33
Uveitis Investigations
| Date post: | 27-Jan-2017 |
| Category: |
Education |
| Upload: | pratik-mohod |
| View: | 115 times |
| Download: | 0 times |

Uveitis Investigations


IUSG Clinical Classification of Uveitis**
InfectiousBacterialViralFungalParasiticOthers
Non-infectiousKnown systemic associationNo known systemic association
MasqueradeNeoplasticNon-neoplastic
**Deschenes J, Murray PI, Rao NA, Nussenblatt RB. International Uveitis Study Group. International Uveitis Study Group (IUSG): clinical classification of uveitis. Ocul Immunol Inflamm 2008;16:1-2.
• Regardless of the choice of laboratory tests, a thorough history and physical examination are essential as it may give you a clue to the underlying disease.
• Many systemic manifestations may either precede or appear much later that the uveitic episode.

Ocular investigation Anterior Uveitis
• Circumcorneal congestion

Keratic precipitates
• Deposits of corneal endothelium composed of inflammatory cells
• Types A)Mutton fat KPs-Granulomaous iridocyclitisB)Small and medium KPs –Non granulomatousC)Fine (Stellate) –Fuch’s heterochromic
iridocyclitis ,herpetic irities D)Old KPs –Healed uveitis
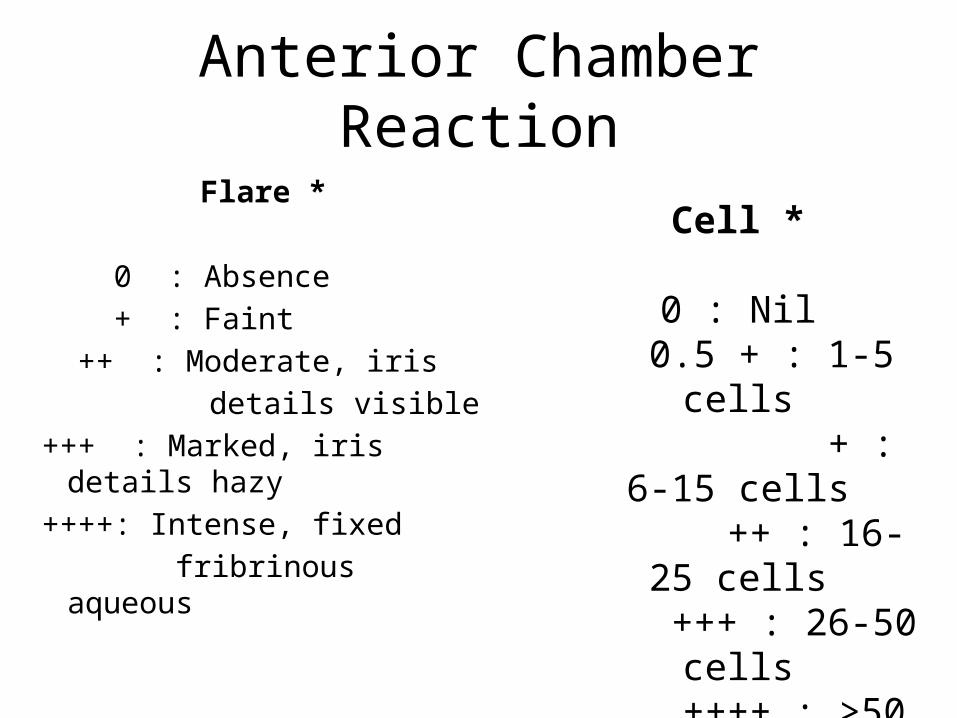
Anterior Chamber Reaction
Flare *
0 : Absence + : Faint ++ : Moderate, iris details visible+++ : Marked, iris
details hazy++++: Intense, fixed
fribrinous aqueous
Cell *
0 : Nil 0.5 + : 1-5 cells
+ : 6-15 cells
++ : 16-25 cells
+++ : 26-50 cells
++++ : >50 cells

Iris Nodules
• Koeppe Nodule Busacca Nodules

Posterior synechiae
Early synechiae formation in active acute anterior uveitis; (B) extensive synechiae andpigment on the lens following a severe attack of acute anterior uveitis
Lens
• Many patients with uveitis develop cataracts because of underlying inflammation and the use of corticosteroids to treat the disease.
• Posterior subcapsular opacities are commonly seen

