Vacuum-Assisted Vaginal DeliveryUnzila A. Ali, MD, Errol R. Norwitz, MD, PhD
Department of Obstetrics, Gynecology & Reproductive Sciences, Yale University School of Medicine, New Haven, CT
Approximately 5% (1 in 20) of all deliveries in the United States are opera-tive vaginal deliveries. The past 20 years have seen a progressive shift awayfrom the use of forceps in favor of the vacuum extractor as the instrument of choice. This article reviews in detail the indications, contraindications, patient selection criteria, choice of instrument, and technique for vacuum-assisted vaginal delivery. The use of vacuum extraction at the time of cesareandelivery will also be discussed. With vacuum extraction becoming increasinglypopular, it is important that obstetric care providers are aware of the mater-nal and neonatal risks associated with such deliveries and of the optionsavailable to effect a safe and expedient delivery.[Rev Obstet Gynecol. 2009;2(1):5-17]
Operative vaginal delivery refers to the application of either forceps or avacuum device to assist the mother in effecting vaginal delivery of a fetus.The incidence of operative vaginal delivery in the United States is cur-
rently estimated at around 5%, or approximately 1 in 20 deliveries,1-4 althoughthere are large geographic differences in the rates of operative vaginal deliveryacross the country.2 The lowest rates of instrumental vaginal delivery (� 5%) areseen in the Northeast and the highest rates (20%-25%) are in the South.2 Al-though the overall rate of operative vaginal delivery has been declining, the pro-portion of vacuum-assisted deliveries has been increasing and now accounts foralmost 4 times the rate of forceps-assisted vaginal births.2
Historical PerspectiveThe first instrumental deliveries wereperformed to extract fetuses fromwomen at high risk of dying due toprolonged or obstructed labor. Inthese cases, saving the mother’s lifetook precedence over possible harmto the fetus. With the development ofsafer techniques for vaginal extrac-tion, however, the focus of these pro-cedures has changed dramatically and
the major indications for operativevaginal delivery in modern obstetricpractice are to safeguard the well-being of the fetus. Vacuum extractionwas first described in 1705 by Dr.James Yonge, an English surgeon,several decades before the inventionof the obstetric forceps. However, itdid not gain widespread use until the1950s, when it was popularized in aseries of studies by the Swedish ob-stetrician Dr. Tage Malmström.5 Bythe 1970s, the vacuum extractor hadalmost completely replaced forcepsfor assisted vaginal deliveries in mostnorthern European countries, but itspopularity in many English-speakingcountries, including the United Statesand the United Kingdom, was limited.By 1992, however, the number of vac-uum assisted deliveries surpassed thenumber of forceps deliveries in theUnited States, and by the year 2000approximately 66% of operative vagi-nal deliveries were by vacuum.6
IndicationsAn operative vaginal delivery shouldonly be performed if there is an ap-propriate indication. In 2000, TheAmerican College of Obstetriciansand Gynecologists (ACOG) publishedguidelines on the use of operativevaginal delivery (both forceps andvacuum), which included a list of
accepted indications for such pro-cedures.4 These are summarized inTable 1. It should be made clear thatnone of these indications are absolutebecause the option of cesarean deliv-ery is always available.
Earlier data suggested that fetalmorbidity was higher when the sec-ond stage of labor (defined as the timefrom full cervical dilatation to deliv-ery of the fetus) exceeded 2 hours,
irrespective of fetal testing. As such,obstetric care providers were encour-aged to expedite delivery once thesecond stage of labor was noted tobe prolonged (defined in Table 1).4
More recent data collected after routineuse of epidural analgesia, however,have disputed this assertion and haveshown that continued expectant man-agement of women with prolongedsecond stage of labor is a safe and
reasonable option if fetal testing isreassuring.4,7,8 As such, prolongedsecond stage of labor—although stillan indication—should no longer beregarded as an absolute indication foroperative delivery. The risks to themother of a prolonged second stageof labor include severe perineal injury(defined as a third or fourth degreeperineal laceration) and postpartumhemorrhage, and appear to be associ-ated more strongly with obstetric in-strumentation rather than the lengthof the second stage of labor.9
Suspected fetal compromise in theform of a nonreassuring fetal heartrate tracing is perhaps the most com-mon and widely accepted indicationfor operative vaginal delivery, al-though the interpretation of fetalheart rate tracings is subjective andhighly variable.10 Women with con-traindications to Valsalva manuevermay benefit from elective operativevaginal delivery. This includeswomen with select cardiac or neuro-logic diseases, such as some women
Vacuum extraction was first described in 1705 by Dr. James Yonge, an Eng-lish surgeon, several decades before the invention of the obstetric forceps.
Table 1Indications for Vacuum-Assisted Vaginal Delivery
Indication Definition
Prolonged second stage of labor In nulliparous women, this is defined as lack of progress for 3 hours with regionalanesthesia or 2 hours without anesthesia. In multiparous women, it refers to lack ofprogress for 2 hours with regional anesthesiaor 1 hour without anesthesia.
Nonreassuring fetal testing Suspicion of immediate or potential fetal compromise (nonreassuring fetal heart ratepattern, abruption) is an indication for opera-tive vaginal delivery when an expeditious delivery can be readily accomplished.
Elective shortening of the second Vacuum can be used to electively shorten thestage of labor second stage of labor if pushing is contraindi-
cated because of maternal cardiovascular orneurologic disease.
Maternal exhaustion Largely subjective and not well defined.
Data from The American College of Obstetricians and Gynecologists.4
with New York Heart Association(NYHA) class III/IV cardiac diseaseand uncorrected intracerebral vascu-lar malformations. Operative vaginaldelivery may also be required if thereis inadequate maternal expulsive ef-forts, such as women with spinal cordinjuries or neuromuscular diseases.Maternal exhaustion is another com-monly used indicator for operativevaginal delivery, but is not welldefined and is highly subjective. Assuch, providers should make everyeffort to avoid using this as thesole indication for operative vaginaldelivery.
ContraindicationsA number of clinical situations exist inwhich operative vaginal deliveryshould not be attempted because of the
potential risks to the fetus (Table 2).4
For example, an underlying fetal con-dition such as a documented bleedingdiathesis or bone demineralizing dis-ease will predispose the fetus to majorinjury including intraventricular hem-orrhage and skull fracture and, as
such, should be regarded as an ab-solute contraindication to operativevaginal delivery. Such deliveriesshould also not be attempted if thefetal vertex is not engaged in the ma-ternal pelvis, if the cervix is incom-pletely dilated, if the fetal membranesare not ruptured, if the fetal position(defined as the relationship of a
nominated site of the presenting partto a denominating location on the ma-ternal pelvis) is not known, if there issuspected cephalopelvic disproportion,or if there is fetal malpresentation(such as breech, brow, or face presen-tation).11 Vacuum-assisted vaginal de-
livery should not be performed prior to34 weeks of gestation because of therisk of fetal intraventricular hemor-rhage.4 Prior scalp sampling or multi-ple attempts at fetal scalp electrodeplacement are also relative contraindi-cations to vacuum extraction becausethese procedures may increase therisk of cephalohematoma or externalbleeding from the scalp wound.12-14
There is no consensus regardingminimum and maximum estimatedfetal weights that preclude operativevaginal delivery. Performance of anoperative vaginal delivery in a fetuswith suspected macrosomia is sup-ported by ACOG,4 but should be per-formed with caution given the possi-ble increased risk of fetal injury15 andof shoulder dystocia, especially whenthe second stage of labor is pro-longed. Because of the risk of intra-ventricular hemorrhage, vacuum ex-traction is not recommended infetuses with an estimated weightless than 2500 g (which correspondsto � 34 weeks of gestation).
