Vol. 4, 2625-2634, November 1998 Clinical Cancer Research 2625
Vascular Integrin av1�3: A New Prognostic Indicator in
Breast Cancer1
Giampietro Gasparini,2 Peter C. Brooks,
Elia Biganzoli, Peter B. Vermeulen,
Emanuela Bonoldi, Luc Y. Dirix,
Girolamo Ranieri, Rosalba Miceli, and
David A. ChereshDivision of Medical Oncology, Azienda Ospedaliera “Bianchi-
Melacrino-Morelli,” 89100 Reggio Calabria, Italy [G. G., 0. R.],Departments of Immunology and Vascular Biology, The Scripps
Research Institute, La Jolla, California 92037 [P. C. B., D. A. C.];Oncological Center and Angiogenesis Laboratory, St. AugustinusHospital, Wilrijk, B-2610, Belgium [P. B. V., L. Y. D.]; Departmentof Medical Statistics and Biometry, National Cancer Institute, Milan,20122 Milan, Italy [E. B., R. M.]; and Institute of Pathology, St.
Bortolo Hospital 36100 Vicenza, Italy [E. B.]
ABSTRACTBlood vessel density is a prognostic indicator of multi-
plc tumor types. Recently, it has been established that tu-
mor-associated blood vessels express elevated levels of inte-
grin aj�3. In fact, there is evidence that integrin avI�3identifies the most proliferative endothelial cells within hu-
man breast carcinomas. Therefore, we evaluated breast can-
cer tissue in terms of both blood vessel density and a��33
expression. We found that the antibody LM609 to integrin
a�I�3 preferentially stains the blood vessels of small caliber.
Furthermore, comparative studies between LM609 and
anti-CD31 antibodies on normal breast indicate that very
low and weak expression of integrin aj33 was found on
vessels within normal tissue, whereas CD31 antigen was
expressed in almost all vasculature. Indeed, expression of
integrin #{176}�vI�3was significantly higher in tumors of patients
with metastasis than in those without metastasis. In a series
of 197 consecutive patients with invasive breast cancer and
long follow-up, vascular expression of integrin a��33 in tu-
mor vascular “hot spots” was found to be the most signifi-
cant prognostic factor predictive of relapse-free survival in
both node-negative and node-positive patients. These find-
ings support the contention that angiogenesis plays a critical
role in breast cancer progression and suggest that integrin
