25
Venous Access in Apheresis Daniel Putensen, Apheresis Nurse
Venous Access in Apheresis
Daniel Putensen, Apheresis Nurse

Why is Vascular Access so important?
Henrikson et al. Adverse events in apheresis: An update of the WAA registry data.Transfus Apher Sci. 2016; 54: 2-15

Vascular Access options for Apheresis
PERIPHERAL
Peripheralcannulation
Non-Tunneled
CVC
Tunneled CVC
Portsingle/double
CENTRAL
AV Fistula/Graft
USG-PIVA Via one arm Via artery

Vascular Access devices
4
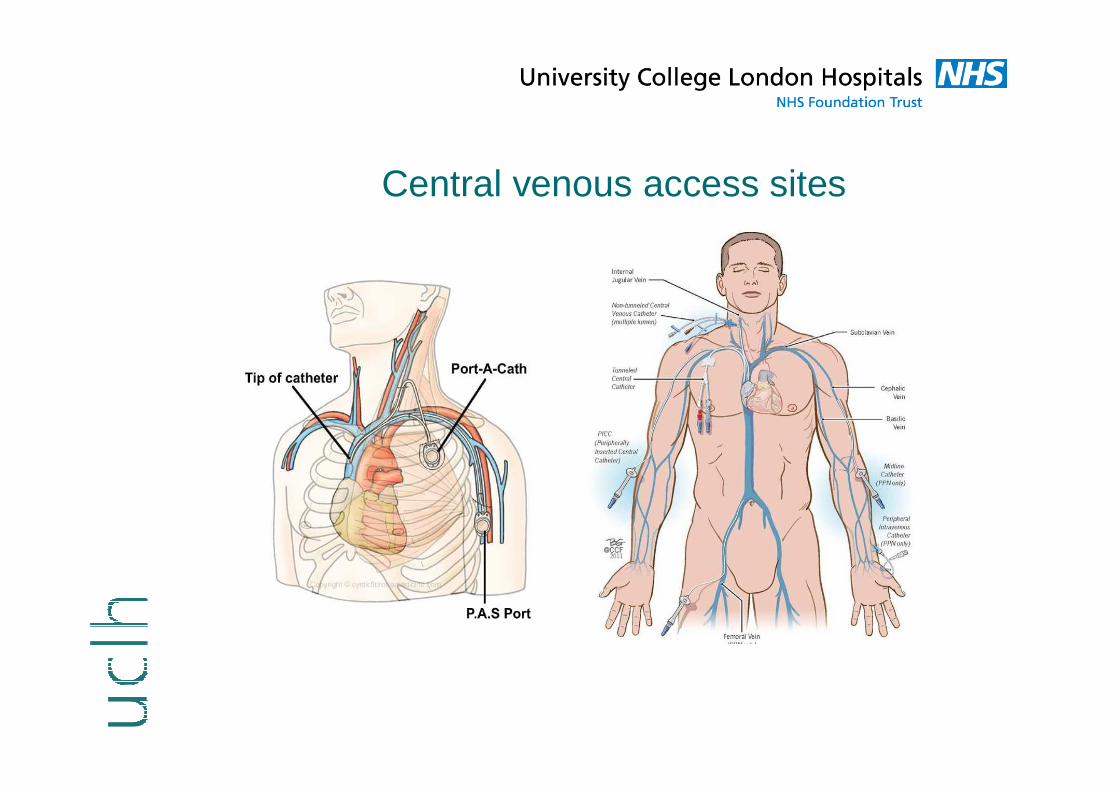
Central venous access sites

