UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl) UvA-DARE (Digital Academic Repository) Prevention of gingival trauma Hennequin-Hoenderdos, N.L. Link to publication Citation for published version (APA): Hoenderdos, N. L. (2017). Prevention of gingival trauma: Oral hygiene devices and oral piercings DIDES General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: http://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. Download date: 28 Jun 2018
Transcript
UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Prevention of gingival trauma
Hennequin-Hoenderdos, N.L.
Link to publication
Citation for published version (APA):Hoenderdos, N. L. (2017). Prevention of gingival trauma: Oral hygiene devices and oral piercings DIDES
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: http://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
The eff ect of tapered toothbrush fi laments compared to end-rounded fi laments on dental
plaque, gingivitis and gingival abrasion: a systematic review
and meta-analysis
FCR HoogteijlingNL Hennequin-HoenderdosGA van der WeijdenDE Slot
International Journal of Dental Hygiene 2017 Early view
Chapter 3
44
Abstract
AimThis systematic review was performed to establish the effect of a manual toothbrush with tapered toothbrush filaments (TFTBs) compared to a manual toothbrush with end-rounded toothbrush filaments (ERTB) on clinical parameters of dental plaque, gingivitis and gingival abrasion.
Materials and methodsMEDLINE-PubMed and Cochrane-CENTRAL databases were searched. The inclusion criteria were (randomized) controlled clinical trials, participants ≥18 years and papers evaluating the effect of a TFTB compared to an ERTB. Data were extracted for dental plaque index (PI), bleeding scores (BS), gingival index scores (GI) and gingival abrasion scores (GA). A descriptive analysis and a meta-analysis were performed when appropri-ate.
ResultsAn independent screening of 33 unique papers resulted in seven eligible publications, which included eight comparisons. Meta-analysis did not show a significant difference between TFTB and ERTB with respect to PI scores. The meta-analysis of the GI scores showed a significant mean difference in favour of the TFTB (DiffM=−0.12 [95% CI: −0.17; −0.07]). Of the three comparisons evaluating GA, no differences were found.
ConclusionWith respect to plaque removal, evidence that supports the recommendation for usage of a TFTB over an ERTB is lacking. Regarding GI, there is minimal evidence favouring a TFTB over an ERTB and the clinical relevance of this difference is probably negligible. Therefore, based on the collective evidence emerging from this systematic review, the strength and direction of the recommendation, there appears to be no firm evidence for a dental healthcare professional to advise the use of a TFTB over the use of an ERTB.
Tapered filaments
45
3
Introduction
It is well known that dental plaque on teeth and gingival surfaces eventually leads to gingival inflammation1. Therefore, effective plaque removal is most important for maintaining and improving dental health. Gingivitis can primarily be prevented by the daily use of a toothbrush with an adequate brushing technique. Many variations of manual toothbrushes are currently available on the market with the claim that they are effective for plaque removal and safe for use2. Brush head and filament shapes and even the placement of the filaments in the handle are the subjects of new improve-ments3,4. Ever since the introduction of nylon filaments in the 1930s, much imagination and inventiveness has been applied to toothbrush design. The number and length of filaments in a tuft, the number of tufts and the arrangement of tufts are aspects that may vary with toothbrush filament designs5.Manufacturers claim their own specific specialty in numerous surveys for each new designed toothbrush4. The American Dental Association (ADA) recommends that the toothbrush bristle ends be “free of sharp or jagged edges and endpoints” to minimize gingival and dental abrasions6. Consequently, most manual toothbrushes have conical or end-rounded filaments. The latest development is a manual toothbrush with tapered toothbrush filaments (TFTBs) originally produced by toothbrush manufacturers from Asia. Those manufacturers that produce toothbrushes with tapered filaments claim better plaque removal, which can result in increased gingival health and a decrease in potential gingival tissue trauma compared to toothbrushes with end-rounded filaments. A systematic review evaluating the efficacy of a tapered filament toothbrush (TFTB) on the parameters of dental plaque index scores (PI), gingival health (bleeding scores (BS), gingivitis index (GI)) and gingival abrasion (GA) is currently not available. Thus, the aim of this article was to systematically collect and appraise the scientific evidence that as-sesses the effect of a manual toothbrush with tapered filaments compared to a manual toothbrush with end-rounded filaments on the clinical parameters of plaque, gingivitis and GAs.
Materials and methods
This systematic review was prepared and described in accordance with the Cochrane Handbook7 for Systematic Reviews of Interventions, which provides guidance for the preparations, and the guidelines of Transparent Reporting of Systematic Reviews and Meta-analyses (PRISMA statement)8,9. The protocol that details the review method was developed “a priori” following an initial discussion among the members of the research team.
Chapter 3
46
Focused questionBased on the outcome of Randomized Controlled Clinical Trials (RCT), what is the sum-marized effect of a manual toothbrush with tapered filaments compared to a flat-trim manual toothbrush with end-rounded filaments on the clinical parameters of plaque, gingivitis and gingival abrasion?
Search strategyInternet sources were used to search for appropriate papers that satisfied the study purpose. These sources included the National Library of Medicine, Washington, D.C. (MEDLINE-PubMed) and the Cochrane Central Register of Controlled Trials (CENTRAL). A comprehensive search of the databases was conducted through October 2016 for appropriate studies regarding the focused question. All references cited in the included trials were checked for additional studies. Hand searching was performed as part of the Cochrane Worldwide Hand Searching Programme and uploaded to CENTRAL. Ad-ditionally, the manufacturer of the Meridol toothbrush (GABA/Colgate in Switzerland) was contacted for unpublished data. The structured search strategy was designed to include any relevant published papers that evaluated the adjunctive effect of a manual toothbrush with tapered filaments vs the end-rounded manual toothbrush. For details regarding the search terms used, see Box 1.
box 1. Search strategySearch terms used for PubMed-MEDLINE and Cochrane-CENTRAL are shown. The search strategywas customized according to the database being searched.The following strategy was used in the search:{ (Intervention) AND (Specific characteristics) }{<Toothbrush: [MeSH terms /all subheadings] Toothbrushing OR [textwords] Toothbrush* OR Toothbrush >AND<Filament design: Tapered OR Conical OR (Needle shaped) OR (ultra thin) OR Pointed OR lessened OR narrowed >}The asterisk (*) was used as a truncation symbol.
Screening and selectionTitles and abstracts of studies obtained from the searches were independently screened by two reviewers (FH and DES) and were categorized as definitely eligible, definitely not eligible or questionable. The reviewers were not blinded to names of authors or institutions and journals while making the assessment.
Tapered filaments
47
3
The eligibility criteria were as follows:– RCTs– Papers written in the English language– Studies conducted on humans
• ≥18yearsold
• Ingoodgeneralhealth
• Participantbrushing
– Intervention: a TFTB– Comparison: a ERTB– Evaluation with one or more of the following clinical evaluation parameters: PI, BS,
GI and GA.
If eligible aspects were present in the title, the paper was selected for further reading. If none of these aspects were mentioned in the title, the abstract was read in detail to screen for suitability. Papers that potentially would meet the inclusion criteria were obtained and read in detail by the two reviewers (FH and DES). Disagreements in the screening and selection process concerning eligibility were resolved by consensus or, if disagreement persisted, by arbitration through a third reviewer (GAW). The papers that fulfilled all of the inclusion criteria were processed for data extraction.