Received 7/10/98; accepted 8/10/98.
The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby marked
advertisement in accordance with 18 U.S.C. Section 1734 solely to
indicate this fact.
I This study was supported in part by grants from the Associazione
Italiana per Ia Ricerca sul Cancro (Milan, Italy) and the Regione Veneto(Progetto Sanitario Finalizzato No. 675-01-96; Venice, Italy). D. A. C.was supported by NIH grants HL5444, CA50286, and CA45726.
2 To whom requests for reprints should be addressed, at Division ofMedical Oncology, Ospedali Riuniti, Via Melacrino, 89100 Reggio
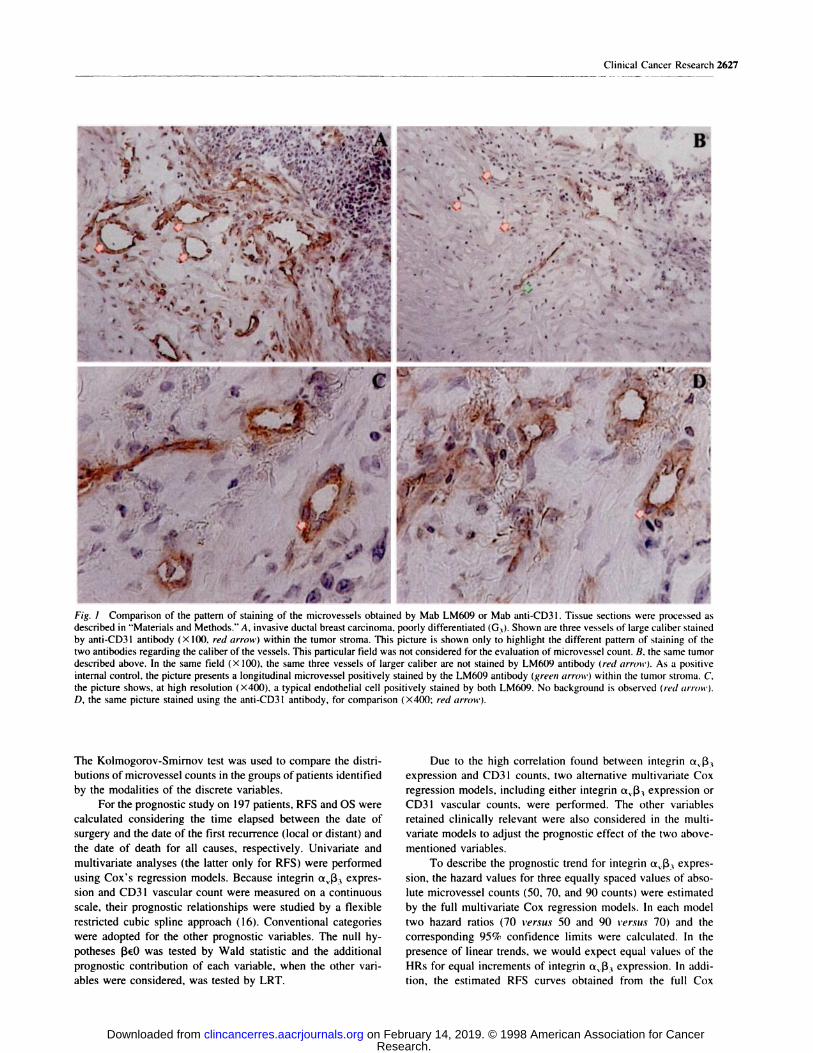
� . �.--.-. .� �r �Fig. I Comparison of the pattern of staining of the microvessels obtained by Mab LM609 or Mab anti-CD3 1 . Tissue sections were processed as
described in “Materials and Methods.” A, invasive ductal breast carcinoma, poorly differentiated (G3). Shown are three vessels of large caliber stained
by anti-CD31 antibody (X 100, red arrow) within the tumor stroma. This picture is shown only to highlight the different pattern of staining of the
two antibodies regarding the caliber of the vessels. This particular field was not considered for the evaluation of microvessel count. B. the same tumordescribed above. In the same field (X 100). the same three vessels of larger caliber are not stained by LM609 antibody (red arrmt-). As a positive
internal control, the picture presents a longitudinal microvessel positively stained by the LMflO9 antibody (green arrow) within the tumor strorna. C.the picture shows, at high resolution (X400), a typical endothelial cell positively stained by both LM609. No background is observed (red arrott’).
D, the same picture stained using the anti-CD3I antibody, for comparison (X400; red arrow).
The Kolmogorov-Smirnov test was used to compare the distri-
butions of microvessel counts in the groups of patients identified
by the modalities of the discrete variables.
For the prognostic study on 197 patients, RFS and OS were
calculated considering the time elapsed between the date of
surgery and the date of the first recurrence (local or distant) and
the date of death for all causes, respectively. Univariate and
multivanate analyses (the latter only for RFS) were performed
