50
UTERINE LEIOMYOMATA Dr Zeinab Abotalib MD, MRCOG Associate Professor & Consultant Obstetrics & Gynecology Infertility And Assisted Conception
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | terence-parsons |
| View: | 218 times |
| Download: | 0 times |
UTERINE LEIOMYOMATA
Dr Zeinab Abotalib MD, MRCOG
Associate Professor & Consultant
Obstetrics & Gynecology
Infertility And Assisted Conception
Uterine Leiomyomata
• Benign tumor comprised mostly of smooth muscle cells
• First described by Reinier De Graff 1641Reinier De Graff 1641
• Most common tumor of the female pelvis
• Represent 1/3 of all GYN admissions to hospitals
Incidence
• Usually quoted 50% (Underestimate)– Cramer and Patel
• 100 serial Uteri
• Sectioned at 2mm
• 77 of 100 had myomas– 84% had multiple myomas
– 649 myomas found in all
• No difference in incidence within pre or post menopausal uteri
Am J Clin Pathol. 1990 Oct;94(4):435-8
Incidence
• More common in African-Americans than More common in African-Americans than whitewhite– Torpin et al. investigated 1741 UteriTorpin et al. investigated 1741 Uteri
• Overall incidence 3 times higher in blacksOverall incidence 3 times higher in blacks
• Also tended to be largerAlso tended to be larger
• Also occurred at a younger ageAlso occurred at a younger age
J Obstet Gynecol 1942;44:569
Incidence
• Cumulative incidence by age 50, > 80% for African American and nearly 70% for Caucasian women.
• One in four women have at least one submucosal fibroid.
• Overall prevalence of uterine fibroids increases with age from 3.3% in women 25-32 to 7.8% in women 33-40 years.
- Baird et al, Am J Obstet Gynecol 2003.
- Borgfeldt et al, Acta Obstet Gynecol Scand 2000.
Etiology
• Arise from a single muscle cell (monoclonal).
