Page 1
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1500
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
VARIABILITY AND INFLUENCE OF ACID-BASE BALANCE IN
PATIENTS WITH RENAL DYSFUNCTION
Minnu Anna Chacko*, Akshatha G., Anitha Vani M. and K. A. Sridhar
Department of Pharmacy Practice, East West College of Pharmacy, Bengaluru,
Karnataka- 560091.
ABSTRACT
An acid-base imbalance is the most common complication of renal
dysfunction and appears to contribute to the progression of kidney
disease, hence it is necessary to understand the acid- base physiology
and management of acid-base imbalance in renal dysfunction patients.
To study the variability and influence of acid-base balance in patients
with renal dysfunction. This was a prospective and observational study
which was performed on 102 renal dysfunction patients, by enrolling
the subjects based on the inclusion and exclusion criteria using a
statistical method. Among 102 patients included in the study, the
majority 72.42% were males and 31.62% were females, frequency of
patients suffering from CKD (64.70%) was found to be higher than
AKI (15.68%) and acute on CKD (19.60%). According to serum bicarbonates level, it was
found that 47.06% of subjects had metabolic acidosis, 39.22% had a normal range of
bicarbonates and 13.72% had metabolic alkalosis. Distribution of drugs used for the
management of acid-base imbalance in renal failure showed that loop diuretics and thiazide
diuretics were effective and dialysis was recommended for patients whose potassium levels
and serum creatinine levels were high. PPI’S were prescribed to counteract the GI side effects
of the drugs and to maintain the pH of the blood. Around 15-20% of renal dysfunction patients
suffer from some degree of acid-base imbalance (commonly metabolic acidosis) and
prevalence increases with lower GFR. Hence, we have undertaken the responsibility of clinical
pharmacist to understand and analyze the influence and variability of acid-base changes in renal
dysfunction.
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 7.632
Volume 10, Issue 2, 1500-1527 Research Article ISSN 2278 – 4357
*Corresponding Author
Minnu Anna Chacko
Department of Pharmacy
Practice, East West College
of Pharmacy, Bengaluru,
Karnataka- 560091.
Article Received on
25 Nov. 2020,
Revised on 15 Dec. 2020,
Accepted on 05 Jan. 2021
DOI: 10.20959/wjpps20212-18150
Page 2
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1501
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
KEYWORDS: Acid-base balance, acid-base imbalance management, patient-specific
management.
INTRODUCTION
Maintenance of normal pH in the body is very much required for normal health, the state of
equilibrium between proton donors and proton acceptors in the buffering system of blood is
known as acid-base balance.[1]
The lungs, kidney, and a complex system of buffers allow the
body to maintain acid-base homeostasis. The pH of human body ranges between 7.35 to
7.45.[2] Proper acid-base balance is required to be maintained for many biological processes to
happen, one most being the oxygenation of blood, to maintain normal physiology of body and
cellular metabolism.[3] Values of arterial pH 7.35 and lower are termed as acidemia and
values of arterial pH 7.45 and higher are termed as alkalemia. By evaluating ABG’s we can
assess a patient’s acid-base status. Arterial blood gases (ABGs) include the pH, arterial partial
pressure of oxygen and carbon dioxide (paO2 and paCO2), and the bicarbonates (HCO3-)
concentration. The serum anion gap and lactate concentration provides additional information
to classify and evaluate acid-base disorders.
Generally acid-base homeostasis is maintained by the lungs and kidneys. Acid-base disorders
are categorized according to the primary abnormality, the underlying pathological event that
disturbs the pH.
When the primary abnormality is a decrease in excretion of carbon dioxide by the lungs, the
disorder is termed as respiratory acidosis.
When the primary abnormality is excessive excretion of carbon dioxide by the lungs, the
disorder is termed as respiratory alkalosis.
When the primary abnormality is deficit of bicarbonate handled by the kidneys, the
disorder is termed as metabolic acidosis.
When the primary abnormality is excessive of bicarbonates, the disorder is termed as
metabolic alkalosis.
Laboratory assessment of acid-base status is usually performed on samples of arterial blood,
which accurately reflect acid base status in the body under most conditions.[2]
Acid base physiology
Metabolism of glucose, fats and proteins as an energy source results in the daily production of
15,000 mmol of carbon dioxide, which acts as an acid in the body and 50-100mEq of
Page 3
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1502
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
nonvolatile acids. This continual load of acidic substances must be buffered initially to prevent
acute acidosis and then excreted to prevent exceeding body’s buffer capacity.
The principal buffer system in body is carbonic acid/bicarbonate system. Other buffers,
including proteins, phosphates and hemoglobin also contribute to maintain normal Ph.[4]
Carbonic acid (H2CO3), a weak acid, and its conjugate base, bicarbonate (HCO3-), exist in
equilibrium with hydrogen ions (H+):
HCO3- + H
+ H2CO3
If hydrogen ions are added to the body or released as a result of a cellular metabolism, the H+
ion concentration rises and is reflected by a fall in pH. However a large portion of the hydrogen
ions combines with bicarbonates to form carbonic acid, lessening the effect on pH.
In aqueous solutions, carbonic acid reversibly desiccate to form water and carbon dioxide. This
reaction is enhanced and catalyzed by the enzyme carbonic anhydrase, which is present in the
body:
HCO3- + H
+ H2CO3 CO2 + H2O
Nearly all carbonic acid in the body is present as carbon dioxide gas. Hence, carbon dioxide
is the acid form of carbonic acid/bicarbonate buffer system.
The Henderson-Hassel Balch equation for the carbonic acid/bicarbonate buffer system
describes the mathematical relationship among pH, bicarbonate concentration and partial
pressure of carbon dioxide.
This equation demonstrates an important point: the ratio of the bicarbonate and carbon dioxide
concentrations, not the absolute values, determines pH.
𝑝𝐻 = 6.1 + log [𝐻𝐶𝑂3/0.03 × 𝑃𝑎𝐶𝑂2]
Role of kidney’s in acid- base balance: The principal role of kidneys is maintaining acid-base
homeostasis to regulate the concentration of bicarbonate in the blood. Since bicarbonate are
readily filtered in the glomerulus, the kidneys reabsorb filtered bicarbonate to avoid its
depletion. This reabsorption takes place in the proximal tubule and is catalyzed by carbonic
anhydrase. The other major role of the kidneys, is to excrete nonvolatile acids that are produced
by the body. This process occurs primarily in the distal tubule and also requires carbonic
Page 4
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1503
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
anhydrase. The hydrogen ions that are secreted into the tubule lumen are buffered by
phosphates and ammonia, so the final urine pH is usually acidic but typically not less than
4.50.[2] Hence kidneys play a major role in regulation of acid base balance. Kidney diseases
and dysfunction leads to impaired regulatory functions, resulting in alterations of acid base
balance which can be life threatening.[5] Hence there is a need to analyze and monitor the ABG
(arterial blood gases) in high risk patients, as well as in critically ill patients in the intensive
care unit.[6]
Components of arterial blood gases:- ABG evaluation include measurements of arterial pH,
PaO2 and PaCO2. The bicarbonate concentration is calculated from the pH and PaCO2 by
using Henderson-Hassel Balch equation.
