Report Finalized in February 2020 Report Presented in March 2021
Drug Regimen Review Center
Valerie Gonzales, Pharm.D., Clinical Pharmacist Elena Martinez Alonso, B.Pharm., MSc MTSI, Medical Writer Lauren Heath, Pharm.D., MS, BCACP, Assistant Professor (Clinical) Alan Mark Abbinanti, Pharm.D. Candidate Jacob Crook, MStat, Data and Statistical Analyst Joanne LaFleur, Pharm.D., MSPH, Associate Professor
Contents Abbreviations ............................................................................................................................................................................ 3 Introduction ............................................................................................................................................................................... 4 How CGM Works ...................................................................................................................................................................... 5 Approved Indication and Device Features of Personal-Use CGM ........................................................................ 6
Table 1. CGM Device Features .............................................................................................................................. 8 rtCGM vs. isCGM ................................................................................................................................................................ 10 Insulin Pump Compatibility .......................................................................................................................................... 10
Safety Considerations .......................................................................................................................................................... 11 When to Use Fingerstick Testing (ie, SMBG) While on CGM ........................................................................... 11
Table 2. Finger-stick Testing for CGM Calibration and Initialization ................................................ 12 Other Key Warnings, Precautions, or Limitations............................................................................................... 12
Table 3. Select Warnings for CGM Devices ................................................................................................... 13 Adverse Event Information .......................................................................................................................................... 14
CGM Place in Therapy .......................................................................................................................................................... 15 Practical Considerations ................................................................................................................................................ 16 Candidates for CGM, Per Clinical Guidelines ......................................................................................................... 17 Considerations for Certain Subpopulations........................................................................................................... 18
Pregnant Women ......................................................................................................................................................... 18 T2DM with or without intensive insulin therapy ........................................................................................... 19 Pediatrics ......................................................................................................................................................................... 20
Recommendations Regarding How to Use CGM .................................................................................................. 21 CGM Glycemic Parameters ............................................................................................................................................ 21
Table 4. Time in Range Goals According to Expert Consensus Statement ....................................... 23 Medicaid Utilization .............................................................................................................................................................. 23 Prior Authorization Considerations .............................................................................................................................. 24 Summary ................................................................................................................................................................................... 28 References ................................................................................................................................................................................ 29 Appendix A: Additional CGM/Insulin Pump Systems Information ................................................................... 35 Appendix B: Additional Background Information ................................................................................................... 36
Table 1. Clinical Practice Guideline Recommendations for Continuous Glucose Monitoring .. 36 Table 2. Glycemic Targets per ADA and AACE/ACE Guidelines ........................................................... 38
3
Abbreviations A1c, glycosylated hemoglobin
AACE, American Association of Clinical Endocrinologists
Maintaining glycemic control in patients with diabetes mellitus reduces microvascular complications (eg, retinopathy, nephropathy) and macrovascular complications (eg, myocardial infarction, stroke) associated with chronic hyperglycemia.1 For certain patients, continuous glucose monitoring (CGM) serves as a tool for achieving and/or maintaining glycemic control. CGM can help reduce the burden of frequent self-monitoring of blood glucose (SMBG) by fingerstick testing. There is greater granularity in the glycemic data produced by CGM compared to SMBG.2 This can contribute to proactive response by the patient (via alerts or predictions from the device) and improve the provider’s ability to make more refined interpretations for optimizing insulin regimens or other medications, and advice regarding life-style factors.
This report will review the personal-use CGM devices, their unique features, along with the clinical guideline recommendations regarding the use of CGM. Personal-use devices owned by the patient are generally intended for ongoing use and provide un-blinded glycemic information to the patient so that they can intervene promptly to address problematic levels and trends. Professional CGM devices that are owned by healthcare clinics may also be used by the provider and patient, but on a temporary basis, to assess response to therapy adjustments and/or uncover problematic glycemic patterns and patient-specific factors influencing excursions.3,4 The personal-use devices reviewed can serve as stand-alone CGM devices. Some components can also interface with insulin pumps (Dexcom G6 pairs with the t:slim X2 insulin pump; and Guardian Sensor 3 and Link 3 transmitter pair with MiniMed 630G, 670G, and 770G insulin pumps).
Stand-Alone CGM Personal Systems • Dexcom G6 CGM System1 • Guardian Connect CGM System • FreeStyle Libre 14-day Flash Glucose Monitoring System • FreeStyle Libre 2 Flash Glucose Monitoring System • Eversense CGM System (with implantable sensor)
Key components of a CGM system include a glucose sensor, data transmitter, and a receiver (or referred to as a “reader”) by which the measured glucose level, trends, and alerts are communicated to the patient. Most CGM systems have a high level of accuracy for correspondence to blood glucose so are approved for patients with diabetes as a replacement for blood glucose testing such that the patient/provider can use the sensor glucose measurements to directly base treatment decisions.5-8 The exception is the Guardian Connect system, which is labeled for use as an adjunct to SMBG.9 Glucose readings from this device are not intended to be used for directly making therapy decisions but instead should be used to indicate when to perform SMBG fingerstick testing to confirm the CGM-sensor measurement.9 Yet, even CGM devices intended to replace SMBG for therapy decisions do not entirely eliminate the need to perform fingerstick testing. Fingerstick testing is required for calibration of some CGM devices and may be needed for verification purposes when symptoms or expectations do not correspond to the sensor-measured glucose reading.5-9 Further information regarding key features of
1 The Dexcom G5 CGM system is being phased out, no longer available after 2020
5
these devices will be reviewed along with CGM place in therapy for the management of diabetes mellitus (DM).
Methods
User manuals, manufacturers’ websites, and FDA 510(k) documents were referenced for information regarding the devices’ approved indication, features, directions for use, and safety warnings.
For information regarding the place in therapy of CGM for type 1 and 2 diabetes mellitus, clinical guidelines for the management of diabetes were accessed at the following websites:
• American Diabetes Association: https://care.diabetesjournals.org/content/44/Supplement_1 • American Association of Clinical Endocrinology: https://pro.aace.com/disease-state-
We were also aware of the 2017 guideline from the International Consensus Statement by an expert panel of the Advanced Technologies & Treatments for Diabetes (ATTD) Congress.10 References regarding CGM treatment goals and metrics (eg, Battelino et al 2019)2 were found among the citations of these recent clinical guidelines. To further clarify the place in therapy for subpopulations where evidence is more limited, particularly for patients who are not on intensive insulin therapy or for pregnant women, randomized controlled trials cited as rationale for guidelines recommendations and perspective related to these subgroups were reviewed. Literature produced from the article search of the February 2021 Utah Medicaid Pharmacy and Therapeutics Committee Review, Personal-Use Continuous Glucose Monitoring (CGM) Systems in Diabetes Mellitus, was also referenced for information to incorporate into this document.
How CGM Works
Continuous glucose monitoring systems measure glucose levels in the subcutaneous, interstitial fluid with a thin sensor filament placed through the skin (or implanted entirely under skin, as with Eversense).5-9,11,12 Readings are taken about every 1 to 5 minutes depending on the device. The glucose level in the interstitial fluid corresponds to the blood glucose level but can lag behind especially during times when the blood glucose is rapidly changing (≥ 2 mg/dL/minute, which can occur during exercise, post-prandially, or after an insulin dose).5-9,11,12 CGM devices are classified as real-time CGM (rtCGM) systems if they automatically display glucose levels continuously to the user: these include Dexcom G6, Eversense, and Guardian Connect. 5-9,11,12 The FreeStyle systems are classified as intermittently scanned CGM (isCGM) devices. While isCGM systems continuously measure glucose, the levels are displayed on the receiver only after the user has manually swiped the reader (ie, scanned) by the sensor on their arm.6,7,13 Data viewable between scans is largely retrospective; nonetheless, with a real-time alarm feature now incorporated into the newer isCGM model (FreeStyle Libre 2), patients are alerted to scan when reaching a high and low glucose threshold such that they are less likely to miss a hyper- or hypoglycemic episode.
The CGM data receiver (also called a reader or scanner for FreeStyle products) typically displays the measured glucose level, a trend arrow to reflect glucose change rates, a glucose trend graph covering
the last 8 hours, low glucose event tallies, time in target range, and visual alerts.5-9,11,12 Devices may also display recordings of meals/snacks, insulin use, exercise, and other events. Systems have varying alert and alarm capabilities to prompt the user to resolve low/high glucose levels or problematic trends. The user can make treatment decisions (eg, tailor insulin injection timing and doses) based on the glucose readings; or should confirm the reading with SMBG before making a treatment decision if using the device not approved for directly basing treatment decisions (Guardian Connect). Most devices also have predictive high/low alerts that allow the patient to proactively address scenarios where the device algorithm predicts their glucose will fall into the hypo or hyperglycemic threshold within the next 10 to 60 minutes (depending on the device and customization). This feature is intended to help prevent hypo and hyperglycemia episodes from occurring.5-9,11,12
Some systems must be used with a compatible smart-device (eg, iOS or Android smart-phone) that serves as the receiver since there is not a separate receiver offered by the manufacturer (as with Guardian Connect and Eversense). Data from CGM receivers, regardless of type, is uploadable to computer or web-based software where further data analysis can be carried out by the patient and prescriber. Cell phone applications that interface with CGM devices may also have sharing capabilities such that home caregivers (ie, family or friends) can see real-time glycemic levels and alerts to potentially help the patient respond to problematic levels if needed.
Considerable training and support, along with clinician follow-up for assessment of collected data is necessary to ensure proper device use and maximal benefits.13 Educational websites supported by device manufacturers are available with user-friendly manuals, quick guides, videos, etc. Patients need assistance not only learning the features of their device but also learning how to interpret the information displayed on the CGM receiver or from glucose profile summary reports generated from data analysis software; and how to respond to different alarms. The ADA guideline notes that “Programs that involve training and support have been shown to improve outcomes in both adults and children using isCGM …”13 Authors recommend “…robust diabetes education, training, and support…” in conjunction to the prescribing of CGM.13
In contrast to personal-use CGM, professional-use CGM devices owned by the clinic may be used in a blinded mode (ie, glucose levels not displayed to patient until the next office visit) depending on if the provider wishes to capture data in the patient’s natural state (ie, with glycemic patterns un-influenced by information from the device).4 Professional CGM can also be used to assess response to therapy adjustments and/or uncover problematic glycemic patterns (eg, nocturnal hypoglycemic) and patient-specific factors influencing excursions.10,14 If available to the patient, a clinic-owned device may be used if a patient does not have access to a personal device,13 or as a trial run for introduction to CGM; however, these are for temporary use (eg, up to 14 days depending on the device and prescriber direction).4
Approved Indication and Device Features of Personal-Use CGM
CGM systems are approved for the management of diabetes. Indications are not specific to diabetes mellitus type. Three systems are approved for adults and pediatric patients (Dexcom G6, Guardian Connect, and FreeStyle Libre 2; see specific approved age below) and 2 devices, Eversense and FreeStyle Libre 14 day system, are approved only for adults. Each device, except Guardian Connect, is approved to
7
replace SMBG for treatment decision-making. Guardian Connect is approved as an adjunctive device to SMBG where sensor glucose levels should be verified with fingerstick testing before making medication adjustments.
