36
Vincent [email protected]
Poliomyelitis
Polio (grey), myelon (marrow) = Greekitis (inflammation of) = Latin
“A common, acute viral disease characterized clinically by a brief febrile illness with sore throat, headache and vomiting, and often with stiffness of the neck and back. In many cases a lower neuron paralysis develops in the early days of illness”
—J.R. Paul, “Poliomyelitis (Infantile Paralysis)”, in A Textbook of Medicine, 1959.
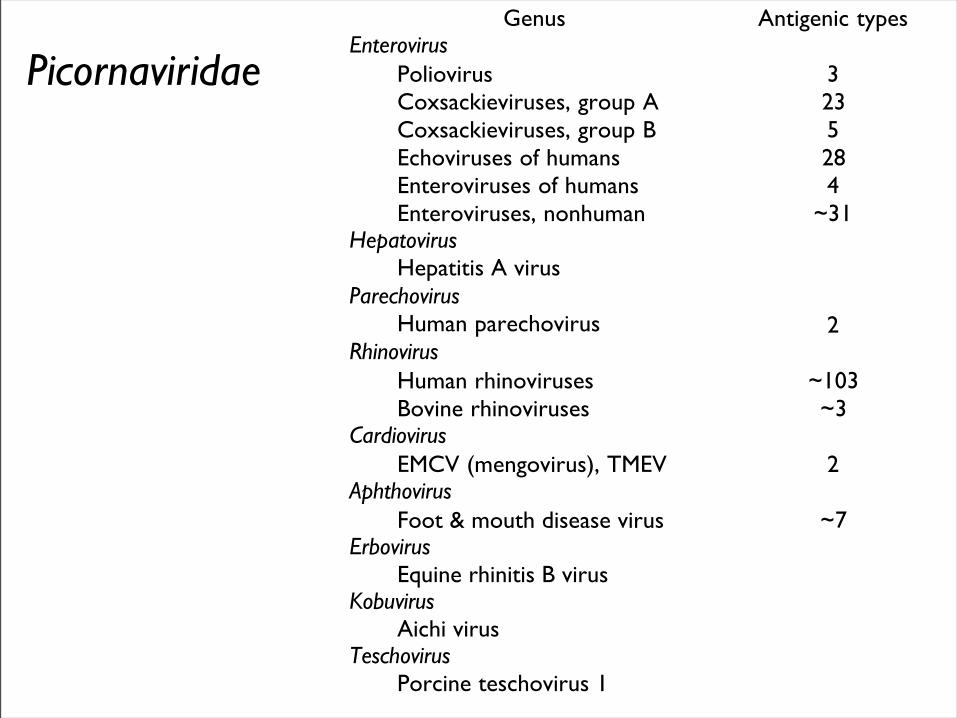
Genus Antigenic typesEnterovirus
Poliovirus 3Coxsackieviruses, group A 23Coxsackieviruses, group B 5Echoviruses of humans 28Enteroviruses of humans 4Enteroviruses, nonhuman ~31
HepatovirusHepatitis A virus
ParechovirusHuman parechovirus 2
RhinovirusHuman rhinoviruses ~103Bovine rhinoviruses ~3
CardiovirusEMCV (mengovirus), TMEV 2
AphthovirusFoot & mouth disease virus ~7
ErbovirusEquine rhinitis B virus
KobuvirusAichi virus
TeschovirusPorcine teschovirus 1
