100
14 Vascular Portfolio: DVT Reflection Paige Fabre 13654584
14
Vascular Portfolio: DVT Reflection Paige Fabre
13654584

DVT Reflection
To demonstrate a level of competence in DVT studies I have compiled the notes (audio and written) from an in house tutorial on arm DVT’s, a presentation of imaging protocol and patient preparation and self-directed report on DVT.
Evidence Piece 1 – Tutorial Notes
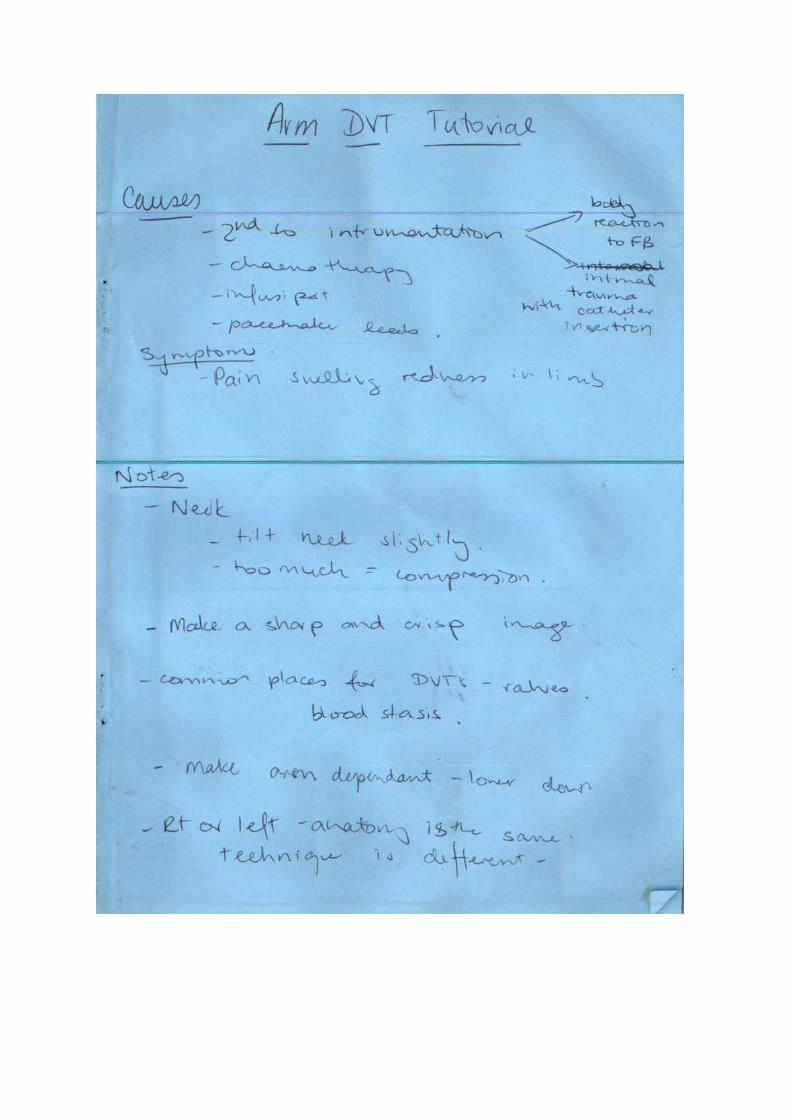
In our practice it was decided that all newly qualified sonographers should be able to perform arm DVT scans as we all standardly perform leg DVT scans. To facilitate this, an in-house tutorial by a senior sonographer was conducted. The notes taken for this piece were made into a booklet that I now keep for future reference. The notes make reference to anatomical points of confusion (mistaking nerves for non-compressible veins) as well as recognising normal. In addition they cover reasons why we may be asked to complete the scans and what areas of patient history are highly important.
Before this tutorial I had seen two arm scans and completed two with the assistance of my supervising sonographers. The technique for the scans I found very similar to lower limb scans but variations in respiration reactions and anatomy variations made me nervous to perform the scan alone. After completing this tutorial and revising these notes I now feel more comfortable completing the scan. In addition I have also had a chance to practice techniques and on other trainee and newly qualified sonographers (with the assistance of more experienced sonographers) which has improved my confidence in identifying DVT in the upper limb. I do however recognise that it still takes me longer than others to complete the scan but with continued practice I intend to become more than competent with these scans.
I have intended this piece to aid in demonstrating my competence in statements 1 and 3. In terms of competence 1, this piece has helped me to better understand our practice protocols regarding upper arm DVT studies. The information that I gained from this tutorial has been incorporated into Evidence Piece 2 – DVT protocols.
It is my belief that is our in our duty of care to our patients to gain further knowledge about how to best to perform imaging examinations. By attending this tutorial and endeavouring to increase my knowledge base and confidence in these scans I am better equipped to perform their diagnostic study. In addition learning about various patient positioning techniques allows me to accommodate for patients with additional needs. For example, upon reflection I believe that learning to scan a patient erect gives me the ability to adjust my scanning technique for patients in wheelchairs without them having to transfer to the bed. In terms of patient management, this adjustment to my usual scanning technique (lying the patient down) can make the patient feel safe as they do not have to physically move. This may particularly important for patients who are falls risks.
Evidence Piece 2- DVT Protocol PowerPoint
This piece is presented as a demonstration of my imaging ability and patient care. The protocol presented here is a combination of our practice protocol and techniques and skills that I have learnt from tutors, colleagues and radiologists. In describing our practice protocol I was able to reaffirm

that I am completing studies to a diagnostic standard and therefore providing the best imaging service for my patients. By providing images that I had taken alongside the protocol description it was my intention to show that I understand what is expected from these examinations.
Reflecting on this piece I realised that I had tried to use clear examples of each image and consequently used images from multiple patients. Though most of the images were from one particular patient, this piece highlighted areas where I may need to improve my imaging. Though I understand that my technique will improve with experience and that “perfect” pictures are not always possible, where a high image quality is possible it should be obtained. In my original submission for review, a comment was made about incomplete compression of vessels on an image and that I should possibly make not of why this occurred. My first initiative was to replace the image in the series. After completing the piece I realised it is not just a point of replacing an image but recognising that I have displayed an image where a vessels did not appear completely compressed and suggest that there was no DVT in this area. I know that in this particular case a valve was present in the area of compression however this was not made clear. In the future I intend to be a little more aware of this when imaging DVT studies, in particularly including images that appear pathological in the absence of pathology. Through my demonstration of imaging I believe that this piece supports competency in Statement 1.
In addition I believe this piece also supports my competency in statement 3. Descriptions of patient preparation show my consideration of the differences in patients including cultural and physical. Each patient is an individual and how you interact with them in an examination should be tailored to them. Reflecting on this part of the piece I have come to recognise that I did not include techniques for bed bound patients. I think that this is mostly because it is an area in which I have limited experience. Though I am competent in patient management in the outpatient clinical setting, I believe to become more proficient I will need to expand my techniques to incorporate the hospital setting.
Evidence Piece 3: Self Direct DVT Report
This report is a demonstration of my competence as it relates statement 2. While I am confident and competent in identifying DVT, I decided to present this piece display how I have broadened my knowledge of deep vein thrombosis so that I am better able to perform these scans. When I initiated this piece I had a basic understanding of DVT. I was able to identify it on ultrasound and understood the importance or recognising thrombosis. While compiling this information, I learnt more about disorders and the factors that may affect the probability of DVT in certain groups; in particular those with hypercoagulability disorders. One thing that I discovered was that there is still a lot of research needed to find alternative methods of thrombosis resolution with less impact on coagulation states. In combination with Evidence Piece 1, I believe I have demonstrated competence in the identification and investigation of pathology in the deep vein system.

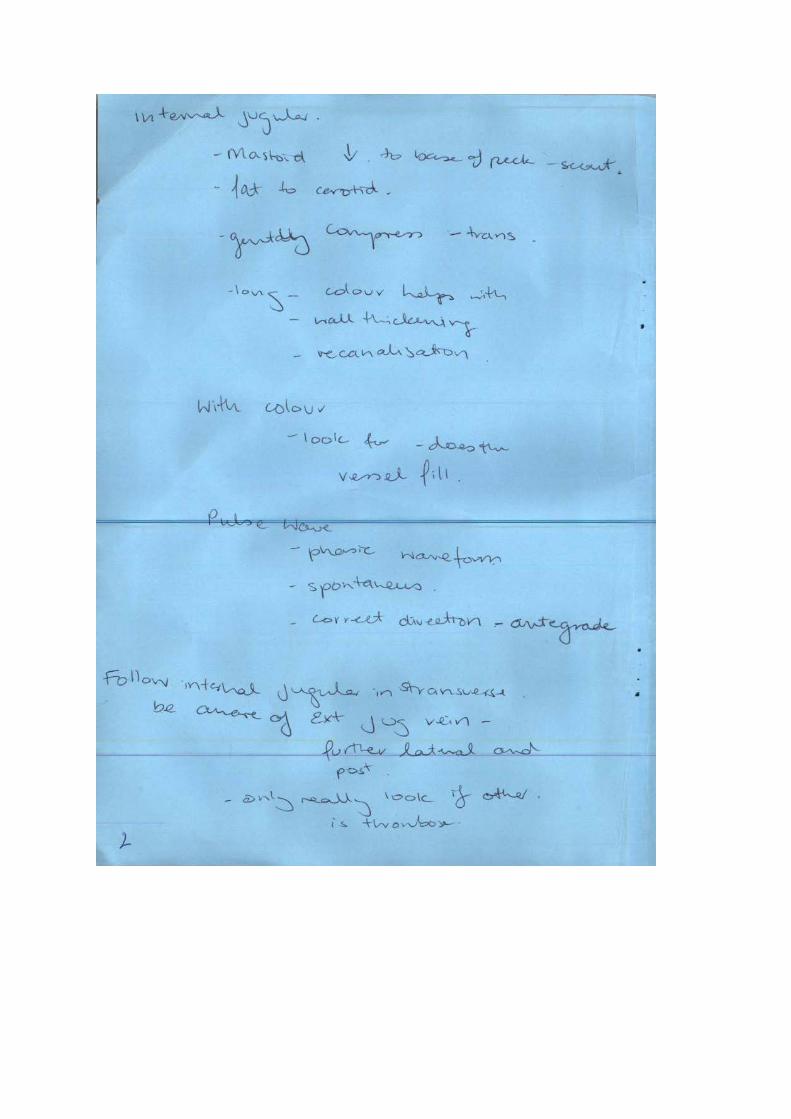
The following are the notes taken from an in-house tutorial aimed at trainee and newly qualified sonographers to allow
them to confidently perform upper limb DVT studies as part of their daily practice.
DVT Portfolio Paige Fabre 13654584







Reflection
This tutorial was taken by one of my senior colleagues. The tutorial was hands on and we used other trainees and newly qualifies sonographers to practice on. During the tutorial we were able to ask questions to better help with our understanding.
Prior to this tutorial I had only seen one upper limb DVT and scanned, with assistance, one myself. When I watched the scan with one of my colleagues I first found it a little confusing I wasn’t quite sure of how you correctly obtain the image and what you were looking for in the waveforms.
When I first attempted an upper limb scan I did so with a lot of assistance navigating the jugular to axillary region which appears to be the most difficult and the most important area.
After this tutorial I feel a lot more comfortable in performing upper limb DVT studies. The hands on approach on normal patients allowed me to better understand what I was looking for and how to obtain the images needed.
As a supplement to this piece I have also attached and audio file coving the upper limb from the axilla to the wrist.
Points of Practice learned from this tutorial:
• It all starts with good patient preparation and technique – The examination will be easier if you have correct machine settings, good patient positioning and good ergonomics
• A simple method to remember what “normal” blood flow is – SAP. Flow should be: o S – Spontaneous o A – Ante grade o P – Phasic
• Obtain a good clinical history to ascertain if the patient has any underlying factors - previous infusaports, Picc lines, traumatic catheter insertions.
• Where vessels are difficult to compress, colour Doppler imaging is imperative
DVT Protocols The following provides details of Upper and Lower Limb DVT protocols used in our practice.
Paige Fabre 13654584

