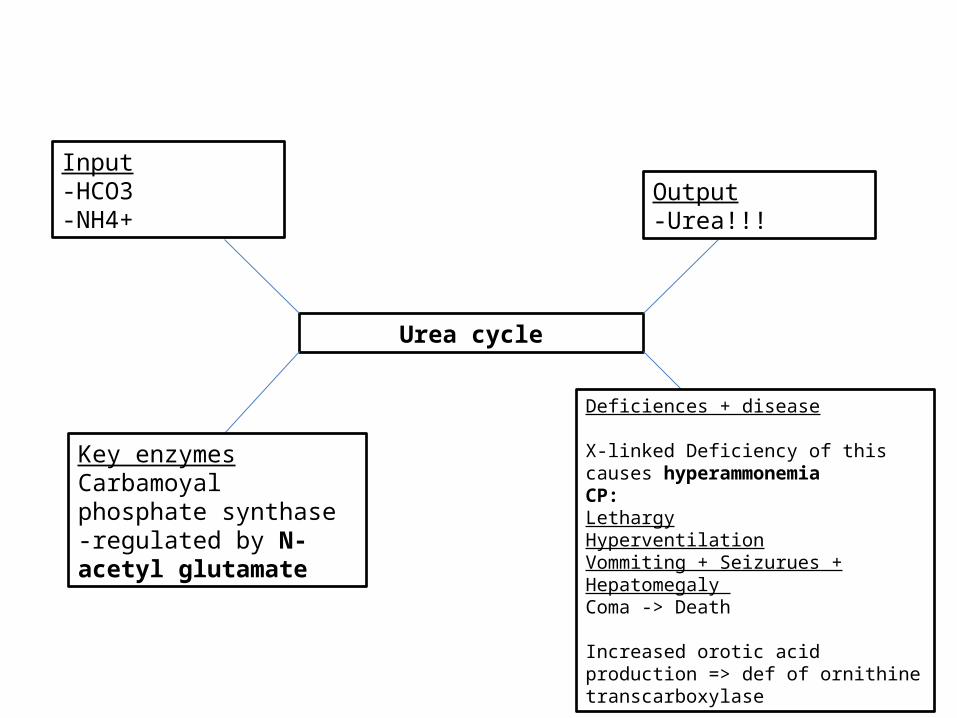
Urea cycle
Input-HCO3-NH4+
Output-Urea!!!
Key enzymesCarbamoyal phosphate synthase-regulated by N-acetyl glutamate
Deficiences + disease
X-linked Deficiency of this causes hyperammonemia CP:LethargyHyperventilationVommiting + Seizurues + Hepatomegaly Coma -> Death
Increased orotic acid production => def of ornithine transcarboxylase
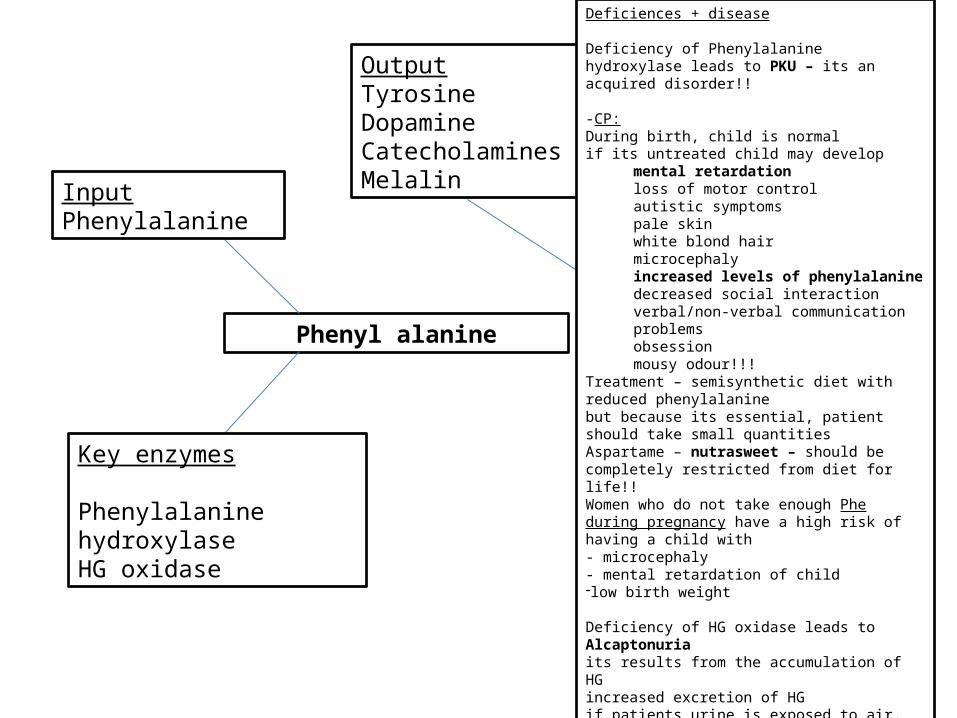
Phenyl alanine
InputPhenylalanine
OutputTyrosine DopamineCatecholaminesMelalin
Key enzymes
Phenylalanine hydroxylaseHG oxidase
Deficiences + disease
Deficiency of Phenylalanine hydroxylase leads to PKU – its an acquired disorder!!
-CP:During birth, child is normal if its untreated child may develop
mental retardationloss of motor controlautistic symptomspale skin white blond hairmicrocephalyincreased levels of phenylalanine decreased social interactionverbal/non-verbal communication problemsobsession mousy odour!!!
Treatment – semisynthetic diet with reduced phenylalanine but because its essential, patient should take small quantities Aspartame – nutrasweet – should be completely restricted from diet for life!!Women who do not take enough Phe during pregnancy have a high risk of having a child with - microcephaly- mental retardation of child -low birth weight
Deficiency of HG oxidase leads to Alcaptonuria its results from the accumulation of HGincreased excretion of HGif patients urine is exposed to air, it turns dark colored CP: Ochrosis its an autosomal recessive disorder results in pigmentation and calcification of bones and cartlidge – leads to arthritis
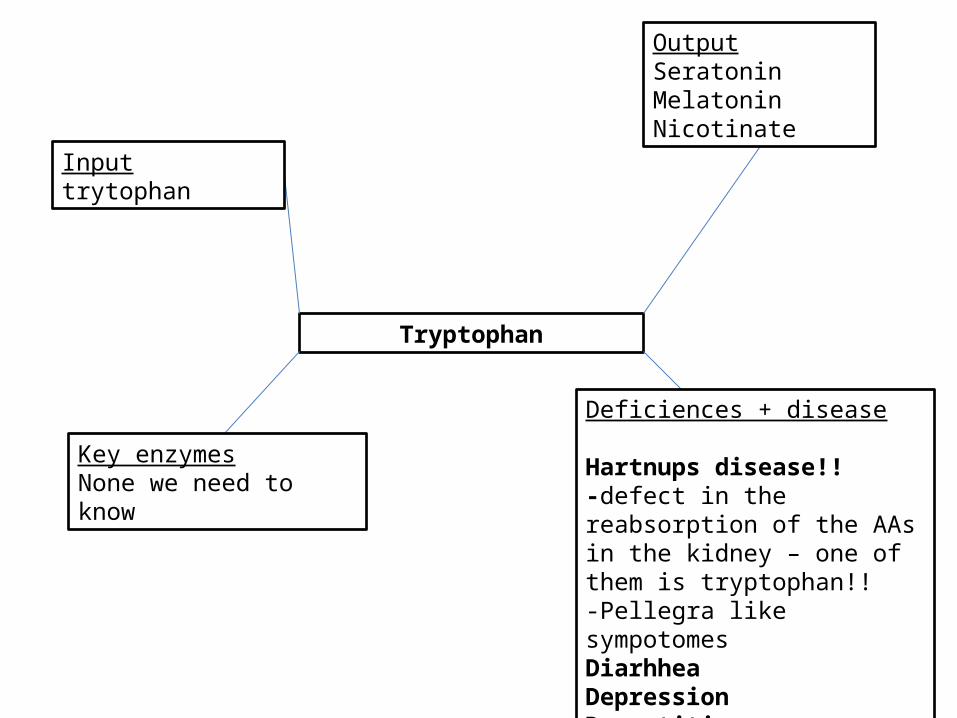
Tryptophan
Inputtrytophan
OutputSeratoninMelatoninNicotinate
Key enzymesNone we need to know
Deficiences + disease
Hartnups disease!!-defect in the reabsorption of the AAs in the kidney – one of them is tryptophan!!-Pellegra like sympotomes Diarhhea Depression Dermatitis Sometimes cerebellar ataxia

Tryptophan

BCAs
InputBCAs
OutputHMG CoAAcetyl CoA + Propionyl CoA
Key enzymes
2-ketoacid dehydrogenase complex of enzymes
Deficiences + disease
Maple syrup urine diseaselethargy, dehydration, and vomiting-hypotonia-dramatic weight loss-ketoacidosis (if untreated)- eventually leads to coma and death There are 5 types:-classical MSUD *** MOST SEVERE-Intermediate MSUD-Thiamine responsive MSUD-Enzyme responsive MSUD w/ lactic acidosis
Propanoic acidemia-deficeny in propionyl CoA carboxylase = met. Acidosis, dehydrtation -accumulation of propanoic acid -drives formation of acetyl CoA to the formation of ketone bodies

BSA disease hypoglycemia Ketoacidosis
MUSD increased Increased
Propanoic acidosis increased Increased more!-drives formation of ketone bodies form acetyl CoA
Methylmalonyl CoA acidosis
Increased more!
-inhibition of pyruvate carboxylase + gluconeogenesis by methylmalonyl CoA
Increased more!-accumulated methylmalonic + propanoic acids

