Giving A Voice To Patient SafetIn New South Wales The Centre for Clinical Governance Research in Health undertakes strategic research, evaluations and research-based projects of national and international standing with a core interest to investigate health sector issues of policy, culture, systems, governance and leadership. CENTRE FOR CLINICAL GOVERNANCE RESEARCH
The Centre for Clinical Governance Research in Health undertakes strategic research, evaluations
and research-based projects of national and international standing with a core interest toinvestigate health sector issues of policy, culture, systems, governance and leadership.
This monograph is the nal in a series prepared by the Centre for Clinical Governance Research (CCGR)
at the University of New South Wales (UNSW) for the Clinical Excellence Commission (CEC). In the rst
two monographs, we reviewed the technical literature on patient safety (Hindle, Braithwaite and Iedema,
2005) and examined major Australian and international patient safety inquiries (Hindle, Braithwaite,
Travaglia and Iedema, 2006). The aim of the series is to shed light on what has become one of the most
important questions in health care practice and management: what do we know about patient safety and
what we can do about it?
This is a social scientic as opposed to a scientic study. We did not design a randomised trial or run an
experiment. Instead, we did something more simple, perhaps more telling: we asked people at the coalface
to talk to us about their concerns about patient safety, what they thought was being done well and what we
could do to make things better. It is very important to capture real life experiences and views in this way,
in order to understand what is going on in the health system from the standpoint of the stakeholder groups
themselves.
In this study we gathered the views of nurses, doctors, pharmacists, allied health professionals, academics
and managers in 30 focus groups across NSW. In total 195 people added their voice to the study. Some
participants were recent graduates; most were senior clinicians and executives. Some of the focus
groups came together as a single discipline; the majority was constituted in mixed groups. We explored
their experiences, sought their opinions about the causes of and possible solutions to breakdowns in
patient safety, and asked them what they thought it would take to achieve the goal of reducing errors and
improving safety for all patients. In answering these questions, participants provided valuable insights into
the ways in which signicant cultural change, leading to improved patient safety, might be achieved.
The information presented in this report shows that patient safety is a problem requiring cohesive and
coordinated solutions. Participants were strongly committed to the current direction and strategies for
addressing medical errors and adverse events, and believed that more work can and should be done.
There was a rm belief that patient safety problems occurred not so much as a result of individual error,
but rather as a result of a combination of poor communication, ineffective teamwork, cultural barriers and
inadequate or inappropriate resource management.
Participants had clear views about the role, and more especially the approach, that the CEC should take
within this context. The CEC, they felt, should take a proactive, strategic and consultative approach, andone which is inclusive of all stakeholders - patients, their carers and families, and health professionals.
In addition, participants thought that the central issues for patient safety were communication and workforce
and workload matters. There was strong support for current initiatives to improve the governance of the
health system, and provide responses to patient safety issues.
Giving a voice to patient safety in New South Wales
2 Introduction
2.1 Patientsafetyasacorehealthcareproblem
Sparked by a series of international inquiries and reports into medical errors and adverse events,
patient safety has become one of the dening movements in health care in the late 20th and early
21st centuries (Bleich, 2005). At all levels of health services including the World Health Organisation
(WHO), policy-makers, bureaucrats, managers and clinicians, there is concern about the causes
and rates of harm. Many people are committed to improving patient safety. Despite this commitment,
health systems, services and professionals are struggling to nd ways to reduce the incidence of
critical incidents and adverse events (Leape, Berwick, Bates, 2002; Watcher, 2004). This is proving
to be what is sometimes called a “wicked problem” – one that is resistant to policy efforts, and ishard to address (Rittel and Webber, 1973).
This monograph is the third in a series produced by CCGR for the CEC. In the rst two monographs,
we reviewed the technical literature on patient safety (Hindle, Braithwaite and Iedema, 2005) and
examined major Australian and international patient safety inquiries (Hindle, Braithwaite, Travaglia
and Iedema, 2006). The aim of the series is to shed light on what has become one of the most
important questions in health care practice and management: what do we know about patient safety
and what can we do about it?
In this monograph we examine some of the human dimensions of this issue. In order to understand
and respond to the causes and consequences of adverse events, it is vital for us to document the
experiences and concerns of health professionals who are, along with patients, at the centre of theincidents causing harm and the efforts to prevent them (Wu, 2000). This has become particularly
important since reviews of patient safety over the last ve years have come to the same conclusion:
progress has been made, but it is limited, patchy and slow, and signicant developments in both
research and practice are required (Watcher, 2004; Bleich, 2005; Longo, Hewett, Ge and Schubert,
Forsyth, Jorm and Pawsey, in press; Iedema, Jorm, Long, Braithwaite, Travaglia and Westbrook,
2006).
In addressing this fundamental question of why, after all that we know about the causes and
consequences of patient harm, the rate of progress remains slow, Pauker, Zane and Salem (2005)
invoke the theory of constraints. Most individuals (and systems), they argue, resist change insome form or another. Factors can include difculties in negotiating what to do, politics, lack of
resources, insufcient training or poor implementation. In order to facilitate the desired change, six
key conditions must be met. There must be agreement: rst, that there is a problem; second, on its
duration; third that the proposed resolutions will actually solve or address it; fourth that initiatives
won’t introduce new problems; fth that it is possible to overcome any obstacles that have been
identied; and sixth, stakeholders must agree to implement the change. We add a seventh: that
progress must be evaluated.
The literature reviewed in the rst monograph of this series (Hindle, Braithwaite and Iedema,
2005) leaves no doubt as to the evidence for the scale of the problem. While there remain some
disagreements about the actual number of errors (Macdonald, Weiner and Hui, 2000; Leape,
2000) and the methods used to identify them (Vincent, 2003: Thomas and Petersen, 2003), it is
not feasible to deny that patient safety is a major concern over and above other technical and
procedural challenges to providing good care (Classen and Kilbridge, 2002). Although there is
O’Beirne, Palacios-Deringher, Reid, Sheps and Tamblyn, 2004).
2.2 Tacklingpatientsafety
The direction of the solutions to the problem, and agreement that the proposed solutions will
be more effective and will not introduce additional problems, is more difcult to determine.
As responses to patient safety proliferate it becomes more, rather than less, difcult to gain
consensus about what should be done, when by whom, and why (Braithwaite, Westbrook and
Iedema, 2005).
What has become evident in recent years is that the complexity of the patient safety problem
requires a comprehensive and concerted, longitudinal approach (Braithwaite, Travaglia,
Westbrook, Jorm, Hunter, Carroll, Iedema, Ekambareshwar, 2006). Current research points
to the need for a combination of approaches: organisational, technological, educational, and
cultural (Braithwaite, Westbrook, Travaglia, Iedema, Mallock, Long, Nugus, Forsyth, Jorm and
Pawsey, in press; Iedema, Jorm, Long, Braithwaite, Travaglia and Westbrook, 2006; Institute
of Medicine, 2001; Larson, 2002; Cohen, Kimmel, Benage, Hoang, Burroughs and Roth, 2004;
Amalberti, Aurory, Berwick and Barach, 2005; Institute of Medicine, 2000; Rosenthal and
Sutcliffe, 2002; Watcher, 2004) at four levels: systemic, organisational, team and individual(Ferlie and Shortell, 2001). This is why the CEC and its programs and projects aiming at
improving quality and safety in multiple ways are so important.