DVT Studies • The aim of this examination is to determine the patency of the of the deep
vessels in the lower limb.
• To be determined patent a vessel must: Collapse completely on compression NOT display thrombus in the longitudinal or transverse plane Exhibit complete colour filling on Colour Doppler Display appropriate spectral trace characteristics:
Phasicity Spontaneity Response to augmentation/ Valsalva
• If these criteria are not met, a DVT may be present
• An image example of a thrombosis in the lower and upper limb as demonstrated in the following slides

DVT of the Lower Limb Note the incomplete compression with echogenic material within the vessel lumen.
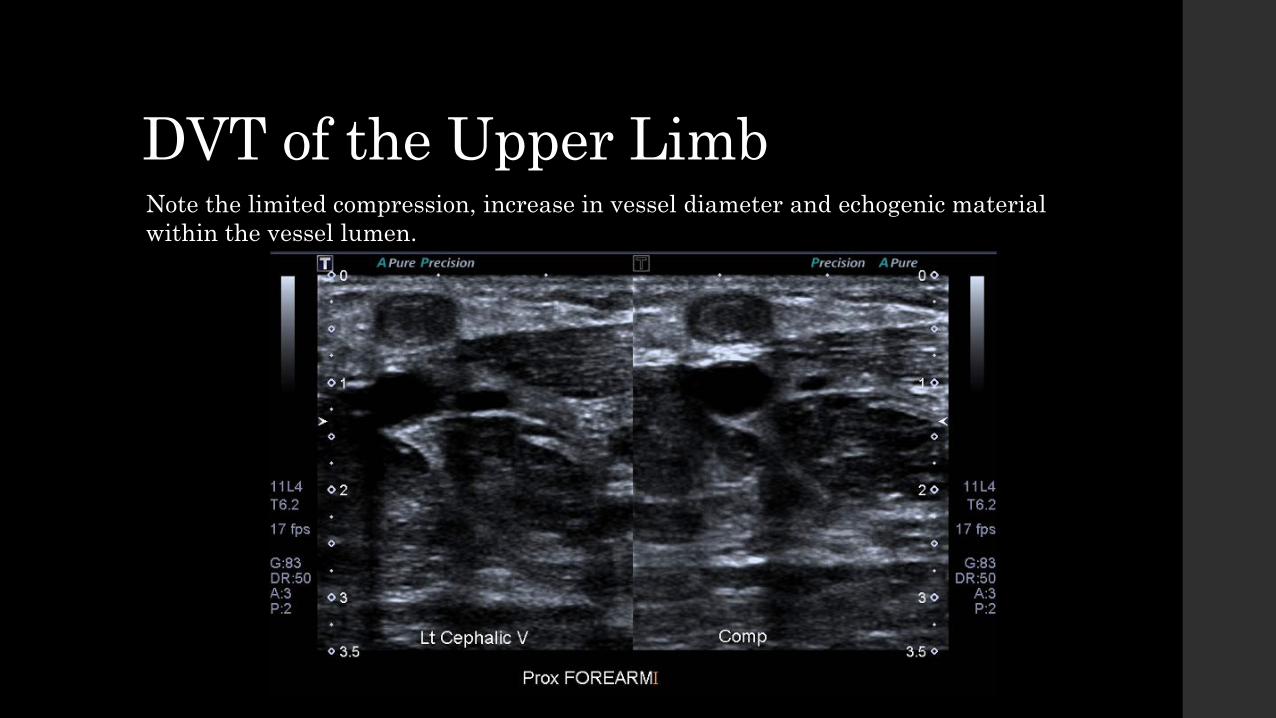
DVT of the Upper Limb Note the limited compression, increase in vessel diameter and echogenic material within the vessel lumen.
DVT Studies • Pitfalls include of DVT studies include
Non compression of vessels due to inadequate pressure as a result of user error, increased patient body habitus or muscle tension
Inadequate colour filling due to poor colour Doppler settings Lack of spectral Doppler information due to
Poor Doppler settings Increased age causing decreased spontaneity and phasicity in the venous system Inadequate venous pressure due to patient position
Inadequate B-mode imaging due to User error Increased patient body habitus Poor acoustic window

Lower Limb DVT

Work Sheet for Examination • At our practice the adjacent
worksheet is used to document the study. It should be completed with every study
• This is to allow for a better understanding of any thrombosis by the reporting radiologist as well as aid in reproducibility when the patient returns for a follow up scan.
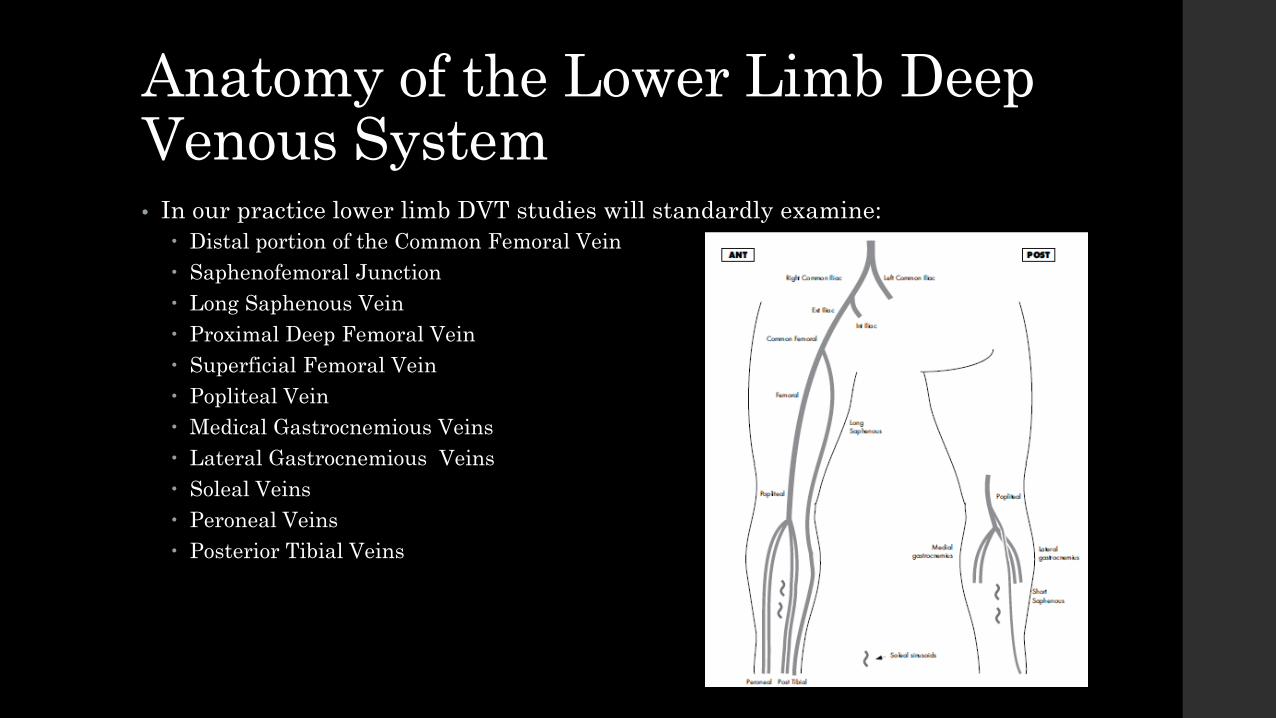
Anatomy of the Lower Limb Deep Venous System • In our practice lower limb DVT studies will standardly examine:
Distal portion of the Common Femoral Vein Saphenofemoral Junction Long Saphenous Vein Proximal Deep Femoral Vein Superficial Femoral Vein Popliteal Vein Medical Gastrocnemious Veins Lateral Gastrocnemious Veins Soleal Veins Peroneal Veins Posterior Tibial Veins

Patient and Room Preparation

Patient and Room Preparation • Before the patient is collected from the waiting area the room should be
prepared for them.
• This means: The head of the bed should be raised to allow for patient comfort and adequate
pressure on the lower circulatory system Adequate amounts of gel should be easily available throughout the scan The machine should be set at an appropriate height either for sitting or standing A variety of transducers should be easily accessible before and during the
examination. These should include: High frequency linear probes for superficial structures and thin patients e.g. 12 MHz High frequency linear probe for slightly deeper vessels to allow for high resolution imaging at
depth e.g. 7 MHz Lower frequency curved probe for deeper vessels (for example soleal, posterior tibial and
peroneal veins) and for patients of larger body habitus e.g. 3-5 MHz As these examination can be very messy, a towel should be made available to clean
off gel as the scan progresses and at its conclusion. In addition, a towel should be provided for patient modesty.

Patient and Room Preparation
Appropriate Gel
Curvilinear Probe for deeper penetration
Linear Vascular Probe for deep veins
High Frequency Linear Probes for superficial structures
Higher Frequency Curvilinear Probe for deeper penetration while maintaining resolution

Patient and Room Preparation • Once previous examinations and current examination request have been
reviewed the patient should be: Collected from the waiting area Greeted and made to feel welcome Identified as the correct patient in a private area to ensure that their privacy is
respected Changed into an appropriate gown.
• In my practice the patient is asked to change into the gown provided and remove their garments from the waist down, leaving their underpants on.

Patient and Room Preparation • Once the patient has changed they are brought into the room.
• A brief explanation of the examination should be given to the patient and their consent gained.
• The patient should be informed about results delivery. At our practice, after discussion with the radiologist, the patient is informed whether a DVT is present. If there is no DVT present the patient may leave the department and return to their
doctor as usual and the report is forwarded to the referrer If there is a DVT the patients referring doctor is advised by telephone and how they
proceed from there is dependant on the discussion between the referring radiologist and the patients practitioner.
• After the patient’s identity has again been confirmed then the patient is asked to lie of the bed with their head on the pillow.

Patient History • A good patient history should be established at the beginning of the scan
however it is very important not to limit dialogue to the beginning and the conclusion of the scan.
• Communication between oneself and patient should remain open to allow the sonographer to ask additional questions where needed and patient to communicate any additional information (tender areas, if they are feeling faint or uncomfortable etc.).
• Questions asked of the patient should include but are not limited to: Any history of previous DVT? Are they currently on anticoagulants? Has there been any recent long distance travel or period of immobility? Is there any history of previous surgery to the leg, in particular to the venous
system including vein stripping? Is there/ where is the site of pain/swelling? And how long has the persisted?

Patient Positioning
Upper: Patient lies with the head and upper body elevated to increase pressure on the lower venous system.
Lower: Patient is asked to sit up and swing their legs to the side of the bed with their effected leg resting on the sonographers lap. This also allows for increased pressure on the venous system and relaxes the muscles in the calf to allow for easier compression of the vessels.
During the examination I have been taught to employ the following positions for the upper and lower portions of the leg.