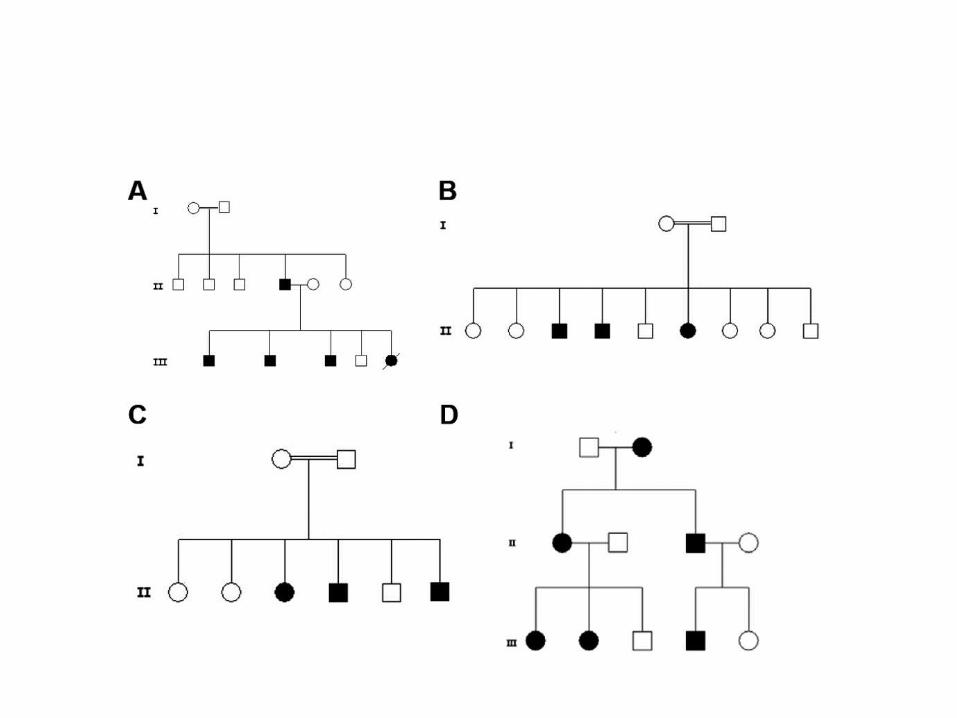
Genetics USMLE problem
Population
Carriers
Find pFind q
Find F(Aa) = 2pq
Subtract patient + subtract diseased
Affected
Find F(aa) = q^2
Children
Find ratio of affected vs. Non-
affected
If both conditions – multiply with
carrier prob
If either one condition, add
with carrier prob
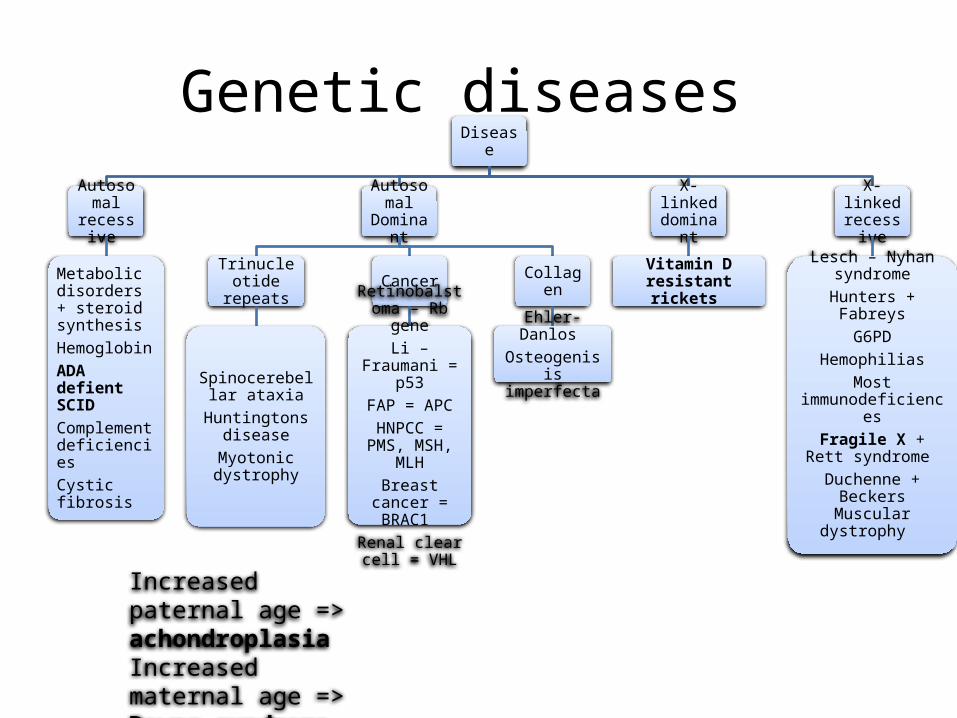
Genetic diseases Disease
Autosomal
recessive
Metabolic disorders + steroid synthesisHemoglobin ADA defient SCIDComplement deficiencies Cystic fibrosis
Autosomal
Dominant
Trinucleotide repeats
Spinocerebellar ataxia
Huntingtons disease
Myotonic dystrophy
Cancer
Retinobalstoma – Rb gene
Li – Fraumani = p53
FAP = APCHNPCC = PMS,
MSH, MLHBreast cancer =
BRAC1 Renal clear cell
= VHL
Collagen
Ehler-Danlos Osteogenisis imperfecta
X-linked dominan
t
Vitamin D resistant rickets
X-linked recessive
Lesch – Nyhan syndrome
Hunters + FabreysG6PD
HemophiliasMost
immunodeficiencesFragile X + Rett
syndrome Duchenne + Beckers Muscular dystrophy
Increased paternal age => achondroplasia Increased maternal age => Downs syndrome
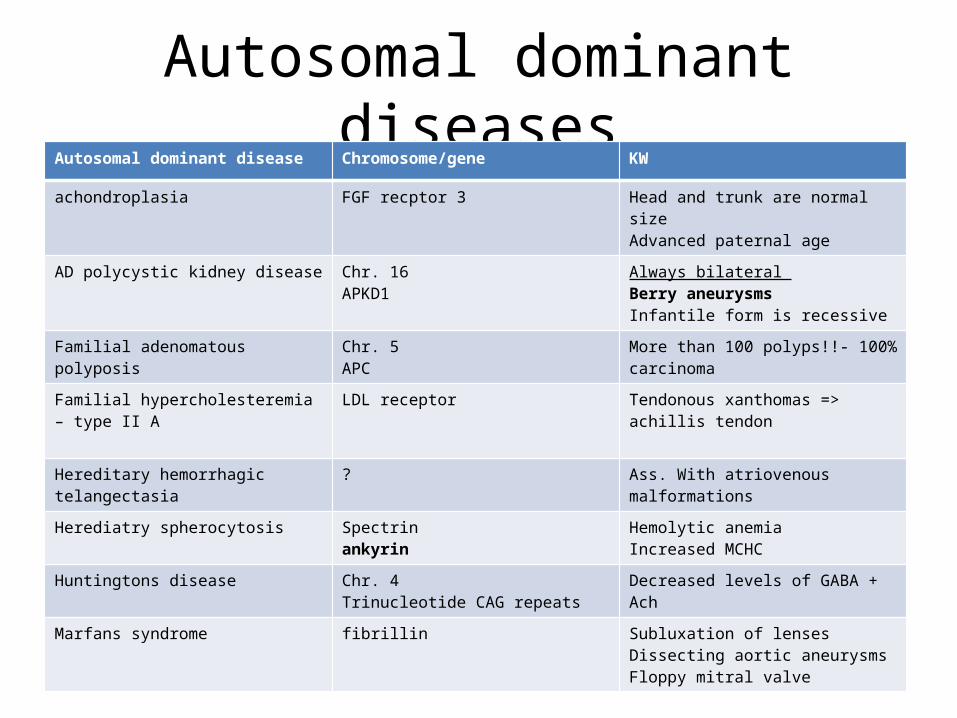
Autosomal dominant diseasesAutosomal dominant disease Chromosome/gene KW
achondroplasia FGF recptor 3 Head and trunk are normal sizeAdvanced paternal age
AD polycystic kidney disease Chr. 16APKD1
Always bilateral Berry aneurysmsInfantile form is recessive
Familial adenomatous polyposis Chr. 5 APC
More than 100 polyps!!- 100% carcinoma
Familial hypercholesteremia – type II A LDL receptor Tendonous xanthomas => achillis tendon
Hereditary hemorrhagic telangectasia ? Ass. With atriovenous malformations
Herediatry spherocytosis Spectrinankyrin
Hemolytic anemiaIncreased MCHC
Huntingtons disease Chr. 4Trinucleotide CAG repeats
Decreased levels of GABA + Ach
Marfans syndrome fibrillin Subluxation of lensesDissecting aortic aneurysms Floppy mitral valve
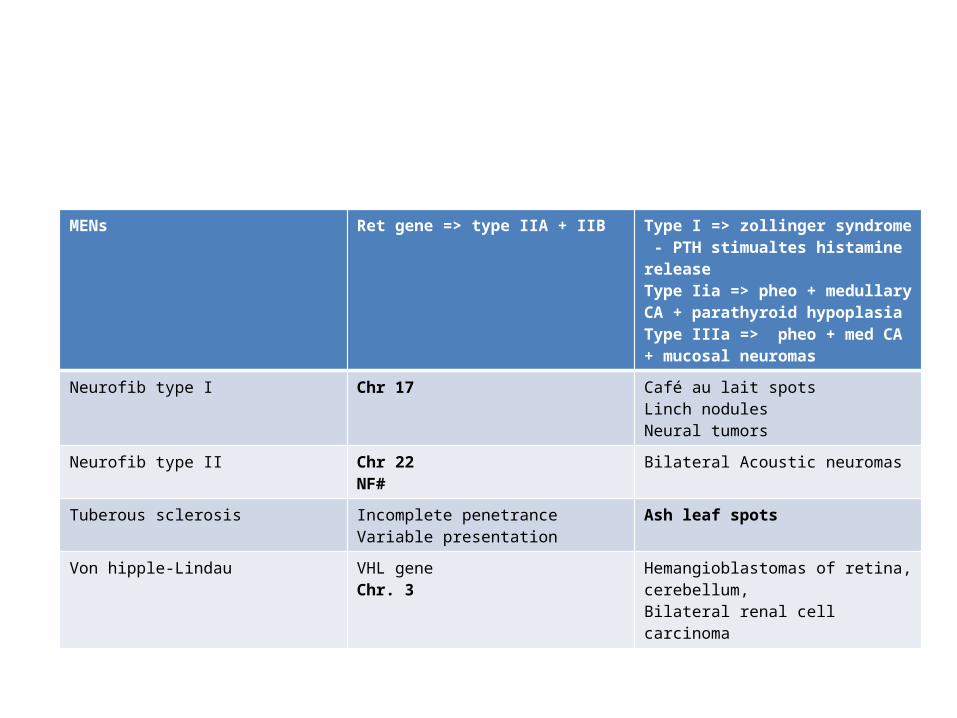
MENs Ret gene => type IIA + IIB Type I => zollinger syndrome - PTH stimualtes histamine releaseType Iia => pheo + medullary CA + parathyroid hypoplasiaType IIIa => pheo + med CA + mucosal neuromas
Neurofib type I Chr 17 Café au lait spotsLinch nodulesNeural tumors
Neurofib type II Chr 22NF#
Bilateral Acoustic neuromas
Tuberous sclerosis Incomplete penetranceVariable presentation
Ash leaf spots
Von hipple-Lindau VHL geneChr. 3
Hemangioblastomas of retina, cerebellum, Bilateral renal cell carcinoma
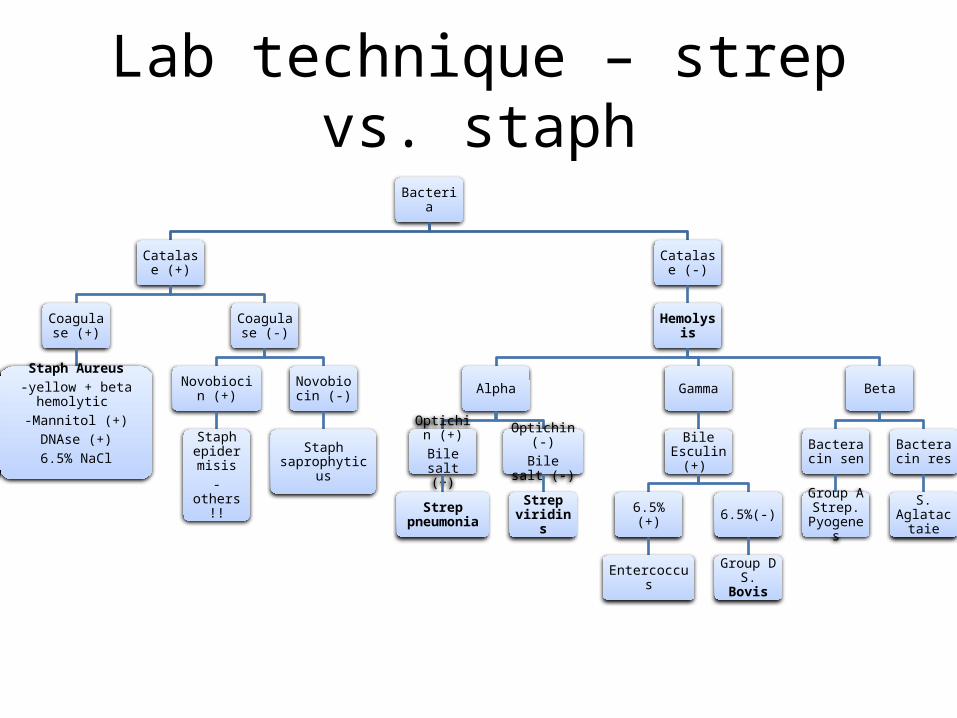
Lab technique – strep vs. staphBacteria
Catalase (+)
Coagulase (+)
Staph Aureus-yellow + beta hemolytic
-Mannitol (+)DNAse (+)6.5% NaCl
Coagulase (-)
Novobiocin (+)
Staph epidermis
is-others!!
Novobiocin (-)
Staph saprophyticus
Catalase (-)
Hemolysis
Alpha
Optichin (+)
Bile salt (+)
Strep pneumonia
Optichin (-)Bile salt (-)
Strep viridins
Gamma
Bile Esculin (+)
6.5% (+)
Entercoccus
6.5%(-)
Group D S. Bovis
Beta
Bacteracin sen
Group A Strep.
Pyogenes
Bacteracin res
S. Aglatactai
e

Capsulated bacteriaOrganisms
Strep pneumonia
Klebsiella pneumonia
Bacillus anthracis
Haemophilus influenza B
Pseudomonos Aerug
Neisseria meningitis
Cryptococcus neoformans
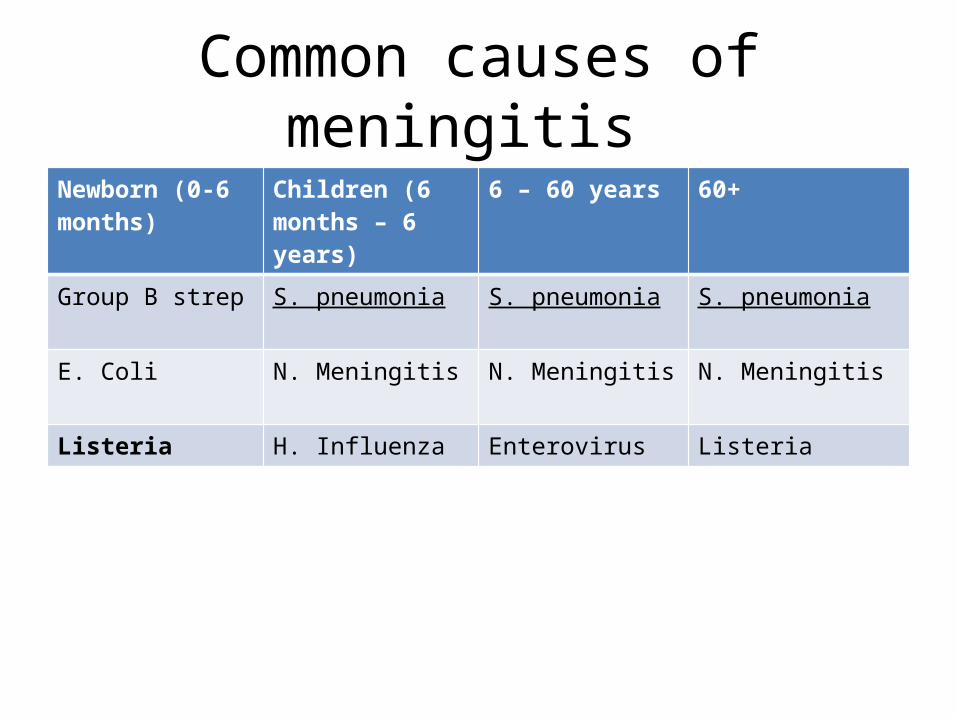
Common causes of meningitis Newborn (0-6 months)
Children (6 months – 6 years)
6 – 60 years 60+
Group B strep S. pneumonia S. pneumonia S. pneumonia
E. Coli N. Meningitis N. Meningitis N. Meningitis
Listeria H. Influenza Enterovirus Listeria