CVC position
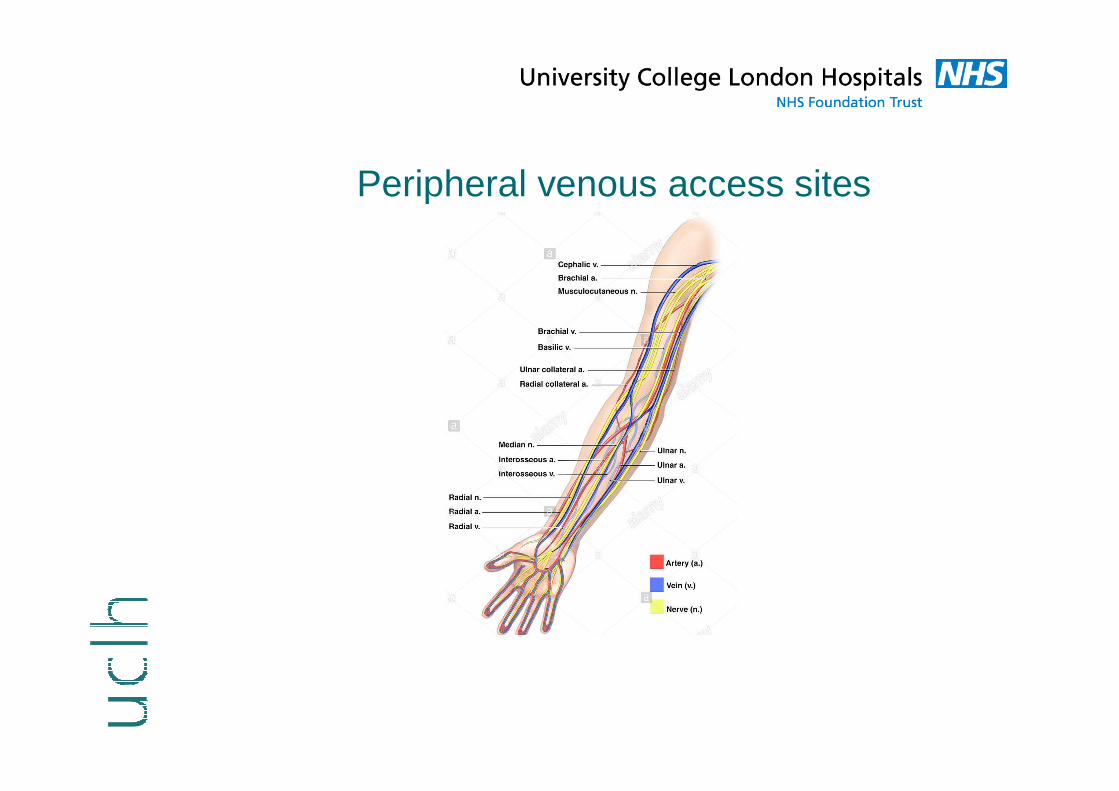
Peripheral venous access sites
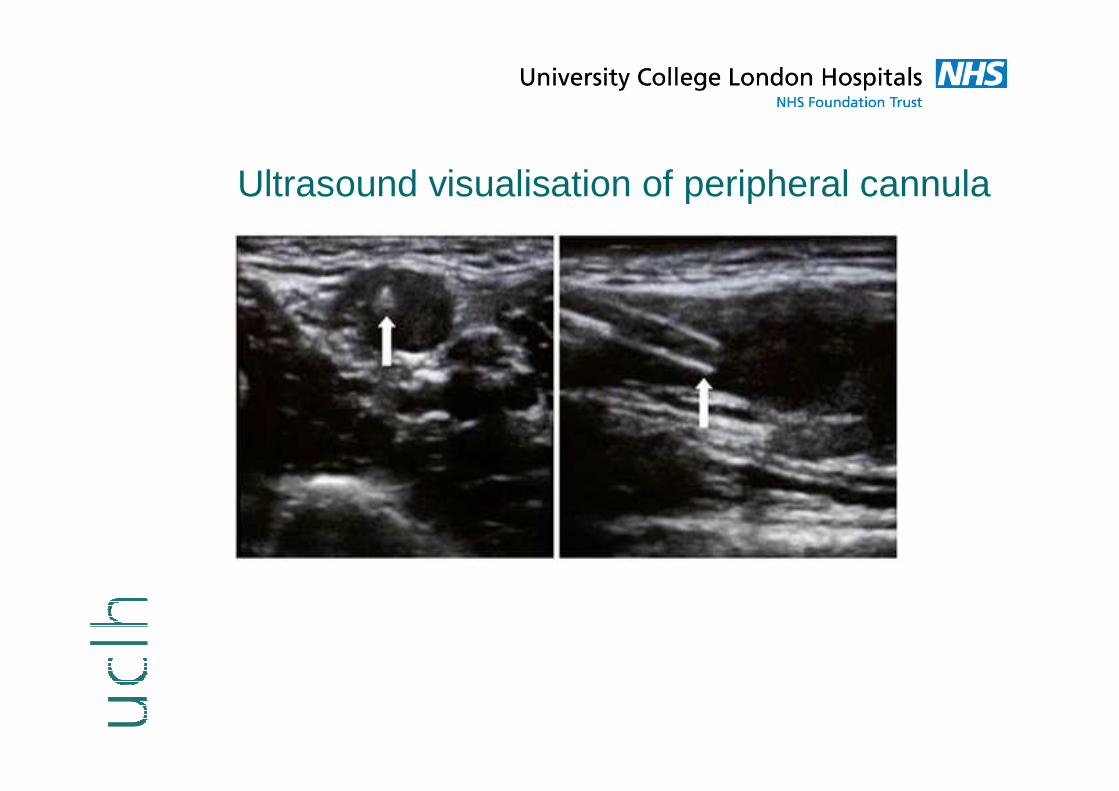
Ultrasound visualisation of peripheral cannula
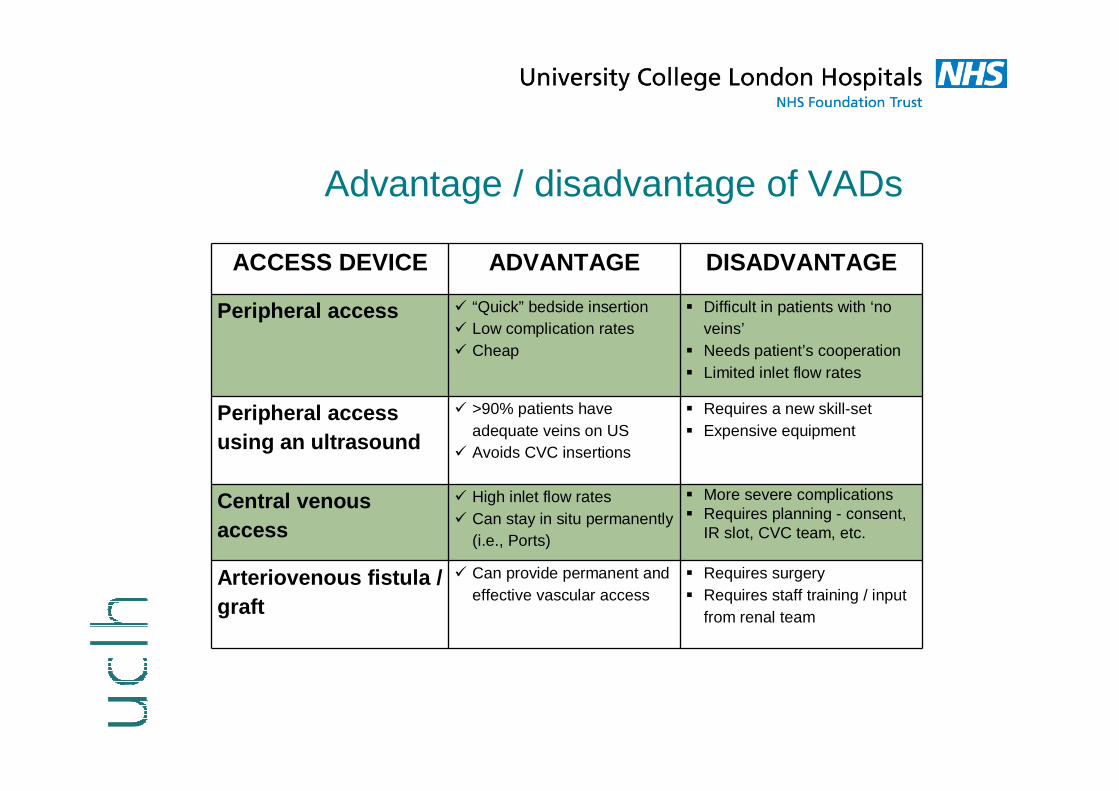
Advantage / disadvantage of VADs
ACCESS DEVICE ADVANTAGE DISADVANTAGE
Peripheral access � “Quick” bedside insertion� Low complication rates� Cheap
� Difficult in patients with ‘no veins’
� Needs patient’s cooperation� Limited inlet flow rates
Peripheral access using an ultrasound
� >90% patients have adequate veins on US
� Avoids CVC insertions
� Requires a new skill-set� Expensive equipment
