Validity of Polymerase Chain Reaction Using Liquid Transport Media During a Pertussis Outbreak Cynthia Schulte, RN, BSN VPD Surveillance Officer Bureau of Immunization New York State Department of Health (NYSDOH)
Transcript
Validity of Polymerase Chain Reaction Using Liquid Transport
Media During a Pertussis Outbreak
Cynthia Schulte, RN, BSNVPD Surveillance OfficerBureau of Immunization
New York State Department of Health (NYSDOH)
Pertussis Laboratory Testing Bacterial culture
“Gold standard” Highly specific Prone to false negatives because organism is fastidious Early specimen collection, nasopharyngeal aspirate, proper
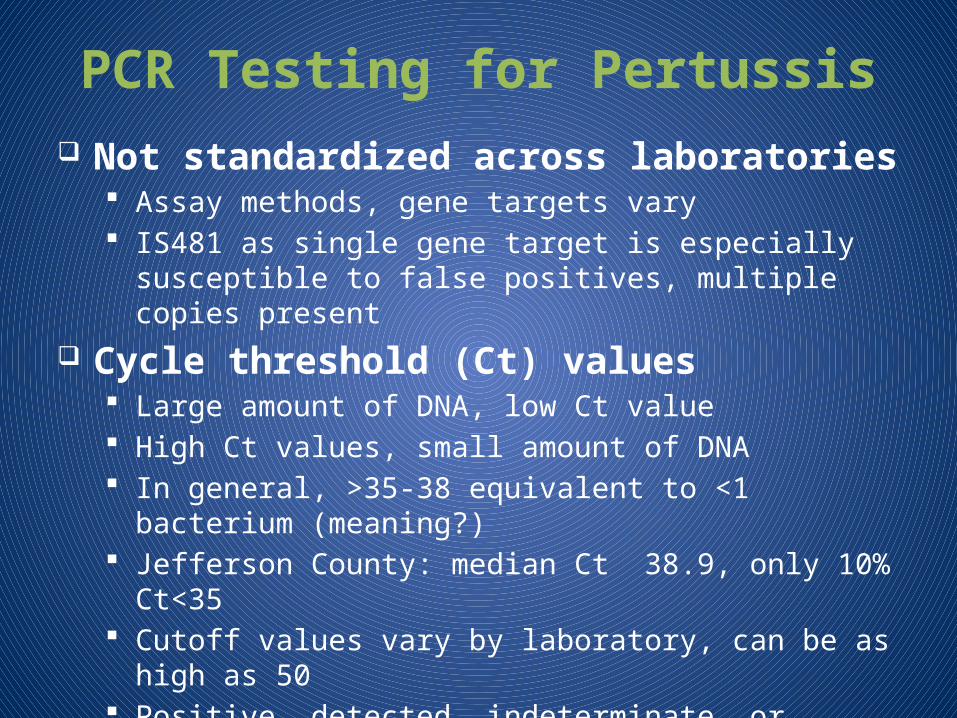
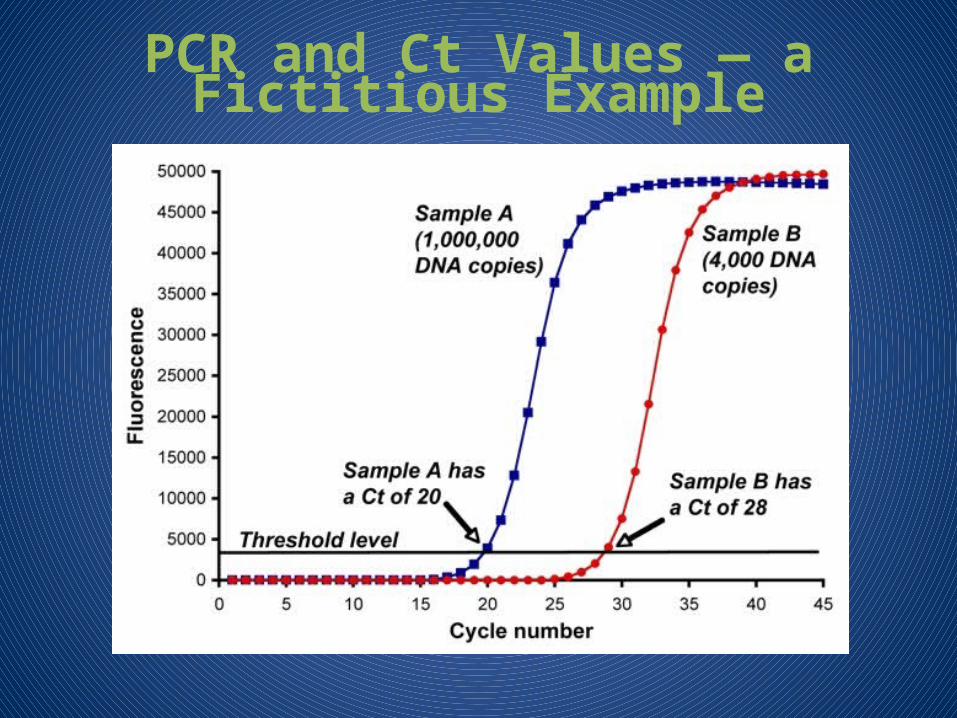
Large amount of DNA, low Ct value High Ct values, small amount of DNA In general, >35-38 equivalent to <1 bacterium (meaning?) Jefferson County: median Ct 38.9, only 10% Ct<35 Cutoff values vary by laboratory, can be as high as 50 Positive, detected, indeterminate, or equivocal
PCR and Ct Values — a Fictitious Example
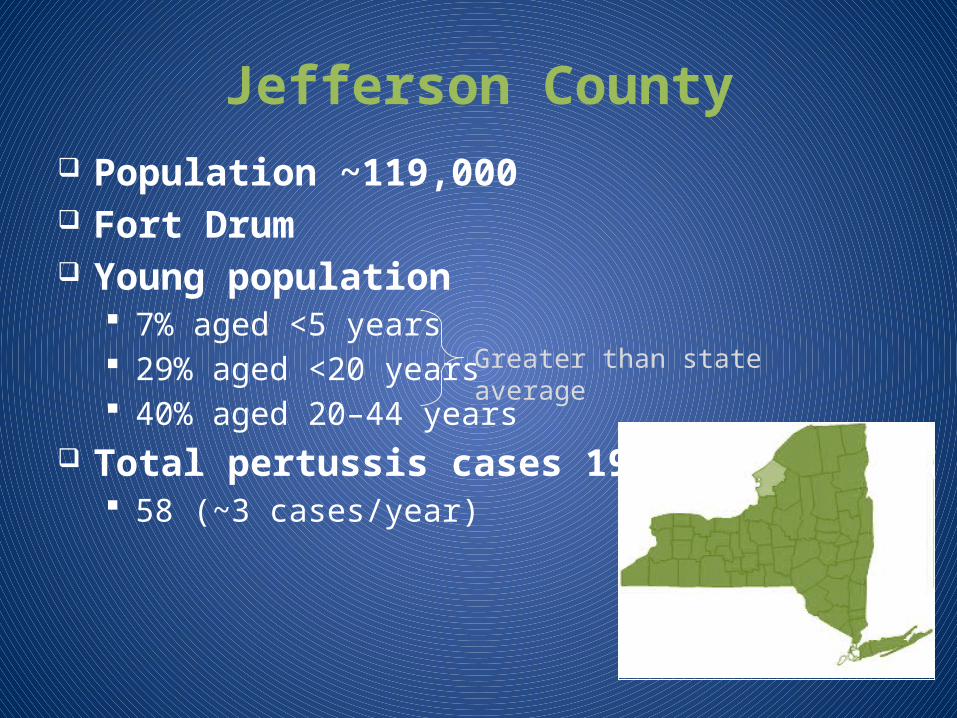
Jefferson County Population ~119,000 Fort Drum Young population
7% aged <5 years 29% aged <20 years 40% aged 20–44 years
Total pertussis cases 1992–2009 58 (~3 cases/year)
Greater than state average
Descriptive Epidemiology
