50
Vaccine Refusal: How to Get Around It Regina LaRocque, M.D., M.P.H. Harvard Medical School/ Massachusetts General Hospital Travelers’ Advice & Immunization Center Global TravEpiNet

Vaccine Refusal: How to Get Around It
Regina LaRocque, M.D., M.P.H. Harvard Medical School/
Massachusetts General Hospital Travelers’ Advice & Immunization Center
Global TravEpiNet

I have no conflicts to disclose.

Overview
• Landscape of vaccine refusal
– measles
• Vaccine refusal in travelers
• Strategies to increase the uptake of travel-related vaccines

Vaccines are among the most effective prevention tools available
Roush and Murphy, JAMA, 2007

People refuse vaccines
MMWR 2014
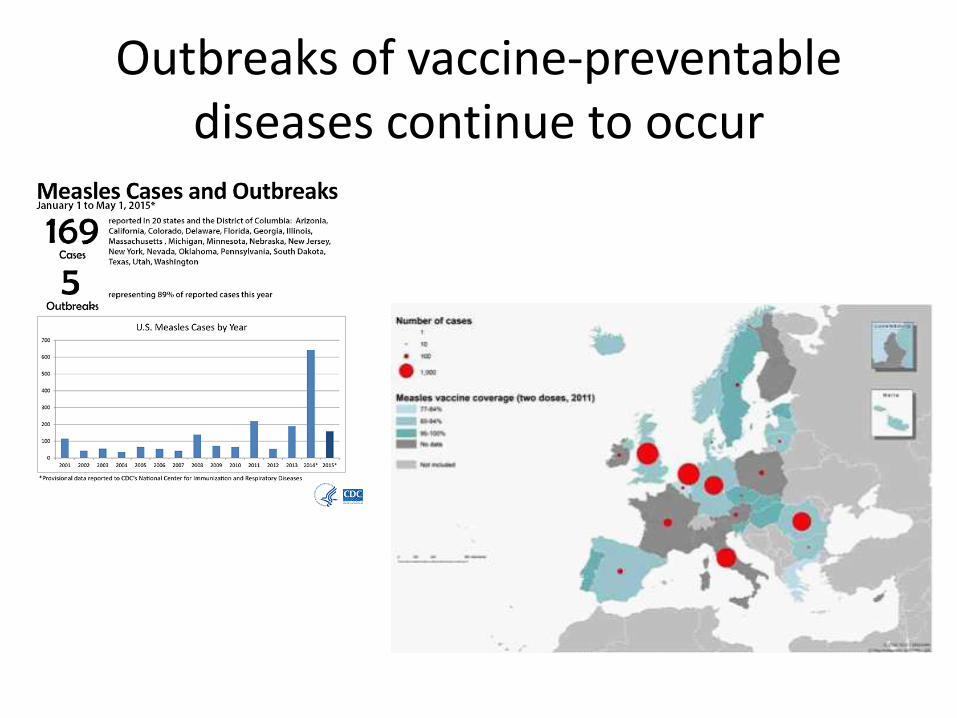
Outbreaks of vaccine-preventable diseases continue to occur

International travelers are important in outbreaks of vaccine-preventable diseases
There are two distinct groups who don’t receive vaccines
Those who lack access to
vaccines
Those who refuse
vaccines

Anti-vaccinationists have been around as long as vaccines
Poland & Jacobson, NEJM, 2011 “The Wonderful Effects of the New Inoculation!”

Who chooses not to vaccinate?
• White
• College graduates
• Higher household income
• Four or more children
• Alternative health beliefs or fundamental religious beliefs
• May have a direct experience with an assumed adverse event (child or relative with autism or someone who had a seizure)
Smith et al Pediatrics 2004

Non-vaccination is regional
Eisenstein Nature 2014

Common Misconceptions Among Those Who Choose Not to Vaccinate
• “Overloaded immune system”
• “Disappeared diseases”
• Certain ingredients (thimerosal and aluminum salts) in vaccines are dangerous
• Vaccines cause autism

“Utterly False” Publication in Lancet

Ready access to vaccine-critical messages perpetuates fear and mistrust

There is a spectrum of responses to offered vaccination
Refuser Late or selective vaccinator Hesitant Cautious acceptor Unquestioning acceptor
Leask et al BMC Pediatrics 2012
“Convince-ability”

Non-Vaccination in Travel Medicine
Those who lack access to
vaccines
Those who refuse
vaccines

Foreign-born (VFR) travelers lack access to pre-travel vaccines
• Less than ½ of travelers to low- and low-middle income countries sought any pre-travel health care
• Being foreign-born (VFR) was predictive of not pursuing pre-travel health care
• VFR travelers sought health advice from primary care practitioners (57%) and internet (31%)
LaRocque et al JTM 2010; Heywood et al BMC PH 2012; Toovey et al JTM 2004; Hamer JTM 2004; Van Herck JTM 2004; Wilder-Smith JTM 2004

Non-Vaccination in Travel Medicine
Those who lack access to
vaccines
Those who refuse
vaccines ?