Dexcom G65
• Indicated for the management of diabetes in patients ≥2 years of age (youngest age for approval vs. other devices) and is intended to replace SMBG for making treatment decisions
• Has real-time alarms/alerts for high/low glucose levels, including predictive alert and rapid rise/fall alerts
• Sensor wear time is 10 days and does not need to be manually calibrated; the sensor has a 2-hour warm-up period following insertion during which time SMBG should be used as needed
• Does not require a smartphone for use; a receiver is available from the manufacturer but the system is also compatible with some smart devices that can serve as the receiver
Eversense8
• Indicated for continual measurement of glucose levels in patients ≥18 years of age and is intended to replace SMBG for treatment decisions
• Has real-time alarms/alerts for high/low glucose levels, including predictive alert, rate of change alerts, and on-body vibration alert (only device with on-body vibration capability)
• Implantable sensor that lasts up to 90 days and requires fingerstick calibration at least twice daily; the sensor has a 24-hour warm-up period after implantation during which time SMBG should be used as needed
• The transmitter is secured over the sensor using a silicone-based adhesive that is to be changed daily; the transmitter is removable—without wasting a sensor as would occur if removing other CGM transmitters in the middle of the sensor’s life-span
• Requires a smart device to serve as the receiver (eg, smartphone iOS or Android; no receiver available from the manufacturer)
Guardian Connect9
• Indicated for patients 14 to 75 years of age with diabetes and is intended for use adjunctive to SMBG, as it is not approved for directly basing treatment decisions
• Has real-time alarms/alerts for high/low glucose levels, including customizable predictive alerts and rapid rise/fall alerts
• The sensor wear time is 7 days and requires fingerstick calibration at least twice daily; SMBG is to be used during the 2-hour warm-up period as needed
• This system requires a smart device to server as the receiver (eg, smartphone iOS or Android; no receiver is available from the company)
8
FreeStyle Libre Systems6,7,15,16
• The newer FreeStyle Libre 2 system is approved for the management of diabetes in patients ≥4 years of age, whereas the earlier version, FreeStyle Libre 14-day, is approved for ≥18 years of age. Both devices are intended to replace blood glucose testing for diabetes treatment decisions.
• An up-grade in the Libre 2 system is its ability to provide a real-time high/low glucose alarm. The device alarms when the glucose passes the high or low glucose threshold (without having to scan) but the patient must scan the sensor with the reader to view the actual measured glucose level. The older device (Libre 14 day) does not have this real-time alarm capability, so the patient would receive an alert only after having scanned the sensor.
• For both FreeStyle Libre systems, the sensor and transmitter are in the same unit which simplifies application, whereas other CGM systems have these components separate. Both generations of Libre sensors have a 14-day wear time and use near field communication to transmit glucose levels/data when scanned by the receiver (ie, reader). These sensors do not require fingerstick calibration; however, during the first 12 hours of placing a new sensor, fingerstick testing must be used for treatment decisions.
• These Libre systems do not require a smart device since there is receiver available for each from the manufacturer. As an option, the Libre 14 day system can also be paired with a compatible smart device; the mobile application for Libre 2 is under FDA review.15
Table 1 summarizes the personal CGM device features.
Table 1. CGM Device Features 5-9,11,15-18 Device
Manufacturer
Dexcom G6
Dexcom
Guardian Connect
Medtronic
FreeStyle Libre 14-day
Abbott
FreeStyle Libre 2 Abbott
Eversense
Senseonics
Application Subcutaneously placed sensor filament attaches to skin patch to hold it in place and physically attaches to the transmitter
Sensor is implanted
Approved age for use ≥ 2 years 14 to 75 years ≥ 18 years ≥ 4 years ≥ 18 years
Approved for dosing
decisions
Yes No Yes; but, during first 12 hours of use fingerstick method must be used
Yes
Sensor 10 day maximum wear Site: abdomen
for adults; abdomen or buttock for
children ages 2-17 years
7 day maximum wear
(Guardian 3 sensor) Site: abdomen or the back of upper
arm
14 day maximum wear
Site: back of upper arm Holds 8 hours of data
Up to 90 day wear time Sensor is
implanted by the HCP to upper arm
Requires fingerstick
calibration of sensor
Noa Yes, twice daily; first and second
calibration up to 6 hours apart, then up
to 12 hours apart thereafter
No Yes, twice daily; levels will be unavailable if ≥16 hours have elapsed since previous calibration
9
Table 1. CGM Device Features 5-9,11,15-18 Device
Manufacturer
Dexcom G6
Dexcom
Guardian Connect
Medtronic
FreeStyle Libre 14-day
Abbott
FreeStyle Libre 2 Abbott
Eversense
Senseonics
Transmitter Lasts up to 3 months
Lasts up to 1 year or up to 122 cleanings (whichever comes
first); needs recharging about
every 7 days which can take up to 2
hours
Single sensor/transmitter unit lasting 14 days; uses near field communication
for reader scan
Lasts about 1 year; must
recharge daily x15 minutes.
Secured on skin directly over the
sensor; removable transmitter
without wasting a sensor
Libre 2 also uses bluetooth to send
high/low alarm
Receiver options
Dexcom G6 receiver
(touchscreen display);
receives data every 5 minutes
OR certain iOS and Android, smartphones and watches
Smartphone (iOS or android); no
separate product-specific receiver
available
Libre 14-d reader (has built-in test strip port for use
with FreeStyle Precision Neo
strip)
OR smartphone (iOS)
with LibreLink
Libre 2 reader: has built-in test strip port for use with
Yes, optional high/low rt-alarm (vibration/sound from receiver);
Has other messages but not in real-time (eg, predictive going
low message)
Yes; transmitter alerts with on-body vibration, and alerts with
sound/vibration via smart device;
high/low threshold alert;
customizable predictive alerts 10-30 minutes
in advance, and rate of change
alerts (1.5 - 5mg/dL/min);
calibration alert Warm Up
Time 2 hours; use SMBG during
warm up
2 hours; use SMBG during warm up
After 1 hour, readings will display but should not base treatment decisions on readings until after 12 hours; use SMBG
for first 12 hours
24 hours; use SMBG during
warm up
Insulin pump compatible
Can interface t:slim X2 pump
The Guardian Sensor 3 (plus Link 3 transmitter) can interface Minimed
Not able to interface with insulin pumps Not able to interface with insulin pumps
10
Table 1. CGM Device Features 5-9,11,15-18 Device
Manufacturer
Dexcom G6
Dexcom
Guardian Connect
Medtronic
FreeStyle Libre 14-day
Abbott
FreeStyle Libre 2 Abbott
Eversense
Senseonics
630G, 670G, 770G pumps
Data Sharing and Software
CLARITY Software: highlights patterns, trends and statistics; data sharable to patient’s clinic Dexcom Follow App allows data/alerts sharing with family/friends
Interfaces with CareLink website for data sharing with HCP and family/friends Sugar IQ App for iOS receivers: to analyze glucose levels in relation to food, exercise and insulin.
Can download last 90 day data to LibreView with either receiver; LibreView allows data share with HCP FreeStyle Libre Software: can view reports and change reader settings LibreLink for smartphone: sharable reports to up to 20 people with LibreLinkUp
Eversense data software application enables patients, caregivers, and provider to view and analyze glucose data
a A calibration code comes with the sensor to carry out auto-calibration; though, manual calibration is optional. If user selects manual calibration, it requires two fingerstick glucose values during start up and every 24 hours thereafter. Abbreviations: HCP, health-care provider;
rtCGM vs. isCGM
Small studies in adults with T1DM comparing rtCGM with isCGM have suggested that rtCGM may have greater benefits on outcomes such as prevention of hypoglycemia, reduced time in hypoglycemia, or improved time in range. The head-to-head comparative studies involved rtCGM with Guardian Connect or Dexcom G5 devices versus isCGM with FreeStyle Libre 14-day.19-21 Comparative randomized control trial (RCT) data is lacking to determine how rtCGM compares with the newer isCGM device, FreeStyle Libre 2, with real-time high/low alarms.13
With the FreeStyle Libre 14-day system there are no real-time alerts or real-time glucose levels provided; thus, the patient may miss the opportunity to address problematic levels at the time it occurs if they have not just scanned the sensor— likely a contributing reason rtCGM is superior to this particular isCGM device. With the Libre 2 system now having a real-time alarm, this prompts the patient to act at the time of the problematic level rather than only observing a problematic event retrospectively. Nonetheless, this device does not have a real-time predictive alert as most rtCGM devices do, to motivate proactive action by the patient before a problematic level occurs.
Insulin Pump Compatibility
Some insulin pumps are compatible with the Dexcom G6 CGM system or with certain Guardian Connect components (ie, Guardian Sensor 3). Integrated CGM/pump systems may be referred to as a sensor augmented insulin pump (SAP) system.13 SAPs have the ability to suspend insulin delivery when sensor-measured glucose is low (ie, low glucose suspend [LGS] function22), and some can also suspend insulin delivery based on a predicted low event (ie, predictive low glucose suspend [PLGS] function). PLGS
11
technology uses a predictive algorithm accounting for glucose trends to predict whether the sensor-measured glucose will reach/pass a preset low or high glucose value within the next 30 minutes.23 Some integrated CGM/insulin pump systems are known as automated insulin delivery (AID) systems if programmed to increase/decrease insulin delivery rates based on sensor measured levels in addition to insulin suspend functions. The term “hybrid closed-loop” (HCL) refers to first-generation AID systems with algorithmic technologies to automatically control insulin delivery, but which require the user to manually enter and confirm bolus doses for meals/snacks (ie, carbohydrate load must be announced).13,24
CGM/Insulin Pump Integrated Systems
o MiniMed 630G insulin pump with Guardian Sensor 3 and Guardian Link 3 transmitter CGM components functions a an SAP system with low glucose suspend (LGS) technology
o t:slim X2 insulin pump interfaced with Dexcom G6 CGM is available as an SAP system with predictive low glucose suspend (PLGS) technology (with Basal IQTM technology) or as a hybrid closed loop system (with Control IQTM technology)
o MiniMed 670G and 770G insulin pumps with Guardian Sensor 3 and Guardian Link 3 transmitter CGM components function as hybrid closed-loop systems
Appendix A provides more information regarding the MiniMed and t:slim X2 insulin pumps and related ADA guideline recommendations regarding pump/CGM systems.
Safety Considerations When to Use Fingerstick Testing (ie, SMBG) While on CGM Although CGM devices have potential to reduce the burden of fingerstick testing, depending on how often the patient was previously using SMBG per day, these devices do not entirely eliminate the need to perform fingerstick blood glucose testing. A fingerstick reading may be needed for any of the following scenarios:
a) When the user’s symptoms do not match or seem to correspond with the CGM measured glucose readings
b) When the device does not show a glucose value, or whenever the device signals to the patient to perform a fingerstick blood glucose test
c) Fingerstick testing may be needed during times of rapidly changing glucose (eg, ≥ 2 mg/dL per minute)7 prior to making a treatment decision
d) As required during the warm-up or initialization phase after a newly placed sensor (all devices); and for manual calibration of some devices (Guardian Connect and Eversense)
i. During the warm up period (first 2 hours for Dexcom G6 sensor and first 24 hours for Eversense sensor) or initialization phase (first 12 hours of use of the FreeStyle Libre sensors)5,8,18
ii. For calibration: both Guardian Connect and Eversense systems require ongoing fingerstick calibrations at least twice daily. The CGM readings from Eversense can be used to base treatment decisions only if daily calibration has been carried out properly.8,9
12
e) When making dosing/treatment decisions while using Guardian Connect, sensor measurements should be verified with SMBG and when the device indicates problematic glucose levels9
f) When temporarily taking medications that may interfere with the CGM glucose reading, SMBG should be relied upon for basing treatment decisions
Table 2. Fingerstick Testing for CGM Calibration and Initialization 5-9,15 Dexcom G6 Guardian Connect
FreeStyle
Libre 14-day FreeStyle
Libre 2 Eversense
No calibration required; SMBG is required during
initial 2 hour warm up of a newly placed sensor; sensor
replaced every 10 days
Calibration 3X on day 1 of new sensor, then
twice daily thereafter; sensor
replaced every 7 days
No calibration required; however SMBG is
required during first 12 hours of use of a newly placed sensor; sensor
replaced every 14 days
Calibrations required twice daily; SMBG also
required during the first 24 hours of a newly
placed sensor; the sensor is replaced every 90 days
Abbreviation: SMBG, self-monitoring of blood glucose Other Key Warnings, Precautions, or Limitations Dexcom G65
• The user guide advises to not use the device if the patient is pregnant, on dialysis, or critically ill due to the lack of information regarding the accuracy in these populations.
Eversense8
• Eversense CGM has not been tested in patients who are o pregnant or nursing, o critically ill or hospitalized, o receiving immunosuppressant therapy, chemotherapy, or anti-coagulants, o have another implanted device (eg, implanted defibrillator) o have allergies to glucocorticoids or who are using systemic glucocorticoids High level accuracy cannot be guaranteed in these patients
• This product incorporates a dexamethasone acetate, drug-eluting ring that slowly releases very low drug levels (about 3 micrograms per day25) to help minimize the body’s inflammatory response to the inserted sensor— a feature in common with implantable devices such as pacemakers where a steroid is used to improve tolerability. The systemic risk of such a low dose of dexamethasone is unclear.8
• A warm sensor, transmitter, or insertion site may signal local infection; if this occurs, the patient should remove the transmitter and contact their provider.