Lower Limb Protocol

Lower Limb DVT Study Protocol The following protocol is as dictated in our practice protocol manual:
Image 1 to 5 completed in a duel screen format. These images are taken in the transverse plane in B mode.
1. Common Femoral Vein (non compressed and compressed)
2. Common Femoral Vein and Long Saphenous Vein Junction (non compressed and compressed)
3. Femoral Vein Proximal (non compressed and compressed)
4. Femoral Vein Mid (non compressed and compressed)
5. Femoral Vein Distal (non compressed and compressed)
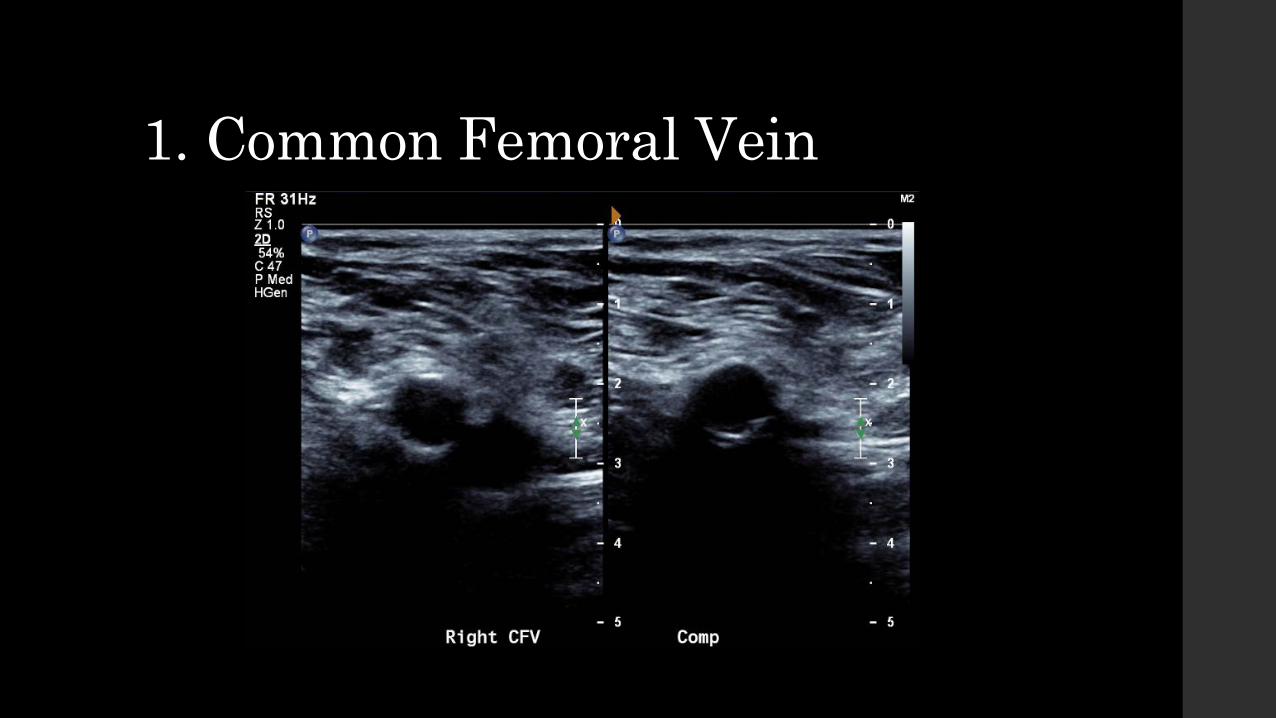
1. Common Femoral Vein
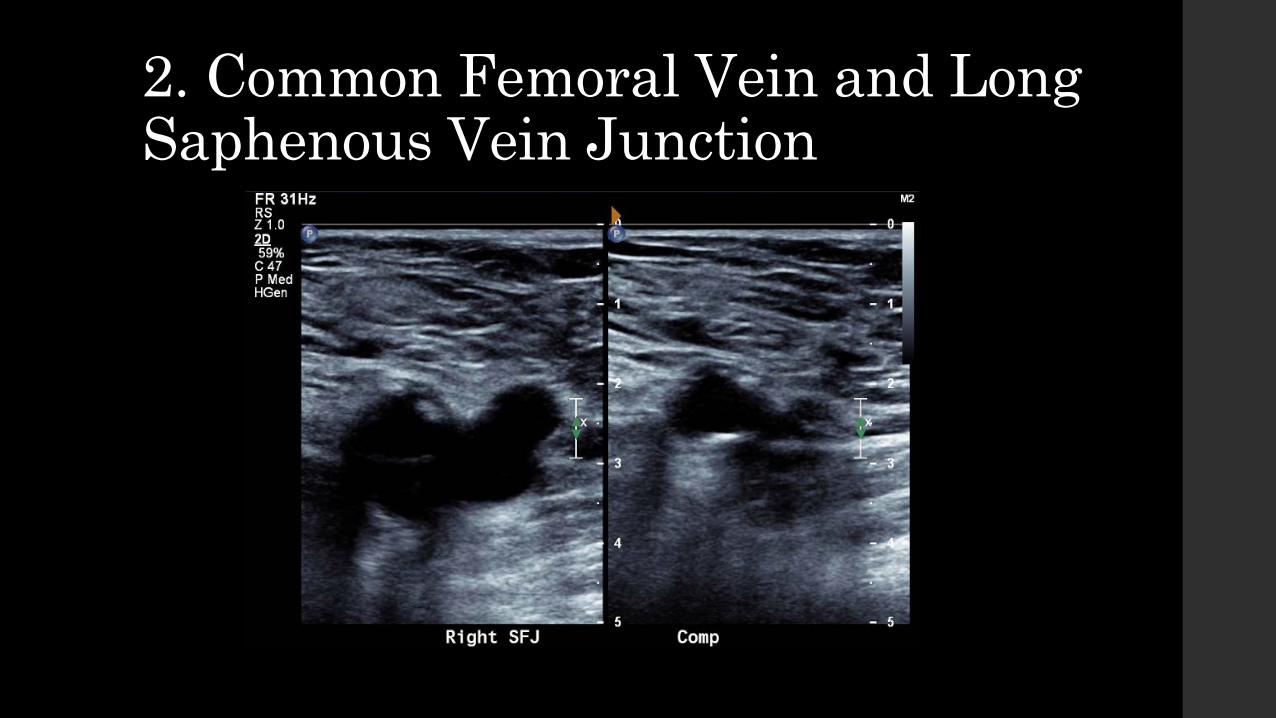
2. Common Femoral Vein and Long Saphenous Vein Junction
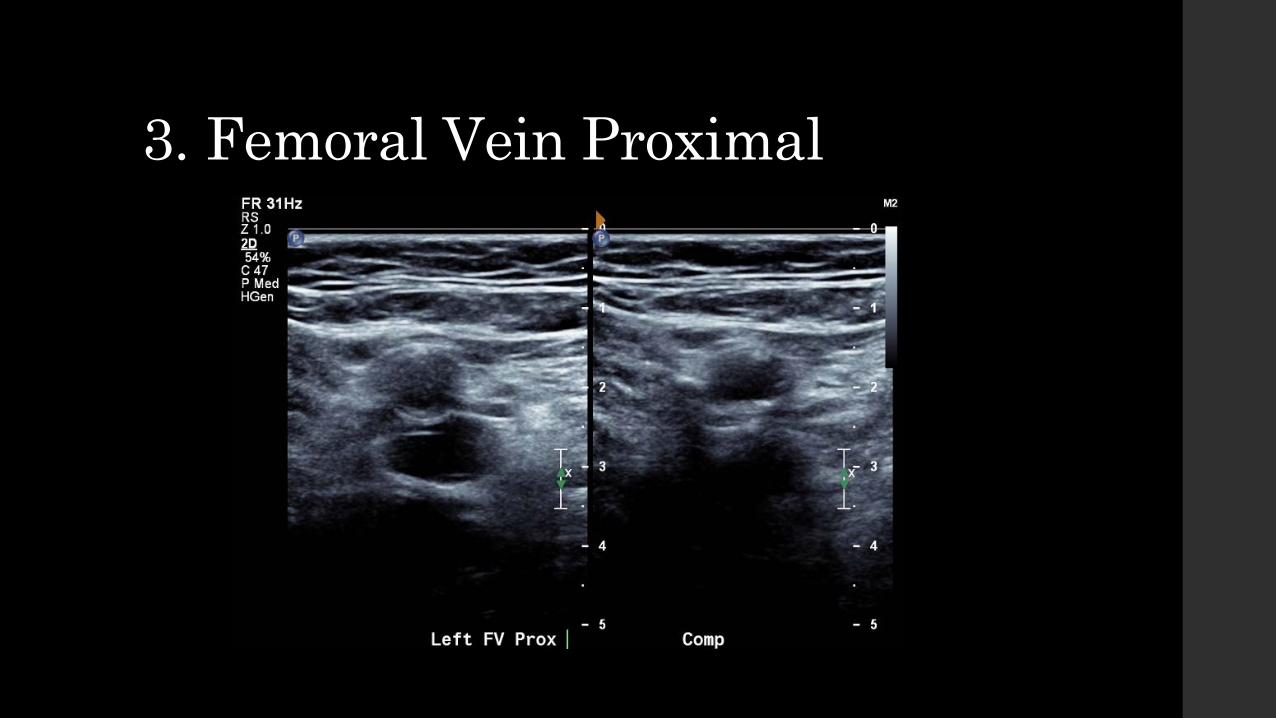
3. Femoral Vein Proximal

4. Femoral Vein Mid

5. Femoral Vein Distal

Lower Limb DVT Study Protocol Images 6 through 13 are taken in single screen format.
6. Spectral trace of the Common Femoral Vein
7. Colour Doppler image of the Common Femoral Vein and Long Saphenous Vein
8. Colour Doppler Image of the Common Femoral Vein and Femoral Vein
9. Spectral trace of the Deep Femoral Vein
10. Spectral trace of the Proximal Femoral Vein
11. Spectral trace of the Mid Femoral Vein
12. Spectral trace of the Distal Femoral Vein
13. Spectral trace of the Distal Femoral Vein with augmentation
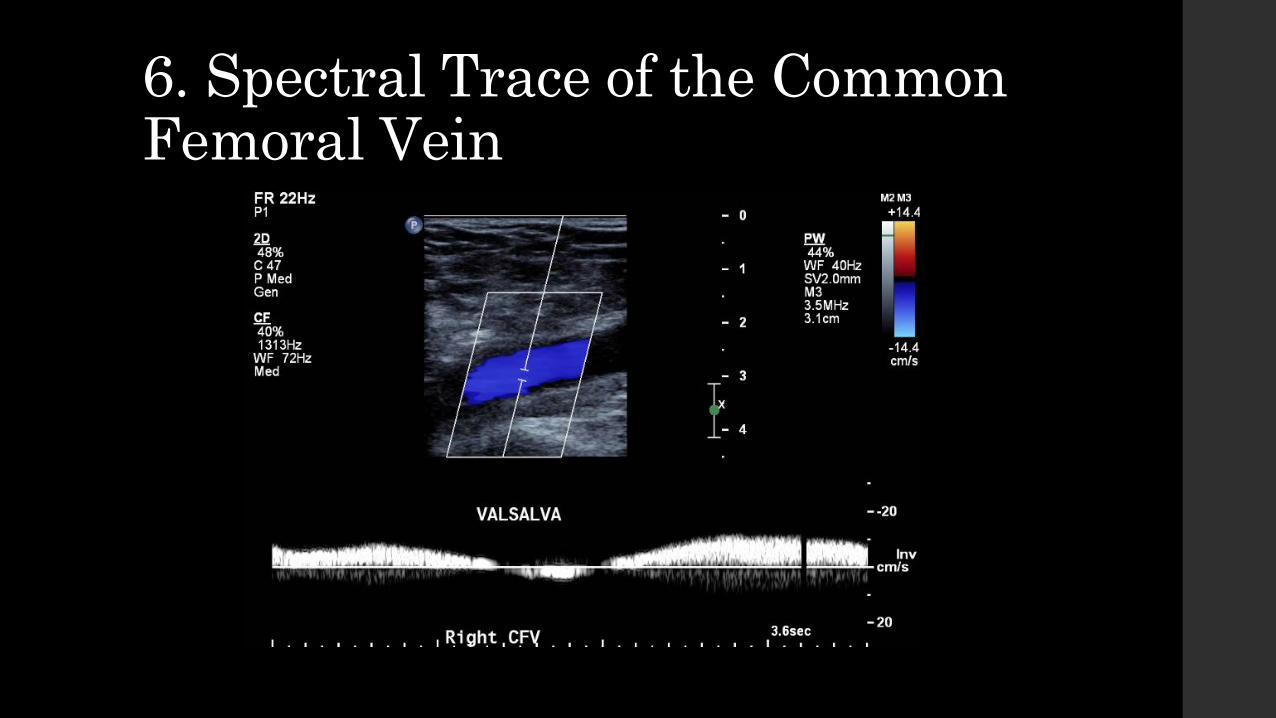
6. Spectral Trace of the Common Femoral Vein