Viral Protein synthesis
(-) RNA
RNA dep RNA Pol
Reverse transcriptaise
(+) RNA
Translation
RNA dep RNA Pol
RNA
Reverse Transcriptase
cDNA
mRNA
DNA-dep DNA Pol
DNA
DNA dep RNA Rol (host)
mRNA
Structural proteins
How retroviruses (HIV) does it!
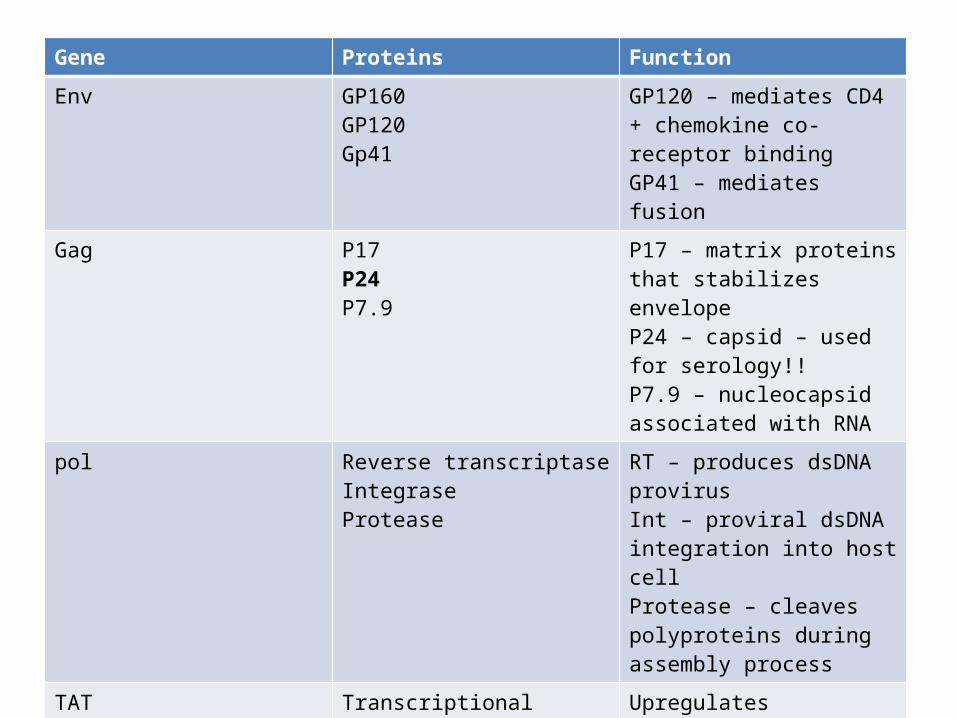
HIV virus Gene Proteins Function
Env GP160GP120Gp41
GP120 – mediates CD4 + chemokine co-receptor binding GP41 – mediates fusion
Gag P17P24P7.9
P17 – matrix proteins that stabilizes envelopeP24 – capsid – used for serology!!P7.9 – nucleocapsid associated with RNA
pol Reverse transcriptaseIntegrase Protease
RT – produces dsDNA provirus Int – proviral dsDNA integration into host cell Protease – cleaves polyproteins during assembly process
TAT Transcriptional activator Upregulates transcription
REV Regulator of virion protein expression
Viral replication
NEF Regulatory factor Negative regulator factor
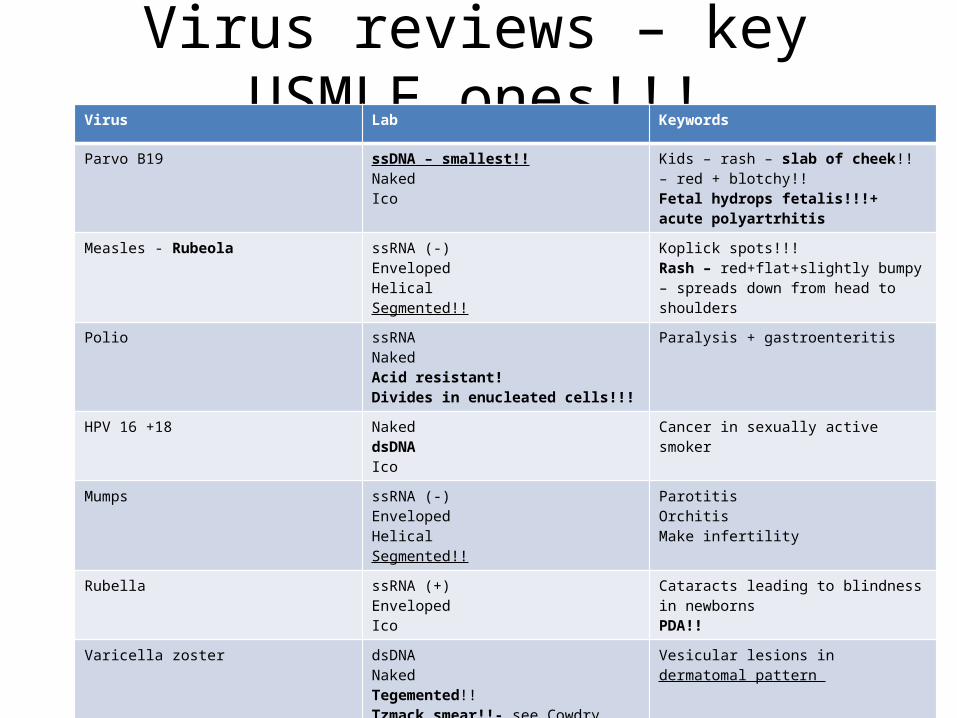
Virus reviews – key USMLE ones!!!Virus Lab Keywords
Parvo B19 ssDNA – smallest!!NakedIco
Kids – rash – slab of cheek!! – red + blotchy!!Fetal hydrops fetalis!!!+ acute polyartrhitis
Measles - Rubeola ssRNA (-) Enveloped Helical Segmented!!
Koplick spots!!!Rash – red+flat+slightly bumpy – spreads down from head to shoulders
Polio ssRNANakedAcid resistant!Divides in enucleated cells!!!
Paralysis + gastroenteritis
HPV 16 +18 NakeddsDNAIco
Cancer in sexually active smoker
Mumps ssRNA (-) Enveloped Helical Segmented!!
Parotitis OrchitisMake infertility
Rubella ssRNA (+)EnvelopedIco
Cataracts leading to blindness in newborns PDA!!
Varicella zoster dsDNANakedTegemented!!Tzmack smear!!- see Cowdry type cells!!
Vesicular lesions in dermatomal pattern
CMV dsDNANakedTegemented!!
Acute retinitis in AIDS patients
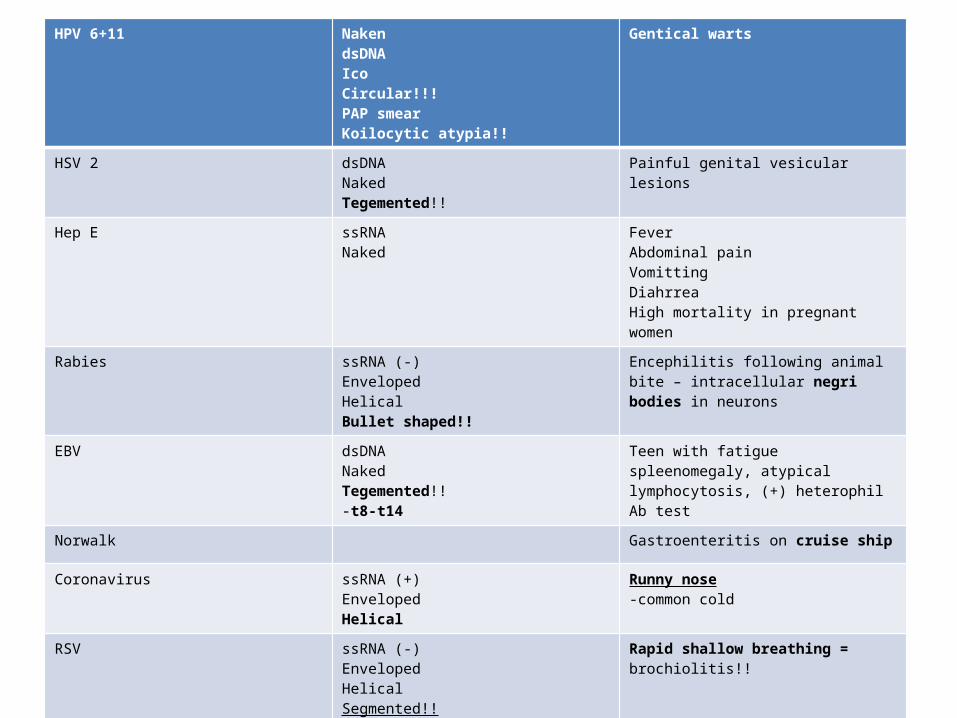
HPV 6+11 NakendsDNAIcoCircular!!!PAP smear Koilocytic atypia!!
Gentical warts
HSV 2 dsDNANakedTegemented!!
Painful genital vesicular lesions
Hep E ssRNA Naked
FeverAbdominal painVomittingDiahrrea High mortality in pregnant women
Rabies ssRNA (-) Enveloped HelicalBullet shaped!!
Encephilitis following animal bite – intracellular negri bodies in neurons
EBV dsDNANakedTegemented!!-t8-t14
Teen with fatigue spleenomegaly, atypical lymphocytosis, (+) heterophil Ab test
Norwalk Gastroenteritis on cruise ship
Coronavirus ssRNA (+)EnvelopedHelical
Runny nose-common cold
RSV ssRNA (-) Enveloped Helical Segmented!!
Rapid shallow breathing = brochiolitis!!
Hanta ssRNA (+/-) – only ambisense!!!Enveloped Helical
Hantavirus – pulmonary edema- fever, muscle, aches, increased WBC, low platelet counts - ARDS
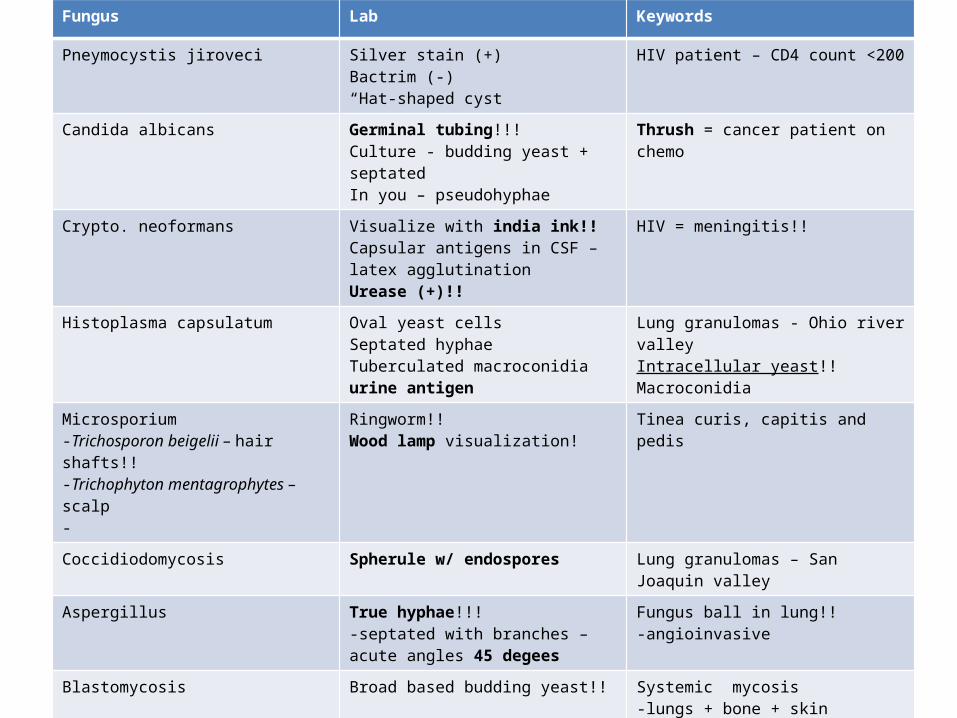
Fungus Lab Keywords
Pneymocystis jiroveci Silver stain (+)Bactrim (-)“Hat-shaped cyst
HIV patient – CD4 count <200
Candida albicans Germinal tubing!!!Culture - budding yeast + septatedIn you – pseudohyphae
Thrush = cancer patient on chemo
Crypto. neoformans Visualize with india ink!!Capsular antigens in CSF – latex agglutination Urease (+)!!
HIV = meningitis!!
Histoplasma capsulatum Oval yeast cellsSeptated hyphaeTuberculated macroconidia urine antigen
Lung granulomas - Ohio river valleyIntracellular yeast!!Macroconidia
Microsporium -Trichosporon beigelii – hair shafts!!-Trichophyton mentagrophytes – scalp-
Ringworm!!Wood lamp visualization!
Tinea curis, capitis and pedis
Coccidiodomycosis Spherule w/ endospores Lung granulomas – San Joaquin valley
Aspergillus True hyphae!!!-septated with branches – acute angles 45 degees
Fungus ball in lung!!-angioinvasive
Blastomycosis Broad based budding yeast!! Systemic mycosis -lungs + bone + skin Microconidia
Sporothrix Cigerette shaped!!Resembles a daisy flower
Ascending lymphadenitisRose gardening!!!
Mucormycosis Non-septated!!90 degree branching!!
Rhinocerebral infection Diabetic ketoacidosis

Malaria treatment Plasmodium Primaquine Chloroquine Quinine Mefloquine
Vivax Yes – in the liver
NOPregnancy
Pregnancy Prophylaxis – if res to chloro
Ovale Yes – in the liver
NO – resistantPregnancy
Pregnancy Yes – if resistant to chloro
Malarae NO Yes + primaPregnancy
Preganancy Prophylaxis – if res to chloro
Falciparum NO NOpregnancy
IV – if cerebral + pregnancy
Prophylaxis – if res to chloro
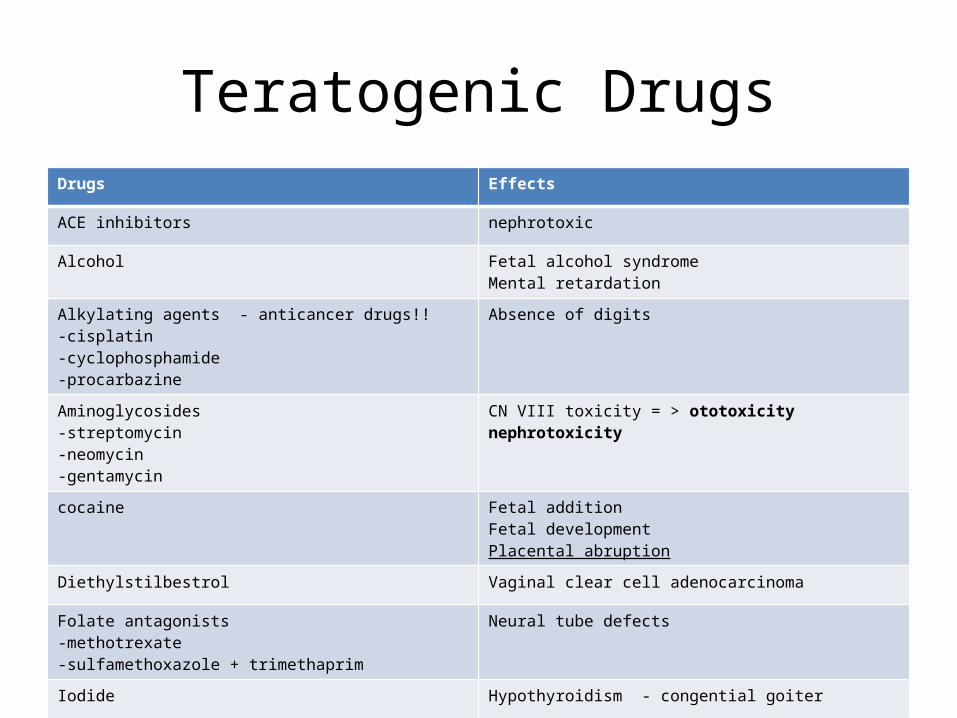
Teratogenic DrugsDrugs Effects
ACE inhibitors nephrotoxic
Alcohol Fetal alcohol syndromeMental retardation
Alkylating agents - anticancer drugs!!-cisplatin-cyclophosphamide-procarbazine
Absence of digits
Aminoglycosides -streptomycin-neomycin-gentamycin
CN VIII toxicity = > ototoxicitynephrotoxicity
cocaine Fetal additionFetal development Placental abruption
Diethylstilbestrol Vaginal clear cell adenocarcinoma
Folate antagonists-methotrexate-sulfamethoxazole + trimethaprim
Neural tube defects
Iodide Hypothyroidism - congential goiter
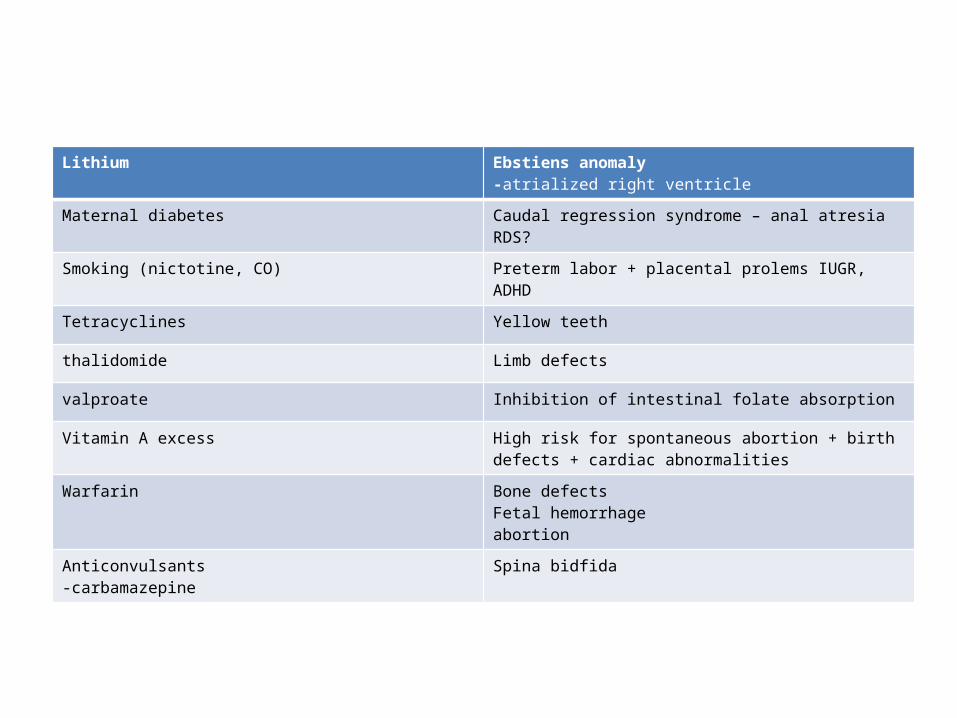
Lithium Ebstiens anomaly -atrialized right ventricle
Maternal diabetes Caudal regression syndrome – anal atresia RDS?
Smoking (nictotine, CO) Preterm labor + placental prolems IUGR, ADHD
Tetracyclines Yellow teeth
thalidomide Limb defects
valproate Inhibition of intestinal folate absorption
Vitamin A excess High risk for spontaneous abortion + birth defects + cardiac abnormalities
Warfarin Bone defectsFetal hemorrhage abortion
Anticonvulsants-carbamazepine
Spina bidfida
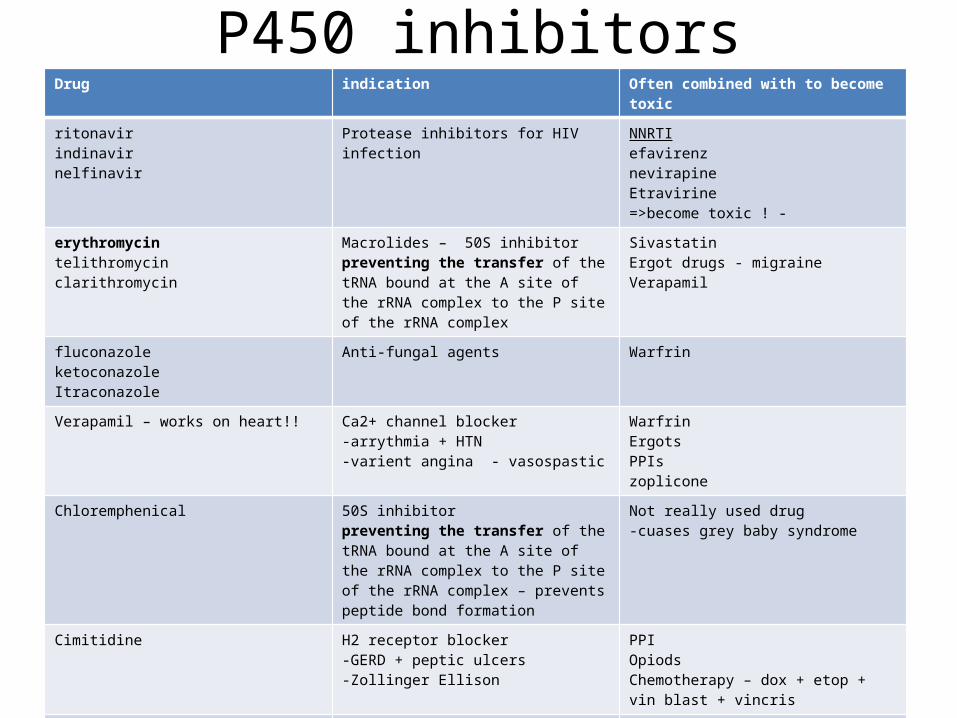
P450 inhibitorsDrug indication Often combined with to become toxic
ritonavirindinavirnelfinavir
Protease inhibitors for HIV infection NNRTIefavirenznevirapineEtravirine=>become toxic ! -
erythromycintelithromycinclarithromycin
Macrolides – 50S inhibitorpreventing the transfer of the tRNA bound at the A site of the rRNA complex to the P site of the rRNA complex
SivastatinErgot drugs - migraineVerapamil
fluconazoleketoconazoleItraconazole
Anti-fungal agents Warfrin
Verapamil – works on heart!! Ca2+ channel blocker -arrythmia + HTN -varient angina - vasospastic
Warfrin ErgotsPPIszoplicone
Chloremphenical 50S inhibitorpreventing the transfer of the tRNA bound at the A site of the rRNA complex to the P site of the rRNA complex – prevents peptide bond formation
Not really used drug-cuases grey baby syndrome
Cimitidine H2 receptor blocker-GERD + peptic ulcers-Zollinger Ellison
PPIOpiodsChemotherapy – dox + etop + vin blast + vincris
Amiodareone Antiarrythmic Class III– K+ and Beta blocking action
WarfrinSildenafil ProcainamideDigoxencyclosporine