PH: - Normal range- 7.36 to 7.44
The pH is the first value to be considered when using the ABG’s to assess a patient’s acid-base
status. PH of 7.35 and lesser represents acidemia, pH values of 7.45 and higher indicates
alkalemia.
Arterial partial pressure of carbon dioxide: - Normal range – 36 to 44mmHg.
Evaluation of PaCO2 provides information about the adequacy of lung function in excreting
carbon dioxide. An elevated PaCO2 usually implies inadequate ventilation.
Arterial partial pressure of oxygen: - Normal range- 80 to 100mmHg
Evaluation of the PaO2 provides information about the level of oxygenation of arterial blood.
In state of hypoventilation PaO2 is reduced with an elevation of PaCO2
Serum bicarbonate: - Normal range- 24 to 30 mEq/l
Once the PaCO2 and pH are measured, the bicarbonate concentration is calculated and
reported with the ABG results.[2]
PH and PaCO2 move in contrapositive directions. HCO3- and PaCO2 move in together in
same direction. When the pH and paCO2 change in the equal direction, the primary issue is
metabolic; when pH and paCO2 move in contrasted direction and paCO2 is normal, then the
Page 5
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1504
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
primary issue will be respiratory.
Mixed Disorder–if HCO3- and PaCO2 change in contrasted direction (which they should not
normally), then it said to be a mixed disorder, pH may be normal with abnormal paCO2 or vice
versa.[6]
Other tests to assess acid-base status are:- Anion gap: - Normal range- 3 to 11 mEq/l
The anion gap is a calculated value that will be helpful in classifying and evaluating possible
causes of metabolic acidosis. Normally the number of unmeasured anions exceeds the number
of unmeasured cations. When this difference is increased to the upper limit of normal, it often
indicates an increase in negatively charged, weak acids. The presence of increased anion gap
in conjugation with metabolic acidosis provides the clinician with useful information about
possible causes of acidosis. The anion gap is calculated by using sodium to approximate the
measured cations, and chlorides and bicarbonates to approximate the measured anions.
Serum lactate: - Normal range – 0.5 to 1.5 mEq/l (venous), 0.5 to 2.0 mEq/l (arterial).
When tissues are normally oxygenated, pyruvate is converted to acetyl coenzyme A and it’s
utilized as an energy source through aerobic metabolism. In patients with insufficient tissue
perfusion or enhanced tissue metabolic rates, anaerobic metabolism dominates. Anaerobic
metabolism increases the conversion of pyruvate to lactate, increasing the lactate concentration.
If these process is severe or not reversed, lactic acidosis can occur.
For each disorder, the primary abnormality will be accompanied by a compensatory change.
For example: the primary abnormality is metabolic acidosis is fall in serum bicarbonate, and
compensatory change is a fall in PaCO2.[2]
Complications of metabolic acidosis in renal failure are- bone-mineral disorder, muscle
wasting, protein degradation, encephalopathy, progression of kidney disease.[7]
Hypokalemia
and kaliuresis are common complications of metabolic alkalosis. Metabolic alkalosis are
predisposed to cardiac arrhythmias.[8]
Acid base disorders commonly accompany diuretics
use.[9]
The mortality associated with severe metabolic alkalosis is substantial; a mortality rate
of 45% was found in patients with an arterial blood pH of 7.55 and 80% when the pH was
greater than 7.65.[10]
Metabolic acidosis is a common complication kidney disease. Based on a
Page 6
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1505
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
cross sectional analysis of the national health and nutrition examination survey, an estimated
40 million adults in the united states have renal dysfunction, and approximately 700,000
individuals have an estimated as 30-50% of individuals with GFR less than 30 ml/min/1.73m2
have metabolic acidosis, approximately 200,000 to 350,000 individuals with CKD stage 4
and 5 have chronic metabolic acidosis in the united states.[1] Also the cross sectional study on
35 patients conducted at two centers in western part of India, found 22 out of 35 patients
(62.85%) have the mean predialysis serum pH and HCO3 of 7.32± 0.083 and 20.37 ±4.94
mmol/L.[12] The prevalence of acidosis begins to rise when GFR falls below 40ml/min per
1.73m2 and further progress to increase as GFR decreases. Lower bicarbonates levels fastens
the kidney disease progression.[13]
Since the incidence of kidney disease is increasing day by day in India and one of the common
complication of renal dysfunction is acid base imbalance. Chronic metabolic acidosis is the
most common condition to be reported which worsens the condition of the patient by
progression of the disease, reducing quality of life and increasing mortality rate by causing
complications and even death, hence there is a need for maintaining acid base balance in renal
dysfunction patients. We can reduce patient’s exposure to acidosis and alkalosis by providing
qualitative pharmaceutical care services.
Methodology
Study site
The study was conducted in the Nephrology Department of Sagar Hospitals, Bengaluru.
Study design
This was a Prospective and Observational study performed on 102 patients to assess the
variability and influence of acid-base balance in renal dysfunction patients.
Sample size
A total of 102 patients from the department of Nephrology, Sagar hospitals were included in
the study.
Study period
The study was conducted over a period of six months from October 2019 to March 2020.
Ethical approval
Ethical committee clearance was obtained by the Institutional Ethical Committee of Sagar
Hospitals, Bengaluru.
Study criteria
Page 7
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1506
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
Inclusion criteria
1. Patients admitted in Nephrology department
2. Patients of all stages of kidney disease
3. Patients of either gender
Exclusion criteria
1. Pregnant and lactating women
2. Patients of age <18 years
3. Patients with renal replacement therapy
Source of data
Patients demographics, clinical findings, laboratory and therapeutic data were collected from
inpatient department and the main sources for the collection of data were:
Patients case notes
Treatment charts/ medication charts
Lab reports
Progress notes
Discharge cards
Study procedure
1. Patient enrollment
A hospital based prospective study was conducted in Nephrology inpatient department of Sagar
Hospitals. The study was conducted using the data of patients who have consented to
participate. Patients who were below 18 years, pregnant and lactating women, and patients with
renal replacement therapy were excluded for the study.
2. Method of data collection
The study was carried by collecting the necessary information from the patients admitted in
nephrology department of Sagar hospitals. Data collection form, was designed to incorporate
the details of the patients. The details include demographics, past medical history, complaints
on admission, diagnosis and treatment provided with respect to renal impairment and acid-base
balance. The patients were observed on daily basis to identify the variability in acid base
balance. The treatment given to correct the acid base imbalance was recorded for the further
evaluation.
