Validation of a simple method for measuring cranial deformities (plagiocephalometry) Léon N.A. van Adrichem 1 Leo A. van Vlimmeren 2 Dominika Cadanová 1 Paul J.M. Helders 3 Raoul H.H. Engelbert 3 Han J.W. van Neck 1 Anton H.J. Koning 4 1 Department of Plastic and Reconstructive Surgery, Erasmus University Medical Center Rotterdam, Sophia Children's Hospital, Rotterdam 2 Department of Physical Therapy, Bernhoven Hospital, Veghel 3 Department of Pediatric Physical Therapy and Exercise Physiology, University Medical Center; Wilhelmina Children's Hospital, Utrecht 4 Erasmus Center for Bioinformatics, Erasmus University Medical Center, Rotterdam The Netherlands Submitted for publication Chapter 5 Chapter 5 Chapter 5 Chapter 5
Transcript
Validation of a simple method for measuring cranial deformities (plagiocephalometry)
Léon N.A. van Adrichem1
Leo A. van Vlimmeren2
Dominika Cadanová1
Paul J.M. Helders3
Raoul H.H. Engelbert3
Han J.W. van Neck1
Anton H.J. Koning4
1Department of Plastic and Reconstructive Surgery,
Erasmus University Medical Center Rotterdam,
Sophia Children's Hospital, Rotterdam 2Department of Physical Therapy,
Bernhoven Hospital, Veghel 3Department of Pediatric Physical Therapy and
Exercise Physiology, University Medical Center;
Wilhelmina Children's Hospital, Utrecht 4Erasmus Center for Bioinformatics,
Erasmus University Medical Center, Rotterdam
The Netherlands
Submitted for publication
Chapter 5 Chapter 5 Chapter 5 Chapter 5
Abstract
Context
Craniofacial measuring is essential for diagnosis or evaluation of growth and therapies. Skull
deformities in children are mainly caused by craniosynostosis or by external pressure in
positional skull deformations. Traditional anthropometry does not sufficiently analyse
craniofacial shape. In CT scanning radiation loads are considerable and both CT and MRI
scanning, due to their long acquisition time, require anaesthesia in children if an accurate
picture is needed. This makes CT and MRI unsuitable for long term follow up of paediatric
patients, unless there is a compelling reason to do so. Other non-invasive 3D surface scanners
still have limited practical use.
Van Vlimmeren et al. presented plagiocephalometry as a simple and versatile instrument to
quantify skull deformities and reliability was proven by high intrarater and interrater reliability,
but concurrent validity was not investigated.
Objective
To explore concurrent validity of plagiocephalometry and 3D-CT scanning, being the golden
standard of 3D monitoring, including correlations and clinical agreement between the scores of
both measurements.
Methods
At the Erasmus University Medical Center Rotterdam, Sophia Children’s Hospital
plagiocephalometry was compared to 3D-CT scanning in 21 children with craniosynostosis early
in life, in order to investigate concurrent validity of plagiocephalometry.
Results
The plagiocephalometry ring proved to fit closely to the skin with mean differences less than 1
mm (p<0.05). The shape of the plagiocephalometry ring was not significantly changed when
taken off the head (p>0.05). Finally no significant differences are shown between
measurements on the skull (CT-scan) and plagiocephalometry ring off the head (p>0.05).
Conclusions
The study supports concurrent validity of the measurements for all of the explorations:
plagiocephalometry fitting to the skin, retaining plagiocephalometry shape off the head and
correspondance of the actual asymmetry of the skull as acquired by plagiocephalometry and CT
scanning. Plagiocephalic measurements are in agreement with the measurements from 3D-CT
scanning, the present golden standard.
Although only 2 dimensional measurements are done by plagiocephalometry, the combination
of simplicity, reliability and validity make it a promising tool for daily practice.
68
Introduction Measurement of craniofacial structures is essential for the diagnosis or evaluation of growth
and subsequent intervention. Skull deformities in children are mainly caused by craniosynostosis
or by external pressure in positional skull deformations.
In traditional anthropometry, distances and angles are measured, but shape is not recorded.
Furthermore, on the skull, especially in the deformed skull, no clear landmarks are present.