Vaccine Refusal in U.S. Travel Clinics: Global TravEpiNet (GTEN)

Vaccine Refusal in GTEN
• All international travelers seen at GTEN sites between July 1, 2012 and June 30, 2014
• Clinicians use a secure internet tool to collect data regarding traveler, itinerary and pre-travel health care (vaccines, medicines, advice) provided
• Clinicians are prompted to consider vaccines that are recommended by CDC guidelines current at the time of the traveler’s trip
• When a traveler declined a recommended vaccine, providers were required to indicate one of three reasons: (1) cost concerns (2) safety concerns (3) not concerned about the illness
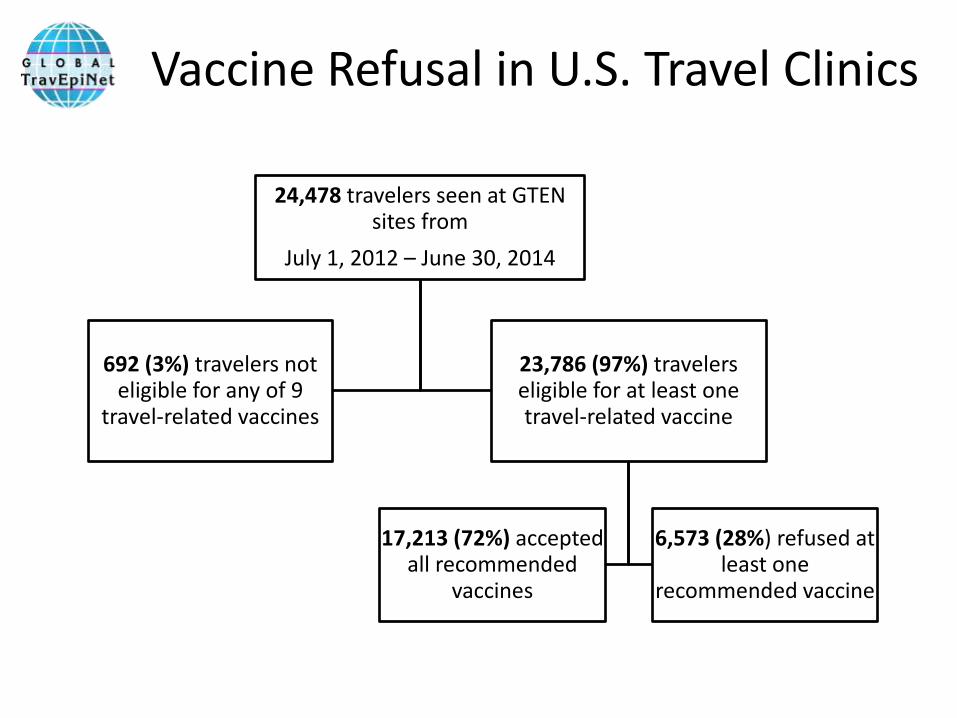
Vaccine Refusal in U.S. Travel Clinics
24,478 travelers seen at GTEN sites from
July 1, 2012 – June 30, 2014
692 (3%) travelers not eligible for any of 9
travel-related vaccines
23,786 (97%) travelers eligible for at least one travel-related vaccine
17,213 (72%) accepted all recommended
vaccines
6,573 (28%) refused at least one
recommended vaccine

Who refuses travel vaccines?
Accepters (N = 17,213)
Refusers (N = 6,573)
P-value
Gender (female) 9,618 (56%) 3,760 (57%) N.S.
Age, median (Q1, Q3) 35 years (23, 53) 34 years (23, 51) <0.0001^
Purpose of travel Leisure Business Humanitarian VFR Research/education Other*
8,549 (50%) 2,961 (17%) 2,187 (13%) 1,425 (8%) 1,357 (8%) 734 (4%)
2,664 (41%) 861 (13%) 1,083 (17%) 859 (13%) 417 (6%) 689 (10%)
<0.0001
Medical problem (yes)
11,182 (65%) 3,539 (54%) <0.0001
* adoption, receiving medical care, military, adventure, attending large gathering, and other activities.