The second monograph in this series (Hindle, Braithwaite, Travaglia and Iedema, 2006) provides
some insights into the obstacles involved in the implementation of patient safety programs. The
authors identied common features in health services that had experienced major breaches in
patient safety. These included: decient quality monitoring processes; the dismissal of concerns
raised by health care providers, patients and families over long periods of time prior to major
patient safety incidents; the ignoring and abuse of active critics of systems or services; decient
teamwork; and lack of involvement of patients and families as part of health care teams.
Various initiatives have been proposed to tackle patient safety. These include: system-wide
quality approaches (Institute of Medicine, 2000; Affonso and Doran, 2002; Ketring and White,
This literature provides signicant insights into the strategies and approaches which are currently
being employed to reduce errors and improve safety. This phase has been referred to as the “end
of the beginning” (Watcher, 2004). The next era of patient safety has been labelled, a little less
prosaically, as the “hard phase”. It is hard, because it will ask “… health professionals to change not
only their traditional ways of thinking and doing but their images of themselves ….” (Schyve, 2006).In other words, it will demand a signicant culture change from all health professionals, and the
active involvement of health care organisations, policy-makers, educators and other stakeholders
(Mccarthy and Blumenthal, 2006).
2.3 Givingavoicetopatientsafety
In this monograph we sought to give a voice to the health professionals who have lived through
the (at times tumultuous) end of the beginning and who are currently faced with transition to the
hard phase. We gathered the views of nurses, doctors, pharmacists, allied health professionals,
academics and managers in 30 focus groups across NSW. In total 195 people added their voice to
the study. Some participants were recent graduates; most were senior clinical staff and executives.Some of the focus groups came together as a single discipline; the majority was constituted in mixed
groups. We explored their experiences, sought their opinions about the causes of, and possible
solutions to, breakdowns in patient safety, and asked them what they thought it would take to
achieve the goal of reducing errors and improving safety for all patients.
In the monograph we report the major ndings and key themes from our study: what were
participants’ biggest concerns, that is, what kept them awake at night? Had their concerns changed
in recent years? Were there any groups that they felt were at higher risk than others in the health
care system? What were participants’ experiences of medical errors? What is the health system
currently doing well and what needs to be improved? What key factors need to be addressed to
continue improvements? If they could do one thing to improve patient safety, what would it be? Whatshould be the major focus of the Clinical Excellence Commission? The participants provided frank
and honest responses to what were, at times, difcult questions. Most importantly they provided
valuable insights into the ways in which signicant cultural change, leading to improved patient
Two sets of focus groups were conducted in order to sample views at different points in time.
The rst set, of 25 groups, was carried out in August and December 2004 by the three authors
from CCGR. Participants were recruited through the Area Health Services (AHSs) in NSW.
Contact was made via Patient Safety Ofcers in each AHS, who helped distribute information
(yers and emails) about the study and arrange suitable times and places for the groups. The
groups were conducted in three major cities in NSW (Sydney, Newcastle and Wollongong) and
in a number of locations, including hospitals, community health centres, ofces, and in one case
a University. Participants were drawn from AHSs, a state-wide health service, and two state-wide health advisory groups. A total of 171 individuals participated in the 2004 groups. Over two
years later the second set of ve focus groups was conducted in order to gauge any changes
in concerns and perceptions of health professionals. This work was conducted in March 2007.
Contact was made via Clinical Governance Units in each AHS. Three AHSs and three state-wide
services responded. The AHSs included both metropolitan and rural locations. Participants were
drawn from a variety of hospital, community health and geographic locations in each service. A
total of 24 participants participated in the 2007 study.
In both sets of focus groups participants came from a range of discipline backgrounds,
metropolitan and rural AHSs, and had different levels of seniority and experience. This was
a convenience sample of academic clinicians, allied health workers (including pharmacists,
physiotherapists, occupational therapists and social workers), nurses (both hospital and
community health), doctors, managers, executives, policy-makers and patient safety and quality
ofcers. We actively sought out a sample which would represent the diversity of professions and
experience in the current NSW health workforce. Participants did not receive payment for their
attendance at the focus groups, but where appropriate, morning or afternoon tea was provided.
For reasons of condentiality, individuals are not identied by name, organisation or AHS, in
either transcripts or this monograph. This requirement meets both ethics requirements and
expressed wishes of a number of participants. The studies were approved by UNSW’s Social
Giving a voice to patient safety in New South Wales
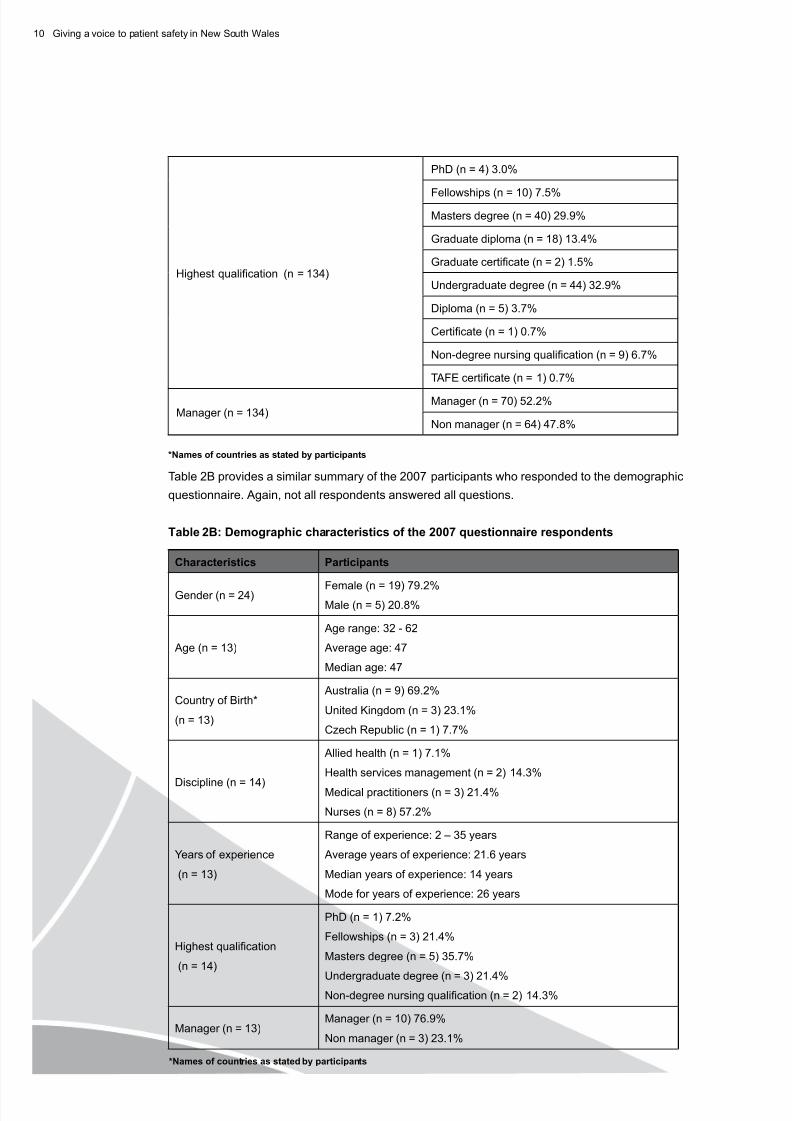
3.2 Participants’characteristics
A total of 195 participants attended 30 focus groups. Table 1 below provides details of the numbersof participants in each group, their eld of expertise and discipline backgrounds.
