17
VATS Treatment of Spontaneous Pneumothorax William R. Mayfield, MD, FACS WellStar Thoracic Surgery March 2009
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | collin-wells |
| View: | 222 times |
| Download: | 2 times |

VATS Treatment of Spontaneous Pneumothorax
William R. Mayfield, MD, FACS
WellStar Thoracic SurgeryMarch 2009

• Etiology– Bleb rupture
• Primary • Secondary

Consensus Statement
Management of Spontaneous Pneumothorax
An American College of Chest Physicians Delphi Consensus Statement
MICHAEL H. BAUMANN, MD, FCCP, et al
FOR THE ACCP PNEUMOTHORAX CONSENSUS GROUP†
CHEST FEBRUARY 2001 VOL. 119 NO. 2 590-602

Primary Spontaneous Pneumothorax• Clinically Stable
• Small Pneumothorax– Observe in ER for 3-6 hrs– Repeat CXR– If no progression: discharge home– If distant from ER, or compliance unreliable,
then admit

Primary Spontaneous Pneumothorax• Clinically stable
• Large pneumothorax– Small bore catheter, 14 fr to 22 fr– Water seal– Suction if no re-expansion– Remove chest tube when no air leak– Discharge with one-way valve if unwilling to
be admitted

Primary Spontaneous Pneumothorax• Unstable• Large pneumothorax
– Chest tube 16 – 22 fr if small leak anticipated– Chest tube 24 – 28 fr if large leak anticipated,
or positive pressure ventilation anticipated– Water seal– Suction if lung fails to expand– Remove tube when no leak and lung
expanded

Persistent Air Leak
• Greater than 4 days
• Thoracoscopy – Closure of leak– Pleurodesis
• Bedside pleurodesis– Only if surgery contra-indicated or patient
refuses surgery– Doxycycline or talc slurry

Pneumothorax Recurrence Prevention• First pneumothorax 15% of panel• Second pneumothorax 85% of panel• Decision modified by desire to fly or scuba• Thoracoscopy is treatment of choice
– 95 – 100% success– Bullectomy– Parietal pleural abrasion of upper 50%– Pleurectomy is acceptable– Talc: no consensus
• Bedside pleurodesis for high risk patients– 78 – 91% success

Primary Spontaneous Pneumothorax• CT scanning
– No consensus for first time pneumothorax– No consensus for second time pneumothorax,
persistent air leak, or planned surgery

VATS Bullectomy and Pleurectomy

• Position– Lateral decubitus, flexed
• Incisions– Two incision technique: 3rd and 6th interspace

• Video– 5 mm chip on a stick (Olympus)
• Endo GIA– Green load
• Duet in bullous disease

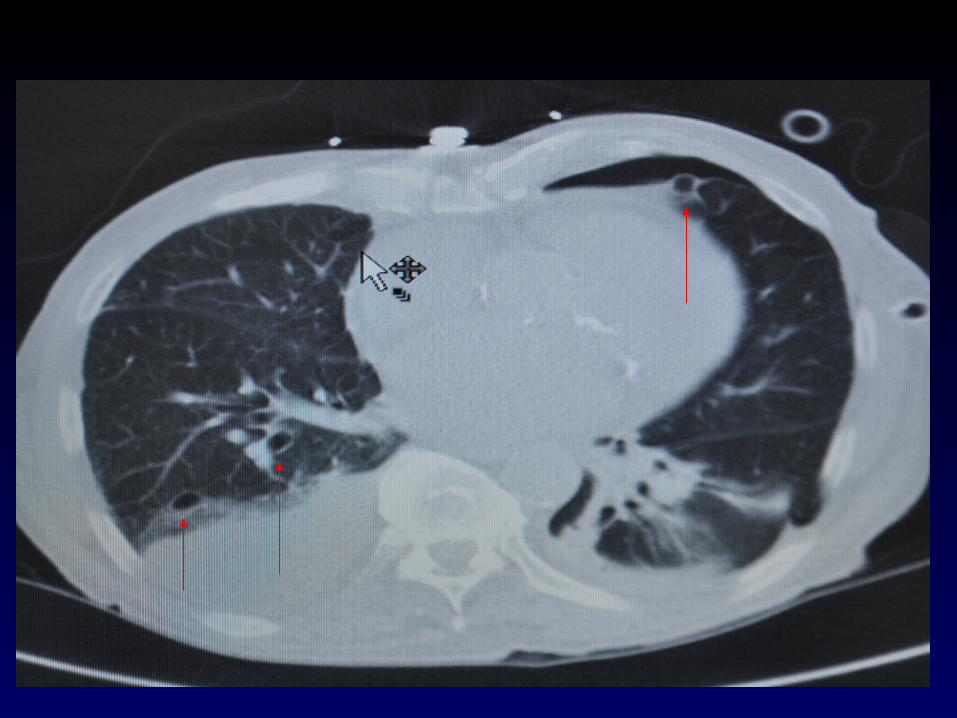
Case Report
• 87 yo male
• Metastatic angio-sarcoma
• Multiple pulmonary blebs after chemotherapy
• Recurrent left pneumothorax
• Failed bedside talc pleurodesis – prior admission


VATS Pleurectomy with talc

Conclusions
• There is consensus on treatment of spontaneous pneumothorax
• It is acceptable to operate on first time pneumothorax
• Thoracoscopy is the preferred method
• Pleurodesis by abrasion, pleurectomy, or (sometimes) talc is acceptable

