using Cox’s regression models. Because integrin a��33 expres-
sion and CD3 1 vascular count were measured on a continuous
scale, their prognostic relationships were studied by a flexible
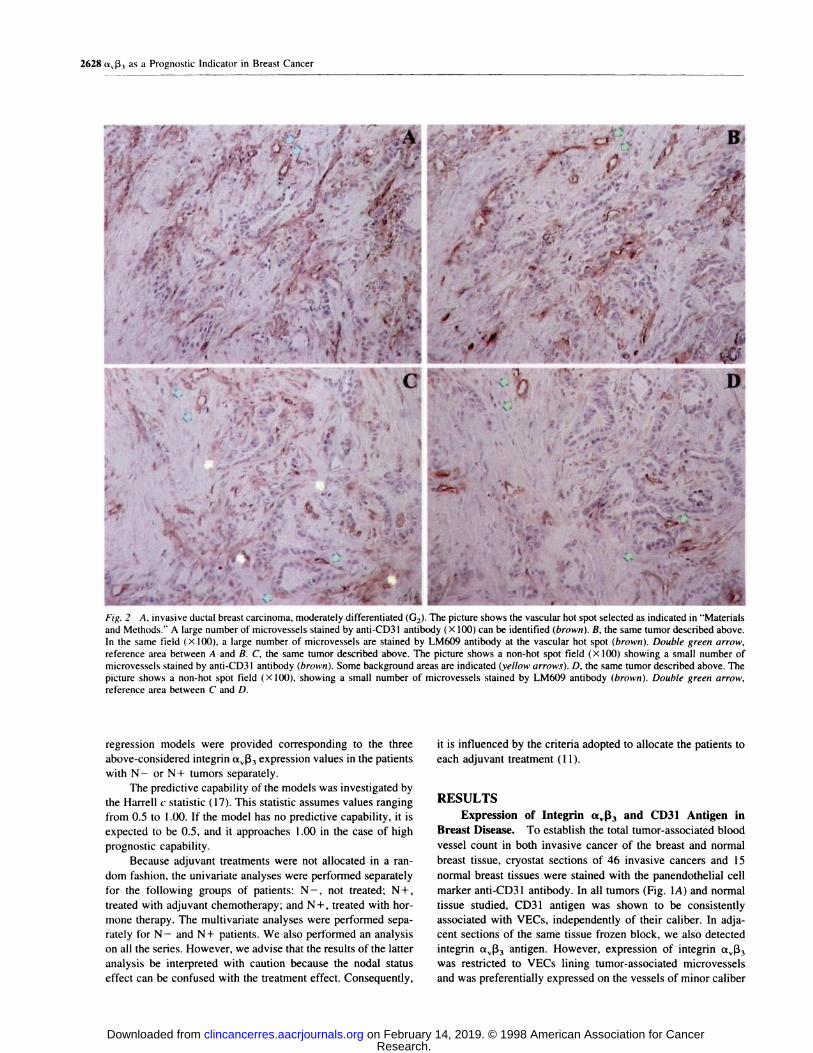
Fig. 2 A, invasive ductal breast carcinoma, moderately differentiated (02). The picture shows the vascular hot spot selected as indicated in “Materials
and Methods.” A large number of microvessels stained by anti-CD3I antibody (X 100) can be identified (brown). B, the same tumor described above.In the same field ( X I 00), a large number of microvessels are stained by LM609 antibody at the vascular hot spot (brown). Double green arrow,
reference area between A and B. C, the same tumor described above. The picture shows a non-hot spot field (X 100) showing a small number of
microvessels stained by anti-CD3 I antibody (brown). Some background areas are indicated (yellow arrows). D, the same tumor described above. Thepicture shows a non-hot spot field (X 100), showing a small number of microvessels stained by LM609 antibody (brown). Double green arrow,
reference area between C and D.
regression models were provided corresponding to the three
above-considered integrin ttv�33 expression values in the patients
with N - or N + tumors separately.
The predictive capability of the models was investigated by
the Harrell c statistic ( 17). This statistic assumes values ranging
from 0.5 to 1 .00. If the model has no predictive capability, it is
expected to be 0.5, and it approaches 1.00 in the case of high
prognostic capability.
Because adjuvant treatments were not allocated in a ran-
dom fashion, the univariate analyses were performed separately
for the following groups of patients: N-, not treated; N+,
treated with adjuvant chemotherapy; and N+, treated with hor-
mone therapy. The multivariate analyses were performed sepa-
rately for N - and N + patients. We also performed an analysis
on all the series. However, we advise that the results of the latter
analysis be interpreted with caution because the nodal status
effect can be confused with the treatment effect. Consequently,
it is influenced by the criteria adopted to allocate the patients to
each adjuvant treatment (1 1).