Picornaviridae
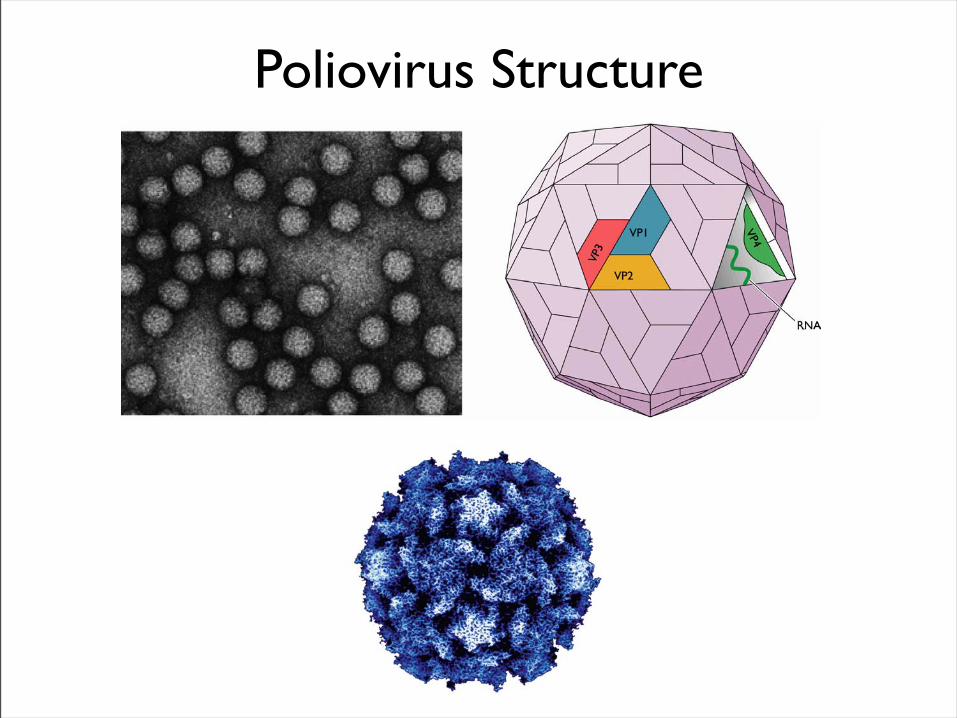
Poliovirus Structure
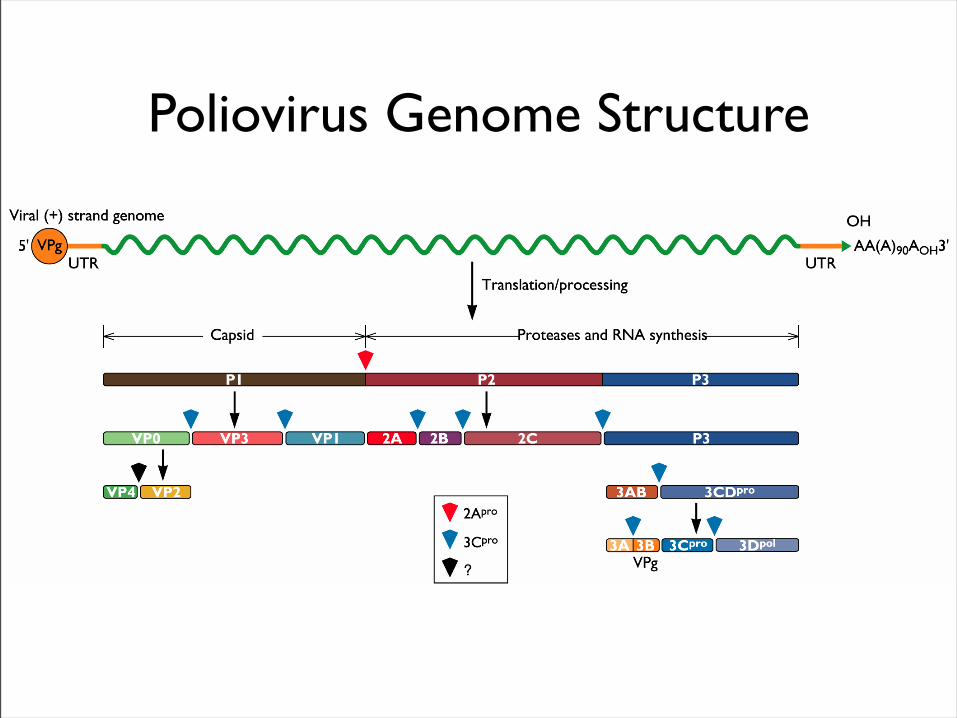
Poliovirus Genome Structure
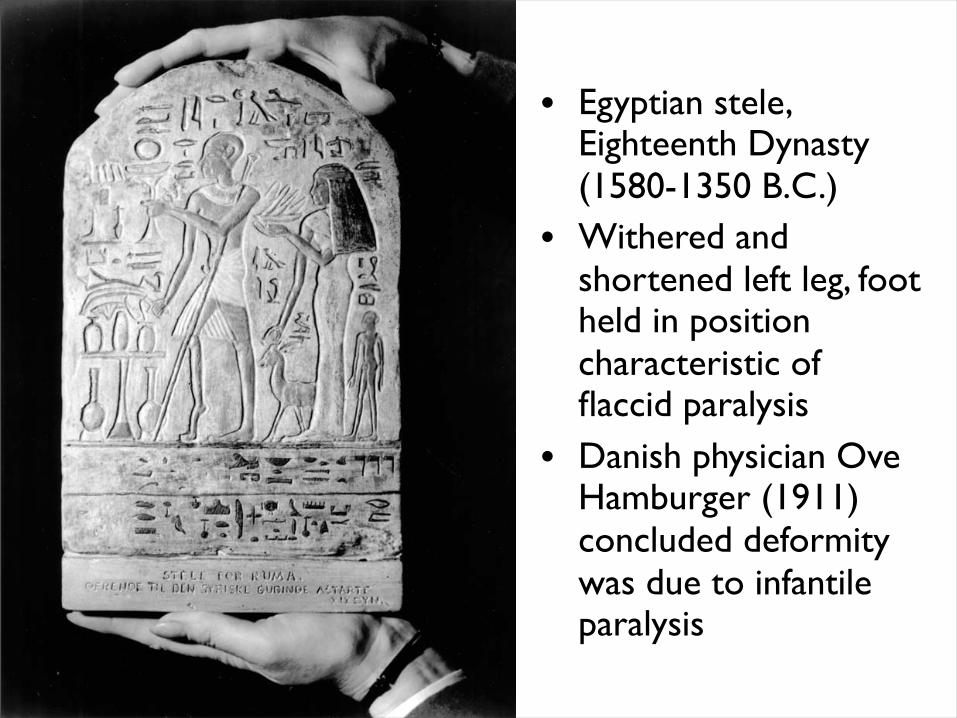
• Egyptian stele, Eighteenth Dynasty (1580-1350 B.C.)
• Withered and shortened left leg, foot held in position characteristic of flaccid paralysis
• Danish physician Ove Hamburger (1911) concluded deformity was due to infantile paralysis
• •First epidemics of poliomyelitis occurred in Sweden: 1868 (14 cases), 1881 (13 cases).
• •Rutland, Vermont, 1894 (132 cases)
• •New York City, 1907 (750 cases)
Epidemic poliomyelitis
Polio Research1908
• Karl Landsteiner isolates poliovirus in monkeys after injection with sterile filtrate from the spinal cord of a boy who had died of polio
1949
• Enders, Weller, Robbins grow poliovirus in cultures of human cells from non-nervous tissue. Replaces the monkey for detecting and studying poliovirus. Nobel Prize, 1954.