Alternatives to Operative Vaginal DeliveryInformed consent (either verbal orwritten) is required prior to perform-ing an operative vaginal delivery.Alternative management strategiesshould be discussed and will vary de-pending on the clinical circumstancesand on the indication for the opera-tive vaginal delivery. For example, ifthe indication is a prolonged second
Table 2Contraindications for Vacuum-Assisted Vaginal Delivery
stage of labor in the setting of reas-suring fetal testing, alternatives to anoperative vaginal delivery includecontinued expectant management,oxytocin augmentation, and cesareandelivery. Because existing data sug-gest that most women with a pro-longed second stage will ultimatelydeliver vaginally and that a secondstage exceeding 2 hours in durationdoes not adversely affect neonataloutcome,4,7,8 continued expectantmanagement is reasonable. Changesin maternal positioning, a reductionin neuraxial anesthesia, increasedemotional support to the patient, and“laboring down” (delayed pushing) inthe second stage have all been shownto increase the likelihood of a suc-cessful vaginal delivery.16-20 If suchconservative interventions fail toachieve a vaginal delivery, either anoperative vaginal delivery or a ce-sarean delivery can be performed. Ifthe patient does not meet criteriafor an operative vaginal delivery orif the operator does not feel com-
fortable performing the procedure,then a cesarean delivery should berecommended.
Prerequisites for Operative Vaginal DeliveryA series of criteria all need to be ful-filled before an operative vaginal de-livery can be attempted. These aresummarized in Table 3.21 The cervixshould be fully dilated and the mem-branes ruptured. The head must beengaged in the maternal pelvis,meaning that the biparietal diametermust have passed through the pelvicinlet. This is best assessed on abdom-inal examination using the Leopold’smaneuvers, although confirmation offetal station (defined as the leadingbony edge of the fetal presenting partrelative to the maternal ischial spines)of more than 0/�5 on transvaginalexamination can also be used todocument engagement. A large fetus,excessive molding of the fetal skullbones, a deflexed attitude (extension)of the fetal head, and asynclitism
(lateral flexion of the fetal head) canmake it appear as though the vertex isengaged when the leading bony edgeis actually above the level of the is-chial spines. Fetal lie, presentation,and position should all be docu-mented. The type of operative vaginaldelivery is classified according to thestation and the degree of rotationof the fetal head within the pelvis(Table 4).22 If the position is unclearon clinical examination—which maybe seen in upwards of 25% of cases inwhich operative vaginal delivery isbeing considered23—an intrapartumultrasound can be done to confirmfetal position. Prior to attempting anoperative vaginal delivery, clinicalpelvimetry should be performed withdocumentation of adequate mid andoutlet pelvic dimensions. The esti-mated fetal weight should also bedocumented.
Once the obstetric care provider hasconfirmed that the patient is an ap-propriate candidate for an operativevaginal delivery, informed consent
Table 3Prerequisites for Operative Vaginal Delivery
Maternal Criteria Fetal Criteria Uteroplacental Criteria Other Criteria
Adequate analgesia
Patient in the lithotomy position
Bladder empty
Clinical pelvimetry must beadequate in dimension andsize to facilitate an atrau-matic delivery
Verbal or written consent obtained
Vertex presentation
The fetal head must be engaged in the pelvis
The position of the fetal headmust be known with certainty
The station of the fetal headmust be � 0/�5
The estimated fetal weight must be documented (ideally2500-4500 g)
The attitude of the fetal headand the presence of caputsuccedaneum and/or mold-ing should be noted
Cervix fully dilated
Membranes ruptured
No placenta previa
An experienced operator who isfully acquainted with the useof the instrument
Ability to monitor fetal well-being continuously
The capability to perform anemergency cesarean deliveryif required
should be obtained. This can be eitherverbal or written. Either way, the po-tential risks, benefits, and alternativesto operative vaginal delivery shouldbe discussed, and the discussionshould be clearly documented in themedical record.
Selection of Instrument: Forceps or Vacuum?Selection of the appropriate instru-ment depends on both the clinicalsituation and the operator’s level ofcomfort and experience with the spe-cific instrument. Factors that need tobe considered include the availabilityof the instrument in question, thedegree of maternal analgesia, and anappreciation of the risks and benefitsof each of the individual instruments.
Published data suggest that forcepsdeliveries are associated with morematernal morbidity, whereas vacuumdevices cause more neonatal injury.For example, a meta-analysis of 10 clin-ical trials concluded that vacuum-assisted deliveries were associated
with significantly less maternaltrauma than forceps, including alower rate of severe perineal injury(odds ratio [OR], 0.41; 95% confidenceinterval [CI], 0.33-0.50).24 Indeed, theshift toward vacuum-assisted deliver-ies over forceps has led to a signifi-cant reduction in the incidence of se-vere perineal injuries in the motherover the last 10 years. In this meta-analysis, vacuum devices were alsoassociated with a reduced need forgeneral and regional anesthesia, andwith less postpartum pain than for-ceps.24 In contrast, this same reviewshowed that forceps deliveries have alower risk of scalp injury and cephalo-hematoma than vacuum.24 Additionaladvantages of forceps are that theycan be used safely in premature in-fants, they can be used to effect rota-tion of the fetal head (which is nottrue of vacuum), and they are lesslikely to detach from the fetal head.Although vacuum deliveries are morelikely to fail, the overall cesareandelivery rate is still lower when the
vacuum device is used rather than for-ceps. The reason for this is not entirelyclear. It may have to do with patientselection or with the fact that, in yearspast, a failed vacuum delivery wastypically followed by an attemptedforceps delivery, whereas a failed for-ceps was more likely to be followed bya cesarean delivery.
Although the decision of which in-strument to use is dependent in largepart on the preference of the individ-ual care provider, there are certainclinical situations where one instru-ment may be preferred over another.For example, delivery of an occiput-posterior vertex with molding is besteffected using forceps, whereas avacuum extraction would be the in-strument of choice when performingan outlet procedure on an occiput-anterior vertex in a woman withminimal analgesia.