RESULTSExpression of Integrin a��3 and CD31 Antigen in
Breast Disease. To establish the total tumor-associated blood
vessel count in both invasive cancer of the breast and normal
breast tissue, cryostat sections of 46 invasive cancers and 15
normal breast tissues were stained with the panendothelial cell
marker anti-CD3 1 antibody. In all tumors (Fig. 1A) and normal
tissue studied, CD3 1 antigen was shown to be consistently
associated with VECs, independently of their caliber. In adja-
cent sections of the same tissue frozen block, we also detected
integrin ttv1�3 antigen. However, expression of integrin ttv�33
was restricted to VECs lining tumor-associated microvessels
and was preferentially expressed on the vessels of minor caliber
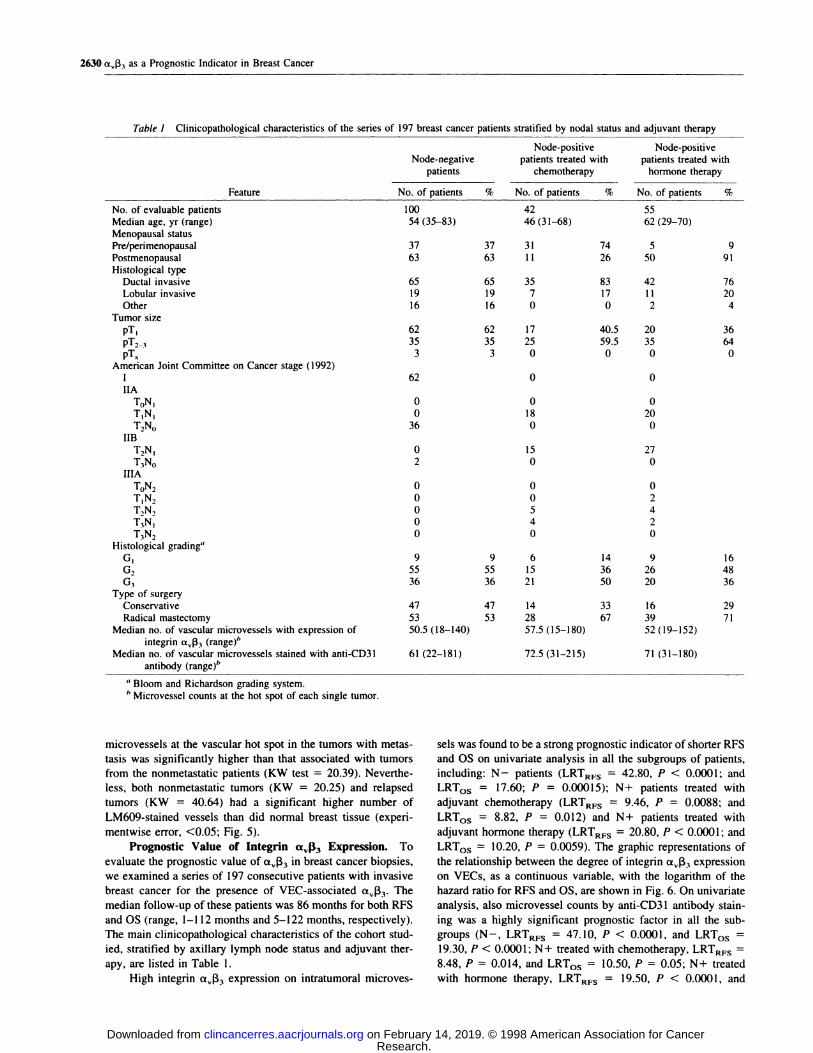
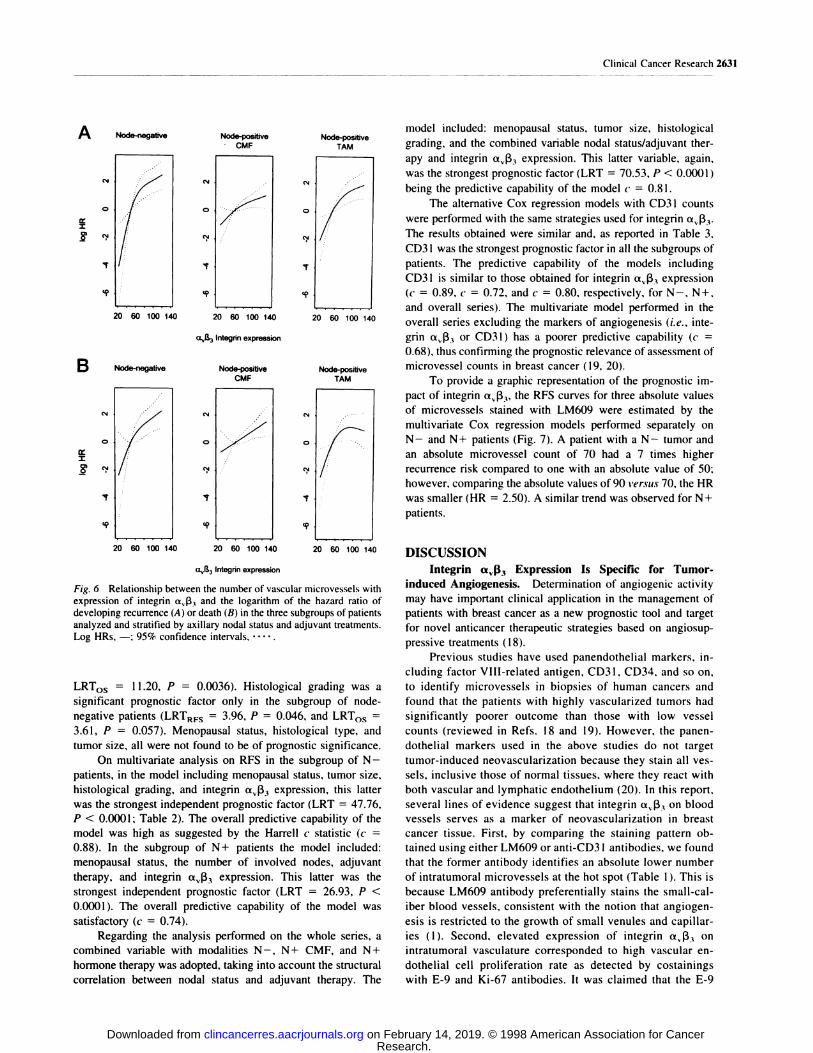
Fig. 6 Relationship between the number of vascular microvessels withexpression of integrin aJ33 and the logarithm of the hazard ratio ofdeveloping recurrence (A) or death (B) in the three subgroups of patients
analyzed and stratified by axillary nodal status and adjuvant treatments.Log HRs, -; 95% confidence intervals. . . ...
LRT05 = 1 1.20, P = 0.0036). Histological grading was a
significant prognostic factor only in the subgroup of node-
negative patients (LRTRFS 3.96, P 0.046, and LRT05
3.61, P = 0.057). Menopausal status, histological type, and
tumor size, all were not found to be of prognostic significance.
On multivariate analysis on RFS in the subgroup of N -
patients, in the model including menopausal status, tumor size,
histological grading, and integrin ttv�33 expression, this latter
was the strongest independent prognostic factor (LRT 47.76,
P < 0.0001 ; Table 2). The overall predictive capability of the
model was high as suggested by the Harrell c statistic (c
0.88). In the subgroup of N+ patients the model included:
menopausal status, the number of involved nodes, adjuvant
therapy, and integrin aj33 expression. This latter was the
strongest independent prognostic factor (LRT = 26.93, P <
0.0001). The overall predictive capability of the model was
satisfactory (c = 0.74).