1954Francis clinical trial of Salk's formalin-killed poliovirus (IPV): 1,800,000 children. >50% protection; IPV licensed 12 April 1955.
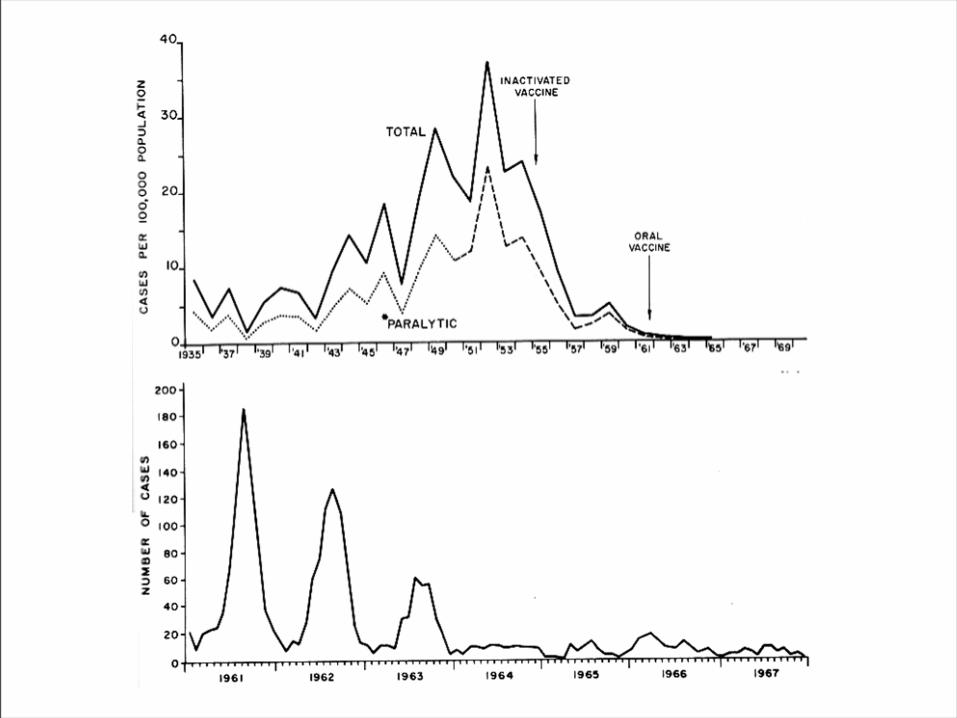
1955-1960Paralytic poliomyelitis fell from 20,000 cases/yr. to 2,500/yr.
1961Sabin's live, attenuated strains are licensed in the U.S. and replace IPV.
1979Last case of poliomyelitis (wild type virus) in U.S.
2000IPV replaces OPV in U.S.
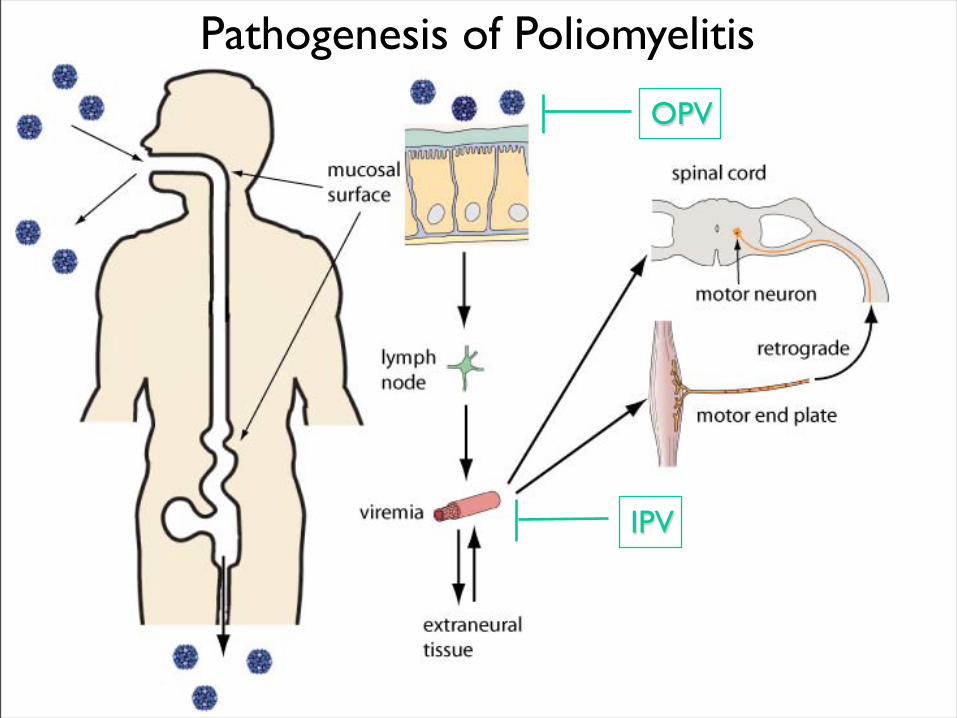
Pathogenesis of Poliomyelitis OPV
IPV
Pathogenesis of Poliomyelitis