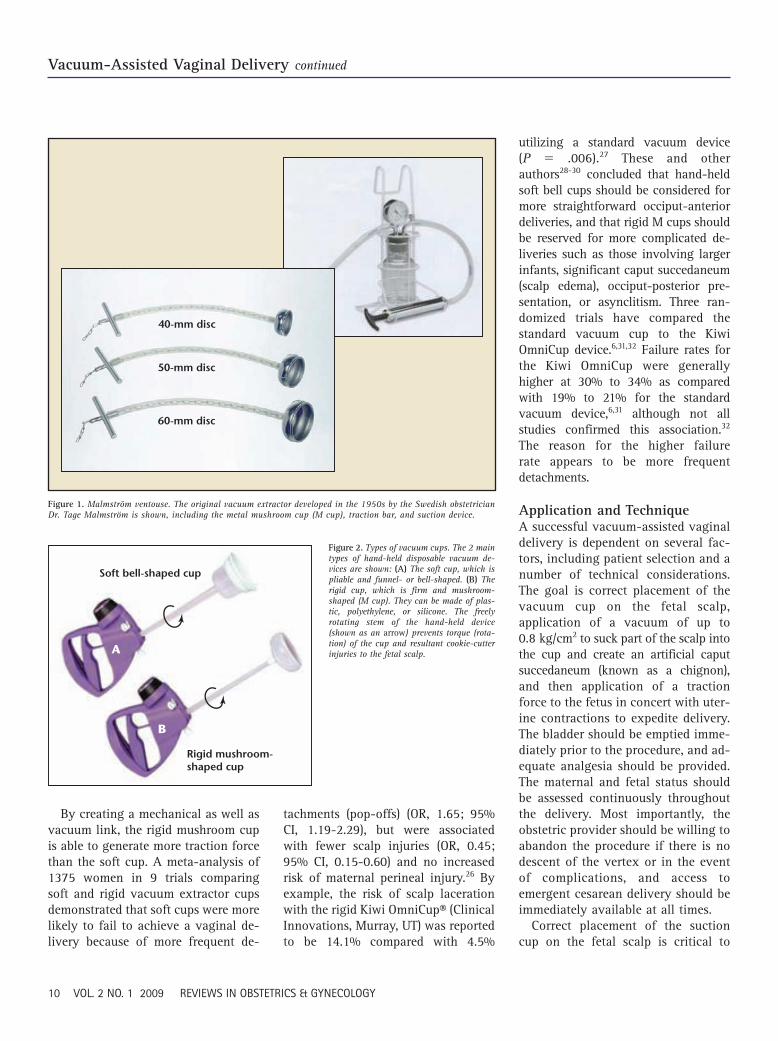
Selection of Instrument: Which Vacuum Cup?Having decided to perform a vacuumextraction, the operator must decidewhich cup to use. The original vacuumdevice developed in the 1950s by theSwedish obstetrician Dr. Tage Malm-ström was a disc-shaped stainless steelcup attached to a metal chain for trac-tion (Figure 1). Due to technical prob-lems and lack of experience with thisinstrument, vacuum devices did notgain popularity in the United Statesuntil the introduction of the dispos-able cups in the 1980s. There are2 main types of disposable cups,which can be made of plastic, poly-ethylene, or silicone. The soft cup is apliable funnel- or bell-shaped cup,which is the most common type usedin the United States (Figure 2A). Therigid cup is a firm mushroom-shapedcup (M cup) similar to the originalmetal disc-shaped cup, and is avail-able in 3 sizes (40, 50, and 60) (Fig-ure 2B). Commercially available suc-tion cups are summarized in Table 5.25
Table 4Classification of Operative Vaginal Deliveries
Type of Procedure Criteria
Outlet (1) Scalp is visible at the introitus without separating the labia
(2) Fetal skull has reached the level of the pelvic floor
(3) Sagittal suture is in the direct anteroposterior diameter orin the right or left occiput anterior or posterior position
(4) Fetal head is at or on the perineum
(5) Rotation is � 45°
Low Leading point of the fetal skull (station) is station �2/�5 ormore but has not as yet reached the pelvic floor
(a) Rotation is � 45°
(b) Rotation is � 45°
Midpelvic The head is engaged in the pelvis but the presenting part isabove �2 station
High (Not included in this classification)
Adapted from The American College of Obstetricians and Gynecologists.22
By creating a mechanical as well asvacuum link, the rigid mushroom cupis able to generate more traction forcethan the soft cup. A meta-analysis of1375 women in 9 trials comparingsoft and rigid vacuum extractor cupsdemonstrated that soft cups were morelikely to fail to achieve a vaginal de-livery because of more frequent de-
tachments (pop-offs) (OR, 1.65; 95%CI, 1.19-2.29), but were associatedwith fewer scalp injuries (OR, 0.45;95% CI, 0.15-0.60) and no increasedrisk of maternal perineal injury.26 Byexample, the risk of scalp lacerationwith the rigid Kiwi OmniCup® (ClinicalInnovations, Murray, UT) was reportedto be 14.1% compared with 4.5%
utilizing a standard vacuum device (P � .006).27 These and otherauthors28-30 concluded that hand-heldsoft bell cups should be considered formore straightforward occiput-anteriordeliveries, and that rigid M cups shouldbe reserved for more complicated de-liveries such as those involving largerinfants, significant caput succedaneum(scalp edema), occiput-posterior pre-sentation, or asynclitism. Three ran-domized trials have compared thestandard vacuum cup to the KiwiOmniCup device.6,31,32 Failure rates forthe Kiwi OmniCup were generallyhigher at 30% to 34% as comparedwith 19% to 21% for the standardvacuum device,6,31 although not allstudies confirmed this association.32
The reason for the higher failurerate appears to be more frequentdetachments.
Application and TechniqueA successful vacuum-assisted vaginaldelivery is dependent on several fac-tors, including patient selection and anumber of technical considerations.The goal is correct placement of thevacuum cup on the fetal scalp,application of a vacuum of up to0.8 kg/cm2 to suck part of the scalp intothe cup and create an artificial caputsuccedaneum (known as a chignon),and then application of a tractionforce to the fetus in concert with uter-ine contractions to expedite delivery.The bladder should be emptied imme-diately prior to the procedure, and ad-equate analgesia should be provided.The maternal and fetal status shouldbe assessed continuously throughoutthe delivery. Most importantly, theobstetric provider should be willing toabandon the procedure if there is nodescent of the vertex or in the eventof complications, and access toemergent cesarean delivery should beimmediately available at all times.
Correct placement of the suctioncup on the fetal scalp is critical to
40-mm disc
50-mm disc
60-mm disc
Figure 1. Malmström ventouse. The original vacuum extractor developed in the 1950s by the Swedish obstetricianDr. Tage Malmström is shown, including the metal mushroom cup (M cup), traction bar, and suction device.