Staff inexperience was seen as problematic in three ways. Firstly there was a need to supervise
and support new staff more closely, an activity which took more experienced staff members away
from their other duties. Secondly, the lack of experience of junior staff was seen as contributing
to time pressures, as more experienced staff “… get through the work twice as fast and they
don’t miss things.” (Nurse Unit Manager). Agency and casual pool (n = 2) staff were seen as
contributing to time pressures because of the constant need to inform them about the hospital
or teams’ particular policies and procedures. Thirdly, in a small number of groups concern was
expressed about the ability or skills of staff to undertake the work required. Both experienced
and less experienced staff described potential and preventative errors as causing high levels of
anxiety, with one respondent still able to describe waking “… out of a sleep in a sweat thinking
‘oh my God’ ….” years after the event.
While quality improvement strategies were seen as a positive step forward, some questions
remained. These included: the need for standardisation and dissemination of quality andsafety approaches and procedures (which was raised by three groups) to stop “… every facility
reinvent[ing] the wheel as far as policy and protocols go…” ; the question of how to increase
participation in quality improvement activities, particularly by doctors; and how to translated
policies and procedures “… down to oor level.”
At the “oor level” focus groups described issues including: communication, documentation and
and or referral procedures (n = 6); falls (n = 5); equipment and environmental issues (n = 5);
and infections (n = 2). Communication, documentation and feedback were seen as impeding
patient safety in two competing ways. Lack of adequate communication and feedback was
seen as preventing improvements in quality and services. Conversely, trying to keep up withdocumentation was seen by one group as impeding the time available to spend with patients.
Similarly, effective feedback was seen as a positive contributor to improvements in safety, but
one participant felt that “… there’s a lack of feedback to staff too, so that problems aren’t xed in
a timely fashion.”
Communication was a recurring theme. The need was expressed for multidisciplinary teamwork,
which was particularly raised by nurses and allied health professionals. The most common
concern was the perceived difculty of allied health, nurses and junior staff in having their
opinions considered and respected, in particular by medical staff. Appropriate discharge and
planning procedures was an offshoot of this concern. Here too, participants raised the issue of
patients being discharged before all professionals, but in particular allied health professionals,
were able to provide input into their ongoing care planning.
There is not a good system of communication. It is very much ad hoc sometimes. We
have many patients. One person says one thing and another person says something
else. Doctors will often walk in and suggest sending someone home. The patient is from
the country somewhere, so there is a lack of planning and lack of forethought in the
communication. In addition, how far do you push things? You do get to the point after so
many years, of being tired of it all – the ethical side of it and the legal side of things. You
sometimes feel that you are not doing as much as you can, but you know that the doctor
does not want to do that sort of thing, so you back off …. (Mixed Focus Group)
Medications were seen as a serious concern, both in relation to the prevention of errors and alsobecause of the potential hazards of multiple medications on factors such as falls. Of the range of
potential medical errors, it was medication errors and falls that were most often raised as specic
examples of patient safety concerns. A pharmacist said this:
There is much more emphasis on the governance issues …. Everybody is much more
focussed on that - patient safety issues - and making sure that the systems are in place to
support us in reporting RIBS. We have had training on how to do RCAs and all those things
have improved over the last ve years. (Nursing Focus Group)
Overall, the 2004 focus groups indicated that their concerns about patient safety had changed
in recent years, with most of the systems changes seen as positive. Increased focus ongovernance (n = 4) and patient safety (n = 6) in general was seen as a positive move, along
with staff taking greater accountability (n = 3). The gradual acceptance of a no-blame systems
There’s going to be issues everywhere but we’re looking at health systems that started as little
systems, then technology and knowledge changed. So those systems had to incorporate the
new systems which provided the new technology but they’re not blending well. So the mergers
of all those systems have got little splinters all through them. Now you’ve got people training
through systems and they’re back-breaking workloads. Every three months I’m training new
residents. They get half an hour with me [to] tell them how to order safely. (Senior Nursing
Focus Group)
In relation to patients, a number of issues have emerged, most notably the rise of the “awarepatient” (n = 7). This was seen to have both positive and negative manifestations. From the positive
perspective, aware “… patients know now what their medications are, they know what they have to
do if there are any problems.” (Allied Health Focus Group). Patients were seen as being:
… a lot more savvy about their own rights now. I think that’s been a very big transition in the
last ten years, all that American focus on their rights and what they can and can’t do. I think that
creates an element of concern in terms of have we done all we can do to limit or lower the risk
of incidents…. (Nursing Focus Group).
Increased patient awareness was linked to the rise in litigation (n = 4) and negative media coverage
(n = 5). Increases in information technology, especially use of the internet, was identied as having
shaped patients’ expectations (n = 2).
I think also it’s the information age, there’s a lot more medical information easily available via
the internet and other sources, so the average consumer is much more aware; they can go
home from the doctor’s ofce and see if the information they’ve been given is correct, or if
something goes wrong with a relative in hospital they can straightaway get the information to
nd out what’s going on, whereas in the past they couldn’t do that. (Senior Health Executive
Focus Group)
There was also a perception that patients and their families had become more demanding
(n = 2). Aggression, from patients and from other staff (n = 2), was seen as a signicant and
I think there’s another way that our customer base has changed too, and that is I think that
issues to do with aggression and violence in the workplace are there now in a way they
were not even ve years ago. It can be verbal and it can be physical, and that introduces a
whole new dimension of stress that causes horizontal problems in teams as well. (Senior
Health Executive Focus Group)
Responsibility for patient safety was seen much more than in the past as being the responsibility
of “everyone” (n = 10). Two groups specically mentioned staff responsibility, and three groups
mentioned the need for patient, or patient and family, responsibility.
I think it’s everybody’s job and we all add to the picture. We all have a piece of the puzzle.
For me, a lot of it is around policy development and strategic planning but for the nursing
sister whom I supervise it is assuring that it actually comes off and they report if they think
something has happened, so I think it’s everybody’s job but once again I think you really
need that time to actually sit and discuss where we all put our pieces together and I don’t
think some people can actually start to think that broadly and widely. It’s not a criticism; I
think that’s just where they are at. (Senior Nursing Focus Group)
The responses from the 2007 participants closely mirrored those of the previous focus groups,
with a perception that commitment to improving patient safety had continued to increase in
recent years (n = 5). One participant described it as reaching “critical mass in terms of safety
awareness” (Management Focus Group). Risk assessment and clinical redesign were mentioned
by one group each as an example of signicant improvements in recent years.
Changes in concerns in recent years were attributed to a combination of factors. These
matched those in the previous focus groups, and included: increased patient awareness (n = 2)particularly as a result of the internet (n = 1); increased expectations from patients and families
(n = 1) including issues of litigation (n = 1) and increased complaints (n = 1) – neither of which
were necessarily seen as negative; increased patient acuity and demographic changes (n = 2)
“safety needs are reecting changes in the client population” ; and shorter stays in hospitals of
sicker patients (n = 1).