• Proliferate under the influence of sex hormones, including estrogen, progesterone & androgens.
• Effects of steroids are modulated by local growth factors.
- Rein et al, Am J Obst Gyne 1995.
- Ichimura et al, Fertil Steril 1998.
- Stewart et al, Obstet Gynec 1998.
- Wer et al, Fertil Steril 2002.
Etiology
• Fibroblast growth factor
• Vascular endothelial growth factor
• Heparin-binding epidermal growth factor
• Platelet-derived growth factor
• Transforming growth factor
• Parathyroid hormone-related protein
• Prolactin
Etiology
• Risk Factors– Nurses Health Study II
• 95,061 nurses completed questionnaires in 1989, 1991, 1993
– Obesity
– Early menarche
– Nulliparity
Fertil Steril. 1998 Sep;70(3):432-9
Etiology
• Oral Contraceptives– High dose pills have been assoc. with
stimulation of fibroid tumors
• Smoking
Presentation
• Most fibroids do not cause symptoms.
• 20-50% experience tumor-related symptoms:
- Menstrual dysfunction- Bowel and bladder dysfunction- Bulk effects
• Such symptoms, account for up to 35% of all hysterectomies.
- Lefebvre et al, J Obstet Gynecol Can 2003.
- Myers et al, Agency for Health Care Research and Quality, 2001.
Symptoms
• Pelvic Pain• Menstrual
Irregularities• GI complaints• Bladder
complaints• Dyspareunia
• Back pain• Leg pain• Vascular
symptoms• Infertility
• Asymptomatic
Diagnosis
• History
• Bimanual pelvic or abdominal exam
• Pelvic ultrasound - most common
• MRI, HSG, sonohysterogram, hysteroscopy
Appearance
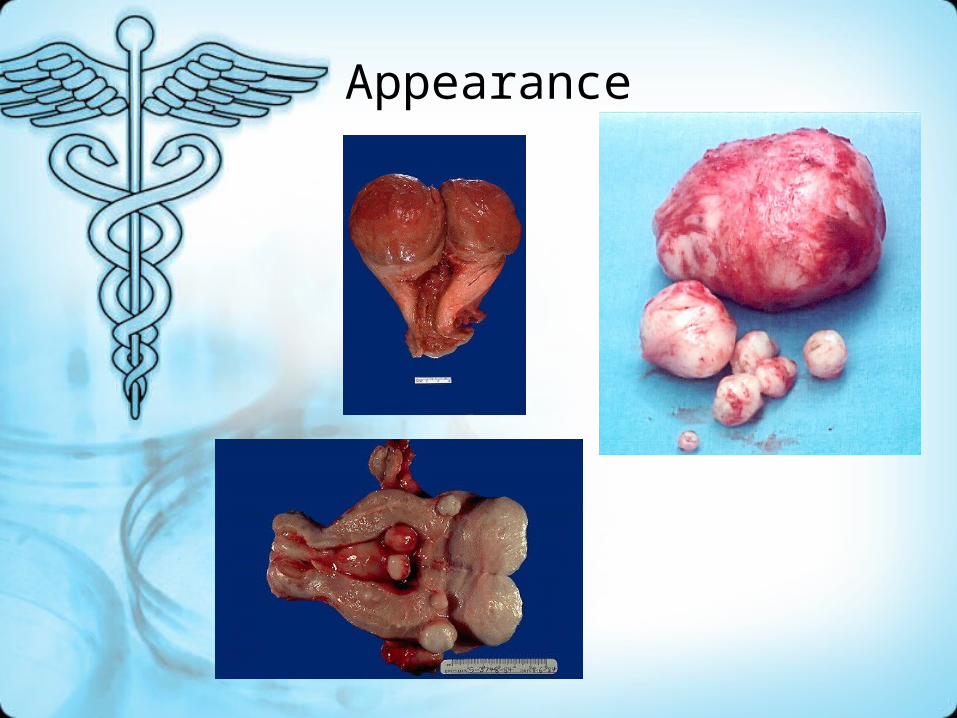
Appearance
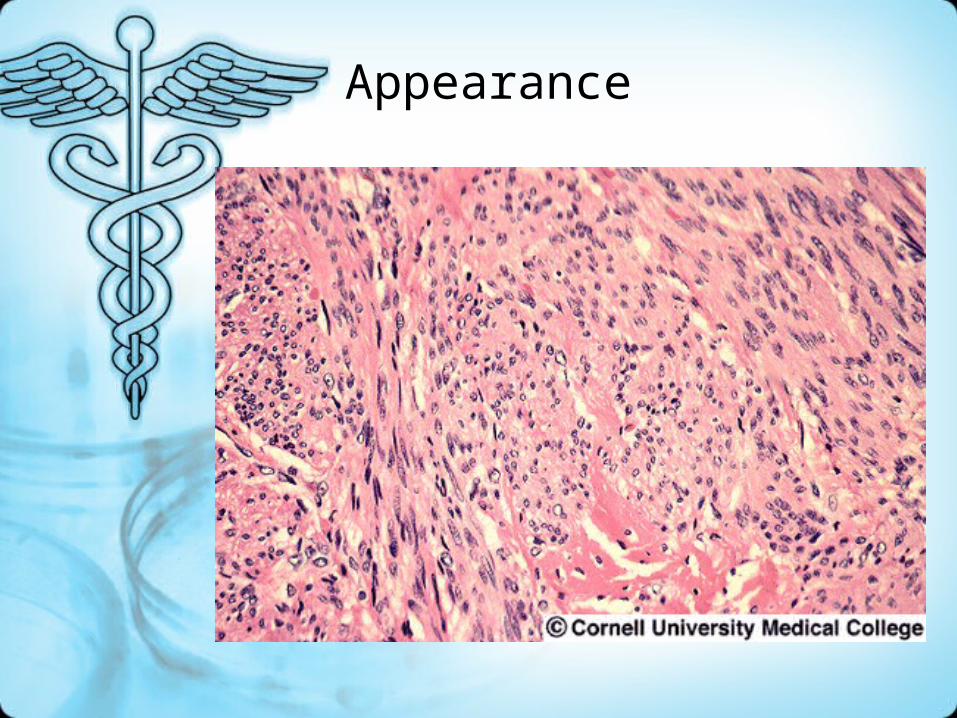
Appearance

Degenerative Changes
• Degenerative changes are reported in approximately two-thirds of all specimens, but most of them have no clinical significance.