Soft bell-shaped cup
A
B
Rigid mushroom-shaped cup
Figure 2. Types of vacuum cups. The 2 maintypes of hand-held disposable vacuum de-vices are shown: (A) The soft cup, which ispliable and funnel- or bell-shaped. (B) Therigid cup, which is firm and mushroom-shaped (M cup). They can be made of plas-tic, polyethylene, or silicone. The freelyrotating stem of the hand-held device(shown as an arrow) prevents torque (rota-tion) of the cup and resultant cookie-cutterinjuries to the fetal scalp.
success of the procedure. The suctioncup should be placed symmetricallyastride the sagittal suture at the me-dian flexion point (also known as thepivot point), which is 2-cm anterior tothe posterior fontanelle or 6-cmposterior to the anterior fontanelle(Figure 3). Extreme care should betaken to avoid placement directlyover the fontanelle. Correct placementwill facilitate flexion, descent, and ro-tation of the vertex when traction isapplied and will minimize injury toboth the fetus and soft tissues of thebirth canal. After the cup is applied,the circumference of the cup should
be swept to ensure that no vaginal orcervical tissues have been inadver-tently trapped within the vacuum cup.The placement of the cup on the scalpshould be again confirmed. Suctioncan then be applied. Vacuum pres-sures should be raised initially to 100to 150 mm Hg to maintain the cup’sposition before being increased fur-ther to facilitate traction.
In the past, a slow incremental in-crease in vacuum pressure was rec-ommended before applying traction,starting at a negative pressure andincreasing gradually at 0.2 kg/cm2
every 2 minutes to achieve a pressure
of approximately 0.8 kg/cm2 (alterna-tively expressed as 500-600 mm Hg,500-600 torr, 23.6 in Hg, or 11.6 lbs/in2)within 8-10 minutes. The explanationgiven was that this slow incrementalapproach would allow for a morefirm attachment of the vacuum cup tothe fetal head and, thereby, a lowerfailure rate. However, there is noevidence that such an approach isassociated with an improved rate ofsuccessful vaginal delivery. In fact, arandomized control trial of 94 womencomparing stepwise versus rapid pres-sure application demonstrated thatthe rapid technique was associatedwith a significant reduction in theduration of vacuum extraction by anaverage of 6 minutes without ad-versely impacting fetal and maternaloutcome.33 A vacuum pressure of 0.6to 0.8 kg/cm2 (500-600 mm Hg) andan artificial caput succedaneum canbe achieved in a linear, rapid fashionin less than 2 minutes.34,35
The absolute safe traction force forvacuum extraction is unknown. How-ever, because traction force varieswith cup size, suction pressure, and al-titude as well as the individual clinicalcircumstances, it is reasonable andpractical to rely on the suction pres-sure that is displayed on all the com-mercially available devices. Once thedesired pressure has been achieved,sustained downward traction shouldbe applied along the pelvic curveusing 2 hands. The dominant hand ex-erts traction while the nondominanthand monitors the progress of descentand prevents cup detachment by ap-plying counter pressure directly to thevacuum cup. The traction should beapplied in concert with uterine con-tractions and maternal expulsiveefforts. An observational study of 119vacuum-assisted vaginal deliveriesusing a device with a traction forceindicator revealed that a traction forceof 11.5 kg (450 mm Hg) was sufficientto achieve vaginal delivery in at least
Table 5Types of Vacuum Suction-Cup Devices
for Operative Vaginal DeliveryDevice Size Material
Soft Cups
Gentle Vac™ (OB Scientific, 60 mm Soft rubberGermantown, WI)
Kiwi ProCup® (Clinical Innovations, 65 mm Soft plasticMurray, UT)
Mityvac MitySoft Bell® (Cooper- 60 mm Soft siliconeSurgical, Trumball, CT)
Secure Cup™ (Utah Medical, 63 mm RubberMidvale, UT)
Silc Cup 50-60 mm Silicone rubber
Soft Touch™ (Utah Medical) 60 mm Soft polyethylene
Tender Touch® (Utah Medical) 60 mm Soft silicone
Vac-U-Nate™ (Utah Medical) 65 mm Soft silicone
Rigid Anterior Cups
Flex Cup™ (Utah Medical) 60 mm Polyurethane
Kiwi OmniCup® (Clinical Innovations) 50 mm Rigid plastic
Malmström (Dickinson Healthcare, 40-60 mm MetalHungerford, UK)
Mityvac M-Style® (CooperSurgical) 50 mm Rigid polyethylene
Rigid Posterior Cups
Bird posterior cup 40-60 mm Metal
Kiwi OmniCup® (Clinical Innovations) 50 mm Rigid plastic
Mityvac M-Select® (CooperSurgical) 50 mm Rigid polyethylene
80% of cases. Moreover, all deliverieswere achieved with a maximum trac-tion force of 13.5 kg (500-600 mm Hg),although, at these higher levels,neonatal scalp abrasions and cephalo-hematomas were more common.36
Traction should be discontinued whenthe contraction ends and the motherstops pushing. Between contractions,suction pressure can be maintained orreduced to lower than 200 mm Hg.There appears to be no difference infetal morbidity with either regimen.37
As it flexes and descends, the fetalhead may rotate, resulting in passiverotation of the handle of the vacuum.Although this is to be expected, theaccoucheur should at no time attemptto manually rotate the fetal head withthe vacuum. This will lead to the clas-sic cookie-cutter injury in the fetalscalp. Descent of the vertex shouldoccur with each application of trac-tion. Once the fetal head is seen to be crowning, the suction should be re-leased, the cup removed, and theremainder of the delivery effected inthe normal fashion.
The decision to continue withoperative vaginal delivery must be re-evaluated continuously during
each step of the delivery. The maxi-mum time to safely complete a vac-uum extraction and the acceptablenumber of detachments is unknown.In an observational study of 393 sin-gleton term pregnancies, 82% of suc-cessful deliveries were achieved within1 to 3 pulls, and more than 3 pullswas associated with a 45% risk ofneonatal trauma.38 Based on theseand similar data,39,40 it is generallyrecommended that vacuum-assisteddeliveries be achieved with no morethan 3 sets of pulls and a maximumof 2 to 3 cup detachments (pop-offs).The total vacuum application timeshould be limited to 20 to 30 min-utes.4 These recommendations arebased more upon common sense andexperience than scientific data as ob-servational series have shown nolong-term differences in neonataloutcome related to these variables.25
Reasons for Failed Vacuum ExtractionVacuum-assisted vaginal deliveriesmay fail because of poor patient se-lection (such as attempting vacuumextraction in pregnancies complicatedby cephalopelvic disproportion) or
errors in application or technique. Forexample, selection of the incorrectcup size, accidental inclusion of ma-ternal soft tissues within the cup,and/or incorrect placement of thevacuum cup, resulting in worseningasynclitism (lateral traction) or de-flexion (extension) of the fetal head,may all contribute to failed vacuumattempts. Failure to apply traction inconcert with maternal pushing effortsor traction along the incorrect planemay also result in failed vacuum ex-traction. To avoid fetal injury, the ob-stetric care provider should not beoverly committed to achieving avaginal delivery and should be will-ing to abandon the procedure if it isnot progressing well. Delay may in-crease the risk of neonatal or mater-nal morbidity. The ability to performan emergency cesarean deliveryshould always be at hand.