P450 inducersDrug indications Will inactivate the
following drugsphenytoincarbamazepineoxcarbazepine
Anticonvulsants BDZSex hormone agonists + antagonists SSRIs
Phenobarbitol For Fibrile seizures!!! BDZ
efavirenznevirapineetravirine
NNRTIs for HIV PI’s
rifampin Tb infection
St.Johns Wort Major depression
Grisofulvin Antifungal/bacterial
pioglitazone Oral hypoglycemic -peroxisome proliferator-activated receptors
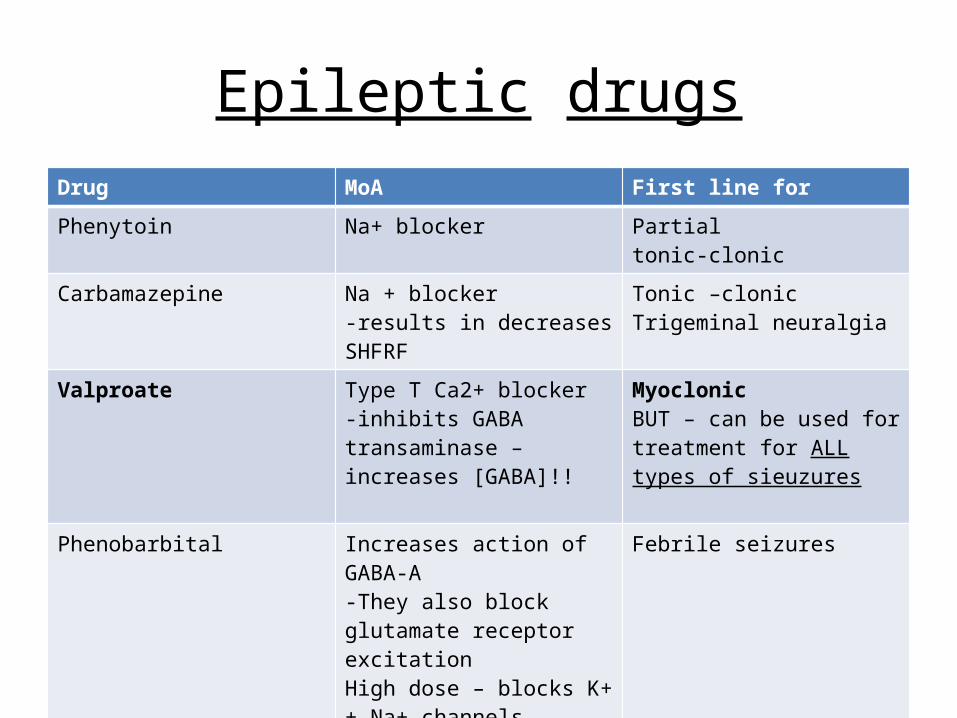
Epileptic drugsDrug MoA First line for
Phenytoin Na+ blocker Partial tonic-clonic
Carbamazepine Na + blocker-results in decreases SHFRF
Tonic –clonicTrigeminal neuralgia
Valproate Type T Ca2+ blocker-inhibits GABA transaminase – increases [GABA]!!
Myoclonic BUT – can be used for treatment for ALL types of sieuzures
Phenobarbital Increases action of GABA-A-They also block glutamate receptor excitationHigh dose – blocks K+ + Na+ channels
Febrile seizures
Diazepam + lorazepam Facilitates actions of GABA-results in hyperpolarization of the membrane
For acute status epilepticus
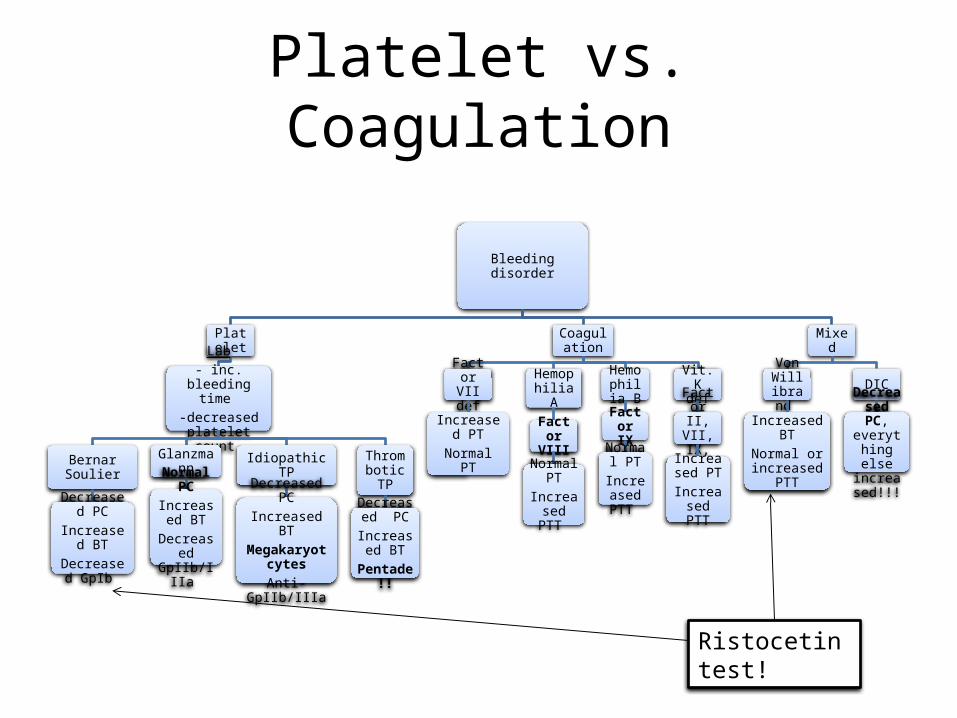
Platelet vs. Coagulation
Bleeding disorder
Platelet
Lab- inc. bleeding
time -decreased
platelet count
Bernar Soulier
Decreased PC
Increased BTDecreased
GpIb
Glanzmann
Normal PCIncreased
BTDecreased GpIIb/IIIa
Idiopathic TP
Decreased PCIncreased BT
Megakaryotcytes
Anti-GpIIb/IIIa
Thrombotic TP
Decreased PC
Increased BT
Pentade!!
Coagulation
Factor VII def
Increased PTNormal PT
Hemophilia A
Factor VIII
Normal PT
Increased PTT
Hemophilia
BFactor
IXNormal
PTIncreased PTT
Vit. K def
Factor II, VII, IX, X
Increased PT
Increased PTT
Mixed
Von Willibrand
Increased BTNormal or increased
PTT
DIC
Decreased PC,
everything else
increased!!!
Ristocetin test!
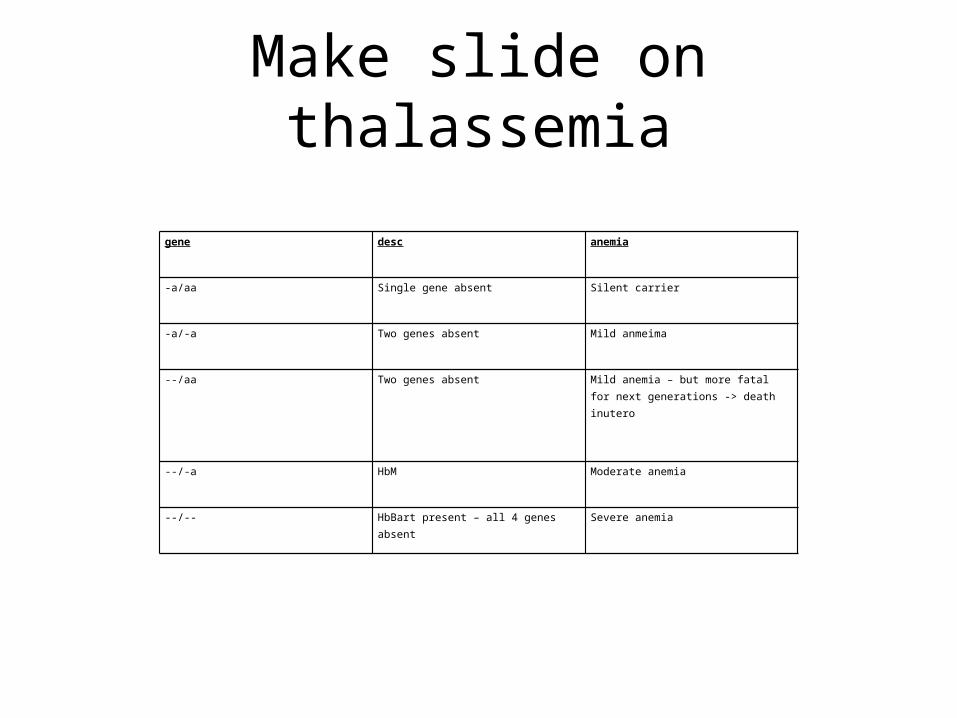
Make slide on thalassemia
gene desc anemia
-a/aa Single gene absent Silent carrier
-a/-a Two genes absent Mild anmeima
--/aa Two genes absent Mild anemia – but more fatal for next generations -> death inutero
--/-a HbM Moderate anemia
--/-- HbBart present – all 4 genes absent Severe anemia
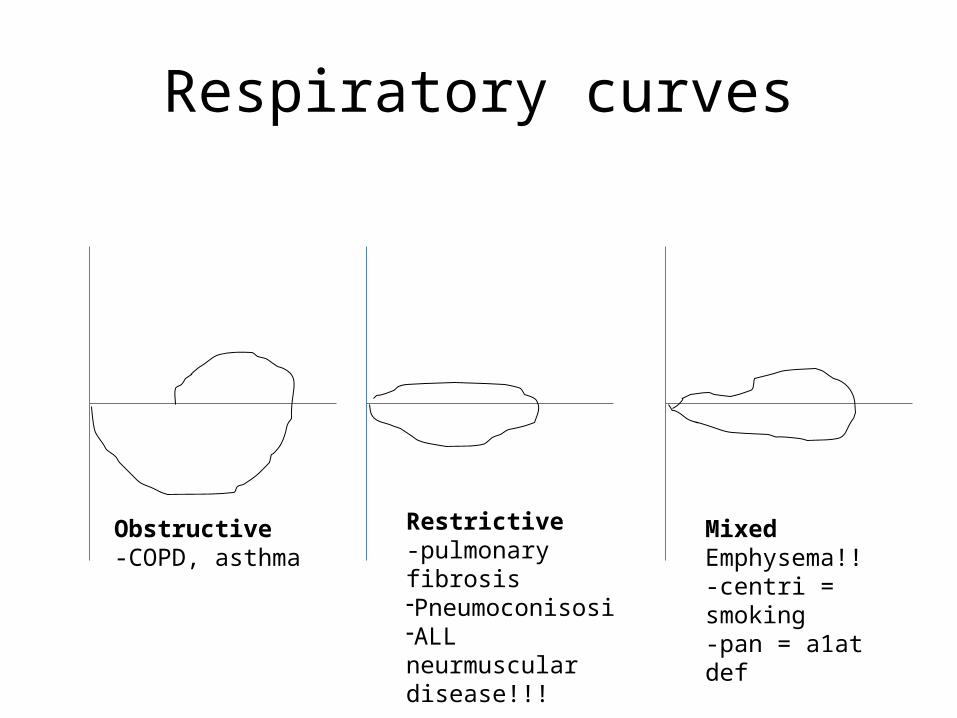
Respiratory curves
Obstructive-COPD, asthma
Restrictive-pulmonary fibrosis-Pneumoconisosi-ALL neurmuscular disease!!!
MixedEmphysema!!-centri = smoking-pan = a1at def

Coombs test
Coombs test
Direct
RBCs with IgG antibodies
Combines with rabbit anti-IgG
If agglutinates => Hemolytic anemia
Indirect
Add test blood O RBCs to test tube of IgG antibodies
Combines with rabbit anti-IgG
If agglutinates => erythroblastosis
fetalis
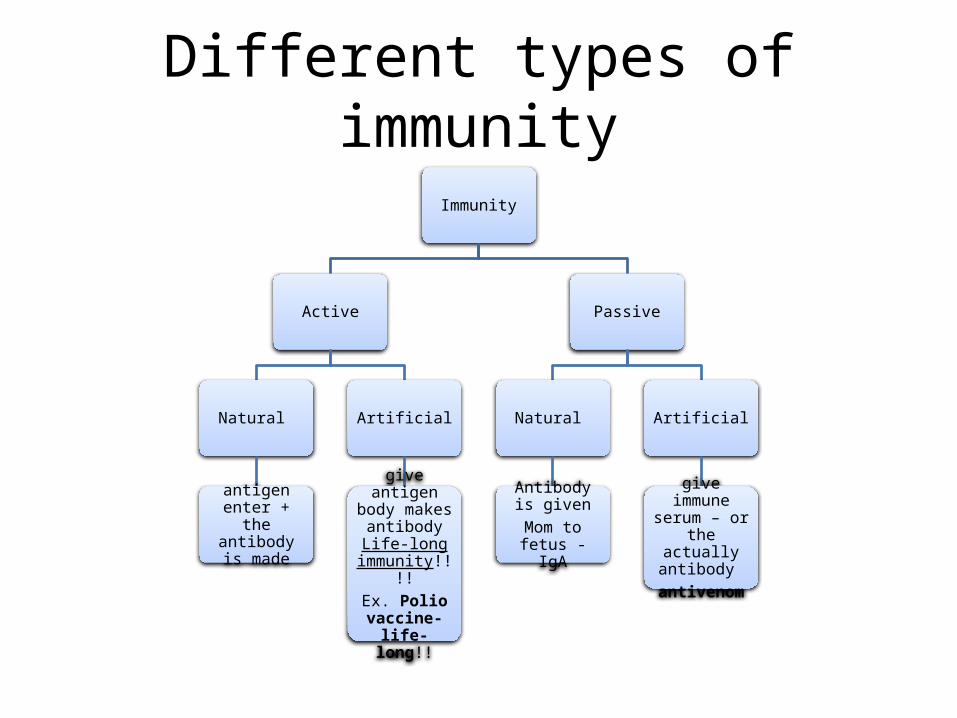
Different types of immunity
Immunity
Active
Natural
antigen enter + the antibody is
made
Artificial
give antigen body makes
antibody Life-long
immunity!!!!Ex. Polio
vaccine- life-long!!
Passive
Natural
Antibody is given
Mom to fetus - IgA
Artificial
give immune serum – or the
actually antibody
antivenom