Grading of vitreous haze

intraocular pressure (IOP)
• Low may occur as a result• of reduced secretion of aqueous by the ciliary
epithelium.• Occasionally the intraocular pressure may be
elevated (hypertensive uveitis) as in herpetic uveitis and Posner–Schlossman syndrome
Investigation not indicate
• A single episode of unilateral mild/moderate non granulomatous Uveitis
• Typical clinical feature • A systemic diagnosis compatible with clinical
feature has already been confirmed

Investigation indicate in
• Recurrent Uveitis• Severe uveitis• Bilateral uveitis• Granulomatous sign• Associated with Intermediate or posterior
uveitis• Routine syphilis serology
HLA tissue typing (HLA B27)
• HLA B27 is common cell surface protine that present peptides to T cells
• Very strong association with acute anterior uveitis ,ankyosing spondylitis, Reiter syndrome, psoriatic arthrities, arthrities in IBD

Syphilis serology
• ELISA are highly sensitive and specific but take around 3 months to become positive
• Non specific titratable cardiolipin antibody test such as Rapid plasma reagin(PRP) or VDRL are positive in early infection. The patient’s serum is mixed with commercially prepared carbon-like cardiolipin antigen
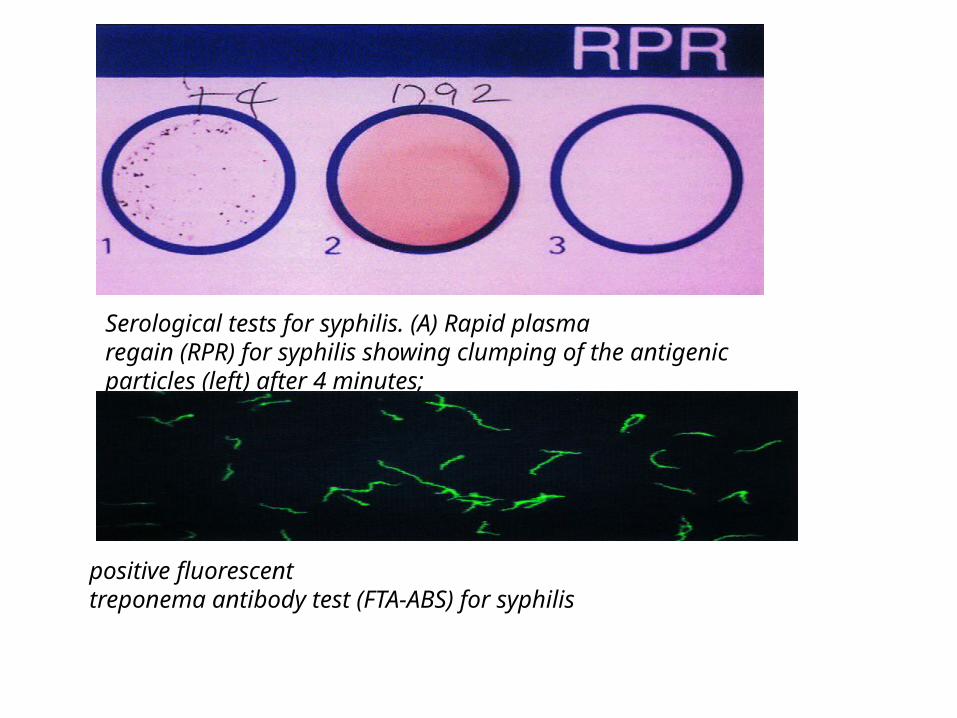
Serological tests for syphilis. (A) Rapid plasmaregain (RPR) for syphilis showing clumping of the antigenicparticles (left) after 4 minutes;
positive fluorescenttreponema antibody test (FTA-ABS) for syphilis
Toxoplasmosis• 1. Dye test (Sabin-Feldman) utilizes live organisms which are
exposed to the patient’s serum complement. The cell membranes of the organisms are lysed in the presence
of the specific anti-toxoplasma IgG, and as consequence the organisms fail to stain with methylene blue dye. This test remains the gold standard for the diagnosis of toxoplasmosis.
• 2. Immunofluorescent antibody tests utilize dead organisms exposed to the patient’s serum and antihuman globulin labelled with fluorescein. The results are read using a fluorescent microscope
• 3. Haemagglutination tests involve the coating of lysed organisms on to red blood cells which are then exposed to the patient’s serum; positive sera cause the red cells to agglutinate
Enzyme-linked immunosorbent assay (ELISA)
• involves binding of the patient’s antibodies to an excess of solid phase antigen. This complex is then incubated with an enzyme-linked second antibody.
• Assessment of enzyme activity provides measurement of specific antibody concentration.
• The test can also be used to detect antibodies in the aqueous which are more specific than those in the serum, and is useful in other conditions such as cat-scratch fever and toxocariasis.
• Any positive titre, even in undiluted serum, is significant in the presence of a fundus lesion
Enzyme assay -Serum angiotensin-converting enzyme
• A non specific test that indicate the presence of granulomatous diseases such as sarcodosis ,tuberculosis and leprosy.
• Elevation occurs in upto 80% of patients of sarcodosis• The normal serum level in adults is 32.1 ± 8.5IU• In patients with suspected neurosarcoid ACE can be
measured in the cerebrospinal fluid.• ACE may also be elevated in other conditions such as
tuberculosis, lymphoma and asbestosis.