Maternal ComplicationsThere is substantial evidence that in-strumental deliveries increase mater-nal morbidity, including perineal painat delivery, pain in the immediatepostpartum period, perineal lacera-tions, hematomas, blood loss andanemia, urinary retention, and long-term problems with urinary andfecal incontinence. A randomized trialof 118 nulliparous term deliveriesshowed significant maternal soft tis-sue trauma in 48.9% of forceps deliv-eries, 36.1% of deliveries using thesilastic vacuum extractor, and 21.6%of deliveries using the Mityvac®vacuum extractor (CooperSurgical,Trumball, CT) deliveries.41 Another re-view of over 50,000 vaginal deliveriesat the University of Miami reportedthat the rates of third and fourth de-gree perineal lacerations were higherin vacuum-assisted (10%) and forcepsdeliveries (20%) compared with spon-taneous vaginal deliveries (2%).42 Thehighest rates of maternal perinealtrauma are associated with deliveries
Parietal eminence
Frontal eminence
Bregma oranterior fontanelle
Frontal suture
Coronal suture
Lambdoidalsuture
Occipitalbone
Posteriorfontanelle
Figure 3. Placement of the obstetric vacuum. Correct placement of the suction cup on the fetal scalp is shown. Thesuction cup should be placed symmetrically astride the sagittal suture at the median flexion point (also known asthe pivot point), which is 2 cm anterior to the posterior fontanelle or 6 cm posterior to the anterior fontanelle.
involving rotations larger than 45°and with midforceps procedures.43
The risk of maternal trauma is higherfor fetuses in the occiput-posteriorposition.44,45 For example, a retrospec-tive cohort study of over 390 vacuum-assisted vaginal deliveries found thatan occiput-posterior position was as-sociated with a 4-fold increased riskof anal sphincter injury comparedwith an occiput-anterior position,which persisted after controlling formultiple covariables.45
Urinary and anal dysfunction (in-cluding incontinence, fistula forma-tion, and pelvic organ prolapse) areadditional risks of instrumental deliv-ery that typically present months toyears after delivery. A 5-year follow-up of a cohort of 228 women andchildren delivered by forceps or vac-uum extractor as part of a previousrandomized, controlled study reportedthat 47% experienced urinary incon-tinence, 44% reported bowel habit ur-gency, and 20% experienced loss ofbowel control.46 There were no appar-ent differences between the types ofinstruments used and no noninstru-mental spontaneous delivery controlgroup.
Maternal morbidity from instru-mental deliveries is often comparedwith that of cesarean deliveries be-cause this is the most likely alterna-tive procedure. Compared with ce-sarean delivery, operative vaginaldelivery is associated with less short-term maternal morbidity. In a retro-spective review of 358 midcavityoperative vaginal deliveries and486 cesarean deliveries, febrile morbid-ity was significantly lower in womendelivered vaginally (25% vs 4%) andall thromboembolic events occurredin women delivered by cesarean.47
However, long-term data suggest thatlaboring women delivered with theuse of obstetric instruments have ahigher rate of urinary incontinence at1 and 3 years postpartum compared
with laboring women delivered bycesarean.48,49
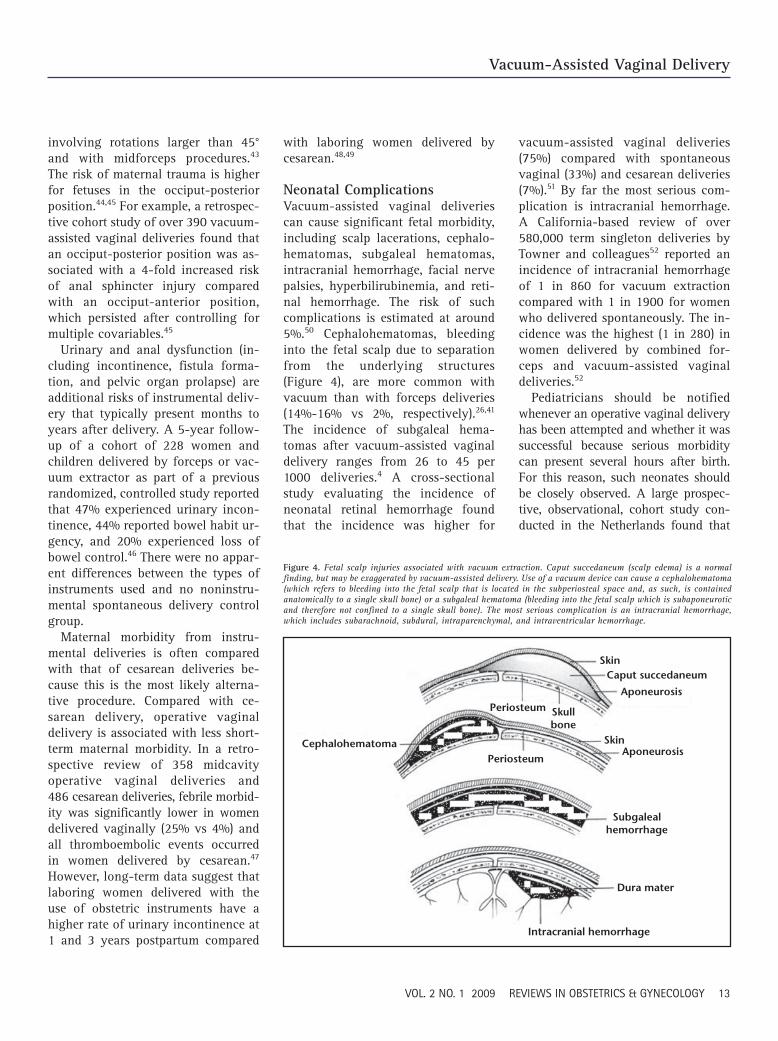
Neonatal ComplicationsVacuum-assisted vaginal deliveriescan cause significant fetal morbidity,including scalp lacerations, cephalo-hematomas, subgaleal hematomas,intracranial hemorrhage, facial nervepalsies, hyperbilirubinemia, and reti-nal hemorrhage. The risk of suchcomplications is estimated at around5%.50 Cephalohematomas, bleedinginto the fetal scalp due to separationfrom the underlying structures(Figure 4), are more common withvacuum than with forceps deliveries(14%-16% vs 2%, respectively).26,41
The incidence of subgaleal hema-tomas after vacuum-assisted vaginaldelivery ranges from 26 to 45 per1000 deliveries.4 A cross-sectionalstudy evaluating the incidence ofneonatal retinal hemorrhage foundthat the incidence was higher for
vacuum-assisted vaginal deliveries(75%) compared with spontaneousvaginal (33%) and cesarean deliveries(7%).51 By far the most serious com-plication is intracranial hemorrhage.A California-based review of over580,000 term singleton deliveries byTowner and colleagues52 reported anincidence of intracranial hemorrhageof 1 in 860 for vacuum extractioncompared with 1 in 1900 for womenwho delivered spontaneously. The in-cidence was the highest (1 in 280) inwomen delivered by combined for-ceps and vacuum-assisted vaginaldeliveries.52
Pediatricians should be notifiedwhenever an operative vaginal deliveryhas been attempted and whether it wassuccessful because serious morbiditycan present several hours after birth.For this reason, such neonates shouldbe closely observed. A large prospec-tive, observational, cohort study con-ducted in the Netherlands found that
Cephalohematoma
Periosteum Skullbone
Periosteum
SkinCaput succedaneum
Aponeurosis
SkinAponeurosis
Subgalealhemorrhage
Dura mater
Intracranial hemorrhage
Figure 4. Fetal scalp injuries associated with vacuum extraction. Caput succedaneum (scalp edema) is a normalfinding, but may be exaggerated by vacuum-assisted delivery. Use of a vacuum device can cause a cephalohematoma(which refers to bleeding into the fetal scalp that is located in the subperiosteal space and, as such, is containedanatomically to a single skull bone) or a subgaleal hematoma (bleeding into the fetal scalp which is subaponeuroticand therefore not confined to a single skull bone). The most serious complication is an intracranial hemorrhage,which includes subarachnoid, subdural, intraparenchymal, and intraventricular hemorrhage.