Stafng and workforce issues (n = 4) including fewer and more junior staff, a general lack of
resources (n = 2) continue to remain a concern. Increasing administrative demands led one
participant to comment “… I could spend one and a half times my working life in front of a computer.”
The more recent focus groups in effect reected on the maturing of safety improvement
strategies. These include a focus on the sustainability and transfer of quality and safety
improvement programs and projects (n = 3) and integration of a wide variety of projects and
priorities (n = 1). Incident reporting (n = 3) and RCAs (n = 2) were seen as contributing to a
positive change. Although participants openly acknowledged that these strategies contributed
to the identication, reporting and assessment of errors, they also raised concerns about: the
system’s capacity to respond to the causes identied; the focus on RCAs to the perceived
exclusion of other modes of analysis; and the lack of engagement of clinicians, particularly senior
clinicians and doctors, in these processes (n = 2):
I think there has been a cultural change, particularly with nursing staff, I think a lot of
this has been driven by nursing staff who generate the [IIMS] reports, whereas I am not
sure the cultural change is there with the medical staff yet … the issue is more in focus… but the problem I have is getting … senior clinicians to serve on RCAs because they
don’t understand what it’s all about – at that level the message hasn’t gotten through yet.
The 2004 focus group participants mentioned specic population group categories as being at
higher risk than others in the health system. Most common were the elderly (n = 17), followed by
people from non English speaking backgrounds (n = 13), people with mental illnesses (n = 10),
young people and children (n = 4), Aboriginal and Torres Straight Islanders (n = 3) and patients with
disabilities (n = 2). Elderly people were seen as being at risk as a result of a combination of frailty,
increased co-morbidity including cognitive impairments and dementia, and organisational difculties
in providing adequate care.
Thinking about the frail aged, we don’t even have the appropriate physical environment for
them a lot of the time. We don’t have dementia-specic accommodation with secure units; we
don’t have the physical environment to deal with [elderly] patients. We need to look at moreoutside the box stuff, padding oors, pressure-sensitive alarms, those sorts of things. (Senior
Nursing Focus Group)
One focus group also identied the issue of attitudes towards elderly people as a cause of higher
risk. As a Senior Executive put it:
I think there is a need for education, refocusing, particularly, there are growing numbers of
elderly people going into the public hospital system and they call them bed blockers which I
think is a dreadful term. It’s no wonder people develop an attitude that we shouldn’t be looking
after them, they shouldn’t be here…. (Senior Health Executive Focus Group)
People from non English speaking backgrounds were identied as being at risk because of lack of ability to communicate, lack of family members and difculties in accessing interpreters and support
workers. These last three issues were also said to apply to Aboriginal and Torres Straight Islanders.
The second most common group acknowledged as being at risk were patients experiencing various
forms of disadvantage. These included: isolated patients and those without family or support
systems (n = 9); patients from lower socio-economic backgrounds (n = 6); patients who live in
locationally disadvantaged areas (n = 3); patients who are illiterate or can’t communicate (n = 3);
patients experiencing domestic violence (n = 2); and the homeless (n = 1).
A patient without an advocate, whether that be a nurse or relative as an advocate, I think
that patient is at risk. My dad was in hospital last year and I wouldn’t leave his bed, I wanted
to double-check everything that went through, everything he received. Anyone without anadvocate I think is at risk. (Senior Nursing Focus Group)
Locational disadvantage was seen as stemming from three factors. Firstly, rural patients had
to either travel or be transported long distances for adequate treatment. Secondly, there was a
perception that services in locationally disadvantaged areas had fewer resources, and that these
were stretched by the complexity of social and health problems in these areas. Thirdly, there was
a sense that areas of high need were conversely, the least likely to attract highly qualied health
professionals they required.
Patients with co-morbidities (n = 3), cognitive impairment (n = 3), those who were malnourished (n
= 2), obese patients (n = 2), patients with dual diagnoses (n = 1), and patients with drug and alcohol
problems (n = 1), were also identied as being at risk. So too were patients who were bedridden
(and at particular risk of pressure sores), those who were post surgery, and those who had been
Examples of medication errors included cases of omission and commission, that is, both where
the wrong medication was given, and where the correct medication was not provided or delayed
or withheld:
… there’s a lot around warfarin management as well, probably a lot of medical errors and
omissions with that sort of thing, the managing of warfarin and complications at home,
taking it themselves. I don’t know how it’s managed in the community…. (Nursing Focus
Group)
As well as providing an i llustration of medication errors, this example also highlights broader
issues of patient safety. These include patient education and the potential for longer term errors
once the patient has been discharged.
A small number (n = 5) of errors was not identied by focus groups in their discussions. This
included failure to employ indicated tests and use of outmoded tests or therapy, errors inadministering treatments, inappropriate care and other systems failures.
The adverse events identied in 2007 highlight a small range of persistent problems. Error in
performance of an operation, procedure or test (including wrong site surgery) was witnessed by
four groups.
ICU patient received dialysis where the machine was not set up properly - so they arrested,
and they wouldn’t have if the machine was right. (Allied Health Focus Group)
Three groups identied communication failures and a further three “other systems failures”
including two which resulted in completed suicides. Two groups each identied error in the dose
or method or using a drug, failure to act on the results of monitoring or testing, and in avoidabledelay in treatment or in responding to abnormal test.
A double of anti-coagulant effectively and they ended up in ICU – and nearly didn’t make it
and that was very serious. (Allied Health Focus Group)
Groups also gave examples of a range of other errors. These included: error or delay in
diagnosis; inappropriate (not indicated) care; failure to provide prophylactic treatment; work
environment/scheduling; knowledge skills and competence; and failure of safety mechanisms.
An elderly patient with dementia was sent to radiology for an x-ray with a wardsman, but
when they got there the wardsman pointed out … to the radiographer that the patient
appeared … very ill. The radiographer sent them to the ward, but by the time they got there,
the patient was dead. (Medical Focus Group)
As in 2004, a small number of errors was not identied by the 2007 focus groups. This included
failure to employ indicated tests and use of outmoded tests or therapy, equipment failure, patient
factors and policies, procedures and guidelines.
Focus group participants were provided with a handout (Appendix 3) asking about their
perceptions of rates of adverse events in their institutions. A range of staff had experienced
adverse events.
We also asked about minor events. In 2004 medication errors represented the largest category
of minor adverse events identied in the questionnaire. Safety mechanisms (including falls with
no major injuries) ranked second. In 2007 medication errors and falls were equal rst.
Patient safety was considered to have improved signicantly in recent years as a result of
changes to the system, and improved organisational and professional cultures. Overall, the focus
on patient safety and the shift to a systems approach (n = 7) was acknowledged as a signicant
step forward in safety, as was incident reporting (n = 5) and a move towards a proactive and
preventative approach to safety (n = 3). The conceptual move from a “blame and shame”
through to a no blame or just blame approach was afrmed as a good development by three
groups. Good care overall was cited by one group.