1. Hyaline degeneration- It is the most common
2. Cystic degeneration
3. Mucoid degeneration
4. Fatty degeneration
5. Carneous degeneration
6. Calcification
7. Sarcomatous degeneration(malignant transformation)
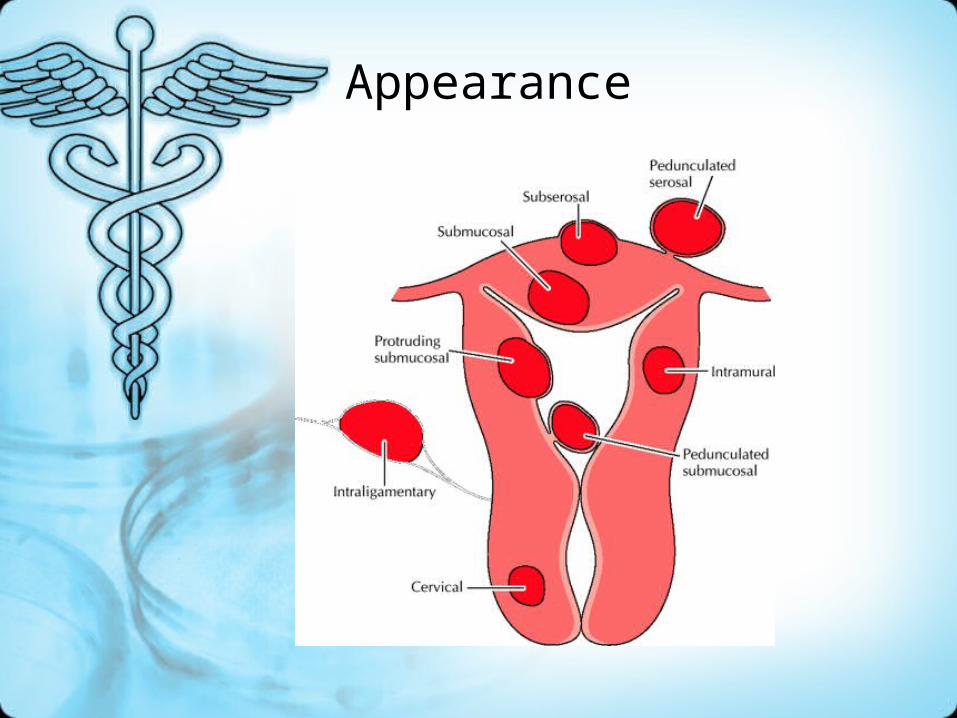
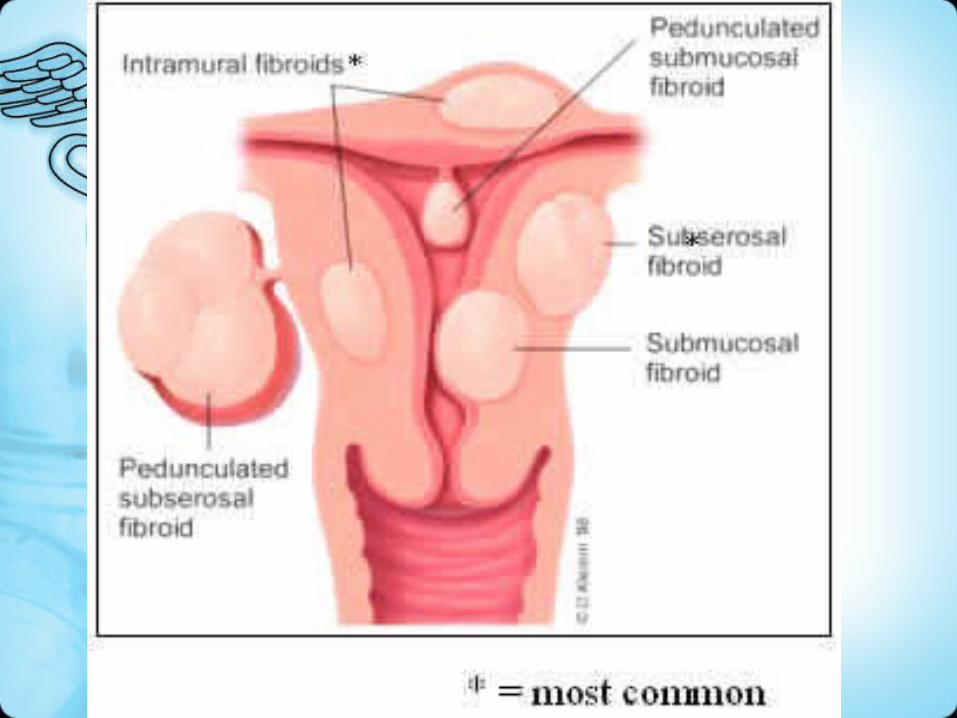
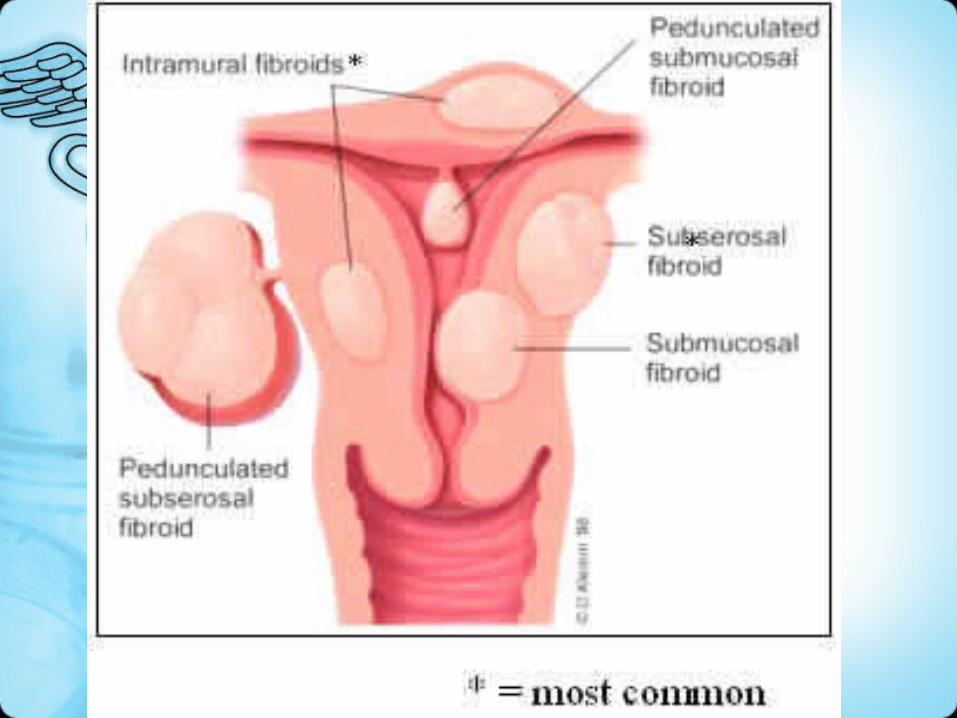
Uterine Fibroids
Benign tumour of uterine tissue