Assessment of heterogeneityThe heterogeneity of the primary outcome parameters across studies was detailed according to the following factors:– Study design, research groups and evaluation period– Intervention: type of manual toothbrushes and procedures– Industry funding and side effects
Quality assessmentTwo reviewers (FH and DES) scored the methodological qualities of the included studies according to the method described in detail by Keukenmeester et al. (2013)10 In short, when random allocation, defined eligibility criteria, masking of examiners, masking of patients, balanced experimental groups, identical treatment between groups (except for the intervention) and reporting of follow-up were present, the study was classified as having an estimated low risk of bias. When one of these criteria was missing, the study was considered to have an estimated moderate risk of bias. When two or more of these criteria were missing, the study was estimated to have a high risk of bias, as previously proposed by Van der Weijden et al. (2009)11.
Chapter 3
48
Statistical analysesData extractionThe data from the papers that met selection criteria were extracted and processed for further analysis. Two reviewers (FH and DES) evaluated the selected papers for mean baseline and end trial values and standard deviation (SD). For studies that presented an intermediate outcome assessment, only the baseline and final evaluations were used. Disagreements were resolved by discussion and, if the disagreement persisted, the judgement of a third reviewer (GAW) was decisive.
Data analysisAs a summary, a descriptive data presentation was used for all studies. For studies that had multiple treatment arms and for which data from the control group were com-pared with more than one other group, the number of subjects (n) in the control group was divided by the number of comparisons. The primary variable of interest was PI. The secondary variables were BS, GI and GA. When appropriate, a meta-analysis was per-formed, and the DiffM was calculated using the Review Manager 5.1 software (RevMan version 5.1 for Windows, Copenhagen: The Nordic Cochrane Centre, The Cochrane Col-laboration, 2011). Primarily the random effects model was used to calculate a weighted average of the treatment effects across the studies under review. If fewer than four studies were included, a fixed-effect analysis was used as the estimate of between-study variance7. Heterogeneity was tested by the chi-square test and the I2 statistics.
Grading the body of evidenceThe Grading of Recommendations Assessment, Development and Evaluation system, as proposed by the GRADE working group, was used to rank and grade the evidence emerging from this review12,13. Only for the outcome parameters, for which a meta-analysis was applicable, a GRADE evidence profile was performed. Two reviewers (GAW and DES) rated the quality of the evidence as well as the strength and direction of the recommendations according to the following aspects: risk of bias of the individual studies; consistency and precision among the study outcomes; directness of the study results; and detection of publication bias. Any disagreement between the two review-ers was resolved after additional discussion.
Results
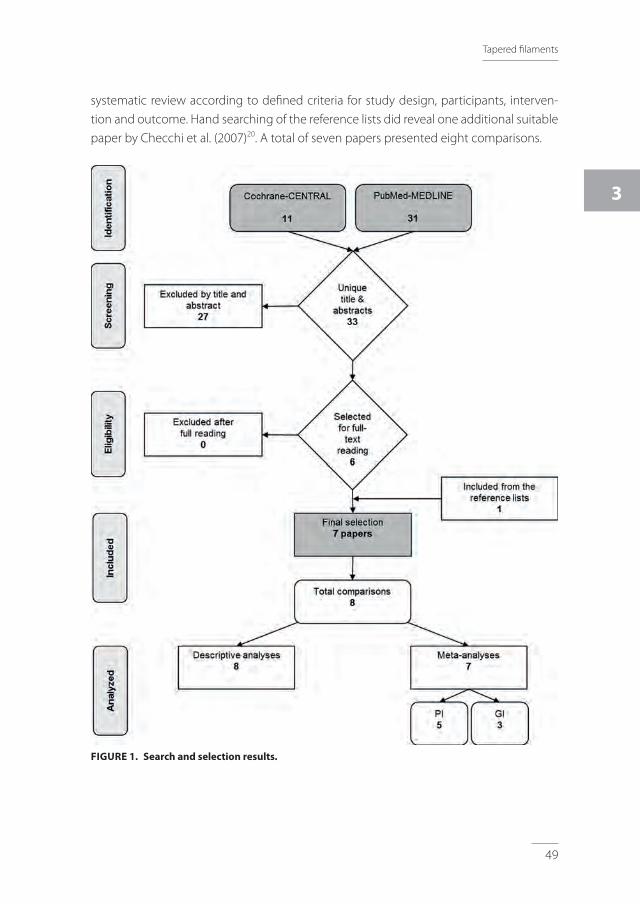
Search & selection resultsThe databases searches resulted in 33 unique papers (for details, see Figure 1). The screen-ing of titles and abstracts resulted in six papers14-19 that were eligible for inclusion in this
Tapered filaments
49
3
systematic review according to defined criteria for study design, participants, interven-tion and outcome. Hand searching of the reference lists did reveal one additional suitable paper by Checchi et al. (2007)20. A total of seven papers presented eight comparisons.
FIGuRe 1. Search and selection results.
Chapter 3
50
TAb
le 1
. O
verv
iew
of t
he in
clud
ed s
tudi
es a
nd c
hara
cter
isti
cs p
roce
ssed
for d
ata
extr
acti
on.
# Aut
hors
(yea
r)
Stud
y de
sign
, du
rati
onbl
indi
ngO
ral p
roph
ylax
is
(OP)
# Pa
rtic
ipan
ts
base
line
(end
)G
ende
rM
ean
age
Age
rang
e in
yea
rs
Gro
ups
(bra
nd)
TFT b
: tap
ered
fila
men
ts to
othb
rush
eRTb
: end
roun
ded
toot
hbru
shTo
othp
aste
Regi
men
:u
se &
inst
ruct
ion
Fund
ing
Conc
lusi
ons
of th
e or
igin
al
auth
ors
I Dör
fer
et a
l. 20
0314
RCT
Split
mou
thSi
ngle
use
Sing
le b
lind
OP:
No
87 (8
7)♀
: 0♂
: 87
(87)
Mea
n ag
e: 2
7Ag
e ra
nge:
18-
63
TFTB
: Mer
idol
GA
BA C
HER
TB: fl
at-t
rim m
anua
l too
thbr
ush
(AD
A
refe
renc
e to
othb
rush
)D
F: S
tand
ard
fluor
ide
dent
ifric
e Bl
end
a m
ed
clas
sic,
Pro
cter
& G
ambl
eFo
r 12-
day
accl
imat
izat
ion
perio
d
12-d
ay a
cclim
atiz
atio
n pe
riod
Brus
h on
alte
rnat
e da
ys w
ith th
e to
othb
rush
esSu
perv
ised
bru
shin
g w
ithou
t DF
30 s
econ
ds p
er q
uadr
ant
Fund
ing:
GA
BA C
H
The
TFTB
was
sta
tistic
ally
m
ore
sign
ifica
nt o
n th
e ov
eral
l pla
que
redu
ctio
n an
d th
e re
mai
ning
pla
que
than
the
ERTB
.
II Sgan
-Coh
enet
al.