Page 8
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1507
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
3. Statistical methods
Descriptive statistical analysis has been carried out in the present study. Mean and standard
deviation were used to measure the central tendencies of given data.
4. Statistical software
The statistical software namely SPSS version 25.0, was used for the analysis of data
Microsoft word and excel were used to generate tables and graphs respectively
RESULTS AND DISCUSSION
The descriptive statistical analysis was performed for the given data of 102 subjects and the
results were obtained as shown below:
Table 1: Age and Gender distribution of subjects (N=102).
Age in
years
No. of subjects
(Frequency)
Total
(Percentage)
M F
31-40 02 00 02 (1.96%)
41-50 11 06 17 (16.67%)
51-60 14 07 21 (20.59%)
61-70 20 10 30 (29.41%)
71-80 16 05 21 (20.59%)
>80 08 03 11 (10.78%)
Total 71 31 102 (100%)
Fig. 01.
As shown in table 1 & Fig 1, the age distribution of the given population showed that 2 (1.96%)
of patients belong to the age group of 31-40 years, 17 (16.67%) patients belong to the age group
of 41-50 years, 21 (20.59%) belong to the age group of 51-60 years, 30 (29.41%) belong to the
group of 61-70 years, 21 (20.59%) subjects belong to the age group of 71-80 years and 11
Page 9
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1508
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
(10.78%) of subjects belong the age group of >80 years. According to the data obtained, it is
observed that the majority of the patients who suffer from renal dysfunction are males. Similar
results were seen in a study conducted by Wel Chen, et al. On Epidemiology of acid-base
derangements in renal dysfunction. The study results showed that the maximum number of
cases was seen in the mean age of 59 years or an average age group of 21-74 yrs with GFR
between 20 and 70ml/min per 1.73m2 was conducted the nephro study test in France. This
unlike in the more developed countries where it affects mainly middle-aged and elderly
patients.[13]
Another study conducted by Wel Chen, et al. On the epidemiology of acid-base
derangements in renal dysfunction was studied. The highest number of patients observed in
different areas of studies were male. The study results showed that in 1038 out of patients with
having 63% were male & 31% were female & 6% were black. This study was conducted in a
prospective hospital-based; France. According to this field of study, the majority of the patients
who suffer from renal diseases are males than females.[13] In table no: 1 and fig no: 1
representation of patient distribution based on age and gender. From this study, it was found
that the largest number of patients was present in the age group of 61-70 yrs with a total of 30
patients out of which 20 were male and 10 were female. The lowest number of patients was
seen in the age group of 31-40 years with 2 patients out of which all were male.
Analysis and distribution of social history
Table 2a: Distribution of subjects based on dietary habits (N=102).
Diet No. of Subjects
(Frequency)
ePatPecreP
Veg 45 44.12%
Mixed 57 55.88%
Total 102 100%
Fig. 2a.
Page 10
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1509
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
Both table 2a & Fig 2a revealed that, out of 102 patients, 45 (44.12%) were vegetarians, 57
(55.88%) were having mixed dietary habits. In the similar study conducted by Golaleh Asghari,
etal. on Dietary pattern and incidence of KD among adults a population based study in west
Asian. This study results shows that 1630 participants, with high fat dietary pattern was
associated with an increase of 46% of incident for developing KD, whereas a vegetarian dietary
pattern may be protective against the occurrence of KD by 43%. And also a study from the
China health and nutrition survey shows that a traditional southern dietary pattern characterized
by high intakes of rice, pork, vegetables, and low intake of wheat leads to increased prevalence
of KD and a modern dietary patterns featured by high intakes of fruits, soy milk, egg, milk and
deep fried products decreased risk of KD.[51]
Table no. 2b: Distribution of subjects based on the habits of smoking and alcohol
consumption.
Social habit No. of subjects (Frequency) Total
(Percentage) Yes No
Smoking 06 (5.88%) 96 (94.12%) 102 (100%)
Alcohol
consumption
05 (4.91%) 97 (95.09%)
Fig. 2b.
According to the table 2b & Fig 2b, the distribution of subjects based on smoking and alcohol
consumption showed that, 6 (5.88%) subjects were smokers and 5 (4.91%) were alcoholics.
out of 102 patients, 96 (94.12%) were non-smokers and 06(5.88%) were smokers this results
shows that the prevalence of Renal dysfunction is more in patients who are not smoking even
though smoking is a risk factor of renal diseases with co morbities of DM, HTN and obesity
etc. The study revealed that only 5 (4.91%) were alcoholic out of 102 patients and remaining
Page 11
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1510
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
97(95.09%) were non alcoholics. Based on the study conducted by Anoop Shankar, etal. On
the association among smoking, heavy drinking, and CKD. The field of study seen that the
prevalence of renal diseases was similar in both smokers and non-smokers also alcoholic and
non-alcoholic patients. High risk in the age group of 43-86 yrs of patients is may be due to life
style changes, obesity, smoking, alcoholism (male).[52]
Analysis and distribution of subjects according to diagnosis of renal dysfunction based
on stages
Table no. 3a: Distribution of subjects according to diagnosis of renal dysfunction
Diagnosis No. of Subjects
(Frequency)
PercePtaPe
CKD 66 64.70%
AKI 16 15.68%
Acute on CKD 20 19.60%
Total 102 100%
Fig. 3a.
Table no. 3b: Distribution of subjects according to diagnosis of renal dysfunction based
on stages.
Diagnosis and Stages of
renal failure
CKD AKI
Stage – I - 3
Stage - II 3 5
Stage – III 13 8
Stage – IV 19 -
ESRD 31 -
Fluid overload 23 -
Dialysis 57 -
Page 12
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1511
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
Fig. 3b.
According to table 3 (3a & 3b) & Fig 3 (3a & 3b), the analysis and distribution of the number
of subjects according to a diagnosis of renal dysfunction based on stages revealed that, out of
102 subjects, 66 subjects were diagnosed with CKD, 16 subjects were diagnosed with AKI and
20 subjects were found to be in the acute condition of CKD. From table 3b, it was found that
the majority (31) of the subjects were found to be in end-stage renal failure, 23 had a fluid
overload, and were on dialysis. The total number of subjects on dialysis was found to be 57
(Dialysis was done irrespective of fluid overload based on the severity of renal dysfunction and
condition of the subject). In the current study conducted, several patients in AKI were in stage
1 (3), stage 2(5), and stage 3(8). And also in CKD stages, it shows that stage 1-5 the number
of patients was increased like 3, 13, 19, &31 respectively. Patients were under fluid overload
was 23. Similar to the study conducted by Griffin P Rodgers on kidney disease statistics for
Page 13
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1512
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
the United States revealed that the overall prevalence of CKD increases by years to years
largest increases occurred in people with stage3 CKD. This study shows that women had more
likely to have stages 1 to 4 than men. In AKI the medicare patients ages 66 and older with an
AKI hospitalization having the risk of prevalence.[53]
Analysis of acid-base imbalance based on laboratory data obtained Table No. 4a –
Distribution of subjects based on serum bicarbonate levels.