Young children are lively, which complicates anthropometry. Plain X-rays of the skull do
visualize cranial sutures, but shape is not sufficiently recorded.1
Ideally, sequential, complete 3D craniofacial pictures should be obtained. In CT scanning,
radiation loads are considerable and both CT and MRI scanning, due to their long acquisition
time, require anaesthesia in children if an accurate picture is needed.2-4 This makes CT and MRI
unsuitable for long term follow up of paediatric patients, unless there is a compelling reason to
do so.
Non-invasive 3D surface scanning might be a good solution, but although numerous articles
using various forms of 3D surface data acquisition have been described since the late 70's,
these methods are of limited practical use. The acquisition time of these devices is in the range
of several seconds, not sufficiently short to capture a highly mobile child. Three-D
photogrammetry, however, is accurate, fast, non contact and non-invasive and is a promising
system to obtain sequential complete 3D surface data.5 Disadvantages are the price and the size
of this system, so acquisition can only be done in specialized centres.
Van Vlimmeren et al.6 recently presented a simple and versatile instrument to quantify skull
deformities: Plagiocephalometry (PCM). PCM is performed with a strip of thermoplastic
material, which is positioned around the infant’s head at the widest transverse circumference.
Landmarks of the ear and the nose bridge are traced. PCM turned out to be easy applicable,
non-invasive at low costs, while intrarater and interrater reliability were high as illustrated by
intraclass correlations and limits of agreement.6 Although the method is 2D, sufficient
information was obtained by PCM to quantify the skull deformities.
Present study was performed to explore concurrent validity of PCM and 3D-CT scanning, being
the golden standard of 3D monitoring, including correlations and clinical agreement between
the scores of both measurements.
The aim of this study was:
1. To investigate how closely the thermoplastic strip of PCM fits to the skin.
2. To investigate whether the thermoplastic strip of PCM retains its shape after taking it off
the infants head.
3. To determine to what extends the asymmetry, as acquired from the thermoplastic PCM ring,
corresponds with the actual asymmetry of the skull as acquired from 3D-CT scanning.
Chapter 5
69
Patients and methods
Patients
All measurements were performed at the Erasmus University Medical Center Rotterdam, Sophia
Children’s Hospital, from September 2004, till March 2005. All of 21 included patients were
scheduled for 3D-CT scanning of the head due to a serious suspicion of existing
craniosynostosis (age in months: mean 12.6 +/- 12.7; median 10,5; minimum 3.8; maximum
62,7). The parents agreed that PCM with a thermoplastic strip was performed simultaneously.
No children with positional skull deformations were included, because in these patients CT
scanning is redundant and not ethical due to anaesthesia.
Methods
Plagiocephalometry is performed with a strip of thermoplastic material (3.2 mm thick) of 18 mm
x 50 cm (Thermo extra-comfort, non-perfo by GeniMedical, the Netherlands), which is
positioned around the infant’s head at the widest transverse circumference. In less than two
minutes, the ring is fixed and the three landmarks (both ears and nose) are marked
perpendicular on the ring in a standardized manner. Both landmarks at the posterior edge of
the tragus, correspond best with the meatus acousticus externus. The third landmark is traced
off at the middle of the nose bridge. In this way it is possible to trace the exact positions of the
ears and the nose in relation to the transverse circumference and contours of the head.
Afterwards, the ring is removed from the head and a fourth landmark is marked representing
the middle of the posterior circumferential distance between the left and right ear, measured
with a measuring tape. Using a standard copying machine, the upper side of the ring is copied
on paper. Nine lines are drawn on the paper copy and measured to the nearest millimetre, by
which the degree of asymmetry can simply be determined by calculating the differences
between the lengths of the left and right lines. The clinically most important measures are
arranged in three parts:6
Part 1. Position of the ears, nose and local flattening of the skull.
Part 2. Diameter difference: Oblique diameter difference (ODD). The oblique diameter left (ODL)
and oblique diameter right (ODR) lines are drawn from points located 40o either side of the
antero-posterior (AP) line. The ODD is calculated as ODL– ODR. The angle of 40o is chosen
because this has been used by other authors formerly, probably because the differences
between the diameters of the typical shape of the skull at these angles are the most
outstanding.7 The ratio between the ODL and the ODR is calculated as the longest/shortest
diameter x 100% and is called oblique diameter difference index (ODDI).