I think it’s good to have something that will be state-wide, so there’ll be more sharing of
information across the board, so the idea is that we’ll be able to catch something that’s only
happening a couple of times a year in each hospital, but as a whole is happening a lot, so it
will be quicker to put things in place to prevent it happening again. (Nursing Focus Group)
Improvements in various forms of communication were mentioned by a number of groups.
Examples included improvements in: gaining consent from patients (n = 2); collaboration
between groups (n = 2); sharing information (n = 1); talking to patients (n = 1); risk assessments
(n = 1); and feedback (n = 1).
The collaboration with the dieticians and the nurses has again come to the forefront. We are
talking about things, like food charts and understanding the signicance of it, rather than
thinking it is another piece of paper that we have to ll out. The dieticians and nurses are
talking to each other and getting the doctors on board. The doctors are listening to what
everybody is saying and doing it, rather than one group dominating it all. There is more
collaboration now…. (Mixed Focus Group)
A number of groups mentioned particular areas where they felt health services were doingespecially well in terms of safety. These included: infection control (n = 2); aged care
rehabilitation and risk assessments (n = 2); education and training on safety issues (n = 2);
improvements in equipment and technology (n = 2); and the employment of Enrolled Nurses (n =
1). The introduction of Patient Safety Ofcers was also seen as a constructive step (n = 1).
Changes to some aspects of professional and organisational culture were also believed to be
promising. A commitment to, and support of multidisciplinarity (n = 6) was considered a very
positive development, as was the willingness to acknowledge, take accountability for, and learn
from, mistakes (n = 5) and openness, including open disclosure (n = 5).
I think the focus on patient safety is great and it’s very topical at the moment … and the
openness, while it’s still not perfect, it is improving. It’s no longer the sacred domain of the
doctors to be just in the M&M … the doors are slowly opening to allow the multi-disciplinary
teams to participate … people want to be learning; they want to talk about the mistakes that
occur and learn from [them] …. (Nursing Focus Group)
The 2007 focus groups identied a range of strategies, activities and approaches which were
contributing to positive improvements in patient safety at a variety of levels. Clinical governance,
safety champions and more effective responses to patient complaints were each identied by
one group.
The Clinical Governance Unit [in this service] has made a huge difference to the working life
of managers and nurses and patients … having a functioning clinical governance unit, it’s
taken an awful lot of pressure away from patients who were making complaints, and who
[had in the past] not been taken seriously … forcing NUMS and other managers to take the
Referred to Patient Safety or Quality Manager or Unit (n = 4)
Presented to Mortality and Morbidity Review (M&M) (n = 2)
Discussion at clinical review or safety meeting (n = 3)
Feedback to facility or team (n = 2)
Identication of strategy to support staff (n = 2)
Requested support from colleague or related professionals (ambulance, police) (n = 3)
Individual responses
Discussion with involved parties (staff, General Practitioners) (n = 2)
Discussion with involved parties (patients, carers or families) (n = 3)
Positive response from senior management (n = 3)
Negative response from senior management (n = 1)
Other
No support, response or feedback (n = 11)
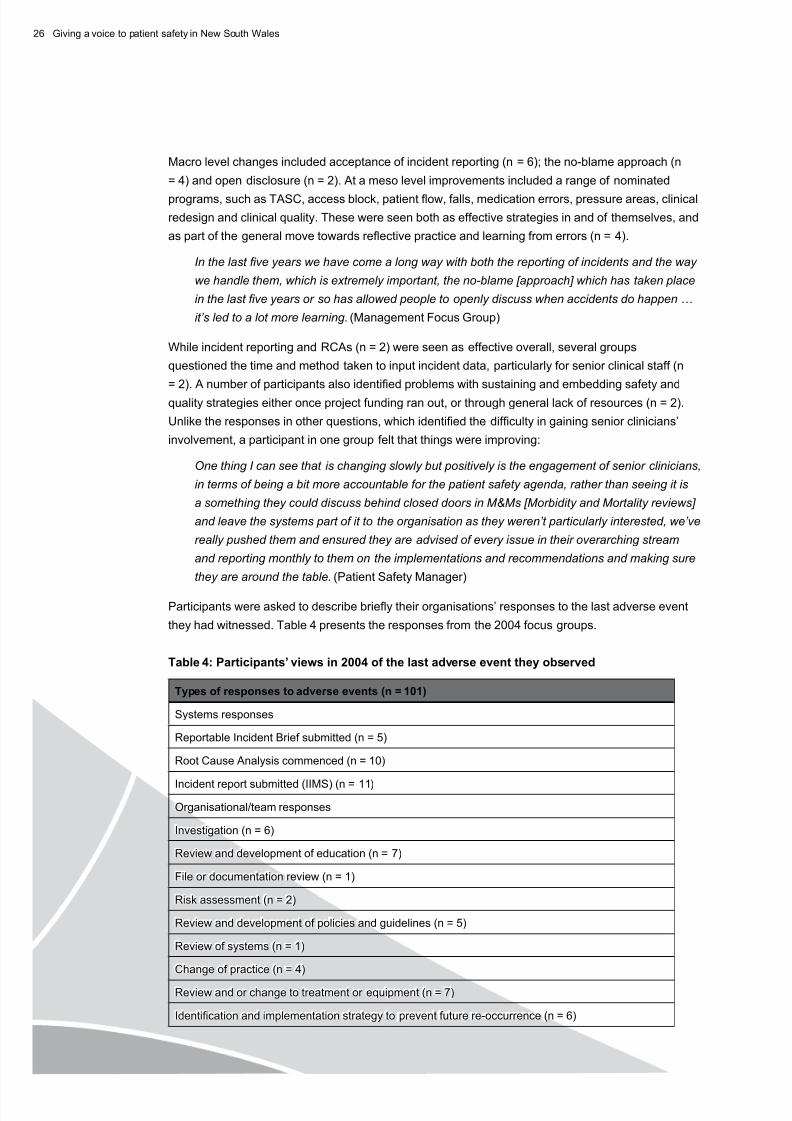
Participants’ responses to adverse events can be seen as dividing along systems, organisation
and individual lines. At a systems level, the introduction of various forms of error reporting and
analysis is evident in participants’ responses. At an organisational level a range of investigations
and reviews are undertaken. As well as reactive approaches, proactive changes in practice,
treatment, equipment, policies, and education were identied (n = 23). Some 11 participantsmentioned that they had received no support or feedback in relation to past errors.
The 2007 focus groups recorded similar types of responses. The most common responses were:
IIMS report submitted (n = 4); discussion with involved parties - staff (n = 5) and patients and
their families (n = 3); investigations (n = 3); RCAs; review and development of education; review
and development of policies and guidelines; and referral to Patient Safety or Quality Manager
(each n = 2). Other individual responses included: RIB submitted; review of system; change of
practice; review and or change to treatment or equipment; identication and implementation of
strategy to prevent future re-occurrence; and SAC rating given.
Participants were asked to rate their service’s response to the last adverse event (Table 5).