Sr. HCO3-(MEq/Lt) No. of subjects
(Frequency)
Percentage Mean±SD
Normal ( 22-28) 40 39.22% 22.55±6.78
Metabolic acidosis (< 22) 48 47.06%
Metabolic alkalosis (> 28) 14 13.72%
Total 102 100%
Fig. 4a.
From the above table No: 4a and fig No: 4a, the analysis, and assessment of acid-base
imbalance in subjects showed that the majority 48 of the subjects out of the 102 were found to
have metabolic acidosis with having 47.06%, 40 subjects were found to have normal
bicarbonates levels with having 39.22% and 14 subjects were found to have metabolic alkalosis
with having 13.72%. In our study, the bicarbonate levels were advised, if the patients were
under hemodialysis have been increasing the bicarbonate levels and the patient’s condition
were better. The kidney excretes acids in the urine and they regulate the concentration of HCO3
in the blood. Acid-base changes due to increases or decreases in HCO3 occur more slowly than
changes in CO2. Similarly, vashistha et.al, carried out a study by randomizing the data from
121,351 maintenance dialysis 91.4% on hemodialysis treated were increasing serum
bicarbonates levels in the patients. As most epidemiologic studies have used only the serum
Page 14
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1513
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
bicarbonate to define metabolic acidosis, the prevalence of other acid-base disorders has not
been well characterized.[28]
Table no. 4b: Distribution of subjects based on PaCO2 levels.
PaCO2 (mmHg) No. of subjects
(Frequency)
Percentage Mean±SD
Normal ( 32-45) 53 51.97% 38.58±10.44
Metabolic
acidosis/Respiratory
alkalosis (< 32)
22 21.57%
Metabolic
alkalosis/Respiratory
acidosis (> 45)
19 18.62%
Test not advised 08 7.84%
Total 102 100%
Fig. 4b.
From the above table 4b & Fig 4b, the analysis and assessment of acid-base imbalance based
on the arterial partial pressure of carbon dioxide in subjects with renal failure showed that the
majority (53) of the subjects out of 102 were found to have normal levels of PaCO2, 22 subjects
were found to have metabolic acidosis/respiratory alkalosis, 19 subjects were found to have
metabolic alkalosis/respiratory acidosis and 08 subjects were not advised with the test. Similar
findings were observed in a study conducted by Ishita Ghatak.et al, on analysis of arterial blood
gas report in CKD. The aim of the study shows that to explore the type and prevalence of acid-
base disorders in 31 critically ill CKD patients from tertiary care hospitals in Maharashtra,
compare with two methods like systematic method and bedside method. The systematic method
Page 15
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1514
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
showed a higher prevalence of metabolic acidosis having 48.39% in 15 cases and the No: of
metabolic alkalosis cases were 3 having 9.68%. In this study it revealed that the most common
acid-base disorder was both simple respiratory alkalosis and mixed metabolic acidosis with
respiratory alkalosis.[54]
Table no. 4c: Distribution of subjects based on PaO2 levels.
PaO2 (mmHg) No. of subjects
(Frequency)
Percentage Mean±SD
Normal ( 75-100) 34 33.34% 67±29.3
Hypoxia (< 75) 59 57.84%
Test not advised 09 8.82%
Total 102 100%
Fig. 4c.
From the above table 4c & Fig 4c, the analysis and assessment of acid-base imbalance based
on the arterial partial pressure of oxygen in subjects with renal failure showed that the majority
(34) of the subjects out of 102 were found to have normal levels of PaO2, 59 subjects were
found to have hypoxia and breathing difficulties and 09 subjects were not advised with the test.
In the study of Qiangwei Fu. et al, on Hypoxia: indicated that the force which drives to CKD
was chronic hypoxia or renal tissue hypoxia. The evidence indicated that CKD is driven by
renal tissue hypoxia that has lead to the development of therapeutic strategies that increase
kidney oxygenation and the chronic hypoxia is the final common pathway to ESRF. The lower
oxygen concentration can cause alterations of renal dysfunction, these may affects the
maintenance of a balance of the body fluids, electrolytes, pH and blood pressure homeostatic.
Increases in blood uremia profile, toxicity markers and lipid peroxidation indicated that
hypoxia causes the renal dysfunction.[55]
Page 16
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1515
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
Table no. 4d: Distribution of subjects based on SaO2 levels.
SaO2 (%) No. of subjects
(Frequency)
Percentage Mean±SD
Normal (95-100%) 28 27.45% 92.76±10.26
Hypoxemia (< 90%) 29 2.84%
Test not advised 45 44.11%
Total 102 100%
Fig. 4d.
From the above table 4d & Fig 4d, the analysis and assessment of acid-base imbalance based
on arterial saturation of oxygen in subjects with renal failure showed that the majority (45) of
the subjects out of 102 were not tested for oxygen saturation, 29 subjects were found to have
hypoxemia and breathing difficulties and 28 subjects were found to have normal arterial
oxygen saturation value of 95-100%. When the kidney has low level of oxygen in the blood
they can produce a protein called erythropoietin which stimulates red blood cell production
which in turn increases Hb levels in the blood. That can bind to oxygen molecules hence
increasing oxygen saturation in the blood. In this study only 29 subjects have been tested the
SaO2 levels and the majority were not tested. Hb is the protein in red blood cells to tissues
throughout the renal tissue and all over the body.
Page 17
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1516
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
Table no. 4e: Distribution of subjects based on blood pH levels.
Blood pH No. of subjects
(Frequency)
Percentage Mean±SD
< 7.20 (Severe academia) 08 7.84% 7.32±0.36
7.20 – 7.29 (Moderate academia) 09 8.82%
7.30 – 7.34 (Mild academia) 08 7.84%
7.35 7.45 (Normal) 63 61.76%
7.46 – 7.50 (Mild alkalemia) 11 10.78%
7.51 – 7.55 (Moderate alkalemia) 00 00
>7.55 (Severe alkalemia) 00 00
Test not advised 03 2.94%
Total 102 100%
Fig. 4e.