Part 3. Transversal shape and proportion of the skull.
The ratio between the sinistra-dextra (SD) and the anterior-posterior (AP) is calculated as SD/AP
x 100%, and is called the cranio proportional index (CPI) (Fig. 1-2).
70
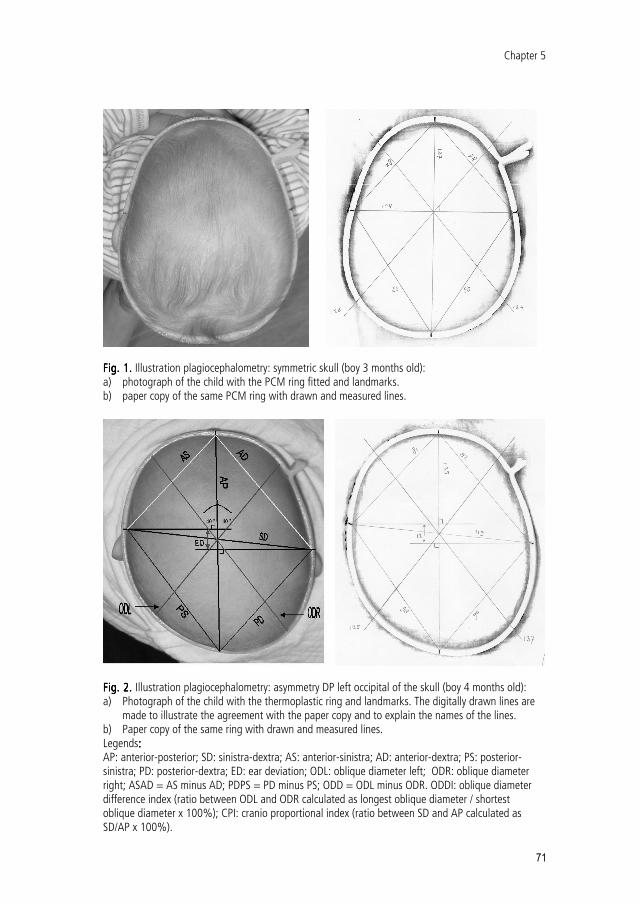
Fig. 1.Fig. 1.Fig. 1.Fig. 1. Illustration plagiocephalometry: symmetric skull (boy 3 months old): a) photograph of the child with the PCM ring fitted and landmarks. b) paper copy of the same PCM ring with drawn and measured lines.
Fig. 2. Fig. 2. Fig. 2. Fig. 2. Illustration plagiocephalometry: asymmetry DP left occipital of the skull (boy 4 months old): a) Photograph of the child with the thermoplastic ring and landmarks. The digitally drawn lines are
made to illustrate the agreement with the paper copy and to explain the names of the lines. b) Paper copy of the same ring with drawn and measured lines. Legends: : : : AP: anterior-posterior; SD: sinistra-dextra; AS: anterior-sinistra; AD: anterior-dextra; PS: posterior-sinistra; PD: posterior-dextra; ED: ear deviation; ODL: oblique diameter left; ODR: oblique diameter right; ASAD = AS minus AD; PDPS = PD minus PS; ODD = ODL minus ODR. ODDI: oblique diameter difference index (ratio between ODL and ODR calculated as longest oblique diameter / shortest oblique diameter x 100%); CPI: cranio proportional index (ratio between SD and AP calculated as SD/AP x 100%).
Chapter 5
71
Medical Student (DC) was trained to measure PCM using a standardized protocol. Prior to CT
scanning the PCM ring was obtained. During CT scanning the PCM ring was in place. After CT
scanning the PCM ring was copied on paper, and finally all lines were drawn and the distances
were measured in millimetres.