Hypersensitivity reactionsHS type Source mediators Discription ClinicalsType I IgE-mediated Basophils
Mast cellsHistamineBradykinin IgETNFIFN gammaPLA2
Initiall exposure-body sees antigen -> B-cells -> increase in plasma cells -> antibodies from IgE 2nd exposure-ab is already formed-it binds to mast cells + basophils First get degranulation-primary mediators – heparain, histamine, proteases-cytokines – TNF, IFN gamme, IL-1-phospholipase A2 – prostaglandins + LTB4
Anaphylaxis
Type II Complement dependentADCCAb mediated cellular dysfunction
MAC complexC3a + b - opsininC5a
Comp dep-Lysis – Ag+Ab -> stimulates complement system + disrupts membrane integrity by forming pores -Opsinins – fixed complement coats Antigen with Ab – enhances phagocytosis
ADCC-IgG coats -> non-sensitized cells destroy-for worms and tumors-facilitate the killing of insulin-producing cellsAb mediated-Ab against surface receptor + changing their function
ADCCParasitic infectionTumorsType II diabetes M – juvenille!Pernicious anemiaCellular dysfunctionMysinia Gravis – DDx- lambert eaton – defect in release of Ach from neuronGraves diseaseWegner’s granulomatosis-antibodies against proteinase 3 – patch necrosis of BVsP.ANCA – Ab against myeloperoxidasePemphigus – Ab attack desmosomes – lung hemorhagesComplement dependent-transfusion-erythroblastosis fetalis-autoimmune haemolytic anema-Drug reactions
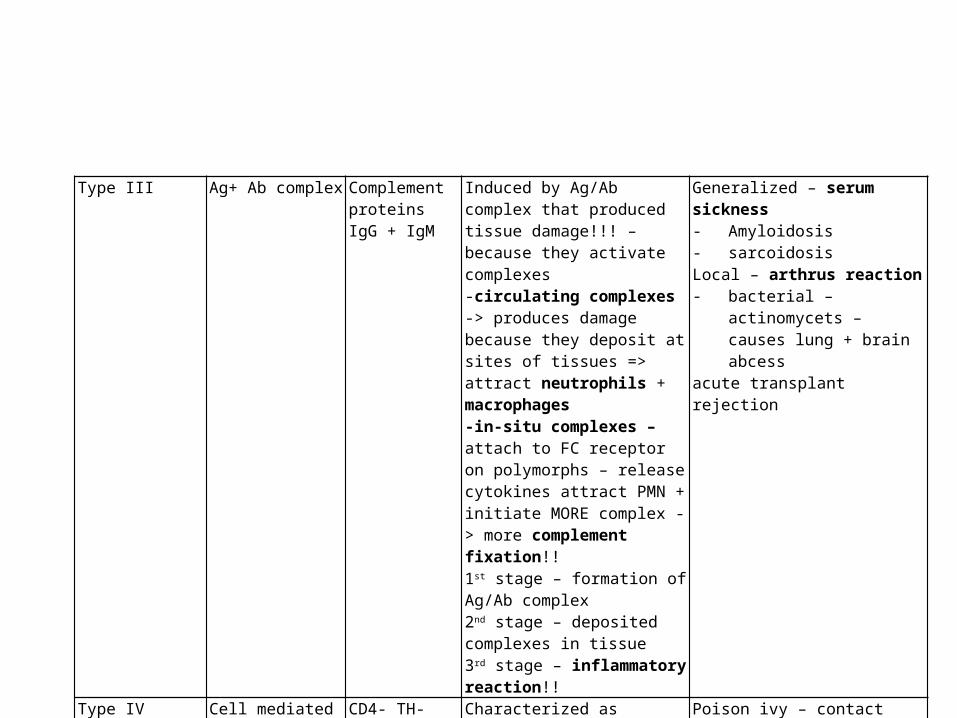
Type III Ag+ Ab complex Complement proteinsIgG + IgM
Induced by Ag/Ab complex that produced tissue damage!!! – because they activate complexes -circulating complexes -> produces damage because they deposit at sites of tissues => attract neutrophils + macrophages-in-situ complexes – attach to FC receptor on polymorphs – release cytokines attract PMN + initiate MORE complex - > more complement fixation!!1st stage – formation of Ag/Ab complex2nd stage – deposited complexes in tissue3rd stage – inflammatory reaction!!
Generalized – serum sickness- Amyloidosis- sarcoidosisLocal – arthrus reaction- bacterial – actinomycets –
causes lung + brain abcessacute transplant rejection
Type IV Cell mediated CD4- TH-cells - TNFIFN gammaIL-1macrophages
Characterized as granulomatous inflammation – chronic!
Poison ivy – contact dermatitisTuberculin sensitivityHistoplasmosisSacrcoidosisMS
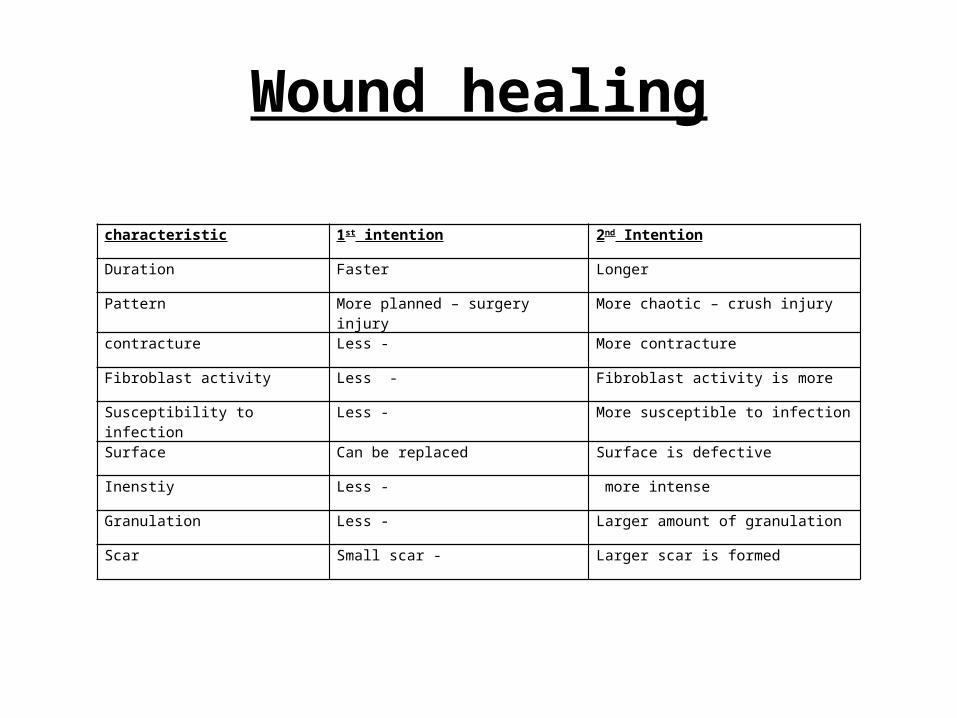
Wound healing
characteristic 1st intention 2nd Intention
Duration Faster Longer
Pattern More planned – surgery injury More chaotic – crush injury
contracture Less - More contracture
Fibroblast activity Less - Fibroblast activity is more
Susceptibility to infection Less - More susceptible to infection
Surface Can be replaced Surface is defective
Inenstiy Less - more intense
Granulation Less - Larger amount of granulation
Scar Small scar - Larger scar is formed
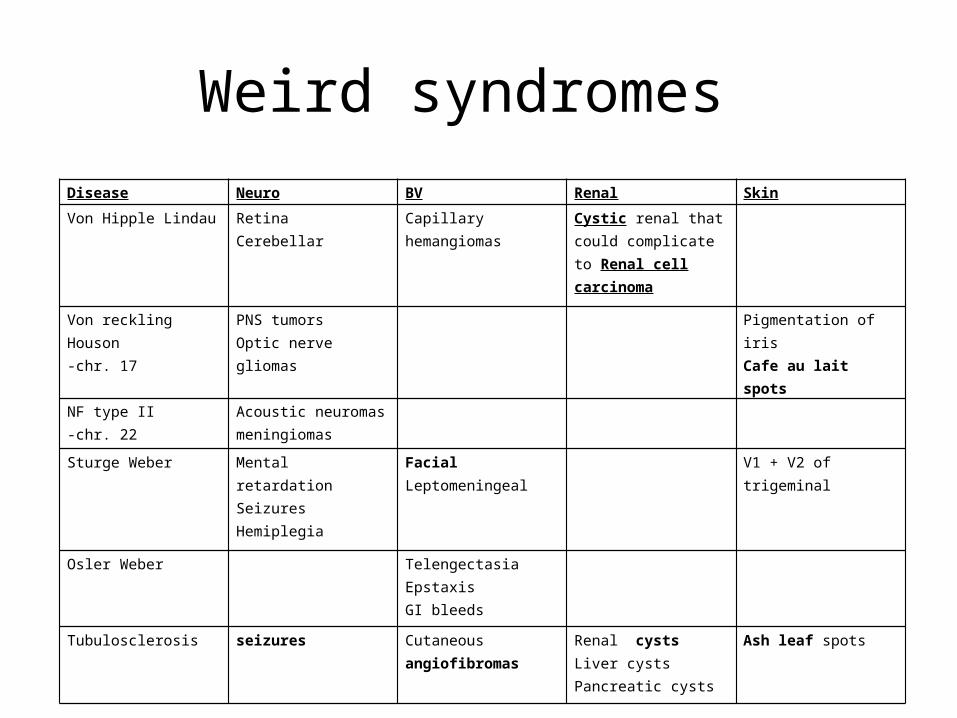
Weird syndromes Disease Neuro BV Renal Skin
Von Hipple Lindau Retina Cerebellar
Capillary hemangiomas Cystic renal that could complicate to Renal cell carcinoma
Von reckling Houson-chr. 17
PNS tumorsOptic nerve gliomas
Pigmentation of irisCafe au lait spots
NF type II-chr. 22
Acoustic neuromasmeningiomas
Sturge Weber Mental retardationSeizuresHemiplegia
Facial Leptomeningeal
V1 + V2 of trigeminal
Osler Weber TelengectasiaEpstaxisGI bleeds
Tubulosclerosis seizures Cutaneous angiofibromas Renal cystsLiver cystsPancreatic cysts
Ash leaf spots
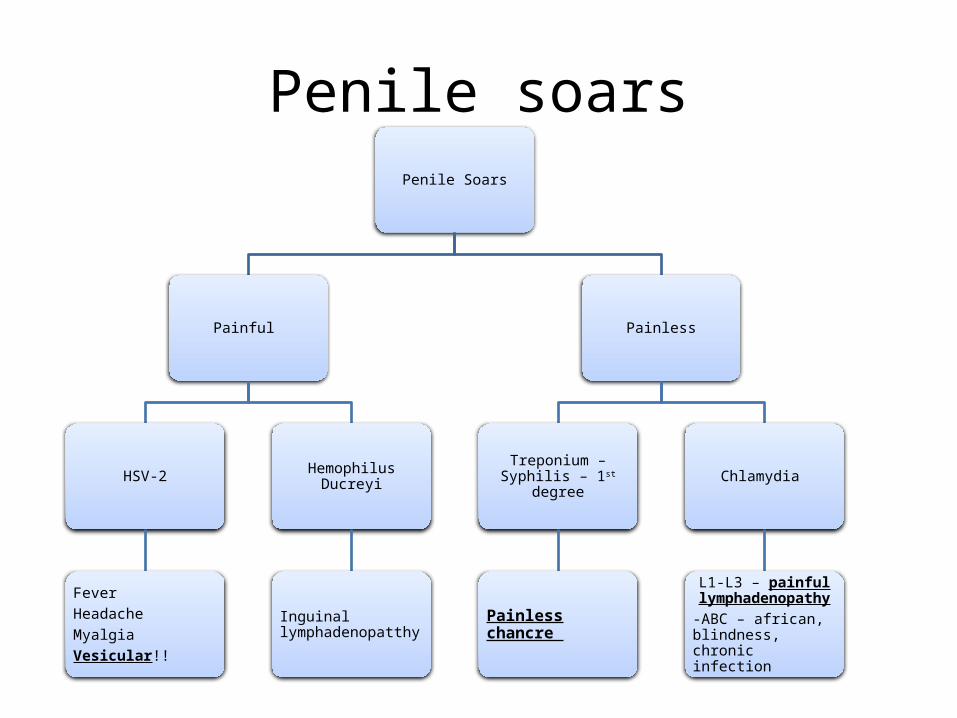
Penile soarsPenile Soars
Painful
HSV-2
FeverHeadacheMyalgiaVesicular!!
Hemophilus Ducreyi
Inguinal lymphadenopatthy
Painless
Treponium – Syphilis – 1st degree
Painless chancre
Chlamydia
L1-L3 – painful lymphadenopathy
-ABC – african, blindness, chronic infection

Alveolar pressure vs. Intrapleural pressure
Conditions Transpulmonary pressure
Alveolar pressure Pleural pressure
Physiological Always (+)!!! + during inspiration(-) During expiration
(-) 5
Pneumothorax 0 +1 +1
Transpulmonary = alveolar – pleural
1) Any lung volume - transpulmonary pressure is equal to and opposite to elastic recoil pressure of the lung
-thus, if elastic recoil pressure is (+) on exhalation, TP is (-)
2) Inhalation – lung volume pressure (inhalation) < lung volume pressure (exhalation)Exhalation – lung volume pressure (inhalation) > lung volume pressure (exhalation)
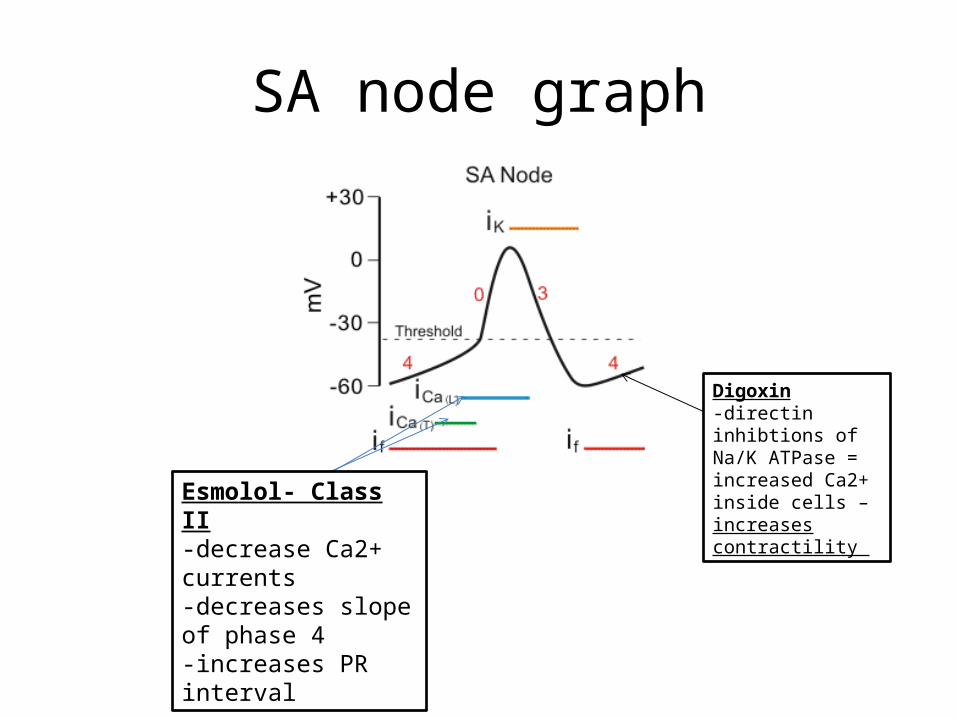
SA node graph
Digoxin-directin inhibtions of Na/K ATPase = increased Ca2+ inside cells – increases contractility Esmolol- Class II
-decrease Ca2+ currents-decreases slope of phase 4-increases PR interval