• The Eversense transmitter can move at night (related to physical contact of the area) leading to loss of connection with the transmitter.
13
FreeStyle Libre systems6,7,15,16,18
• User guides for the Libre CGM systems advise against their use in pregnant women, patients on dialysis, or critically ill patients since these devices have not been FDA approved for use in these groups.6,7,12
• Additionally, the user guide for Libre 14-day states that the device’s performance is undetermined during use with another implanted medical device such as a pacemaker.
• While the Libre 2 system has a real-time alarm, the previous generation does not have a real-time alarm so the alerts are only activated once the patient scans the sensor. This system without alarms has not been studied in patients with hypoglycemic unawareness.
Guardian Connect9 • This device is contraindicated for patients who are unwilling or unable to perform a minimum of 2
blood glucose tests by fingerstick per day (as required for calibration of the device) or for patients who do not maintain contact with healthcare professional.
Drug Interactions: Table 3 lists interfering agents for these products. Specific dosage thresholds may not be available for every offending agent. The patient should not rely on the sensor measured glucose reading for basing treatment decisions while taking these agents or surpassing the interference dosage threshold; fingerstick testing should be used as appropriate.
intended for pregnant women, people on dialysis, or critically ill patients
• CI: Remove device before MRI, CT, or HFEH
• Avoid AIT and placing device parts through baggage x-ray machine
• CI: Not intended for those unwilling or unable to (a) perform a minimum of 2 BG tests (fingersticks) per day, or (b) maintain contact with healthcare professional
• Remove device before MRI, CT, HFEH or other devices generating strong magnetic fields (eg, x-ray)
• CI: Remove device before MRI, CT scan, X-ray, or HFEH
• Not approved for pregnant women, people on dialysis, or critically ill patients
• Not intended for pregnant women, people on dialysis, or critically ill patients; or to be used with implanted devices such as pacemakers
• CI: Remove sensor and transmitter before MRI, CT, HFEH, and X-ray
• CI: Not intended to use with AID systems
• MRI, X-ray, and CT are safe when transmitter is removed (CI otherwise)
• Close contact with direct EMI may interfere with data transmission to receiver
• CI: do not use if patient has contraindication to dexamethasone (DEX) or DEX acetate
• Has not been studied in pregnant or nursing women; people <18 years; critically ill or hospitalized patients; people on immunosuppressants, chemotherapy, or anti-coagulants; those with another active implantable device (eg, defibrillator); or with known allergies to or use with systemic glucocorticoids (including inhaled). Accuracy in these populations is unclear
may falsely raise reading APAP >1g every 6 hours may falsely raise reading
APAP may falsely raise reading (specific levels not defined in user guide)
Vitamin C can falsely raise reading; aspirin >650mg may falsely lower reading16
Vitamin C >500 mg/day can falsely raise reading
CI: IV mannitol and IV sorbitol (or as a component of an irrigation or peritoneal dialysis solution) may falsely raise reading Tetracycline antibiotics may falsely lower sensor glucose level
Adhesive patches used to attach CGM sensor/transmitters to the skin can cause skin irritation or allergic reaction.26 These CGM devices come with their own incorporated adhesive, but there are various adhesive options by other manufacturers that can be used for additional support or as a skin barrier for managing skin irritation.26,27 Full transparency regarding the complete list of ingredients used in adhesive products is often lacking which can obscure determination the culprit ingredient contributing to irritation or allergic reaction;28,29 trial and error approach is often used. Allergy patch testing may also be considered.13,30
If a patient requires a physical skin barrier in order to tolerate a certain device’s adhesive, the skin barrier may need replacing sooner than would otherwise be needed for the sensor, for example every 7 days31,32 (per product directions for use); thus, patients may need additional sensors to accommodate skin irritation prevention measures. Additional sensors may also be needed if dislodged, unintentionally from physical contact or intentionally (eg, for CT/MRI scan or for other reasons), as sensors are not re-usable once taken out from their insertion site.
Eversense incorporates a silicone-based adhesive for attachment of the transmitter. The silicone adhesive is associated with a low risk of skin irritation and is expected to cause less reactions than acrylate-based adhesives;25 though, direct comparisons are lacking. As with other devices, some patients may require additional adhesives or barriers depending on patient-specific factors (eg, sports, heavy perspiration, restless sleep, skin irritation).33
Adverse Event Information
Adverse Events (AEs) Reported in User Guides
• Dexcom G6: No device-related, serious AE occurred during trials. Among 374 sensors placed, 24 mild to moderate AEs occurred including skin irritation (eg, erythema or edema), and mild to moderate excoriation and infection.5
15
• Eversense: based on data from the PRECISE II and PRECISION studies, the most frequent AE reported was pain/discomfort (4% of patients). Others at lower incidence included device fragment unrecovered or additional procedure to remove sensor following a first attempt (each in 1.6% of patients); AEs occurring in <1% of patients included redness, dermatitis, bruising, hyperpigmentation, paresthesia, and syncope.8
• FreeStyle Libre 14-day: No device-related serious AEs from studies are reported. Mild skin irritations at the insertion site occurred in 8% of patients (eg, erythema, bruising, bleeding, infection).7
• FreeStyle Libre 2: No device-related serious AEs from studies are reported. Mild skin irritations were reported at the insertion site/adhesive area in 7% of adults (eg, pain, erythema, bruising, bleeding, scabbing); and in children, erythema, edema, mild bleeding, mild induration, and mild rash were reported (patient incidence not reported).6
• Guardian Connect: No device-related moderate or severe AEs were reported. General risks related to sensor insertion (as with other sensors) are the following: skin irritation, bruising, swelling, discomfort, redness, bleeding, pain/soreness/tenderness, rash, scarring, local infection, allergic reaction to adhesive, and fainting.9
Observational registry data from 2010-2014 (with previous generations of CGM devices) showed the top reason for discontinuing a personal CGM device within the first year was discomfort (18% of patients who were on CGM); others included inadequate adhesive bonding (13%), too many alarms (12%), interference with sports and activities (8%), and skin reactions (8%).34
CGM Place in Therapy Patients on intensive-insulin therapy (ie, multiple daily insulin injections [MDI; prandial and basal insulin] or continuous subcutaneous insulin infusion [CSII]) who monitor glucose by SMBG typically require 6 to 10 fingerstick tests per day to determine pre-meal/snack glucose, bedtime glucose, occasional post-prandial glucose, and pre-exercise glucose; to address suspected hypoglycemia or to monitor levels after having treated hypoglycemia symptoms; and for monitoring prior to performing critical tasks (ie, driving).1 Intensive insulin therapy users are most all T1DM patients, a subset of T2DM patients, and may potentially include others classified/diagnosed with other forms of diabetes mellitus (eg, monogenic diabetes syndrome, diseases of the exocrine pancreas such as cystic fibrosis and pancreatitis, drug- or chemical-induced diabetes, gestational diabetes mellitus).35,36 CGM has the potential to reduce the burden of fingerstick testing in high frequency users of SMBG. Integration of CGM into diabetes management can also be a useful tool for tailoring medication dosing/timing, preventing hypoglycemia, and improving glycemic control. Nonetheless, personal-use CGM devices do require dedication for near daily use for optimal benefits beyond those with SMBG.13,37 Improved glycemic control with CGM vs. SMBG was demonstrated in RCTs where CGM was used on a near daily basis (eg, wear time of at least 85%), particularly in pediatric patients.13,34,38-40 CGM summary metrics such as time in range and the ambulatory profile graph are reliable if at least 70% of possible readings are captured over the previous 14 days.10 Further information regarding CGM glycemic metrics and targets are provided on page 21.
16
Practical Considerations Pros of CGM over SMBG
• CGM can uncover hypoglycemic and hyperglycemic events otherwise undetected in between SMBG readings.41 SMBG method often misses nocturnal and asymptomatic hypoglycemia events.10
• Real-time glucose information and real-time alarms with CGM systems can lead to prompt action by the patient to resolve problematic levels or trends; predictive alarms can help the patient prevent hypoglycemia episodes.
• Continuous monitoring reveals whether the patient’s glucose levels are rising, falling, or constant; whereas, dispersed SMBG measurements do not reveal the direction of change. Not knowing the direction of glucose change could result in suboptimal response by the patient (eg, carbohydrate intake or insulin dose too high or too low).10
• The metrics provided with CGM can allow the prescriber to better tailor the patient’s medication regimen. The standardized CGM ambulatory glucose profile graph visually shows the patient/provider the general time frame of glycemic excursions and glycemic variability based on data over several days (eg, 14 days collapsed into a 24-hour period with median and various percentiles shown); individual day to day reports can also be generated for comparisons.
• Patients may be more willing to tightly manage their glucose (ie, with less fear about hypoglycemia42 or nocturnal hypoglycemia) while using CGM devices that have alarms/alerts to help the patient proactively address an impending low glucose event (via predictive low alert).
• With CGM, patients have opportunity to better understand how decisions regarding food, activity, or lifestyle directly impact their glycemic control.38 These daily factors may become more tangible for the patient, possibly motivating more positive behavior with respect to physical activity and food choices.43 Improved understanding of glycemic patterns may also help relieve reluctance to advance pharmacotherapy for improvement of glycemic control.3
• RCT evidence has shown a reduction in emergency department (ED) visits with rtCGM vs. SMBG in adults with T1DM or T2DM;44 positive outcomes in ED or hospital admission in T1DM have also been reported in observational studies using rtCGM.45-48 Observational evidence suggests a tendency of reduced diabetic ketoacidosis admissions in T1DM following initiation of isCGM; however, there is some inconsistent findings from these isCGM observational studies regarding improvements in hypoglycemia-related hospital admissions.49,50
Cons of CGM
• Requires more training and support compared to SMBG (ie, more resources and time by provider). Patient/or their caregiver must be able to understand all the features of the device, directions for use, and how to interpret and respond to CGM data and alerts. Providers must dedicate ample time for training patients as some patients may prefer in-person training. CGM does not eliminate the need for SMBG so patients should also know how and when SMBG testing should be carried out while using their CGM device.
• Alert fatigue is possible (ie, patient thinking there are too many alarms)34,51 • Local skin reactions to adhesives may become a barrier28
17
• Depending on the patient’s physical activities, size or placement location may be an issue.34 Depending on the device, sensors are inserted either on the abdomen, upper buttock, or back of upper arm.
Candidates for CGM, Per Clinical Guidelines
A summary table for clinical guideline recommendations regarding CGM is provided in Table 1 of Appendix B.
The ADA guideline describes that “CGM serves an important role in assessing the effectiveness and safety of treatment in many patients with type 1 diabetes, including prevention of hypoglycemia, and in selected patients with type 2 diabetes, such as in those on intensive insulin regimens and in those on regimens associated with hypoglycemia.”1
ADA 2021 summary recommendations2: When devices are used properly, rtCGM is useful for lowering and/or maintaining hemoglobin A1c (A1c) levels and/or reducing hypoglycemia in adults and youth with diabetes while treated with intensive insulin therapy (A level evidence) or other forms of insulin therapy, though with lower level of evidence (C level evidence) with non-intensive insulin therapy.13 rtCGM can be particularly useful for patients with hypoglycemia unawareness and/or frequent hypoglycemic episodes who are on insulin. isCGM can be useful while on MDI, CSII (B level evidence), or other insulin regimens (C level evidence), for lowering A1c and/or reducing hypoglycemia to replace SMBG in adults and youth with diabetes. In patients with diabetes on non-insulin or basal insulin regimens, professional-use CGM or intermittently-used CGM can be helpful for improving A1c and identifying and correcting patterns of hyper- and hypoglycemia (C level evidence).13
AACE/ACE 2020 and 2016 consensus statements: For patients with T2DM, personal CGM devices are recommended for patients who are on intensive insulin therapy (3+ injections/day or CSII), patients with hypoglycemia unawareness, or patients with recurrent hypoglycemia.3,52 Professional-use CGM is recommended for consideration if patients are not achieving glycemic goals after 3 months of therapy or for those on medications associated with hypoglycemia (sulfonylurea, glinide, or insulin).3 These recommendations were based on previous work of the panel for their 2016 consensus statement regarding glucose monitoring. In the 2016 consensus statement authors also recommended CGM for adults and children with T1DM, especially those with history of severe hypoglycemia or hypoglycemia unawareness, or those not meeting glycemic goals.52
The 2017 International Consensus recommended that CGM (in conjunction with A1c monitoring) should be considered for all patients with T1DM and patients with T2DM receiving intensive insulin therapy who are not meeting glycemic targets especially if having problematic hypoglycemia episodes.