Three-D-CT scanning was performed at the radiology department of the Erasmus University
Medical Center Rotterdam, Sophia Children’s Hospital. All of the children were under general
anaesthesia. The CT scanner equipment was Siemens Emotion 6; a slice thickness of 2.5 mm
with an interslice distance of 1.2 mm was used (Fig. 3). The 3D-CT data sets were imported into
“I-Space” at the Department of Bioinformatics of the Erasmus University Medical Center
Rotterdam. The “I-Space” is a CAVETM-like virtual reality system with 3D-processing tools.8
I-Space, equipped with 3D volume rendering software, uses eight projectors on three walls and
the floor, to create a true 3D image in a special viewing arena.9 Users can then interact with the
image using a 6 degrees-of-freedom pointing device, and investigate the 3D data wearing a
pair of glasses with polarizing lenses. The person interacting with the data is presented with the
correct perspective by means of wireless head tracking.
In I-Space the plane of the PCM ring was determined visually by rotating and clipping the
volume. In this plane the same ear and nose markers of the PCM method were placed on the
bone and visually checked for accuracy by looking at the volume from different angles. After
this, a screen dump was made and printed on A4 size paper, closely cropped on the skull. All
the measurements described in the PCM part were performed on the bone.
To investigate how close the PCM ring fits to the skin and the underlying bone, the distance
between the PCM ring and the skin, and the distance between the PCM ring and the bone were
measured at positions of 0o, 45o, 90o, 135o, 180o, 225o, 270 o, 315 o (Fig. 4). A difference of 1
mm between the skin and the PCM ring was defined as an acceptable difference due to the
