46
Sehrish fatima 08-172 batch-K Final year MBBS
| Date post: | 16-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | ayub-medical-college |
| View: | 191 times |
| Download: | 0 times |

Sehrish fatima
08-172
batch-K
Final year MBBS
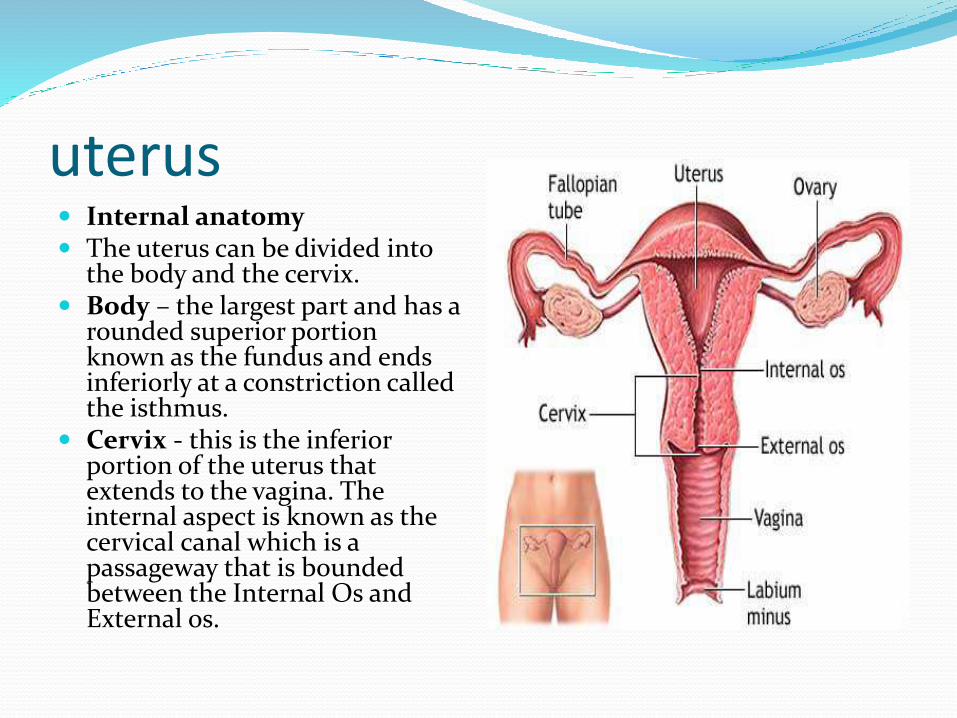
uterus Internal anatomy The uterus can be divided into
the body and the cervix. Body – the largest part and has a
rounded superior portion known as the fundus and ends inferiorly at a constriction called the isthmus.
Cervix - this is the inferior portion of the uterus that extends to the vagina. The internal aspect is known as the cervical canal which is a passageway that is bounded between the Internal Os and External os.
Internal anatomy
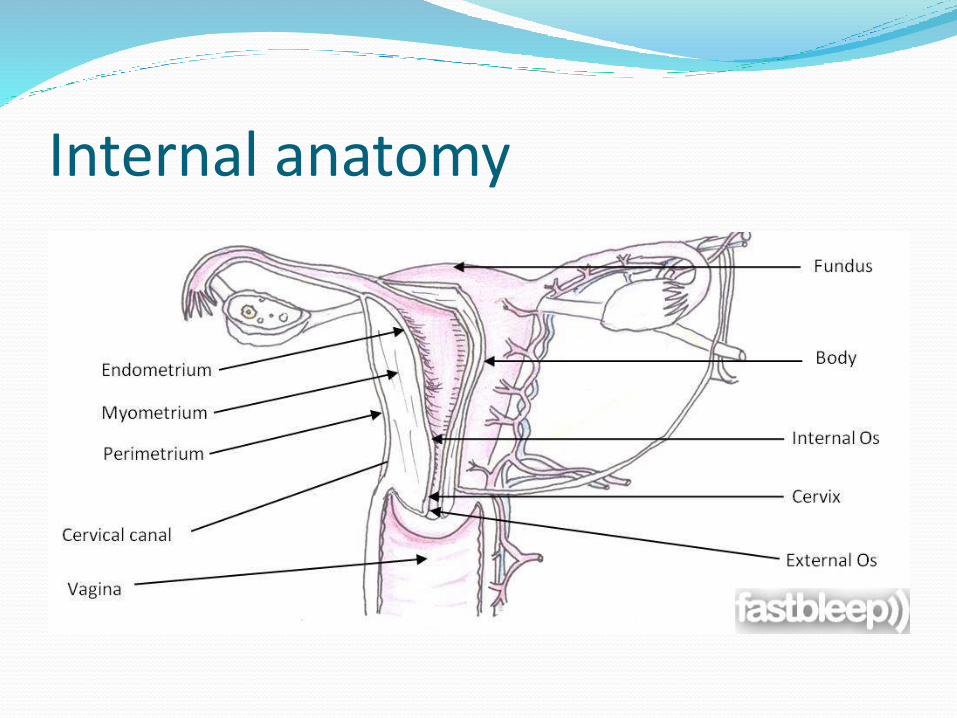
Uterine wall The wall of the uterus consists of: Endometrium – a thin glandular layer (mucosa) that is shed
every month as part of the menstrual cycle Myometrium – thick smooth muscle layer that contracts
when pushing a fetus out Perimetrium – outermost layer known as serosa which is
covering the fundus and posterior surface of uterine body
Internal anatomy
Definition