Almost 100 participants responded in 2004. They were provided with three possible measures:
effective, efcient and whether they felt the action was ethical. While most participants felt that
their services’ response to the last adverse event was effective, efcient and ethical, a notable
In 2004, participants overwhelmingly said that they would go to their immediate supervisor or
manager in the rst instance after encountering an adverse event, or to their Head of Department
or Team Leader (n = 72). Fewer would go directly to their Patient Safety or Quality Manager or Unit
(n = 20), although 15 participants mentioned that in the rst instance they would ll out an incident
form. Overall, of the 205 responses (more than one response was possible for each participant),
70.4% mentioned going directly to management of some kind, while 4.3% mentioned speaking tocolleagues, friends or peers. The same general pattern held in 2007. Participants said they would
go to their own, or to the line manager of the individual involved, rst. Two participants said that they
would make an incident report in IIMS at the same time.
0 Giving a voice to patient safety in New South Wales
Potentialcausesoffutureadverseevents(n=181)
Medication errors (n = 17)
Falls (n = 8)
Pathology error (n = 1)
Aspiration (n = 1)
Other
No idea (n = 1)
Litigation (n = 1)
Once again, responses can be mapped to broad systems categories. Responses to this question
reect participants’ responses to the question of frequency of errors: across the board, failure of communication (in its various forms) is identied as the number one contributor to errors (19.3%),
followed closely by workforce issues such as stafng shortages (12.7%), skills (3.9%) and
experience (5.0%) of existing staff, and workload (7.2%).
The 2007 responses (n = 18) showed a similar pattern, although medical errors (22.2%) rather
than communication failures (16.7%) was perceived as the likeliest cause of future events. Other
Co-ordination between services was identied as a problem (n = 3), and both an acute and
community focus group (n = 2) identied the lack of 24 hour support for patients within their
homes as a signicant concern. Difculties in identifying, communicating with and handing
over to General Practitioners (GPs) was noted by the same groups as an issue in the longer
term safety of patients. In this last case, the impact of bulk-billing, the increase in large medical
centres rather than individual practices and the reticence of GPs to do home visits were issues
of note causing particular concern.
At an organisational level the matter of stafng once again ranked highly. Staff numbers were
identied by three groups as an issue, staff mix and level of experience by four groups, with an
additional two mentioning the increasing “casualisation rate” of staff. The implications of this
were seen as “… if we don’t grab hold of the challenges of training people in those situations
to be part of and recognised as part of the teams as they exist, then we’re gone ….” (Senior
Executive Manager). One group identied concerns about the Enrolled Nurse to RegisteredNurse levels, and expressed concern that this would be an increasing problem in the future.
Three groups mentioned their concern about the ability of staff to meet patients’ needs.
It is time consuming so it’s partly a time factor because you’re so busy trying to look after
your patient and then learning these new skills is taking extra time, to get everything
done on your shift. I stayed back until 11 o’clock the other night because I type with just
one nger and it was past 10 o’clock and I had to write my notes. I had to double check
everything. I had to deal with patients, equipment; there was an in-service on, etcetera….
(Senior Nursing Focus Group)
Resourcing for both staff and services was mentioned by ve focus groups. Two groups
mentioned pressure from senior management about roles and workloads as potentially affecting
patient safety. Two groups mentioned the need to provide training with the introduction of new
technologies, and one group specically mentioned the need for staff release to attend training,
and another supervision, in particular for junior staff (n = 2) as an additional concern. Workload
matters were raised by three groups, with one group mentioning in particular increases in
workload after the introduction of new safety systems.
… the junior medical staff … often have excessive expectations put upon them in terms of
their role and responsibilities by consultants … I think that always produced problems and
to change that really requires consultants to change their practices, how frequently they
come in, how frequently they review the patients, how much they let the registrars do on
their own and how much they actually supervise them. (Senior Nursing Focus Group)
Spanning organisational, team and individual levels were issues of communication and culture.
Discharge and care planning was identied at an organisational level (n = 2). Lack of effective
communication between staff was mentioned as a key factor preventing safety improvements
in ve focus groups. One group also mentioned lack of communication during handovers and a
lack of other types of follow-up as a more generalised organisational-clinical problem.
Existing organisational and team cultural decits were identied as a problem by ve groups,
with one group also mentioning difculty with resistance to change. An additional group
mentioned the need for “… better recognition of adverse events happening …” in other words an
Giving a voice to patient safety in New South Wales
I think we need to change the culture of task orientation, to know that there’s more than just
the simple one, two, three things that you have to do for that patient – a more holistic point of
view, that there might be problems with a patient that are identied before something actually
happens. (Senior Executive Focus Group)
At an organisational and facility level, the workplace environment, including the layout of wards,
was also an issue (n = 2). Follow-up of recommendations of RCAs was identied by one group, with
another mentioning the need for greater creativity in seeking solutions to patient safety issues.
At an individual level, fear was identied as an obstacle to patient safety. Three groups mentioned
fear of litigation as affecting both clinician behaviour and patient safety. In one group a participant
offered the following observation “I still think there’s a big problem of litigation hanging over people’s
heads too. I think it has improved a bit in trying not to have the culture of blame so much ....” In two
cases, focus groups mentioned this fear manifested itself in hyper-vigilance:
So I can well understand where some of the junior doctors are coming from with regards to
over-ordering of tests, they are also aware that it’s becoming a more litigious environment and
they feel the more rudderless they are from up top and the less they feel they can ask, the
more they defend themselves with tests …. (Pathology Focus Group)
The 2007 focus groups identied a different range of issues, although within the same broad
categories of organisational, team and clinician concerns. In terms of organisational issues, it was
systems design, the impact of restructuring and amalgamation “the whole amalgamation of health
services on top of trying to drive the patient safety agenda, in a way that amalgamation dismantled
stuff that we already had in place, and we’ve had to go back and start again” (n = 3). The translation
of research into practice was equally seen as a major factor (n = 3) in preventing improvements.
We talk about evidence, and we spend so much money on research, but it never really gets
to practice – the service model, we still have the same old range of service models despite a
wealth of evidence that they need to change. (Management Focus Group).
Resource issues (n = 4), the volume of work (n = 2), and staff competency and skill mix (n = 2)
continue to be a concern, with the lack of administrative and middle management support receiving
special mention (n = 3). So were demands of increasing workloads on staff in general.
Attitudinal issues were also noted. The silo mentality was identied by one group as being a
problem, as were the attitudes of some staff to patient safety initiatives (n = 3) in general. Some
staff were seen as being affected by burn-out from “too many” different initiatives. The lack of engagement of medical practitioners and senior clinicians in general (“it’s so hard to get medical
compliance on these sorts [TASC] of issues” ) was identied by three groups. This was seen as
being the result of a lack of effective consultation with clinicians and indicated a need to develop
safety and quality improvement strategies specically for this group.
I think that this [lack of clinician engagement] is because they see this as people running
around with clip-boards and the data they do see, they are not sure they can trust … what do
you do right at the very front about what you have to do about getting people to do it, why don’t
you talk to them? ... You need someone very senior and clinical to speak to someone very
senior and clinical to justify their practice. (Medical Focus Group)
… the patient has got to be at the forefront of everybody’s mind really, that is not just fromthe safety perspective, but you always think you have someone on the end of what you
are doing ... [and] something that goes hand in hand with that [is] working well above your
minimum professional standards, but also keeping the patient always in mind too …. (Allied
Health Focus Group)
The strategies identied by the 2004 focus groups as potentially improving patient safety closely
mirror the factors identied as preventing patient safety. Participants identied the following
categories of improvements: stafng; practice issues; culture; development; environment; and
systems and organisational issues.