Adrenal physiology Cholesterol
Pregnolone
Progesterone
11 – DOC
Corticosterone
Aldosterone
17 OH preg
17-OH Progesterone
11 Deoxycortisol
Cortisol
Dehydroepialdosterone
Androstenodione
Testosterone
DHT
21
11 11
17
18
17
21
17 OH def => Hypertenion, decreased androgen synthesis21 OH def => Hypotension, increased androgen synthesis11 Oh def => Hypertension, increased androgen synthesis

Normal Adult DiahrreaWhole blood loss
Excessive infusion of normal saline
DiureticsAddisons 21-OH deficiency
EdemaRHFCirrhosisNephrotic syndrome
SIADHInc. H2O consumption
Osmotic diuresisSweating
Diabetic InsipidusFever
Antibiotics Inc. HCO3
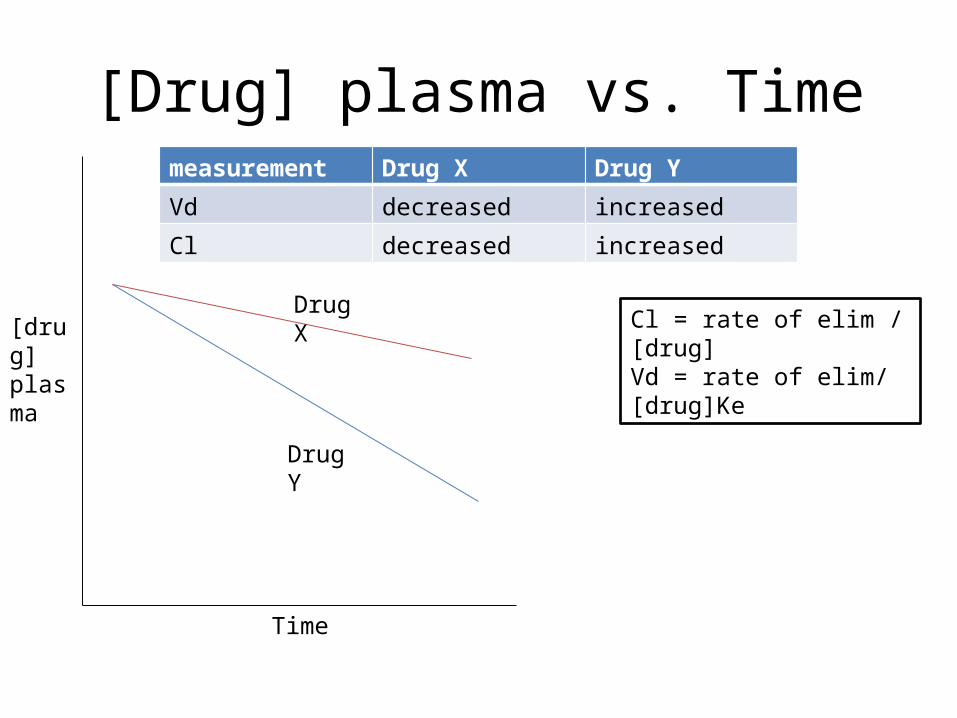
[Drug] plasma vs. Time
[drug]plasma
Time
Drug X
Drug Y
measurement Drug X Drug Y
Vd decreased increased
Cl decreased increased
Cl = rate of elim / [drug]Vd = rate of elim/ [drug]Ke
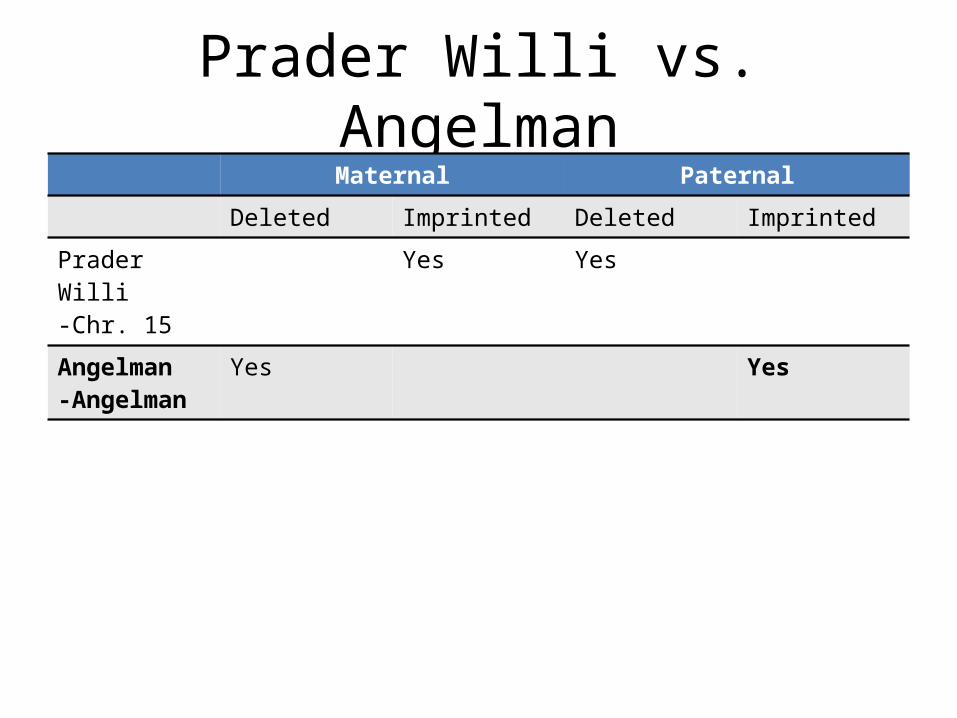
Prader Willi vs. AngelmanMaternal Paternal
Deleted Imprinted Deleted Imprinted
Prader Willi -Chr. 15
Yes Yes
Angelman-Angelman
Yes Yes

Galactose metabolism?Enzyme Clinical presentation Accumulation
Galactokinase K for cataracts!!!-galactosemia-no smile
Galactol
Uridyl transferase JaudiceHepatomegaly Mental retardation
Galactol
B-galactosidase Abdominal distentionDiahrrea
UDP galatose

ANP production
Hypertension
ANP release in response to
increased pressure
Atria
Increased blood volume?
Kidney-decreased
reabsorption of Na+ H2O
Ventricles
Due to LV hypertrophy due to
HTN
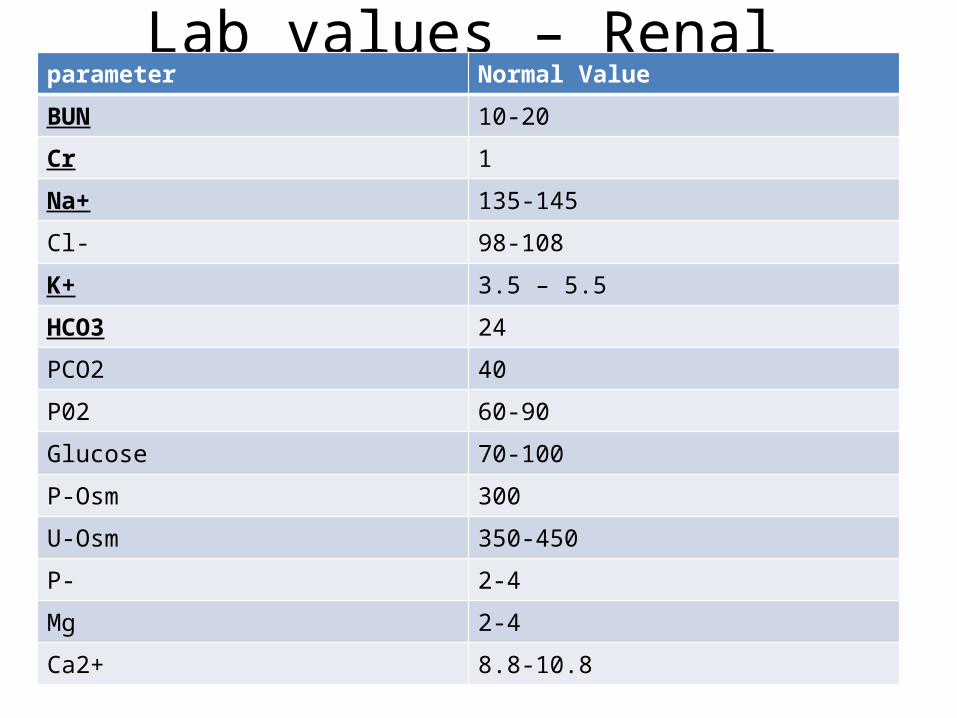
Lab values – Renal parameter Normal Value
BUN 10-20
Cr 1
Na+ 135-145
Cl- 98-108
K+ 3.5 – 5.5
HCO3 24
PCO2 40
P02 60-90
Glucose 70-100
P-Osm 300
U-Osm 350-450
P- 2-4
Mg 2-4
Ca2+ 8.8-10.8
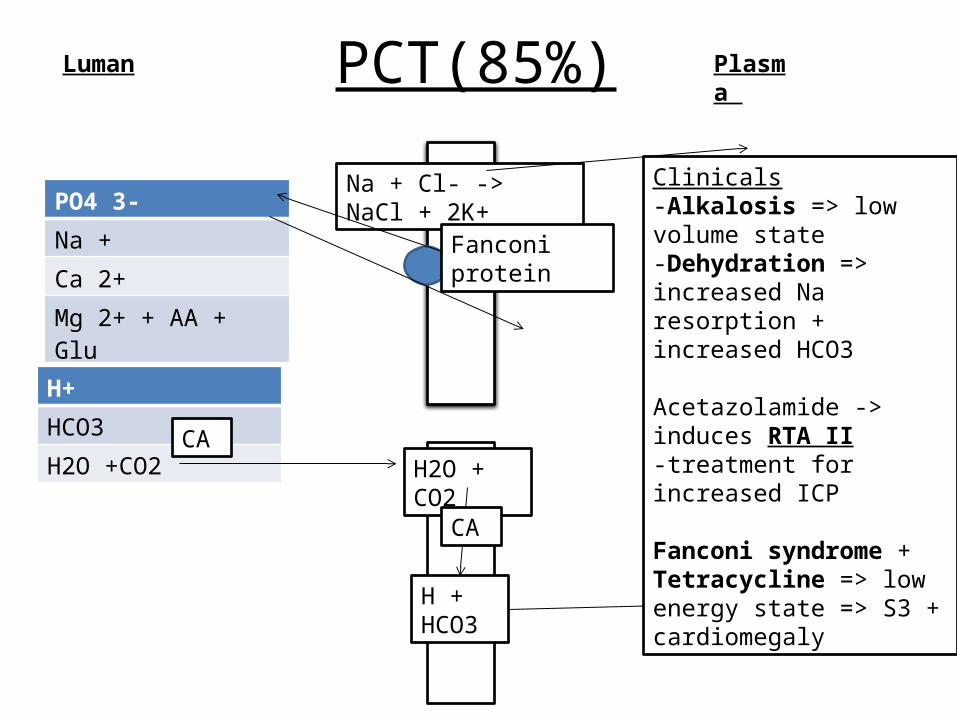
PCT(85%)Luman Plasma
H+
HCO3
H2O +CO2 H2O + CO2
H + HCO3 HCO3
Na + Cl- -> NaCl + 2K+ Clinicals-Alkalosis => low volume state-Dehydration => increased Na resorption + increased HCO3
Acetazolamide -> induces RTA II-treatment for increased ICP
Fanconi syndrome + Tetracycline => low energy state => S3 + cardiomegaly
CA
CA
PO4 3-
Na +
Ca 2+
Mg 2+ + AA + Glu
Fanconi protein

Loop of Henle – ascending Luman Plasma
Na
K
Mg
Ca
Cl- What to know:
1) Decreased urine Osm – diluting portion -
2) Furosemide, Toresemide, Butemide, Ethrynic acid
3) Barters syndrome!! – defective Na+/K+ ATPase – thus – hypomagnesmia + hypocalcemia
Gymnastics + Aneorexia + Bulemia

DCT lateLumen Plasma
K+
Na+
Ca2+
Aldosterone
PTHVit.DATPase
Clinical notes -Thiazides that act here cause hypokalemia How? – Low volume state – response is to increase aldosterone – results in hypokalemia!
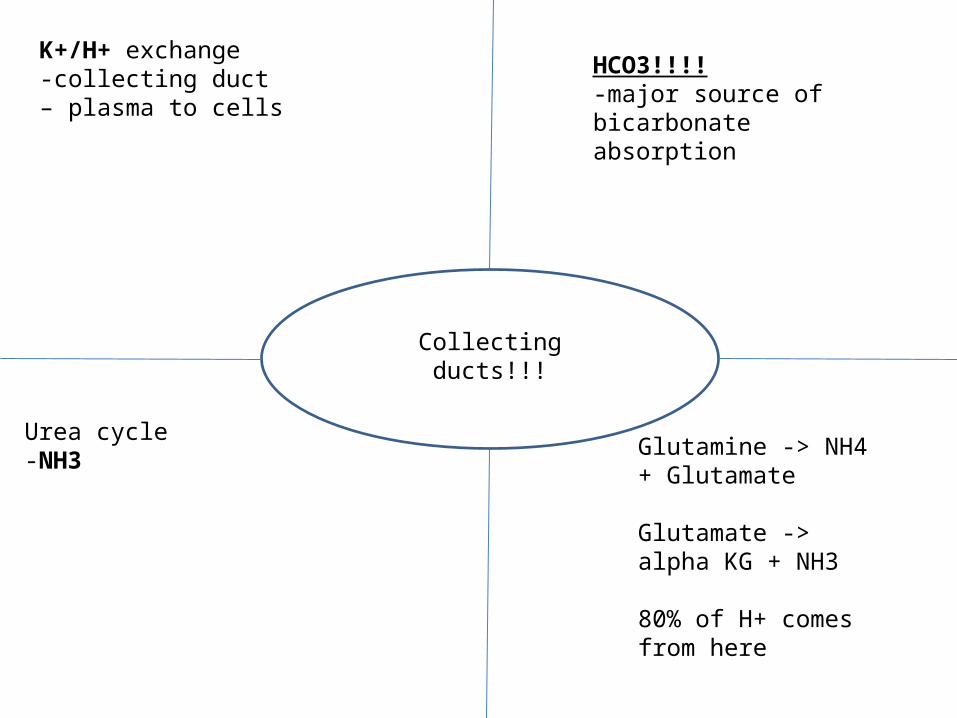
Collecting ducts!!!
K+/H+ exchange-collecting duct – plasma to cells
HCO3!!!!-major source of bicarbonate absorption
Urea cycle-NH3 Glutamine -> NH4 +
Glutamate
Glutamate -> alpha KG + NH3
80% of H+ comes from here