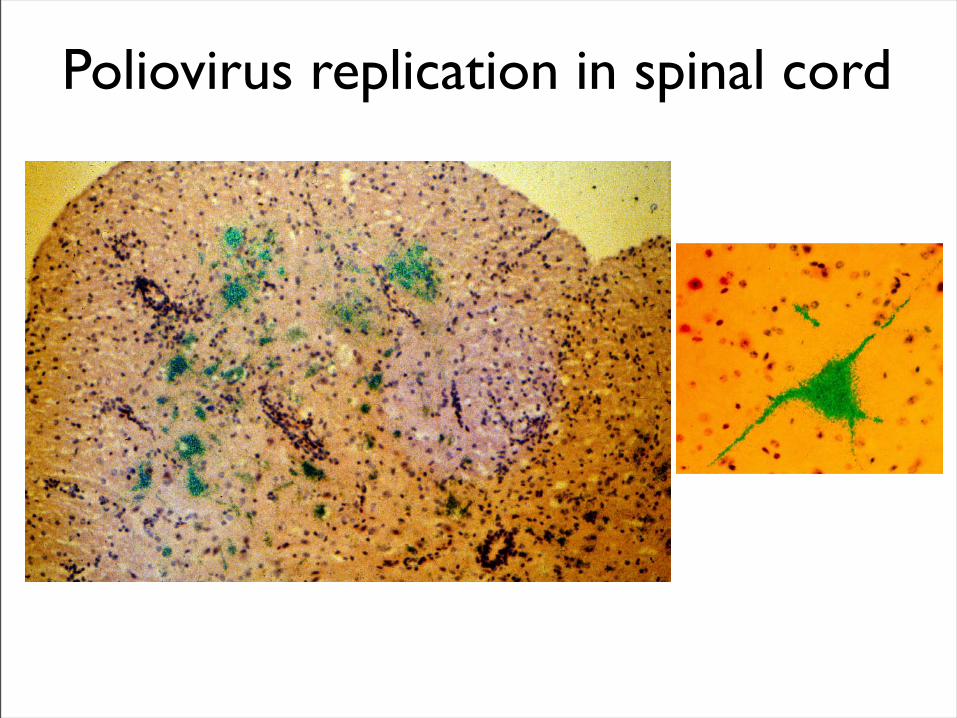
Poliovirus replication in spinal cord
Poliovirus vaccines• Inactivated poliovirus vaccine, IPV
– must be injected
– when properly prepared does not cause disease– does not produce intestinal immunity
– used 1955 - 1961 and 2000 - present in U.S.
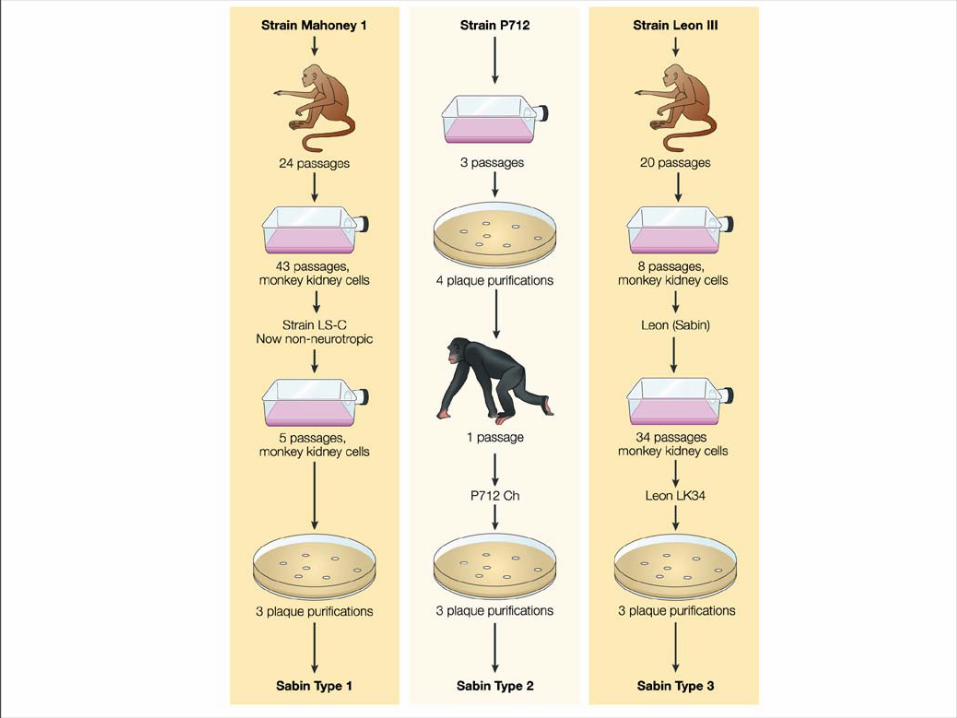
• Oral poliovirus vaccine, OPV– easy to administer– produces intestinal immunity
– mutant viruses empirically derived from virulent strains– usually reverts during intestinal replication
– used 1961 - 2000 in U.S.