From the above table 4e & Fig 4e, the analysis and assessment of acid-base imbalance based
on blood pH in subjects with renal failure showed that the majority (63) of the subjects out of
102 were found to have normal blood pH levels. Normal blood pH must be maintained within
a narrow range of 7.35- 7.45, to ensure the proper functioning of metabolic processes and
delivery of the right amount of the oxygen to the tissues. In this study it shows that majority 63
of the subjects out of 102 were found to have normal blood PH levels, 08 subjects were found
to have severe academia, 09 subjects were found to have moderate academia, 08 subjects were
found to have mild academia, 11 subjects were found to have mild alkalemia and 03 subjects
were not tested for pH. In these 25 subjects were found to have metabolic acidosis and 11
subjects were found to be metabolic alkalosis. Majority of 63 subjects having normal pH values
in this study. In our study we had totally 57 subjects on dialysis, after the dialysis most of the
pH values are becoming normal to the patients. Blood pH depends on the balance of Co2 and
Page 18
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1517
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
HCO3, a change in the amount of Co2 will not change in pH until is a change in the amount
of HCO3 that preserves the balance.
Table no. 5: Assessment of management used in acid-base imbalance in subjects with
renal failure.
Drug class Generic name Frequency of use Total
Antacid Sodium bicarbonate 09 09
Calcium Supplements Calcitriol+calcium+Zinc 01 39
Calcium Carbonate 02
Calcium carbonate+Vitamin D3 31
Calcium Gluconate 04
Vitamin D3 03
Calcitriol 01
H2 Antagonists Ranitidine 06 06
Iron Supplements Iron+Vitamin B12+Folic
acid+Vitamin C
02 11
Iron Sucrose 08
Ferric Carboxymaltose 01
K+ Binder Calcium polysterene
sulfonate
16 16
Loop Diuretics Furosemide 74 102
Torsemide 28
NS Fluid Saline 04 04
Phosphate binders Calcium acetate 03 07
Sevelamir 04
PPIs Pantoprazole 92 92
Thiazide Diuretics Metolazone 09 10
Moxonidine 01
Vitamin Supplements Vitamin K 01 07
Multivitamin 02
Vitamin B complex + Lactobacillus 01
Vitamin B complex 01
Vitamin B complex+Vitamin C 02
Page 19
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1518
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
Fig. 5.
From the above table No: 5 and fig No: 5, distribution of drugs used for the management of
acid-base imbalance in renal failure. In this study most frequently used drug was loop
diuretics like furosemide and torsemide were used in all the subjects to cause diuresis by
inhibiting the sodium-potassium-chloride cotransporter in the thick ascending loop of Henle.
This loop diuretics reduce the reabsorption of calcium and magnesium. There might be
chances of calcium absorptions in the renal dysfunction patients so to rectify that calcium
supplements are given. So that 39 subjects were prescribed with calcium supplements like
Calcitriol+ calcium+ zinc, calcium carbonate, calcium carbonate + vitamin D3, calcium
Gluconate, vitamin D3 and calcitriol to balance the serum concentrations of calcium. PPIs
like pantoprazole was given in 92 subjects to counteract the GI side effects of other drugs,
and help to maintain the pH of the blood. The main use of the PPIs is the distribution of No:
of drugs used in per subjects was more in this study (13-15) this drug is more useful in
elderly patients according to their health conditions. This drug suppresses the gastric acid
production to maintain the acid-base balance in the patients. 9 subjects were prescribed with
sodium bicarbonate for antacid action to normalize the blood pH. Sodium bicarbonate is a
systemic and urinary alkalinized used to increases serum or urinary HCO3 concentration and
raise pH. Thiazide diuretics like metolazone and moxonidine were given in 10 subjects to
regulate fluid balance and blood pressure. One of the main symptoms of renal patients was
edema or fluid accumulation, this drug is used to increases the amount of water and salt
expelled from the body to urine. This drug also increases calcium reabsorption at the distal
tubule. Calcium polysterene sulfonate was given as a potassium binding agent in 16 subjects.
This drug exchanges calcium for potassium in the distal colon, thus potentially limiting the
sodium retention and providing calcium supplementation. Iron supplements like Iron +
Page 20
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1519
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
vitamin B12 + folic acid + vitamin C, iron sucrose, and ferric carboxymaltose were given for
anemia to restore Hb in 11 subjects. Iron supplementations are advisable for all iron deficient
CKD patients receiving erythropoiesis stimulating agents and intravenous iron may be
preferable to oral iron. Phosphate binders like calcium acetate and sevelamir were given to
increases the calcium absorption and preserve BMD in 7 subjects. In CKD patients,
controlling serum phosphate is associated with bone pathology and to regulate together with
calcium by the parathyroid hormone. It also prevents the progression of mineral and bone
disorders in renal patients. Phosphate binders help to prevent complications of kidney disease,
but sevelamir may be preferred upon calcium binders as they tend to reduce the deaths in
patients when compared to that of calcium. 6 subjects were receiving H2 antagonists like
ranitidine and 7 subjects were receiving vitamin supplements. Vitamin supplements are used
to reduce the loss of vitamins during dialysis treatment. The waste products that build up in
your body each day can change, the manner of utilization of minerals and vitamins. In our
study, all these medications used in the patients were safe and effective.
Table no. 6: Distribution of No. of drugs used per subject in management of renal
failure.
No. of drugs
used/subject
No. of subjects
(Frequency)
Percentage Mean±SD
7 to 9 10 9.80% 13.15±2.90
10 to12 36 35.29%
13 to 15 39 38.23%
16 to 18 13 12.74%
19 to 21 04 3.92%
Total 102 100%
Fig. 6.
Page 21
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1520
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
From the above table No: 6 and fig 6, the distribution of No. of drugs used per subject in 102
subjects revealed that, majority (39) of subjects were prescribed with 13 to 15 drugs, 36
subjects were prescribed with 10 to 12 drugs, 13mwere prescribed with 16 to 18 drugs, 10 were
prescribed with 7 to 9 drugs and 4 subjects were prescribed with 19 to 21 drugs. On average,
most of the subjects were receiving at least 13 drugs indicating polypharmacy. In our study we
observed that majority of the patients suffer from renal dysfunction between the ages of 61-70
years. And the second least of the patients age between 51-60 & 71-80 respectively. As the
aging, polypharmacy has become an important risk factor for poor outcomes in the elderly
patients. To reduce the incidence of polypharmacy and ensure the patients safety, we conducted
medication reconciliations, eliminating duplicate medications, assessing the drug-drug
interaction and reviewing dosages are decreased associated costs. Elderly patients are at the
greater risk for ADRs because of the metabolic changes and reduce drug clearance associated
with ageing: this risk is increased with the number of drugs used.[60]
Statistical methods: Descriptive statistical analysis has been carried out in the present study.
Mean and Standard deviation were used to measure the central tendencies of given data
Microsoft Word and Excel are used to generate tables and graphs respectively.
CONCLUSION
According to the WHO study, they estimated that 1.2 million people died from kidney failure,
and additionally each year around 1.7 million people are thought to die from AKI. Overall an
estimated 5-10 million people die annually from kidney diseases. Hence, our study aimed at
observing the variability and influence of acid-base balance in patients with renal dysfunction.