all vacuum-related injuries in termneonates were evident within 10 hoursof birth. The authors concluded thatneonates may be discharged 10 or morehours after vacuum delivery if no com-plications are evident.53
In 1998, the United States Food andDrug Administration (FDA) issued a
public health advisory to informindividuals that fetal complicationsincluding subgaleal hematomas andintracranial hemorrhage had been as-sociated with vacuum extraction.54,55
In support of their assertion, the FDAidentified 12 deaths and 9 seriouscomplications reported among infantsexposed to vacuum-assisted devicesbetween 1994 and 1998, a rate thatwas 5-fold higher than that reportedin the previous 11 years. The FDA ad-vised caution and offered a series ofrecommendations for the appropriateand safe use of vacuum extractor de-vices. Specifically, they recommendedthat operators refrain from rockingmovements and from the applicationof torque (rotation). They advised in-stead that providers use “steady trac-tion in the line of the birth canal.”54
They also stressed the importance ofnotifying pediatricians that a vacuumdevice had been applied so that theneonates could be monitored moreclosely during the first hours anddays of life.
Long-term sequelae from vacuum-associated injuries such as intracra-nial hemorrhage and neuromuscularinjury are uncommon. For example, a9-month follow-up study of childrenrandomized at term to vacuum versusforceps delivery found no significantdifferences in head circumference,weight, head circumference-to-weightratio, testing of vision and hearing,and hospital readmission rates.56
Vacuum-assisted vaginal delivery also
does not appear to adversely impactlong-term cognitive development. A10-year follow-up evaluation of 295children delivered at term by vacuumextraction and 302 control patientsdelivered by spontaneous vaginaldelivery showed no differences infine- and gross-motor control, per-
ceptual integration, and behavioralmaturity between the 2 groups.57
Clinical ControversiesA number of clinical controversiesstill surround vacuum-assisted vagi-nal delivery. These are discussedbriefly below.
Sequential Attempts at Instrumental Vaginal DeliveryACOG does not generally supportmultiple attempts at vaginal deliveryusing different instruments becauseof concerns about a higher rate ofmaternal and neonatal injury.4,52 Ini-tial small clinical studies failed todemonstrate any adverse effects fromcombined or sequential vacuum andforceps deliveries, but larger studiessuggest otherwise.58,59 The previouslymentioned study by Towner and col-leagues52 reviewed the mode of deliv-ery and subsequent perinatal morbid-ity in 583,340 nulliparous terminfants weighing 2500 g to 4000 gborn in California between 1992 and1994. The authors reported that theincidence of intracranial (subarach-noid, subdural, intraparenchymal,and/or intraventricular) hemorrhagewas highest in infants delivered byboth vacuum and forceps (1 in 256) ascompared with infants born by for-ceps (1 in 664) or vacuum extractionalone (1 in 860), cesarean delivery inlabor (1 in 907), spontaneous vaginaldelivery (1 in 1900), and electivecesarean delivery prior to labor (1 in
2705). A similar study by Gardellaand colleagues60 used Washingtonstate birth certificate data linked tohospital discharge records to compareperinatal outcome in 3741 vaginal de-liveries by both vacuum and forceps,3741 vacuum deliveries, 3741 forcepsdeliveries, and 11,223 spontaneousvaginal deliveries. The study foundthat the sequential use of vacuum andforceps was associated with signifi-cantly increased risk of both neonataland maternal injury.60
Not all cases of intracranial hemor-rhage are symptomatic. A prospectivestudy on 111 asymptomatic term in-fants who underwent routine mag-netic resonance imaging shortly afterdelivery found that infants deliveredafter a failed vacuum extraction werethe most likely to have a subduralhemorrhage with a rate of approxi-mately 28% versus 6% after sponta-neous vaginal delivery and 8% after asuccessful vacuum delivery.61
Routine Use of Antibiotics at theTime of Assisted Vaginal DeliveryThere is insufficient evidence to sup-port the routine administration of an-tibiotic prophylaxis during assistedvaginal deliveries to prevent postpar-tum infection. A retrospective reviewof 393 women compared the rates ofendomyometritis among women de-livered by vacuum or forceps, andfound no statistical difference in therates of infection or the length of hos-pitalization among those who re-ceived prophylactic antibiotics andthose who did not.62 As such, the rou-tine use of antibiotic prophylaxis atthe time of operative vaginal deliverycannot be recommended.
Use of Episiotomy at the Time of Assisted Vaginal DeliveryEpisiotomy refers to a surgicalincision in the perineum designed toenlarge the vagina and assist inchildbirth. Although episiotomy hasoften accompanied operative vaginal
Neonates may be discharged 10 or more hours after vacuum delivery if nocomplications are evident.
delivery, recent evidence suggeststhat routine use of episiotomy withvacuum extraction is associated withan increased rather than decreasedrisk of perineal trauma and rectal in-juries.63,64 Episiotomy during opera-tive vaginal delivery also increasesthe incidence of postpartum hemor-rhage and perineal infection, the needfor stronger analgesia, and neonatalbirth trauma.63 Moreover, pressureexerted by the soft tissues of thepelvic floor promotes flexion and ro-tation of the fetal head as it descendsthrough the birth canal, which willnot be possible if these tissues havebeen surgically transected. Taken to-gether, these data suggest that routineepisiotomy during vacuum extractionshould be discouraged.
Routine Use of Vacuum ExtractionDuring Cesarean DeliveryVacuum devices can be used at thetime of cesarean delivery to effect de-livery of a high unengaged fetal heador as an alternative to extension ofthe hysterotomy when delivery of thevertex is difficult. Once the head is
visible through the uterine incision,the vacuum device can be applieddirectly to the vertex and deliveryachieved with gentle upward tractionin concert with fundal pressure.Although such an approach mayreduce the risk of extension of the
original hysterotomy, it is not recom-mended for all cesarean deliveries.