542 PCR+ reports investigated 103 confirmed cases
53% male Median age 5 years (range 5 weeks to 58 years) Where vaccine status was known (N=93)
• 59% were age-appropriately vaccinated• 4% never vaccinated• 85% had minimum 3 DTaP doses required for school entry• 27% of patients ≥11 years had dose of Tdap
5 case patients hospitalized • 1 mo, 2 mo (2), 4 yr, and 6 yr• No deaths
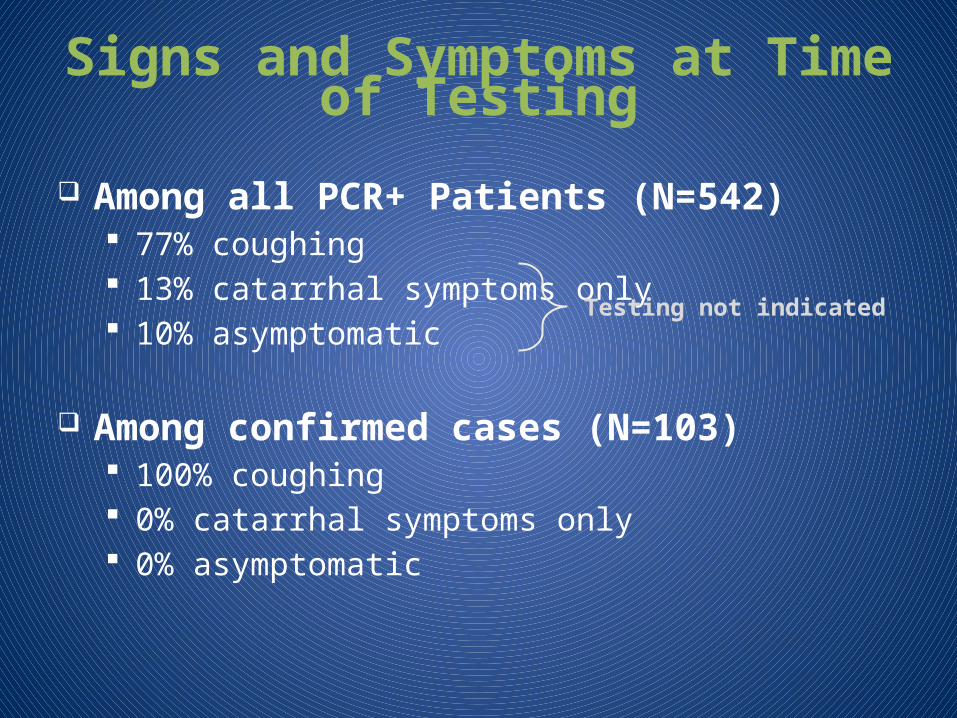
Signs and Symptoms at Time of Testing
Among all PCR+ Patients (N=542) 77% coughing 13% catarrhal symptoms only 10% asymptomatic
Among confirmed cases (N=103) 100% coughing 0% catarrhal symptoms only 0% asymptomatic