Regarding the analysis performed on the whole series, a
combined variable with modalities N- , N+ CMF, and N+
hormone therapy was adopted, taking into account the structural
correlation between nodal status and adjuvant therapy. The
model included: menopausal status, tumor size, histological
grading, and the combined variable nodal status/adjuvant flier-
apy and integrin ttv1�3 expression. This latter variable, again,
was the strongest prognostic factor (LRT 70.53, P < 0.0001)
being the predictive capability of the model � 0.81.
The alternative Cox regression models with CD3 I counts
were performed with the same strategies used for integrin ttv�33.
The results obtained were similar and, as reported in Table 3,
CD3 I was the strongest prognostic factor in all the subgroups of
patients. The predictive capability of the models including
CD3 I is similar to those obtained for integrin a,j33 expression
(c 0.89, c 0.72, and c = 0.80, respectively, for N-, N+,
and overall series). The multivariate model performed in the
overall series excluding the markers of angiogenesis (i.e. , inte-
grin ttv1�3 or CD3 1 ) has a poorer predictive capability (c
0.68). thus confirming the prognostic relevance of assessment of
microvessel counts in breast cancer ( 1 9, 20).
To provide a graphic representation of the prognostic im-
pact of integrin ttv1�3� the RFS curves for three absolute values
of microvessels stained with LM609 were estimated by the
multivariate Cox regression models performed separately on
N- and N+ patients (Fig. 7). A patient with a N- tumor and
an absolute microvessel count of 70 had a 7 times higher
recurrence risk compared to one with an absolute value of 50;
however, comparing the absolute values of 90 versus 70, the HR
was smaller (HR = 2.50). A similar trend was observed for N+
patients.
DISCUSSIONIntegrin a�I.33 Expression Is Specific for Tumor-
induced Angiogenesis. Determination of angiogenic activity
may have important clinical application in the management of
patients with breast cancer as a new prognostic tool and target
for novel anticancer therapeutic strategies based on angiosup-
pressive treatments (18).