2005
15
RCT
Para
llel
60 d
ays
Sing
le b
lind
OP:
Yes
70 (6
8)♀
: 40
♂: 3
0M
ean
age:
36◊
Age
rang
e: ?
TFTB
: Mer
idol
, GA
BA C
HER
TB: fl
at-t
rim m
anua
l too
thbr
ush
(AD
A
refe
renc
e to
othb
rush
)D
F: s
tand
ard
dent
ifric
e
Ora
l pro
phyl
axis
took
pla
ce 7
-10
days
prio
r bas
elin
eBr
ush
2x d
aily
Fund
ing:
GA
BA C
H
Ther
e w
as n
o si
gnifi
cant
di
ffere
nce
betw
een
the
TFTB
and
the
ERTB
.
III Ren
et a
l. 20
0716
RCT
Para
llel
30 d
ays
Sing
le b
lind
OP:
No
? (5
7◊)
♀: 4
8♂
: 42
Mea
n ag
e: 3
3Ag
e ra
nge:
?
TFTB
A: E
SES
Elm
ex s
ensi
tive
extr
a so
ft, G
ABA
CH ER
TB: s
tand
ard
flat-
trim
man
ual t
ooth
brus
h (A
DA
refe
renc
e to
othb
rush
)D
F: S
tand
ard
fluor
ide
dent
ifric
e(C
olga
te C
avity
Pro
tect
ion)
Was
hout
per
iod
of 7
day
sBr
ush
2x d
aily
in u
sual
man
ner
Fund
ing:
Stip
end
from
GA
BA C
H
The
TFTB
was
sig
nific
antly
m
ore
effec
tive
in
rem
ovin
g de
ntal
pla
que
and
redu
cing
gin
giva
l in
flam
mat
ion
inte
rpro
xim
al
than
the
ERTB
.
IV Vers
teeg
et a
l. 20
0817
RCT
Split
-mou
th30
day
sEx
perim
enta
l gi
ngiv
itis
stud
ySi
ngle
blin
dO
P: Y
es
35 (3
2)♀
: 23
♂: 9
Mea
n ag
e: 2
4Ag
e ra
nge:
21-
42
TFTB
: Mer
idol
, GA
BA C
HER
TB: fl
at-t
rim m
anua
l too
thbr
ush
(AD
A
refe
renc
e to
othb
rush
)D
F: S
tand
ard
dent
ifric
e (E
verc
lean
, HEM
A, T
he
Net
herla
nds)
Fam
iliar
izat
ion
phas
e of
14
days
: br
ush
2x d
aily
for 2
min
utes
, “Ba
ss”
met
hod
Trea
tmen
t pha
se: s
plit-
mou
th b
oth
brus
hes
1 m
inut
eFu
ndin
g: G
ABA
CH
Both
toot
hbru
shes
im
prov
ed g
ingi
val h
ealth
an
d eff
ectiv
ely
rem
oved
pl
aque
.
Tapered filaments
51
3
# Aut
hors
(yea
r)
Stud
y de
sign
, du
rati
onbl
indi
ngO
ral p
roph
ylax
is
(OP)
# Pa
rtic
ipan
ts
base
line
(end
)G
ende
rM
ean
age
Age
rang
e in
yea
rs
Gro
ups
(bra
nd)
TFT b
: tap
ered
fila
men
ts to
othb
rush
eRTb
: end
roun
ded
toot
hbru
shTo
othp
aste
Regi
men
:u
se &
inst
ruct
ion
Fund
ing
Conc
lusi
ons
of th
e or
igin
al
auth
ors
V Chec
chi
et a
l. 20
0720
RCT
Para
llel
6 m
onth
sSi
ngle
blin
dO
P: Y
es
30 (3
0)♀
: 15
♂: 1
5M
ean
age:
22◊
Age
rang
e: ?
TFTB
: Mer
idol
, GA
BA C
HER
TB: fl
at-t
rim m
anua
l too
thbr
ush
(AD
A
refe
renc
e to
othb
rush
)D
F: s
tand
ard
toot
hpas
te
No
fam
iliar
izat
ion
phas
eBr
ush
2x d
aily
for 2
min
utes
, “Ba
ss
met
hod”
Fund
ing:
GA
BA C
H
For t
he p
laqu
e in
dex
and
ging
ival
inde
x,
impr
ovem
ent w
as s
how
n in
bot
h gr
oups
, but
mor
e re
leva
nt in
bot
h ta
pere
d te
st g
roup
s.
VI Sgan
-Coh
enet
al.
2008
18
RCT
Para
llel
60 d
ays
Sing
le b
lind
OP:
Yes
120
(107
)♀
: ?♂
: ?M
ean
age:
45◊
Age
rang
e: 3
0-?
TFTB
: ESE
S El
mex
sen
sitiv
e ex
tra
soft
, GA
BA
CH ERTB
: flat
-trim
man
ual t
ooth
brus
h (A
DA
re
fere
nce
toot
hbru
sh)
DF:
Elm
ex s
ensi
tive
toot
hpas
te, G
ABA
CH
Fam
iliar
izat
ion
phas
e of
14
days
Brus
h 2x
dai
ly, n
o or
al h
ygie
ne
inst
ruct
ions
Fund
ing:
GA
BA C
H
For a
ll th
ree
inde
x co
mpo
nent
s (p
laqu
e,
blee
ding
, GI),
the
leve
l at
two
mon
ths
is lo
wer
th
an b
asel
ine
for t
he T
FTB
grou
p.
VII
Capo
ross
i et a
l. 20
1619
RCT
Split
mou
thCr
oss
over
Sing
le u
seSi
ngle
blin
dO
P: Y
es
39 (3
9)♀
: 21
♂: 1
8M
ean
age:
24
Age
rang
e: ?
TFTB
: Col
gate
360
Dee
p Cl
ean,
Sao
Ber
nard
o do
Cam
po, B
razi
lER
TB: O
ral-B
Indi
cato
r Plu
s, si
ze 3
5, G
ross
-G
erau
, Ger
man
yD
F: O
ral -
B pr
o Sa
ude,
Pro
cter
& G
ambl
e,
Gro
ss-G
erau
, Ger
man
y
Fam
iliar
izat
ion
phas
e of
10
days
: on
alte
rnat
e da
ys w
ith th
e to
othb
rush
esbr
ush
2x d
aily
“Bas
s m
etho
d”Br
ush:
sin
gle
use,
30
seco
nds
per
quad
rant
Fund
ing:
?
End
roun
ded
bris
tles
rem
oved
pla
que
mor
e eff
ectiv
ely
with
out c
ausi
ng
a hi
gher
inci
denc
e of
gi
ngiv
al a
bras
ion
whe
n co
mpa
red
with
tape
red
bris
tles.
ERTB
, end
-rou
nded
toot
hbru
sh; T
FTB,
tape
red
filam
ent t
ooth
brus
h; D
F, de
ntifr
ice;
♀, f
emal
e; ♂
, mal
e; N
A, n
ot a
pplic
able
; OP,
oral
pro
phyl
axis
; ◊, c
alcu
late
d by
the
auth
ors
of th
is re
view
bas
ed o
n th
e pr
esen
ted
data
in th
e se
lect
ed p
aper
.