3 locations:
• subserosal
• intramural
• submucosal
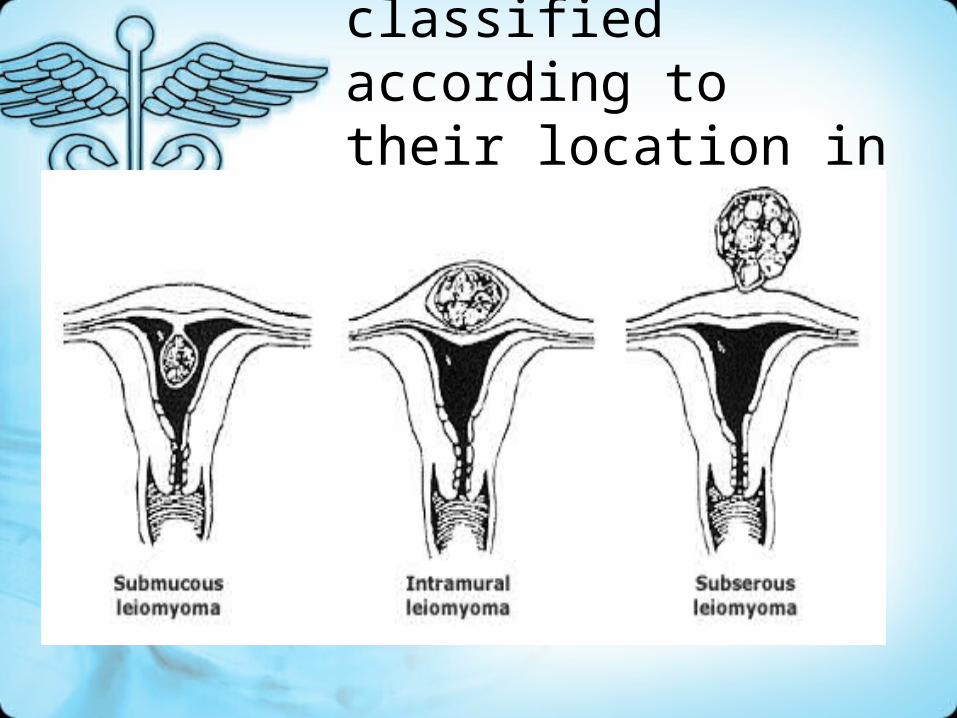
Leiomyomas classified according to their location in the uterus
How are they diagnosed?
• Usually detected on an internal gynecological exam
• Diagnosis is usually confirmed by ultrasound but can also be made with magnetic resonance (MR) or computed tomography (CT) scans.