Fibroid is a benign tumor arising from the smooth muscles of uterus .Consisting predominantly of smooth muscle fibers admixed with small amount of connective tissue.
It should be more appropriately myoma or leiomyoma.
Incidence
They are the most common pelvic tumors
It is found in 25% of white women & 50% of black women.
Age : greater than 30

Etiology Unknown
Estrogen: It has been implicated in growth of myomas. Studies show that :
1. Myomas contain estrogen receptors in higher concentration than surrounding myometrium.
2. Myomas may increase in size with estrogen therapy & in pregnancy 3. They are not detectable before puberty4. Regress after menopause due to fall in estrogen levels.
Progesterone1. increase mitotic activity & reduce apoptosis in size
Genetic predisposition
Risk Factors AGE-Reproductive age group more common(Thirty & forty)
FAMILY HISTORY-Increases risk
RACE-African & Caribbean –American women
OBESITY-Higher risk
EATING HABITS-Red meat & ham
PARITY-Develop in women who have no children, with genetic determinant.
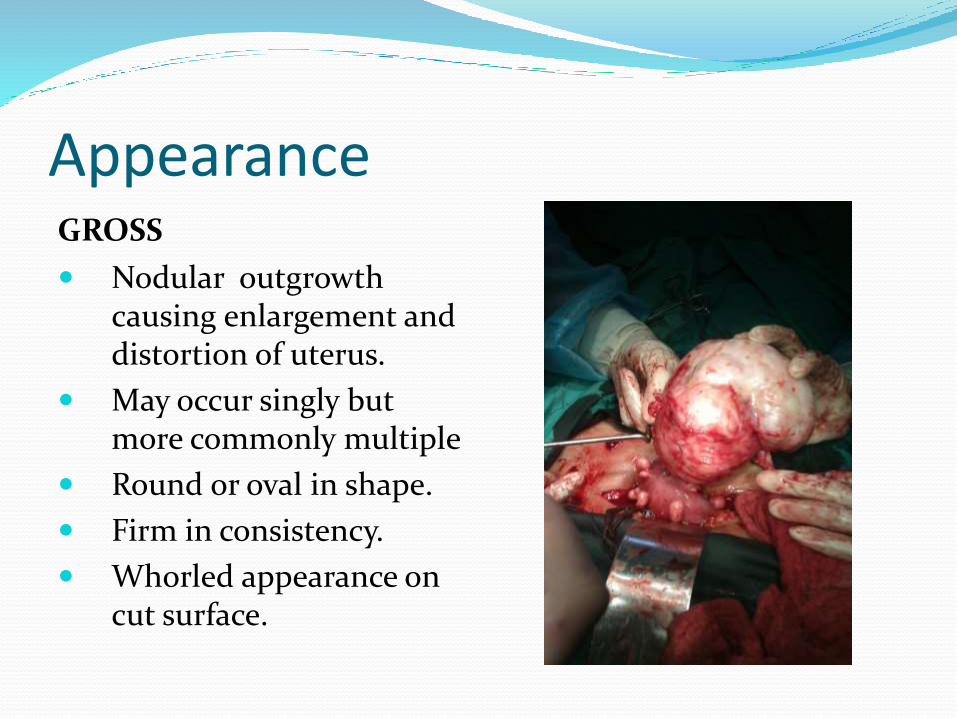
AppearanceGROSS
Nodular outgrowth causing enlargement and distortion of uterus.