7. Colour Doppler of the Common Femoral Vein and Long Saphenous Vein

8. Colour Doppler of the Common Femoral Vein, Deep Femoral Vein and the Femoral Vein

9. Spectral Trace of the Deep Femoral Vein

10. Spectral Trace of the Proximal Femoral Vein

11. Spectral Trace of the Mid Femoral Vein

12. Spectral Trace of the Distal Femoral Vein
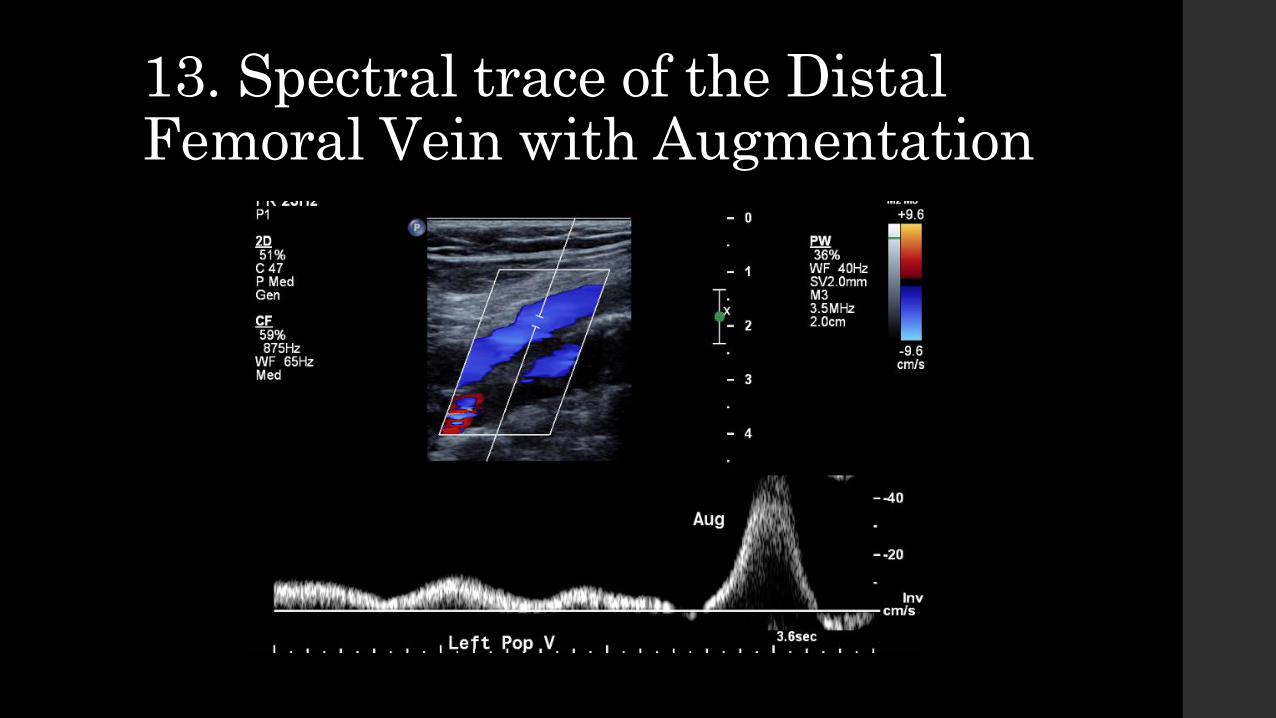
13. Spectral trace of the Distal Femoral Vein with Augmentation

Lower Limb DVT Study Protocol Imaging of the limb below the knee is variable and is dependant on the individual sonographers preference as well as reporting radiologist preference.
Imaging must contain:
• Compression of the Popliteal Vein in duel screen format
• Colour Doppler Image of the Popliteal Vein
• Spectral trace of the Popliteal Vein
• Duel screen compression images of the calf veins either singly or as a group – most of the variation between studies occurs in these images

14. Compression of the Popliteal Vein

15. Colour Doppler Image of the Popliteal Vein
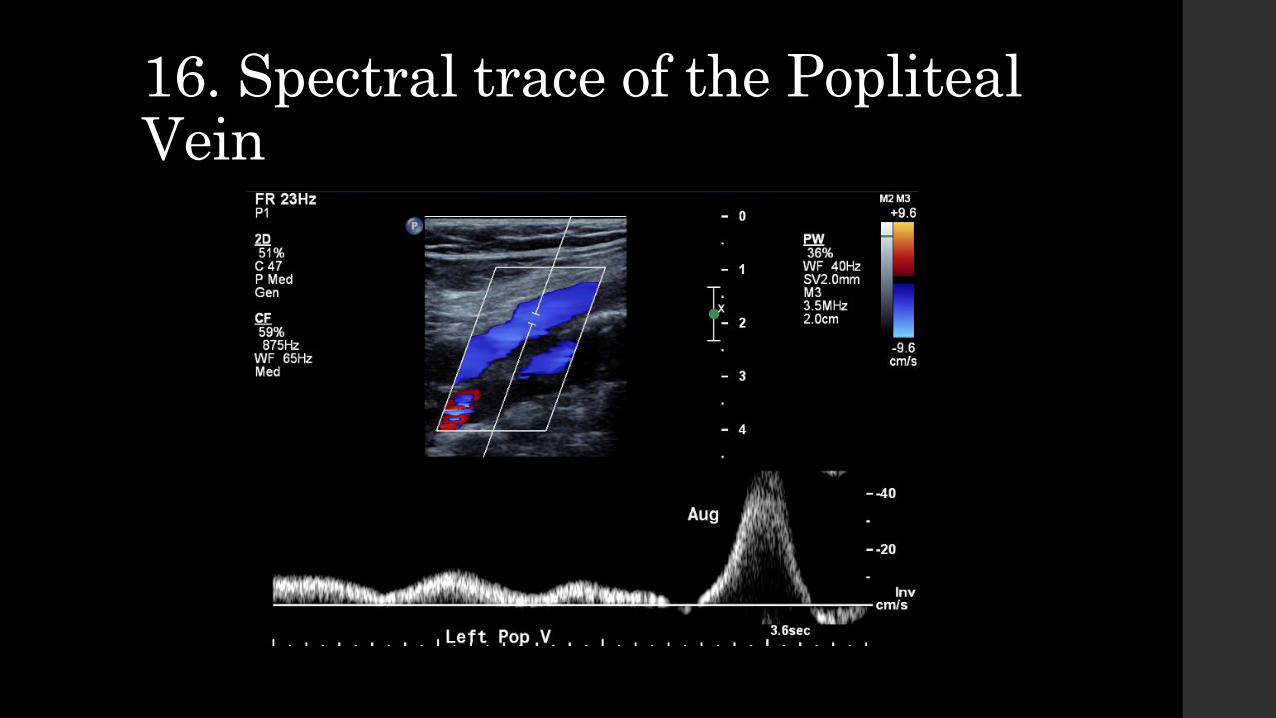
16. Spectral trace of the Popliteal Vein

Calf Veins Protocol for the Calf Veins is variable between sonographers. The protocol that I have encountered most often through different trainers includes:
• Medial Gastrocnemious Veins (Duel screen - non compressed and compressed)
• Lateral Gastrocnemious Veins (Duel screen - non compressed and compressed)
• Short Saphenous Vein (Duel screen - non compressed and compressed)
• Long Saphenous Vein (Duel screen - non compressed and compressed)
• Soleal Veins (Duel screen - non compressed and compressed)

Calf Veins Continued • Either:
Posterior Tibial Veins (Duel screen - non compressed and compressed) Peroneal Veins (Duel screen - non compressed and compressed)
• OR Posterior Tibial Veins and Peroneal Veins (Duel screen - non compressed and compressed, Prox,
Mid And Dist)
• In addition, some radiologists also like a transverse colour Doppler image of Peroneal and Posterior Tibial Veins with augmentation to demonstrate colour filling