Testing not indicated
11/1
/201
0
11/8
/201
0
11/1
5/20
10
11/2
2/20
10
11/2
9/20
10
12/6
/201
0
12/1
3/20
10
12/2
0/20
10
12/2
7/20
10
1/3/
2011
1/10
/201
1
1/17
/201
1
1/24
/201
1
1/31
/201
10
20
40
60
80
100
120
140
160
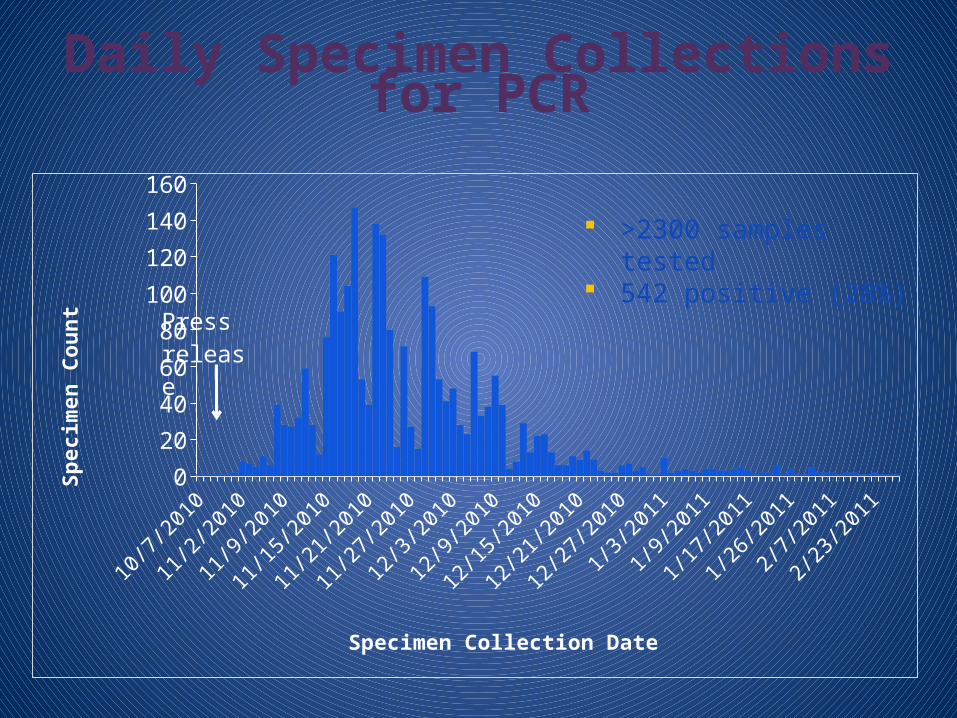
Specimen Collection Date
Sp
eci
men
Cou
nt Press re-
lease
Daily Specimen Collections for PCR
>2300 samples tested
542 positive (28%)
11/1
11/7
11/1
3
11/1
9
11/2
512
/112
/7
12/1
3
12/1
9
12/2
5
12/3
11/
61/
121/
180
10
20
30
40
50
60
70
80
90
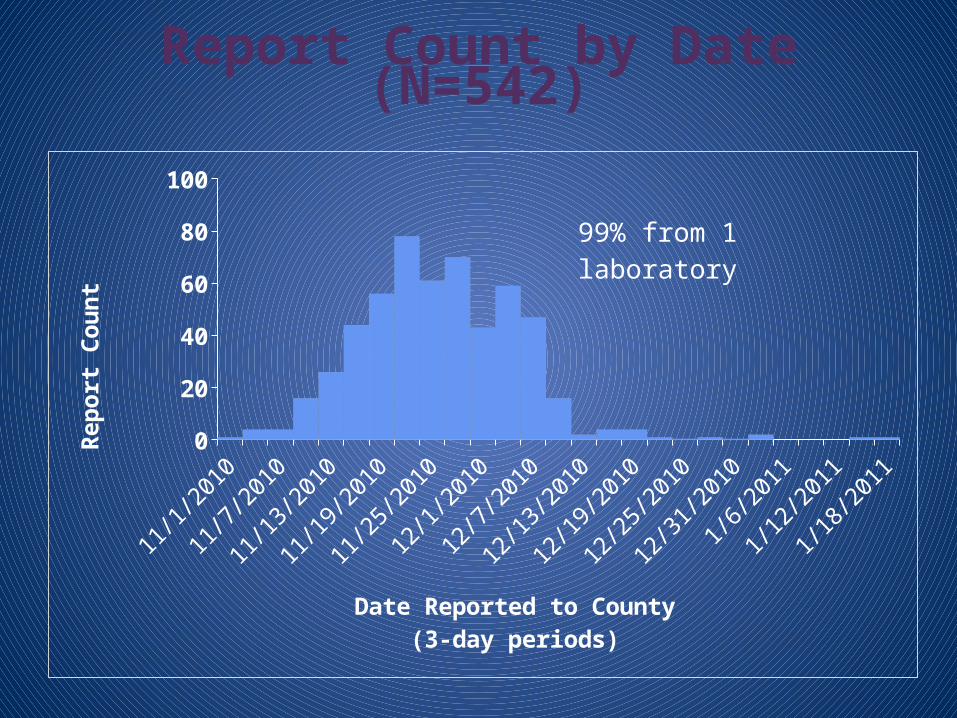
Date Reported to County(3-day periods)
Rep
ort
Cou
nt
99% from 1 laboratory
Report Count by Date (N=542)