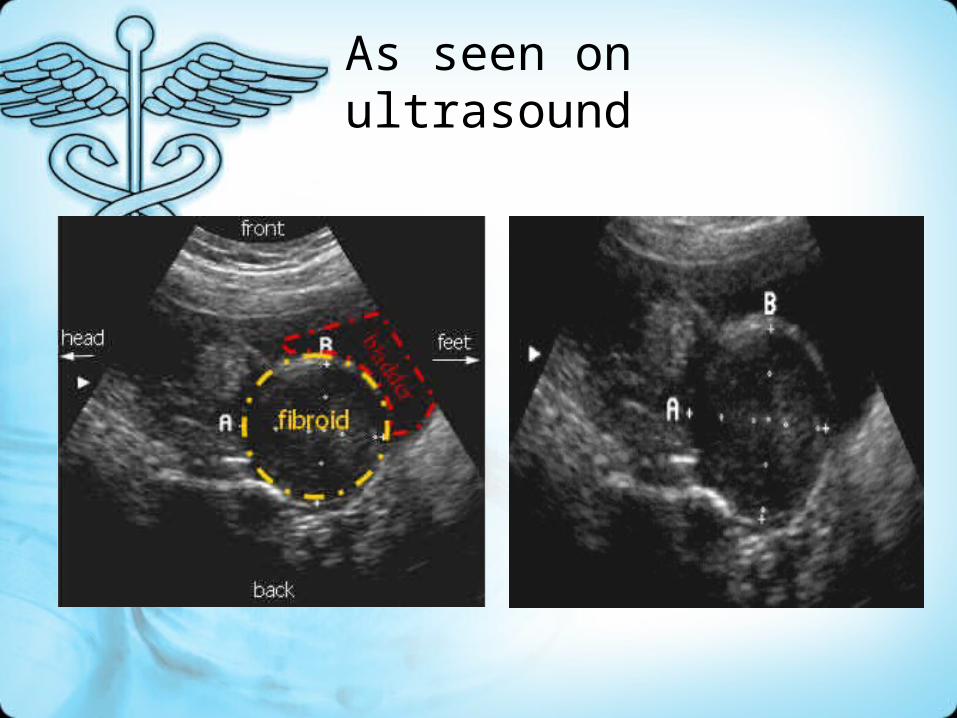
As seen on ultrasound
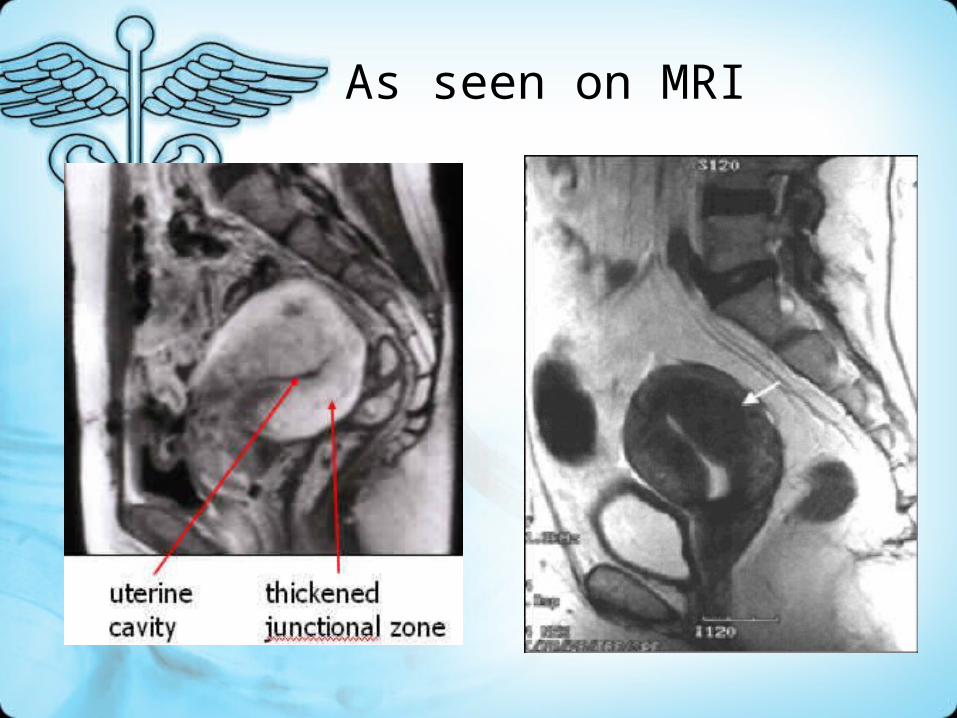
As seen on MRI
Factors that should be considered prior to initiating treatment include:
• Size of the myoma(s)
• Location of the myoma(s) (Symptoms
• Woman's age (eg, is she near menopause?)
• Reproductive plans
How are they treated?
• Depends on size and location
• Surgical therapy - hysterectomy, myomectomy
• Drug therapy - pain relievers, hormone therapy (to shrink them)
• Uterine artery embolization
Treatment
• Expectant management - most cases• Indications for treatment
– Abnormal uterine bleeding, causing anemia
– Severe pelvic pain– Large or multiple– Obscuring evaluation of adnexa– Urinary tract symptoms– Postmenopausal or rapid growth

Treatment Choices
• Medical therapies– Medroxyprogesterone (Provera)– Danazol– GnRH agonists (nafarelin acetate,
Depot Lupron)
Treatment
– RU486• Anti-progestin
– High affinity to Progesterone and glucocorticoid receptors
• Murphy et al (1995) showed decrease of volume an average 49%
• Recent reviews supports usage, but has been associated with
– Hot flashes
– Endometrial hyperplasia
– Is not associated with trabecular bone lossFertil Steril. 1995 Jul;64(1):187-90Obstet Gynecol. 2004 Jun;103(6):1331-6Clin Obstet Gynecol. 1996 Jun;39(2):451-60

Treatment
• Gestrinone– Antiestrogen/antiprogesterone
• GnRH analogues– Suppresses pituitary mediated
secretion of estrogens– Basically treat 3-6 months– Expect 50% reduction of uterine
volume

Treatment Choices
• Uterine Artery Embolization (UAE)
UAE
• Within three months following embolization:- 45% and 55% reduction in total uterine and
myoma volume.- Reduction in symptoms in approximately 80%
of women.