Previous studies have used panendothelial markers, in-
cluding factor VIII-related antigen, CD31, CD34, and so on,
to identify microvessels in biopsies of human cancers and
found that the patients with highly vascularized tumors had
significantly poorer outcome than those with low vessel
counts (reviewed in Refs. 18 and 19). However, the panen-
dothelial markers used in the above studies do not target
tumor-induced neovascularization because they stain all yes-
sels, inclusive those of normal tissues, where they react with
both vascular and lymphatic endothelium (20). In this report,
several lines of evidence suggest that integrin x��3 on blood
vessels serves as a marker of neovascularization in breast
cancer tissue. First, by comparing the staining pattern ob-
tamed using either LM609 or anti-CD3 I antibodies, we found
that the former antibody identifies an absolute lower number
of intratumoral microvessels at the hot spot (Table 1 ). This is
because LM609 antibody preferentially stains the small-cal-
iber blood vessels, consistent with the notion that angiogen-
esis is restricted to the growth of small venules and capillar-
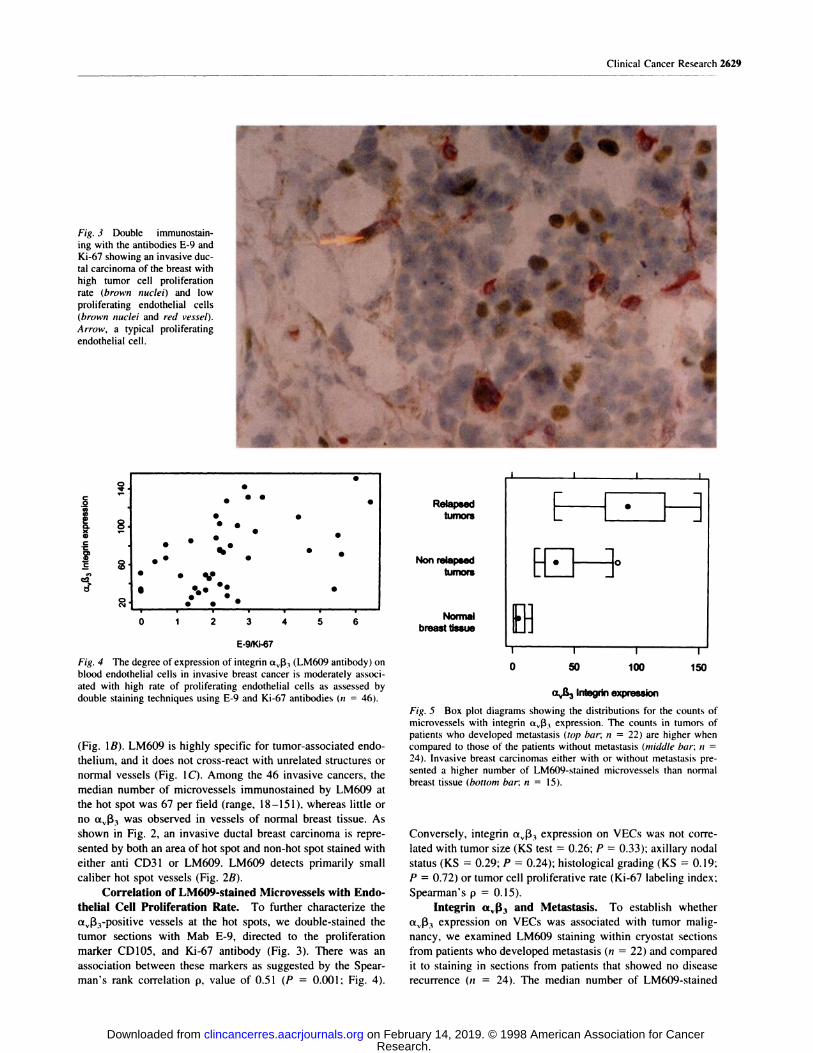
ies (1). Second, elevated expression of integrin a�ft, on
intratumoral vasculature corresponded to high vascular en-
dothelial cell proliferation rate as detected by costainings
with E-9 and Ki-67 antibodies. It was claimed that the E-9
P., Caffo, 0., Barbareschi, M., Boracchi, P., Marubini, E., and Pozza, F.Tumor microvessel density. p53 expression. tumor size and peritumorallymphatic vessel invasion are relevant prognostic markers in node-
negative breast carcinoma. J. Clin. Oncol., 12: 454-466, 1994.