Chapter 3
52
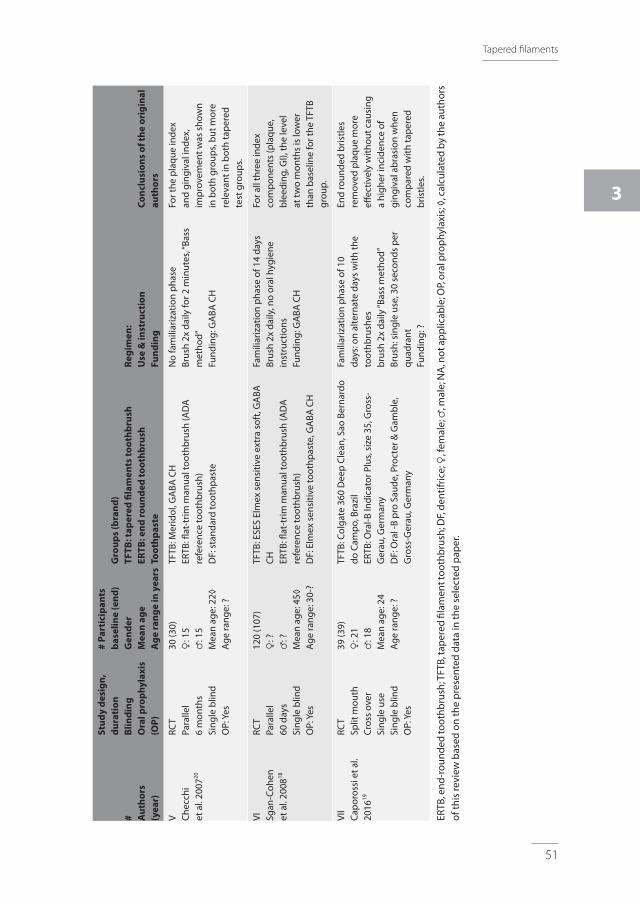
Assessment of heterogeneityConsiderable heterogeneity was observed in the seven clinical trials with respect to study design, evaluation period, study population, number, gender and age of partici-pants. Information regarding the study characteristics is displayed in detail in Table 1. Various clinical indices and their modifications were used.
Study design, research groups and evaluation periodAll included studies were RCTs. Six studies used a parallel design (I, II, III, IV, V and VI), of which one used an experimental gingivitis model (IV). Three studies used a split-mouth design (studies I, IV and VII) of which one (VII) used a cross over design. The approximate mean age of the included participants was 30 years. All the studies excluded participants with periodontitis. In study I, no females were included. The evaluation period varied from single use (I and VII), 30 days (III and IV), 60 days (II and VI) and 6 months (V). Procedures for allocation concealment were not described in any of the selected studies with the excep-tion of study IV. Masking (blinding) of the examiner was described in all studies. Blinding of the participant is difficult as the filament design is visible for participants. Nevertheless, one study (VI) mentioned double-blinding. In this study and study III, participants were not informed if they were assigned a test or control toothbrush.
Intervention: type of manual toothbrush and proceduresStudies mentioned a washout period of 7 days (III), a familiarization phase of 10 days (VII) or 14 days (IV and VI) or an acclimatization period of 12 days (I) prior baseline measurements. Five studies (II, IV, V, VI and VII) provided oral prophylaxis before the start of the study. A period of non-brushing before measurements was reported: 2-3 hours (IV), 48 hours (I), ≥12 hours (II and III, VI) and 72 hours (VII). In one study, it was unclear how many hours participants brushed prior the measurements (V). All papers that were identified, used toothbrushes from one and the same manufacturer (Colgate-GABA) however under different brands names. For details, see Table 1. In all studies, par-ticipants brushed with dentifrice during the course of the study. One study mentioned that no dentifrice was used during the brushing procedure (I). Another study used a split-mouth design to brush with dentifrice or water with both toothbrushes (VII).
Industry funding & side effectsAll but one (VII) of the selected studies were supported by GABA International, which is now part of Colgate Palmolive. Further details explaining what this support implied were not given. All authors were affiliated academics, although only one (VII) mentioned disclosure or statement of any conflict of (financial) interest. The majority of papers did not report any adverse events during the follow-up period. However, Dörfer et al. (2003) (I) observed one case in which, after toothbrushing, a small GA was observed on the
Tapered filaments
53
3
palatal mucosa between the two middle incisors (papilla incisiva). It was not possible for these authors to determine which brush, TFTB or end-rounded toothbrush filaments (ERTB), caused the abrasion.
Quality assessmentThe quality assessment items, including external, internal and statistical validity are presented in the Appendix S1. Based on a summary of these criteria, the estimated potential risk of bias is low in all studies. Because less than 10 studies were included in the meta-analysis7 ,the formal testing for publication bias that was proposed by Egger et al. (1997)21 could not be used owing to insufficient statistical power.
Results of study outcomesThe Appendix S2 (a-d) shows the results from the data extraction. In the current review, different indices and their modifications were used. Information regarding the changes within each intervention group for the various indices was also presented.
Between groupsTable 2 presents the descriptive analysis. In general, the overall descriptive analyses for PI showed three comparisons in favour of the TFTB and three in favour of the ERTB. Two comparisons resulted in no difference. Regarding GI, two of three experiments showed a positive significant effect towards the TFTB. For BS, one comparison showed a significant effect for the ERTB and one comparison found no difference between the two toothbrushes. The three comparisons (17, 2×19) that evaluated the parameter of GA showed that there is no difference between the TFTB and the ERTB. One experiment also evaluated the effect of both toothbrushes with and without dentifrice. No differ-ence in the incidence of GA was detected between the toothbrushes when used with dentifrice nor with water.
Meta-analysisOnly the available data for PI by the use of the Quigley & Hein22 and GI by Löe & Sillness23 were amenable to meta-analysis (MA). Some studies could not be included in the MA due to the use of incompatible indices. None of the MA at baseline showed a significant difference between the groups (Appendix S3 a & b). Table 3 shows the MA for outcome measures as end scores and reveals a significant effect favouring the use of the TFTB for GI23 (difference in means, DiffM=−0.12; P=.00001; 95% CI:[ −0.17; −0,07]. No significant difference between TFTB and ERTB on PI22 was observed (DiffM=0.10; P=0.41; 95% CI:[ −0.13,0.32].
Chapter 3
54
TAble 2. A descriptive summary of the comparison and intervention indicating whether there is a significant difference post-brushing between the intervention and comparison.
Study # Intervention PI GI bS GA Comparison
IDörfer et al. 200314
TFTB + no DF O o o o ERTB + no DF
IISgan-Cohen et al. 200515
TFTB + DF O O O o ERTB + DF
IIIRen et al. 200716
TFTB-ES + DF + + o o ERTB + DF
IVVersteeg et al. 200817
TFTB + DF - o - O ERTB + DF
VChecchi et al. 200720
TFTB + DF + + o o ERTB + DF
VISgan-Cohen et al. 200818
TFTB-ES + DF + o o o ERTB + DF
VIICaporossi et al. 201619
TFTB + DF - o o O ERTB + DF
TFTB + water - o o O ERTB + water
PI, plaque index; GI; gingival index; GA, gingival abrasion; ERTB, end-rounded toothbrush; TFTB, tapered filament toothbrush; TFTB-ES, tapered filament toothbrush extra soft; O, no difference; +, significant differ-ence in favour of intervention; −, significant difference in favour of comparison; o, no data available; DF, dentifrice.