Out of 102 subjects, males were found to be affected more with renal dysfunction than females
comparatively. Most of the subjects were suffering from CKD than AKI and metabolic acidosis
was found to be more common based on various laboratory analyses in patients with renal
dysfunction.
The analysis of the management of acid-base balance revealed that loop diuretics like
furosemide and torsemide were used to cause diuresis and balance the pH of the blood. Other
drugs like Thiazide diuretics, proton pump inhibitors & phosphate binders were also given to
support the acid-base balance.
Hence based on the results the study concludes that fluid and electrolyte balance with the
pharmacological management of renal dysfunction helps in balancing the acid-base variations.
Page 22
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1521
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
Therefore, focusing on treating the renal impairment will bring out the effective management
of acid-base imbalance.
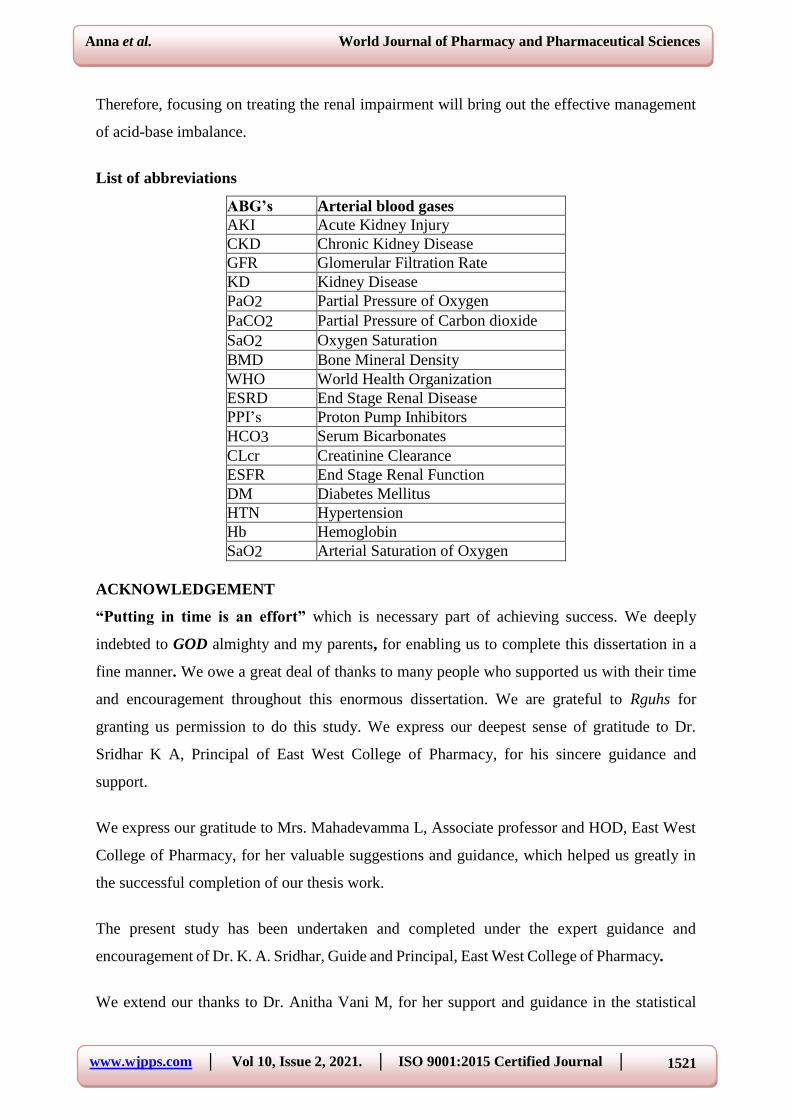
List of abbreviations
ABG’s Arterial blood gases
AKI Acute Kidney Injury
CKD Chronic Kidney Disease
GFR Glomerular Filtration Rate
KD Kidney Disease
PaO2 Partial Pressure of Oxygen
PaCO2 Partial Pressure of Carbon dioxide
SaO2 Oxygen Saturation
BMD Bone Mineral Density
WHO World Health Organization
ESRD End Stage Renal Disease
PPI’s Proton Pump Inhibitors
HCO3 Serum Bicarbonates
CLcr Creatinine Clearance
ESFR End Stage Renal Function
DM Diabetes Mellitus
HTN Hypertension
Hb Hemoglobin
SaO2 Arterial Saturation of Oxygen
ACKNOWLEDGEMENT
“Putting in time is an effort” which is necessary part of achieving success. We deeply
indebted to GOD almighty and my parents, for enabling us to complete this dissertation in a
fine manner. We owe a great deal of thanks to many people who supported us with their time
and encouragement throughout this enormous dissertation. We are grateful to Rguhs for
granting us permission to do this study. We express our deepest sense of gratitude to Dr.
Sridhar K A, Principal of East West College of Pharmacy, for his sincere guidance and
support.
We express our gratitude to Mrs. Mahadevamma L, Associate professor and HOD, East West
College of Pharmacy, for her valuable suggestions and guidance, which helped us greatly in
the successful completion of our thesis work.
The present study has been undertaken and completed under the expert guidance and
encouragement of Dr. K. A. Sridhar, Guide and Principal, East West College of Pharmacy.
We extend our thanks to Dr. Anitha Vani M, for her support and guidance in the statistical
Page 23
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1522
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
analysis. We take this opportunity to thank librarian Mr. Nagesh, East West College of
Pharmacy and for extending library facilities throughout this study.
Our sincere expression of gratitude to the Dr. (Major) Mahendra Kumar (Medical Director &
Member Secretary, Institutional Ethics Committee) & Justice. B.A. Muchandi, (Chairman,
Institutional Ethics Committee), Sagar Hospitals, Bangalore.
We extend our special thanks to computer operator, printers and binders for their technical
assistance and preparation of this manuscript in time. Last but not the least, we extend our
thanks to all those who have been directly or indirectly associated with our study.
Signature of the candidate
(Minnu anna chacko) (Akshatha G.)
Date:
Place:
BIBLIOGRAPHY
1. Merriam Webster. Acid base balance, 2019; 16. Available URL: www.merriam-
webster.com.
2. Thomas G. Hall. Arterial blood gases and acid-base balance. In: Scott L. Traub. Basic
skills in interpreting laboratory data: ASHP, 1: 159 – 69.
3. Hopkins E, Sharma S. Physiology, Acid Base Balance. In: StatPearl, 2019, 2020; 16(2):
1-13.
4. Rose B D. Clinical physiology of acid-base and electrolyte disorders, New York:
McGraw-Hill; 1994.
5. Tsering Dhondup and Qi Qian. Acid-base and electrolyte disorders in patients with and
without chronic kidney disease: an update. Kidney Dis (Basel), 2017; 3(4): 136-148.