Medial Gastrocnemious Veins
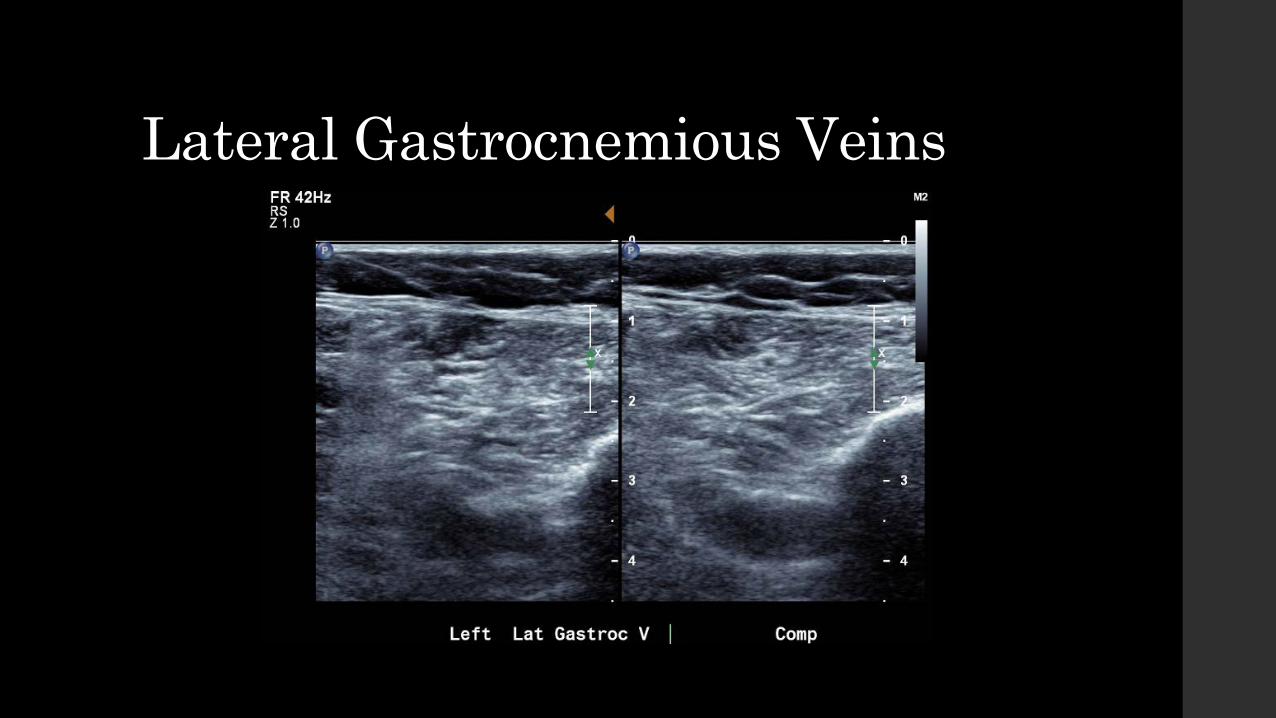
Lateral Gastrocnemious Veins
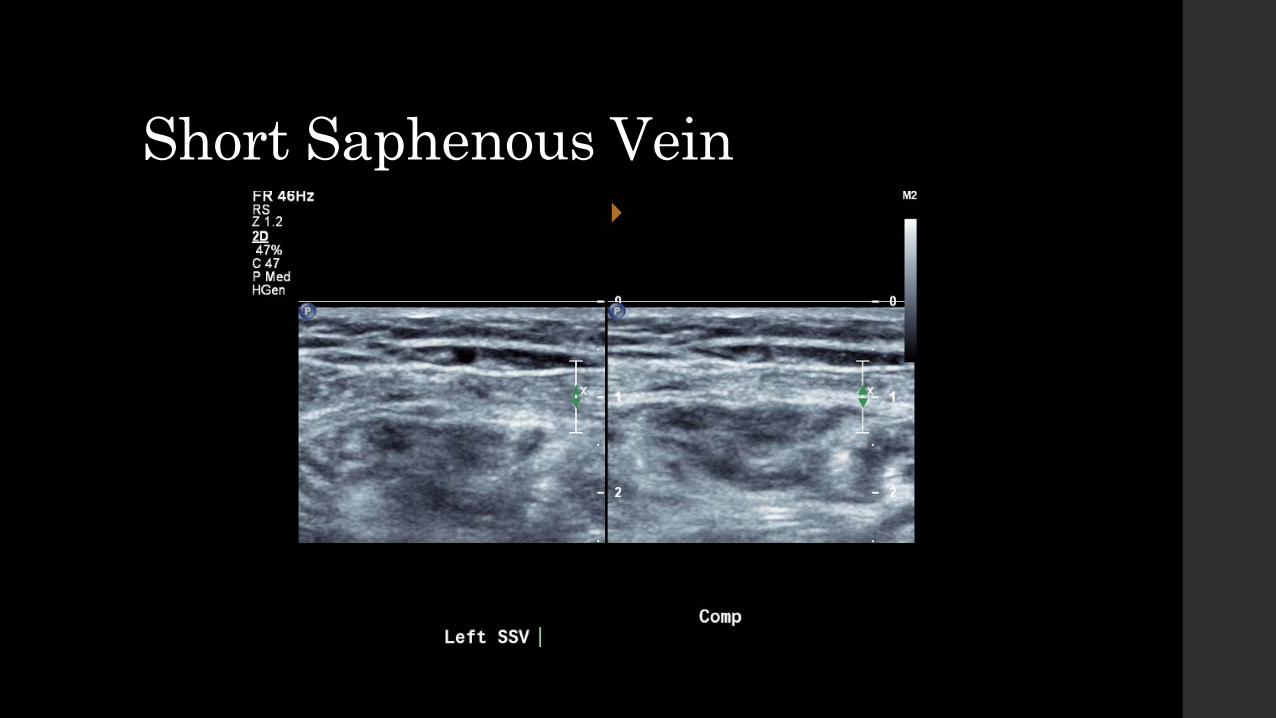
Short Saphenous Vein
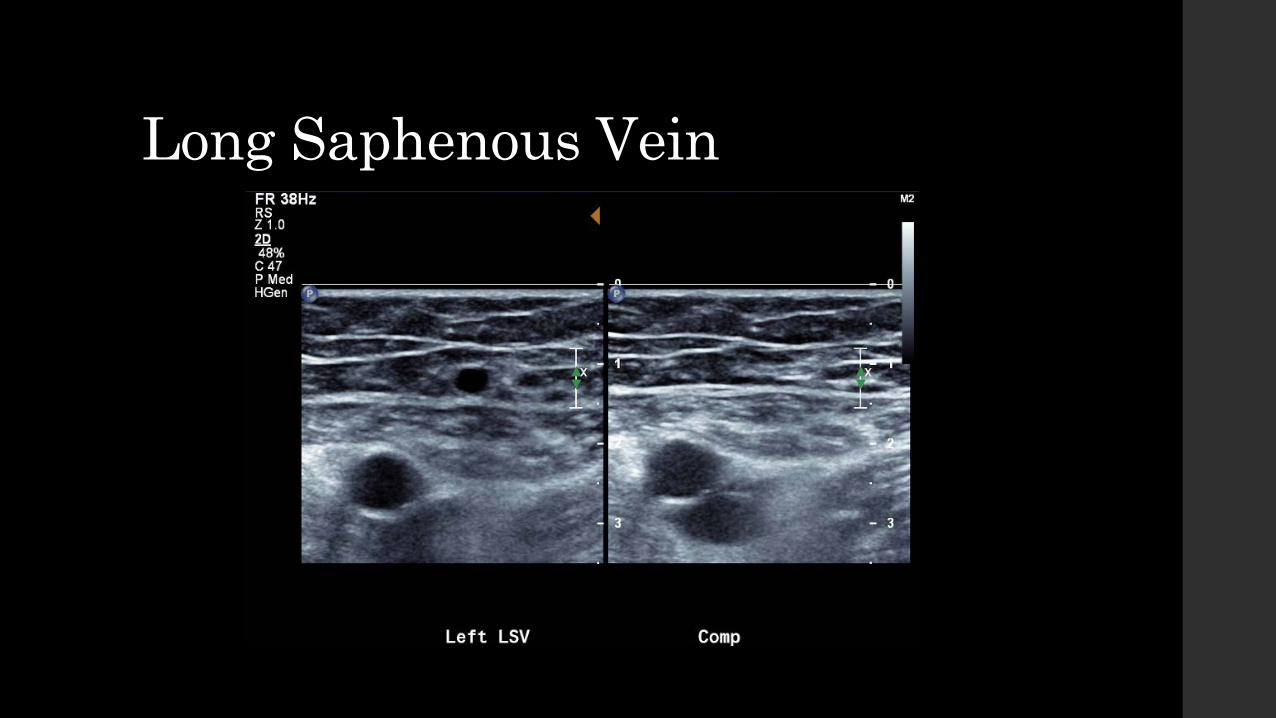
Long Saphenous Vein

Soleal Veins

Posterior Tibial Veins and Peroneal Veins

Posterior Tibial Veins and Peroneal Veins
Examination Extension • If abnormal flow is indicated at the common femoral vein distally, then the
examination is extended superiorly into the abdomen to determine if there is a more proximal stenosis
• The region of interest should be examined. If the patient presents with leg swelling and extensive oedema is seen this should be
imaged If the patient has a tender area for investigation this should be imaged. If there is thrombophlebitis in the patients ROI then this should be documented as well
are the vein that it drains to and apparent proximity to veins
• If the patient has popliteal fossa pain (in the absence of a DVT) the fossa and calf should be examined for the presence of a Baker’s cyst.
• If a duplication of vessels is noted i.e. two femoral veins, then both should be examined and the duplication drawn on to diagram.
• Some examples of examination extension are given in the following slides.
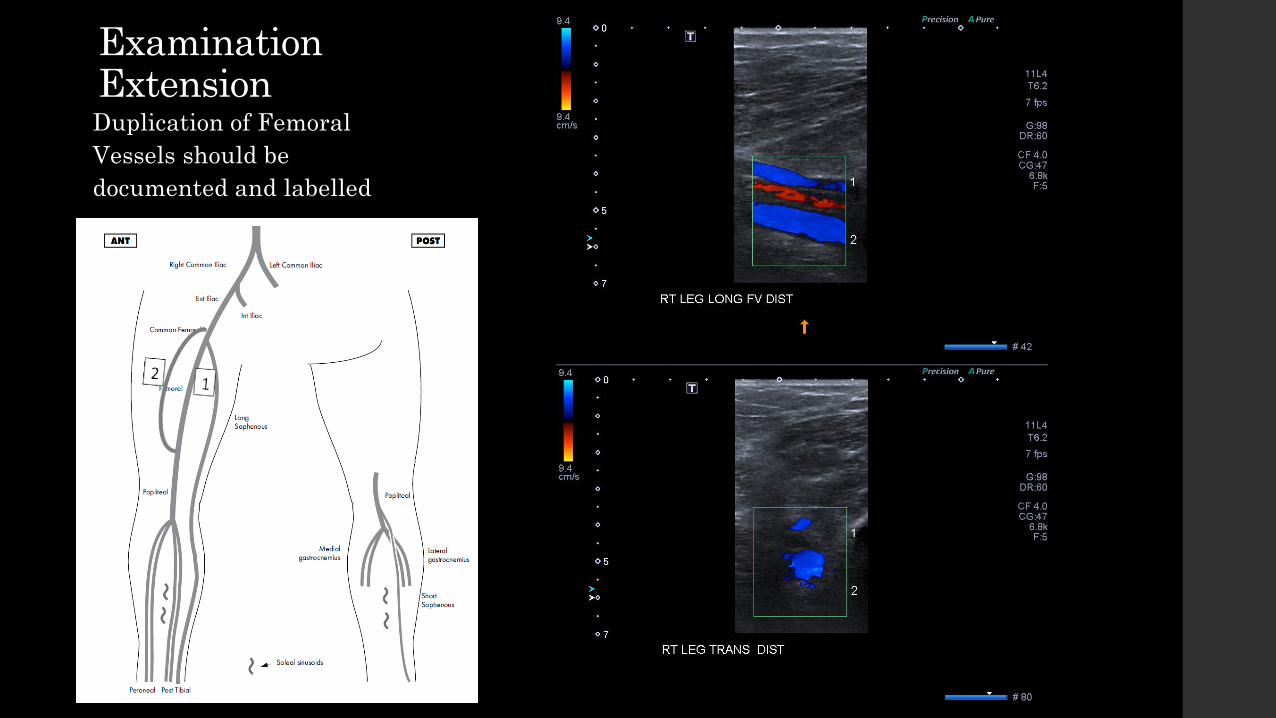
Examination Extension Duplication of Femoral Vessels should be documented and labelled

Examination Extension Thrombophlebitis should also be document, especially if it related to the ROI.

Upper Limb DVT

Worksheet for Examination • As with the lower limb study a
worksheet should be completed for every upper limb venous study.
• Adjacent is the worksheet used by our practice.
Anatomy of the Upper Limb Deep Venous System • A DVT study of the Upper Limb will examine:
Jugular Vein from the mastoid to the base of the neck Subclavian Vein Axillary Vein Brachial Vein Basilic Vein Cephalic Vein Radial and Ulnar Veins

Anatomy of the Upper Limb Deep Venous System

Patient and Room Preparation

Patient and Room Preparation • Preparation for an upper limb venous study is very similar to a lower limb
study in terms of: Revision of previous studies Greeting Obtaining patient identification, history and consent Basic room preparation
• Differences can be noted in: Changing the patient appropriate patient positioning
Patient and Room Preparation • In my practice how the patient is
changed is largely based on patient gender.
• Male patients are asked if they would be happy to simply remove their shirts or if they would like to be provided a gown.
• Female patients are asked to remove the clothing from their waist up (including their bra or at least slipping their arm out of the strap) and place on an appropriate gown as displayed.