Asprin OD
Early • Respiratory alkalosis
Later• ASA gets absorbed• Results in met. Acidosis +
Resp. Alk • pH is NORMAL!!!
Increased absorption of ASA• Mixed acidosis => you
are ingesting more acid and retaining more CO2
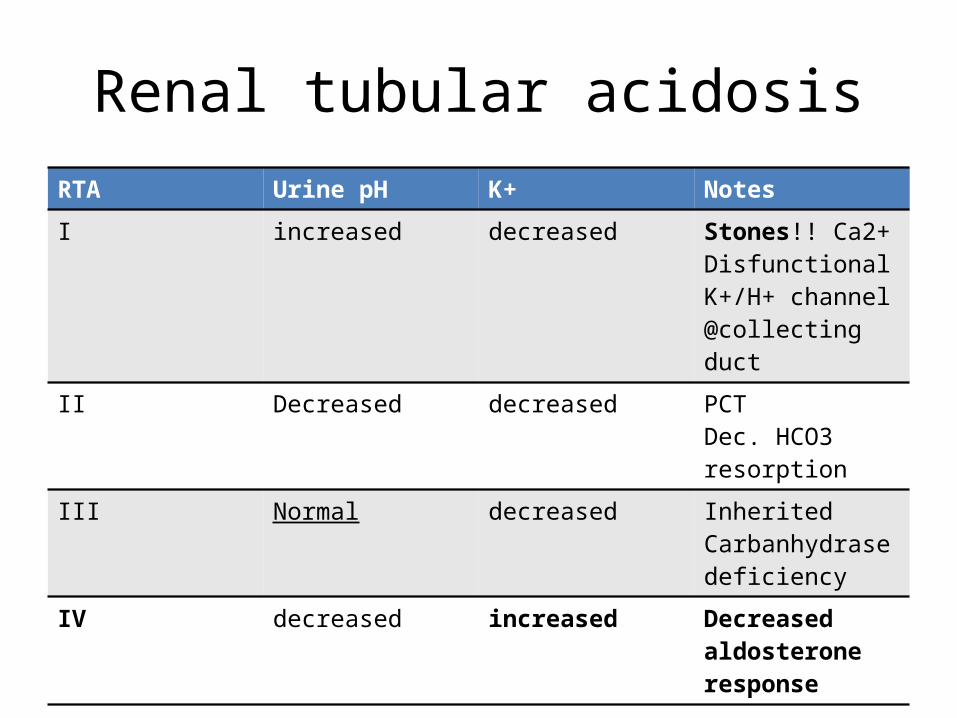
Renal tubular acidosisRTA Urine pH K+ Notes
I increased decreased Stones!! Ca2+Disfunctional K+/H+ channel @collecting duct
II Decreased decreased PCTDec. HCO3 resorption
III Normal decreased Inherited Carbanhydrase deficiency
IV decreased increased Decreased aldosterone response
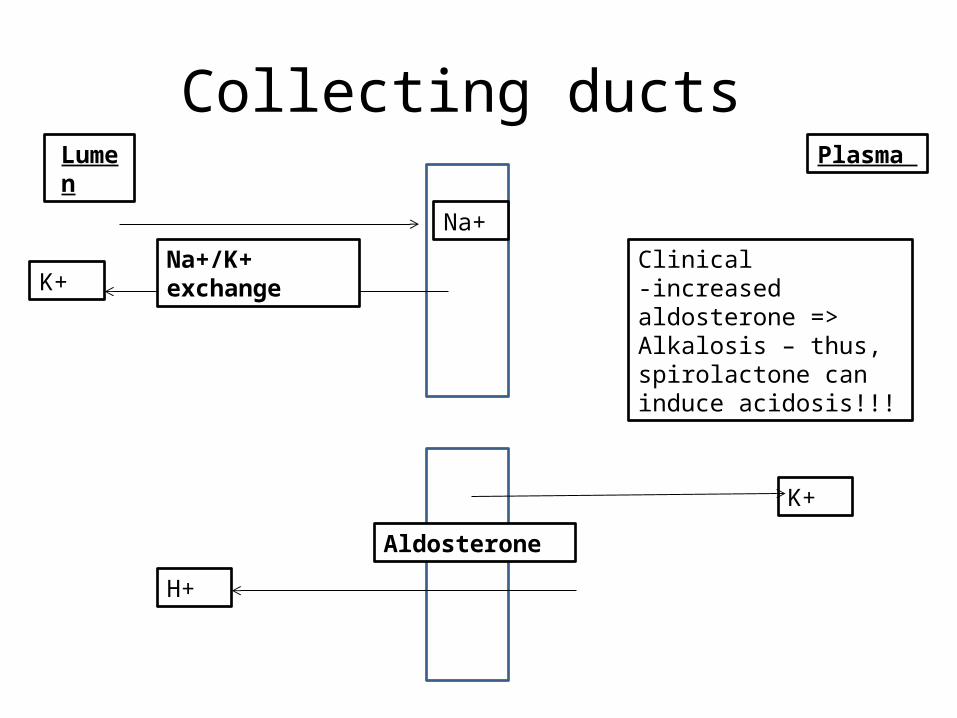
Collecting ducts Lumen Plasma
Na+
K+
K+
Na+/K+ exchange
Aldosterone
H+
Clinical-increased aldosterone => Alkalosis – thus, spirolactone can induce acidosis!!!
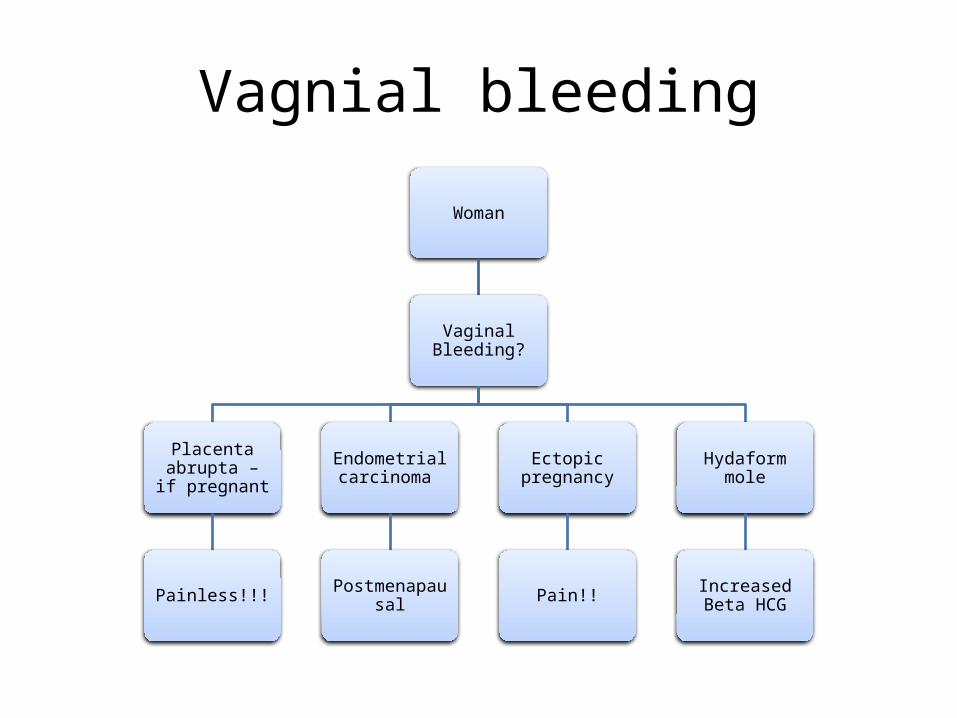
Vagnial bleeding
Woman
Vaginal Bleeding?
Placenta abrupta – if pregnant
Painless!!!
Endometrial carcinoma
Postmenapausal
Ectopic pregnancy
Pain!!
Hydaform mole
Increased Beta HCG
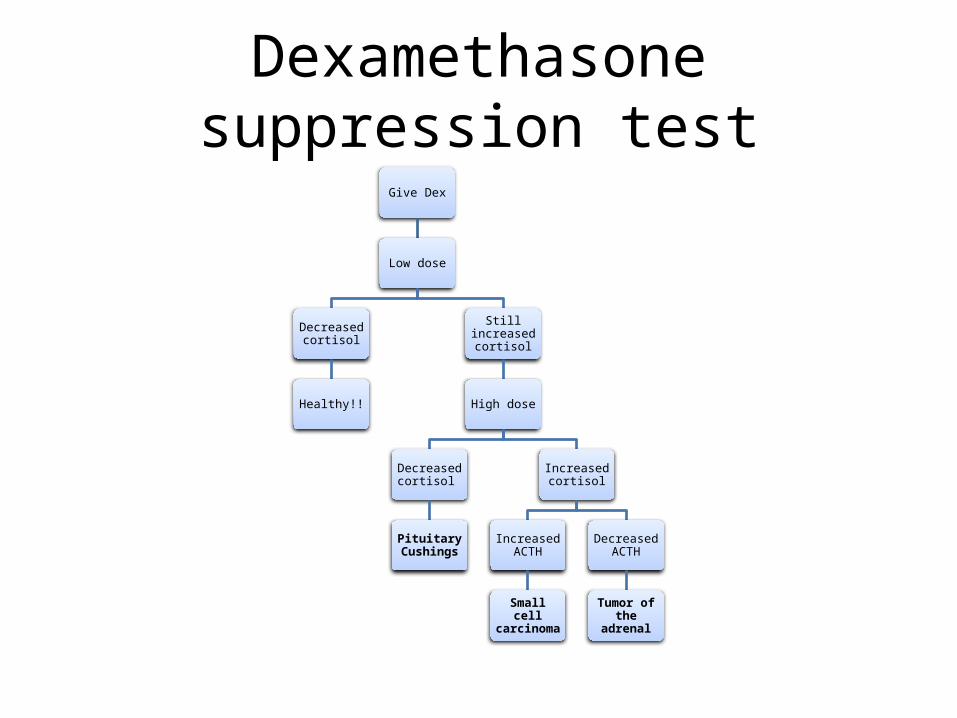
Dexamethasone suppression testGive Dex
Low dose
Decreased cortisol
Healthy!!
Still increased cortisol
High dose
Decreased cortisol
Pituitary Cushings
Increased cortisol
Increased ACTH
Small cell carcinoma
Decreased ACTH
Tumor of the adrenal
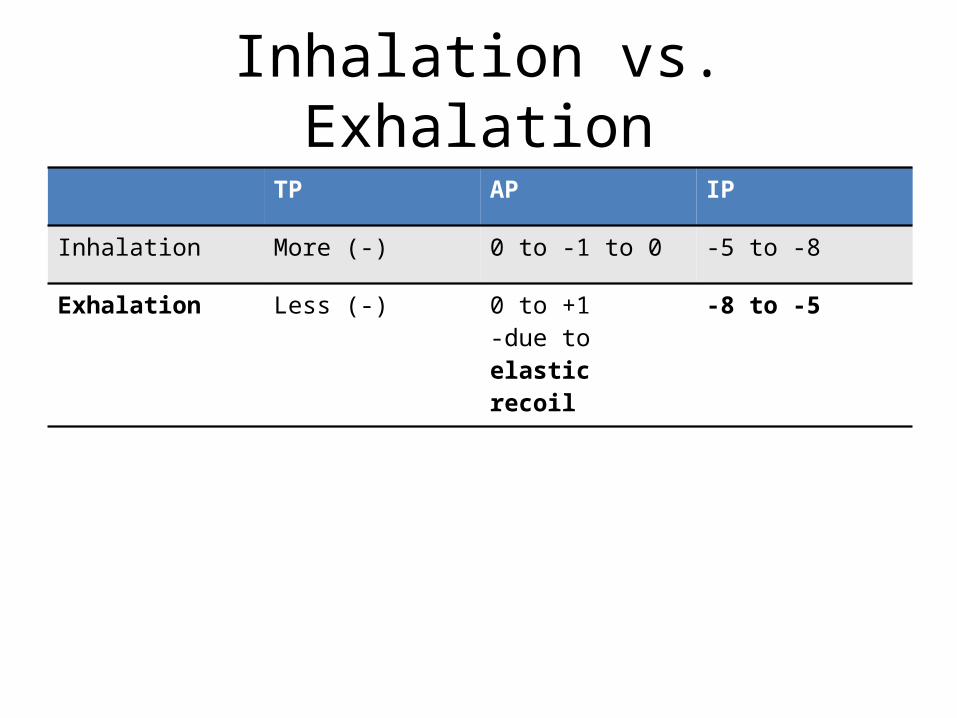
Inhalation vs. ExhalationTP AP IP
Inhalation More (-) 0 to -1 to 0 -5 to -8
Exhalation Less (-) 0 to +1-due to elastic recoil
-8 to -5

Joint pathologyJoint pain?
Erosive
1 joint
Asym
Goutpseudogout
Multiple joints
Asym
ReitersLyme
disease
Sym
B-19 infectionRheumatic feverRheumatoid arthritis – hours!Osteoarthritis - <30 mins + distal joints
Non-erosive
SLEFibromyalgia