6. Pramod Sood, Gunchan Paul, Sandeep Puri. Interpretation of arterial blood gas. Indian J
Crit Care Med, 2010; 14(2): 57-64.
7. Tsering Dhondup Qi Qian. Electrolyte and acid- base disorders in chronic kidney disease
and end stage kidney failure. Blood Puif, 2017; 43: 179-188.
8. Larry R Engelking. Metabolic alkalosis. The textbook of veterinary physiological
chemistry, 2015; 3: 576-83.
9. Arthur Greenberg. Diuretic complications. Am. J. Med scl, 2000; 319: 10-24.
10. John H. Galla. Metabolic alkalosis. J Am Soc Nephrol, 2000; 11(2): 369-75.
Page 24
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1523
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
11. Wei chen, Matthew K Abramowitz. Metabolic acidosis and the progression of chronic
kidney disease. BMC Nephrol, 2014; 15: 55.
12. Atul D Sajgure, Tushar A Dighe, Jayraj S Korpe, Charan B Bale, Ashwini O Sharma,
Nilesh S Shinde. Prevalence and severity of metabolic acidosis in patients on
maintenance haemodialysis in India. Medical journal of DR. D. Y. Patil Vidyapeeth,
2016; 9(6): 716-20.
13. Wei Chen, Matthew K. Abramowitz. Epidemiology of acid base derangements in CKD.
J.ackd, 2017; 24(5): 280-88.
14. Gaggl M, Cejka D, Plischke M, Heinze G, Fraunschiel M, Schmidt A, etal. Effect of oral
sodium bicarbonate supplementation on progression of chronic kidney disease in patients
with chronic metabolic acidosis. Department of medicine III, division of nephrology and
dialysis, medical university of Vienna, Austria: trials, 2013; 14(1): 196.
15. Nimrit Goraya, Jan simony, Chan- Hee Jo, Donald E Wesson. Treatment of metabolic
acidosis in patients with stage 3 chronic kidney diseases with fruits and vegetables or oral
bicarbonate reduces urine angiotensinogen and preserves glomerular filtration rate.
International society of nephrology, 2014; 86(5): 1031-38.
16. Hodgkin JE, Soeprono FF, Chan DM. Incidence of metabolic alkalemia in hospitalized
patients. Crit Care Med, 1980; 8(12): 725-8.
17. Mindy Pike, Thomas G Stewart, Jennifer Morse, Patrick Ormsby, Edward D
Siew,Adriana Hung, et al. APOL1, Acid Load and CKD progression. Kidney Int Rep,
2019; 4: 946-54.
18. Olivier Moranne, Marc Froissart, Jerome Rossert, Cedric Gauci, Jean Jacques Boffa,
Pascal H. Timing of onset of CKD Related metabolic complications. J Am Soc Nephrol,
2009; 20: 164- 71.
19. Silvano Salgueiro Geraldes, etal. The Effect of Intermittent Haemodialysis on the
Haematological and Serum Biochemistry Profile in Dogs with Chronic Kidney Disease.
Topics in companion animal medicine, 2019; 38: 265-78.
20. Abramowitz MK, Hostetter TH, Melamed ML. Association of serum bicarbonate levels
with gait speed and quadriceps strength in older adults. Am J Kidney Dis, 2011; 58 (1):
29-38.
21. Yenchek R, Rifkin DE, Shlipak MG, Sarnak MJ, Garcia M, etal. Association of serum
bicarbonate with incident functional limitation in older adults. Clin J Am Soc Nephrol,
2014; 9: 2111-16.
22. Driver TH, Shlipak MG, Katz R, Goldenstein L, Sarnak MJ, Hoofnagle AN, Siscovick
Page 25
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1524
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
DS, et.al. Low serum bicarbonate and kidney function decline: the Multi-Ethnic Study of
Atherosclerosis (MESA). Am J Kidney Dis, 2014; 64(4): 534-41.
23. Nadeau-Fredette AC, Bouchard J. Fluid management and use of diuretics in acute kidney
injury. Advances in chronic kidney diseases, 2013; 20(1): 45-55.
24. Hoffman SB, Massaro A N, Soler-García AA, Perazzo S. A novel urinary biomarker
profile to identify acute kidney injury (AKI) in critically ill neonates: a pilot study. Pediatr
Nephrol, 2013; 28(11): 2179-88.
25. Allegretti AS, Flythe JE, Benda V, Robinson ES, Charytan DM. The effect of bicarbonate
administration via continuous venovenous hemofiltration on acid-base parameters in
ventilated patients. Biomed Research International, 2015; 8.
26. Goraya N, Simoni J, Sager LN, Pruszynski J, Wesson DE. Acid retention in chronic
kidney disease is inversely related to GFR. Am J Physiol Renal Physiol, 2018; 314:
985-991.
27. Sow A, Morelle J, Hautem N, Bettoni C, Wagner CA, Devuyst. Mechanisms of acid-base
regulation in peritoneal dialysis.Nephro. Dial Transplant, 2018; 33: 864-73.
28. Vashistha T1, Kalantar-Zadeh K, Molnar MZ, Torlen K, Mehrotra R. Dialysis modality
and correction of uremic metabolic acidosis: relationship with all-cause and cause-
specific mortality. Clin J Am Soc Nephrol, 2013; 8: 254-64.
29. Morishita M, Matsuo N, Maruyama Y, Nakao M, Yamamoto I, Tanno Y, et.al. The
differences in acid-base status and the calcium parathyroid axis between peritoneal
dialysis and hemodialysis. Clin Nephrol, 2016; 86(2): 55-61.
30. Goraya N, Simoni J, Jo CH, Wesson DE. A comparison of treating metabolic acidosis in
CKD stage 4 hypertensive kidney disease with fruits and vegetables or sodium
bicarbonate. Clin J Am Soc Nephrol, 2013; 8: 371-81.
31. Abramowitz MK1, Hostetter TH, Melamed ML. The serum anion gap is altered in early
kidney disease and associates with mortality. Kidney Int, 2012; 82(6): 701-709.
32. Marques FO, Libório AB, Daher EF. Effect of chloride dialysate concentration on
metabolic acidosis in maintenance haemodialysis patients. Braz J Med Biol Res, 2010; 43
(10): 996- 1000.
33. Leal VO, Delgado AG, Leite M Jr, Mitch WE, Mafra D. Influence of renal function and
diet on acid-base status in chronic kidney disease patients. Journal of Renal Nutrition,
2009; 19(2): 178-182.
34. Sean M. Bagshaw, R.T. Noel Gibney, Peter Kruger, Imran Hassan, Rinaldo Bellomo, The
effect of furosemide in critically ill patients with early acute kidney injury (the SPARK
Page 26
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1525
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
study).bio med central: 2010: http://www.trialsjournal.com/content/11/1/50.