TAble 3. Meta-analysis for the end scores of the primary outcome parameters of interest (PI and GI).
Index StudiesMeasure-ment Model DiffM
Test for overallTest for heterogeneity
95% CI p-value I2 value (%)
p-value
PI I Dörfer 200314
III Ren 200716
IV Versteeg 200817
VII Caporossi et al. 2016(2x)19
Baseline Random 0.02 [-0.08; 0.11] 0.73 0% 1.00
End Random 0.10 [-0.13; 0.32] 0.41 85% <0.0001
Difference Random 0.07 [-0.18; 0.32] 0.59 89% <0.00001
A chi-square test resulting in a P<.1 was considered an indication of significant statistical heterogeneity. As a rough guide for assessing the possible magnitude of inconsistency across studies, I2 statistic of 0%-40% was interpreted as not to be imperative, and above 40% indicated that moderate to considerable hetero-geneity was most likely present.
Evidence profileTable 4 shows a summary of the various factors used to rate the quality of evidence and strength and direction of recommendations according to GRADE12,13 including the level of certainty24. A meta-analysis could be performed only for Pl and Gl, and consequently,
Tapered filaments
55
3
an evidence profile was created. The TFTB studies that were evaluated were from one manufacturer only, which may introduce a publication bias. With respect to PI scores, the strength of the underlying evidence was estimated to be low. Given that the meta-analysis provides no evidence supporting that the TFTB removes dental plaque better than an ERTB, the direction of the recommendation is that currently, no preference for the TFTB over the ERTB is evident. Concerning the data for the gingival index (GI), the strength of the underlying evidence is moderate. With a small clinical benefit, the direction of the recommendation was therefore weak in favour of the TFTB for reducing gingivitis.
TAble 4. GRADe evidence profile for impact of the use of a tapered filament toothbrush in com-parison with an end-rounded toothbrush on plaque scores and gingival inflammation from the pre-sented systematic review and meta-analysis.
GRADe Plaque index Gingival index
Study design RCT RCT
Studies #Comparisons #
45
33
Risk of bias Low Low
Consistency Inconsistent Consistent
Directness Generalizable Generalizable
Precision Rather imprecise Precise
Publication bias Possible Possible
level of certainty24 Low Moderate
Magnitude of the effect No difference Small
Direction of the recommendation Expert opinion not favouring TFTB over ERTB
Weak certainty favouring TFTB over ERTB
Discussion
Summary of main findingsThis systematic review aimed to determine the clinical efficacy of manual tooth-brushes with different filament designs. Tapered filaments have endings in the shape of an extreme rotational ellipsoid as opposed to end-rounded filaments shaped like a hemisphere. Tapered toothbrushes are processed by chemical agents and not by a grinding machine24. The performance differs from a cylindrical filament in how it bends in response to the load and deflection. A cylindrical filament bends like a beam with little deflection until the load surpasses the cross-sectional strength of the filament. The clinical studies that emerged from the search evaluated the effect of a TFTB and an ERTB on the parameters plaque and gingivitis. A meta-analysis was performed on PI22 and GI23 which showed a statistically significant effect in favour of the TFTB on GI.
Chapter 3
56
The aim of this study was to systematically collect and appraise the scientific evidence that assesses the effect of a manual toothbrush with tapered filaments compared to a manual toothbrush with end-rounded filaments on the clinical parameters of plaque, gingivitis and GAs. The hypothesis that the use of a manual toothbrush with tapered filaments provides better results than a manual toothbrush with end-rounded fila-ments could not be accepted. The analyses of the current available studies included in this systematic review did not result a thorough conclusion concerning the effects of TFTBs or ERTB.
Strength of evidence for outcomesThe discrepancy between the findings in descriptive summary (Table 2) and the results of the meta-analysis (Table 3) may be clarified by the origin of the analysis itself. The fact that the meta-analysis restricted to the Quigley & Hein22 PI and the Löe & Silness23 GI. While the descriptive analysis is irrespective of the index used in the original study may be of influence. All eight included study comparisons that evaluated dental plaque are presented in the descriptive analysis but only five comparisons could be used in the meta-analysis. All three comparisons evaluating the GI were used in both analysis and are in line with each other. Dental healthcare professionals can advise their patients a toothbrush with TF which is effective in plaque removal and has a small benefit with respect to gingival inflammation over a toothbrush with end-rounded cylindrical fila-ments.
In vitro studiesEspecially for areas that are difficult to access, the filament and bristle design can be important in relation to the efficacy of the toothbrush25. Several in vitro studies have specifically evaluated the efficacy of tapered filaments. In one study, the TFTB was compared with an ADA-referenced brush on artificial plaque removal at the gingival margin and the subgingival area26. The TFTB was found to be more effective. Another in vitro study concluded that a TB with filaments at two different levels with the TF at the high level resulted in a significantly improved removal of the artificial plaque from the interproximal areas27. TF also appear to have an advantage for reaching into the occlusal fissure compared to ER28. All these in vitro findings considered together are in support of the clinical data with respect to TF, although none of the included clinical studies made a separation of scores related to the gingival margin or the approximal areas.
End roundingWith cylindrical filaments, end-rounding is an issue. Using scanning electron micros-copy, a recent evaluation of children’s toothbrushes showed that the percentage
Tapered filaments
57
3
of acceptable end-rounded bristles ranged from 1.4% to 20.2%29. Therefore, these toothbrushes labelled as end-rounded had the potential to harm oral tissue. Their study demonstrated that quality control for the rounding of bristle ends as well as for the labelling of end-rounded bristles is needed. We recently demonstrated that fila-ments that are not end rounded are more abrasive than partially or fully end-rounded filaments30. In the past, we have also shown that the form of end-rounding had an effect on toothbrush abrasivity. The dome-shaped end-rounding was significantly less abrasive than the pointed type of end-rounding31.Tapered filaments have a cross section that varies along its length with very thin endings. Additionally, these filaments have good stability of the filament corpus14. As a result, more flexibility is introduced in the filaments, which are presumably less harmful14,17. For the present study, only three experiments emerged that assessed GA in relation to TFTBs. One study observed that in comparison to an end-rounded ADA-referenced toothbrush, usage of the TFTB resulted in a tendency towards fewer sites with GA (IV). The other comparison did also not find a statistical difference. The latter was a study with as primary outcome focussed on GA as based on an “a priori” sample size calculation but could not find a difference.
Post-surgical hygiene care and safety for daily useTwo studies recently evaluated the use of a TFTB for post-surgical care compared to the use of an ERTB. Each patient received the assigned toothbrush after periodontal surgery32 or after extraction of a wisdom tooth33. The TFTB showed no adverse effects during wound closure and was preferred by the patients over the ERTB. In the stud-ies included in the present review, patient preference was only described in two of the included studies (II and IV). A higher score was given for “pleasant in use” by those participants using the TFTB. The exact reasons for this preference were not specified in the papers. Because a toothbrush has value in particular if the patient is prepared to use it on a regular basis34, it is important that the patient is satisfied with the recom-mended toothbrush. This will have a positive impact on compliance to oral self-care recommendations.