Patient and Room Preparation • During my training I have been shown a variations for patient position.
• The common factors that are seen: Arm below the head level to allow for increased circulatory pressure Patient comfort Sonographer ergonomics
• Variation of position are demonstrated in following slides.

Patient and Room Preparation Patient with head at “head end” of the bed.
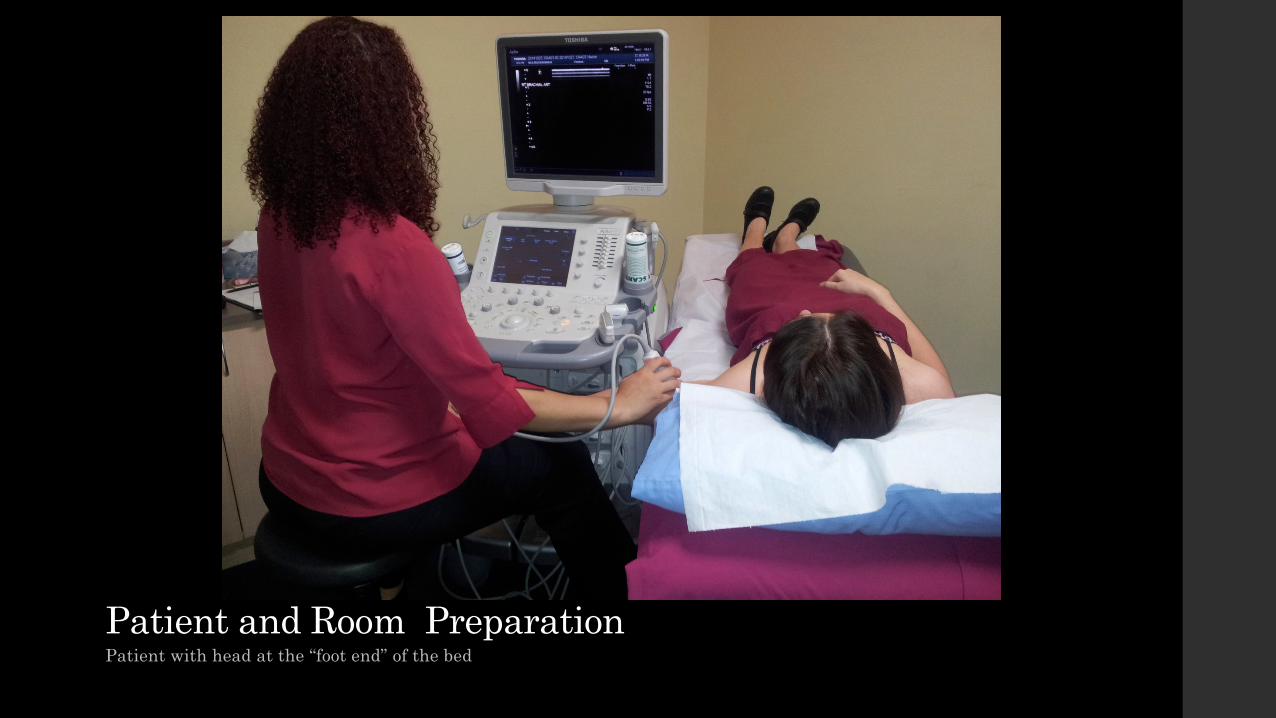
Patient and Room Preparation Patient with head at the “foot end” of the bed

Patient and Room Preparation Patient seated

Upper Limb DVT Study Protocol • Jugular Vein Transverse (Duel screen - non compressed and compressed)
• Jugular Vein Long with Colour and Spectral Trace
• External Jugular Vein and Subclavian Junction in Colour
• Subclavian Vein Long B-mode Colour flow with spectral trace
Prox Mid Distal
• Axillary Vein Transverse (Duel screen - non compressed and compressed)
• Axillary Vein Long with Colour and Spectral trace proximally and distally

Upper Limb DVT Study Protocol • Basilic Vein, Brachial Veins, Cephalic Vein, Radial Veins, Ulnar Veins
Transverse (Duel screen - non compressed and compressed) Longitudinal Colour and Spectral Trace - Prox, Mid, Distal if possible
Augmentation can be used if needed but should be documented

1. Jugular Vein

2. Jugular Vein
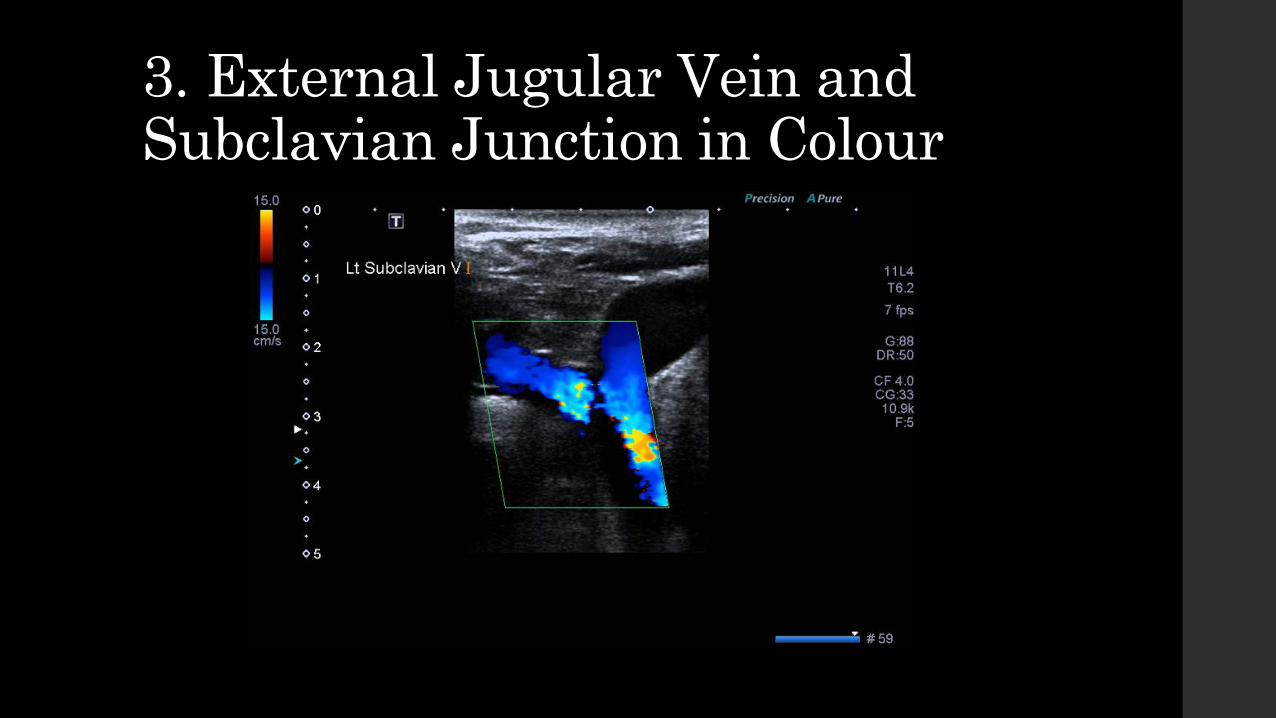
3. External Jugular Vein and Subclavian Junction in Colour
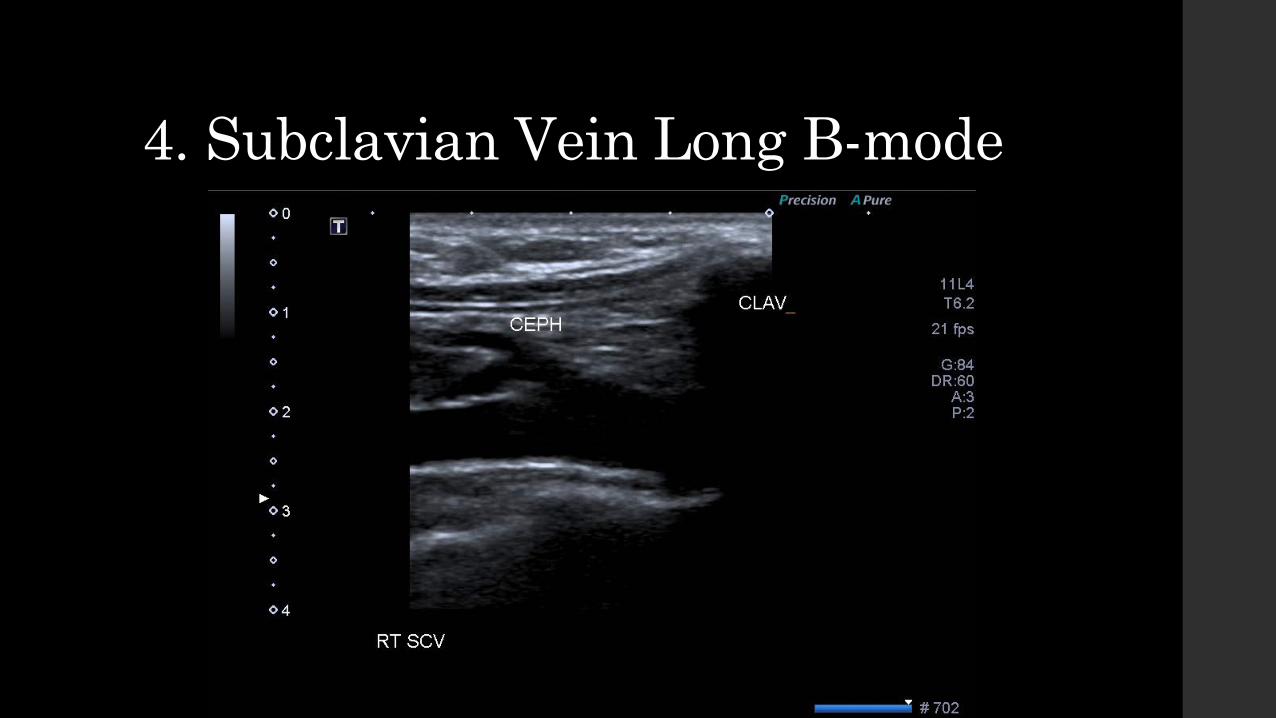
4. Subclavian Vein Long B-mode

5. Subclavian Vein Proximal

6. Subclavian Vein Mid

7. Subclavian Vein Distal

8. Axillary Vein

9. Axillary Vein Spectral Trace

10. Basilic Vein Transverse Longitudinal

11. Brachial Vein Transverse Longitudinal

12. Cephalic Vein Transverse Longitudinal

13. Radial Vein Transverse Longitudinal

14. Ulnar Vein Transverse Longitudinal
Examination Extension • Extension of the examination of the upper limb is similar to that of the lower
limb.
• Region of interest, anatomical variants and other incidental pathologies should be examined and documented accordingly.