May occur singly but more commonly multiple
Round or oval in shape.
Firm in consistency.
Whorled appearance on cut surface.

Gross features
microscopy
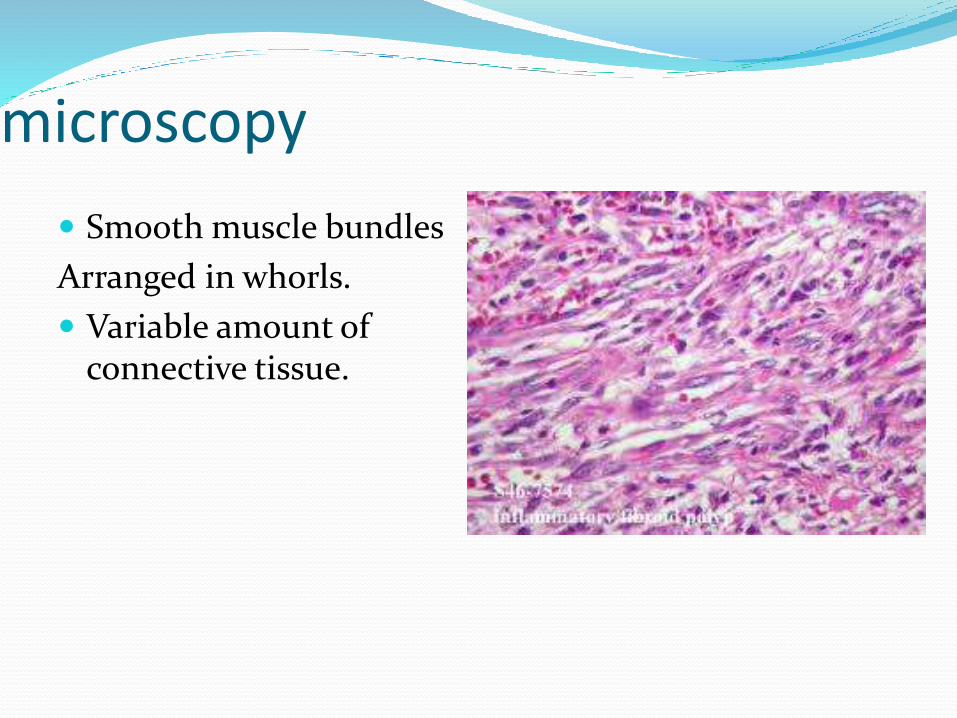
Smooth muscle bundles
Arranged in whorls.
Variable amount of connective tissue.