Altogether, guidelines cite numerous studies in children and adults with T1DM on CSII or MDI showing improvement in glycemic outcomes such as reduced A1c in previously uncontrolled patients and 2 ADA Standards of Care and ATTD International Consensus levels of evidence: A= Clear evidence from well-conducted, generalizable RCTs that are adequately powered; B= Supportive evidence from well-conducted cohort or case-control studies; C= Supportive evidence from poorly controlled or uncontrolled studies; E= Expert consensus or clinical experience.
18
reduced episodes of hypoglycemia or time spent in hypoglycemia with CGM vs. SMBG.10,13,52-54 Observational evidence also suggests improvements in quality of life with CGM.13 ADA guideline recommendation for the use of CGM in pediatric and adult T1DM is supported by level A and B evidence respective to rtCGM and isCGM.13 In T2DM, significant reductions in A1c have been demonstrated with unblinded, personal-use rtCGM in those on intensive-insulin therapy,38 and with non-intensive insulin or noninsulin regimens (but in low quality studies).13,55,56 Studies with unblinded personal-use isCGM reporting outcomes for T2DM (separately from T1DM) have been inconsistent; but, individually, one study suggested reduced time spent in a hypoglycemia57 and another suggested greater A1c reduction58 with isCGM vs. SMBG, both in patients on intensive insulin therapy. Guidelines note limited data showing benefit of rtCGM for gestational diabetes mellitus or T2DM not requiring insulin.10,13
Considerations for Certain Subpopulations Pregnant Women
Uncontrolled diabetes during pregnancy is associated with poor perinatal and neonatal outcomes such as fetal anomalies, preeclampsia, macrosomia, and neonatal hypoglycemia.59 Insulin is the first-line therapy for pregnant women with diabetes.60 In all pregnant women with diabetes, fasting and postprandial SMBG are recommended. In addition, for those on intensive insulin therapy, pre-prandial testing is also recommended for optimization the rapid-acting insulin dosage.60
While the 2021 ADA guideline states that CGM can be useful as an adjunct to pre and post-meal SMBG for pregnant women with diabetes to achieve A1c targets (level B evidence), CGM metrics should not be used as a substitute for pre- and post-prandial SMBG.60 In other words, patients should continue to perform fasting and postprandial SMBG since robust studies are not yet available to support CGM as a replacement to SMBG for treatment decision-making in pregnant women. Furthermore, high level accuracy of these devices has not been verified in this population per CGM device user manuals. Alternatively, evidence supporting adjunctive use of CGM in pregnancy is based on a well-designed RCT showing small improvements in A1c (eg, 0.2% A1c reduction) and some perinatal and neonatal outcomes (birth weight, length of stay, and hypoglycemia) with rtCGM+SMBG versus SMBG alone.60,61 This 2017 RCT, CONCEPTT, was performed in pregnant women with T1DM who were intensive-insulin therapy and who used rtCGM adjunctive to SMBG fingerstick testing at least 7 times a day (vs. SMBG alone).61 There have been other RCTs assessing supplementary CGM but used on an intermittent basis in pregnant women with T2DM or GDM; these did not result in improved glycemic or neonatal outcomes over SMBG alone.52,62-64 Intermittent use in one of these studies was CGM 2-3 days per week, and in the other, CGM was used for a period of 6 days every 4 to 9 weeks.63,64
• The 2021 ADA guideline slightly revised their recommendation wording regarding CGM use in pregnancy which, in 2020, was specifically recommended for pregnancy with T1DM: “Real-time continuous glucose monitors may be used effectively to improve A1c levels, time in range, and neonatal outcomes in pregnant women with type 1 diabetes. B”65 More recent wording in the 2021 guideline inferring the broader pregnancy population with diabetes (also including those with GDM or with pre-existing T2DM) is based on evidence of benefit with adjunctive rtCGM in pregnancy with pre-existing T1DM.13,60 Guideline authors also likely consider the potential
19
benefits of CGM for patients on insulin, especially intensive insulin therapy, in general; the ability of CGM to catch hyper and hypoglycemia events that go unrecognized with SMBG; and that diabetes-related complications during pregnancy are concerning regardless of the classification of diabetes in pregnancy (whether it is pre-existing T1DM or T2DM, or GDM).
Other guideline recommendations that occurred prior to the publication of the CONCEPTT RCT include those by the AACE and the Endocrine Society. The 2016 AACE/ACE consensus statement noted that the benefits of CGM during pregnancy were unclear but that CGM could be used to supplement SMBG for detection of nocturnal hypo or hyperglycemia and post-prandial hyperglycemia; and to serve as a “…teaching tool, to evaluate glucose patterns, and to fine-tune insulin dosing.”52 The 2013 Endocrine Society guideline for the treatment of pregnant women with diabetes gave a weak-rated recommendation, suggesting CGM for patients with “overt or gestational diabetes when self-monitored blood glucose levels (or, in the case of the woman with overt diabetes, HbA1C values) are not sufficient to assess glycemic control (including both hyperglycemia and hypoglycemia).”62 At the time there were some RCTs available using intermittent-use rtCGM in pregnant women with T1DM and T2DM; and other studies, mostly observational, assessing short-term use of professional CGM devices (retrospective CGM) in pregnant women (with GDM, T1DM, or T2DM), where unrecognized hyper and hypoglycemia events were identified with CMG.62,66 The panel acknowledged the “…paucity of literature on continuous glucose monitoring use during pregnancy…,” but highlighted that CGM could be useful, nonetheless, to alert the patient/prescriber of hypo and hyperglycemia episodes that go unrecognized with SMBG.62
T2DM with or without intensive insulin therapy
T2DM managed with intensive insulin therapy
The DIAMOND RCT was a key study demonstrating glycemic benefit, greater A1c reduction with rtCGM vs. SMBG, in patients with uncontrolled T2DM who were on MDI therapy. This study has been used to support recommendations in the ADA and international consensus guidelines for the use of CGM in patients with T2DM who are on insulin treatment.10,13 The DIAMOND RCT was rated as B level evidence by the 2017 international consensus of experts (of the Advanced Technologies & Treatments for Diabetes [ATTD] Congress).10 There are also RCTs supporting the use of isCGM in patients with uncontrolled T2DM on intensive insulin therapy. While the change in A1c from baseline was similar between the isCGM- and SMBG-treated groups in the 2017 RCT, there was a significantly greater A1c reduction with isCGM for the strata of patients <65 years of age.57 isCGM use was associated with a greater reduction in the time spent in hypoglycemia, including time in nocturnal hypoglycemia and the number of hypoglycemic events, along with reduced glycemic variability versus SMBG for the total study population (rated as B level evidence by the ATTD).10,57 A 2019 RCT in T2DM, managed with MDI, found a significantly greater reduction in A1c with isCGM versus usual care.58
Adults with T2DM not yet receiving prandial insulin (ie, on non-intensive insulin regimen or oral-only therapy)
One RCT (N=100), rated as lower strength evidence (level C, by the ATTD consensus),10 showed a significant reduction in A1c after 3 months with intermittent-use rtCGM (2 weeks on, 1 week off) versus
20
SMBG in adults with baseline A1c≥ 7% (who were not yet on MDI at baseline; about two thirds were with non-insulin therapy and a third with basal insulin at baseline).67 Significantly fewer patients in the CGM group required transition to insulin. The A1c reduction magnitude (~1%) with intermittent-use rtCGM was similar to what would be expected with the addition of second antihyperglycemic medication.67 Another small RCT (N=65) assessing efficacy of intermittent rtCGM (ie, only 3 days of CGM per month, for 3 months) suggested a reduction in A1c could be achieved in patients with uncontrolled T2DM who were not on insulin (about half of the included population); yet, outcomes were not assessed separately from those on insulin therapy.55
Overall, there is limited, lower strength evidence from small, heterogeneous study populations10,13 for CGM use in T2DM treated with regimens other than intensive insulin therapy, and guidelines differ regarding this subpopulation. The 2017 international consensus does not make a recommendation for CGM use in T2DM without intensive insulin therapy;10 yet, the 2021 ADA guideline recommends consideration of rtCGM or isCGM in patients on non-intensive insulin (although supported by lower strength evidence).13 Additionally, the 2020 AACE/ACEE guideline supports CGM in T2DM with history of hypoglycemia unawareness or with recurrent hypoglycemia.3 Other suggested options in guidelines for patients with T2DM on noninsulin (ie, oral only therapy) or basal insulin regimens (ie, non-intensive insulin) include either intermittent-use or professional-use CGM.13,37
Pediatrics
Reductions in A1c and hypoglycemia have been demonstrated in several RCTs including children with T1DM when pediatric data were analyzed with adult data; but, A1c reduction has been inconsistent when analyzing pediatric data alone.13 Benefits of CGM with respect to A1c or time in range were associated with near daily use (ie, 6 or more days per week).13,68,69 Moreover, observational evidence from registry data has found an association with rtCGM and lower A1c.13
The ADA recommends consideration of CGM (or SMBG) for all children and adolescents with T1DM to help improve glycemic control and as needed to ensure safety during situations such as exercise, driving, or for managing hypoglycemia symptoms (based on level B evidence).70,71 Authors state that CGM is a potential strategy for youth with T2DM who require frequent blood glucose monitoring.70
The following devices are approved for use in children: • Dexcom G6, approved for ≥2 years of age • Guardian Connect, approved for 14 years of age and older
- This device requires a compatible smartphone for use, which can present a financial barrier particularly for adolescents
- Requires fingerstick calibration twice daily and not approved for basing treatment decisions • FreeStyle Libre 2, approved for 4 years and older
- Patients should remember to scan the sensor at least once every 8 hours with the receiver
21
Recommendations Regarding How to Use CGM
In order to achieve maximal benefits, optimal CGM implementation includes the following, as highlighted in clinical guidelines:
• In patients on rtCGM who receive MDI or CSII, devices should be used on a daily basis as much as possible; isCGM devices should be scanned at least once every 8 hours (per ADA).13 Data in children (analyzed independent of adult data), showed glycemic benefits with CGM over SMBG mainly when used on a near daily basis (≥ 6 days/week).13 The Endocrine Society also recommended CGM for indicated patients if the patient is willing and able to use the device close to daily.37
• As part of CGM initiation and ongoing use, patients should have robust diabetes education, training, clinical and technical support, along with follow-up in order to ensure (a) proper use of devices, (b) that patients understand how to interpret and respond to their CGM-related readings/summary data/alarms, and (c) to improve adherence of CGM device use.10,13
• CGM users should have ability to perform SMBG13 since (a) some device sensors may require manual calibration with fingerstick testing, and (b) glucose readings may need to be verified via SMBG, especially if symptoms or expectations do not seem to match the reading (applies to all CGM devices).
• Continuation of care with respect to CGM device access is recommended in the ADA guideline, as discontinuation of CGM, related to gaps in insurance coverage, has been associated with worsening of outcomes (eg, increased A1c in youth with T1DM).13,72
CGM Glycemic Parameters
While hemoglobin A1c is a standard monitoring parameter for diabetes management, blood glucose monitoring is also a key assessment for understanding how to optimize medication regimens and lifestyle factors, and for indicating when to quickly respond to problematic glucose levels.1,13 A1c reflects the average blood glucose over approximately the preceding 3 months.73 However, A1c does not inform patients about the precise time points during the day when a high or low glycemic event occurs, nor does it provide details regarding glycemic variability or how glucose changes are related to various daily factors (eg, food intake, exercise, etc). Glycemic control is best evaluated using a combination A1c and glucose measurements (via SMBG or CGM) in patients prone to glycemic variability such as those with severe insulin deficiency.1 Patients with intensive insulin regimens (ie, MDI or CSII), are encouraged to assess glucose levels prior to eating, exercising, and prior to performing critical tasks such as driving; at bedtime; occasionally post-prandially; when low blood glucose is expected or suspected; and after treating low levels.13 This can amount to 6 to 10+ fingersticks per day with SMBG.1 CGM has potential to reduce the burden of SMBG in patients with high frequency SMBG use. Moreover, CGM can better indicate how to respond to a problematic level since it provides the glucose trend (ie, direction of change; whether glucose is rising for falling) and the rate of change, rather than a single time-point level with SMBG which on its own does not indicate the direction of change.