Deep Vein Thrombosis
2014
AETIOLOGY, FORMATION, PROGRESSION, ULTRASOUND DIAGNOSIS AND TREATMENT OF DEEP VEIN THROMBOSIS PAIGE FABRE 13654584

Deep Vein Thrombosis
Introduction
Deep Vein Thrombosis (DVT) is a serious and potentially life threatening pathology. If left untreated, DVT can lead to pulmonary embolism and/or post-thrombic syndrome (Dumantepe, Tarhan and Ozler 2013, 366)(Beyer and Schellong 2005)(Cronan 2011, 421). Over the last few years Doppler ultrasound examinations have taken over from traditional venograms as the preferred method for detecting thrombus in the deep vein system (Cronan 2011, 241). Ultrasound is low in cost, easily accessible, relatively well tolerated by the patient with high specificity making it ideal for DVT diagnosis.
As medical imaging professionals it is important that we learn and attempt to understand the signs, symptoms and preferred imaging pathway for such a prevalent pathology. This report therefore aims to describe the aetiology, formation and progression of thrombosis in the venous system as well as how diagnosis is made with dedicated ultrasound studies and the treatment that follows.
Definition
Ahuja defines deep vein thrombosis as “a condition by which blood changes from liquid to solid state and produces a blood clot within the deep venous system”(2007, 36). Alternatively Kumar, Abbas and Fausto define thrombosis as the formation of a blood clot within intact vessels (2012, 80).

Clinical Presentation
Comerota suggests that clinical presentation will be the dependant on the anatomy involved, the extent of thrombus and the degree of occlusion (2013, 1).
Common presenting symptoms include:
• Swelling of the limb (Beyer and Schellong 2005, 239) (Cronan 2011, 421) (Ahuja 2007, 14:38) • Pain and tenderness and the site of probable thrombosis (Beyer and Schellong 2005, 239)
(Cronan 2011, 421) (Ahuja 2007, 14:38) • Oedema (Beyer and Schellong) (Cronan 2011, 421)
Many studies into the effectiveness of diagnosis by clinical examination have found that these symptoms can be very vague leading to false positive diagnosis. Beyer and Schellong suggest that up to 30% of cases with DVT do not exhibit these common symptoms (2005, 239) while Thrush and Hartshorne propose up to a 50% inaccuracy in detecting DVT based only on clinical symptoms (2005, 190).
Groups at Risk
In the clinical setting, those patients at higher risk for developing DVT should be identified to assist with clinical diagnosis.
Risk factors for DVT include:
• History of DVT (Comerota 2013, 19) (Cronan 2011, 422) (Ahuja 2007,14:38) • Increasing age (Comerota 2013, 9) • Vessel trauma through medical intervention especially in areas of central venous
catheterisation (Ahuja 2007, 14:36) (Comerota 2013, 9) (Cronan 2011, 421) • Areas of blood stasis (Comerota 2013, 9) • Obesity (Comerota 2013, 19) (Ahuja 2007,14:38) • Sedentary lifestyle factors –post operative, illness (Cronan 2011, 421) • Malignancy (Cronan 2011, 421) (Thrush and Hartshorne 2005, 190) • Child birth, pregnancy and the oral contraceptive pill (Cronan 2011, 421) (Ahuja 2007,14:38)

Aetiology
In the normal venous system respiration, muscle contractions and venous valve actions propel the blood back towards to the heart (Henningson 2004, 510). When this sequence is interrupted DVT formation may occur.
Sources suggest that DVT most commonly results from impaired venous return (venous stasis), endothelial injury or dysfunction, and states of hypercoagulability (Douketis 2014) (Henningson 2004, 510) (Kumar, Abbas and Fausto 2012, 88). These factors may be better known as Virchow’s Triad and are more likely to occur in concurrence with each other. (Henningson 2004, 510) (Kumar, Abbas and Fausto 2012, 88). In all three situations, prolonged contact between platelets and clotting agents along the vein wall will lead to the creation of thrombus (Comerota 2013, 9).
In the both the venous and arterial systems, thrombus will propagate back towards the heart (Kumar et al. 2012, 88). In the venous system this means that the thrombus will form in the direction of blood flow making it prone to dislodgement giving rise to emboli (Kumar, Abbas and Fausto 2012, 88).
Venous stasis
In the lower limb, soleal sinusoids may be considered the leading site for thrombosis due to it being an area of frequent stasis (Comerota 2013, 9). The abductor canal may also be a site of stasis due to the curved shape of the popliteal vein and femoral vein as they pass through this region.
Venous stasis may be considered the most like cause of DVT (Kumar, Abbas and Fausto 2012, 88).
Endothelial Damage and Dysfunction
In the setting of damage or dysfunction of the endothelium an increase in procoagulant factors and a decrease in anticoagulant factors will occur (Kumar, Abbas and Fausto 2012, 86). This arrangement will cause thrombus formation within the vessel.
Hypercoagulability
Hypercoagulability is often the result of a genetic variation or mutation of specific coagulation factor genes (Smallberg et al. 2011, 486). Smallberg et al. suggests that those related to DVT include antithrombin, protein C and protein S deficiencies (2011, 486). When the body is in a state of hypercoagulability the prevalence for clot formation is exacerbated and thus DVT formation occurs.
Ultrasound Diagnosis
The aim of a venous Doppler ultrasound is to determine the patency of the system and exclude or diagnose deep vein thrombosis and other incidental pathology. It utilises the compressibility of the normal venous system to allow the user to determine if there is a thrombus within the target vessels. Colour Doppler and Spectral Doppler are also used to further to add to the diagnosis. Colour Doppler can be used to better visualise hypoechoic or anechoic acute thrombus by detecting a lack of colour filling. Spectral traces can add information about possible thrombus proximal to the site of interrogation using Valsalva, or inferior to the site of interrogation using augmentation. In addition, spectral traces can also be used to detect valve incompetence in the deep system.
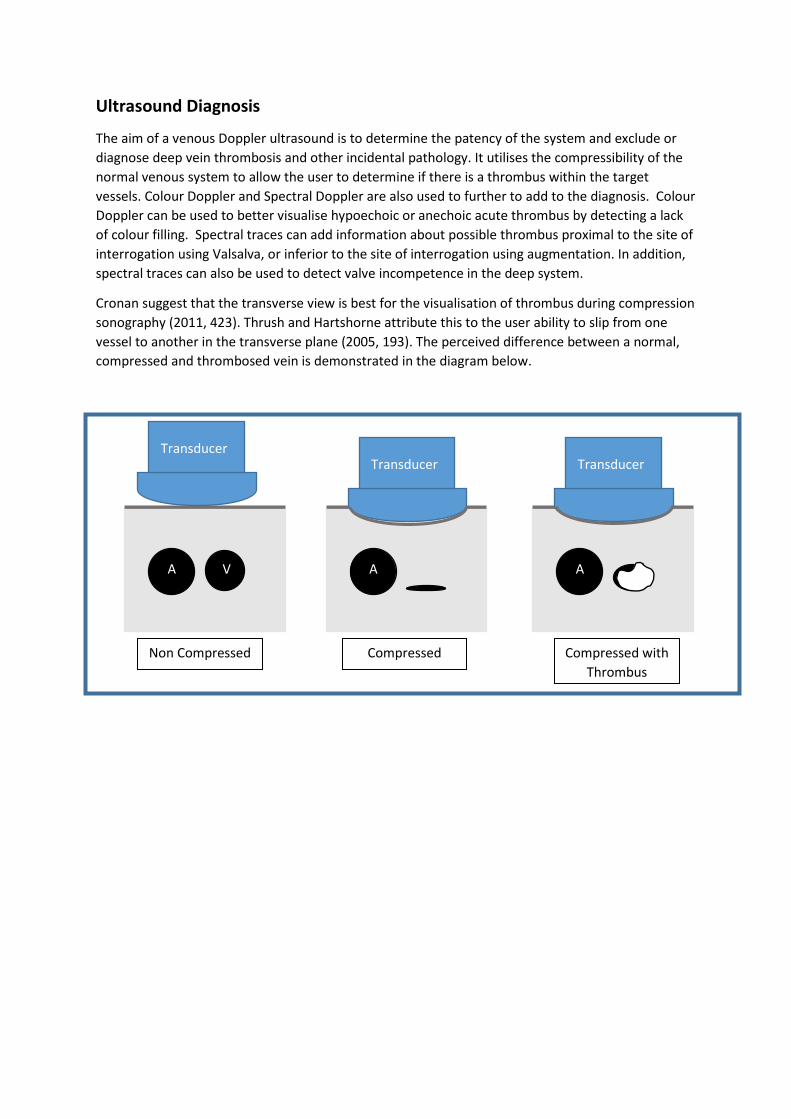
Cronan suggest that the transverse view is best for the visualisation of thrombus during compression sonography (2011, 423). Thrush and Hartshorne attribute this to the user ability to slip from one vessel to another in the transverse plane (2005, 193). The perceived difference between a normal, compressed and thrombosed vein is demonstrated in the diagram below.
A V A A
Non Compressed Compressed Compressed with Thrombus
Transducer Transducer Transducer
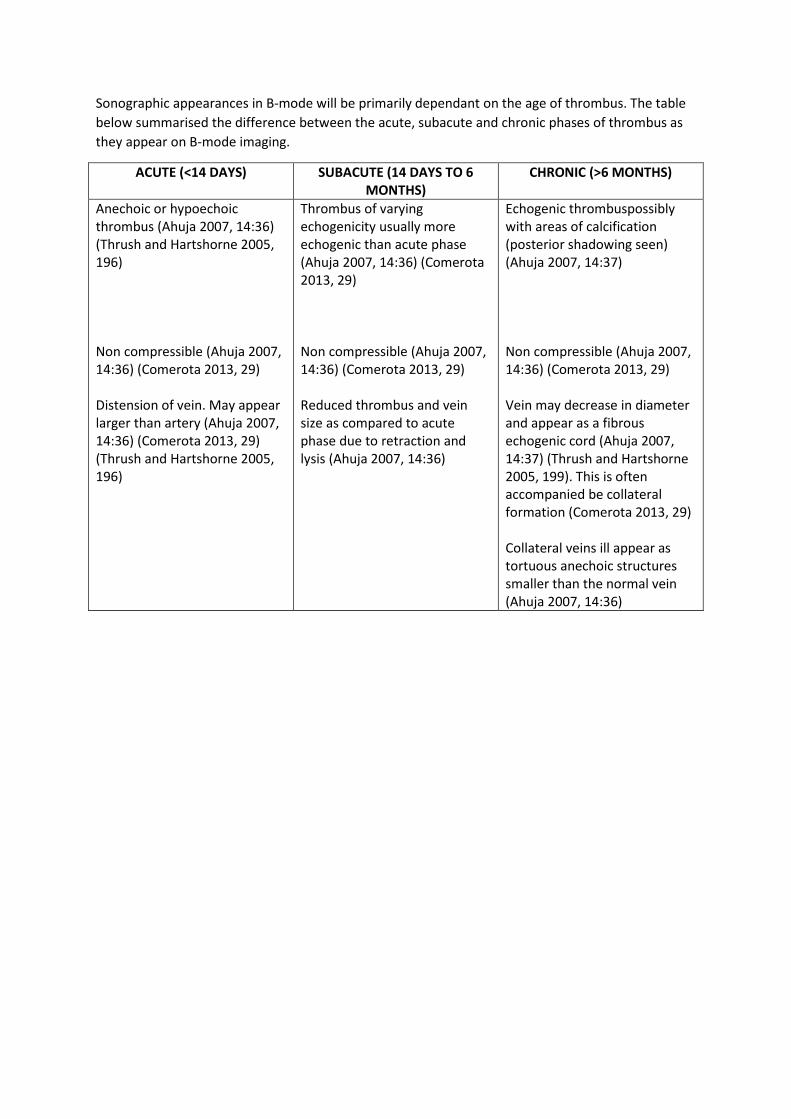
Sonographic appearances in B-mode will be primarily dependant on the age of thrombus. The table below summarised the difference between the acute, subacute and chronic phases of thrombus as they appear on B-mode imaging.
ACUTE (<14 DAYS) SUBACUTE (14 DAYS TO 6 MONTHS)
CHRONIC (>6 MONTHS)
Anechoic or hypoechoic thrombus (Ahuja 2007, 14:36) (Thrush and Hartshorne 2005, 196) Non compressible (Ahuja 2007, 14:36) (Comerota 2013, 29) Distension of vein. May appear larger than artery (Ahuja 2007, 14:36) (Comerota 2013, 29) (Thrush and Hartshorne 2005, 196)
Thrombus of varying echogenicity usually more echogenic than acute phase (Ahuja 2007, 14:36) (Comerota 2013, 29) Non compressible (Ahuja 2007, 14:36) (Comerota 2013, 29) Reduced thrombus and vein size as compared to acute phase due to retraction and lysis (Ahuja 2007, 14:36)
Echogenic thrombuspossibly with areas of calcification (posterior shadowing seen) (Ahuja 2007, 14:37) Non compressible (Ahuja 2007, 14:36) (Comerota 2013, 29) Vein may decrease in diameter and appear as a fibrous echogenic cord (Ahuja 2007, 14:37) (Thrush and Hartshorne 2005, 199). This is often accompanied be collateral formation (Comerota 2013, 29) Collateral veins ill appear as tortuous anechoic structures smaller than the normal vein (Ahuja 2007, 14:36)