Central venous access
� High inlet flow rates� Can stay in situ permanently
(i.e., Ports)
� More severe complications � Requires planning - consent,
IR slot, CVC team, etc.
Arteriovenous fistula / graft
� Can provide permanent and effective vascular access
� Requires surgery� Requires staff training / input
from renal team
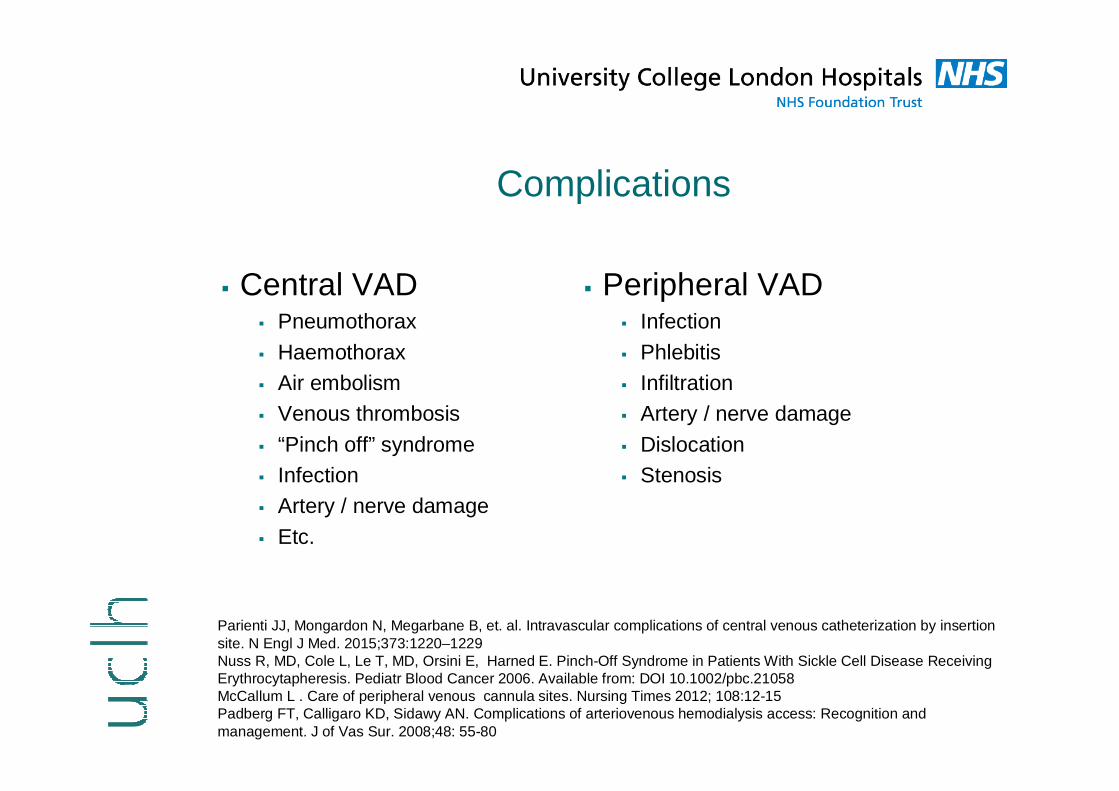
Complications
� Central VAD� Pneumothorax
� Haemothorax� Air embolism� Venous thrombosis
� “Pinch off” syndrome� Infection� Artery / nerve damage
� Etc.
� Peripheral VAD� Infection
� Phlebitis� Infiltration� Artery / nerve damage
� Dislocation� Stenosis
Parienti JJ, Mongardon N, Megarbane B, et. al. Intravascular complications of central venous catheterization by insertion site. N Engl J Med. 2015;373:1220–1229Nuss R, MD, Cole L, Le T, MD, Orsini E, Harned E. Pinch-Off Syndrome in Patients With Sickle Cell Disease Receiving Erythrocytapheresis. Pediatr Blood Cancer 2006. Available from: DOI 10.1002/pbc.21058McCallum L . Care of peripheral venous cannula sites. Nursing Times 2012; 108:12-15Padberg FT, Calligaro KD, Sidawy AN. Complications of arteriovenous hemodialysis access: Recognition and management. J of Vas Sur. 2008;48: 55-80

Factors that determine type of VAD
Vascular Access – Experience from 3 different centres

VADs for RBC exchange at Imperial College(Paediatric patients)
Ong, M. Using peripheral venous access for automate d exchange using Spectra Optia® is safe and feasible for sickle cell disease in the paediatric population. B one Marrow Transplant. 2013; 48:489

USG-PIVA at St. Georges
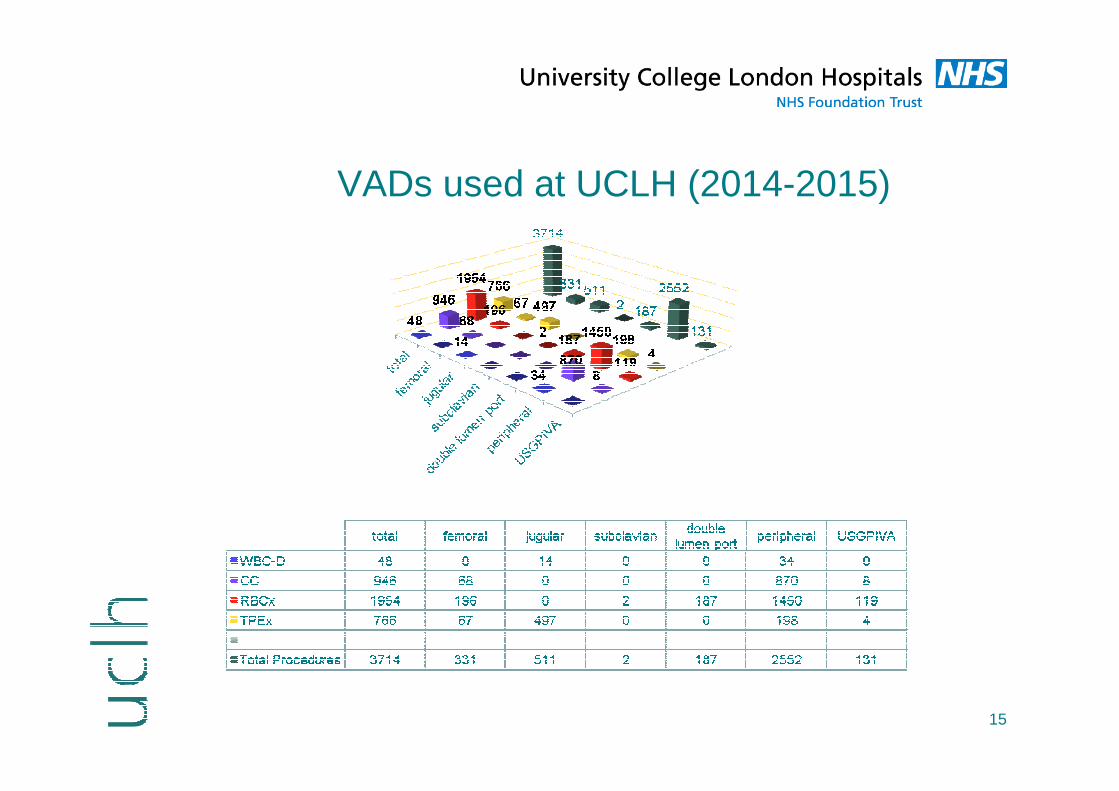
VADs used at UCLH (2014-2015)
15
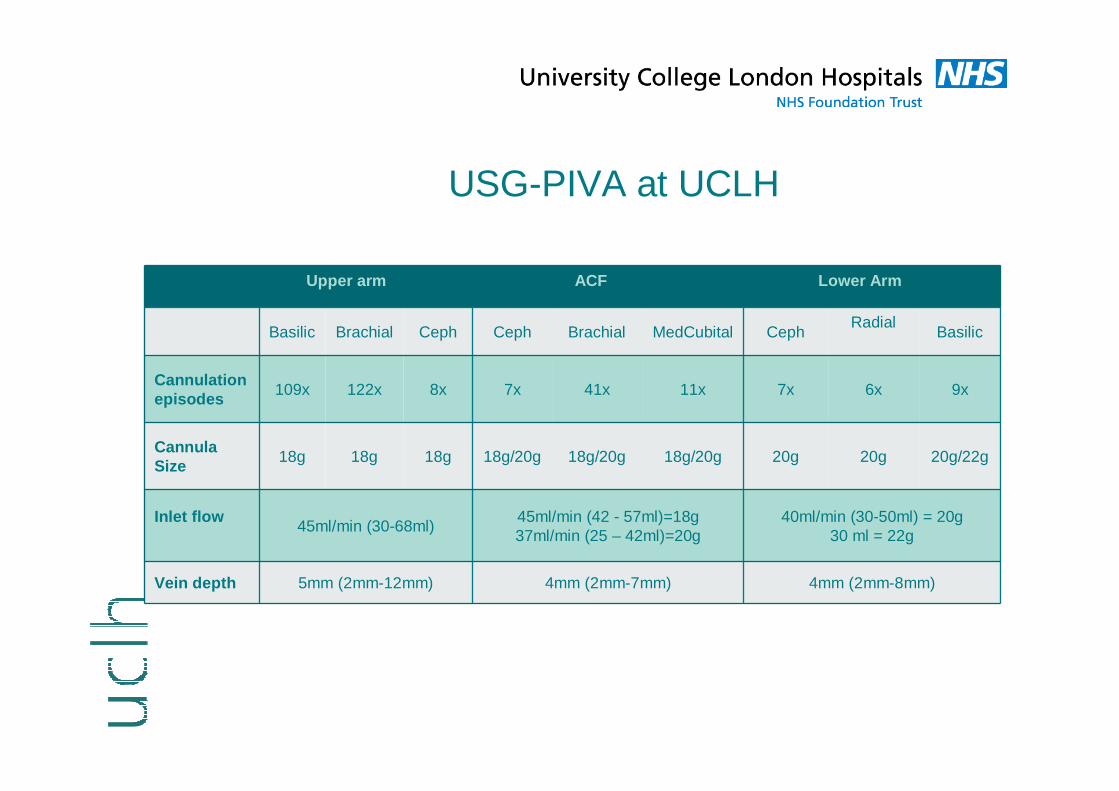
USG-PIVA at UCLH
Upper arm A CF Lower Arm
Basilic Brachial Ceph Ceph Brachial MedCubital CephRadial
Basilic
Cannulation episodes
109x 122x 8x 7x 41x 11x 7x 6x 9x
Cannula Size
18g 18g 18g 18g/20g 18g/20g 18g/20g 20g 20g 20g/22g
Inlet flow45ml/min (30-68ml)
45ml/min (42 - 57ml)=18g37ml/min (25 – 42ml)=20g
40ml/min (30-50ml) = 20g30 ml = 22g
Vein depth 5mm (2mm-12mm) 4mm (2mm-7mm) 4mm (2mm-8mm)

USG-PIVA literature overview
Author (Year) Study type Apheresis procedure
Notes
Keyes (1999) Prospective study n/a A&E setting (101 pts; 91% success rate)
Hanafusa(2015)
Report GMA 4 pts with poor venous access; total of 33 procedures successfully performed
Putensen et al. (2015)
Prospective study RBC exchange 38 pt’s; total of 84 procedures of which 85% (71 US cannulations) were successful, 49 CVC avoided
Salazar et al(2016)
Prospective study TPE, RBC exchange, CC
186 pt’s; total of 831 procedures20% decrease of pt’s needing CVC
Mayhew and Stylianou(2017)
Retrospective study
CC 203 pt’s; total of 383 procedures.Decreases CVC insertion from 33% to 7% over the study period
Gopalasingam et al(2017)
Prospective, descriptive study
TPE, ECP, CC Implementation of USG-PIVA in apheresis unit: decrease of CVC insertion from 45.8% (125 CVCs) to 13.2% (30 CVCs)

Access sites

19

Return line
Access line 17 G Fistula
needle
Fistula



How to increase the number of peripherally placed cannulas?
�Elective Procedure? Make pre-procedure vein assessment mandatory
�Consider required Inlet Flow rates �Cooperation (i.e., patient, parents, play specialist)
�Consider access sites beyond the ACF area
�Consider type of peripheral vascular access device
�Utilise vein-enhancing methods (e.g., warmth, hydration, etc.)
�Use technology (e.g., near infrared light or ultrasound devices)�Etc.

???

References for USG-PIVA
Keyes et al. Utltrasound-Guided Brachial and Basilic Vein Cannulation in Emergency Department Patients With Difficult Intravenous Access. An Emerg Med. 1999; 34, 711-714
Hanafusa N et al. Deep Vein Puncture Under Ultrasonographic Guidance – An Alternative Approach for Vascular Access of Apheresis Theraphies. J Clin Apher [Internet] 2015. Available from: doi: 10.1002/jca.21389
Putensen, D., Pilcher, L., Collier, D., McInerney, K. Ultrasound-guided peripheral deep vein cannulation to perform automated red cell exchange-a pilot study in a single centre. J Clin Apher. 2015;1098–1101. doi:10.1002/jca.21440
Mayhew M, Stylianou J. Ultrasound-guided peripheral vein cannulation reduces the need for central venous catheterization for peripheral blood stem cell harvest procedures. Poster presented at the 43rd annual meeting of the European Society for Blood and Marrow Transplantation 2017, Marseille, France
Salazar et al. Ultrasound-guided peripheral venous access for therapeutic apheresis procedures reduces need for central venous catheters. J Clin Apher [Internet] 2016. Available from: DOI 10.1002/jca.21493
Gopalasingam et al. A successful model to learn and implement ultrasound-guided venous catheterization in apheresis. J Clin Apher [Internet] 2017.Available from: DOI: 10.1002/jca.21533

