FundingFor this systematic review, the possibility of publication bias cannot be ruled out because studies were supported or funded by one manufacturer (GABA CH, currently owned by Colgate Palmolive). All participants from all studies used a tapered toothbrush that originated from the same manufacturer. As the funding source is not definitive evidence of bias, it is an indication that for instance reporting bias may exist. Analyses of the methodology of the studies, interpretation of the data and comparison of the products studied can, up to some point, help resolve whether a funding effect exists35.
Chapter 3
58
Although different study models were used, subanalysis of the data showed that this had no impact on the outcome of the meta-analysis. Additionally, it is relevant to know that the included studies were initiated by the investigator, which limits the influence of the commercial party. The included studies applied internationally agreed models and standards of study design, analysis and reporting and were, therefore, deemed important to accommodate in the systematic review.
Limitations– Blinding of the participant is hardly possible as the filament design being either
tapered or end-rounded is clearly visible. Nevertheless, one study (VI) in this SR reported double-blinding which is interpreted by these authors as not informing the participants whether they were assigned to a test or control toothbrush.
– Although all being categorized as tapered, different TFTB brands were used in the included studies with different toothbrush characteristics, such as extra soft cross-angled filaments (III and VI) and a toothbrush with a raised cleaning tip and soft rubber polishing cups that are made of a synthetic thermoplastic elastomer (VII).
– Brushing duration can influence the efficacy of plaque removal36. This factor was not standardized in all included studies.
– There is cumulative evidence demonstrating that there is moderate certainty that toothbrushing with a dentifrice does not provide an added effect for the mechani-cal removal of dental plaque37. The majority of the comparisons used a dentifrice. One experiment (VII) also evaluated the effect of both test and control toothbrushes with and without dentifrice. Although no difference in the incidence of GA was detected between the toothbrushes, the use of dentifrice resulted in an increase of marginal GA, irrespective of the toothbrush.
Implications for future researchRecently, the new ADA guideline6 on toothbrushes was published, for the design and conduct of clinical studies using manual toothbrushes to provide evidence on safety and effectiveness in reducing gingivitis and removing plaque. Only one (II) of included papers did comply with these guidelines. The majority of the included studies did not fulfil the criteria for instance a minimum of 30 participants per product group and safety assessments that should be continued for a total of 90 days. If researchers are willing to design and conduct a clinical study investigating the safety and effectiveness of manual toothbrushes, it is recommended to adhere to the ADA guidelines. This could improve the quality of individual studies and makes a comparison such as this SR possible. If more studies can be included in SRs and MAs, the level of certainty could be increased.
Tapered filaments
59
3
Conclusion
With respect to plaque removal, evidence was not conclusive to recommend the TFTB over an ERTB. Regarding GI, a small effect in favour of a TFTB was noted, the clinical relevance of this difference is probably negligible. Therefore, based on the collective evidence emerging from this systematic review, the strength and direction of the recommendation there appears to be no firm evidence for a dental healthcare profes-sional to advise the use of a TFTB over the use of an ERTB.
Clinical relevance
Scientific rationale for the studyManual toothbrushes with TFTB are available on the market. Manufacturers claim that TFTBs have better plaque removal capabilities, which can result in lower bleeding scores and gingival index scores.
Principal findingsNo significant difference in plaque scores was found, while the gingival index scores showed a significant positive effect with unknown clinical relevance.
Practical ImplicationsThe results are applicable for dental healthcare professionals. There is no firm evidence to advise the use of a TFTB over the use of an ERTB.
LimitationThe evaluated TFTBs are from one manufacturer, which might have introduced bias.
Acknowlegdements
The authors of this review are grateful to the following authors for their response, time and effort to search for additional data: Professor Dörfer, Dr. Checchi, Professor Ren, Dr. Rosema and Professor Sgan-Cohen. This article was initiated as a part of the obliga-tion of the first author to fulfil the requirements of the AMC/UvA master’s programme in Evidence-Based Practice; therefore, Erik Bakker is kindly acknowledged for his help preparing the protocol.
Chapter 3
60
Conflict of interest
The authors declare that they have no conflict of interests. For this study, no funding was accepted, except for support from the listed institutions. Ethical approval was not required. Van der Weijden, Slot and their research team at ACTA have previously received either external advisor fees, lecturer fees or research grants from toothbrush and dentifrice manufacturers. Those manufacturers included Colgate, Dentaid, GABA, Lactona, Oral-B, Procter & Gamble, Sara Lee, Sunstar and Unilever.
Tapered filaments
61
3
References
* = included publications in this systematic review
1. Löe H, Theilade E, Jensen SB. Experimental gingivitis in man. J Periodontol. 1965;36:177–187.
2. Van der Weijden GA, Timmerman MF, Danser MM, Van der Velden U. Relationship between the plaque
removal efficacy of a manual toothbrush and brushing force. J Clin Periodontol. 1998;25:413–416.
3. Barnes CM, Covey DA, Shi X, Yankell SL. Laboratory evaluations of a bi-level, extremely tapered bristled
toothbrush and a conventional uniform bristled toothbrush. Am J Dent. 2009;22:84–88.
4. Rosema NA, Timmerman MF, Versteeg PA, Van Palenstein Helderman WH, Van der Velden U, Van der
Weijden GA. Safety and efficacy of two manual toothbrushes. Int J Dent Hyg. 2010;8:280–285.
5. Van der Weijden FA, Slot DE. Efficacy of homecare regimens for mechanical plaque removal in manag-
ing gingivitis a meta review. J Clin Periodontol. 2015;42(Suppl 16):S77–91.
6. American Dental Association (ADA), Council on Scientific Affairs, Acceptance Program Require-
ments; Toothbrushes (2016). Available from: http://www.ada.org/~/media/ADA/Science%20and%20
Research/Files/guide_toothbrushes.pdf?la=en. Accessed November 9, 2016.
7. Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version
5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from cochrane-handbook.
org. Accessed November 9, 2016.
8. PRISMA statement. Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Checklist
2009. Available from: http://www.prisma-statement.org/. Accessed November 9, 2016.
9. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-
analyses: the PRISMA statement. J Clin Epidemiol. 2009;62:1006–1012.
10. Keukenmeester RS, Slot DE, Putt M, Van der Weijden GA. The effect of sugar-free chewing gum
on plaque and clinical parameters of gingival inflammation: a systematic review. Int J Dent Hyg.
2013;11:2–14.
11. Van der Weijden F, Dell’Acqua F, Slot DE. Alveolar bone dimensional changes of post-extraction
sockets in humans: a systematic review. J Clin Periodontol. 2009;36:1048–1058.
12. GRADE Working Group. Grading of Recommendations Assessment, Development and Evaluation
(GRADE) Working Group. Available from: http://www.gradeworkinggroup.org/. Accessed November
9, 2016.