10/1
10/7
10/1
3
10/1
9
10/2
5
10/3
111
/6
11/1
2
11/1
8
11/2
4
11/3
012
/6
12/1
2
12/1
8
12/2
40
2
4
6
8
10
12
14
16
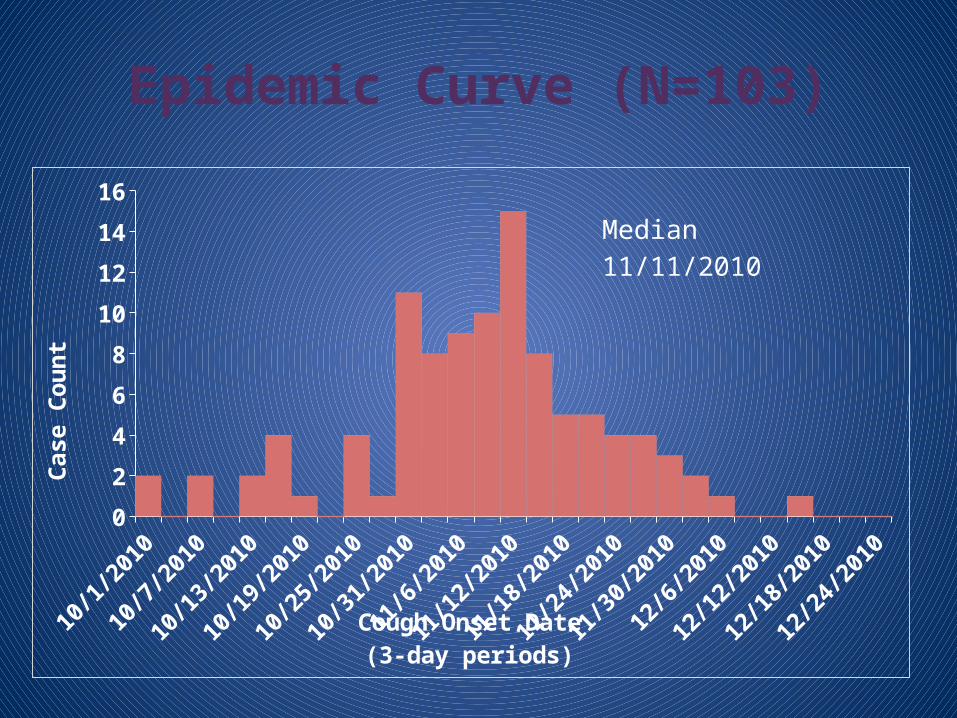
Cough Onset Date(3-day periods)
Case C
ou
nt
Median 11/11/2010
Epidemic Curve (N=103)
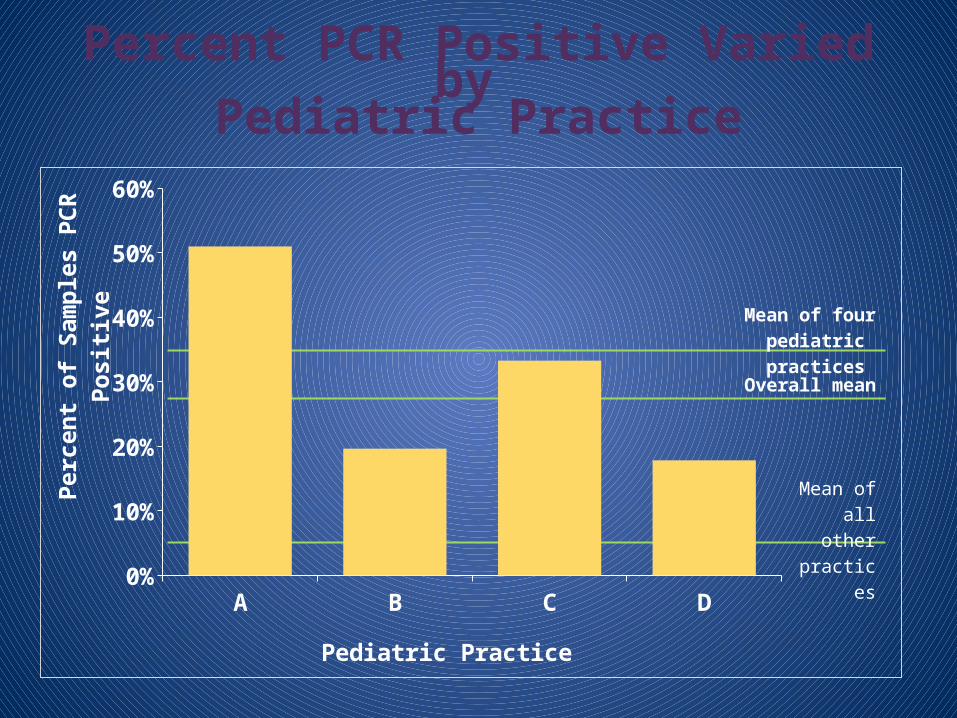
Percent PCR Positive Varied by Pediatric Practice
A B C D0%
10%
20%
30%
40%
50%
60%
Pediatric Practice
Perc
en
t of
Sam
ple
s P
CR
Pos-
itiv
e
Mean of four pediatric practices
Overall mean
Mean of all other
prac-tices
Factors Affecting Outbreak — Testing Issues
Testing of patients with symptoms inconsistent with pertussis 23% of PCR+ patients did not have cough