Glycemic targets and A1c are tailored to individual patient considerations such as patient age, duration and progression of disease, co-morbidities, motivation, self-management ability, preferences, risk for hypoglycemia, and hypoglycemia awareness.1 Table 2 of Appendix C lists the A1c and glycemic targets
22
described in US treatment guidelines. CGM summary parameters such as time in ranges and ambulatory glucose profile information can also be used to assess glycemic control.1,2,10 However, assessment of cumulative CGM data should be accompanied with at least 70% of CGM wear time (ie, 70% of all possible readings captured) over the previous 14 days; otherwise, the generated CGM summary metrics can be inaccurate.2,10 Key CGM summary metrics include the following:
o Ambulatory glucose profile (AGP) typically includes a visual graph that collapses the glucose levels measured (for example over the previous 14 days) into a 24-hour period, with the median and various percentiles shown with respect to the target range and hyper- and hypoglycemia thresholds. The AGP report also incorporates other core CGM metrics and bar charts to reflect time in range information, mean glucose, glycemic variability and the glucose management indicator. The ADA recommends providing a standardized, single-page report that contains visual cues such as the AGP, to convey CGM metrics to the patient.1,2
o Time in range (TIR); time above range; and time below range: these metrics are expressed as % of glucose readings or hours per day in the target glycemic range or above/below the threshold. The ADA supports using TIR as an assessment for glycemic control and as an end point for
clinical trials (C level recommendation).1 Time in range captures fluctuations in glucose levels whereas A1c does not fully account for glycemic variability (ie, TIR is more specific and sensitive for fluctuations).1 The ADA also supports using the time below range (TBR) and time above range (TAR) for treatment evaluation of patients managed with CGM (C level recommendation).1
There is a strong correlation between TIR and A1c.1,2 A TIR goal of 70% in the range of 70-180 mg/dL corresponds to an A1c of ∼7% based on prospective studies.1 An increase of TIR by 10% corresponded to a decrease in A1c by about 0.5-0.8%.2
Reduced TIR correlates with diabetes-related, microvascular complications such as retinopathy.74 A small RCT over 1 year showed that increased TIR while using CGM was associated with decreased albuminuria in patients with type 1 diabetes; A1c was also significantly improved from baseline.75
o Mean glucose, glucose management indicator (GMI), and glycemic variability metrics can be used to discuss glucose trends with the patient.1 The GMI is a rough estimate of the patient’s A1c, derived from the patient’s mean glucose using CGM.76 Glycemic variability is characterized by the amplitude, frequency, and duration of fluctuations. Glycemic variability has been found to be an independent risk factor for diabetic-related cardiovascular disease, and is attributed to negative effects on cognitive function and quality of life.10
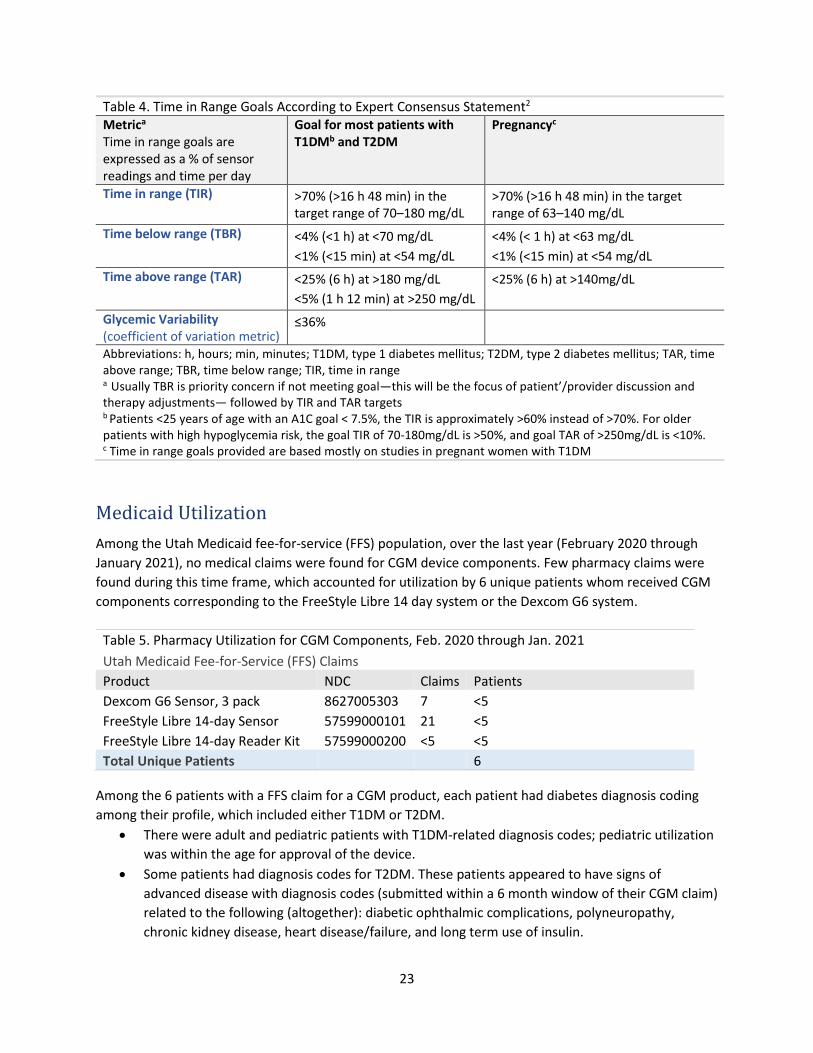
Table 4 summarizes treatment goals related to CGM metrics as recommended in the 2019 international expert-consensus statement and supported by the ADA guideline.1,2,13
23
Table 4. Time in Range Goals According to Expert Consensus Statement2 Metrica
Time in range goals are expressed as a % of sensor readings and time per day
Goal for most patients with T1DMb and T2DM
Pregnancyc
Time in range (TIR)
>70% (>16 h 48 min) in the target range of 70–180 mg/dL
>70% (>16 h 48 min) in the target range of 63–140 mg/dL
Time below range (TBR) <4% (<1 h) at <70 mg/dL <1% (<15 min) at <54 mg/dL
<4% (< 1 h) at <63 mg/dL <1% (<15 min) at <54 mg/dL
Time above range (TAR) <25% (6 h) at >180 mg/dL <5% (1 h 12 min) at >250 mg/dL
<25% (6 h) at >140mg/dL
Glycemic Variability (coefficient of variation metric)
≤36%
Abbreviations: h, hours; min, minutes; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; TAR, time above range; TBR, time below range; TIR, time in range
a Usually TBR is priority concern if not meeting goal—this will be the focus of patient’/provider discussion and therapy adjustments— followed by TIR and TAR targets b Patients <25 years of age with an A1C goal < 7.5%, the TIR is approximately >60% instead of >70%. For older patients with high hypoglycemia risk, the goal TIR of 70-180mg/dL is >50%, and goal TAR of >250mg/dL is <10%. c Time in range goals provided are based mostly on studies in pregnant women with T1DM
Medicaid Utilization Among the Utah Medicaid fee-for-service (FFS) population, over the last year (February 2020 through January 2021), no medical claims were found for CGM device components. Few pharmacy claims were found during this time frame, which accounted for utilization by 6 unique patients whom received CGM components corresponding to the FreeStyle Libre 14 day system or the Dexcom G6 system.
Among the 6 patients with a FFS claim for a CGM product, each patient had diabetes diagnosis coding among their profile, which included either T1DM or T2DM.
• There were adult and pediatric patients with T1DM-related diagnosis codes; pediatric utilization was within the age for approval of the device.
• Some patients had diagnosis codes for T2DM. These patients appeared to have signs of advanced disease with diagnosis codes (submitted within a 6 month window of their CGM claim) related to the following (altogether): diabetic ophthalmic complications, polyneuropathy, chronic kidney disease, heart disease/failure, and long term use of insulin.
24
Prior Authorization Considerations
• Consider requiring a diabetes-related diagnosis as these devices are approved for the management of diabetes
o May consider reserving CGM to patients with diabetes (ie, any diabetes-related diagnosis) receiving intensive-insulin therapy; and potentially for patients on other insulin regimens if meeting additional clinical characteristics (eg, hypoglycemia issues or suboptimal glycemic control) as described below
• Consider product-specific criteria based on the device’s age for approval
o Dexcom G6 is approved for ages ≥2 years o Eversense is approved for ages ≥18 years o Freestyle Libre 14 day is approved for ages ≥18 years o Freestyle Libre 2 is approved for ages ≥4 years o Guardian Connect is approved for ages 14-75 years
• Patients must be capable and committed to using SMBG (fingerstick testing) when indicated
according to the instructions for their device to ensure proper functioning and safety.13 o CGM devices do not completely eliminate the need to perform SMBG fingerstick testing
(required occasionally with some devices, or at least twice daily for devices requiring calibration; refer to page 11). Patients should have an SMBG meter/materials on hand.
Regarding adults and children managed with insulin
• Consider personal CGM devices as a tool for lowering and/or maintaining A1c or reducing hypoglycemia, for all patients with diabetes receiving intensive insulin therapy (ie, multiple daily insulin injections or continuous subcutaneous insulin infusions).
o CGM devices may reduce SMBG burden in these patients while helping patients meet or maintain A1c, and/or reduce the incidence of hypoglycemia. An intensive insulin regimen would otherwise require 6+ fingerstick tests per day for monitoring blood glucose. There are supportive studies in both T1DM and T2DM, managed with intensive insulin regimens, showing improved glycemic control using personal-use CGM compared to usual care with SMBG. Recent guidelines by the ADA (2021) recommend CGM for all patients, adults and youth, with diabetes on intensive insulin therapy, supported by level A and B evidence, with respect to rtCGM and isCGM. The 2017 International Consensus statement is largely congruent with this, recommending CGM for all patients with T1DM (as these patients generally require intensive-insulin therapy); but, the consensus statement also has an extra parameter regarding use in T2DM, as CGM is recommended for those with T2DM on intensive-insulin therapy who are not achieving glycemic goals, especially if hypoglycemia is an issue.3,10,13
• Patients who may be on CSII may request a certain device based on the compatibility with their insulin pump.
o Dexcom G6 CGM interfaces with Tandem t:slim X2 insulin pump
25
o Medtronic MiniMed insulin pumps interface with Medtronic CGM devices (eg, Guardian Sensor 3, Link 3 transmitter, or Enlite sensor)
• Consider personal CGM devices for patients with diabetes who are on non-intensive insulin regimens particularly if they are not meeting their glycemic targets and/or having hypoglycemia episodes, or hypoglycemia unawareness.
o The ADA guideline recommends use of CGM for patients on non-intensive insulin regimens but the strength of supportive evidence is low (level C). Thus, additional potential criteria may be considered: for example, demonstration of inadequate glycemic control despite prescribing of frequent SMBG (eg, at least 3 or 4 fingersticks per day over the last couple months), OR documentation of hypoglycemia unawareness, recurrent hypoglycemic episodes, or severe hypoglycemia.
o Consider requiring prescriber attestation that these patients are able and willing to carry out fingerstick monitoring as appropriate during use of their CGM device.
Regarding pregnant women with diabetes
• May consider CGM adjunctive to SMBG in pregnant women with diabetes, especially those who are on intensive insulin therapy, as a tool to achieve glycemic targets and to mitigate hypoglycemia
o May have the provider attest that the patient will continue to use regular pre- and postprandial SMBG as recommended by guidelines, and will verify problematic CGM readings with SMBG since CGM is not intended to replace SMBG in pregnancy for therapy decision-making. The 2021 ADA guideline highlights the utility of CGM in this population when used
adjunctive to pre and postprandial SMBG.13,61 The AACE/ACE also notes that CGM can be a useful supplement to SMBG for detection of nocturnal hypo or hyperglycemia and post-prandial hyperglycemia; and to help assess glucose patterns and optimize insulin dosing.52
The accuracy of these devices is undetermined during pregnancy per warnings in device user manuals, some which specifically recommend against use in this population. Thus, if CGM is used during pregnancy, it should be used adjunctive to SMBG.