• long- term data on durability and effects on fertility and pregnancy outcomes are very limited.
Pron et al, Fertil Steril 2003
Burbank et al, J Am Assoc Gynecol Laparosc 2000
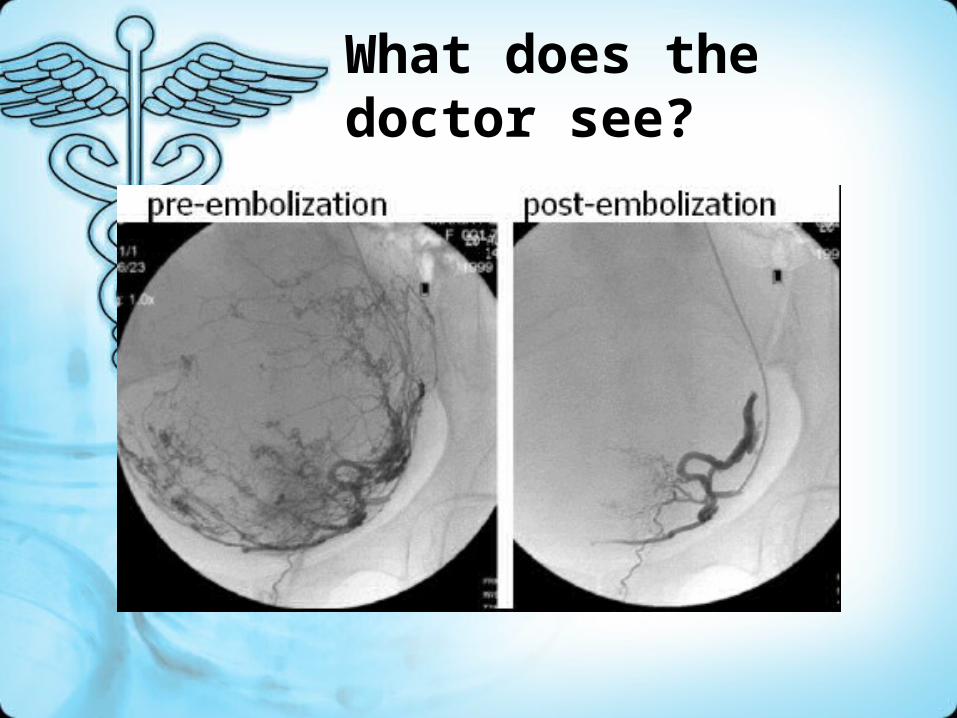
What does the doctor see?
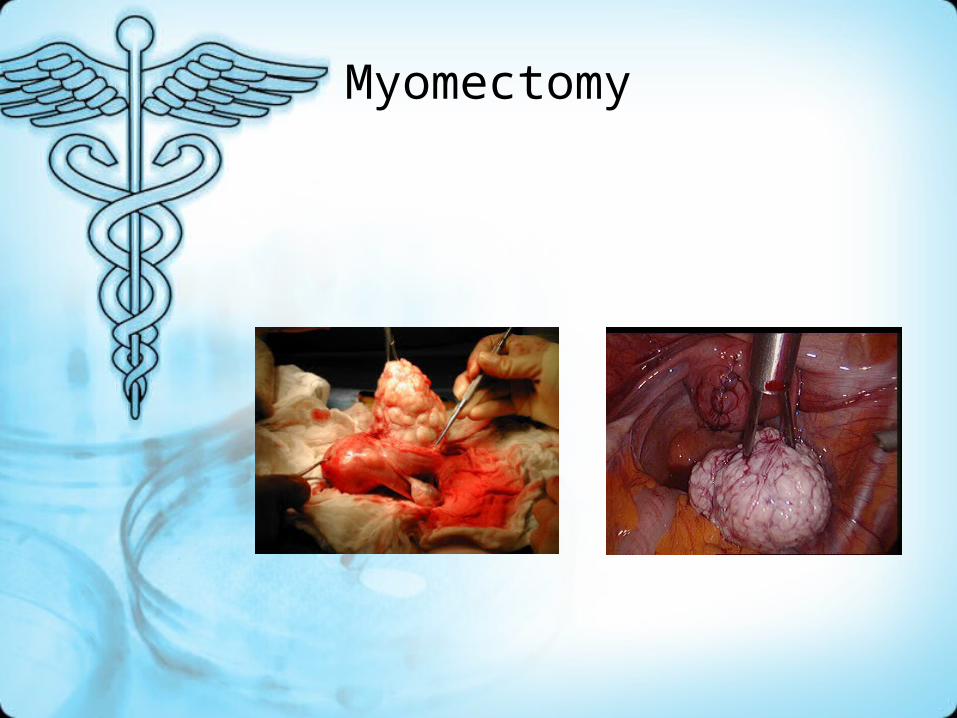
Myomectomy
Myomectomy
• First performed by Washington and John Atlee, 1844
• May be approached in a variety of ways– Abdominally (open)– Laparoscopic– Hysteroscopic
• Primarily for submucosal/intramural fibroids impacting the endometrial cavity
– Vaginal• Primarily for pedunculated submucous fibroids
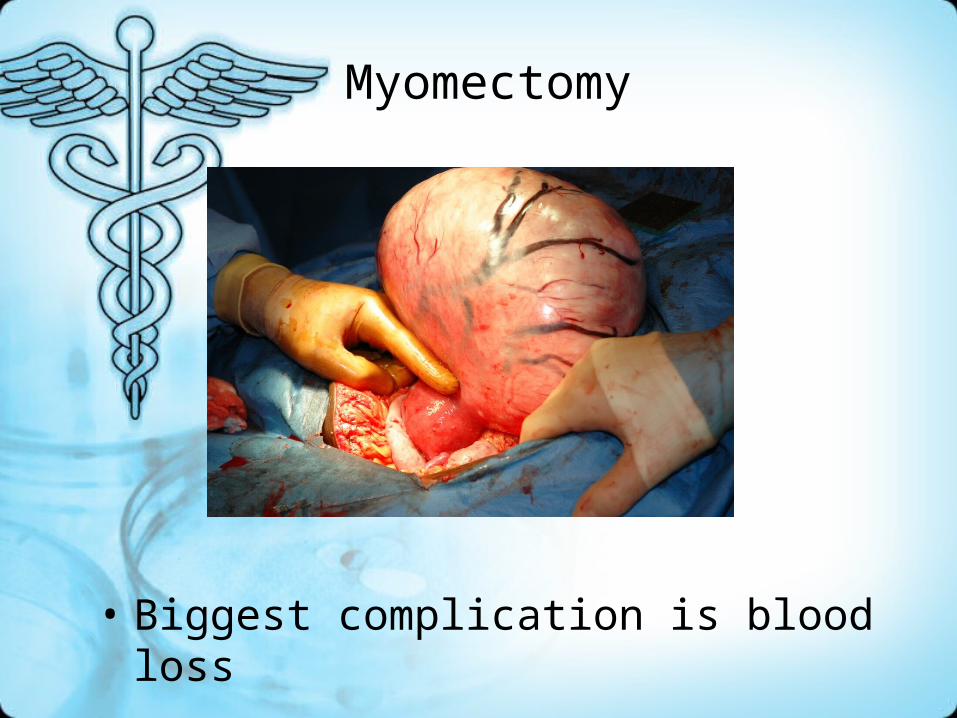
Myomectomy
• Biggest complication is blood loss
Myomectomy (local surgical removal of fibroids)
• Sparing the uterus
• Complications significant blood loss could require hysterectomy
• Fibroids can recur20 - 25% will need another procedure for treatment of new fibroids
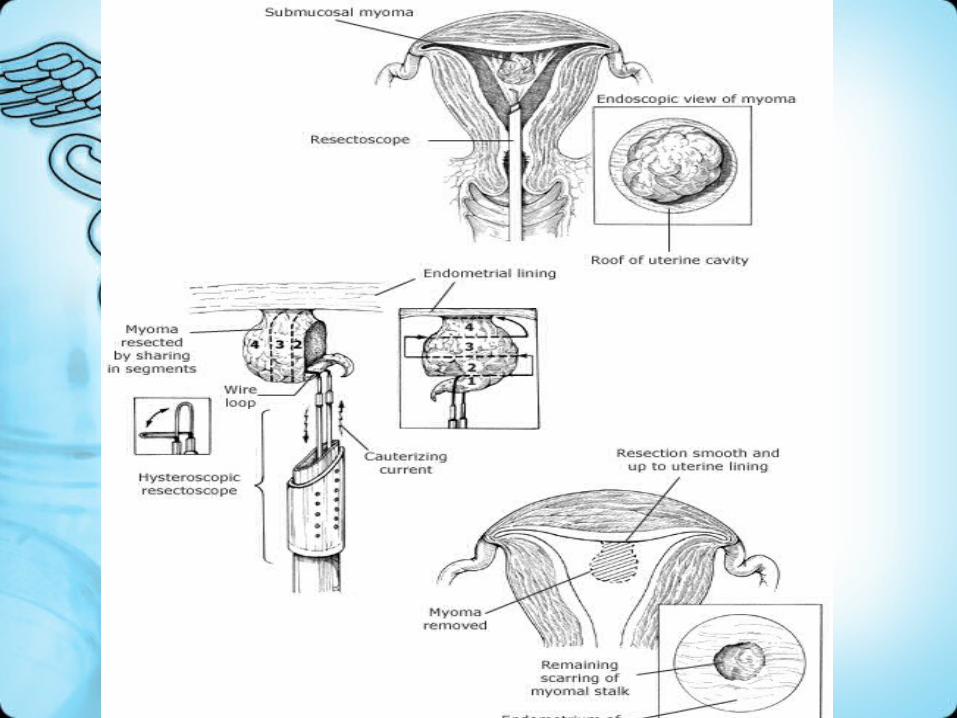