High proportion of false positive test results Sensitivity: ~100% (assumed) Specificity: 80% ~90% PCR positive samples had low amounts of DNA detected
Positive predictive value (PPV) of PCR in this outbreak: 19% (103/542)
4.5% (103/2300) of patients tested were confirmed pertussis cases
Factors Influencing Pertussis PCR Test Results
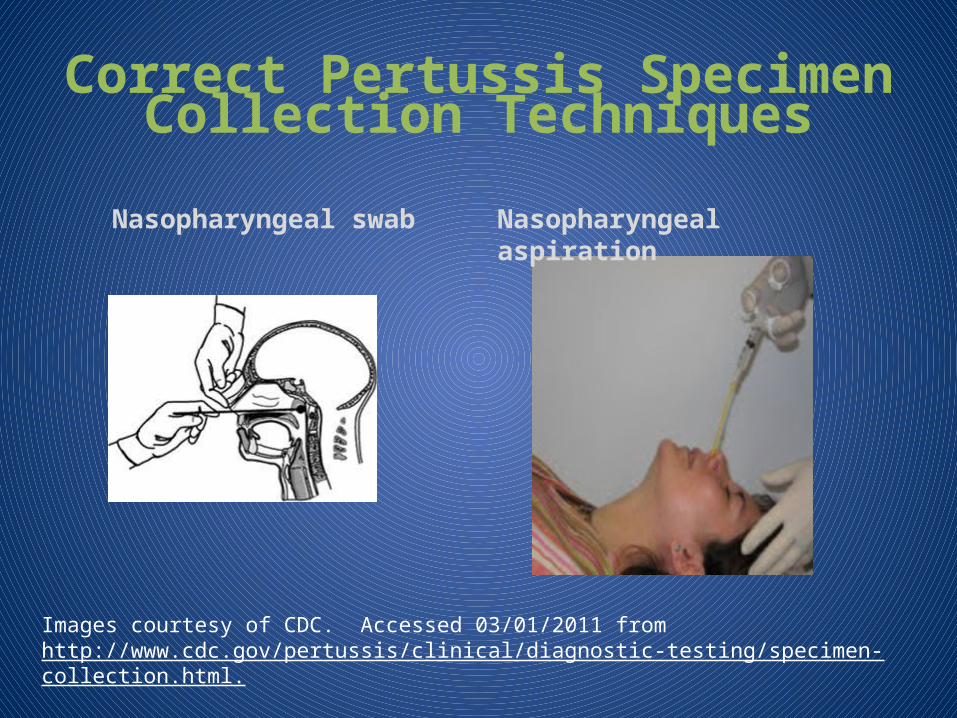
Prevalence of disease among patients tested Specimen collection technique
Specimens should be collected from the nasopharynx, not the nose or throat
Environmental contamination of clinical specimens Some pertussis vaccines contain PCR-detectable B.