ConclusionsApproximately 5% (1 in 20) of all de-liveries in the United States are oper-ative vaginal deliveries. There is anincreasing trend toward the use ofvacuum devices rather than forcepsfor such procedures due, at least inpart, to mounting data suggestingthat vacuum extraction is associatedwith less maternal morbidity. Tosafely perform a vacuum delivery, it isimportant that the operator under-stand the indications and contraindi-
cations for this procedure. As a gen-eral rule, the soft (bell-shaped) cupsshould be used for uncomplicatedocciput-anterior deliveries, whereasthe rigid M cups should be reservedfor more complicated deliveries suchas those involving larger infants, sig-
nificant caput succedaneum, occiput-posterior position, or asynclitism.Informed patient consent must beobtained. With appropriate trainingand careful patient selection, vacuum-assisted vaginal delivery can be avaluable tool in the armamentariumof the practicing obstetric careprovider to effect delivery of an at-risk fetus. In all instances, the poten-tial risks and benefits of a vacuum-assisted delivery must be weighedagainst the available alternative,including continued expectant man-agement, oxytocin augmentation, andcesarean delivery.
Main Points• An operative vaginal delivery should only be performed if there is an appropriate indication. No indication is absolute because
the option of cesarean delivery is always available.
• A number of clinical situations exist in which operative vaginal delivery should not be attempted because of the potential risksto the fetus.
• A series of criteria all need to be fulfilled before an operative vaginal delivery can be attempted.
• Selection of the appropriate instrument depends on both the clinical situation and the operator’s level of comfort and experiencewith the specific instrument.
• Soft bell-shaped cups are associated with fewer scalp injuries and no increased risk of maternal perineal injury.
• Soft bell-shaped cups should be considered for straightforward occiput-anterior deliveries and rigid M cups should be reserved formore complicated deliveries.
• A successful vacuum-assisted vaginal delivery is dependent on several factors, including patient selection and a number oftechnical considerations. The goal is correct placement of the vacuum cup on the fetal scalp, application of a vacuum of up to0.8 kg/cm2 to suck part of the scalp into the cup and create an artificial caput succedaneum (known as a chignon), and thenapplication of a traction force to the fetus in concert with uterine contractions to expedite delivery.
• There is evidence that instrumental deliveries increase maternal morbidity. The risk of maternal injury is much higher with forcepscompared with vacuum-assist devices.
• Vacuum-assisted vaginal deliveries can cause significant fetal morbidity. Pediatricians should be notified whenever an operativevaginal delivery has been attempted.
With appropriate training and careful patient selection, vacuum-assistedvaginal delivery can be a valuable tool in the armamentarium of the prac-ticing obstetric care provider to effect delivery of an at-risk fetus.
References1. Martin JA, Hamilton EB, Sutton PD, et al. Cen-
ters for Disease Control and Prevention NationalCenter for Health Statistics National Vital Statis-tics System. Births: final data for 2002. NatlVital Stat Rep. 2007;56:1-103.
2. Clark SL, Belfort MA, Hankins GD, et al. Varia-tion in the rates of operative delivery in theUnited States. Am J Obstet Gynecol. 2007;196:526.e1-5.
4. The American College of Obstetricians and Gy-necologists (ACOG). Operative Vaginal Delivery.Washington, DC: ACOG; 2000. Practice BulletinNo. 17.
5. Malmström T. The vacuum extractor: an obstet-rical instrument. Acta Obstet Gynecol Scand.1957;36:5-50.
6. Attilakos G, Sibanda T, Winter C, et al. A ran-domised controlled trial of a new handheld vac-uum extraction device. BJOG. 2005;112:1510-1515.
7. Cohen WR. Influence of the duration of secondstage labor on perinatal outcome and puerperalmorbidity. Obstet Gynecol. 1977;49:266-269.
8. Myles TD, Santolaya J. Maternal and neonataloutcomes in patients with a prolonged secondstage of labor. Obstet Gynecol. 2003;102:52-58.
9. Gerber S, Vial Y, Hohlfield P. Maternal andneonatal prognosis after a prolonged secondstage of labor [in French]. J Gynecol Obstet BiolReprod (Paris). 1999;28:145-150.
10. Macones GA, Hankins GD, Spong CY, et al. The2008 National Institute of Child Health andHuman Development workshop report on elec-tronic fetal monitoring: update on definitions,interpretation, and research guidelines. ObstetGynecol. 2008;112:661-666.
11. Gei AF, Belfort MA. Forceps-assisted vaginal de-livery. Obstet Gynecol Clin North Am. 1999;26:345-370.
12. Lucas MJ. The role of vacuum extraction in mod-ern obstetrics. Clin Obstet Gynecol. 1994;37:794-805.
13. Thiery M. Fetal hemorrhage following bloodsamplings and use of vacuum extractor. Am JObstet Gynecol. 1979;134:231.
14. Roberts IF, Stone M. Fetal hemorrhage: compli-cation of vacuum extractor after fetal bloodsampling. Am J Obstet Gynecol. 1978;132:109.
15. Kolderup LB, Laros RK Jr, Musci TJ. Incidence ofpersistent birth injury in macrosomic infants:association with mode of delivery. Am J ObstetGynecol. 1997;177:37-41.
16. Chestnut DH, Vandewalker GE, Owen CL, et al.The influence of continuous epidural bupiva-caine analgesia on the second stage of labor andmethod of delivery in nulliparous women. Anes-thesiology. 1987;66:774-780.
17. Gupta JK, Hofmeyr GJ. Position for women dur-ing second stage of labour. Cochrane DatabaseSyst Rev. 2004;(1):CD002006.
18. Roberts CL, Algert CS, Cameron CA, Torvaldsen S.A meta-analysis of upright positions in thesecond stage to reduce instrumental deliveries inwomen with epidural analgesia. Acta ObstetGynecol Scand. 2005;84:794-798.
36. Vacca A. Vacuum-assisted delivery: an analysisof traction force and maternal and neonataloutcomes. Aust N Z J Obstet Gynaecol. 2006;46:124-127.
37. Bofill JA, Rust OA, Schorr SJ, et al. A random-ized trial of two vacuum extraction techniques.Obstet Gynecol. 1997;89:758-762.
38. Murphy DJ, Liebling RE, Patel R, et al. Cohortstudy of operative delivery in the second stage oflabour and standard of obstetric care. BJOG.2003;110:610-615.
39. Sjöstedt JE. The vacuum extractor and forceps inobstetrics. A clinical study. Acta Obstet GynecolScand. 1967;46(suppl 10):1-208.
40. Johanson RB, Rice C, Doyle M, et al. A ran-domised prospective study comparing the newvacuum extractor policy with forceps delivery.Br J Obstet Gynaecol. 1993;100:524-530.
41. Dell DL, Sightler SE, Plauché WC. Soft cup vac-uum extraction: a comparison of outlet delivery.Obstet Gynecol. 1985;66:624-628.
42. Angioli R, Gomez-Marin O, Cantuaria G, O’SullivanMJ. Severe perineal lacerations during vaginaldelivery: the University of Miami experience.Am J Obstet Gynecol. 2000;182:1083-1085.
44. Damron DP, Capeless EL. Operative vaginal de-livery: a comparison of forceps and vacuum forsuccess rate and risk of rectal sphincter injury.Am J Obstet Gynecol. 2004;191:907-910.