13. Guyatt GH, Oxman AD, Kunz R, et al. Incorporating considerations of resources use into grading
recommendations. BMJ. 2008;336:1170–1173.
14. *Dörfer CE, von Bethlenfalvy ER, Kugel B, Pioch T. Cleaning efficacy of a manual toothbrush with
tapered filaments. Oral Health Prev Dent. 2003;1:111–8 (Study ID:I).
15. *Sgan-Cohen Vered Y. A clinical trial of the meridol toothbrush with conical filaments: evaluation of
Each aspect of the score list was given a rating of ‘+’ for an informative description of the item at hand and a study design meeting the quality standard, ‘-’ for an informative description without a study design that met the quality standard and ‘?’ for missing or insufficient information. When random allocation, defined eligibility criteria, blinding of examiners and patients, balanced experimental groups, identical treatment between groups (except for intervention) and report of follow-up were present, the study was classified as having a low risk of bias. When one of these seven criteria was missing, the study was considered to have a moderate potential risk of bias. When two or more of these criteria were missing, the study was considered to have a high potential risk of bias, as proposed by Van der Weijden et al. (2009).+, Yes; -, No; ?, unknown / not reported; ◊, calculated by the authors of this review based on the presented data in the selected paper; *, reporting criteria for estimation the potential risk of bias; NA, not applicable
Tapered filaments
65
3
APP
eND
Ix S
2 (a
-d).
Ove
rvie
w o
f clin
ical
out
com
es o
f the
sel
ecte
d st
udie
s an
d pa
ram
eter
s of
inte
rest
wit
h va
riou
s in
dice
s an
d th
eir
mod
ifica
tion
s ar
e sh
own.
bas
elin
e, e
nd a
nd
incr
emen
tal d
ata
are
pres
ente
d as
the
mea
ns a
nd s
tand
ard
devi
atio
ns (S
D) i
n pa
rent
hese
s. S
tati
stic
ally
sig
nific
ant c
hang
es w
ithi
n gr
oups
are
pre
sent
ed.
A.
PlA
Qu
e In
dex
Scor
es (P
I)
#Pl
aque
Inde
x Sc
ores
Gro
ups
Mea
n (S
D)
Sign
ifica
nt
wit
hin
grou
psba
selin
een
dD
iffer
ence
I Dör
fer e
t al.
2003
14Tu
resk
y-G
ilmor
e-G
lickm
an (1
970)
mod
ifica
tion
of th
e Q
uigl
ey a
nd H
ein
plaq
ue in
dex
(196
2)TF
TB +
no
DF
ERTB
+ n
o D
F1.
95 (0
.48)
1.93
(0.5
1)1.
02 (0
.41)
1.09
(0.4
4)-0
.93
(0.4
1)-0
.84
(0.3
7)Ye
sYe
s
III Ren
et a
l. 20
0716
Ture
sky-
Gilm
ore-
Glic
kman
(197
0) m
odifi
catio
n of
the
Qui
gley
and
Hei
n pl
aque
inde
x (1
962)
TFTB
-ES
+ D
FER
TB +
DF
2.43
(0.5
6)2.
41 (0
.53)
2.10
(0.4
2)2.
42 (0
.53)
-0.3
3 (0
.27)
♦+0
.01
(0.3
0)♦
No
No
IV Vers
teeg
et a
l. 20
0817
Mod
ified
Qui
gley
& H
ein
Inde
x (1
962)
TFTB
+ D
FER
TB +
DF
1.86
(0.5
6)1.
87 (0
.53)
1.62
(0.4
5)1.
33 (0
.45)
-0.2
3 (0
.60)
♦-0
.54
(0.5
6) ♦
Yes
Yes
VII
Capo
ross
i et a
l.20
1619
Qui
gley
& H
ein
Inde
x (1
962)
TFTB
+ D
FER
TB +
DF
3.06
(0.4
5)3.
04 (0
.45)
1.43
(0.6
1) ♦
1.12
(0.3
4) ♦
-1.6
3 (0
.50)
-1.9
2 (0
.51)
Yes
Yes
TFTB
+ w
ater
ERTB
+ w
ater
3.11
(0.5
7)3.
09 (0
.56)
1.52
(0.5
3) ♦
1.25
(0.4
4) ♦
-1.5
9 (0
.45)
-1.8
4 (0
.54)
Yes
Yes
II Sgan
-Coh
en e
t al.
2005
15Pa
tient
Hyg
iene
Per
form
ance
(PH
P) In
dex
of
Pods
hadl
ey a
nd H
aley
TFTB
+ D
FER
TB +
DF
TFTB
+ D
FER
TB +
DF
Pre
brus
hing
Ba
selin
e:0.
75 (0
.22)
0.81
(0.1
5)60
day
s:0.
75 (0
.26)
0.85
(0.2
0)
Post
bru
shin
gBa
selin
e:0.
56 (0
.25)
0.63
(0.1
7)60
day
s:0.
44 (0
.23)
0.47
(0.2
7)
-0.1
9 ◊
-0.1
8 ◊
-0.3
1 ◊
-0.3
8 ◊
No
No
Yes
Yes
VI Sgan
-Coh
en e
t al.
2008
18Re
fined
Nav
y Pl
aque
Inde
x, m
odifi
ed b
y Ru
stog
i (19
92)
TFTB
-ES
+ D
FER
TB +
DF
4.52
(1.2
6)4.
56 (1
.19)
2.83
(1.4
6)3.
79 (1
.45)
? ?? ?
V Chec
chi e
t al.
2007
20O
’Lea
ry T
J, Th
e pl
aque
con
trol
reco
rd (1
972)
TFTB
+ D
FER
TB +
DF
68.5
3 (1
9.44
◊)72
.47
(16.
92◊)
37.4
0 (1
1.70
◊)51
.33
(15.
68◊)
-31.
13 ◊
-21.
14 ◊
Yes
Yes
Chapter 3
66
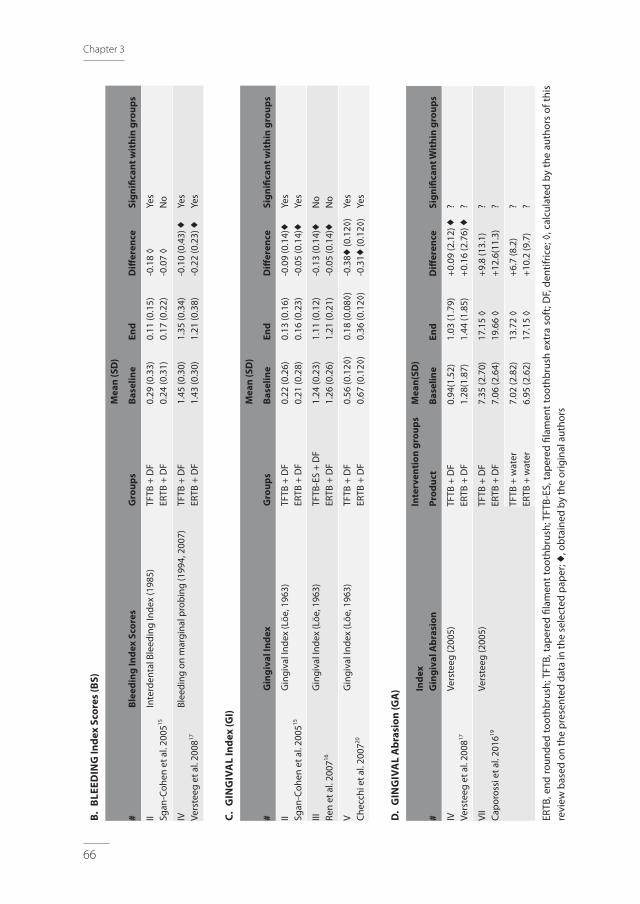
b. b
leeD
ING
Inde
x Sc
ores
(bS)
#bl
eedi
ng In
dex
Scor
esG
roup
s
Mea
n (S
D)
Sign
ifica
nt w
ithi
n gr
oups
base
line
end
Diff
eren
ce
II Sgan
-Coh
en e
t al.