Stafng was identied as a major factor in improvement, with ten groups identifying increased stafng
as their top priority, with two groups specifying increasing the numbers of Registered Nurses (RNs)
and one arguing for a general increase in experienced staff. Two groups asked for more planners,
one for discharge planners and the other for patient case managers. Two groups wanted more time
to spend with patients and another so that staff are “… not feeling so overwhelmed that they can
actually think about what they are doing and why they are doing it.” Workload was mentioned by two
groups, with one allied health participant making the following plea:
I would increase the number of medical staff in terms of junior doctors available because
the way they have been stretched creates some of the issues. They are not able to listen,
they are not able to attend the meeting and they are truly very stretched. I don’t know how
anyone can work under those conditions. (Allied Health Focus Group)
Practice issues can be essentially patient centred and staff centred. Patient centred issues
included a strong call for patient centred care (n = 8). Two groups suggested taking a holistic
approach to patient care, including pre-screening for issues such as nutritional levels, which
could translate into an increased risk of adverse events (such as pressure sores or infections)
later on.
In relation to staff, the creation of cohesive teams was identied by three groups as a key
issue, with one group mentioning in particular the need for teams with a mix of staff experience.
Improving communication between groups was mentioned by one group, with another identifying
the need for improved communication with patients. One group mentioned a need to increase
staff “heedfulness”, or keeping their focus on the job.
Cultural issues were raised by ve groups. Two issues were identied. These were the need
for a culture shift (n = 3) in relation to patient safety, and the need for awareness, reexivity and
responsibility in staff (n = 2).
… the thing I’ve seen most often is just inaccurate things on medical records, it just
happens because people rush, because they are not listening properly, because of poor
communication, all that sort of thing. They’re the sorts of mistakes I’ve seen, and I’ve seen
a lot of them, and all are completely understandable. I’ve seen very few things happen
because people are basically very poor at what they are doing. The things I’ve seen happen
have been due to stress or due to a particular system. But people are so defensive about
– rather than going ‘I was really tired’. So there’s defensiveness about not correcting things
so things get compounded. (Senior Nursing Focus Group).
Giving a voice to patient safety in New South Wales
Development was another strong category of suggestions for improvement. Peer review (n = 1),
education and training (n = 5), mentoring, involvement in RCA teams, compulsory peer reviews and
strategies for the reduction of isolation of staff (particularly, but not only locationally isolated staff)
were all identied.
Environment was seen as a factor for improvement for both patients and staff. For staff, one group
mentioned the need for a communal space, away from patients, within which staff could talk about
issues. For patients, the re-organisation of the ward environment for patients, and especially ageing
patients at risk of falls, was raised as a needed improvement. One group asked for increased
resources to improve the ward environment overall. A nal group mentioned a successful strategy
that had already been implemented, as a model for the types of improvements they wanted to see:
I was working in rehab and their system had everyone in it. They have a tick list that asks
consultants ‘What are your goals? Have they been achieved? What is going on here?’ so they are
all demanding to get [the patient] out the door in a cohesive system, so that would be great, to do
that and have the consultants more involved on the ward level and for us, to be able to address our
issues as well. Then maybe, we can say to the patient ‘… these are your options. It is ultimately
your decision, and you can decide what happens’ …. (Allied Health Focus Group)
One of the largest groups of comments related to systems and organisational solutions. These
ranged from the very broad such as health care taking a proactive rather than a reactive approach
to patient safety and care (n = 2), including following patients through the system (n = 1), through
to the very specic, such as the re-institution of ward rounds led by NUMS, on a daily basis (n = 1).
A national mandatory reporting system was raised by two groups, as well as a patient identication
system (n = 2), dissemination of information and learning from safety initiatives (n = 1) and co-
operation between health care sectors (n = 1). Services in the community and improvements in
patient transport were each raised by one group. The standardisation of care at all levels (including
the institutionalisation of guidelines) was identied by three groups.
The suggested categories of improvements shifted slightly for the 2007 participants. Increased
staff and reduction in workloads continued to be a major issue (n = 5) for all discipline groups, but a
specic mention of middle management and administrative staff by two groups was new. Improved
communication at all levels of the system remained important (n = 3), with an emphasis on improved
consultation and communication at the “coal face” (n = 2). One group suggested that all services and
departments should “work collaboratively like aged care and rehab … with case conferences and family
conferences” . Improved staff competency (n = 2) was considered fundamental. Better use of information
technology was raised by two groups, particularly in relation to medical practitioners:
The IT strategy is nothing really clinical, its about patient administration, nancial
administration, IIMS which is separate … there is a whole world of clinician decision support
that is just not there – it’s not even a branch of what they are doing … we all know it can be
done … some clinically linked thing that a specialist could say this is the pathway for this
condition and we could all be on the same page. (Medical Focus Group)
Improving the skills of clinicians as well as their procedures was identied as an issue by one group.
They saw the root cause not in individual error itself, but in the training and skills levels of some
clinicians:
If you do the wrong patient’s x-ray … as an example … that would be a SAC 1 – but what my concern which is deeper is the number of unnecessary referrals in the rst place, we are talking
about radiation, which are given in an emergency situation … lack of knowledge of junior
clinicians is much more important to look at . (Allied Health Focus Group)
0 Giving a voice to patient safety in New South Wales
Three issues were seen as currently limiting the CEC’s signicant potential impact on health
service delivery. The rst was the visibility of the CEC as an entity independent of the DOH, and
distinguished from other quality and safety bodies. The second was the perceived lack of effective
consultation to AHSs and then to the “grass roots” levels of health services (i.e., to clinicians) and
the CEC’s ability to respond to the needs of people at those levels. Third was the need to improve
co-ordination between CEC and DOH requirements and strategies in order to reduce frustration
amongst managers and clinicians about which activities to prioritise. One focus group pointed out
that some of the issues which were perceived as limiting the CEC’s effectiveness were currently
being addressed by the CEC and that signicant improvements had been made in co-ordination and
communication with AHS over the last couple of months. This positive change was attributed to new
staff at the CEC.
Participants in 2007 also provided some additional suggestions about the future activities of the
CEC. These were very similar to those identied in 2004. They included: the careful selection byCEC of key issues or themes for co-ordinated safety improvement efforts (suggestions included
risk analysis, handover, deteriorating patients, clinical report writing); increased public and clinician
prole, including improvements to feedback and communication to all levels of health services;
return to site visits; provision of best practice models and examples of frontline interventions;
provision, co-ordination and direction of safety and quality educational activities; and specic
strategies to engage senior and other clinical staff.
5 Discussion
These results show that the issue of patient safety in NSW has been identied as a challenge requiring
cohesive and coordinated solutions. The dimensions of the problem have been dened by staff drawn from
various levels and disciplines. Central to the responses was the issue of communication: difculties and
breakdowns in communication, in its various forms, more than any other factor, was seen as contributing to
past and present adverse events.