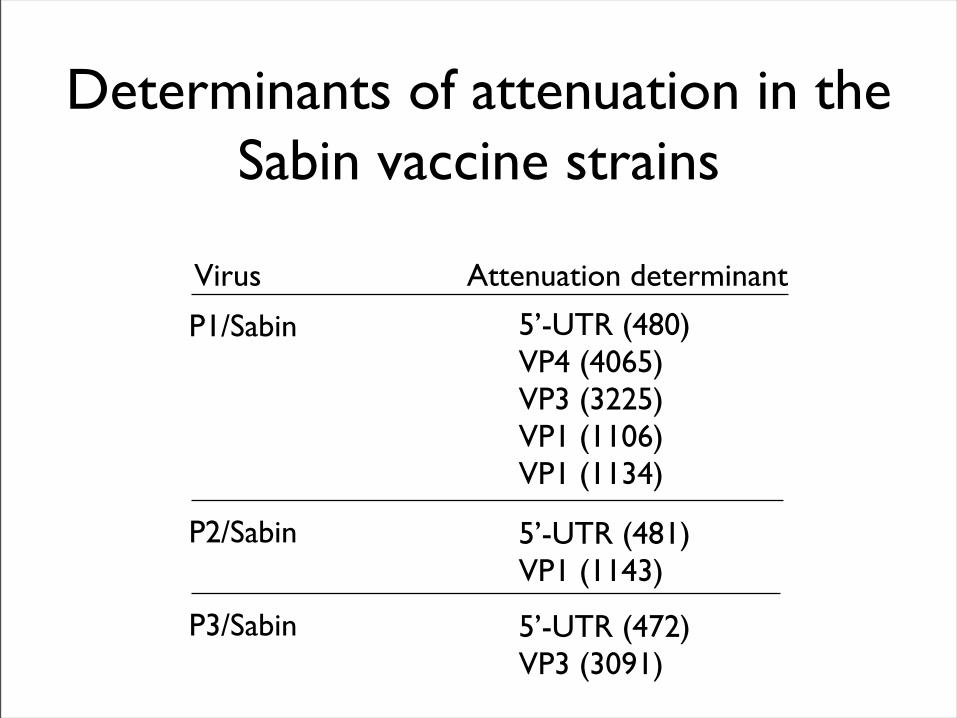
Determinants of attenuation in the Sabin vaccine strains
Virus Attenuation determinant
P1/Sabin
P2/Sabin
P3/Sabin
5’-UTR (480)VP4 (4065)VP3 (3225)VP1 (1106)VP1 (1134)
5’-UTR (481)VP1 (1143)
5’-UTR (472)VP3 (3091)
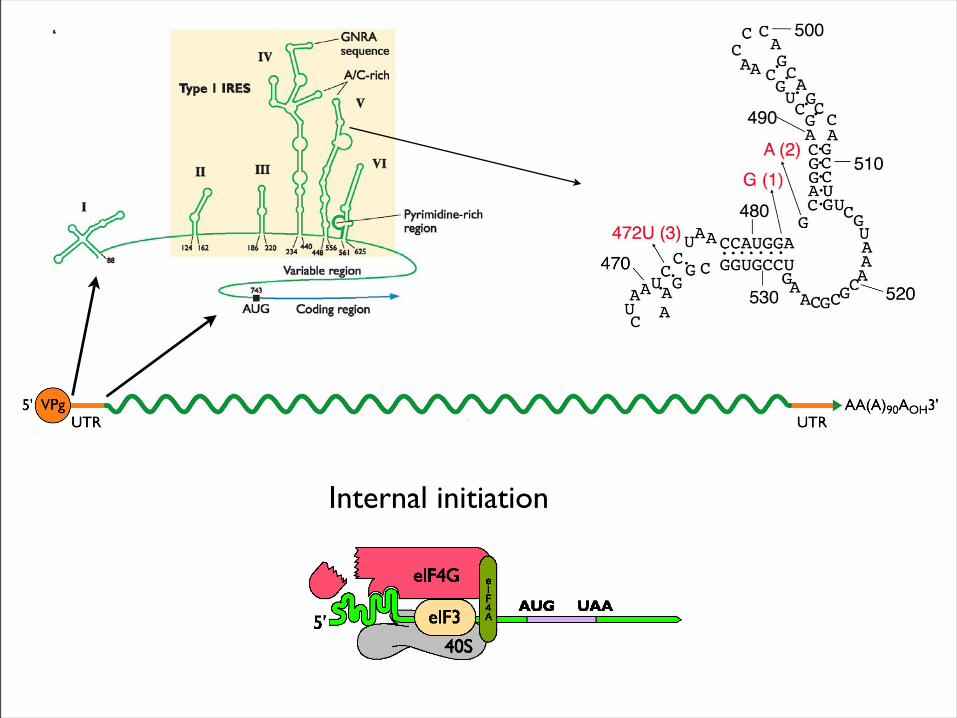
Internal initiation

CD155 Transgenic Mice
Viral growth in mouse brain
Viral growth in HeLa cells
472U
472C
PD50
9 x 103 pfu
>2 x 107 pfu
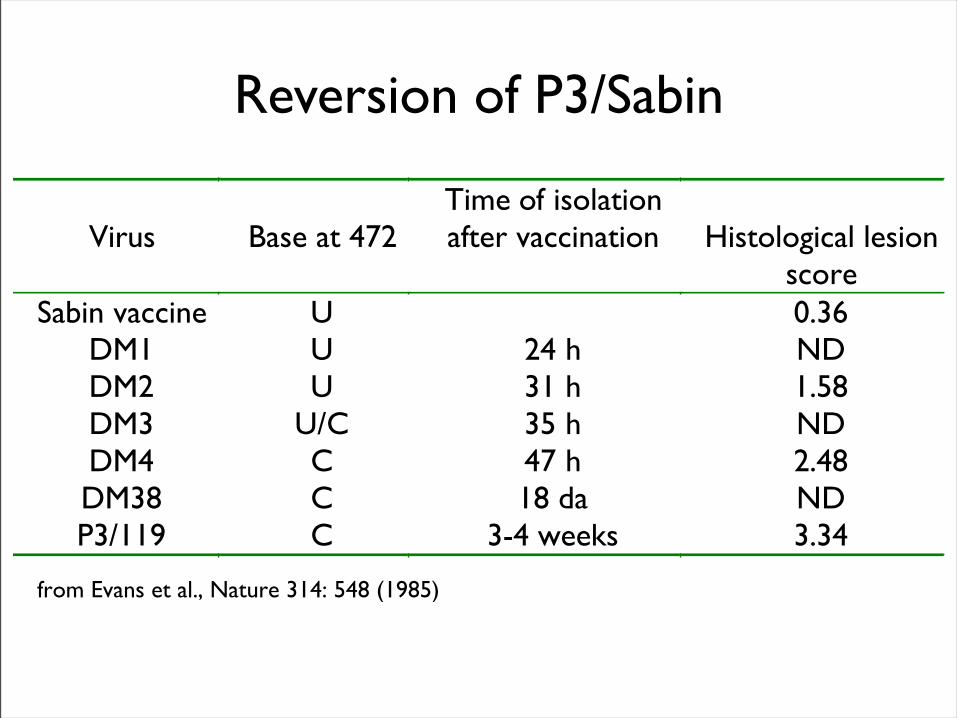
Virus Base at 472Time of isolationafter vaccination Histological lesion
scoreSabin vaccine U 0.36
DM1 U 24 h NDDM2 U 31 h 1.58DM3 U/C 35 h NDDM4 C 47 h 2.48DM38 C 18 da NDP3/119 C 3-4 weeks 3.34
from Evans et al., Nature 314: 548 (1985)
Reversion of P3/Sabin
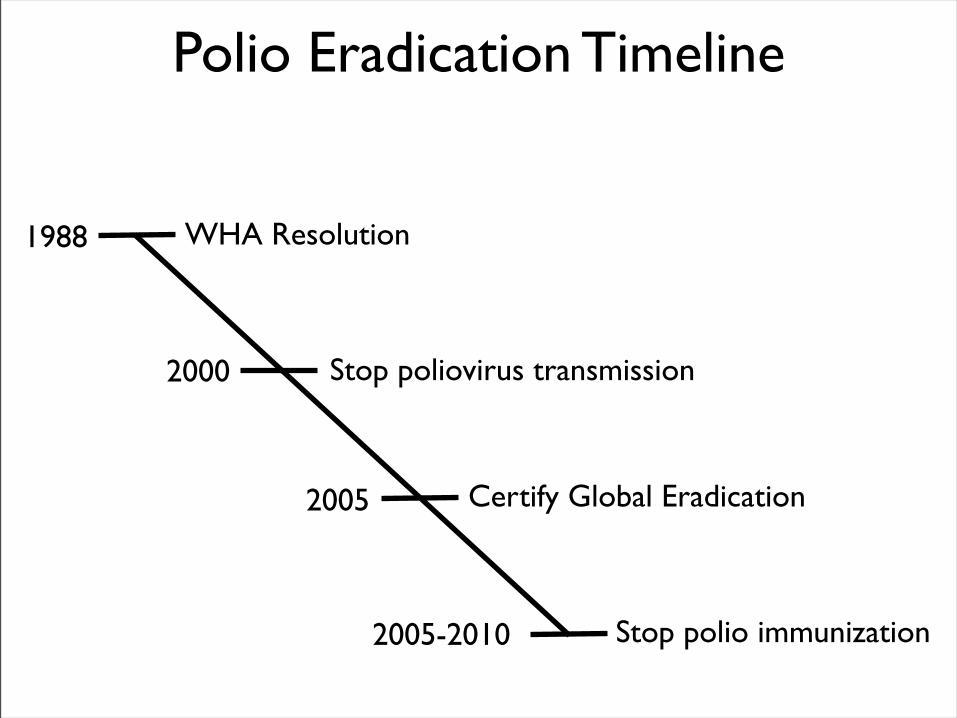
1988
2000
2005
2005-2010
WHA Resolution
Stop poliovirus transmission
Certify Global Eradication
Stop polio immunization
Polio Eradication Timeline
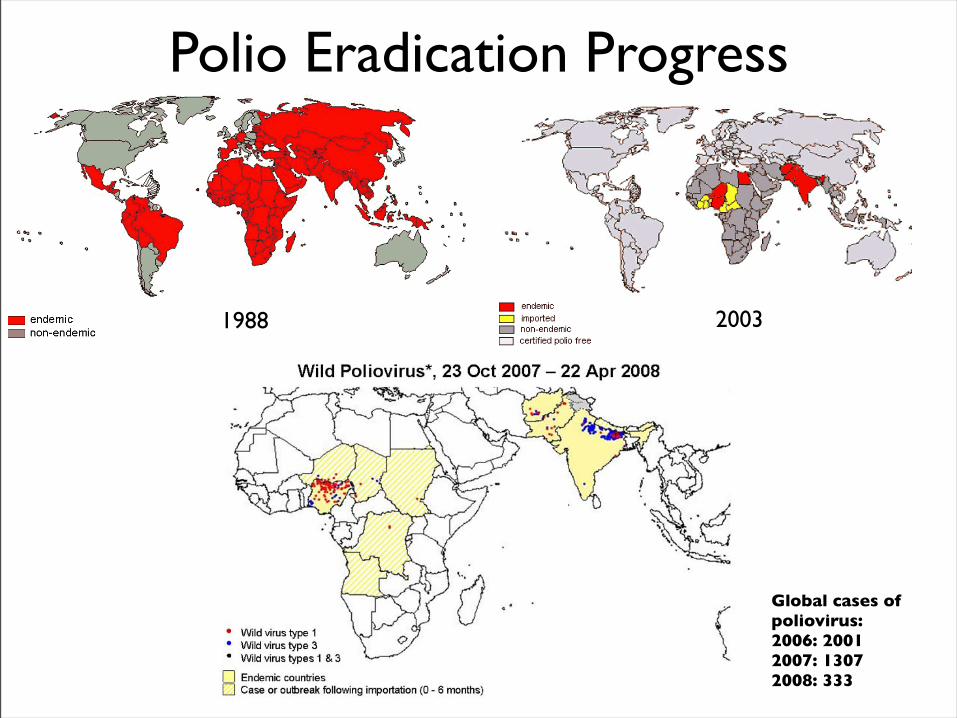
Polio Eradication Progress
1988 2003
Global cases of poliovirus: 2006: 20012007: 13072008: 333