14. Vermeulen. P. B., Dirix, L. Y., Libura, J., Vanhoolst, I. F., VanMarck, E., and Van Oosterom, A. T. Correlation of the fractions of
proliferating tumor and endothelial cells in breast and colorectal adeno-
carcinomas is independent of tumor histotype and microvessel density.
Microvasc. Res., 54: 88-92, 1997.
15. Hollander, M., and Wolfe, D. A. Nonparametric Statistical Meth-
ods. New York: John Wiley & Sons, 1973.
16. Gasparini, G., Toi, M., Gion, M.. Verderio, P.. Dittadi, R.,Hanatani, M., Matsubara, I.. Vinante, 0., Bonoldi, E., Boracchi, P.,
Gatti, C.. Suzuki, N., and Tominaga. T. Prognostic significance of
vascular endothelial growth factor protein in node-negative breast car-
cinoma. J. NatI. Cancer Inst. (Bethesda), 89: 139-147, 1997.
17. Harrell, F. E., Lee, K. L., and Mark, D. B. Tutorial in biostatistics.
Multivariable prognostic models: issues in developing models, evaluat-
ing assumptions and adequacy, and measuring and reducing errors. Stat.
Med., 15: 361-387, 1996.
18. Gasparini, G., and Harris, A. L. Clinical importance of the deter-
mination of tumor angiogenesis in breast carcinoma: much more than a
new prognostic tool. J. Clin. Oncol., 13. 765-782, 1995.
19. Gasparini, G. Current controversies in cancer. Is determination ofangiogenic activity in human tumours clinically useful? Eur. J. Cancer,
34: 615-618, 1998.
20. Vermeulen, P. B., Gasparini, G., Fox, S. B., Toi, M., Martin, L.,
McCulloch. P., Pezzella, F., Viale. G., Weidner, N., Harris. A. L., andDirix, L. Y. Quantification of angiogenesis in solid human tumours: aninternational consensus on the methodology and criteria of evaluation.
Eur. J. Cancer. 32A: 2474-2484, 1996.
21. Wang, J. M., Kumar, S., Pye. D., Haboubi, N., and Al-Nakib, L.
Breast carcinoma: comparative study of tumor vasculature using twoendothelial cell markers. J. Natl. Cancer Inst. (Bethesda), 86: 386-388,
1994.
22. Weidner, N., Folkman, J., Pozza, F., Bevilacqua, P., Allred. E. N.,Moore, D. H., Meli, S., and Gasparini, G. Tumor angiogenesis: a newsignificant and independent prognostic indicator in early-stage breast
carcinoma. J. Nail Cancer Inst. (Bethesda), 84: 1875-1887, 1992.
23. Gasparini, G., Fox, S. B., Verderio, P., Bonoldi, E., Bevilacqua,
P.. Boracchi, P., Dante, S., Marubini, E., and Harris, A. L. Determi-nation of angiogenesis adds information to estrogen receptor status in
predicting the efficacy of adjuvant tamoxifen in node-positive breast
cancer patients. Clin. Cancer Res., 2: 1 191-I 198, 1996.
24. Gutheil, J. C., Campbell, T. N., Pierce, P. R., Watkins, J. D., Huse,
W. D., Bodkin, D. J., Hart, J., and Cheresh. D. A. Phase I study ofvitaxin, an anti-angiogenic humanized monoclonal antibody to vascular
integrin a�l�3 Proc. Am. Soc. Clin. Oncol. 17: 2lSa, 1998.
25. Ruegg, C., Yilmaz, A., Bieler, G., Bamat, J., Chaubert, P., andLejeune, F. J. Evidence for the involvement of endothelial cell integrin
av1�3 in the disruption of the tumor vasculature induced by TNF and
IFN--y. Nat. Med., 4: 408-414, 1998.
26. Gasparini, G. Antiangiogenic drugs as a novel anticancer therapeu-
tic strategy. Which are the more promising agents? What are the clinical
developments and indications? Crit. Rev. Oncol. Hematol., 26: 147-
1998;4:2625-2634. Clin Cancer Res G Gasparini, P C Brooks, E Biganzoli, et al. breast cancer.Vascular integrin alpha(v)beta3: a new prognostic indicator in