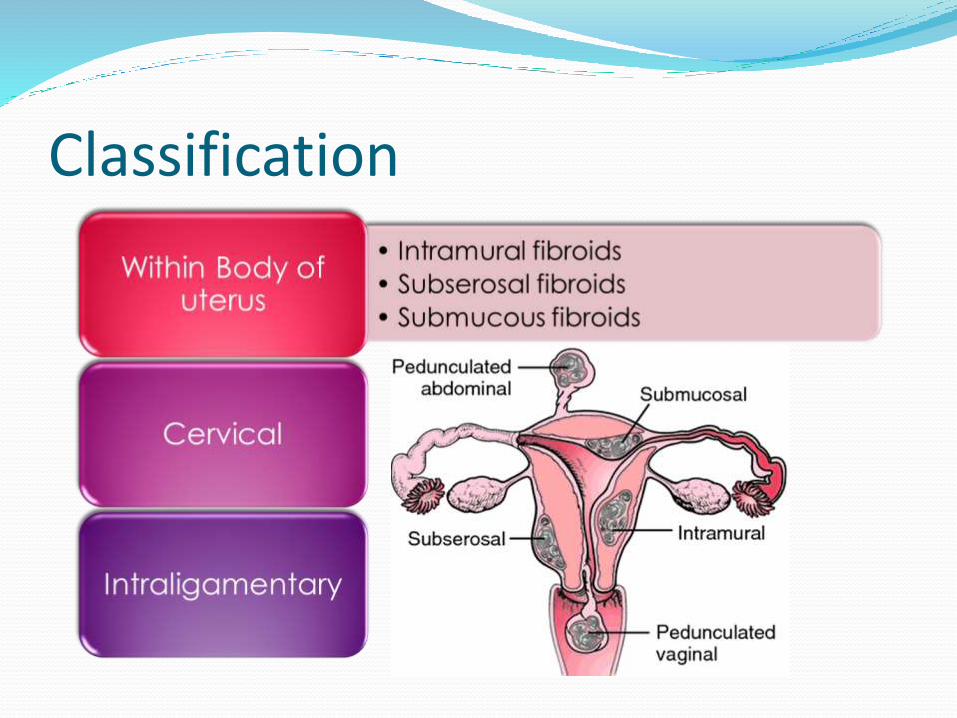
Classification
Intramural/Interstitial Fibroids Within uterine walls ,surrounded by myometrium , non capsulated but pseudocapsule form with growth , blood supply is through nutrient arteries entering through the pseudocapsule.
Originates from outer myometrium & projects outwards from uterus covered with peritoneum, attain large size to lack of surrounding myometrium
Subserosal Fibroids
Pedunculated fibroids Further extrusion outwards with the development
of pedicle makes it a pedunculated fibroid If such a tumor gets attached to a vascular organ
and is cut off from its origin- Parasitic fibroid
Uterine contractions may force the myoma towards the cavity where it is covered only by endometrium it is called submucous fibroid
Submucous fibroids
…Contd• .CERVICAL FIBROID;
1-2% OF CASES.
SINGLE.
SITE: SUPRAVAGINAL PART OF CERVIX.
a.Intramural
b.Subserous
3.INTRALIGAMENTARY FIBROID;
Arising from smooth muscle fibers with in broad ligament.
..
Clinical findings
symptoms Symptomatic in only 35-50% of Pt
Symptoms depend on location, size, changes & pregnancy status
1-Abnormal uterine bleeding
The most common 30%
Heavy / prolonged bleeding (menorrhagia) iron deficiency anemia
…Contd Submucous myoma produce the most pronounced
symptoms of menorrhagia, pre & post-menstrual spotting
Bleeding is due to increase in size of endometrium , venous stasis and ulceration of the overlying endometrium
Pedunculated submucousal fibroids intermenstrtual bleeding
…Contd
Pain : pain usually start when complications occurs e.g
torsion
red degeneration
sarcomatous degeneration
• Pressure symptoms :
Large fibroids causes interference with venous and lymphatic drainage of the lower limb causing edema and varicosities.
Pressure on pelvic vein may cause hemorrhoids.
Urinary symptoms Cervical fibroid – irritation of bladder – increased
frequency
large cervical fibroid – impaction of pelvis – urinary retention
A large fibroid may fill the abdominal cavity causing dyspepsia due to stomach irritation & dyspnea due to pressure on lungs.
Abdominal Mass
ExaminationGeneral physical examination No specific findings Excessive loss of blood may cause anemia ,presenting with
pallor and in extreme cases with breathlessness Edema and varicosities of limbs are rare findings with large
fibroids .Abdominal examination :Uterus palpable abdominally Single fibroid -- central uterus with smooth surface Multiple fibroids – irregular mass maybe shifted to a sidePelvic examination : Protuding fibroids easily seen
Investigations
Investigation of choice
• Ultrasonography
Under special circumstances
• Hysteroscopy and curettage
• Laparoscopy
Other investigation
• Hysterosalpingogram
• Modern imaging techniques
• Complete blood picture
Ultrasonography Investigation of choice
Typical fibroid appearance :mild to moderate echogenic mass in the uterine wall that causes nodular distortion of uterine outline.