Lysozyme
• Group of enzyme found in polymorphonuclear neutrophils and numerous secretion including tears.
• Less sensitive and specific than serum ACE
ESR and CRP
• Acute phase reactant • Elevated in systemis inflammetory disorders

• CBC-Leukocytosis raise in infections uveitis • ANA- Juvenile Idiopathic arthritis • Antineutrophil cytoplasmic antibody-wegner
granulomatosis.• Interferon gamma release
assay(QuantiFERON-TB GOLD)• HIV serology

Skin tests . Tuberculin skin tests (Mantoux and Heaf)
Intradermal injection of purified protein derivative of M. tuberculosis.a. Positive result is characterized by the development of an
induration of 5–14 mm with 48 hoursb. Negative result usually excludes TB, but may alsooccur in patients with advanced consumptive disease.c. Weakly positive result does not necessarily distinguish• between previous exposure and active disease.• BCG d. Strongly positive result (induration > 15 mm) is usually indicative of
active disease since this level of response is not expected after long exposure to the vaccine

Lepromin test
intradermal injection of an extract of leprosy bacilli.
It differs from the tuberculin test because it becomes positive after several weeks.
It is strongly positive in tuberculoid leprosy and negative in lepromatous leprosy.

X Ray
• Sacroiliac joint X ray- Sacroiliitis in ankylosing spondylitis
• Chest X ray –tuberculosis or sarcodosis
Ocular imaging
• B scan –very small pupil/ opaque media• Fundus autoflurescence –suspected posterior
segment pathology such as multiple evanescent white dot syndrome (MEWDS)

Fluorescein angiography (FA) is useful in the followingcircumstances
• Evaluation of retinal vasculitis.• Diagnosis of macular disease, particularly cystoid macular
oedema (CMO) and choroidal neovascularization(CNV).• Demonstrating macular ischaemia as the cause of visual loss
rather than CMO.• Differentiation between inflammatory and ischaemic
causes of retinal neovascularization.• Diagnosis of specific uveitis entities that have characteristic
features on FA (e.g. acute posterior multifocal placoid pigment epitheliopathy and Harada disease).

Indocyanine green angiography (ICGA)
• for evaluating choroidal disease because the dye does not readily leak out of choroidal vessels which are better visualized through the RPE.
• ICGA is able to detect non-perfusion of the choriocapillaris and provide information regarding inflammation affecting the choroidal stroma.

Optical coherence tomography (OCT)
detecting complications such as macular oedema,epiretinal membranes and subretinal fluid.
It is also useful in delineating the anatomical layer of the inflammatory focus.

Aqueous tap
• Send for PCR for viral genetic material • For microscopy ,culture ,and antibody assay

Biopsy
• Conjunctival and lacrimal gland biopsy may useful for the diagnosis of sarcoidosis but only in the presence of clinically apparent disease.
• Vitreous biopsy- infectious endophthalmitis• Retinal and choroidal biopsies may be useful in the
following situations.• Diagnosis not established.• No response to therapy.• Further deterioration despite therapy.• Exclusion of malignancy or infection.

Thank you

