Who refuses travel vaccines?
Accepters (N = 17,213)
Refuser (N = 6,573)
P-value
Destination region (WHO) Sub-Saharan Africa Latin America/Caribbean East Asia/Pacific South Asia Europe/Central Asia Other
6,146 (36%) 4,669 (27%) 3,426 (20%) 2,304 (13%) 191 (1%) 12 (0.1%)
3,030 (46%) 1,360 (21%) 1,234 (19%) 702 (11%) 41 (0.6%) 4 (0.1%)
<0.001
US region* Northeast Midwest West South
7,774 (85%) 911 (78%) 4,581 (71%) 3,947 (56%)
1,351 (15%) 257 (22%) 1,891 (29%) 3,074 (44%)
<0.0001
* Row percentages

Hepatitis A Polio Meningococcal
Yellow fever Rabies MMR
Typhoid Japanese encephalitis Influenza
Legend Vaccine Administered
Traveler Refused
Not Administered*
Which vaccines do travelers refuse?
*Reasons include referral to primary care provider, insufficient time, vaccine not available

Hepatitis A Polio Meningococcal
Yellow fever Rabies MMR
Typhoid Japanese encephalitis Influenza
Legend Not concerned about
illness
Safety
Cost
Why do travelers refuse vaccines?

Reason for Refusing: VFR vs. Non-VFR
VFR Travelers Non-VFR Travelers
p-value < 0.0001

Vaccine Refusal: Lessons from GTEN
• Limitations
– U.S., generalizability, unsolicited reasons
• Even individuals who seek pre-travel care refuse vaccines.
• The barrier to vaccination (lack of concern) may be remediable.

How can we increase vaccine uptake in travelers?
Those who lack access to
travel vaccines
Those who refuse travel
vaccines

How can we increase vaccine uptake in travelers?
Those who lack access to
travel vaccines
Foreign-born (VFR) Seek travel-related information from the internet and PCPs

How can we increase vaccine uptake in travelers?
Those who lack access to
travel vaccines
Foreign-born (VFR) Seek travel-related information from the internet and PCPs
Increase availability of appropriate pre-travel care through primary care practitioners
Internet-based outreach



How can we increase vaccine uptake in travelers?
Those who refuse travel
vaccines
Foreign-born (VFR) Young and healthy Traveling to Africa Not concerned about illness

How can we increase vaccine uptake in travelers?
Those who refuse travel
vaccines
Foreign-born (VFR) Young and healthy Traveling to Africa Not concerned about illness
Increase concern about travel-related illness

Approaches to Increasing “Concern”: Lessons from Pediatricians
• Clinician counseling
• Storytelling
• Electronic tools
• (Mandates)
Pediatric Setting Travel Medicine Setting
Longitudinal One-time
Vaccine refusers are parents Many vaccine refusers are VFR travelers
Many health topics are being discussed
Vaccines are a focus
Safety concerns are paramount Lack of concern about illness is common

Clinician Counseling
• Receiving reassurance and vaccine information from a provider can be effective in changing the minds of vaccine-hesitant individuals.
• The nature of this communication matters: • The use of participatory initiation formats (“What do you want to do
about shots?; “Are we going to do shots today?”) when making vaccine recommendations is associated with an increased odds of vaccine refusal.
• Presumptive initiation formats (“Well, we have to do some shots.”) are associated with vaccine acceptance.
• Nearly half of initially resistant parents accept a provider’s original vaccine recommendation if the provider continues to pursue it.
Gust et al Pediatrics 2008; Opel et al Pediatrics 2013

The Power of Storytelling
• Providing corrective information about vaccine myths based on statistics and evidence can have a paradoxical effect of increasing resistance to vaccines.
• Using storytelling strategies popular with the anti-vaccine movement may be a more powerful communication strategy.
Nyhan et al Pediatrics 2014; Nyhan et al Vaccine 2015

Electronic Tools
• An electronic health record alert to patients (“services your provider will recommend for you today”) and clinicians during an office appointment increased the uptake and completion of the HPV vaccine series.
• Use of a web-based decision aid improved parental attitudes toward MMR vaccine. Ruffin et al JABFM 2015; Wallace et al BMJ 2006

Conclusions • Vaccination of travelers is important for the health of
individuals, as well as to prevent importation of vaccine-preventable diseases into vulnerable home communities.
• Some travelers lack access to vaccines, but travelers also refuse indicated vaccines during a pre-travel encounter.
• Strategies to increase vaccine uptake in travelers should focus on – Increasing access to high-quality pre-travel care in primary care
settings (VFR travelers)
– Increasing concern about vaccine-preventable travel-related diseases during the pre-travel encounter
• We can learn from pediatric experiences with the anti-vaccination movement to develop communication strategies that will promote better vaccine uptake in travelers.