Myomectomy
• Hysteroscopy for intracavitary / submucous
• Laparotomy
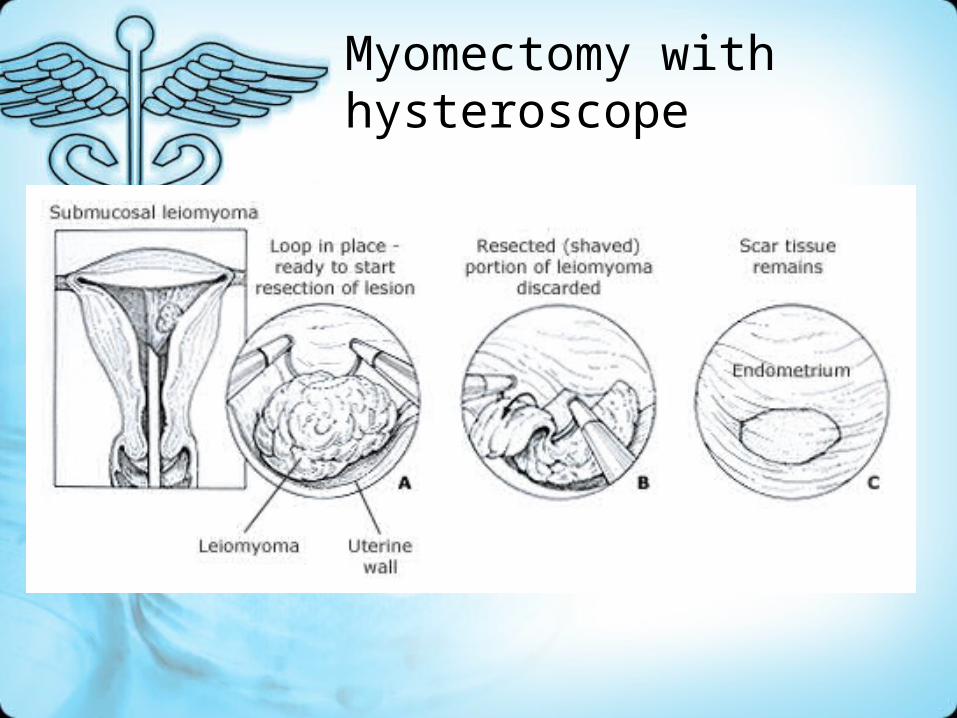
Myomectomy with hysteroscope
Myomectomy
• Hysteroscopy for intracavitary / submucous
• Laparotomy
Treatment Choices
• Hysterectomy– Vaginal– Abdominal
Hysterectomy
• Curative, but irreversible
• Until now, the standard therapy for fibroids 1/3 of all hysterectomies are performed for fibroids
• Complications: bleeding, infection, adhesions, risks associated with general anesthetic
• 6 - 8 week recovery
Comparison of treatment options
TreatmentTreatment ProsPros ConsCons
Pain Pain MedicationMedication
Reduces Reduces PainPain
Doesn't solve Doesn't solve problemproblem, , Pain Pain returnsreturns
luperon luperon Reduces Reduces sizesize Improves Improves symptomssymptoms
side-effects, side-effects, Symptoms Symptoms return on return on discontinuationdiscontinuation
Comparison of treatment options
TreatmentTreatment ProsPros ConsCons
HysterectomyHysterectomy
Complete Complete curecure
Major Major operationoperation can’t become can’t become pregnantpregnant
MyomectomyMyomectomy
successfulsuccessful Can still Can still become become pregnantpregnant
surgical surgical procedureprocedure Fibroids can Fibroids can recurrecur
Comparison of treatment options
TreatmentTreatment ProsPros ConsCons
Uterine Uterine Artery Artery
EmbolizationEmbolization
Non-surgical Non-surgical treatmenttreatment Very Very effectiveeffective
Fibroids Fibroids may recurmay recur

Goal

Thanks !
Method Of Delivery
Vertex- Vertex (50%) Vaginal delivery, interval between
twins not to exceed 20 minutes.
Vertex- Breech (20%)
Vaginal delivery by senior obstetrician

Method Of Delivery
Breech- Vertex( 20%)Safer to deliver by CS
Breech-Breech( 10%)Usually by CS.
Method Of Delivery
• MONO-MONO
• By C/S
• Why?

