Regarding patients with diabetes managed with non-insulin therapy
• Strong recommendations (or recommendations supported by high level evidence) are lacking in clinical guidelines for ongoing personal-use CGM in patients with diabetes who do not receive insulin
o For patients not receiving insulin, the 2021 ADA guideline recommends, based on low level evidence, employing intermittent CGM (ie, either by a professional-use device or intermittent use of a personal device) to address problematic hyper or hypoglycemia patterns or A1c.
o The AACE/ACE 2016 guidance on glucose monitoring (carried over to the 2020 guideline), recommends SMBG for patients with T2DM who are on oral regimens with hypoglycemia risk (sulfonylureas and glinides). SMBG should be performed at least once daily for a fasting level and periodically at other times to assess therapy response and to
26
detect possible hypoglycemia.52 If hypoglycemia issues are occurring despite proper use of medication (ie, timing of meal with respect to medication intake) or trial of lower dosage, alternative oral therapies or combinations that are minimally associated with hypoglycemia should be considered (e.g., metformin, dipeptidyl peptidase-4 [DPP-4] inhibitors, sodium-glucose cotransporter-2 [SGLT-2] inhibitors, thiazolidinediones [TZDs], or glucagon-like peptide-1 [GLP-1] receptor agonists). The guideline does not go as far to recommend CGM for patients on non-insulin regimens but instead points out that studies are limited and ongoing.52
Regarding devices requiring calibration via fingerstick testing (Guardian Connect and Eversense)
• Consider requiring the provider’s attestation that the patient has been compliant with using SMBG at least 3 times per day for the prior couple months in order to demonstrate their commitment to carry out ongoing fingerstick testing at least twice daily for device calibration and for additional scenarios that call for a fingerstick test (eg, prior to making any treatment decision with Guardian Connect; whenever indicated by the device; if a trend arrow and glucose level are not displayed; or when symptoms do not match the glucose reading).
o These 2 devices should not be used in patients unwilling or unable to carry out at least 2 blood glucose fingerstick tests per day for minimum calibration requirements. Otherwise, readings/alerts may not display and/or may be inaccurate. Additionally, the Guardian Connect is not intended to replace SMBG; rather, it is to be used to indicate when the patient should perform a fingerstick test.
• Since the implantable device (Eversense) can incur additional costs related to the implantation and removal procedures and possibly for managing surgical-insertion related infections (though low risk77-79), it is reasonable to consider reserving this product for patients who have failed other CGM options (eg, may require trial of at least 2 other rtCGM devices, demonstration of insufficient glycemic control, contraindication, and/or intolerance).
Counseling and/or additional points for provider outreach
• Consider having the prescriber attest that they will ensure the patient is aware of which agents, including over-the-counter medications, can interfere with their specific device (as listed in the user manual), and what steps to take (eg, SMBG) in the event the patient has a temporary dose of such medication. Directions-for-use education may be provided by the prescriber or their support staff such as a certified diabetes educator.
• Consider having the prescriber attest that they have adequately trained the patient on the device and the patient is aware of the online materials that describe how to use their device (eg, user guide, instructional videos, or product website).
• Patients should be committed to using their personal-CGM device on a near daily basis for maximal benefits and for reliability/interpretation of CGM summary metrics (eg, time in ranges, ambulatory glucose profile).13,37 o The ADA recommends that patients who are on intensive insulin therapy and prescribed
rtCGM should use their device on a daily basis as much as possible; isCGM devices should be
27
scanned at least once every 8 hours.13 The Endocrine Society also recommended CGM under the condition that the patient is willing and able to use the device close to daily.37
o Improved glycemic control with CGM vs. SMBG was demonstrated in RCTs where CGM was used on a near daily basis (eg, wear time of at least 85%), particularly in pediatric patients (when used ≥ 6 days/week).13,34,38-40 Patient-specific CGM summary metrics such as time in range and the ambulatory profile graph are reliable if at least 70% of possible readings are captured over the previous 14 days.10
• Some CGM systems are not available with a manufacturer supplied receiver and instead require the patient to have a compatible smart device. If a patient is considered for one of these CGM devices (Guardian Connect or Eversense), it would be prudent for the provider to review the most recent compatibility list for the CGM device and ensure the patient has a smart-device meeting the software requirements to interface with the CGM system.
• Other implanted devices: Although perhaps a rare scenario, consider asking whether the patient being considered for CGM has another type of implanted medical device (eg, pacemaker). For patients that do, consider having both device prescribers attest they are each in consultation with one another and agree to the compatibility (and have plans for monitoring) based on their professional judgement.
o This criteria idea is aimed at ensuring that the CGM provider has assessed whether the patient is on another implanted device
o There is limited information in user guides or FDA materials regarding the compatibility of CGM devices with other implanted medical devices. The FreeStyle Libre 2 user guide notes that it is not intended to be used with other implanted devices such as pacemakers since its performance has not been evaluated under such condition.
28
Summary
CGM devices are approved for the management of diabetes mellitus. Most personal-use devices (except Guardian Connect) are approved for using the sensor-measured glucose readings to base treatment decisions. Improved clarity in glucose trends and more refined decisions regarding insulin dosing are made possible with CGM data. CGM technology also affords greater transparency in patient-specific factors that affect blood glucose fluctuations and can reveal unrecognized hypoglycemic/hyperglycemic events.10 Not only are patients alerted to problematic levels in real-time, most devices can additionally predict occurrences of hypoglycemia or hyperglycemia if the patient does not otherwise intervene—patients can proactively address their glycemic needs and prevent such highs/lows altogether. Intensive insulin therapy (eg, multiple daily injections or CSII) requires frequent monitoring of blood glucose (eg, 4+ fingersticks per day). CGM devices may reduce the burden of fingerstick testing for some patients on intensive- insulin therapy. Nonetheless, all patients using CGM will still require an SMBG device to verify CGM readings discordant from symptoms, during the sensor warm-up/initialization, to calibrate some devices, etc (see page 11).
Some key features that differentiate products include non-adjunctive or adjunctive SMBG indication, age for approval, requirement for fingerstick calibrations, real-time alarms for highs/lows or predictive events, insulin pump compatibility, implanted vs. traditional transcutaneous placement, and receiver options (eg, whether a smart-device is required). See Table 1 of page 8 of the report for device features. Potential adverse events associated with CGM may include skin reactions, particularly related to the adhesive to secure the device, scars, local infections, and preterm sensor failure or displacement. There is also risk for potential hypoglycemia or hyperglycemia when glucose data provided by the sensor is not accurate and used to make treatment decisions, or when technical issues result in alarm/alert deactivation. Devices accuracy is subject to a few interfering substances that patients should be aware of to ensure safe use (see table 3 on page 14).
Prior authorization criteria considerations have been developed based on the approved indications, requirement for SMBG, guideline recommendations regarding subpopulations recommended for CGM use, and guideline information regarding subpopulations where there is more limited evidence for the use of CGM (eg, patients not using insulin and pregnant women).
29
References 1. American Diabetes Association. 6. Glycemic targets: Standards of Medical Care in Diabetes—
2021. Diabetes Care 2021;44(Suppl. 1):S73–S84. 2. Battelino T, Danne T, Bergenstal RM, et al. Clinical Targets for Continuous Glucose Monitoring
Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care. 2019;42(8):1593-1603.
3. Garber AJ, Handelsman Y, Grunberger G, et al. CONSENSUS STATEMENT BY THE AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AND AMERICAN COLLEGE OF ENDOCRINOLOGY ON THE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM - 2020 EXECUTIVE SUMMARY. Endocr Pract. 2020;26(1):107-139.
4. Longo R, Sperling S. Personal Versus Professional Continuous Glucose Monitoring: When to Use Which on Whom. Diabetes Spectr. 2019;32(3):183-193.
5. Dexcom G6 Continuous Monitoring System: USER GUIDE. San Diego, CA: Dexcom, Inc. Revision Date 3/2020.
6. FreeStyle Libre 2 Flash Glucose Monitoring System: USER MANUAL. Alameda, CA: Abbott (ART40703-001 Rev. D 06/20).
7. FreeStyle Libre 14 day Flash Glucose Monitoring System: Quick Reference Guide. Alameda, CA: Abbott Diabetes Care Inc. (ART39880-001 Rev. A 07/18).
8. Eversense User Guide: A guide for using the Eversense Continuous Glucose Monitoring Stystem. Germantown, MD: Sensonics Inc. (Version LBL-1632-01-001; March 2020).
9. Guardian Connect System User Guide 2020. Minneapolis, MN: Medtronic. https://www.medtronicdiabetes.com/products/guardian-connect-continuous-glucose-monitoring-system. Accessed January 8, 2021.
10. Danne T, Nimri R, Battelino T, et al. International Consensus on Use of Continuous Glucose Monitoring. Diabetes Care. 2017;40(12):1631.
11. U.S. Food and Drug Administration. 510(k) Premarket Notification. Dexcom G6 Continuous Glucose Monitoring System, Dexcom G6 Glucose Program Continuous Glucose Monitoring System; 510(k) SUBSTANTIAL EQUIVALENCE DETERMINATION DECISION SUMMARY: K200876 (Dexcom, Inc). Decision Date 12/04/2020. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm. Accessed January 8, 2021.
12. US Food and Drug Administration. 510(k) SUBSTANTIAL EQUIVALENCE DETERMINATION DECISION SUMMARY (510(k) Number K193371). https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K193371. Accessed.
13. American Diabetes Association. 7. Diabetes technology: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021;44(Suppl. 1):S85–S99.
14. Cappon G, Vettoretti M, Sparacino G, Facchinetti A. Continuous Glucose Monitoring Sensors for Diabetes Management: A Review of Technologies and Applications. Diabetes Metab J. 2019;43(4):383-397.
17. Dexcom Continuous Glucose Monitoring: All Products FAQs>Dexcom G6 CGM Systems>Using Your Dexcom CGM System. Last Updated June 18th 2020. https://www.dexcom.com/faqs/main-differences-between-dexcom-g5-mobile-and-dexcom-g6?sc=&c=g6. Accessed January 8, 2021.
18. FreeStyle: Products>Compare products (healthcare professional website). Abbott Laboratories. https://provider.myfreestyle.com/compare-products.html. Accessed January 12, 2021.
19. Reddy M, Jugnee N, El Laboudi A, Spanudakis E, Anantharaja S, Oliver N. A randomized controlled pilot study of continuous glucose monitoring and flash glucose monitoring in people with Type 1 diabetes and impaired awareness of hypoglycaemia. Diabetic Medicine. 2018;35(4):483-490.
20. Avari P, Moscardo V, Jugnee N, Oliver N, Reddy M. Glycemic Variability and Hypoglycemic Excursions With Continuous Glucose Monitoring Compared to Intermittently Scanned Continuous Glucose Monitoring in Adults With Highest Risk Type 1 Diabetes. Journal of Diabetes Science and Technology. 2019;14(3):567-574.
21. Hásková A, Radovnická L, Petruželková L, et al. Real-time cgm is superior to flash glucose monitoring for glucose control in type 1 diabetes: The corrida randomized controlled trial. Diabetes Care. 2020;43(11):2744-2750.
23. Diabetes Home. Type 2 Diabetes. Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. https://www.cdc.gov/diabetes/basics/type2.html. Published 2018. Updated August 15, 2018. Accessed January 31, 2019.
25. Deiss D, Szadkowska A, Gordon D, et al. Clinical Practice Recommendations on the Routine Use of Eversense, the First Long-Term Implantable Continuous Glucose Monitoring System. Diabetes technology & therapeutics. 2019;21(5):254-264.
26. Messer LH, Berget C, Beatson C, Polsky S, Forlenza GP. Preserving Skin Integrity with Chronic Device Use in Diabetes. Diabetes technology & therapeutics. 2018;20(S2):S254-S264.