pertussis DNA• Daptacel, Pentacel, Adacel
Liquid transport media for pertussis swabs increases potential for contamination
Detection of Pertussis DNA in Vaccines and Clinic Environments
PCR-measurable Bordetella pertussis DNA in Daptacel Pentacel Adacel
Extensive environmental contamination with vaccine DNA; in one study: 17-87% environmental specimens positive, depending on clinic Fewer patient samples with Ct > 37 from clinics where above
Recommended antibiotic prophylaxis to 6,900 close contacts of 542 PCR+ patients Mean: 12 close contacts per report Range: 0-105
Nearly 100% self-reported PEP compliance
>6% of entire Jefferson County population received PEP
Public Health Actions Taken Provider education
Health alert Guidance on specimen collection and selection of patients
for testing Conference call with providers
Additional specimen testing by Wadsworth Center (public health laboratory)
Community vaccination Vaccine clinics at Jefferson County Public Health Services• >1,200 doses of Tdap
Distribution of vaccine to birthing hospitals
Interpretation
Pertussis present, especially early in outbreak Pertussis never culture-confirmed
“pseudo-outbreak” Pertussis over diagnosed
Overtesting False positive PCR results
Possible contamination with vaccine? Vaccine coverage suboptimal, but might have
altered severity of disease
Consequences
Unnecessary treatment/PEP of asymptomatic individuals and their close contacts ~5,500 persons
Healthcare provider offices overwhelmed by testing
County health department overwhelmed by follow-up of patients and their close contacts (especially false PCR+) 3 full time staff
Unnecessary school and work furloughs
CDC Pertussis PCR Testing Recommendations*
PCR complimentary to culture Culture-confirm outbreak early
Test only patients with clinically compatible disease Do not test asymptomatic contacts
Test during first 3 weeks of cough
Use proper specimen collection technique and materials Posterior nasopharyngeal swab or aspirate
*Best Practices for Health Care Professionals on the use of Polymerase Chain Reaction (PCR) for Diagnosing Pertussis. 2011.
CDC Pertussis PCR Testing Recommendations*, continued
Avoid contamination of specimens with vaccine DNA, particularly if liquid media is used Prepare and administer vaccines in separate area from specimen
collection Wear gloves for vaccine preparation and administration Clean clinic surfaces with 10% bleach solution Glove immediately before specimen collection Use solid (charcoal) transport media or dry swab If using liquid media, take care not to handle
swab below line Aspirate kit is closed system, less likely to be contaminated
*Best Practices for Health Care Professionals on the use of Polymerase Chain Reaction (PCR) for Diagnosing Pertussis. 2011.
CDC Pertussis PCR Testing Recommendations*, continued
Understand limitations of PCR testing Results variable across laboratories
Interpret results in context of signs and symptoms and available epidemiological information
*Best Practices for Health Care Professionals on the use of Polymerase Chain Reaction (PCR) for Diagnosing Pertussis. 2011.
Lessons Learned
Rapid provider and community notification can limit the spread of an outbreak But may also lead to over-testing
PCR is not a perfect test for Bordetella pertussis
To maximize the PPV of PCR, limit testing to patients with cough suggestive of pertussis
Thank You Angie Maxted, MS, DVM
Epidemic Intelligence Service OfficerBureau of Communicable Disease Control, NYSDOHEIS Field Assignments Branch, SEPDPO/OSELS, CDC
Elizabeth Rausch-Phung, MD, MPHMedical Director Bureau of Immunization, NYSDOH
Debra Blog, MD, MPHDirectorBureau of Immunization, NYSDOH