interposing of hair, based on clinical findings in children of 1 year of age. At the 8 angles the
distance was measured with a ruler between the centre (crossing of the anterior-posterior and
sinistra-dextra lines) and the PCM ring on the head, the PCM ring off the head, the bone and
the skin. In a pilot study the method appeared to be reproducible.
Statistical analysis
All the obtained data were registered and statistically analysed by making use of the Statistical
Program for the Social Sciences version 12.0.1 (SPSS). The T-test has been used for determining
the significance of the obtained data.
72
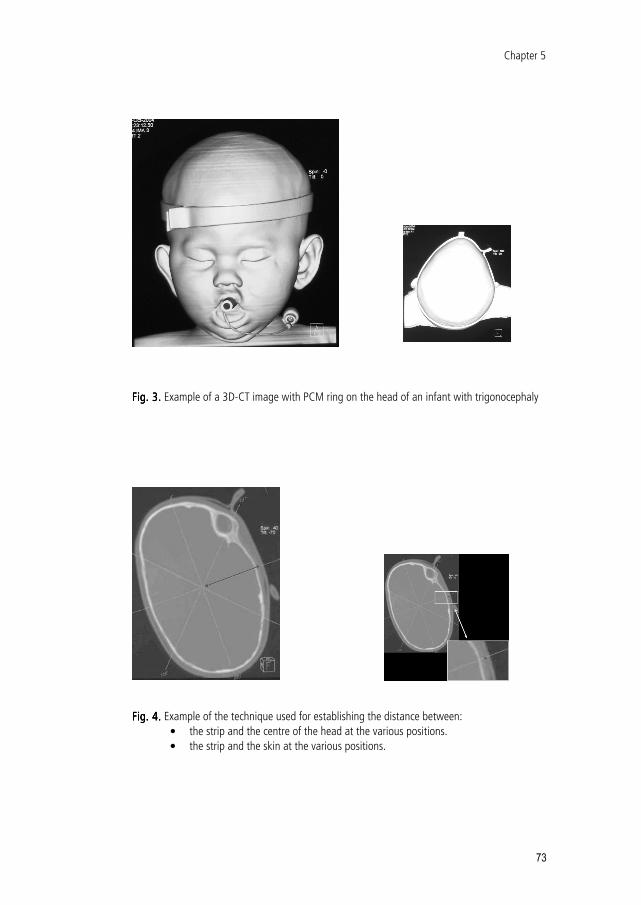
FFFFig. 3.ig. 3.ig. 3.ig. 3. Example of a 3D-CT image with PCM ring on the head of an infant with trigonocephaly
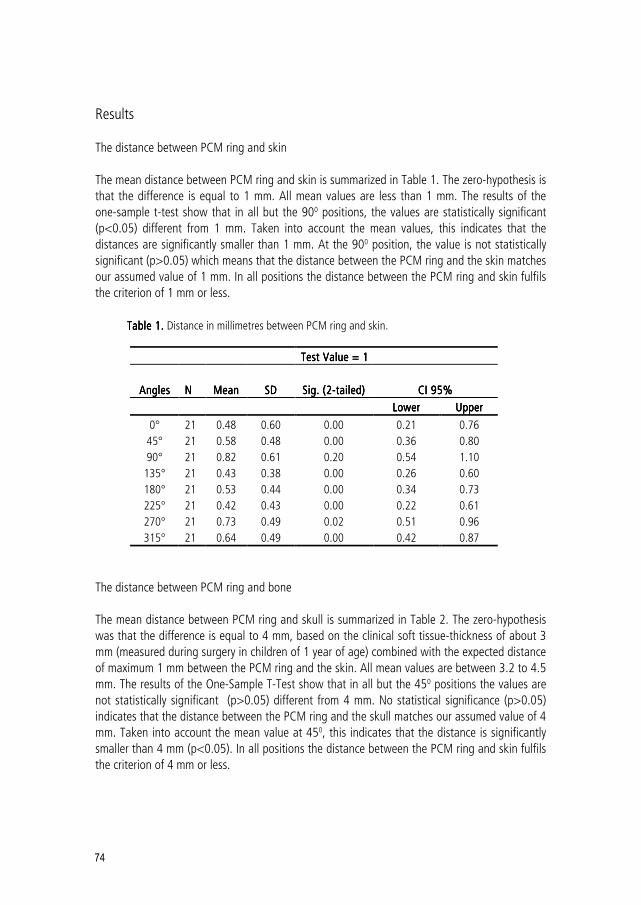
Fig. 4.Fig. 4.Fig. 4.Fig. 4. Example of the technique used for establishing the distance between:
• the strip and the centre of the head at the various positions.
• the strip and the skin at the various positions.
Chapter 5
73
Results
The distance between PCM ring and skin
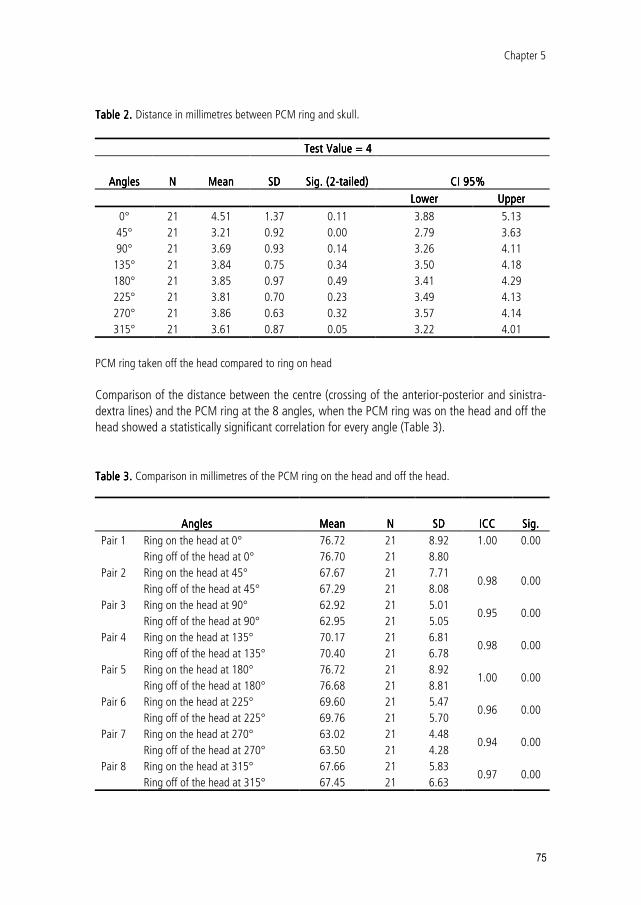
The mean distance between PCM ring and skin is summarized in Table 1. The zero-hypothesis is
that the difference is equal to 1 mm. All mean values are less than 1 mm. The results of the
one-sample t-test show that in all but the 900 positions, the values are statistically significant
(p<0.05) different from 1 mm. Taken into account the mean values, this indicates that the
distances are significantly smaller than 1 mm. At the 900 position, the value is not statistically
significant (p>0.05) which means that the distance between the PCM ring and the skin matches
our assumed value of 1 mm. In all positions the distance between the PCM ring and skin fulfils
the criterion of 1 mm or less.