Polio eradication
• In countries using OPV, only source of polio is the vaccine
• Therefore OPV use will cease in post-eradication period
• The plan to stop vaccination is based on the assumption that there are no non-human reservoirs of poliovirus, and circulation of attenuated strains and their derivatives (VDPV) is limited
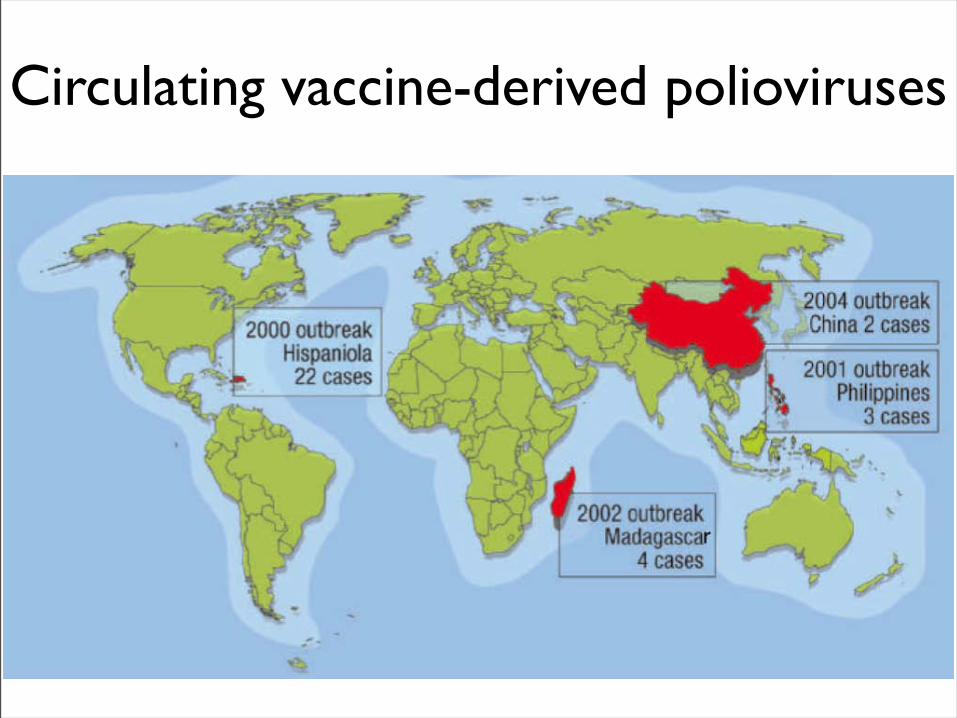
Circulating vaccine-derived polioviruses
• Recent outbreaks of poliomyelitis in Egypt, Dominican Republic/Haiti, Philippines, Madagascar caused by VDPV
• These VDPV strains regained virulence and spread in human populations
• Long-term persistence and excretion of VDPVs in immunocompromised persons
• These recent outbreaks demonstrate that neurovirulent revertants of OPV can circulate for years (even in immune populations) and cause poliomyelitis
Problems associated with VDPV
Minnesota, October 2005
• Poliovirus type 1 isolated from an unvaccinated, immunocompromised child (7 months old) in an Amish community in Long Prairie, MN
• Spread to four other children
• No paralytic disease associated with infections
• Isolates are VDPVs
OPV transmission
• Polio outbreaks caused by VAPP strains demonstrate that neurovirulent revertants of OPV can circulate for years (even in immune populations) and cause poliomyelitis
• These outbreaks mimic the situation that will occur when OPV usage is halted: circulation of neurovirulent revertants when vaccination coverage drops
• In light of this information, we cannot simply stop vaccinating
Vaccination against the vaccine
• After eradication, immunize globally with IPV (not infectious)
– Higher cost than OPV
– Not effective in tropical, underdeveloped countries
• Careful monitoring of environmental samples for poliovirus
• Virus in research laboratories (mislabeled?)
• Stored clinical and environmental samples
• Bioterrorism: Synthesis of infectious DNA readily done
• Elimination of all sources of poliovirus is impossible; assume an outbreak will occur
Why poliovaccine must be stockpiled after immunization ceases
Which vaccine should be stockpiled?