Acute (Ahuja 2007 14:39)
Sub - Acute
Chronic
It is important to also be aware of free floating thrombus at any stage. A free floating thrombus may be seen as an intraluminal echogenicity that is not adherent to the vessel wall (Thrush and Hartshorne 2005, 196).
Doppler
Pulsed Doppler changes will be dependent of the degree of occlusion of the vessel. Common changes seen include:
• Decreased phasicity (Comerota 2013, 29) (Ahuja 2007, 14:37) • Loss of spontaneous venous signal (Comerota 2013, 29) (Ahuja 2007, 14:37) • Abnormal augmentation (Comerota 2013, 29) (Ahuja 2007, 14:37) • Elevated flow velocity (Comerota 2013, 29)
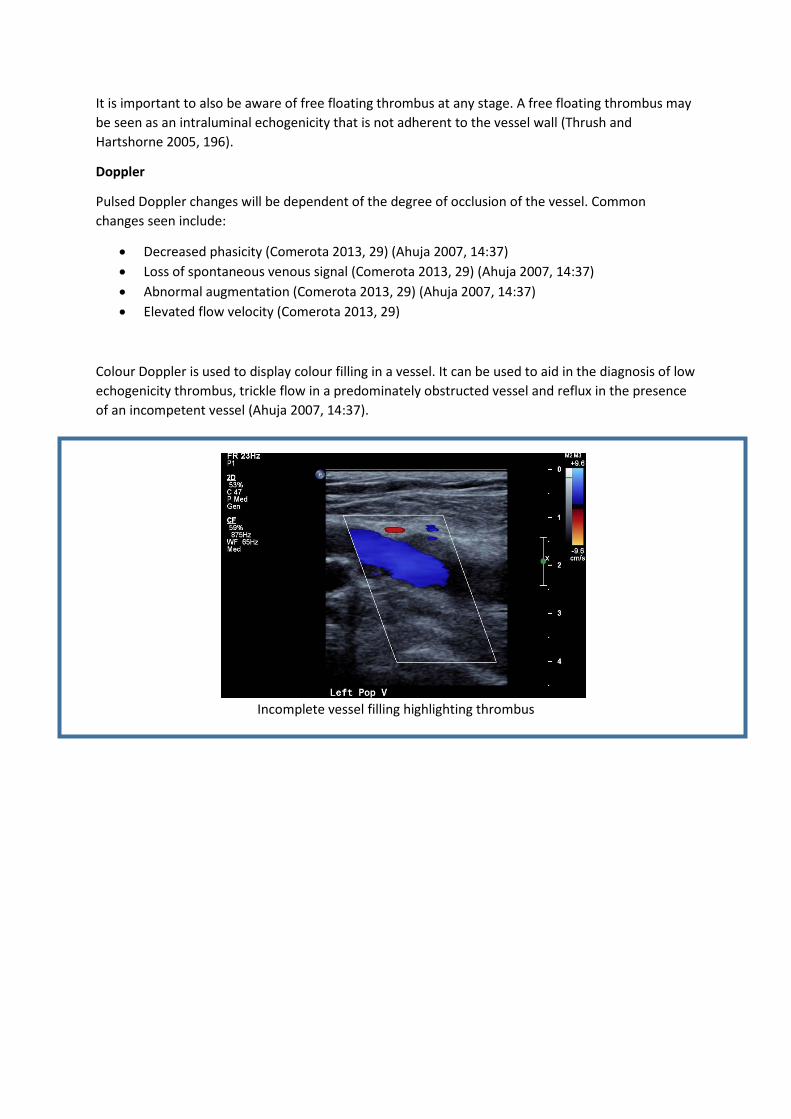
Colour Doppler is used to display colour filling in a vessel. It can be used to aid in the diagnosis of low echogenicity thrombus, trickle flow in a predominately obstructed vessel and reflux in the presence of an incompetent vessel (Ahuja 2007, 14:37).
Incomplete vessel filling highlighting thrombus

Alternative Modalities
Venography
CT and MRI venography has taken the place of traditional venography for detecting DVT. Traditional venography would involve an injection of contrast media into the pedal veins followed by user observation of vein filling (Beyer and Schellong 2005, 243). This method however has a false negative rate of approximately 11% (Ahuja 2007, 14:37). This and other factors including radiation exposure, contrast media contraindications and the painful nature of the injection make traditional venography a less preferred imaging option.
Beyer and Schellong suggest that CT venography has a specificity and sensitivity similar to that of traditional venography (2005, 243). Though overall radiation dose and cost may be higher than with traditional venography, the ability to simultaneously detect pulmonary emboli and iliac vein thrombus make CT venography an acceptable choice where there is a high suspicion of DVT (Thrush and Hartshorne 2005, 192).
Studies into the use of MRI venography have suggested effectiveness with both contrast and non-contrast studies providing another option for those who for which contrast studies are contraindicated (Beyer and Schellong 2005, 243). This combined with the lack of ionising radiation, improved visualisation of iliac vein thrombus make MRI venography an acceptable option for DVT detection. Disadvantages of MRI venography however including high cost and limited availability prevent it from being used as a routine screening tool (Beyer and Schellong 2005, 243) (Thrush and Hartshorne 2005, 192).
Positive D Dimer D-dimer tests have been used for many years to aid with diagnosis of DVT. The simple blood test offers an affirmation of thrombolytic events in the body by testing for an increase in D-dimer in the circulatory system (Beyer and Schellong 2005, 240). Though sensitive, the test itself has a low specificity as acute inflammation may also cause an increase D-Dimer tests (Thrush and Hartshorne 2005, 192). Cronan suggests that the type of test only be used in cases with a low to moderate probability of DVT with positive results warranting venous Doppler ultrasound (2011, 421).

Pre-test scores Pre-tests scores are often referred to in clinical literature as a way to assess the likelihood of DVT in a patient prior to diagnostic imaging. Referred to as “Wells Scores” the image below demonstrates the chart used to identify a patient’s likelihood of DVT. In the clinical setting, the higher the score above 2 the higher the probability of DVT.
A table of Wells score (Cronan 2011, 422)
Treatment
The traditional treatment option for patient with DVT is anticoagulant (Dumantepe, Tarhan and Pzler 2013, 366)(Cronan 2011, 422). Cronan suggests that this treatment option is not without risks, the most concerning of which is significant bleeding complications 2011, 422). Often anticoagulation therapy consists of heparin anticoagulation followed with oral warfarin once a patient’s INR (international normalisation ratio) is within acceptable limits (Ahuja 2007, 14:38).
Surgical intervention may be considered in particular cases. In patients with a high risk of recurrent DVT and PE, and those for whom anticoagulant therapy may be contraindicated, an IVC filter may be considered (Ahuja 2007, 14:38). Other types of surgical intervention include valve repair and transplantation, perforator interruption and venous bypass (Ahuja 2007, 14:37).
Although ultrasound is the preferred method of investigation for DVT, research has been conducted into its use in therapies to resolve thrombus. Ultrasound-accelerated catheter directed thrombolysis (UACDT) is a method by which the thrombus is completely lysed decreasing the risk of post-thrombotic syndrome (Dumantepe, Tarhan and Ozler 2013, 366). Though current research is promising, further long studies may be needed to further confirm its usefulness in the long term.
Conclusion
Requests for venous studies to detect Deep Vein Thrombosis are common in the current clinical setting. Though easily detected on ultrasound, DVT can be potentially life threatening with the possibility of embolus formation. It is important to understand the factors that place a patient at higher risk of DVT including decreased mobility, vessel trauma and hypercoagulability and by understanding that areas of blood stasis are at higher risk of thrombus development we may take extra care to interrogate these patient and these areas. Acknowledging the differences between the sonographic appearance of thrombus at the acute, subacute and chronic stages will assist with diagnosis and aid in the appropriate selection of treatment. Knowledge of the aetiology and formation of thrombosis, diagnosis by ultrasound and treatment that occurs with Deep Vein Thrombosis we as medical imaging professionals are able to provide a higher level of imaging service to our patients.

References
Ahuja, Anil. 2007. Diagnostic Imaging Ultrasound. Canada: Amirsys.
Beyer, Jan, and Sebastian Schellong. 2005. “Deep vein thrombosis: Current diagnostic strategy”. European Journal of Internal Medicine 16(4): 238-246. doi: 10.1016/j.ejim.2005.04.001
Comerota, Anthony. 2013. Practical Phlebology: Deep Vein Thrombosis. Hoboken, New Jersey: Taylor and Francis.
Cronan, John. 2011. “Deep vein thrombosis: Imaging diagnosis and related controversies”. Ultrasound Clinics 6 (4): 421 – 433. doi: 10.1016/j.cult.2011.07.002.
Douketis, James. 2014. “Deep Venous Thrombosis (DVT)”. Merck Manuals Professional Edition. Accessed October 26, http://www.merckmanuals.com/professional/cardiovascular_disorders/peripheral_venous_disorders/deep_venous_thrombosis_dvt.html
Dumantepe, M, I.A. Tarhan, and A. Ozler. 2013. “Treatment of Chronic Deep Vein Thrombosis Using Ultrasound Accelerated Catheter-directed Thrombolysis”. European Journal of Vascular and Endovascular Surgery 46(3): 366-371. doi: 10.1016/j.ejvs.2013.05.019.
Henningson, Charlotte. 2004. Clinical Guide to Ultrasonography. St. Louis, Missouri: Mosby Elsevier.
Kumar, Vinay, Abul Abbas, and Nelson Fausto. 2012. Robbins Basic Pathology. 9th ed. Elsevier.
Smallberg, Jasper, Marieke J.H.A. Kruip, Harry L.A. Janssen, Dingeman C. Rijke, Frank W.G. Leebeek and Moniek P.M. de Maat. 2011. “Hypercoagulability and Hypofibrinolysis and Risk of Deep Vein Thrombosis and Splanchnic Vein Thrombosis: Similarities and Differences”. Arteriosclerosis, Thrombosis, and Vascular Biology 31 (3):485-493. doi: 10.1161/ATVBAHA.110.213371.
Thrush, Abigail, and Timothy Hartshorne. 2005. Peripheral vascular ultrasound: how, why, and when. 2nd ed. Edinburgh: Churchill Livingston.

