2005
15In
terd
enta
l Ble
edin
g In
dex
(198
5)TF
TB +
DF
ERTB
+ D
F0.
29 (0
.33)
0.24
(0.3
1)0.
11 (0
.15)
0.17
(0.2
2)-0
.18
◊-0
.07
◊Ye
sN
o
IV Vers
teeg
et a
l. 20
0817
Blee
ding
on
mar
gina
l pro
bing
(199
4, 2
007)
TFTB
+ D
FER
TB +
DF
1.45
(0.3
0)1.
43 (0
.30)
1.35
(0.3
4)1.
21 (0
.38)
-0.1
0 (0
.43)
♦-0
.22
(0.2
3) ♦
Yes
Yes
C. G
ING
IVA
l In
dex
(GI)
#G
ingi
val I
ndex
Gro
ups
Mea
n (S
D)
Sign
ifica
nt w
ithi
n gr
oups
base
line
end
Diff
eren
ce
II Sgan
-Coh
en e
t al.
2005
15G
ingi
val I
ndex
(Löe
, 196
3)TF
TB +
DF
ERTB
+ D
F0.
22 (0
.26)
0.21
(0.2
8)0.
13 (0
.16)
0.16
(0.2
3)-0
.09
(0.1
4)♦
-0.0
5 (0
.14)
♦Ye
sYe
s
III Ren
et a
l. 20
0716
Gin
giva
l Ind
ex (L
öe, 1
963)
TFTB
-ES
+ D
FER
TB +
DF
1.24
(0.2
3)1.
26 (0
.26)
1.11
(0.1
2)1.
21 (0
.21)
-0.1
3 (0
.14)
♦-0
.05
(0.1
4)♦
No
No
V Chec
chi e
t al.
2007
20G
ingi
val I
ndex
(Löe
, 196
3)TF
TB +
DF
ERTB
+ D
F0.
56 (0
.12◊
)0.
67 (0
.12◊
)0.
18 (0
.08◊
)0.
36 (0
.12◊
)-0
.38♦
(0.1
2◊)
-0.3
1♦ (0
.12◊
)Ye
sYe
s
D.
GIN
GIV
Al
Abr
asio
n (G
A)
#In
dex
Gin
giva
l Abr
asio
n
Inte
rven
tion
gro
ups
Mea
n(SD
)
Sign
ifica
nt W
ithi
n gr
oups
Prod
uct
base
line
end
Diff
eren
ce
IV Vers
teeg
et a
l. 20
0817
Vers
teeg
(200
5)TF
TB +
DF
ERTB
+ D
F0.
94(1
.52)
1.28
(1.8
7)1.
03 (1
.79)
1.44
(1.8
5)+0
.09
(2.1
2) ♦
+0.1
6 (2
.76)
♦? ?
VII
Capo
ross
i et a
l. 20
1619
Vers
teeg
(200
5)TF
TB +
DF
ERTB
+ D
F7.
35 (2
.70)
7.06
(2.6
4)17
.15
◊19
.66
◊+9
.8 (1
3.1)
+12.
6(11
.3)
? ?
TFTB
+ w
ater
ERTB
+ w
ater
7.02
(2.8
2)6.
95 (2
.62)
13.7
2 ◊
17.1
5 ◊
+6.7
(8.2
)+1
0.2
(9.7
)? ?
ERTB
, end
roun
ded
toot
hbru
sh; T
FTB,
tape
red
filam
ent t
ooth
brus
h; T
FTB-
ES, t
aper
ed fi
lam
ent t
ooth
brus
h ex
tra
soft
; DF,
dent
ifric
e; ◊
, cal
cula
ted
by th
e au
thor
s of
this
re
view
bas
ed o
n th
e pr
esen
ted
data
in th
e se
lect
ed p
aper
; ♦, o
btai
ned
by th
e or
igin
al a
utho
rs
Tapered filaments
67
3
APPeNDIx S3 (a & b). Forrest Plots of the performed meta-analysis.
A. PlAQue Index ScoresBaseline
End
Difference
Chapter 3
68
b. GINGIVAl Index ScoreBaseline
End
Difference
Tapered filaments
69
3
APPeNDIx S4. list of abbreviations.
list of abbreviations Abbreviation Meaning
TFTb Tapered filament toothbrush
eRTb End rounded filament toothbrush
FH Fenne Hoogteijling, first author of this paper
DeS Dagmar Else Slot, co-author of this paper
DiffM Difference of means
GAW Godefridus August van der Weijden, co-author of this paper
SD Standard deviation
Se Standard error
SR Systematic review
MA Meta-analysis
RCT Randomized controlled clinical trial
PI Plaque index scores
Tb Toothbrush
Q&H Quigley and Hein plaque index
WM Weighted mean (percentage)
DF Dentifrice
APPeNDIx S5. References used in the appendices.
– American Dental Association (ADA). Council on Scientific Affairs, Acceptance Program Require-
ments; Toothbrushes. 2016 Available from: http://www.ada.org/~/media/ADA/Science%20and%20
Research/Files/guide_toothbrushes.pdf?la=en (accessed 27 October 2016).
– O’Leary TJ, Drake RB, Naylor JE. The plaque control record. Journal of Periodontology: 1972; 43, 38.
– Podshadley AG, Haley JV. A method for evaluating oral hygiene performance. Public Health Rep 1968;
83: 259-264.
– Rustogi KN, Curtis JP, Volpe AR, Kemp JH, McCool JJ, Korn LR: Refinement of the modified Navy Plaque
Index to increase plaque scoring efficiency in gumline and interproximal tooth areas. J Clin Dent 3
1992; (Suppl. C): C9-C12.
– Turesky S, Gilmore ND, Glickman I. Reduced plaque formation by the chloromethyl analotue of
Vitamine C. J Clin Periodontol 1970; 41: 41-43.
– Versteeg PA, Timmerman MF, Rosema NAM, Warren PR, Van der Velden U, Van der Weijden GA. Sonic-
powered toothbrushes and reversal of experimental gingivitis. J Clin Periodontol 2005; 32: 1236-1241.
– Van der Weijden GA, Timmerman MF, Reijerse E, Nijboer A, Van der Velden U. Comparison of different
approaches to assess bleeding on probing as indicators of gingivitis. J Clin Periodontol. 1994; 21: