Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 1 TRIM: D16-43121 [v8.0] August 2017 Venous Thromboembolism (VTE) Prevention Clinical Care Standard Consultation Draft
Transcript
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 1
TRIM: D16-43121 [v8.0]
August 2017
Venous Thromboembolism (VTE) Prevention Clinical Care Standard Consultation Draft
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 2
Published by the Australian Commission on Safety and Quality in Health Care Level 5, 255 Elizabeth Street, Sydney NSW 2000
All material and work produced by the Australian Commission on Safety and Quality in Health Care is protected by copyright. The Commission reserves the right to set out the terms and conditions for the use of such material.
As far as practicable, material for which the copyright is owned by a third party will be clearly labelled. The Australian Commission on Safety and Quality in Health Care has made all reasonable efforts to ensure that this material has been reproduced in this publication with the full consent of the copyright owners.
With the exception of any material protected by a trademark, any content provided by third parties, and where otherwise noted, all material presented in this publication is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International licence.
Enquiries about the licence and any use of this publication are welcome and can be sent to [email protected].
The Commission’s preference is that you attribute this publication (and any material sourced from it) using the following citation:
Australian Commission on Safety and Quality in Health Care. Venous Thromboembolism Prevention Clinical Care Standard Consultation Draft. Sydney: ACSQHC; 2017
Disclaimer
The Australian Commission on Safety and Quality in Health Care has produced this clinical care standard to support the delivery of appropriate care for a defined condition. The clinical care standard is based on the best evidence available at the time of development. Healthcare professionals are advised to use clinical discretion and consideration of the circumstances of the individual patient, in consultation with the patient and/or their carer or guardian, when applying information contained within the clinical care standard. Consumers should use the clinical care standard as a guide to inform discussions with their healthcare professionals about the applicability of the clinical care standard to their individual condition.
The Commission does not accept any legal liability for any injury, loss or damage incurred by the use of, or reliance on, this document.
Quality statement 2 – Develop a VTE prevention plan, balancing the risk of VTE against bleeding ............................................................................................................ 16
Quality statement 3 – Inform and partner with patients ............................................. 18
Quality statement 4 – Document and communicate the VTE prevention plan ........ 20
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 4
Venous Thromboembolism Prevention Clinical Care Standard
1. Assess and document VTE risk
A patient potentially at risk of venous thromboembolism (VTE) receives a timely assessment of VTE risk using a locally endorsed tool to determine their need for VTE prevention. The results are documented at the time of the assessment, in a place that is easily accessible to all clinicians involved in the patient’s care.
2. Develop a VTE prevention plan, balancing the risk of VTE against bleeding
A patient assessed to be at risk of VTE has a VTE prevention plan developed that balances the risk of thrombosis against both the risk of bleeding and any contraindications to VTE prevention.
3. Inform and partner with patients
A patient at risk of VTE receives information and education about VTE and ways to prevent it tailored to their risk and needs, and shares in decisions regarding their VTE prevention plan.
4. Document and communicate the VTE prevention plan
A patient’s VTE prevention plan is documented and communicated to all clinicians involved in their care.
5. Use appropriate VTE prevention methods
A patient requiring mechanical compression and/or anticoagulant medicines to prevent VTE is offered therapy according to a current, locally endorsed, evidence-based guideline taking into consideration the patient’s clinical condition and their preferences.
6. Reassess risk and monitor for VTE-related complications
As VTE risk may change over time, regularly reassess thrombosis and bleeding risk and monitor for VTE-related complications at least every seven days, whenever the patient’s clinical condition changes, and on discharge from hospital.
7. Transition from hospital and ongoing care
A patient at risk of VTE is provided with individualised information and is involved in the development of a written discharge plan or care plan that describes their ongoing care after they leave hospital. The plan includes details of VTE prevention received during their hospital stay and/or prescribed at discharge, ongoing monitoring requirements, the need for follow-up, and a list of any medicines that need to be continued on discharge. The plan is discussed with and provided to the patient before they leave hospital. The plan is also communicated to the patient’s general practitioner or ongoing clinical provider within 48 hours of discharge so that ongoing care to prevent VTE can be provided, and completed in accordance with the plan.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 5
About clinical care standards Clinical care standards aim to support the delivery of appropriate evidence-based clinical care, and promote shared decision-making between patients, carers and clinicians.
A clinical care standard contains a small number of quality statements that describe the clinical care that a patient should be offered for a specific clinical condition. The quality statements are linked to a number of indicators that can be used by health services to monitor how well they are implementing the recommended care in the clinical care standard. A clinical care standard differs from a clinical practice guideline; rather than describing all the components of care for managing a clinical condition, a clinical care standard addresses priority areas for improvement.
Each clinical care standard intends to support key groups of people in the healthcare system in the following ways:
• The public will have a better understanding of what care should be offered by the healthcare system, and will be better able to make informed treatment decisions in partnership with their clinician
• Clinicians will be better able to make decisions about appropriate care • Health services will be better able to examine the performance of their organisation
and make improvements in the care they provide.
This clinical care standard was developed by the Australian Commission on Safety and Quality in Health Care (the Commission) in collaboration with consumers, clinicians, researchers and health organisations. It complements existing efforts that support the prevention of VTE in hospital and follow-up care in the community, including state and territory-based initiatives.
For more information about the development of this clinical care standard, including the evidence base for the quality statements, visit www.safetyandquality.gov.au/ccs.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 6
Introduction
Context
Venous thromboembolism (VTE) is a disease process that encompasses deep vein thrombosis (DVT) and pulmonary embolism (PE). In DVT, a blood clot (thrombus) forms in the deep veins most commonly in the legs or pelvis. The clot may cause pain, tenderness or swelling in the leg. In PE some or all of the clot becomes detached and moves from the vein through the right side of the heart to lodge in one or more of the arteries in the lung (pulmonary arteries). Symptoms of PE can include difficulty breathing, coughing up of blood, chest pain, faintness, loss of consciousness, heart failure, and cardiac arrest. If the clot fully blocks enough of the blood supply to the lungs, it may cause death. Those who survive are at increased risk of complications including post-thrombotic syndrome, pulmonary hypertension, or recurrent thrombosis.
VTE is a common cause of morbidity and mortality in Australia, affecting about 20,000 Australians each year.1 The majority of these clots form as a result of hospitalisation (where they are known as hospital-acquired VTE) and are considered potentially preventable. VTE is a common cause of death, accounting for 7% of all deaths in Australian hospitals.2
Hospitalised patients are 100 times more likely to develop VTE compared to the rest of the community.3 Between 59% and 75% of all VTE cases occur as a result of hospitalisation.4 However, as this risk continues beyond discharge from hospital, a majority of VTE cases are not identified until the patient is back in the community. One study has shown that of patients who experienced VTE in the community, over half were associated with hospitalisation in the previous three months. Furthermore, over half of the affected patients failed to receive appropriate prevention while in hospital.5-7
There is a need to identify patients at risk of VTE so that appropriate prevention can be initiated to reduce the burden of this condition, including death related to PE. Actions to reduce the risk of hospital-acquired VTE can also be taken outside the hospital setting. General practitioners and other primary healthcare workers have a critical role in preventing hospital-acquired VTE by monitoring patients and performing ongoing assessment of VTE risk following a patient’s discharge from hospital.8 They also have an important role prior to a patient’s hospitalisation (for example, if they are organising a planned admission), by highlighting the patient’s VTE risk factors, including those that are potentially modifiable prior to admission, providing a best possible medication history (BPMH), and potentially suggesting a plan for prevention.
Strategies to prevent VTE Strategies to prevent hospital-acquired VTE have been shown to reduce its development by about 70%.9-12 Current evidence-based best practice guidelines recommend all hospitalised patients are assessed using a standardised tool to identify those at risk of VTE so that appropriate prevention can be given. The subsequent method chosen to prevent VTE (which could be either mechanical compression or anticoagulant medicines, or the two in combination) depends on an assessment of the patient’s bleeding risk, contraindications to prevention, and their preferences, all of which are carefully balanced against their risk of thrombosis. All patients should be encouraged to mobilise as soon as possible and maintain hydration (provided mobility and fluid restrictions are not in place) to reduce their risk of VTE.13-17
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 7
Risk assessment
VTE risk assessment The risk of developing VTE during or following hospitalisation is dependent on a combination of risk factors related to both the individual patient and their reason for hospitalisation. Many risk factors have been reported and those that have evidence of increasing the risk of VTE are included in quality statement 1.1, 18, 19 In general, risk factors include the medical condition or surgical procedure for which the patient is admitted to hospital, and individual patient factors. The contribution of individual patient factors such as age, obesity, and other comorbidities can vary depending on whether the patient is admitted for a medical condition or surgical procedure. For surgical patients, the risk of VTE also depends on the type of surgery being performed. While all types of surgery increase VTE risk, hip and knee replacement surgery and hip fracture surgery are associated with a much higher risk of VTE.20
About 50-75% of hospitalised patients have at least one risk factor for developing VTE, while 40% of patients have at least three or more.18, 21 An accurate and standardised assessment of a patient’s risk factors for developing VTE, including the patient’s reason for admission is therefore critical. Several tools and approaches to assessing VTE risk have been published and implemented. However there is no consensus between guidelines regarding the preferred method.13, 14 Approaches to assessing VTE risk in medical and surgical patients are generally based upon two methods. These are risk assessment scoring, which is used to stratify a patient’s level of VTE risk (high, medium or low risk), and risk factor recognition, which identifies whether a patient has risk factors for VTE without assigning a score or level of risk. The results of the risk assessment then translate the patient’s VTE risk into evidence-based recommendations for use of prevention, noting the importance of taking into consideration any contraindications to prevention, bleeding risk, and the patient’s preferences for prevention.
Bleeding risk assessment Anticoagulant medicines used to prevent VTE carry an inherent risk of bleeding. Bleeding risk should be specifically assessed in patients prior to prescribing anticoagulants for VTE prevention. Bleeding risk may be increased in patients who have the characteristics listed in quality statement 2. If these conditions exist, the decision to prescribe anticoagulants is made individually, after carefully balancing the benefits of prevention against the patient’s risk of thrombosis.22, 23
Mechanical compression Not moving for long periods is a risk factor for developing VTE, as the normal pumping mechanisms of the legs is greatly reduced, leading to pooling of blood in the deep veins (venous stasis). Mechanical methods of VTE prophylaxis involve the use of compressive devices to combat this effect.15 Options include the use of thigh or knee-length anti-embolism stockings (AES), or pneumatic venous pumping devices that intermittently compress leg muscles of the foot (known as intermittent pneumatic compression (IPC), or venous foot pumps (VFP)).15 Because methods of mechanical compression are not associated with an increased risk of bleeding they are considered to be relatively safe. However, there are fewer studies of these devices, and their efficacy has been reported to be less than anticoagulant medicines in some patient groups. Furthermore, consistent use is required to achieve maximum effect.15, 24
While mechanical compression may be useful in at-risk patients who are still able to mobilise to some extent, it may be more specifically appropriate for patients who are unable to mobilise, or are at high-risk of bleeding (such as after neurosurgery, retinal surgery, orthopaedic surgery, some plastic surgery, head injury or haemorrhagic stroke). Mechanical
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 8
compression can also be combined with anticoagulant medicines to enhance their effect.15, 24 Contraindications to mechanical compression are described in quality statement 5.15, 16
Anticoagulant medicines: Anticoagulant medicines are the preferred method of VTE prevention in most at-risk patients because of their demonstrated superior efficacy to mechanical compression in some patient groups.25 Given VTE develops by activation of coagulant proteins via different coagulation pathways, a range of anticoagulants can be used and include the following options:
Heparins Factor Xa Inhibitors Direct thrombin inhibitors
• Dabigatran • Warfarin Warfarin is commonly used for the treatment of VTE. However it is occasionally used for prophylaxis in the context of orthopaedic surgery.
Anticoagulant medicines are considered high-risk medicines26-28 and are associated with an increased risk of bleeding. The introduction of direct oral anticoagulants (DOACs) including dabigatran, apixaban, and rivaroxaban has extended the choice of VTE prophylaxis available to patients and clinicians. However, the Commission has received reports that the DOACs are being implicated in adverse events associated with erroneous concomitant prescribing of anticoagulants for example, apixaban (a DOAC) for atrial fibrillation combined with enoxaparin (a LMWH) for VTE prevention.
When prescribing anticoagulant medicines, it is important to undertake an individual assessment of bleeding risk factors, as well as the patient’s clinical condition and their current medicines (including all prescribed, over-the counter, and complementary medicines). Some medicines as well as diet are known to interfere with or enhance the effectiveness of anticoagulants such as warfarin, highlighting the importance of routine monitoring of coagulation time (for example, a patient’s International Normalised Ratio or INR).
While DOACs can be given orally and do not require routine laboratory coagulation tests to monitor therapeutic effect, monitoring adherence and managing thrombotic events is more difficult in patients taking these medicines. There is a heightened need to monitor adherence as the risk of thrombosis is greater if a dose is missed. Renal function should also be assessed before prescribing these medicines and at least annually thereafter (and more frequently in the elderly, those with renal impairment or in conditions such as low blood volume, dehydration, or when certain medicines are taken concomitantly).29, 30 Liver function should also be monitored, as should signs and symptoms of bleeding, changing comorbidities, and any other medicines the patient might be taking. Considerations for the safe selection of anticoagulant medicines are listed in quality statement 5.
Role of aspirin for the prevention of VTE in hip and knee replacement surgery. The use of aspirin as a single agent for the primary prevention of VTE in hip and knee replacement surgery remains controversial.
International guidelines differ on their recommendations regarding the use of aspirin to prevent VTE following hip and knee replacement surgery. North American guidelines list aspirin as an acceptable agent without a preference for one agent over another (highlighting
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 9
that evidence is insufficient to do so)31, or with a preference for LMWH.20 However guidelines issued by the United Kingdom’s National Institute for Health Care Excellence (NICE)15, and Scottish Intercollegiate Guidelines Network (SIGN)16 do not recommend use of aspirin, as ‘other available agents are more effective’.
In 2016, the Arthroplasty Society of Australia recommended that patients about to have hip or knee surgery be assessed for their risks of surgical bleeding and postoperative VTE, and that aspirin was an option for the prevention of VTE when there were no additional risk factors for postoperative bleeding or VTE.32 There is no current national Australian clinical practice guideline for the primary prevention of VTE in hospitalised patients. Because local and international guidelines are in conflict, a rapid review of the evidence in relation to aspirin use for the primary prevention of VTE in hip and knee replacement surgery has been conducted. This review is an appendix to the Venous Thromboembolism (VTE) Prevention Clinical Care Standard Evidence Sources document. Findings from this review are equivocal. Much of the evidence supporting the use of aspirin has methodological limitations and is therefore suggestive, but not definitive. In contrast, clear evidence that aspirin is ineffective was not found.
Why this clinical care standard is needed Despite the availability of evidence-based best practice guidelines for the prevention of VTE, data suggest that a significant proportion of patients at risk of VTE do not receive care as recommended in current guidelines.
In a recent Australian report, only 44% of clinical units surveyed reported assessing patients for VTE risk on admission to hospital using a standardised risk-assessment tool. Furthermore only 74% of those assessed to be at risk were offered VTE prevention based on the results of their risk assessment.33 Similarly, a point-prevalence survey of medical patients admitted to the emergency department of an Australian tertiary referral hospital identified that 65% of patients were not prescribed VTE prevention, despite having no contraindication.34 Low rates of risk assessment and use of VTE prevention methods have been reported in other nations35-37 including multinational studies which include Australia.35
This clinical care standard aims to improve the implementation of recommended care for reducing the likelihood of developing VTE while in hospital or following discharge, by ensuring that patients who present to hospital with risk factors for developing VTE are identified using a timely assessment of VTE risk, are informed about VTE, engaged in decisions about their care, prescribed appropriate prevention, and have their VTE risk regularly reviewed.
Key evidence sources that underpin the Venous Thromboembolism Prevention Clinical Care Standard are current clinical guidelines from the United Kingdom’s National Institute for Health and Clinical Excellence (NICE)15, 38, the Scottish Intercollegiate Guidelines Network (SIGN)16, the American College of Chest Physicians (ACCP)20, 39-42, the American Academy of Orthopaedic Surgeons (AAOS)31, the American College of Physicians (ACP)43, and the Royal College of Obstetrics and Gynaecology (RCOG).44 Other resources include the Agency for Healthcare Research and Quality (AHRQ) Quality Improvement Guide13, and the VTE prevention framework developed by the NSW Clinical Excellence Commission (CEC).45
Clinicians and health services across Australia can use this clinical care standard to support the delivery of high-quality care to prevent VTE in their patients.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 10
Goal of this clinical care standard To ensure that all adults presenting* to hospital who are potentially at risk of hospital-acquired VTE are identified and have an assessment of VTE risk and bleeding risk that is formally documented, and that VTE prevention is appropriately prescribed and used to reduce avoidable death or disability from hospital-acquired VTE. Patients also receive information about VTE and the risks and benefits of prevention so they can share in decisions about their care and ways to prevent VTE.
Scope This clinical care standard relates to the care that all adult patients should receive to reduce their risk of hospital-acquired VTE. It applies to those who have been or are:
• Admitted to a hospital ward, unit, or day procedure service within the preceding 24 hours22
• Discharged home from the emergency department with significantly reduced mobility compared to their normal state (for example, due to a lower-limb injury requiring immobilisation with a plaster cast/brace)22
• Pregnant or gave birth within the preceding six weeks, and who are presenting to outpatient services for antenatal or perinatal care.
This clinical care standard covers the initial presentation to hospital and assessment of VTE risk, through to completion of VTE prevention (which may occur following discharge from hospital back in the community). This clinical care standard applies to all hospital settings where patients are at risk of developing VTE, including public and private hospitals, day procedure services, and sub-acute facilities such as rehabilitation and palliative care. It also applies to community settings where the ongoing monitoring and assessment of VTE risk is required to prevent VTE following hospitalisation.
The use of inferior vena cava (IVC) filters for the prevention of VTE is not covered by this clinical care standard. Patients using these devices should be referred to an appropriate specialist for management.
The treatment of VTE is also not covered by this clinical care standard.
General principles of care
Patient-centred care
Patient-centred care is health care that is respectful of, and responsive to, the preferences, needs and values of patients and consumers.46
Clinical care standards support the key principles of patient-centred care, namely: • Treating patients with dignity and respect • Encouraging patient participation in decision making • Communicating with patients about their clinical condition and treatment options • Providing patients with information in a format that they understand so they can
participate in decision making.47
*This includes all patients identified in the scope of this clinical care standard.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 11
Multidisciplinary care
During a hospital admission and following hospital discharge, patients are likely to need specific types of care provided by other clinicians. In this document, the term clinician refers to any health professional (not only a doctor) who provides direct clinical care to patients. Multidisciplinary care refers to comprehensive care provided by a range of clinicians (for example, nurses, pharmacists, physiotherapists and other allied health professionals) from one or more organisations, who work collectively with the aim of addressing as many of a patient's health and other needs as possible.48
A coordinated multidisciplinary team approach is essential for delivering the care required to reduce the risk of VTE. Multidisciplinary care of patients can improve health outcomes, and offers more efficient use of health resources. Planning, coordination and regular communication between clinicians are essential components of multidisciplinary care.49
Carers and family members
Carers and family members have a central role in the prevention, early recognition, assessment and recovery relating to patients’ health conditions. They often know the patient very well and can provide detailed information about the patient’s history, routines or symptoms, which may assist in determining treatment and ongoing support.46
Although this clinical care standard does not specifically refer to carers and family members, each quality statement should be understood to mean that carers and family members are involved in clinicians’ discussions with patients about their care, if the patient wants carer involvement.
Using this clinical care standard
Integrated approach
Central to the delivery of patient-centred care identified in this clinical care standard is an integrated, systems-based approach supported by health services and networks of services with resources, policies, processes and procedures.
Key elements of this approach include: • An understanding of the capacity and limitations of each component of the health
system across metropolitan, regional and remote settings • Clear lines of communication between components of the healthcare system, including
primary, hospital and community services • Appropriate coordination so that people receive timely access to optimal care
regardless of how or where they enter the system.
To achieve these aims, healthcare services implementing the standard may need to: • Deploy an active implementation plan and feedback mechanisms • Include agreed protocols and guidelines, decision-support tools and other resource
material • Employ a range of incentives and sanctions to influence behaviours and encourage
compliance with policy, protocol, regulation and procedures • Integrate risk management, governance, operational processes and procedures,
including education, training and orientation.50
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 12
Indicators to support local monitoring The Commission has developed a set of indicators to support healthcare providers and local health services to monitor how well they implement the care described in the clinical care standard. The indicators are a tool to support local quality improvement activities. There are no benchmarks set for any of the indicators. Healthcare providers using the indicators can compare their results against themselves during a previous period, or with other healthcare providers with whom they have made such arrangements.
Most of the data underlying these indicators require collection from local sources, chiefly through prospective collection or a retrospective chart review. Some indicators refer to ‘local arrangements’. These can include clinical guidelines, policies, protocols, care pathways or any other documentation providing guidance to clinicians on the care of patients to prevent hospital-asquired VTE.
Monitoring the implementation of the clinical care standards will assist in meeting some of the requirements of the National Safety and Quality Health Service (NSQHS) Standards. Information about the NSQHS Standards is available at: www.safetyandquality.gov.au/accreditation
The process to develop the indicators specified in this document comprised: • An environmental scan of existing local and international indicators • A prioritisation review and refinement of the indicators with the Venous
Thromboembolism Topic Working Group.
In this document, the indicator titles and hyperlinks to the specifications are included with the relevant quality statement under the heading ‘Indicators for local monitoring’. Full specifications of the Venous Thromboembolism Prevention Clinical Care Standard indicators will be found in the Metadata Online Registry (METeOR) on finalisation of the clinical care standard at http://meteor.aihw.gov.au/content/index.phtml/ itemId/<<to_be_inserted_on finalisation_of_the_clinical_care_standard>> METeOR is Australia’s web-based repository for national metadata standards for the health, community services and housing assistance sectors. Hosted by the Australian Institute of Health and Welfare, METeOR provides users with online access to a wide range of national endorse data and indicator definitions.
Indicators to support local monitoring of the overall quality of VTE prevention As the goal of this clinical care standard is to reduce a patient’s risk of hospital-acquired VTE, two overall outcome measures are recommended. These hospital-acquired complications are collected routinely and can assist hospitals in tracking the success of their efforts to prevent VTE. These include:
Outcome indicator 1: Rate of hospital-acquired deep vein thrombosis
Outcome indicator 2: Rate of hospital-acquired pulmonary embolism
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 13
Supporting documents The following resources supporting this clinical care standard are available from the Commission’s website at: https://www.safetyandquality.gov.au/our-work/clinical-care-standards/current-consultations/
• A consumer fact sheet • A clinician fact sheet • An evidence sources document, summarising the evidence base for the clinical care
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 14
Quality statement 1 - Assess and document VTE risk A patient potentially at risk of VTE receives a timely assessment of VTE risk using a locally endorsed tool to determine their need for VTE prevention. The results are documented at the time of the assessment, in a place that is easily accessible to all clinicians involved in the patient’s care.
Purpose To ensure patients potentially at risk of VTE receive a timely assessment of VTE risk to determine their need for VTE prevention, and that the findings are documented at the time of the assessment in a place that is easily accessible to all clinicians involved in the patient’s care.
What the quality statement means: For patients: If you are going to hospital, your doctor or another member of your clinical team (such as a nurse or midwife) will conduct a thorough assessment to see what risk you have of developing blood clots. Your risk of developing blood clots while in hospital depends partly on the reason why you are there and the treatment you need to have. You might also have certain risk factors that make you more likely to develop blood clots. You will be asked about your general health and mobility, whether you or a family member have had blood clots before, and any other health conditions you might have such as cancer, heart disease, or varicose veins, that might make your blood more likely to clot. You will also be asked about any medicines you might be taking (including over-the-counter and complementary medicines) as some medicines, such as the oral contraceptive, can make the blood more likely to clot. Once your risk of developing blood clots has been assessed, your clinician will write up the findings so all the clinicians involved in your care understand what risk you have of developing blood clots and whether you need prevention.
For clinicians: Assess each patient for VTE risk to determine their need for VTE prophylaxis. Use a standardised*, locally endorsed tool to aid the assessment.13, 38, 45, 57 Ensure the tool includes an assessment of the patient and admission related factors that are known to increase risk of VTE as outlined in Box 1. Document the findings on the national inpatient medication chart (NIMC), or where applicable, the patient’s medical record, approved risk assessment form, or other place according to local policy at the time of the risk assessment so they are available to all clinicians involved in the patient’s care.22, 45, 57, 58
* A range of standardised VTE risk assessment tools are available. Some examples are:
• National Institute for Health and Care Excellence – Department of Health Risk Assessment for Venous Thromboembolism53
• Caprini Risk Assessment Model for use in hospitalised surgical patients54 • Padua Risk Assessment Model for use in medical pateints55 • Parvizi – Individualised risk model for venous thromboembolism after total joint arthroplasty56
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 15
For health services: Ensure a robust multidisciplinary VTE prevention program is in place that facilitates an assessment of a patient’s VTE risk according to evidence-based guidelines.57 Ensure a standardised approach to risk assessment is taken by selecting and endorsing a risk assessment tool for use within the health service. Also ensure that monitoring and feedback to clinicians takes place to confirm risk assessments are being conducted in accordance with the tool as ongoing quality improvement.11, 22, 59
Indicator for local monitoring 1. Proportion of patients admitted to hospital who were assessed for VTE risk within 24 hours of admission, using a locally endorsed risk assessment tool, and had the outcome of the risk assessment documented in their medical record.
• Have had, or are expected to have significantly reduced mobility for three days or more
• Are expected to have ongoing reduced mobility relative to their normal state and have one or more of the patient-related risk factors listed below.
Surgical patients • Surgical procedure more than 90 minutes, or more than 60 minutes if the surgery
involves the pelvis or lower limb • Acute surgical admission with inflammatory or intra-abdominal condition • Expected significant reduction in mobility • Have one or more of the patient-related risk factors listed below.
Patient-related risk factors associated with developing VTE • Age over 60 years • Active cancer or receiving cancer treatment • Dehydration • Thrombophilia • Obesity (BMI over 30kg/m2) • One or more significant medical conditions (heart disease, metabolic, endocrine or
respiratory pathology, acute infectious or inflammatory condition) • Personal history or a first degree relative with a history of VTE • Use of hormone replacement therapy, oestrogen-containing contraceptive therapy,
tamoxifen, or antipsychotics25 • Varicose veins with phlebitis.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 16
Quality statement 2 – Develop a VTE prevention plan, balancing the risk of VTE against bleeding A patient assessed to be at risk of VTE has a VTE prevention plan developed that balances the risk of thrombosis against both the risk of bleeding and any contraindications to VTE prevention.
Purpose To ensure a patient’s VTE prevention plan is developed based on an assessment of VTE risk, which is carefully balanced against the risk of bleeding, and that contraindications to VTE prevention are also considered prior to it being initiated.
What the quality statement means: For patients: If you are assessed to be at risk of developing blood clots, your clinician will develop a clot-prevention plan by weighing up your risk of clotting against your risk of bleeding. Your clinician will also check whether you have any other conditions that might prevent you from receiving clot-prevention. Your risk of bleeding will be assessed, as the medicines used to prevent blood clots can themselves cause bleeding, and have the unintended effect of making it harder to stop bleeding once it starts. Your risk of bleeding depends on the reason why you are in hospital and the treatment you need to have, as well as other risk factors you might have that can make you more likely to bleed. You will be asked about whether you or a family member have a history of conditions that cause bleeding, whether you have had any bleeding in the last 48 hours, and any other health conditions such as kidney or liver disease, high blood pressure, stroke, or peptic ulcer disease, that may increase your risk of bleeding. You will also be asked about any medicines you might be taking, including over-the-counter and complementary medicines, to identify if you are already taking a medicine that may cause you to bleed. The information you provide will help your clinician weigh up your risk of bleeding against your risk of clotting, and help to develop the best clot-prevention plan for you.
For clinicians: For patients assessed to be at risk of VTE, develop a plan for VTE prophylaxis by balancing the risk of VTE against the risk of bleeding and contraindications to prophylaxis before offering it to the patient. Assess bleeding risk using a standardised, locally endorsed tool.* Ensure the tool assesses the admission and patient-related factors that may impact on bleeding, including the reason for admission, patient’s comorbidities, bleeding history, and medication history as outlined in Box 2. Obtain a best possible
* A range of standardised bleeding risk assessment tools are available. Some examples are:
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 17
medication history (BPMH)70 using a standardised approach as part of the assessment, to identify medicines the patient might be taking (including complementary and over-the-counter medicines) that increase the risk of bleeding. Balance the risk of bleeding against the risk of thrombosis to formulate an overall assessment of the patient’s VTE risk prior to selecting prophylaxis.22, 23
For health services: Ensure systems are in place to so that a patient at risk of VTE has a VTE prevention plan developed based on an assessment of bleeding risk, which is carefully balanced against the risk of thrombosis and contraindications to VTE prophylaxis. Ensure a standardised approach to bleeding risk assessment is taken by selecting and endorsing a risk assessment tool for use within the health service. Ensure a standardised approach to obtaining a BPMH is in place to identify any medicines the patient might be taking that are associated with an increased risk of bleeding, and that monitoring takes place to identify that VTE prevention plans are developed in accordance with local policy.
• Neurosurgery, spinal surgery or eye surgery • Lumbar puncture, epidural or spinal anaesthesia within the previous four hours, or
expected within the next 12 hours • Surgical procedure with high bleeding risk, such as intracranial surgery, head and neck
surgery, or orthopaedic surgery.
Patient-related risk factors associated with increased bleeding risk • Abnormal renal function or liver disease • History of hypertension (230/120mmHg or higher) or acute stroke • Active peptic ulcer or ulcerative gastrointestinal disease • Thrombocytopenia (platelets <75 x 109/L) • Bleeding history
- family history of bleeding or personal history of bleeding disorders - recent bleeding (within the last 48 hours) or active bleeding
• Medication history - use of other medicines known to increase bleeding risk (such as aspirin, non-
steroidal anti-inflammatory drugs (NSAIDs), clopidogrel, dipyridamole, prasugrel, ticlopidine, tigacrelor), other anticoagulants (such as enoxaparin, warfarin, dabigatran, rivaroxaban, or apixaban), thrombolytics, or alter the metabolism of anticoagulants
- history of heparin-induced thrombocytopenia (HIT).
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 18
Quality statement 3 – Inform and partner with patients A patient at risk of VTE receives information and education about VTE and ways to prevent it tailored to their risks and needs, and shares in decisions regarding their VTE prevention plan.
Purpose To educate patients about VTE and how it can be prevented so they can share in decisions about their care and ways to prevent VTE.61
What the quality statement means: For patients: Your doctor or other member of your clinical team will provide you with information and education about blood clots and why you may be at risk. You will also receive information about possible ways to prevent blood clots tailored to your risk factors and information needs, including the risks and benefits of prevention, its correct use, any monitoring that may be needed, precautions you should take while using clot-prevention, the signs and symptoms of blood clots (such as a hot swollen leg or ankle) or bleeding, and what to do if this occurs. Unless you are told otherwise, you will be encouraged to get out of bed as soon as possible during your hospital stay, and to remain hydrated as not moving for long periods of time and dehydration increase the risk of developing blood clots. You are also involved in the development of your clot-prevention plan which is based on the results of your risk assessment and the methods you prefer to use to reduce your clotting risk. Understanding more about your risk of developing blood clots and the possible ways to prevent them will help you to be more involved in decisions about your clot-prevention plan and the things that you can do to prevent formation of blood clots.
For clinicians: Support the patient to have an active role in preventing VTE by: • Providing information and education about VTE and ways to potentially prevent it
tailored to the patient’s risk and in a format they can understand15, 16, 22, 38, 45 • Informing patients about the findings of their VTE risk assessment and their individual
risk factors for developing VTE16, 44 • Involving patients in decisions about their plan for VTE prophylaxis45 and discussing
factors that may influence the choice of prophylaxis such as bleeding risk, the availability of antidotes to reverse bleeding, needle phobia, or whether they have any personal beliefs (for example, those held by Jehovah’s Witnesses) that could affect their suitability to receive blood products70
• Encouraging patients to mobilise as soon as possible and to remain hydrated, unless mobility and fluid restrictions are in place15, 16
• Explaining the risks and benefits of VTE prophylaxis16, 70, including correct use, monitoring requirements, available options to manage potential adverse events such as bleeding, precautions to be taken while using prophylaxis, and the potential outcomes if prophylaxis is not used correctly16, 28, 71
• Educating patients about the signs and symptoms of VTE and bleeding, how to minimise the risk of these occurring, and what to do if these occur 16, 25, 71
• Monitoring and adjusting the plan for VTE prophylaxis as the patient’s risk factors and clinical condition changes
• Referring the patient to other clinicians or resources for further information about VTE and ways to prevent it
• Discussing the plan for prophylaxis with the patient, and documenting the outcome of the discussion as part of the informed consent process.16
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 19
Useful sources of patient information are listed in Box 3.
For health services: Ensure systems are in place to provide patients with information and education about VTE and how it may potentially be prevented. Ensure information provided to patients covers the risks and benefits of prophylaxis, its correct use, risks associated with the use or misuse of prophylaxis, precautionary measures to be taken while using prophylaxis, the signs and symptoms of VTE and bleeding, and what to do if the patient believes these symptoms are occurring. This will enable the patient to be more engaged in their care and to participate more effectively in decision-making about their VTE prevention plan.
Box 3: Useful sources of information about VTE and ways to prevent it
• NSW Clinical Excellence Commission • NPS MedicineWise • University of Tasmania anticoagulation.com.au • Michigan Anticoagulant Quality Improvement Initiative • The Joint Commission
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 20
Quality statement 4 – Document and communicate the VTE prevention plan A patient’s VTE prevention plan is documented and communicated to all clinicians involved in their care.
Purpose To ensure all clinicians involved in the patient’s care are aware that a plan for VTE prevention is in place.
What the quality statement means: For patients: When your clot-prevention plan has been finalised, your clinician will turn the plan into a written document so that all the clinicians involved in your care know what your clot-prevention plan is.
For clinicians: Once you have finalised a patient’s plan for VTE prophylaxis, document the plan with the results of the risk assessment in the patient’s medical record, or where applicable, the national inpatient medication chart (NIMC), approved risk assessment form, or other place according to local policy.22, 28, 45, 57, 58, 61
For health services: Ensure that systems are in place that specify where to document decisions about VTE prophylaxis, and that monitoring takes place to ensure documentation occurs according to local policy. This might include the patient’s medical record, NIMC, approved risk assessment form, or other place according to local policy.45
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 21
Quality statement 5 – Use appropriate VTE prevention methods A patient requiring mechanical compression and/or anticoagulant medicines to prevent VTE is offered therapy according to a current, locally endorsed, evidence-based guideline taking into consideration the patient’s clinical condition and their preferences.
Purpose To ensure the safe and effective use of VTE prevention and to minimise the risk of adverse events.
What the quality statement means: For patients: If you need mechanical compression such as compression stockings, and/or anti-clotting medicines to prevent blood clots, it will be used according to a current guideline. Before selecting the clot-prevention method that is best for you, your doctor will take into account any other health conditions you may have, any other medicines you are taking (including all prescribed, over-the-counter and complementary medicines), and your preferences for prevention. You will receive information and education about the clot-prevention method selected for you, including its risks and benefits, how it should be used, how long it should be used for, possible side effects and how to manage these, and any special precautions you should take while using clot-prevention.
For clinicians: If mechanical compression and/or anticoagulant medicines are required, use according to a current, locally endorsed, evidence-based guideline.15, 16, 25, 31, 38, 41, 43, 44, 58, 60-62 Provide information and education about the recommended prophylaxis at the time it is initiated to reduce the likelihood of harm associated with its use. This information should include the risks and benefits of prophylaxis, how to use it, how long to use it for, possible side effects and how they should be managed, and precautions associated with using prophylaxis.13, 16, 22, 23, 25, 28, 45, 58, 71 If anticoagulant medicine is prescribed, document on the national inpatient medication chart (NIMC) the fact that information and education about the medicines has been provided.70 For those not using the NIMC, document the fact that information and education has been provided in the patient’s medical record, or other place according to local policy.
For health services: Ensure systems are in place to provide clinicians with access to a current evidence-based guideline that guides the appropriate use of mechanical prophylaxis and quality use of medicines, and that prescribing patterns can be monitored against these guidelines for feedback to clinicians and ongoing quality improvement.28 Ensure that systems support clinicians in providing individualised information and education to patients about their prevention, and that patients have access to ongoing advice when needed. Ensure anticoagulant medicines used to prevent VTE are identified within the organisation as high-risk medicines.26-28 Oversee their storage, prescribing, dispensing and use according to local high-risk medicines policies, and consider the implementation of stewardship activities, such as audit and feedback, to optimise their safe prescribing and use.72
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 22
Indicators for local monitoring 5a) Evidence of local arrangements to ensure that VTE prophylaxis is prescribed in accordance with the local guideline/policy AND the results of the VTE risk assessment 5b) Proportion of patients prescribed VTE prophylaxis appropriate to their level of risk in accordance with the locally approved guideline/policy
Box 4: Top tips for safe use of mechanical compression
Mechanical compression is contraindicated in patients with the following characteristics:15, 16
• Peripheral neuropathy • Peripheral vascular disease • Leg deformity • Leg oedema • Pulmonary oedema • Dermatitis • Morbid obesity, where correct fitting of stockings cannot be achieved • Acute stroke – use IPC devices only.
Patients using mechanical compression should have a comprehensive vascular assessment to exclude peripheral arterial disease, particularly those with diabetes or arteriosclerosis.
Box 5: Top tips for safe selection of anticoagulant medicines
When selecting an anticoagulant medicine consider: • Kidney and liver function • Other medicines the patient might be taking, particularly those like aspirin, clopidogrel,
dypridamole, prasugrel, ticlopidine, ticagrelor, or nonsteroidal anti-inflammatory drugs (NSAIDs) that may exacerbate bleeding, and medicines that alter the metabolism of anticoagulants
• Whether the patient is already taking an anticoagulant medicine (such as warfarin, enoxaparin, dabigatran, rivaroxaban, or apixaban) for another condition
• The presence of gastrointestinal disease • The potential for their interaction with food or other medicines • The need for laboratory monitoring of coagulation tests • Whether an antidote is available to reverse unexpected bleeding • Whether the patient has any personal beliefs that could preclude them from receiving
blood products in the event of a bleed (for example, beliefs held by Jehovah’s Witnesses)
• Adherence, which includes giving consideration to the frequency of dosing, and whether the patient requires a dose administration aid.
For further safety information about anticoagulants see Appendix 1 (under development) Other useful safety information is available from: the NSW Clinical Excellence Commission , University of Tasmania anticoagulation.com.au, the Institute for Safe Medication Practices, the Michigan Anticoagulant Quality Improvement Initiative, and The Joint Commission.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 23
Quality statement 6 – Reassess risk and monitor for VTE-related complications As VTE risk may change over time, regularly reassess thrombosis and bleeding risk and monitor for VTE-related complications at least every seven days, whenever the patient’s clinical condition changes, and on discharge from hospital.
Purpose To ensure that VTE prevention remains suitable to the patient’s condition13, is being used correctly, and to identify VTE-related complications such as bleeding or thrombosis, or erroneous concomitant prescribing of anticoagulants that may have occurred during the patient’s hospital stay.15
What the quality statement means: For patients: Your risk of developing blood clots and whether you have had any problems as a result of using or not using clot-prevention methods will be regularly reassessed throughout your hospital stay to make sure you continue to get the care that you need. If there are any changes to your risk or if you have had any problems as a result of your clot-prevention (for example a clot or bleed) your doctor or other member of your clinical team will discuss this with you. There may be a need to adjust your clot-prevention plan, or review whether you might be at further risk of clotting or bleeding.
For clinicians: Reassess risk of VTE and bleeding at least every seven days22, 45, whenever there is a change in the patient’s clinical condition, and on discharge from hospital.15, 16, 22, 44,
45, 58, 62 Ensure the reassessment also includes a review of any VTE-related complications that may have occurred during the hospital stay, (such as a clot or bleed) and of any medicine-related problems23 associated with the use of anticoagulants, such as erroneous concomitant prescribing. If VTE risk or bleeding risk changes during the admission, review VTE prophylaxis and adjust accordingly in line with a current, locally endorsed, evidence-based guideline and the patient’s preference.
For health services: Ensure there are systems in place to support reassessment of VTE risk at least every seven days, whenever there is a change in the patient’s clinical condition, and on discharge from hospital. Ensure systems are also in place to support monitoring and documentation of complications such as bleeding or thrombosis, or medicine-related problems associated with the use of anticoagulant medicines.
Indicator for local monitoring 6. Proportion of patients with a bleeding complication attributable to anticoagulant prophylaxis.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 24
Quality statement 7 – Transition from hospital and ongoing care A patient at risk of VTE is provided with individualised information and is involved in the development of a written discharge plan or care plan that describes their ongoing care after they leave hospital. The plan includes details of VTE prevention received during their hospital stay and/or prescribed at discharge, ongoing monitoring requirements, the need for follow-up, and a list of any medicines that need to be continued on discharge. The plan is discussed with and provided to the patient before they leave hospital. The plan is also communicated to the patient’s general practitioner or ongoing clinical provider within 48 hours of discharge so that ongoing care to prevent VTE can be provided and completed in accordance with the plan.
Purpose To minimise adverse events during care transition by ensuring patients at risk of VTE, their general practitioner, or ongoing clinical provider, receive a discharge plan or care plan that describes the ongoing care the patient requires to prevent VTE after they leave hospital.
What the quality statement means: For patients: Before you leave the hospital, your doctor or another member of your clinical team will provide you with information and education about the ongoing care you need to prevent blood clots after you leave the hospital. You will be involved in the development of a written discharge plan or care plan, which may need to be updated as your condition changes. The plan will summarise the reason why you came to hospital, the clot-prevention you received, any blood tests or follow-up appointments you need, and a list of any medicines you need to keep taking after you leave hospital. If you need to continue taking anti-clotting medicines, you will be provided with information to ensure you know how to use them safely. You will get a copy of this plan before you leave hospital. Your general practitioner or other ongoing clinical provider will also receive a copy of the plan within two days of you leaving hospital so they can ensure the care you need to prevent blood clots is completed in line with your plan.
For clinicians: Before a patient leaves hospital, reassess risk of VTE and bleeding to determine the need for prophylaxis after discharge.45 Develop a written discharge plan or care plan73 with the patient and provide them with information about their ongoing care required to prevent VTE.15, 16, 25, 38, 44, 51, 58, 74 Ensure the plan summarises the reason for the patient’s admission, their risk factors for VTE and the VTE prophylaxis used while in hospital and/or prescribed at discharge. Provide details about any monitoring requirements specific to VTE prophylaxis, any precautions that need to be taken, and the need for follow-up.62, 71 Provide a current medicines list25 including all the medicines the patient needs to continue on discharge. If anticoagulants are prescribed, provide information to ensure their safe use.15, 28, 71 Provide a copy of the plan to the patient before they leave hospital. Ensure a copy of the plan is communicated to the general practitioner or ongoing clinical provider within 48 hours15, 16, 75 of the patient leaving hospital so that care to prevent VTE can be provided and completed by the ongoing care provider, in accordance with the plan.76
For health services: Ensure systems are in place so clinicians can provide patients with individualised information about the care that they need following hospital discharge and develop a written discharge plan or care plan with the patient prior to discharge. If anticoagulant medicines are prescribed on discharge, ensure systems are in place to enable the provision of information to patients about their safe use before leaving hospital. Ensure a
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 25
multidisciplinary approach to discharge planning is taken, involving a range of clinicians appropriate to the patient’s needs. Ensure systems support clinicians in providing the discharge plan or care plan to the patient’s general practitioner or other ongoing clinical provider within 48 hours of discharge, so that care to prevent VTE can be provided and completed by the ongoing care provider in accordance with the plan, and reduce the likelihood of VTE-related complications following hospital discharge.
Indicator for local monitoring 7. Proportion of patients discharged on anticoagulant medicine that had a documented care plan that included the prescribed dose and duration of treatment.
Box 6: Top tips for the safe use of anticoagulant medicines following discharge from hospital If an anticoagulant medicine is needed to prevent blood clots following discharge from hospital, ensure the following information is provided:
• The name of the medicine, the reason for taking it, how much to take, when to take it, and how long to take it for
• Possible side effects and symptoms that should be reported to a clinician, such as bleeding, and what to do if this occurs
• Precautions that can be taken to reduce the risk of bleeding (such as shaving with an electric razor instead of a razor blade)
• The influence of diet and alcohol on anticoagulant medicines, if relevant • Advice on the importance of patients telling all clinicians involved in their care (including their
dentist) if they are taking a medicine to prevent blood clots • The consequence of not taking anticoagulant medicine, or taking too much, and what to do if a
dose is missed • Whether blood tests or follow-up appointments are needed • Where to go for further information about blood clots and anticoagulant medicines.
Box 7: Top tips for successful transition and ongoing care in the community To minimise adverse events during transitions of care, a discharge plan or care plan outlining the ongoing care the patient requires to prevent VTE should be developed and discussed with the patient prior to leaving hospital. This plan should also be communicated to the patient’s general practitioner or other ongoing clinical providers within 48 hours of discharge to facilitate smooth transition of care. General practitioners or other ongoing clinical providers can ensure VTE prophylaxis is completed in accordance with the plan by:
• Continuing to prescribe anticoagulants for the duration specified in the care plan, as needed • Monitoring the response to prophylaxis, and that it is being used as directed • Checking if any adverse events have occurred, and taking appropriate action to manage these • Monitoring the patient’s co-morbidities and any changes to these • Reviewing all prescribed, over-the-counter, and complementary medicines the patient may be
taking and their potential for interactions with anticoagulant medicines • Checking kidney function, particularly in elderly patients and if a decline in function is suspected,
and verifying the dose of anticoagulant is still correct for the patient’s renal function • Checking liver function, if there is a reason to suspect it is abnormal • Evaluating the need for coagulation tests or a full blood count (only request a full blood count if
anaemia is suspected)76 • Re-assessing VTE risk, if the patient’s clinical condition changes • Checking whether the patient has signs and symptoms of VTE or bleeding, and if so, take
appropriate action.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 26
Appendix 1: Anticoagulant medicines used to prevent VTE NOTE: CURRENTLY UNDER DEVELOPMENT – Using unfractionated heparin (UFH) as an example60, 77
Drug Unfractionated heparin (UFH) Enoxaparin (Clexane)
Dalteparin (Fragmin)
Nadroparin (Fraxiparine)
Danaparoid (Orgaran)
Fondaparinux (Arixtra)
Dabigatran (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)
Warfarin (Coumadin, Marevan)
Approved indication for VTE prophylaxis
• Surgical patients • High risk medical patients
Route of administration Subcutaneous
Frequency of dosing Two to three times a day
Side effects other than bleeding
• Bleeding, bruising, pain at injection site • Hyperkalaemia • Mild reversible thrombocytopenia • Severe thrombocytopenia (Heparin Induced Thrombocytopenia
(HIT)
Use in renal or liver impairment
Contraindicated in severe liver impairment or disease
Antidote to reverse bleeding Protamine
Administration considerations
Do not inject IM as risk of haematoma
Monitoring requirements Monitor platelet count at baseline and periodically throughout heparin administration
Drug interactions Other drugs which can affect the clotting process – monitor closely Other drugs that increase serum potassium levels – monitor closely
Food interactions Heavy alcohol drinkers are a greater risk of major heparin associated bleeding than moderate or non-drinkers
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 27
Glossary Adverse events Adverse events are unintended and sometimes harmful occurrences
associated with the use of a medicine, vaccine or medical device (collectively known as therapeutic goods). Adverse events include side effects to medicines and vaccines, and problems or incidents involving medical devices.78
Assessment A clinician’s evaluation of the disease or condition based on the patient’s report of the symptoms and course of the illness or condition, on information reported by family members and other healthcare team members, and on the clinician’s objective findings (including data obtained through tests, physical examination, medical history, and information reported by family members and other healthcare team members).79
Anticoagulant medicines Medicines that reduce the blood’s tendency to clot on the venous side of the circulation, and therefore used to manage or prevent venous thrombosis (clots made of fibrin).80
Antiplatelet medicines A class of medicines that decreases platelet aggregation and inhibits thrombus formation on the arterial side of the circulation, and therefore used to manage arterial thrombosis (clots made of platelets). They are used to reduce the risk of heart attacks and strokes. They are not normally used in managing VTE (fibrin clots). Antiplatelet medicines include aspirin, clopidogrel, prasugrel, ticlopidine and ticagrelor).
Anti-embolism stockings (AES)
Hosiery which, when worn on the leg, exerts graduated compression on the leg surface and is intended to reduce the development of deep vein thrombosis. These should not be confused with graduated compression stockings (GCS) which have a different pressure profile and are not used for the prevention of venous thromboembolism.15 Graduated compression stockings are used for managing conditions such as venous leg ulcers and lymphedema.
Best available evidence The best systematic research evidence available which is used to support decisions about the care of individual patients.
Best possible medication history (BPMH)
A list of all the medicines a patient is using at presentation to a clinician or health service. The list includes the name, dose, route, and frequency of the medicine, and is documented on a specific form or a specific place. All prescribed, over-the-counter, and complementary medicines should be included. This history is obtained by a trained clinician interviewing the patient (and/or their carer) and is confirmed, where appropriate, by using other sources of medicines information (for example, the patient’s general practitioner, or community pharmacy).81
Best practice The diagnosis, treatment, or care provided, based on the best-available evidence, which is used to achieve the best possible outcomes for the patient.
Evidence-based (or best-practice) guideline
A set of recommended actions that are developed using the best-available evidence. They provide clinicians with evidence-informed recommendations that support clinical practice and guide clinician and patient decisions about appropriate health care in specific clinical practice settings and circumstances.39 Examples include the United Kingdom’s National Institute for Health and Clinical Excellence (NICE)15, the Scottish Intercollegiate Guidelines Network (SIGN)16, the American College of Chest Physicians (ACCP)41, the American
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 28
Academy of Orthopaedic Surgeons (AAOS)31, or the Royal College of Obstetrics and Gynaecology (RCOG).44
Carers People who provide care and support to family members or friends who have a disease, disability, mental illness, chronic condition, terminal illness or general frailty. Carers include parents and guardians caring for children.50
Clinician A trained health professional that provides direct clinical care to patients. Clinicians include registered and non-registered practitioners working individually or as teams. They include doctors, nurses, allied health professionals, nurses’ assistants, Aboriginal health workers and all other people who provide health care.50, 82
Complementary medicines These include products containing herbs, vitamins, minerals, nutritional supplements, homoeopathic medicines, aromatherapy oils, and traditional Chinese medicines. Also called herbal, natural and alternative medicines.83
Deep vein thrombosis (DVT)
Blockage in the large veins of the legs, thighs, or pelvis, caused by the clotting of blood.
Doctor See ‘medical practitioner’.
Dose administration aid (DAA)
A tamper-evident, well-sealed device or packaging system that allows for organising doses of medicine according to the time of administration. Different types of DAAs are available, and can include blister or bubble packs, and packs that are provided by automated dose-packaging systems. A DAA is a tool that can be used as a part of coordinated medication management.84
Graduated Compression Stockings (GCS)
Stockings manufactured to provide compression around legs at gradually increasing pressures. There are two different standards for graduated compression stockings, the British Standard and the European Standard. These are different to anti-embolism stockings which are used for the prevention of venous thromboembolism. Graduated compression stockings are used for managing conditions such as venous leg ulcers and lymphedema.15
Health service A service responsible for the clinical governance, administration and financial management of unit(s) providing health care. A service unit involves a grouping of clinicians and others working in a systematic way to deliver health care to patients and can be in any location or setting, including pharmacies, clinics, outpatient facilities, hospitals, patients’ homes, community settings, practices and clinicians’ rooms.50
High-risk medicine A medicine that has a high risk of causing injury or harm if misused or used incorrectly.27
Hospital A licensed facility providing healthcare services to patients for short periods of acute illness, injury or recovery.85
Mechanical compression See ‘mechanical prophylaxis’.
Mechanical prophylaxis A physical agent that is used, in this context, to prevent thrombosis. Mechanical methods of VTE prophylaxis include: anti-embolism stockings(AES)/graduated compression stockings (GCS), intermittent pneumatic compression devices (IPCD), foot impulse devices (FID), also known as foot pumps.15
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 29
Medical practitioner A medically-qualified person whose primary role is the diagnosis and treatment of physical and mental illnesses, disorders and injuries. This could include general practitioners, medical specialists and non-specialists.
Medicine A chemical substance given with the intention of preventing, diagnosis, curing, controlling or alleviating disease, or otherwise improving the physical or mental wellbeing of people. Prescription, non-prescription, investigational and clinical trial, and complementary medicines are included, irrespective of how they are administered.86
Medicine-related problem Any event involving treatment with a medicine that has a negative effect on a patient’s health or prevents a positive outcome. Consideration should be given to disease-specific, laboratory test-specific and patient-specific information. Medicine-related problems include issues with medicines such as:
• Underuse of a medicine • Overuse of a medicine • Use of inappropriate medicines (including therapeutic
duplication) • Adverse drug reactions, including interactions (drug-drug, drug-
disease, drug-nutrient, drug-laboratory test) • Non-adherence to therapy.86
Medicines list Prepared by a clinician, a medicines list contains, at a minimum: • All medicines a patient is taking, including over-the counter,
complementary, prescription and non-prescription medicines. For each medicine, the medicine name, form, strength and directions for use must be included87
• Any medicines that should not be taken by the patient, including those causing allergies and adverse drug reactions. For each allergy or adverse drug reaction, the medicine name, the reaction type and the date on which the reaction was experienced should be included.
Ideally, a medicines list also includes the intended use (indication) for each medicine. It is expected that the medicines list is updated and correct at the time of transfer (including clinical handover) or when services cease, and that it is tailored to the audience for whom it is intended (i.e. patient or clinician).50
Pharmaceutical treatment See ‘medicine’.
Pharmacological prophylaxis
See ‘medicine’.
Post-thrombotic syndrome Chronic pain, selling, and occasional ulceration of the skin of the leg that occurs as a consequence of previous venous thrombosis.15 Also known as post-phlebitic syndrome.
Prevention Care that is provided to reduce the risk of developing VTE.
Primary care The first level of care or entry point to the health care system, such as general practice clinics, community health practice (for example, clinics, outreach or home visiting services), ambulance services, pharmacists, or services for specific populations (for example Aboriginal or refugee health services).
Prophylaxis A measure taken for the prevention of a disease.15
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 30
Pulmonary embolism (PE) A blood clot that breaks off from the deep veins and travels round the circulation to block the pulmonary arteries (arteries in the lung). Most deaths arising from DVT are caused by PE.15
Pulmonary hypertension Abnormally elevated blood pressure in lung arteries.
Quality improvement The combined efforts of the workforce and others, including consumers, patients and their families, researchers, planners and educators – to make changes that will lead to better patient outcomes (health), better system performance (care) and better professional development. Quality improvement activities may be undertaken in sequence, intermittently, or on a continuous basis.86 Numerous models can be used, all sharing the same focus to reduce errors and unnecessary morbidity and mortality.
Quality of life The general well-being of a person in terms of health, comfort, functional status and happiness.
Risk factor A characteristic, condition, or behaviour that increases the possibility of disease, injury, or loss of well-being.88
Risk assessment Assessment, analysis and management of risks. It involves recognizing which event may lead to harm in the future, and minimising their likelihood and consequence.86
Shared decision-making A consultation process in which a clinician and a patient jointly participate in make a health decision, having discussed the options and their benefits and harms, and having considered the patient’s values, preferences, and circumstances.86
Side effects Unintended effects from a medicine or treatment.89
Significantly reduced mobility
Patients who are bedbound, unable to walk unaided or likely to spend a substantial proportion of the day in bed or in a chair.15
System The resources, policies, processes and procedures that are organised, integrated, regulated and administered to provide health care. Systems enable the objectives of healthcare standards to be accomplished by addressing risk management, governance, operational processes and procedures, implementation and training, and by influencing behavior change to encourage compliance.50
Thrombophilia The genetic or acquired prothrombotic states that increases the tendency to venous thromboembolism. It is a condition which leads to a tendency for a person’s blood to clot inappropriately.15
Thrombosis The formation of a blood clot in a blood vessel.
Thrombus A stationary blood clot along the wall of a blood vessel, causing obstruction of the vessel.90
Veins Vessels that return blood from tissues towards to lungs.
Venous thromboembolism (VTE)
The blocking of a blood vessel by a clot dislodged from its site of origin. It includes both DVT and PE.15
Venous thrombosis A condition in which a blood clot (thrombus) forms in a vein.15
VTE-related complications Bleeding, thrombosis and adverse events related to the use or misuse of VTE prophylaxis.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 31
References 1. Heit JA. Epidemiology of venous thromboembolism. Nature Reviews Cardiology. 2015;12(8):464-74. 2. Access Economics Pty Ltd for the Australia and New Zealand working party on the management and prevention of venous thromboembolism. The burden of venous thromboembolism in Australia, 1 May 2008. Access Economics Pty Ltd; 2008; Available from: https://www.deloitteaccesseconomics.com.au/uploads/File/The%20burden%20of%20VTE%20in%20Australia.pdf. 3. Heit JA, Melton LJ, III, Lohse CM, Petterson TM, Silverstein MD, Mohr DN, et al. Incidence of Venous Thromboembolism in Hospitalized Patients vs Community Residents. Mayo Clinic Proceedings. 2001;76(11):1102-10. 4. Slawomirski L, A. Auraaen, Klazinga N. The economics of patient safety. Paris: OECD Publishing; 2017; Available from: http://dx.doi.org/10.1787/5a9858cd-en. 5. Rahme E, Dasgupta K, Burman M, Yin H, Bernatsky S, Berry G, et al. Postdischarge thromboprophylaxis and mortality risk after hip-or knee-replacement surgery. CMAJ : Canadian Medical Association Journal. 2008;178(12):1545-54. 6. Spencer FA, Lessard D, Emery C, Reed G, Goldberg RJ. Venous Thromboembolism in the Outpatient Setting. Archives of Internal Medicine. 2007;167(14):1471-5. 7. White RH, Romano PS, Zhou H, Rodrigo J, Bargar W. Incidence and time course of thromboembolic outcomes following total hip or knee arthroplasty. Archives of Internal Medicine. 1998;158(14):1525-31. 8. Chapman N, Brighton T, Harris M, Caplan G, Braithwaite J, Chong B. Venous thromboembolism Management in general practice. Australian Family Physician. 2009;38:36-40. 9. Agnelli G. Prevention of venous thromboembolism in surgical patients. Circulation. 2004;110(24 Suppl 1):IV4-12. 10. Assareh H, Chen J, Ou L, Hillman K, Flabouris A. Incidences and variations of hospital acquired venous thromboembolism in Australian hospitals: a population-based study. BMC Health Services Research. 2016;16:511. 11. Kahn SR, Morrison DR, Cohen JM, Emed J, Tagalakis V, Roussin A, et al. Interventions for implementation of thromboprophylaxis in hospitalized medical and surgical patients at risk for venous thromboembolism. Cochrane Database Syst Rev. 2013;16(7). 12. Piazza G, Fanikos J, Zayaruzny M, Goldhaber SZ. Venous thromboembolic events in hospitalised medical patients. Thromb Haemost. 2009;102(3):505-10. 13. Maynard G. Preventing hospital-associated venous thromboembolism: a guide for effective quality improvement, 2nd ed. Rockville, MD: Agency for Healthcare Research and Quality; August 2016. ARHQ Publication No. 16-0001-EF; Available from: http://www.ahrq.gov/professionals/quality-patient-safety/patient-safety-resources/resources/vtguide/index.html. 14. Maynard G, Jenkins IH, Merli GJ. Venous thromboembolism prevention guidelines for medical inpatients: mind the (implementation) gap. J Hosp Med. 2013;8(10):582-8. 15. National Institute for Health and Care Excellence. Venous thromboembolism: reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital. CG 92. London: NICE; 2010 (updated June 2015); Available from: https://www.nice.org.uk/Guidance/cg92. 16. Scottish Intercollegiate Guidelines Network (SIGN). Prevention and management of venous thromboembolism. Edinburgh: SIGN; 2010. (SIGN publication no. 122); Available from: http://www.sign.co.uk. 17. Wickham N, Gallus AS, Walters BN, Wilson A. Prevention of venous thromboembolism in patients admitted to Australian hospitals: summary of National Health and Medical Research Council clinical practice guideline. Intern Med J. 2012;42(6):698-708. 18. Anderson FA, Jr., Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I9-16.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 32
19. Cushman M. Epidemiology and Risk Factors for Venous Thrombosis. Seminars in Hematology. 2007;44(2):62-9. 20. Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, et al. Prevention of VTE in orthopedic surgery patients: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2_suppl):e278S-e325S. 21. Kucher N, Tapson VF, Goldhaber SZ. Risk factors associated with symptomatic pulmonary embolism in a large cohort of deep vein thrombosis patients. Thromb Haemost. 2005;93(3):494-8. 22. NSW Ministry of Health. Policy Directive: Prevention of venous thromboembolism. Sydney: NSW Ministry of Health; 2014; Available from: http://www0.health.nsw.gov.au/policies/pd/2014/pdf/PD2014_032.pdf. 23. NSW Therapeutic Advisory Group Inc. Safe use of heparins and oral anticoagulants for venous thromboembolism prophylaxis in adults. Position Statement. Sydney: NSW Therapeutic Advisory Group Inc; 2010; Available from: http://www.ciap.health.nsw.gov.au/nswtag/documents/publications/position-statements/heparin-vte-aug-2010.pdf. 24. Geerts W. Prevention of venous thromboembolism: a key patient safety priority. J Thromb Haemost. 2009;1:1-8. 25. Cardiology Expert Group. Therapeutic Guidelines: Cardiovascular version 6. Melbourne: Therapeutic Guidelines Limited; 2012. 26. Australian Commission on Safety and Quality in Health Care. Medication safety alerts and notices. 2017 [cited Jul 2017]; Available from: https://www.safetyandquality.gov.au/our-work/medication-safety/high-risk-medicines/. 27. NSW Ministry of Health. High-risk medicines management policy. Sydney: NSW Ministry of Health; 2015; Available from: http://www1.health.nsw.gov.au/pds/ActivePDSDocuments/PD2015_029.pdf. 28. Institute of Safe Medication Practices. ISMP List of High-Alert Medications in Acute Care Settings. ISMP; 2014; Available from: http://www.ismp.org/Tools/highalertmedications.pdf. 29. Therapeutic Goods Administration. Department of Health. Apixaban (Eliquis), dabigatran (Pradaxa) and rivaroxaban (Xarelto): Information for health professionals. 2015 [cited Jul 2017]; Available from: https://www.tga.gov.au/alert/apixaban-eliquis-dabigatran-pradaxa-and-rivaroxaban-xarelto-information-health-professionals. 30. Therapeutic Goods Administration. Department of Health. Dabigatran (Pradaxa) and risk of bleeding: information for health professionals. 2013 [cited Jul 2017]; Available from: https://www.tga.gov.au/alert/dabigatran-pradaxa-and-risk-bleeding-information-health-professionals. 31. American Academy of Orthopaedic Surgeons. Preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. Evidence-based guideline and evidence report. Rosemont, IL: AAOS; 2011; Available from: http://www.orthoguidelines.org/topic?id=1006. 32. The Arthroplasty Society of Australia on behalf of the Australian Orthopaedic Association. Guidelines for VTE prophylaxis for hip and knee arthroplasty. AOA; 2016; Available from: https://www.aoa.org.au/docs/default-source/states/arthroplasty-vte-guidelines-2016.pdf?sfvrsn=2 33. Clinical Excellence Commission. Safer systems better care - Quality Systems Assessment statewide report 2013. Sydney: Clinical Excellence Commission; 2014; Available from: http://www.cec.health.nsw.gov.au/__data/assets/pdf_file/0007/258685/hs14-020-cec-qsa-report-dv3.pdf. 34. NSW Agency for Clinical Innovation. Improving prescription of venous thromboembolism prophylaxis in admitted medical patients. [cited October 2016]; Available from: https://www.aci.health.nsw.gov.au/ie/projects/improving-prescription-of-vte-prophylaxis.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 33
35. Cohen AT, Tapson VF, Bergmann J-F, Goldhaber SZ, Kakkar AK, Deslandes B, et al. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. The Lancet. 2008;371(9610):387-94. 36. Kahn SR, Panju A, Geerts W, Pineo GF, Desjardins L, Turpie AG, et al. Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada. Thromb Res. 2007;119(2):145-55. 37. Tapson VF, Decousus H, Pini M, Chong BH, Froehlich JB, Monreal M, et al. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the International Medical Prevention Registry on Venous Thromboembolism. Chest. 2007;132(3):936-45. 38. National Institute for Health and Care Excellence. Venous thromboembolism in adults: reducing the risk in hospital. QS3. London: NICE; 2010; Available from: https://www.nice.org.uk/guidance/qs3. 39. Australian Nursing and Midwifery Federation (SA Branch). Best practice guidelines. 2016. 40. Gould MK, Garcia DA, Wren SM, Karanicolas PJ, Arcelus JI, Heit JA, et al. Prevention of VTE in Nonorthopedic Surgical Patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e227S-e77S. 41. Guyatt GH, Akl EA, Crowther M, Gutterman DD, Schuunemann HJ. Executive summary: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl). 42. Kahn SR, Lim W, Dunn AS, Cushman M, Dentali F, Akl EA, et al. Prevention of VTE in Nonsurgical Patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e195S-e226S. 43. Qaseem A, Chou R, Humphrey LL, Starkey M, Shekelle P. Venous thromboembolism prophylaxis in hospitalized patients: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2011;155(9):625-32. 44. Royal College of Obstetricians & Gynaecologists. Reducing the risk of venous thromboembolism during pregnancy and puerperium. Green-top Guideline No. 37a. London, UK: RCOG Press; 2015 [cited July 2017]; Available from: https://www.rcog.org.uk/globalassets/documents/guidelines/gtg-37a.pdf. 45. Clinical Excellence Commission. Medication Safety and Quality VTE Prevention Centre. [cited October 2016]; Available from: http://cec.health.nsw.gov.au/patient-safety-programs/adult-patient-safety/vte-prevention. 46. Australian Commission on Safety and Quality in Health Care. Patient-centred care: Improving quality and safety through partnerships with patients and consumers. A discussion paper. Sydney: ACSQHC, 2011. 47. Australian Commission on Safety and Quality in Health Care. Windows into safety and quality. Sydney: ACSQHC, 2011. 48. Mitchell GK, Tieman JJ, Shelby-James TM. Multi-disciplinary care planning and teamwork in primary care. The Medical Journal of Australia.188(8 Suppl):S61-4. 49. Mitchell GK, Tieman JJ, Shelby-James TM. Multidisciplinary care planning and teamwork in primary care. The Medical journal of Australia. 2008;188(8 Suppl):S61-4. Epub 2008/06/17. 50. Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards. Sydney: ACSQHC, 2011. 51. Clinical Excellence Commission. Adult Venous Thromboembolism (VTE) Risk Assessment Tool. [cited January 2017]; Available from: http://cec.health.nsw.gov.au/__data/assets/pdf_file/0009/259515/adult_vte_risk_assessment_tool.pdf. 52. Clinical Excellence Commission. NSW Maternity Venous Thromboembolism Risk Assessment Tool. [cited July 2017]; Available
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 34
from: http://cec.health.nsw.gov.au/__data/assets/pdf_file/0006/362166/Maternity-Venous-Thromboembolism-VTE-Risk-Assessment-Tool-NH700088.pdf. 53. Department of Health. Risk Assessment for Venous Thromboembolism. March 2010. [cited January 2017]; Available from: http://webarchive.nationalarchives.gov.uk/20130123195034/http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_088215. 54. Caprini JA. Thrombosis Risk Assessment as a Guide to Quality Patient Care. Disease-a-Month. 2005;51(2):70-8. 55. Barbar S, Noventa F, Rossetto V, Ferrari A, Brandolin B, Perlati M, et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score. Journal of Thrombosis and Haemostasis. 2010;8(11):2450-7. 56. Parvizi J, Huang R, Rezapoor M, Bagheri B, Maltenfort MG. Individualized Risk Model for Venous Thromboembolism After Total Joint Arthroplasty. The Journal of Arthroplasty.31(9):180-6. 57. Australian Commission on Safety and Quality in Health Care, New South Wales Therapeutic Advisory Group Inc. National Quality Use of Medicines indicators for Australian hospitals. Sydney: ACSQHC; 2014; Available from: http://www.ciap.health.nsw.gov.au/nswtag/pages/indicators.html. 58. Queensland Government Department of Health. Venous thromboembolism (VTE) prophylaxis in pregnancy and the puerperium. Queensland: Queensland Health; 2014; Available from: https://www.health.qld.gov.au/qcg/documents/g-vte.pdf. 59. Tooher R, Middleton P, Pham C, Fitridge R, Rowe S, Babidge W, et al. A Systematic Review of Strategies to Improve Prophylaxis for Venous Thromboembolism in Hospitals. Annals of Surgery. 2005;241(3):397-415. 60. Australian Medicines Handbook 2017 (online). Adelaide: Australian Medicines Handbook Pty Ltd; 2017; July; Available from: https://amhonline.amh.net.au/. 61. New Zealand VTE Prevention. National Policy Framework: VTE prevention in adult hospitalised patients in NZ. New Zealand: NZVTEP; 2012; Available from: http://www.hqsc.govt.nz/our-programmes/other-topics/publications-and-resources/publication/654/. 62. Nicolaides AN, Fareed J, Kakkar AK, Comerota AJ, Goldhaber SZ, Hull R, et al. Prevention and treatment of venous thromboembolism--International Consensus Statement. Int Angiol. 2013;32(2):111-260. 63. Edmonds MJ, Crichton TJ, Runciman WB, Pradhan M. Evidence-based risk factors for postoperative deep vein thrombosis. ANZ journal of surgery. 2004;74(12):1082-97. 64. Heit JA, O'Fallon WM, Petterson TM, Lohse CM, Silverstein MD, Mohr DN, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med. 2002;162(11):1245-8. 65. Heit JA, Silverstein MD, Mohr DN, Petterson TM, O'Fallon W, Melton L, et al. Risk factors for deep vein thrombosis and pulmonary embolism: A population-based case-control study. Archives of Internal Medicine. 2000;160(6):809-15. 66. Pedersen AB, Sorensen HT, Mehnert F, Overgaard S, Johnsen SP. Risk Factors for Venous Thromboembolism in Patients Undergoing Total Hip Replacement and Receiving Routine Thromboprophylaxis. JBJS. 2010;92(12):2156-64. 67. T Rocha A, F Paiva E, Lichtenstein A, Milani R, Cavalheiro-Filho C, H Maffei F. Risk-assessment algorithm and recommendations for venous thromboembolism prophylaxis in medical patients. Vascular Health and Risk Management. 2007;3(4):533-53. 68. Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJGM, Lip GYH. A Novel User-Friendly Score (HAS-BLED) To Assess 1-Year Risk of Major Bleeding in Patients With Atrial Fibrillation. Chest.138(5):1093-100. 69. National Blood Authority Australia. Preoperative bleeding risk assessment tool: guidance for Australian health providers. Canberra: National Blood Authority Australia; 2015; Available from: https://www.blood.gov.au/preoperative-bleeding-risk-assessment-and-intervention-resource.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 35
70. Queensland Government Department of Health. Patient Safety Notice: Anticoagulation management. Patient Safety and Quality Improvement Service, Queensland Government Department of Health; 2017; Available from: http://qheps.health.qld.gov.au/psu/alerts/default.htm. 71. The Joint Commission. Discharge instructions/education materials for venous thromboembolism (VTE): a comprehensive approach to medication management compendium of resources. USA [cited July 2017]; Available from: https://www.jointcommission.org/discharge_instructions_for_venous_thromboembolism_vte/. 72. Padron M, Miyares MA, Ferrell KW, Hill AM. Development of an Anticoagulation Stewardship Program at a Large Tertiary Care Academic Institution. Journal of Pharmacy Practice. 2013;28(1):93-8. 73. Australian Commission on Safety and Quality in Health Care (2017). Top tips for safe health care. ACSQHC; Available from: https://www.safetyandquality.gov.au/publications/top-tips-for-safer-health-care/. 74. Horwitz LI. Self-care after hospital discharge: knowledge is not enough. BMJ Quality Safety. 2016;26(1):7. 75. Australian Commission on Safety and Quality in Health Care 2012. Accreditation outcome results and evidence of implementation of the National Safety and Quality Health Service (NSQHS) Standards. ACSQHC: Sydney. 76. Buckinghamshire Healthcare NHS Trust/Aylesbury Vale and Chiltern Clinical Commissioning Groups. Guideline 295FM.2 Dabigatran, rivaroxaban, apixaban and endoxaban for deep vein thrombosis and pulmonary embolism - amber initiation guide V2. Buckinghamshire Healthcare: NHS Trust; 2014 (updated 2016); Available from: http://www.bucksformulary.nhs.uk/docs/Guideline_295FM.pdf. 77. Pfizer. Heparin Sodium Injection. Product information. Jan 2013. 78. Therapeutic Goods Administration. Overview of adverse events. Department of Health; [cited July 2017]; Available from: https://www.tga.gov.au/reporting-adverse-events. 79. The Free Dictionary. Farlex; [cited March 2016]; Available from: http://medical-dictionary.thefreedictionary.com/assessment. 80. National Health and Medical Research Council. Blood Clots - Reducing your risk. National Health and Medical Research Council 2010 [Cited January 2016]; Available from: https://www.nhmrc.gov.au/guidelines-publications/cp125. 81. The High 5's Project Standard Operating Protocol for Medication Reconciliation. Assuring medication accuracy at transitions of care: medication reconciliation. World Health Organisation; 2014. 82. Australian Commission on Safety and Quality in Health Care. Health literacy:Taking action to improve safety and quality. Sydney: ACSQHC, 2014. 83. NPS Medicinewise. Complementary medicines. [cited June 2016]; Available from: http://www.nps.org.au/medicines/complementary-medicines. 84. Pharmaceutical Society of Australia. Practice guidelines for pharmacists providing Dose Administration Aid services. Deakin West, ACT: Pharmaceutical Society of Australia; 2017 [cited July 2017]; Available from: http://www.psa.org.au/wp-content/uploads/Practice-guidelines-for-pharmacists-providing-Dose-Administration-Aid-services-2017-pdf-7.2MB.pdf. 85. Australian Commission on Safety and Quality in Health Care. National consensus statement: essential elements for recognising and responding to clinical deterioration. Sydney: ACSQHC, 2010. 86. Australian Commission on Safety and Quality in Health Care. DRAFT National Safety and Quality Health Service Standards version 2. Sydney 2016. 87. Australian Pharmaceutical Advisory Council. Guiding principles to achieve continuity in medication management. Canberra: Commonwealth of Australia; 2005. 88. The Free Dictionary. Farlex; [cited November 2016]; Available from: http://www.thefreedictionary.com/risk+factor. 89. NPS Medicinewise. Glossary-side effects. [cited March 2016]; Available from: http://www.nps.org.au/glossary/side-effects.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 37
Acknowledgements Many individuals and organisations have freely given their time and expertise in the development of this document. In particular, the Commission wishes to thank the Venous Thromboembolism Clinical Care Standard Topic Working Group and other key experts who have given their time and advice. The involvement and willingness of all concerned to share their experience and expertise is greatly appreciated.
Members of the Venous Thromboembolism Clinical Care Standard Topic Working Group are: Associate Professor David Campbell, Professor Beng Hock Chong, Ms Helen Dowling, Mr Herbert Down, Professor Alexander Gallus, Ms Lillian George, Ms Glenda Gorrie, Dr Helen Harris, Associate Professor Wayne Hazell, Dr Corinne Mirkazemi, Ms Joanne Muller, Professor Harshal Nandurkar, Mr Rodney Neale, Dr Gary Nielsen, Professor Abdullah Omari, and Ms Tara Redemski.
Venous Thromboembolism Prevention Clinical Care Standard Consultation DraftV8.0 38
Level 5, 255 Elizabeth Street, Sydney NSW 2000 GPO Box 5480, Sydney NSW 2001











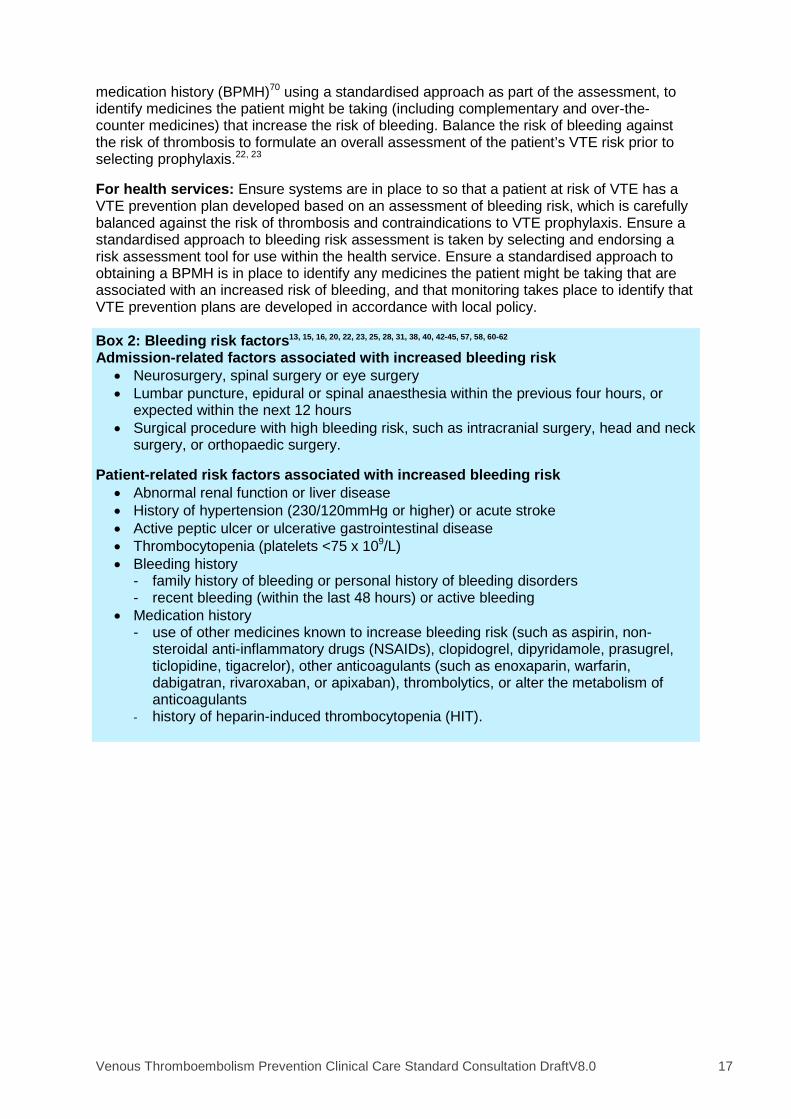




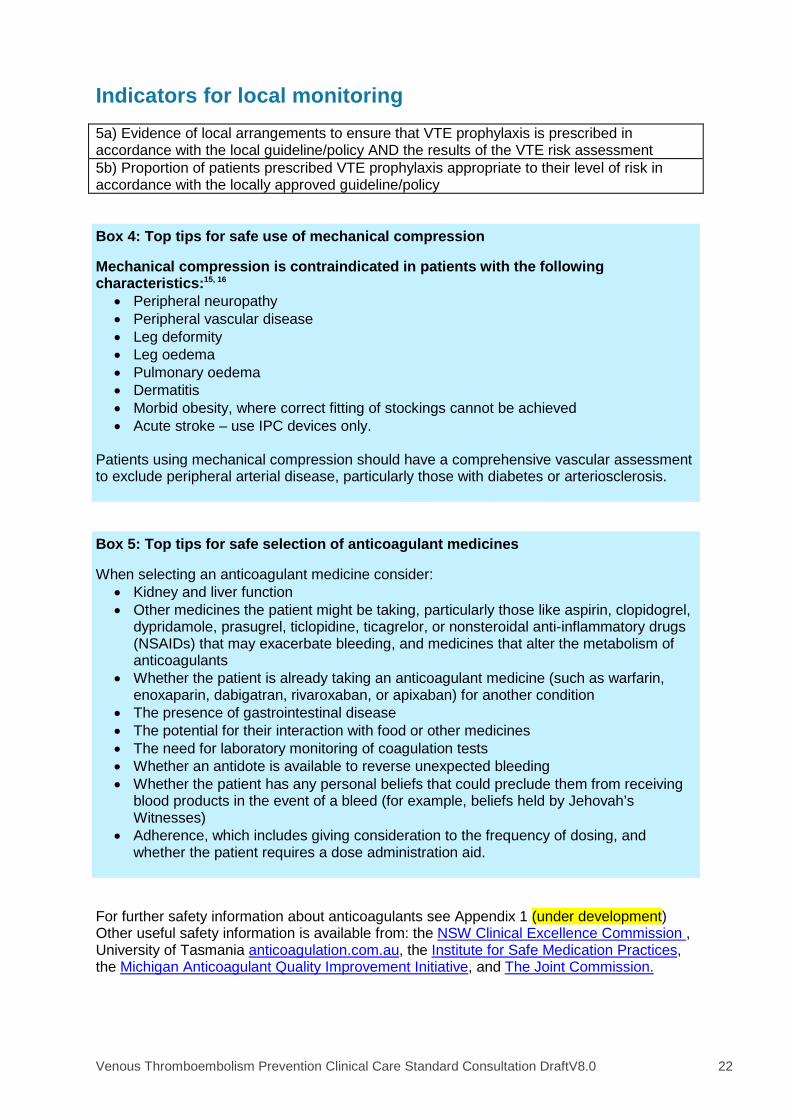


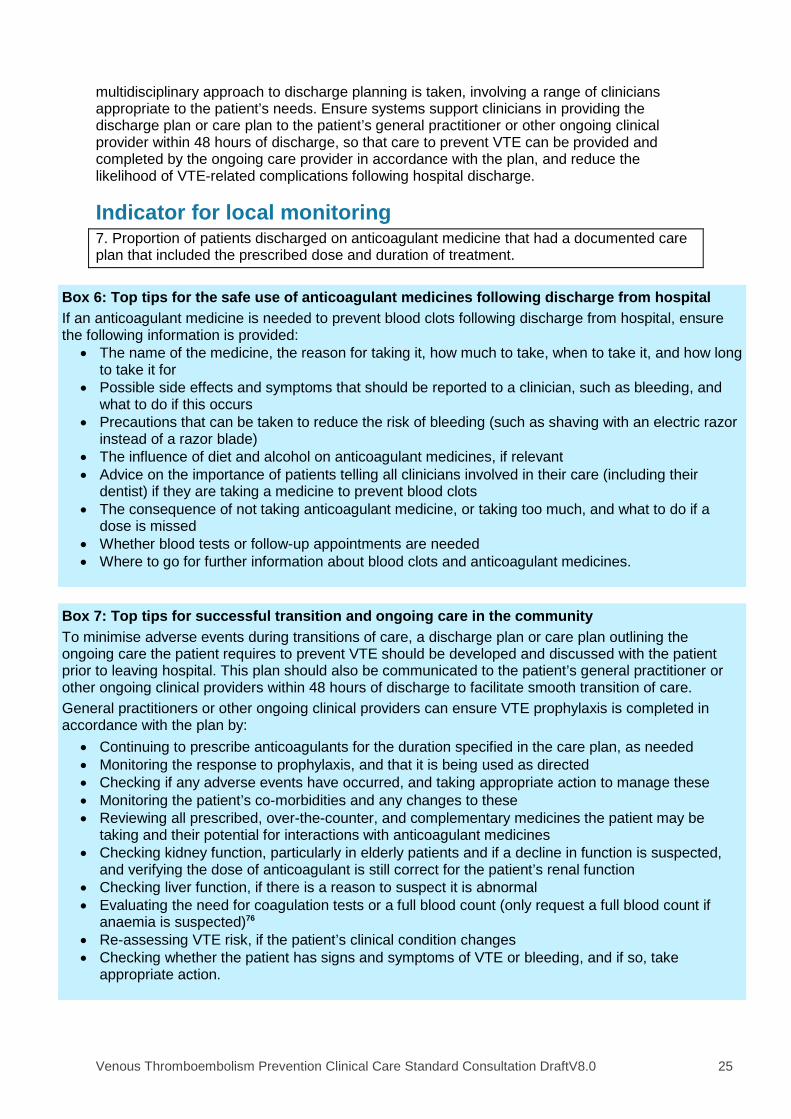



















![Mobile left atrial mass-clot or left atrial myxoma....mass includes thrombus, myxoma, lipoma and non-myxomatous neoplasm [7,8]. Among them, cardiac myxoma is the most common benign](https://static.documents.pub/doc/80x56/60fedab34ecd6d6c000feba7/mobile-left-atrial-mass-clot-or-left-atrial-mass-includes-thrombus-myxoma.jpg)