Small intramural or Submucous fibroid recognized by distortion of the normally linear central endometrial echoes.
Fibroids with hyaline degeneration : anechoic area within fibroid
Fibroids with cystic degeneration: will give Snow storm appearance
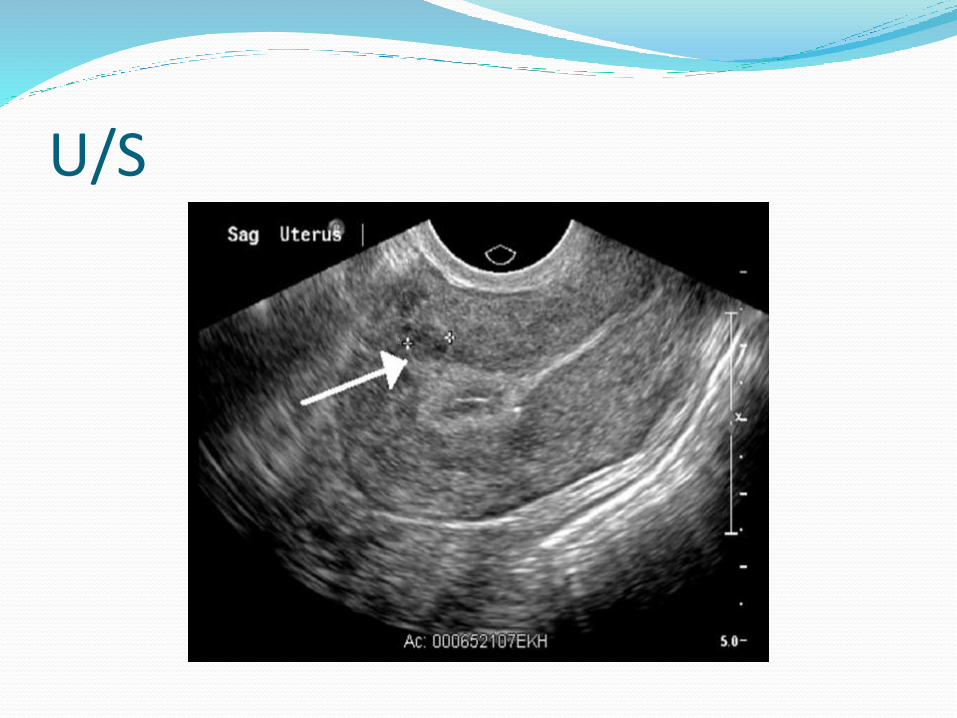
U/S
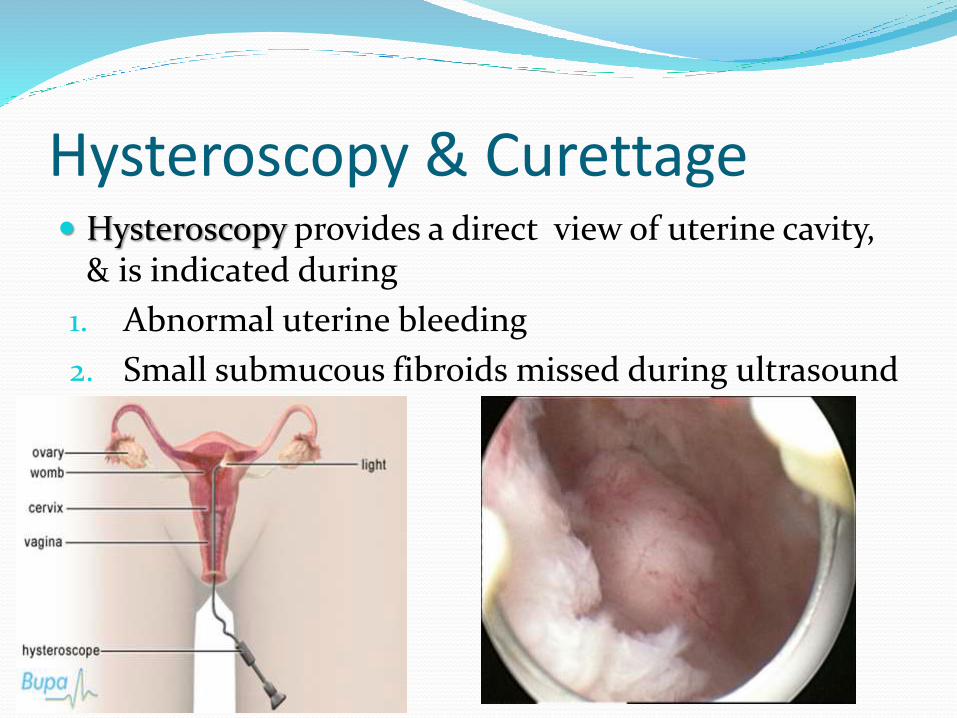