45. Wu JM, Williams KS, Hundley AF, et al. Occiputposterior fetal head position increases the risk ofanal sphincter injury in vacuum-assisted deliver-ies. Am J Obstet Gynecol. 2005;193:525-528;discussion 528-529.
46. Johanson RB, Heycock E, Carter J, et al. Maternal and child health after assisted vaginaldelivery: five-year follow up of a randomizedcontrolled study comparing forceps and ventouse. Br J Obstet Gynaecol. 1999;106:544-549.
47. Bashore RA, Phillips WH Jr, Brinkman CR 3rd. Acomparison of the morbidity of midforceps andcesarean delivery. Am J Obstet Gynecol. 1990;162:1428-1434; discussion 1434-1435.
48. Liebling RE, Swingler R, Patel RR, et al. Pelvicfloor morbidity up to one year after difficultinstrumental delivery and cesarean section in thesecond stage of labor: a cohort study. Am J Obstet Gynecol. 2004;191:4-10.
49. Bahl R, Strachan B, Murphy DJ. Pelvic floormorbidity at 3 years after instrumental deliveryand cesarean delivery in the second stage oflabor and the impact of a subsequent delivery.Am J Obstet Gynecol. 2005;192:789-794.
50. Robertson PA, Laros RK Jr, Zhao RL. Neonataland maternal outcome in low-pelvic and mid-pelvic operative deliveries. Am J Obstet Gynecol.1990;162:1436-1442; discussion 1442-1444.
51. Emerson MV, Peiramici DJ, Stoessel KM, et al.Incidence and rate of disappearance of retinalhemorrhage in newborns. Ophthalmology. 2001;108:36-39.
52. Towner D, Castro MA, Eby-Wilkens E, Gilbert WM.Effect of mode of delivery in nulliparous women
19. Hodnett ED, Gates S, Hofmeyr GJ, Skala C. Con-tinuous support for women during childbirth.Cochrane Database Syst Rev. 2003;(3):CD003766.
20. Hansen SL, Clark SL, Foster JC. Active pushingversus passive fetal descent in the second stageof labor: a randomized controlled trial. ObstetGynecol. 2002;99:29-34.
21. Norwitz ER, Robinson JN, Repke JT. Labor anddelivery. In: Gabbe SG, Niebyl JR, Simpson JL,eds. Obstetrics: Normal and Problem Pregnan-cies. 4th ed. New York: W.B. Saunders Company;2001:353-394.
22. The American College of Obstetricians and Gy-necologists (ACOG). Operative Vaginal Delivery.Washington, DC: ACOG; 1994. Technical BulletinNo. 196.
23. Akmal S, Kametas N, Tsoi E, et al. Comparison oftransvaginal digital examination with intra-partum sonography to determine fetal head po-sition before instrumental delivery. UltrasoundObstet Gynecol. 2003;21:437-440.
25. Greenberg JA. Procedure for vacuum assistedoperative vaginal delivery. UpToDate Web site.http://www.uptodate.com/patients/content/topic.do?topicKey=~cWABY9RJfJlwne. Accessed Feb-ruary 3, 2009.
26. Johanson R, Menon V. Soft versus rigid vacuumextractor cups for assisted vaginal delivery.Cochrane Database Syst Rev. 2000;(2):CD000446.
27. Hayman R, Gilby J, Arulkumaran S. Clinicalevaluation of a “hand pump” vacuum deliverydevice. Obstet Gynecol. 2002;100:1190-1195.
28. Muise KL, Duchon MA, Brown RH. Effect of an-gular traction on the performance of modernvacuum extractors. Am J Obstet Gynecol. 1992;167:1125-1129.
29. Muise KL, Duchon MA, Brown RH. The effect ofartificial caput on performance of vacuum ex-tractors. Obstet Gynecol. 1993;81:170-173.
30. Hayman R, Gilby J, Arulkumaran S. Clinicalevaluation of a “hand pump” vacuum deliverydevice. Obstet Gynecol. 2002;100:1190-1195.
31. Groom KM, Jones BA, Miller N, Paterson-Brown S. A prospective randomized controlledtrial of the Kiwi OmniCup versus conventionalventouse cups for vacuum-assisted vaginaldelivery. BJOG. 2006;113:183-189.
32. Ismail NA, Saharan WS, Zeleha MA, et al. KiwiOmniCup versus Malmström metal cup in vacuumassisted delivery: a randomized comparative trial.J Obstet Gynaecol Res. 2008;34:350-353.
33. Lim FT, Holm JP, Schuitemaker NW, et al. Step-wise compared with rapid application of vacuumin ventouse extraction procedures. Br J ObstetGynaecol. 1997;104:33-36.
34. Svenningsen L. Birth progression and tractionforces developed under vacuum extraction afterslow or rapid application of suction. Eur J ObstetGynecol Reprod Biol. 1987;26:105-112.
54. Center for Devices and Radiological Health. FDAPublic Health Advisory: Need for CAUTION whenusing vacuum assisted delivery devices. May 21,1998. http://www.fda.gov/cdrh/fetal598.html.Accessed January 17, 2009.
55. Ross MG, Fresquez M, El-Haddad MA. Impact ofFDA advisory on reported vacuum-assisted de-livery and morbidity. J Matern Fetal Med. 2000;9:321-326.
56. Carmody F, Grant A, Mutch L, et al. Follow up ofbabies delivered in a randomized controlledcomparison of vacuum extraction and forceps
57. Ngan HY, Miu P, Ko L, Ma HK. Long-term neu-rological sequelae following vacuum extractordelivery. Aust N Z J Obstet Gynaecol. 1990;30:111-114.
58. Revah A, Ezra Y, Farine D, Ritchie K. Failed trialof vacuum or forceps—maternal and fetal out-come. Am J Obstet Gynecol. 1997;176:200-204.
59. Ezenagu LC, Kakaria R, Bofill JA. Sequential use ofinstruments at operative vaginal delivery: is it safe?Am J Obstet Gynecol. 1999;180:1446-1449.
60. Gardella C, Taylor M, Benedetti T, et al. The ef-fect of sequential use of vacuum and forceps forassisted vaginal delivery on neonatal and mater-nal outcomes. Am J Obstet Gynecol. 2001;185:896-902.
61. Whitby EH, Griffiths PD, Rutter S, et al.Frequency and natural history of subduralhemorrhages in babies and relation to obstetricfactors. Lancet. 2004;363:846-851.
62. Liabsuetrakul T, Choobun T, Peeyananjarassri K,Islam M. Antibiotic prophylaxis for operativevaginal delivery. Cochrane Database Syst Rev.2004;(3):CD004455.
63. Kudish B, Blackwell S, Mcneeley SG, et al.Operative vaginal delivery and midline epi-siotomy: a bad combination for the perineum.Am J Obstet Gynecol. 2006;195:749-754.
64. Robinson JN, Norwitz ER, Cohen AP, et al.Episiotomy, operative vaginal delivery, andsignificant perinatal trauma in nulliparouswomen. Am J Obstet Gynecol. 1999;181:1180-1184.