Table 1. Table 1. Table 1. Table 1. Distance in millimetres between PCM ring and skin.
Test Value = 1Test Value = 1Test Value = 1Test Value = 1
AnglesAnglesAnglesAngles
NNNN
MeanMeanMeanMean
SDSDSDSD
Sig. (2Sig. (2Sig. (2Sig. (2----tailed)tailed)tailed)tailed)
CI 95%CI 95%CI 95%CI 95%
LowerLowerLowerLower UpperUpperUpperUpper
0° 21 0.48 0.60 0.00 0.21 0.76
45° 21 0.58 0.48 0.00 0.36 0.80
90° 21 0.82 0.61 0.20 0.54 1.10
135° 21 0.43 0.38 0.00 0.26 0.60
180° 21 0.53 0.44 0.00 0.34 0.73
225° 21 0.42 0.43 0.00 0.22 0.61
270° 21 0.73 0.49 0.02 0.51 0.96
315° 21 0.64 0.49 0.00 0.42 0.87
The distance between PCM ring and bone
The mean distance between PCM ring and skull is summarized in Table 2. The zero-hypothesis
was that the difference is equal to 4 mm, based on the clinical soft tissue-thickness of about 3
mm (measured during surgery in children of 1 year of age) combined with the expected distance
of maximum 1 mm between the PCM ring and the skin. All mean values are between 3.2 to 4.5
mm. The results of the One-Sample T-Test show that in all but the 450 positions the values are
not statistically significant (p>0.05) different from 4 mm. No statistical significance (p>0.05)
indicates that the distance between the PCM ring and the skull matches our assumed value of 4
mm. Taken into account the mean value at 450, this indicates that the distance is significantly
smaller than 4 mm (p<0.05). In all positions the distance between the PCM ring and skin fulfils
the criterion of 4 mm or less.
74
Table 2. Table 2. Table 2. Table 2. Distance in millimetres between PCM ring and skull.
Test Value = 4Test Value = 4Test Value = 4Test Value = 4
AnglesAnglesAnglesAngles
NNNN
MeanMeanMeanMean
SDSDSDSD
Sig. (2Sig. (2Sig. (2Sig. (2----tailed)tailed)tailed)tailed)
CI 95% CI 95% CI 95% CI 95%
LowerLowerLowerLower UpperUpperUpperUpper
0° 21 4.51 1.37 0.11 3.88 5.13
45° 21 3.21 0.92 0.00 2.79 3.63
90° 21 3.69 0.93 0.14 3.26 4.11
135° 21 3.84 0.75 0.34 3.50 4.18
180° 21 3.85 0.97 0.49 3.41 4.29
225° 21 3.81 0.70 0.23 3.49 4.13
270° 21 3.86 0.63 0.32 3.57 4.14
315° 21 3.61 0.87 0.05 3.22 4.01
PCM ring taken off the head compared to ring on head
Comparison of the distance between the centre (crossing of the anterior-posterior and sinistra-
dextra lines) and the PCM ring at the 8 angles, when the PCM ring was on the head and off the
head showed a statistically significant correlation for every angle (Table 3).
Table 3.Table 3.Table 3.Table 3. Comparison in millimetres of the PCM ring on the head and off the head.
AnglesAnglesAnglesAngles
MeanMeanMeanMean
NNNN
SDSDSDSD
ICCICCICCICC
Sig.Sig.Sig.Sig.