Hysteroscopy & Curettage Hysteroscopy provides a direct view of uterine cavity,
& is indicated during
1. Abnormal uterine bleeding
2. Small submucous fibroids missed during ultrasound
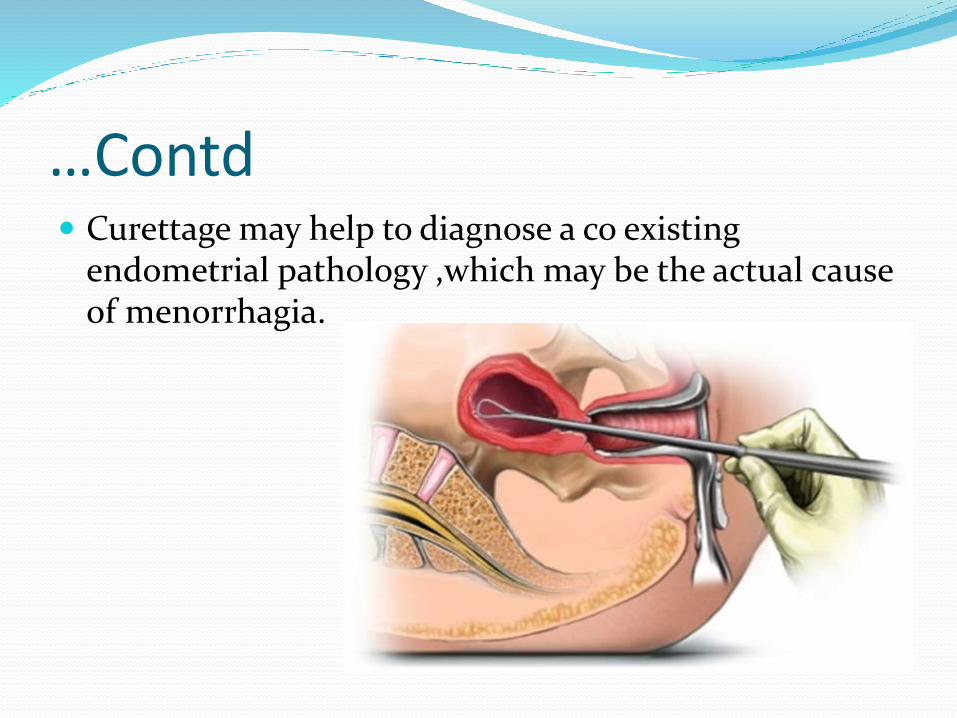
…Contd Curettage may help to diagnose a co existing
endometrial pathology ,which may be the actual cause of menorrhagia.