Platelet vs. CoagulationBernard SoulierPT – normalPTT – normalPC – decreasedBT – increasedKW:GpIbadhesion
GlanzmannPT – normalPTT – normalPC – normalBT – decreasedKW:GpIIb/IIIaNo clumping!
ITPPT – normal PTT – normalPC – decreasedBT – increasedKW:Megakaryotcytes!
TTPPT – normal PTT – normalPC – decreasedBT – increasedKW:Pentade! – feverHUS
Hemophilia – factor VIIIPT – normalPTT – increasedPC – normalBT – increasedKW:-Xlinked recessive-hemarthrosis
VWFPT – normal PTT – normal OR increasedPC – normalBT – increasedKW:ADRistocretin test!
DICPT – increasedPTT – increasedPC – decreasedBT – increasedKW-trauma + spesis-shistocytes-fibrin split products
Vit K. Def PT – increasedPTT – increasedPC – normalBT – increasedKW-general-protein S + C
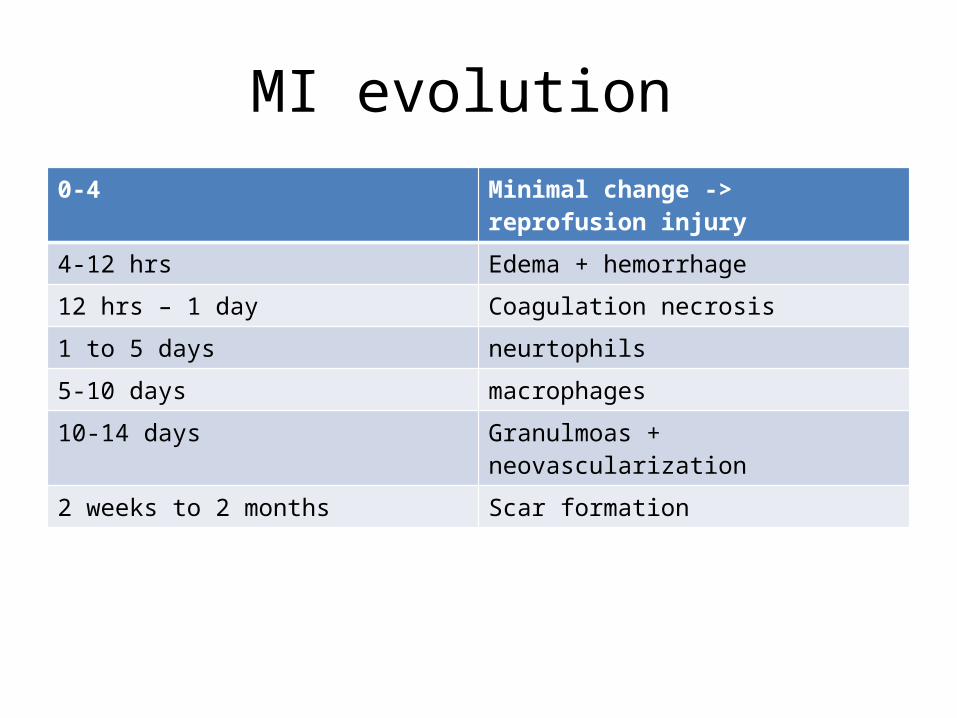
MI evolution 0-4 Minimal change -> reprofusion injury
4-12 hrs Edema + hemorrhage
12 hrs – 1 day Coagulation necrosis
1 to 5 days neurtophils
5-10 days macrophages
10-14 days Granulmoas + neovascularization
2 weeks to 2 months Scar formation
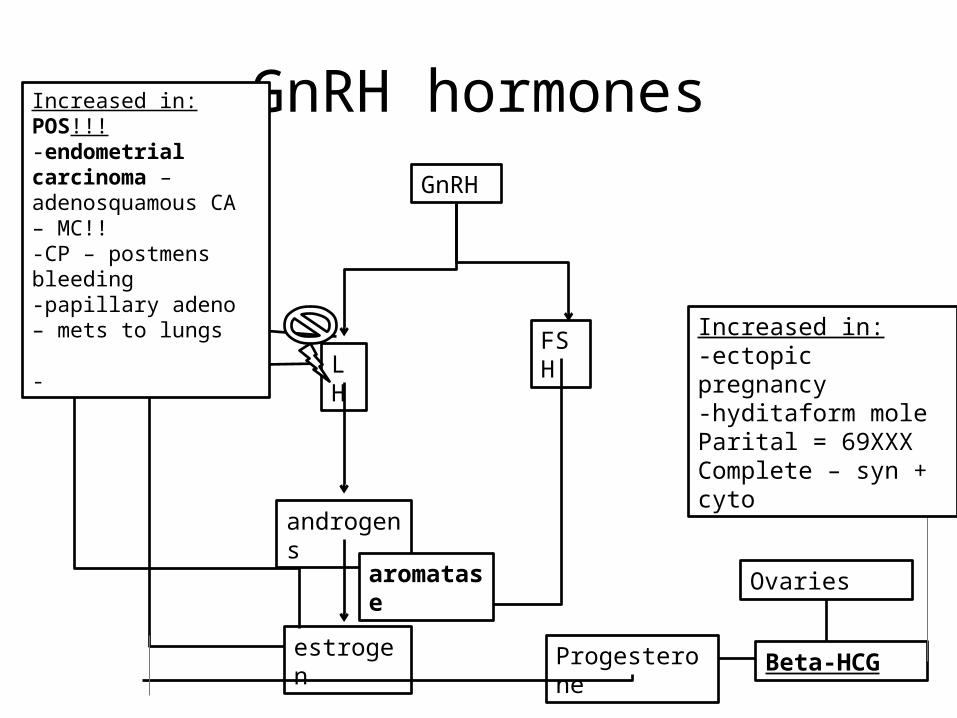
GnRH hormonesGnRH
FSHLH
androgens
estrogen
aromatase Ovaries
Progesterone Beta-HCG
Increased in:-ectopic pregnancy-hyditaform moleParital = 69XXXComplete – syn + cyto
Increased in: POS!!!-endometrial carcinoma – adenosquamous CA – MC!!-CP – postmens bleeding-papillary adeno – mets to lungs
-
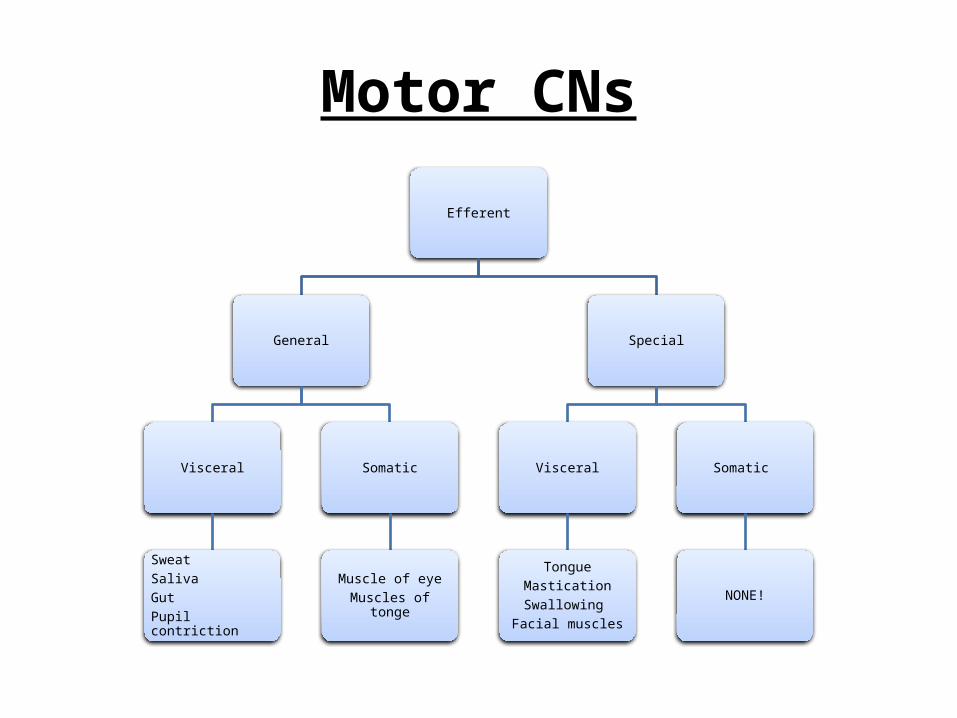
Motor CNs
Efferent
General
Visceral
SweatSalivaGutPupil contriction
Somatic
Muscle of eyeMuscles of tonge
Special
Visceral
TongueMasticationSwallowing
Facial muscles
Somatic
NONE!
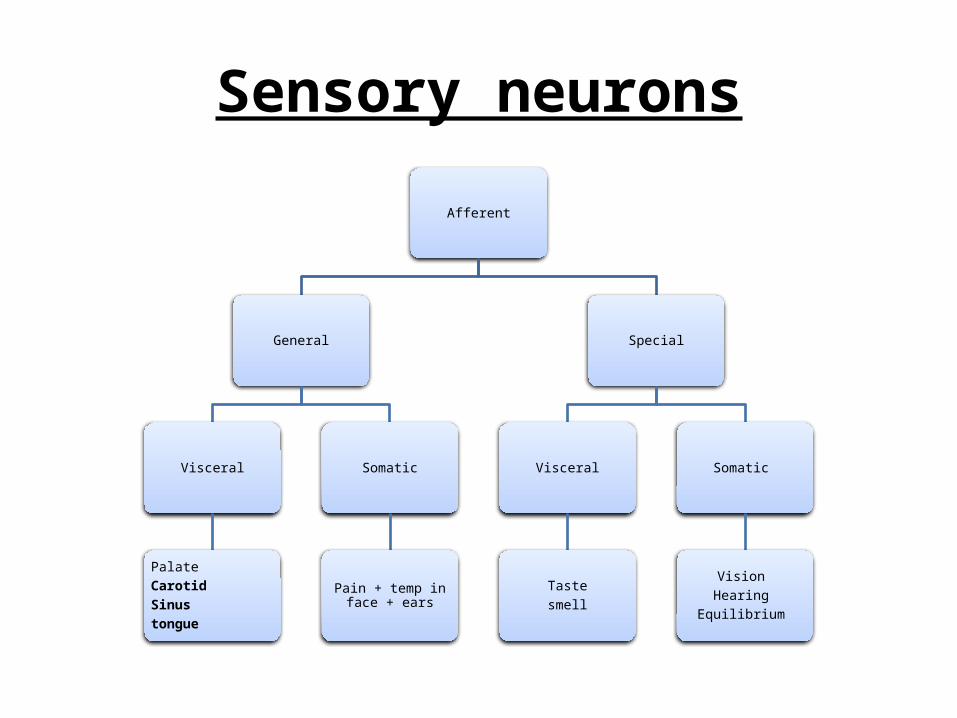
Sensory neurons
Afferent
General
Visceral
PalateCarotidSinustongue
Somatic
Pain + temp in face + ears
Special
Visceral
Tastesmell
Somatic
Vision Hearing
Equilibrium
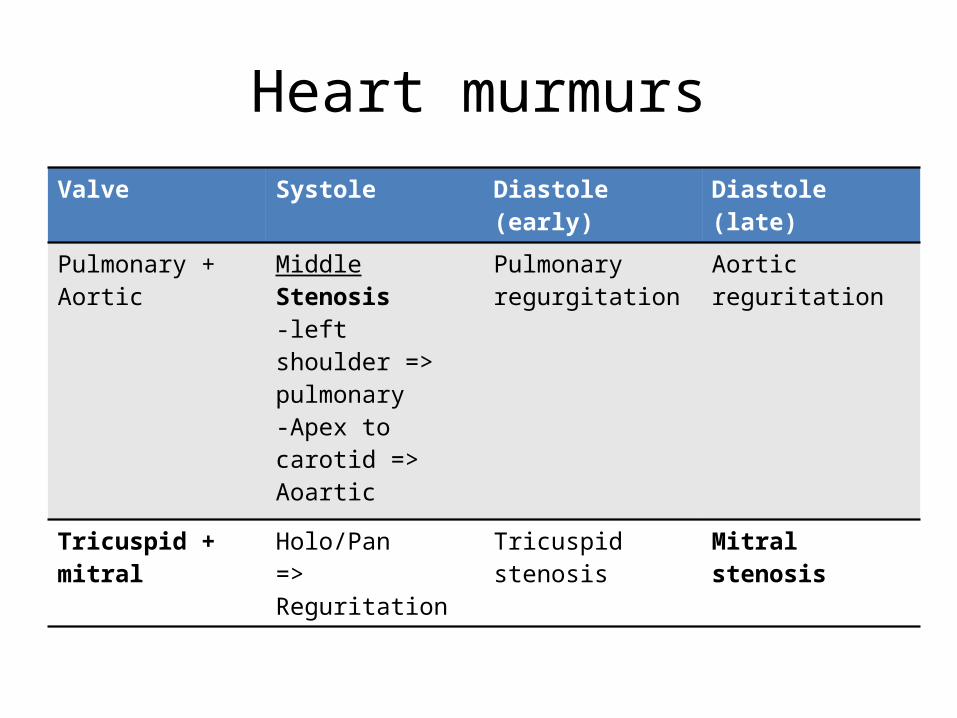
Heart murmursValve Systole Diastole (early) Diastole (late)
Pulmonary + Aortic MiddleStenosis-left shoulder => pulmonary-Apex to carotid => Aoartic
Pulmonary regurgitation
Aortic reguritation
Tricuspid + mitral Holo/Pan=> Reguritation
Tricuspid stenosis Mitral stenosis

Normocytic anemia
Non-haemolytic
ACDAplastic anemiaKidney disease
Hemolytic
Intravascular
Intrinsic extrinsic
Extravascular
Intrinsic Extrinsic
PNH Autoimmune coldMechanical traumaAortic stenosisProstethic valve
SpherocytosisG6PDPK defSickle CellHbC defectAutoimmune - warm
DIC TTPHUSInfectionMethyl DOPAPenicillin
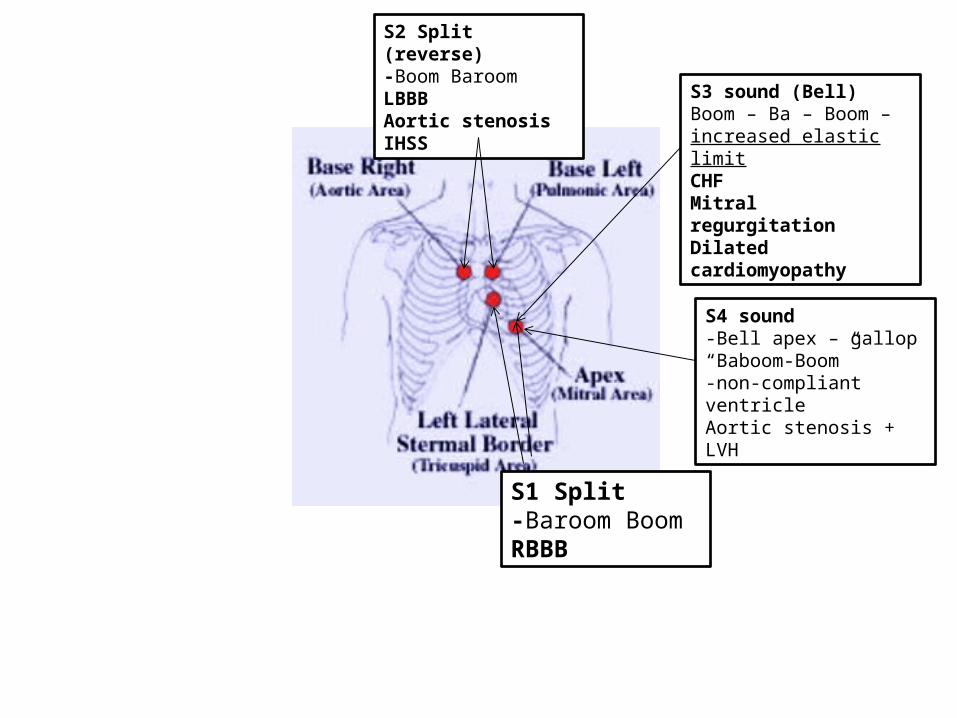
S1 Split-Baroom BoomRBBB
S2 Split (reverse)-Boom BaroomLBBBAortic stenosisIHSS
S3 sound (Bell)Boom – Ba – Boom – increased elastic limitCHFMitral regurgitationDilated cardiomyopathy
S4 sound-Bell apex – gallop“Baboom-Boom”-non-compliant ventricleAortic stenosis + LVH
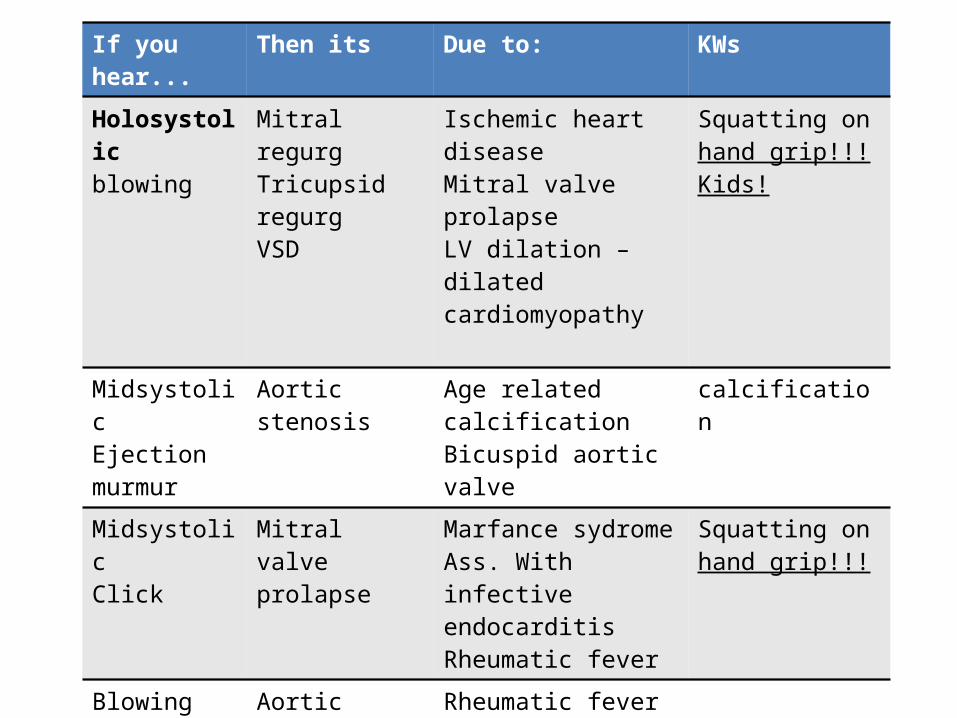
If you hear... Then its Due to: KWs
Holosystolicblowing
Mitral regurgTricupsid regurgVSD
Ischemic heart diseaseMitral valve prolapseLV dilation – dilated cardiomyopathy
Squatting on hand grip!!!Kids!
Midsystolic Ejection murmur
Aortic stenosis Age related calcificationBicuspid aortic valve
calcification
MidsystolicClick
Mitral valve prolapse
Marfance sydromeAss. With infective endocarditisRheumatic fever
Squatting on hand grip!!!
BlowingHigh pitcheddiastolic
Aortic regurgitation
Rheumatic fever Syphalis!!
Opening snap Rumbling
Mitral stenosis 2ndary rheumatic fever – buttonhole – fish mouth
Machinary like murmur
PDA child

