Acknowledgments
Participating Sites
Northwestern University
Jenny Lee
Revere HealthCare Center
Roger Pasinski, Amy Wheeler
Salt Lake Valley Health Department
Dagmar Vitek, Holly Birich
St. Luke’s – Roosevelt
John Cahill
St. Vincent Hospital
George Abraham
St. Vincent’s First Care
Jenn Katsolis
Tulane University
Frederique Jacquerioz, Susan McLellan
University of California, Los Angeles
Paul Allyn, Risa Hoffman, Tara Vijayan
University of California, San Diego
Joseph Vinetz
University of California, San Francisco
Brian Schwartz
University of Southern California, LA
Jeff Goad, Edith Mirzaian
University of Minnesota
Patricia Walker, William Stauffer
University of Utah
DeVon Hale, Brian Kendall, Daniel Leung
Participating Sites
Bronx-Lebanon Hospital Center
Stefan Hagmann
Chelsea HealthCare Center
Elisha Atkins
DeKalb County Board of Health
Alawode Oladele, Hanna Demeke
Emory University TravelWell
Phyllis Kozarsky, Roberta Dismukes, Jessica Fairley, Henry Wu, Carlos Franco-Paredes
Georgetown University
Jessica Rosen, Laura Coster
Johns Hopkins University
Noreen Hynes
Journey Health
Ronke Dosunmu
Kaiser Permanente Hawaii
Vernon Ansdell, Johnnie Yates
Lehigh Valley Medical Center
Mark Knouse
Mayo Clinic Jacksonville
Salvador Alvarez
Mount Auburn Hospital
Lin Chen
New York Center for Travel
& Tropical Medicine
Bradley Connor
OVERSIGHT TEAM CDC Clive Brown Gary Brunette Gary Buckett Margaret Coleman Samantha Dolan Rhett Dunaway Stefanie Erskine Emily Jentes Nancy Gallagher Kenji Hidachi Pauline Han Nomana Khan Kelly Holton Phyllis Kozarsky M.I. Meltzer Mark Sotir Emad Yanni Mass General Edward T. Ryan Regina LaRocque David Schoenfeld Ricky Morse Brett Macaulay Sara Lammert Emily Hyle Rochelle Walensky UMass Sowmya Rao BLMC (NYC) Stefan Hagmann NYCDoHMH Ellen Lee Camille Adolphe
Lucretia Jones
Kimberly Valcin
Stacey Wright-Woolcock

Visit our booth #804 Poster P011.07
www.gten.travel


Increasing Vaccine Acceptance by Travelers: Lessons from Pediatrics
• How to talk to a vaccine hesitant person
– Share honestly what is known and not known about the risks and benefits of the vaccine in question
– Listen respectfully
– Explain the risk of non-immunization
– Discuss the specific concerns
American Academy of Pediatrics Committee on Bioethics

Increasing Vaccine Acceptance by Travelers: Lessons from Pediatrics
• How to talk to a vaccine hesitant person
– Share honestly what is known and not known about the risks and benefits of the vaccine in question
– Listen respectfully
– Explain the risk of non-immunization
– Discuss the specific concerns
American Academy of Pediatrics Committee on Bioethics
TRUST
A Cautionary Tale….

Common Misconceptions
• “Overloaded immune system”
– Began to appear as childhood immunization schedule increased and as combination vaccines were developed
– Science: No evidence to support increase in adverse events when vaccines are administered simultaneously
• Spreading out and hence delaying vaccines increases risk of contracting illness
Poland & Jacobson, NEJM, 2011
Common Misconceptions
• “Disappeared diseases”
– because diseases like polio and measles have disappeared from the United States there is no need to vaccinate against them
– Science: Risk of outbreaks related to importation is real
Poland & Jacobson, NEJM, 2011

Common Misconceptions
• Vaccines cause autism
Poland & Jacobson, NEJM, 2011

Common Misconceptions
• Certain ingredients (thimerosal and aluminum salts) in vaccines are dangerous
– Science: no evidence that thimerosal is harmful
• Vaccine manufacturers removed thimerosal from all products except multidose vials in 2001
Poland & Jacobson, NEJM, 2011













![Vaccine hesitancy, vaccine refusal and the anti-vaccine ... · studies showing no link between measles–mumps–rubella (MMR) vaccination and autism [43–45] – and Wakefield being](https://static.documents.pub/doc/80x56/5d4f476888c993a3378b70e4/vaccine-hesitancy-vaccine-refusal-and-the-anti-vaccine-studies-showing.jpg)