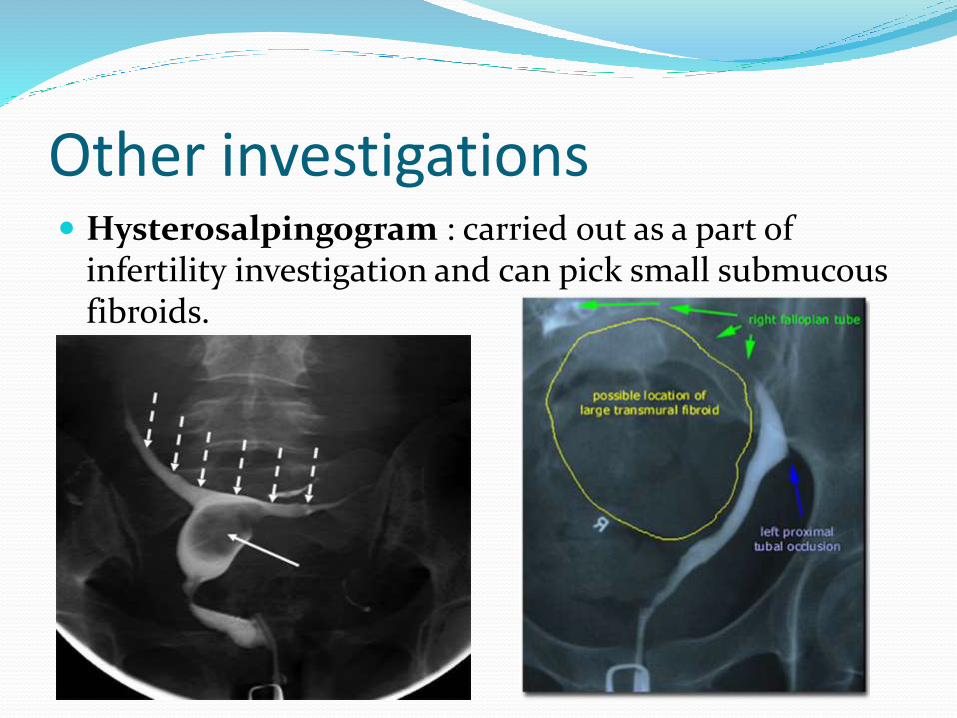
Other investigations Hysterosalpingogram : carried out as a part of
infertility investigation and can pick small submucousfibroids.
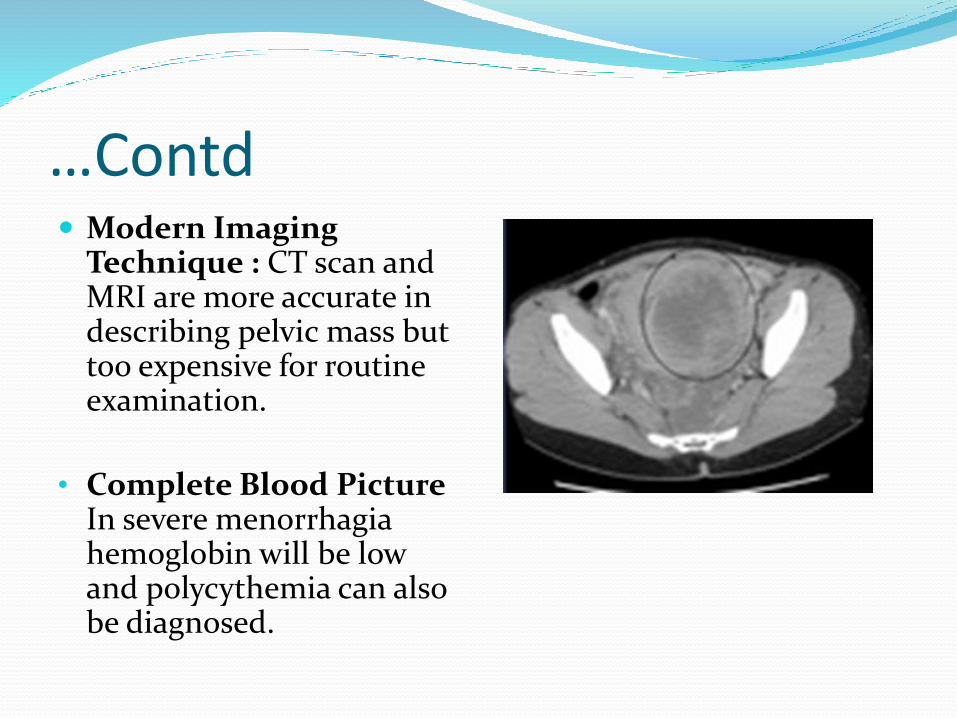
…Contd Modern Imaging
Technique : CT scan and MRI are more accurate in describing pelvic mass but too expensive for routine examination.
• Complete Blood Picture In severe menorrhagia hemoglobin will be low and polycythemia can also be diagnosed.
Treatment .