• IPV: noninfectious, no reintroduction of virus into the environment
• However, IPV is produced from virulent strains
• Poliovirus has escaped from vaccine-manufacturing plants at least twice
• mOPV
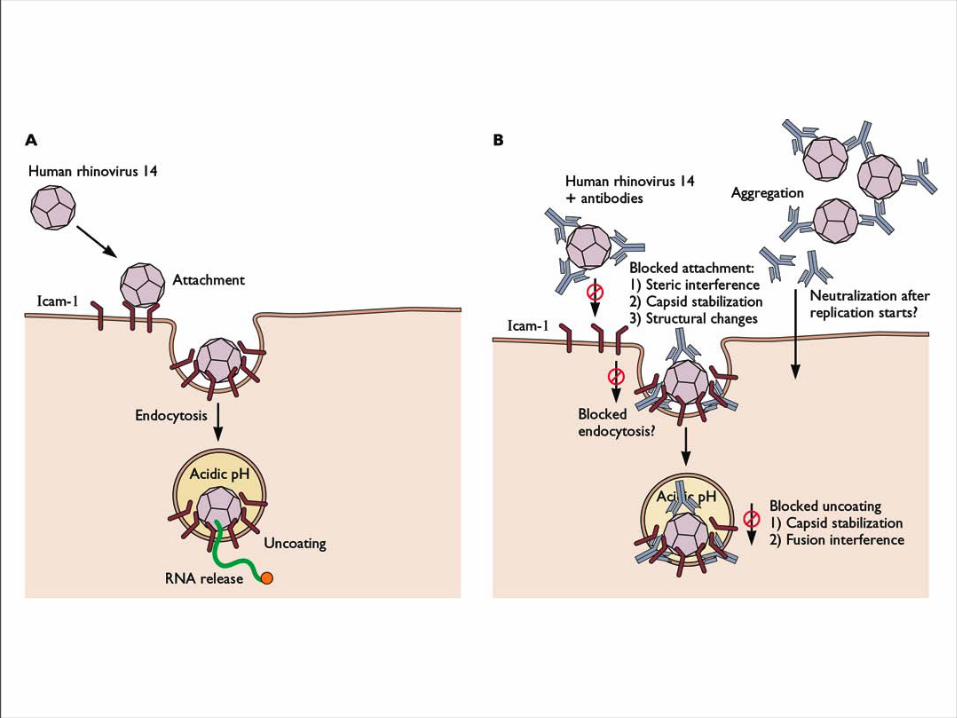
• Typical picornaviruses• Cell receptor is either
ICAM-1 (91 serotypes) or LDLR (10 serotypes)
• Cause half of all common colds, the most common infection of humans
Rhinovirus
Why do we care about the common cold?•Adults get 2-4 colds/yr; children 6-8/yr
•Yearly costs in US > $20 billion: OTC and Rx medicine, doctor visits, lost work days
•Complications include otitis media, sinusitis, serious lower tract infection, particularly in young children, elderly, immunocompromised, and with chronic disorders such as cystic fibrosis
•50-80% of all asthma attacks occur with respiratory infections, the majority being RVs; associated with asthma-induced mortality
•Upper respiratory tract infections are the most common cause of inappropriate antibiotic use, leading to resistant bacteria
•No effective treatments available
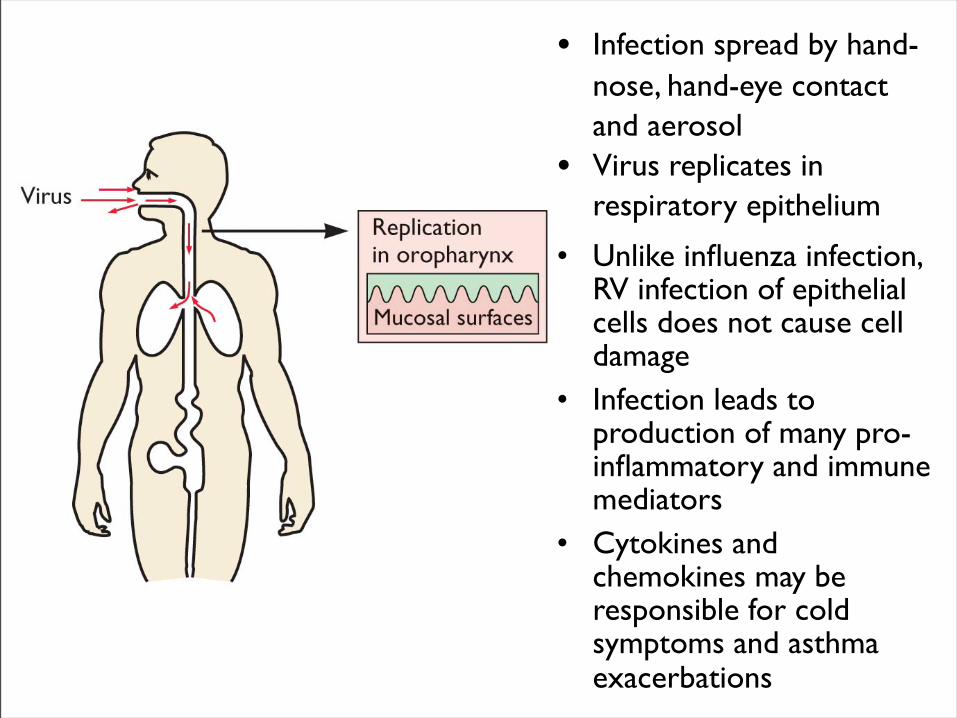
• Infection spread by hand-nose, hand-eye contact and aerosol
• Virus replicates in respiratory epithelium
• Unlike influenza infection, RV infection of epithelial cells does not cause cell damage
• Infection leads to production of many pro-inflammatory and immune mediators
• Cytokines and chemokines may be responsible for cold symptoms and asthma exacerbations
Prevention of rhinovirus infections
• Vaccines are not practical due to large number of viral serotypes
• Capsid-binding antiviral drugs (e.g. Pleconaril)
• Antiviral drugs against other viral targets (proteinases, RNA polymerase)
• Early diagnosis is essential for antiviral therapy - acute infections

