35. D.P.Gabriel, J.T.Caramori, L.C.Martim, P.Barretti1A.L.Balbi. High volume peritoneal
dialysis Vs daily hemodialysis: A randomized, controlled trial in patients with acute
kidney injury. Kidney Int Suppl, 2008; 73: 87-93.
36. Jonatan Barrera-Chimal, Rosalba Pérez-Villalva, Roxana Rodríguez-Romo, Juan Reyna,
Norma Uribe. Spironolactone prevents chronic kidney disease caused by ischemic acute
kidney injury. Kidney international, 2012; 83: 93-103.
37. Marcello Tonelli, Anita M. Lloyd, Aminu K. Bello, Matthew T. James, Scott W.
Klarenbach, Finaly A. McAlister, et.al. Statin use and the risk of acute kidney injury in
older adults. BMC nephrology, 2019; 20: 103.
38. Nawal Salahuddin, Mustafa Sammani, Ammar Hamdan, Mini Joseph, Yasir Al-Nemary,
Rawan Alquaiz, et.al. Fluid Overload is an independent risk factors for acute kidney
injury in critically III patients. BMC nephrology, 2017; 18: 45.
39. Toshiyuki Nakao, Yoshie Kanazawa, Toshimasa Takahashi. Once-weekly hemodialysis
combined with low protein and low salt dietary treatment as a favourable therapeutic
modality for selected patients with end stage renal failure: a prospective observational
study in Japanese patients. BMC nephrology, 2018; 19(151): 0941-2.
40. Asharf I. Mikhail, Staffan Schon, Sylvia Simon, Christopher Brown, Jorgen B.A.
Hegbrant, Gert Jensen, et.al. A prospective observational study of iron isomaitoside in
haemodialysis patients with chronic kidney disease treated for iron deficiency (DINO).
BMC nephrology, 2019; 20(13): 1159.
41. Minseon Park, Rino So, Kwon Wook Joo, Hyung-Jin Yoon. Association between lower
serum bicarbonate and renal hyper filtration in the general population with preserved
renal function: a cross sectional study. BMC nephrology, 2016; 17(3): 0218-24.
42. Rolando Claure Del Granado, Ravindra L Mehta. Fluid Overload in the ICU: evaluation
and management. BMC nephrology, 2016; 17: 109-24.
43. Claus P. Schmitt, Borje Haraldsson, Rouven Doetschmann, Mirjam Zimmering, Christine
Greiner, Michael Boswald, et.al. Effects of pH- neutral, bicarbonates- buffered dialysis
fluid on peritoneal transport kinetics in children. Kidney international, 2002; 61: 1527-36.
44. Michael Blankenburg, Csaba P. Kovesdy, Anne kathrin Fett, Raymond G Griner, Alain
Gay. Disease characteristics and outcomes in patients with chronic kidney and type 2
diabetes: a method cohort study of spironolactone users and non- users. International
society of nephrology, 2012; 83: 93-103.
45. Wei Chen, Matthew K Abramowitz. Metabolic acidosis and the progression of chronic
Page 27
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1526
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
kidney disease. BMC nephrology, 2014; 15: 55.
46. Gomez H1, Kellum JA2. Understanding acid base disorders. Ulster Med J, 2017; 8, 86(3):
161-66.
47. Jason D Guffey, Curtis E Has, Amber Crowley, Kathryn A Connor and David C
Kaufman. Hydrochloric acid infusion for treatment of metabolic alkalosis in ICU: effects
on acid-base balance and oxygenation. Ann Pharmacother, 2018; 52(6): 522-526.
48. Najah R Hadi, Fadhil G Al-Amran, Ayad A Hussein. Effects of thyroid hormone analogue
and a leukotriene pathway- blocker on renal ischemia/reperfusion injury in mice. BMC
nephrology, 2011; 70(12): 3712.
49. Yuichi Maruta, Takeshi Hasegawa, Etsuko Yamakoshi, Hiroki Nishiwaki, Fumihiko
Koiwa,Enyu Imai. Association between serum Na-cl level and renal functions decline in
chronic kidney disease results from the chronic kidney disease japan cohort (CKD-JAC)
study. Clinical and experimental nephrology, 2018; 23: 215-222.
50. Zaw Ther, Aung Ko Win, Eugenie Pedagogos, Jennifer Beavis, Sandra Crikis, Craig
Nelson. Differential effects of phosphate binders on predialysis serum bicarbonate in end-
stage kidney disease patients on maintenance haemodialysis. BMC Nephrology, 2013; 14:
205.
51. Golaleh Asghari, Momenan M, Yuzbashian E. Dietary pattern and incidence of KD
among adults a population based study in west Asian. Nutr Metab Lond, 2018; 15: 88.
52. Anoop Shankar, Klein R, Barbara E. The association among smoking, heavy drinking,
and CKD. American journal of epidemiology, 2006; 164(3): 263-271.
53. Griffin P Rodgers on kidney diseases statistics for the United States.NIDDK:
http://www.niddk.nih.gov/.
54. Ghatak I, Dhat V, Tilak M, and Roy I. Analysis of arterial blood gas report in CKD.
JCDR, 2016; 10(8): BC01-05.
55. Qiangwei Fu, Colgan SP, Shelly C S, Phil D. Hypoxia: the force that drives CKD showed
that the evidence indicating that CKD. Clinical medicine and research, 2016; 14(1):
15-39.
56. Thomas P C, Batuman V. Metabolic acidosis medication. Drugs & Diseases >
nephrology: MedGenMed: www.medicine.medscape.com.
57. Harris AN, Grimm PR, Lee HW, Delpire E, Fang L, Verlander JW, et al. Mechanism of
Hyperkalemia- induced Metabolic acidosis. J Am Soc Nephrol, 2018; 29(5): 1411-25.
58. Natale P, Palmer SC, Ruospo M, Saglimbene VM, Strippoli GF. Potassium binders for
chronic hyperkalaemia in people with chronic kidney disease. The Cochrane Database of
Page 28
www.wjpps.com │ Vol 10, Issue 2, 2021. │ ISO 9001:2015 Certified Journal │
1527
Anna et al. World Journal of Pharmacy and Pharmaceutical Sciences
Systematic Reviews, 2018; 11: 24-27.
59. Ruospo M, Palmer SC, Natale P, Craig JC, Vecchio M, Elder GJ, Srrippoli GFM.
Phosphate binders to prevent complications of chronic kidney diseae. The Cochrane
Database of Systematic Reviews, 2018; 22: 9-14.
60. Maher RL, Hanlon JT, Hajjar ER. Clinical consequences of polypharmacy in elderly.
Epert opin Drug Saf, 2014; 13(1): 57-65.