27. Crotti, Nancy. 3M debuts new silicone adhesive for longer, stronger wear. December 14. Medical Design & Outsourcing. . https://www.medicaldesignandoutsourcing.com/3m-debuts-new-silicone-adhesive-for-longer-stronger-wear/. Accessed Febuary 8, 2021.
28. Heinemann L, Kamann S. Adhesives Used for Diabetes Medical Devices: A Neglected Risk With Serious Consequences? Journal of diabetes science and technology. 2016;10(6):1211-1215.
29. Tsai, Allison. Tips for Tackling Adhesive Irritation and Allergies. March 2017. Diabetes Forcast. http://www.diabetesforecast.org/2017/mar-apr/the-sticking-point.html. Accessed Febuary 8, 2021.
30. Hyry HSI, Liippo JP, Virtanen HM. Allergic contact dermatitis caused by glucose sensors in type 1 diabetes patients. Contact Dermatitis. 2019;81(3):161-166.
31. Smith & Nephew Opsite IV3000 Standard Moisture Responsive Catheter Dressing. HPFY Health Products For You. . https://www.healthproductsforyou.com/p-smith-nephew-opsite-iv3000-standard-moisture-responsive-catheter-dressing.html. Accessed February 22, 2021.
34. Wong JC, Foster NC, Maahs DM, et al. Real-time continuous glucose monitoring among participants in the T1D Exchange clinic registry. Diabetes Care. 2014;37(10):2702-2709.
35. American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021;44(Suppl. 1):S15−S33.
36. American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021;44(Suppl. 1):S111–S124.
37. Peters AL, Ahmann AJ, Battelino T, et al. Diabetes technology-continuous subcutaneous insulin infusion therapy and continuous glucose monitoring in adults: An endocrine society clinical practice guideline. Journal of Clinical Endocrinology and Metabolism. 2016;101(11):3922-3937.
38. Beck RW, Riddlesworth TD, Ruedy K, et al. Continuous Glucose Monitoring Versus Usual Care in Patients With Type 2 Diabetes Receiving Multiple Daily Insulin Injections: A Randomized Trial. Ann Intern Med. 2017;167(6):365-374.
39. Beck RW, Riddlesworth T, Ruedy K, et al. Effect of Continuous Glucose Monitoring on Glycemic Control in Adults With Type 1 Diabetes Using Insulin Injections: The DIAMOND Randomized Clinical Trial. JAMA. 2017;317(4):371-378.
40. Riddlesworth T, Price D, Cohen N, Beck RW. Hypoglycemic Event Frequency and the Effect of Continuous Glucose Monitoring in Adults with Type 1 Diabetes Using Multiple Daily Insulin Injections. Diabetes therapy. 2017;8(4):947-951.
41. Mattishent K, Loke YK. Detection of asymptomatic drug-induced hypoglycemia using continuous glucose monitoring in older people - Systematic review. Journal of diabetes and its complications. 2018;32(8):805-812.
42. Al Hayek AA, Robert AA, Al Dawish MA. Evaluation of FreeStyle Libre Flash Glucose Monitoring System on Glycemic Control, Health-Related Quality of Life, and Fear of Hypoglycemia in Patients with Type 1 Diabetes. Clin Med Insights Endocrinol Diabetes. 2017;10:1179551417746957-1179551417746957.
43. Ehrhardt N, Al Zaghal E. Continuous Glucose Monitoring As a Behavior Modification Tool. Clinical Diabetes. 2020:cd190037.
44. Isaacson B, Kaufusi S, Sorensen J, et al. Demonstrating the Clinical Impact of Continuous Glucose Monitoring Within an Integrated Healthcare Delivery System. Journal of diabetes science and technology. 2020:1932296820955228.
45. Mulinacci G, Alonso GT, Snell-Bergeon JK, Shah VN. Glycemic Outcomes with Early Initiation of Continuous Glucose Monitoring System in Recently Diagnosed Patients with Type 1 Diabetes. Diabetes technology & therapeutics. 2019;21(1):6-10.
46. Charleer S, Mathieu C, Nobels F, et al. Effect of Continuous Glucose Monitoring on Glycemic Control, Acute Admissions, and Quality of Life: A Real-World Study. The Journal of clinical endocrinology and metabolism. 2018;103(3):1224-1232.
47. Parkin CG, Graham C, Smolskis J. Continuous Glucose Monitoring Use in Type 1 Diabetes: Longitudinal Analysis Demonstrates Meaningful Improvements in HbA1c and Reductions in Health Care Utilization. Journal of diabetes science and technology. 2017;11(3):522-528.
48. Gill M, Zhu C, Shah M, Chhabra H. Health Care Costs, Hospital Admissions, and Glycemic Control Using a Standalone, Real-Time, Continuous Glucose Monitoring System in Commercially Insured Patients With Type 1 Diabetes. Journal of diabetes science and technology. 2018;12(4):800-807.
49. Tsur A, Cahn A, Israel M, Feldhamer I, Hammerman A, Pollack R. Impact of flash glucose monitoring on glucose control and hospitalization in type 1 diabetes: A nationwide cohort study. Diabetes/metabolism research and reviews. 2021;37(1):e3355.
50. Stimson RH, Dover AR, Ritchie SA, et al. HbA1c response and hospital admissions following commencement of flash glucose monitoring in adults with type 1 diabetes. BMJ open diabetes research & care. 2020;8(1).
51. Shivers JP, Mackowiak L, Anhalt H, Zisser H. "Turn it off!": diabetes device alarm fatigue considerations for the present and the future. Journal of diabetes science and technology. 2013;7(3):789-794.
52. Bailey TS, Grunberger G, Bode BW, et al. AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AND AMERICAN COLLEGE OF ENDOCRINOLOGY 2016 OUTPATIENT GLUCOSE MONITORING CONSENSUS STATEMENT. Endocr Pract. 2016;22(2):231-261.
53. Dicembrini I, Cosentino C, Monami M, Mannucci E, Pala L. Effects of real-time continuous glucose monitoring in type 1 diabetes: a meta-analysis of randomized controlled trials. Acta Diabetol. 2020.
54. Bolinder J, Antuna R, Geelhoed-Duijvestijn P, Kröger J, Weitgasser R. Novel glucose-sensing technology and hypoglycaemia in type 1 diabetes: a multicentre, non-masked, randomised controlled trial. The Lancet. 2016;388(10057):2254-2263.
55. Yoo HJ, An HG, Park SY, et al. Use of a real time continuous glucose monitoring system as a motivational device for poorly controlled type 2 diabetes. Diabetes Research and Clinical Practice. 2008;82(1):73-79.
56. Ehrhardt NM, Chellappa M, Walker MS, Fonda SJ, Vigersky RA. The Effect of Real-Time Continuous Glucose Monitoring on Glycemic Control in Patients with Type 2 Diabetes Mellitus. Journal of diabetes science and technology. 2011;5(3):668-675.
57. Haak T, Hanaire H, Ajjan R, Hermanns N, Riveline JP, Rayman G. Flash Glucose-Sensing Technology as a Replacement for Blood Glucose Monitoring for the Management of Insulin-Treated Type 2 Diabetes: a Multicenter, Open-Label Randomized Controlled Trial. Diabetes Ther. 2017;8(1):55-73.
58. Yaron M, Roitman E, Aharon-Hananel G, et al. Effect of Flash Glucose Monitoring Technology on Glycemic Control and Treatment Satisfaction in Patients With Type 2 Diabetes. Diabetes Care. 2019;42(7):1178-1184.
59. 14. Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S183-s192.
60. American Diabetes Association. 14. Management of diabetes in pregnancy: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021;44(Suppl. 1):S200–S210.
61. Feig DS, Donovan LE, Corcoy R, et al. Continuous glucose monitoring in pregnant women with type 1 diabetes (CONCEPTT): a multicentre international randomised controlled trial. Lancet. 2017;390(10110):2347-2359.
62. Blumer I, Hadar E, Hadden DR, et al. Diabetes and Pregnancy: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2013;98(11):4227-4249.
63. Secher AL, Ringholm L, Andersen HU, Damm P, Mathiesen ER. The effect of real-time continuous glucose monitoring in pregnant women with diabetes: a randomized controlled trial. Diabetes Care. 2013;36(7):1877-1883.
64. Wei Q, Sun Z, Yang Y, Yu H, Ding H, Wang S. Effect of a CGMS and SMBG on Maternal and Neonatal Outcomes in Gestational Diabetes Mellitus: a Randomized Controlled Trial. Sci Rep. 2016;6(1):19920-19920.
65. American Diabetes Association. 7. Diabetes Technology: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020;43(Suppl. 1):S77–S88.
33
66. Voormolen DN, Devries JH, Evers IM, Mol BWJ, Franx A. The efficacy and effectiveness of continuous glucose monitoring during pregnancy: A systematic review. Obstetrical and Gynecological Survey. 2013;68(11):753-763.
67. Vigersky RA, Fonda SJ, Chellappa M, Susan Walker M, Ehrhardt NM. Short- and Long-Term Effects of Real-Time Continuous Glucose Monitoring in Patients With Type 2 Diabetes. Diabetes Care. 2012;35(1):32-38.
68. Campbell FM, Murphy NP, Stewart C, Biester T, Kordonouri O. Outcomes of using flash glucose monitoring technology by children and young people with type 1 diabetes in a single arm study. Pediatr Diabetes. 2018;19(7):1294-1301.
69. Beck RW, Buckingham B, Miller K, et al. Factors predictive of use and of benefit from continuous glucose monitoring in type 1 diabetes. Diabetes Care. 2009;32(11):1947-1953.
70. American Diabetes Association. 13. Children and adolescents: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021;44(Suppl. 1):S180–S199.
71. Chiang JL, Maahs DM, Garvey KC, et al. Type 1 Diabetes in Children and Adolescents: A Position Statement by the American Diabetes Association. Diabetes Care. 2018;41(9):2026.
72. Addala A, Maahs DM, Scheinker D, Chertow S, Leverenz B, Prahalad P. Uninterrupted continuous glucose monitoring access is associated with a decrease in HbA1c in youth with type 1 diabetes and public insurance. Pediatric Diabetes. 2020;21(7):1301-1309.
73. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S98-s110.
74. Lu J, Ma X, Zhou J, et al. Association of Time in Range, as Assessed by Continuous Glucose Monitoring, With Diabetic Retinopathy in Type 2 Diabetes. Diabetes Care. 2018;41(11):2370-2376.
75. Ranjan AG, Rosenlund SV, Hansen TW, Rossing P, Andersen S, Nørgaard K. Improved time in range over 1 year is associated with reduced albuminuria in individuals with sensor-augmented insulin pump– treated type 1 diabetes. Diabetes Care. 2020;43(11):2882-2885.
76. Bergenstal RM, Beck RW, Close KL, et al. Glucose Management Indicator (GMI): A New Term for Estimating A1C From Continuous Glucose Monitoring. Diabetes Care. 2018;41(11):2275-2280.
77. Kropff J, Choudhary P, Neupane S, et al. Accuracy and Longevity of an Implantable Continuous Glucose Sensor in the PRECISE Study: A 180-Day, Prospective, Multicenter, Pivotal Trial. Diabetes Care. 2017;40(1):63-68.
78. Christiansen MP, Klaff LJ, Brazg R, et al. A Prospective Multicenter Evaluation of the Accuracy of a Novel Implanted Continuous Glucose Sensor: PRECISE II. Diabetes technology & therapeutics. 2018;20(3):197-206.
79. Christiansen MP, Klaff LJ, Bailey TS, Brazg R, Carlson G, Tweden KS. A Prospective Multicenter Evaluation of the Accuracy and Safety of an Implanted Continuous Glucose Sensor: The PRECISION Study. Diabetes technology & therapeutics. 2019;21(5):231-237.
81. t:slim X2 insulin pump with Control-IQ Technology. User Guide. https://www.tandemdiabetes.com/docs/default-source/product-documents/t-slim-x2-insulin-pump/aw-1004379_d_user-guide-tslim-x2-control-iq-7-3-mgd-artwork-web.pdf?sfvrsn=18a507d7_60. Accessed December 21, 2020.