Pair 1 Ring on the head at 0° 76.72 21 8.92
Ring off of the head at 0° 76.70 21 8.80
1.00 0.00
Pair 2 Ring on the head at 45° 67.67 21 7.71
Ring off of the head at 45° 67.29 21 8.08 0.98 0.00
Pair 3 Ring on the head at 90° 62.92 21 5.01
Ring off of the head at 90° 62.95 21 5.05 0.95 0.00
Pair 4 Ring on the head at 135° 70.17 21 6.81
Ring off of the head at 135° 70.40 21 6.78 0.98 0.00
Pair 5 Ring on the head at 180° 76.72 21 8.92
Ring off of the head at 180° 76.68 21 8.81 1.00 0.00
Pair 6 Ring on the head at 225° 69.60 21 5.47
Ring off of the head at 225° 69.76 21 5.70 0.96 0.00
Pair 7 Ring on the head at 270° 63.02 21 4.48
Ring off of the head at 270° 63.50 21 4.28 0.94 0.00
Pair 8 Ring on the head at 315° 67.66 21 5.83
Ring off of the head at 315° 67.45 21 6.63 0.97 0.00
Chapter 5
75
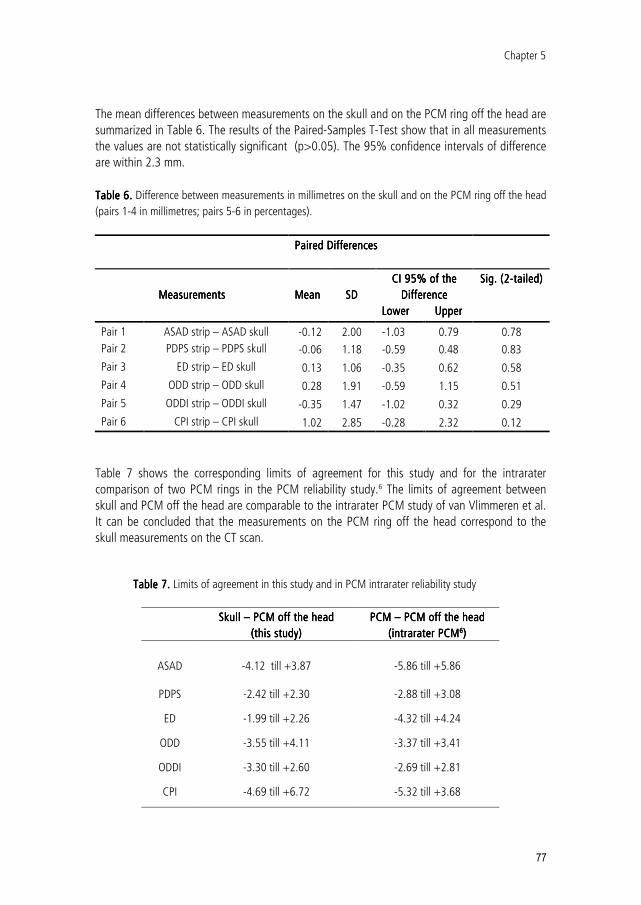
The mean differences between PCM ring on the head and off the head are summarized in Table
4. The results of the paired-samples t-test show that in all positions the values are not
statistically significant (p>0.05). The 95% confidence intervals of difference are within 1.2 mm.
So only a negligible shape difference occurs when the PCM ring is taken off the head
Table 4.Table 4.Table 4.Table 4. Difference in millimetres between PCM ring on and off the head.
1996;166:697-703. 4. Darling CF, Byrd SE, Allen ED, Radkowski MA, Wilczynski MA. Three-dimensional computed tomography
imaging in the evaluation of craniofacial abnormalities. J Natl Med Assoc 1994;86:676-680. 5. Riphage JM, van Neck JW, van Adrichem LNA. 30 Years of 3D surface imaging in medicine: A review of working
principles and implications for imaging the unsedated child. Submitted 2006. 6. van Vlimmeren LA, Takken T, van Adrichem LN, van der Graaf Y, Helders PJ, Engelbert RH. Plagiocephalometry:
a non-invasive method to quantify asymmetry of the skull; a reliability study. Eur J Pediatr 2006;165:149-157. 7. Hutchison BL, Hutchison LA, Thompson JM, Mitchell EA. Plagiocephaly and brachycephaly in the first two years
of life: a prospective cohort study. Pediatrics 2004;114:970-980. 8. Cruz-Neira C, Sandin DJ, DeFanti T. Surround-screen projection-based virtual reality: the design and
implementation of the CAVE. In SIGGRAPH ’93: Proceedings Association for Computing Machinery, August 1993.
9. Koning AHJ. Applications of volume rendering in the CAVE. In B. Enquist et al (eds.), Simulation and visualization on the grid: Paralleldatorcentrum, seventh annual conference, Stockholm, 2000, pp. 112-121.