Conservative Treatment Asymptomatic fibroid of size less than 12 weeks
pregnancy in a patient of 42 years of age is left alone in a hope that It would regress after menopause.
An asymptomatic fibroid of size more that 12 weeks of pregnancy does not justify prophylactic removal as risk of sarcomatous change is less than 0.1%.
Only management required is a regular follow up till menopause.
Removal only indicated in case of a very large fibroid or a rapidly increasing in size due to concern about the nature of the mass .
Medical Treatment GnRH analogues is the only drugs which has shown
promising results .
GnRH analogues :
Monthly IM depot injection
Daily Nasal spray
prescribed for 3 months
improved 80% cases of menorrhegia,
50% of the fibroid size is reduced
Disadvantages: expensive , effects only last during therapy , cause post menopausal symptoms (hot flushes , night sweats , psychological disturbance)
…contd
Therefore only given when reduction in size and vascularity is required prior to myomectomy & hysterectomy.
Long term use (6months or more) only allowed when patient is unfit for surgery ( obese ,extensive adhesions) or approaching her menopause.
Other drugs : these shows reduction in size of fibroids up to some extent
Danazol
Gestrinone
Surgical treatment Surgical treatment is present in the form of Myomectomy Hysterectomy
Myomectomy term myomectomy is used for an operation where the uterus is
conserved and fibroid is removed. Preferred treatment in following conditions, Symptomatic fibroids in young patient, Infertile patients when fibroids are only pathology, Patients wishing to have more children, Patients with recurrent abortion ,fibroids likely to be the underlying
cause, Patients wishing to conserve her uterus.
Hysterectomy It is the treatment of choice when
1. Patient is above 40
2. Multiple fibroids
3. Family is completed
4. Symptoms are more severe
.
Complications
DEGENERATION ATROPHIC (decrease in size, but do not disappear)
due to estrogen withdrawl
HYALINE ( loses typical whorl appearance, tumourlook homogenous & glossy area microscopically)
CYSTIC (hyaline cystic)
Fatty degeneration
Red generation (seen during pregnancy ,similar to ischemic necrosis ,fibroid appears reddish due to thrombotic and haemolytic changes in blood vessles)
SARCOMATOUS CHANGE Very rare
0.1% of cases
Starts in the center of tumour
Any size or type of myoma can undergo sarcomatouschange
Malignant change suspected when:
Rapid increase in size
Painful
tender
INFECTION Submucous or subserous myoma if lies near an
inflammed organ… Infection
More common in the ones that have undergone necrosis
Infection occurs:
During puerperium
After abortion
Inflammed appendix
Diverticulum
TORSION
Pedunculated Subserous Myoma…. Torsion
Sudden attack of pain
Tenderness
Difficult to differentiate from red degeneration or torsion of ovarian cyst
.
Differential diagnosis
.
Pregnancy Other pelvic masses1. -Ovarian Ca2. -Tubo-ovarian abscess 3. -Endometriosis4. -Adenexa, omentum or bowel adherent to the uterus Other causes of uterine enlargement:1. -Adenomyosis2. -Myometrial hypertrophy3. -Congenital anomalies4. -Endometrial Ca
.
Other causes of abnormal bleeding
1. Endometrial hyperplasia
2. Endometrial or tubal Ca
3. Uterine sarcoma
4. Ovarian Ca
5. Polyps
6. Adenomyosis
7. DUB
8. Endometriosis
9. Exogenouse estrogens
10. Endometrial biopsy or D&C is essential in the evaluation of abnormal bleeding to exclude endometrial Ca
.
Pregnancy and myomas
Effects of Myomas on pregnancy
• Myomas are rarely seen associated with pregnancy (3%)• Commonly seen in an elderly primigravida
ABORTION (risk is high) PREMATURE LABOUR MALPRESENTATIONDuring labour: Abnormal uterine action Cervical dystocia ( interference in dilation of cervix) Obstructed labourDuring puerperium: Puerperal sepsis Delayed involution of uterus
Effects of Pregnancy on Myomas
Increase in size
Change in consistency: Become Soft due to congestion & oedema
Red degeneration
Torsion ( in a pedunculated fibroid )
Infection
Thank You

