82. t:slim X2 insulin pump with Basal-IQ Technology. User Guide. https://www.tandemdiabetes.com/docs/default-source/product-documents/t-slim-x2-insulin-pump/user-guide-tslim-x2-basal-iq-6-4-mgdl.pdf?sfvrsn=eeb230d7_139. Accessed December 21, 2020.
83. American association of clinical endocrinologists and american college of endocrinology - clinical practice guidelines for developing a diabetes mellitus comprehensive care plan - 2015. Endocrine practice. 2015;21 Suppl 1:1-87.
84. Rewers MJ, Pillay K, de Beaufort C, et al. ISPAD Clinical Practice Consensus Guidelines 2014. Assessment and monitoring of glycemic control in children and adolescents with diabetes. Pediatr Diabetes. 2014;15 Suppl 20:102-114.
85. 6. Glycemic Targets: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S66-s76.
35
Appendix A: Additional CGM/Insulin Pump Systems Information
Table 1. Integrated Insulin Pump and CGM Systems
Medtronic MiniMed Insulin Pumps22,24,80 Tandem t:slim X281,82 630 G 670 G 770G
Type of System SAP with LGS AID/HCL AID/HCL SAP with PLGS (Basal-IQ)
AID/HCL (Control-IQ) Indicated Population
Patients with diabetes (≥14 y)
T1DM (≥7 y) T1DM (≥2 y)
Patients with diabetes (≥6 y) (Basal-IQ) T1DM (≥6 y) (Control-IQ)
Pairable CGM sensor
Optional CGM with Guardian Sensor (3) or Enlite sensor
Guardian Sensor (3)
Guardian Sensor (3)
Dexcom G6
Abbreviations: AID, automated insulin delivery system; BG, blood glucose; CGM, continuous glucose monitoring; HCL, hybrid closed loop technology; LGS, low glucose suspend feature; PLGS, predictive low glucose suspend feature; SAP, sensor-augmented pump; SG, sensor glucose; y, years of age
2021 ADA Recommendations
• Insulin pumps in general are recommended for consideration in adults and youth with T1DM (A level evidence); or for adults and youth on multiple daily insulin injections who have T2DM or other forms of diabetes, if they are able to safely manage the device (B level evidence).13 Continued access across third-party payers is encouraged for patients who have been successfully using insulin pump therapy.13
o Regarding sensor augmented pump systems with the ability to suspend insulin delivery at a low glucose threshold (ie, automatic low-glucose suspend feature), the ADA recommends considering these systems for adults and youth with diabetes in order to prevent and manage episodes of hypoglycemia. (B level evidence).
o Regarding systems that automatically control insulin delivery (ie, automated insulin delivery systems [AIDs]), where the pump increases and decreases the insulin rate based on the CGM measurements, the ADA recommends these devices be considered in youth and adults with T1DM to improve glycemic control (A level evidence).
36
Appendix B: Additional Background Information
Table 1. Clinical Practice Guideline Recommendations for Continuous Glucose Monitoring Organization
Guideline Key Recommendations
American Diabetes Association (ADA) Standards of Medical Care in Diabetes - 2021 Chapter 7. Diabetes Technology36 - Robust diabetes education, training, and support are needed for optimal CGM device implementation and
ongoing use. People using CGM devices must be capable of using SMBG to calibrate their device and/or confirm readings if they do not match symptoms (Evidence B)
- rtCGM in combination with MDIs and CSII (Evidence A) and other forms of insulin therapy (Evidence C) is a useful tool to reduce and/or maintain A1C levels and/or lower hypoglycemia in adults and youth with diabetes
- isCGM in combination with MDIs and CSII (Evidence B) and other forms of insulin therapy (Evidence C) can be useful and may reduce A1C levels and/or lower hypoglycemia in adults and youth with diabetes to replace SMBG
- In patients on MDI and CSII, rtCGM devices should be used as close to daily as possible for maximum benefit (Evidence A). isCGM devices should be scanned regularly, at least once every 8 h
- When used in addition to pre- and postprandial SMBG, CGM can help to reach A1C goals in diabetes and pregnancy (Evidence B)
- Use of professional CGM and/or intermittent rtCGM or isCGM can be helpful to identify and correct patterns of hyper- and hypoglycemia and improve A1C levels in people with diabetes on noninsulin and basal insulin regimens (Evidence C)
American Association of Clinical Endocrinologists and American College of Endocrinology (AACE/ACE) Consensus statement on the management of type 2 diabetes– 20203 Cites earlier consensus work by the panel on CGM52 - Use of professional CGM systems should be considered in patients not achieving glycemic goals after 3
months of the initial antihyperglycemic therapy and for those who require therapy that is associated with risks of hypoglycemia (sulfonylurea, glinide, or insulin)
- Use of personal CGM systems should be considered for patients on intensive insulin therapy (3 to 4 injections/day or on insulin pump), with history of hypoglycemia unawareness, or with recurrent hypoglycemia
Outpatient glucose monitoring consensus statement--201652 - T1DM: CGM is recommended for adults and children with T1DM, principally for individuals with a history of
severe hypoglycemia and hypoglycemia unawareness, and to assist in correcting hyperglycemia in patients not meeting target ranges for blood glucose level. Before CGM use, patients should know the basics of sensor insertion, calibration, and real-time data interpretation. More in-depth training and more frequent follow-up is recommended for children using CGM
- T2DM patients receiving insulin, sulfonylureas, or glinides: evidence on CGM use is limited. Clinical trials evaluating CGM use in this population are ongoing
- T2DM patients with low risk of hypoglycemia: CGM use is not recommended - Gestational Diabetes: Evidence is unclear concerning the efficacy of CGM in pregnant women with
preexisting diabetes; further studies are ongoing. During pregnancy, CGM can be considered a teaching tool for the assessment of glucose trends and adjusting insulin dosing. Furthermore, CGM can be used as a supplement to SMBG in pregnancy, particularly for monitoring nocturnal hypoglycemia or hyperglycemia and postprandial hyperglycemia
37
Table 1. Clinical Practice Guideline Recommendations for Continuous Glucose Monitoring Organization
Guideline Key Recommendations
Diabetes mellitus comprehensive care plan guideline – 201583 - CGM “should be considered for patients with T1DM and T2DM on basal-bolus therapy to improve A1C
levels and reduce hypoglycemia” (Grade B [Recommendation Grade - Intermediate]; BEL 2 [Evidence Level - Intermediate])
Advanced Technologies & Treatments for Diabetes (ATTD) International Consensus on Continuous Glucose Monitoring, 201710 - CGM should be considered in conjunction with HbA1c for glycemic status assessment and therapy
adjustment in all patients with T1DM and patients with T2DM treated with intensive insulin therapy who are not reaching glucose goals, especially if the patient is experiencing problematic hypoglycemia
Endocrine Society Diabetes Technology-Continuous Subcutaneous Insulin Infusion Therapy and Continuous Glucose Monitoring in Adults: An Endocrine Society Clinical Practice Guideline; 201637 - “Real-time CGM is recommended for adults with well-controlled DM1 and for adults with DM1 who have
HbA1c levels above target. Patients should be willing and able to use a CGM device on a nearly daily basis.” - “Short-term use of real time CGM is suggested for adult patients with DM2 who have HbA1c levels greater
or equal to 7% and are both willing and able to use a CGM device.” - “Education, training, and ongoing support to help achieve and maintain individualized glycemic goals is
suggested for adults with diabetes using CGM” Diabetes and Pregnancy: An Endocrine Society Clinical Practice Guideline; 201362 - It is suggested that CGM be used during pregnancy for women with overt or gestational diabetes when
SMBG is not sufficient to assess glycemic control (expert opinion without evidence ratings) International Society for Pediatric and Adolescent Diabetes The International Society for Pediatric and Adolescent Diabetes 2014 Clinical Practice Consensus Guideline, “Assessment and Monitoring of Glycemic Control in Children and Adolescents with Diabetes”84 “Continuous glucose monitoring (CGM) devices are becoming available that may particularly benefit those with hypoglycemic unawareness, as the devices will alarm when glucose is below a specified range or with rapid rate of fall of glucose (A)” Abbreviations: A1C, hemoglobin A1C; BEL 2, best evidence level 2 (intermediate evidence); CSII, continuous subcutaneous insulin infusion; isCGM, intermittently scanned continuous glucose monitoring; MDI, multiple daily injections; RCT, randomized controlled trial; rtCGM, real-time continuous glucose monitoring; SMBG, self-monitoring of blood glucose ADA 2021 levels of evidence: A= Clear evidence from well-conducted, generalizable RCTs that are adequately powered B= Supportive evidence from well-conducted cohort or case-control studies C= Supportive evidence from poorly controlled or uncontrolled studies E= Expert consensus or clinical experience
38
Table 2. Glycemic Targets per ADA and AACE/ACE Guidelines American Diabetes Association (ADA)- 20211 Monitoring • Test hemoglobin A1c (A1c) twice yearly in patients meeting treatment goals and with stable glycemic
control; otherwise, test A1c quarterly in those with therapy change or unmet glycemic targets • Note that A1c is less reliable conditions affecting red blood cell turnover (eg, anemia hemoglobinopathies,
• Classification of hypoglycemia Level 1 <70 to ≥54 mg/dL
Considered clinically important Level 2 <54 mg/dL
Neuroglycopenic symptoms start. Requires immediate action Level 3 Severe episode characterized by distorted mental and/or physical status
Requires assistance from another person. Can lead to loss of consciousness, seizure, coma, or death
Adults, non-pregnant • A1c target is generally <7% (for patients without significant hypoglycemia); this corresponds to >70% time
in range, with time below range <4%, on the ambulatory glucose profile via glucose management indicator1 o A lower A1c target (eg, A1c <6.5%) can be set for individuals at low risk for hypoglycemia or other
adverse effects.1 Such patients may include those with shorter duration of diabetes, T2DM treated with lifestyle or metformin only, long life expectancy, or no significant cardiovascular disease85
o A1c target of <8% may be appropriate in individuals with limited life expectancy or if harms of more intensive treatment outweigh benefits (eg, history of severe hypoglycemia, advanced macro- or micro-vascular complications, extensive comorbidities, long-standing diabetes and inability to achieve lower threshold targets85)
• Pre-prandial capillary plasma glucose target is 80-130 mg/dL, but can set to a more or less stringent goal per the patient’s needs
• Peak postprandial capillary plasma glucose (1-2 hours after beginning of the meal) target is <180mg/dL, but can be set to a more or less stringent goal per patient need
Older Adults • A1c target of <7 - 7.5% for older adults who are otherwise healthy (eg, few coexisting chronic diseases,
intact cognitive function and functional status) • A1c goal of <8% or <8.5% for older adults with multiple coexisting chronic illnesses, cognitive impairment,
functional dependence Children and Adolescents • A1c target of <7% should be considered for most children (with T1DM or T2DM); a lower goal of <6.5% can
be used if it can be achieved without hypoglycemia or other adverse events o A less stringent goal of <7.5% can be used for patients with increased risk of hypoglycemia (eg,
hypoglycemia unawareness; lack of access to insulin or advanced delivery, or advanced monitoring technology; inability to check blood glucose regularly; or who have nonglycemic factors [eg, high glycators]). Even less stringent goals can be set for patients with severe hypoglycemia or where harms are greater than benefits.
• A1c should be individualized (relatively low rates of hypoglycemia occur in youth with T2DM) Pregnant Women • The A1c goal is <6% to reduce the risk of congenital anomalies if it can be achieved without significant
hypoglycemia; otherwise, it can be relaxed to <7% to prevent hypoglycemia • Fasting plasma glucose target is 70 - 95 mg/dL and either 1-h postprandial glucose 110 – 140 mg/dL or 2-h
postprandial glucose 100 - 120 mg/dL
39
Table 2. Glycemic Targets per ADA and AACE/ACE Guidelines American Academy of Endocrinologists and American College of Endocrinology (AACE/ACE); T2DM Management Guideline, 20203 Adults with T2DM • An A1c target of <6% is considered optimal if it can be achieved without significant hypoglycemia or
complications • An A1c target of >6.5 is appropriate for those in whom the lower target cannot be achieved without adverse
outcomes (eg, patients with history of severe hypoglycemia, limited life expectancy, advanced renal disease or macrovascular complications, extensive comorbid conditions, or long-standing T2DM with difficulty controlling A1c goal despite intensive effort)