While central to the problem and its solutions, communication was not the only factor. Broad systems issues,
especially the question of workforce shortages, training and skills levels were common concerns, particularly
from managers. Groups from all disciplines raised questions of adequate workloads, and the issue of time:
time for training, time for reection, and time to care adequately for, as well as treat, patients. Restructuring
was also seen as a barrier to continuous improvements. Changes in patient proles, in particular increasing
numbers of seriously ill patients, patients with mental illness, and patients with cognitive and communication
problems were seen as contributing to the need for highly skilled and focused health practitioners.
Progress has been made in addressing patient safety. Developments in incident reporting and error analysis
provides an indication of recent and signicant changes. Many staff think the NSW health system is on the right
track toward improvement, notwithstanding the challenges that lie ahead. The health system and individuals
are responding to patient safety concerns. The willingness of many participants to report errors, discuss their
concerns with management and colleagues, and participate in rapid reviews and responses can be seen as
suggesting that changes are occurring in the safety culture. So too can the fact that the majority of changes
in recent years were seen as positive; the increased focus on governance and safety, was seen as a step
forward, for example. Several groups argued for further increases in levels of accountability and responsibility
of staff. There was support for the shift away from the old “blame and shame” culture.
Commitment to the current direction in addressing medical errors and adverse events, as well as a
belief that there is more work to be done, can be seen in the perspectives adduced in this study. We
can be cautiously optimistic, particularly as the results from the latest focus groups showed a sustained
commitment to safety improvement and a maturation of concerns, including the need to sustain and embed
systems and practice improvements.
However, in a number of responses, some participants raised concerns about the level of support they
do and would receive in the event of a major adverse event. Obstacles or factors which were seen as
inhibiting improvements to patient safety, aside from stafng levels, centre on communication and teams:
communication between the health care system and management and staff; teamwork between staff, in
particular across disciplines; interaction between teams and services, especially with GPs; and integration
of effort between professionals, patients and their carers and families. In recent years the impact of
restructuring and amalgamations, limited resources and the workforce skill mix were seen as slowing if not
impeding safety improvements.
Participants’ experiences with adverse events and errors, while distressing, are increasingly common.
The concern of participants was less about blame than in the past. Accountability remains a signicant
issue, and the need to take a proactive, rather than reactive approach. All groups were able to provide
examples of both minor and major adverse events. They were also able to provide examples of advances
and improvements either currently underway, or which they are hoping to see in the near future. It is in this
context that the role and value of the CEC to the practising health professional becomes apparent.
Participants provided a wide range of suggestions as to the potential role and contribution of the CEC to
their work lives. Four major categories were identied including establishing benchmarks, conducting new
programs and activities, facilitating culture change, and undertaking research. In addition, participants hadsome denite suggestions about the approach the CEC should take: it should be proactive, strategic and
consultative, and inclusive of stakeholders, especially of professionals and patients. CEC, for its part, is
starting to do this, as its Directions Strategy, Annual Reports and other documentation make clear. [www.
cec.health.nsw.gov.au/]
6 Conclusion
The information presented in this report shows that patient safety is more than a set of technical problems;
rather, it is an organisational issue. The health professionals who gave their time and expertise to speak
in the focus groups made one point very clearly: the issue of patient safety had affected them all. Their
candour in speaking about the issues of medical errors and adverse events, the way in which they were
willing to discuss events that had happened to them or those close to them, and the depth at which
they were all, new graduates and senior executives alike, able to speak about the causes and possible
solutions, was testimony to the professionalism with which they engage with this issue.
None of that is, perhaps, surprising. The people we spoke to are health professionals who are dedicated
to preserving and improving people’s lives, and who, by nature of the research sampling process, are also
people who were willing to come forward and speak openly in a group setting about this issue. What was
telling, however, was the depth of their concern, the passion and commitment to tackling patient safety, and
what this passion and commitment meant to them. The message was loud and lucid: the advancement of
patient safety is as important for the majority as the advancement of health. The challenge is not merely
about the need to improve patient safety, but rather, nding ways in complex, changing, increasingly
Giving a voice to patient safety in New South Wales
scrutinised workplaces so that safety is improved to the benet and satisfaction of both patients and health
professionals. There was a rm belief that patient safety problems occurred not so much as a result of
individual error, but rather as a result of a combination of poor communication, ineffective teamwork, cultural
barriers or inadequate or inappropriate resource management. This is not to say that everyone in every group
agreed: in some isolated cases, individuals felt that the concerns about patient safety had been conated
somewhat, particularly by a sensationalist media.
An unanticipated nding of the research was the strength with which staff essentially held that they, as well
as patients, were vulnerable within the health system. Participants’ major concerns about patient safety
reected this dual apprehension. The most common concern was lack of trained, reliable staff, in virtually all
disciplines, and poor coordination of care. Closely tied to this were the issues of resources and the distribution
of resources across the health system. These require concerted improvement over time.
Staff spoke about the way in which changes to the health system had affected them, and their patients, inrecent years. On a negative note were high levels of uncertainty, staff shortages and for some a sense of
exhaustion in trying to keep up with the pace of change in almost all aspects of service delivery – from policy
development through to practice. On a positive note, the increased concern with patient safety as a whole was
seen as highly valuable, and it was encouraging for our participants to see programs, and to observe multiple
initiatives, which they thought were beginning to pay dividends.
7 References
Affonso, D. & Doran, D. (2002) Cultivating discoveries in patient safety research: a framework.
International Nursing Perspectives, 2 (1), 33-47.
Amalberti, R., Auroy, Y., Berwick, D. M. & Barach, P. (2005) Five systems barriers to achieving
ultrasafe health care. Annals of Internal Medicine, 142 (9), 756-764.
Australian Institute of Health and Welfare (2006) Australia’s health 2006. Canberra, Australian
Institute of Health and Welfare.
Baker, G. R., Norton, P. G., Flintoft, V., Blais, R., Brown, A., Cox, J., Etchells, E., Ghali, W. A.,
Hebert, P., Majumdar, S. R., O’Beirne, M., Palacios-Deringher, L., Reid, R. J., Sheps, S. & Tamblyn,
R. (2004) The Canadian Adverse Events Study: the incidence of adverse events among hospital
patients in Canada. Canadian Medical Association Journal, 170(11), 1678-1686.
Barach, P. & Small, S. D. (2000) Reporting and preventing medical mishaps: lessons from non-
medical near miss reporting systems. British Medical Journal, 320(7237), 759-763.
Bazeley, P. & Richards, L. (2000) The NVivo Qualitative Project Book. London, Sage.
Bleich, S. (2005) Medical errors: ve years after the IOM report. Issue Brief: The Commonwealth
Fund . Accessed on 16 November, 2006. Available at: http://www.cmwf.org/publications/publications_
show.htm?doc_id=289844
Braithwaite, J., Finnegan, T., Graham, B., Degeling, P., Hindle, D. & Westbrook, M. (2004) How
important are safety and quality for clinician-managers? Qualitative evidence from triangulated
studies. Clinical Governance: An International Journal, 9(1), 34-41.
Braithwaite, J., Travaglia, J., Mallock, N.A., Iedema, R., Westbrook, M.T., Long, D., Nugus, P., Forsyth,
R., Jorm, C. & Pawsey M. (2005) Evaluation of the Safety Improvement Program in New South Wales:
overview of studies. Sydney, Centre for Clinical Governance Research, University of New South Wales.