Nurs Admin Q Vol. 31, No. 4, pp. 284–299 Copyright c 2007 Wolters Kluwer Health | Lippincott Williams & Wilkins Acuity Systems Dialogue and Patient Classification System Essentials Kelle Harper, BSN, RN; Crystal McCully, BSN, RN Obtaining resources for quality patient care is a major responsibility of nurse leaders and requires accurate information in the political world of budgeting. Patient classification systems (PCS) assist nurse managers in controlling cost and improving patient care while appropriately using financial resources. This paper communicates acuity systems development, background, flaws, and com- ponents while discussing a few tools currently available. It also disseminates the development of a new acuity tool, the Patient Classification System. The PCS tool, developed in a small rural hospital, uses 5 broad concepts: (1) medications, (2) complicated procedures, (3) education, (4) psychosocial issues, and (5) complicated intravenous medications. These concepts embrace a 4- tiered scale that differentiates significant patient characteristics and assists in staffing measures for equality in patient staffing and improving quality of care and performance. Data obtained through use of the PCS can be used by nurse leaders to effectively and objectively lobby for appropriate patient care resources. Two questionnaires distributed to registered nurses on a medical-surgical unit evaluated the nurses’ opinion of the 5 concepts and the importance for establishing patient acuity for in-patient care. Interrater reliability among nurses was 87% with the author’s acuity tool. Key words: acuity, classification, patient care, retention, staffing M ANY ARTICLES have been dedicated to healthcare issues such as nursing short- age, higher patient acuities, decreased length of hospital stay, and rising healthcare costs. Almeida and Persson 1 state that these issues have become a major concern of consumers, healthcare professionals, providers, and pur- chasers. These changes within the healthcare system have led administrators to look for im- proved ways to manage a broken system. Healthcare managers are constantly trying to contain cost while still providing excel- lent patient care. The desire to control cost, however, has changed patient care. In the past, doctors admitted patients the day before surgery. This provided ample time for the doc- From the School of Nursing, University of Texas at Arlington. Corresponding author: Kelle Harper, BSN, RN, ER, Uni- versity of Texas at Arlington, FNP Student (e-mail: [email protected] or [email protected]). tor and nurse to provide valuable postsurgi- cal and discharge teaching. To contain cost, however, hospital and insurance companies no longer support this service. This decreased length of hospitalization ultimately increased the average patient acuity on care units. Patient acuity is defined as the categoriza- tion of patients according to an assessment of their nursing care requirements. 2 Owing to increased patient acuity in care units, nurses are taking care of more complex patients than in the past. Fagin 3 notes that this situa- tion is complicated by the fact that increased demands for documentation mean that care- givers can devote fewer hours to direct care and monitoring. To counter these increasing needs, hospital administrators have used pa- tient classification systems to document pa- tient acuity. These tools aid in gathering in- dividual patient care information, identifying acuity ratings, determining staffing, and as- signing patient loads. The purpose of this pa- per is to review the literature on acuity tools, discuss the pros and cons of acuity tools, 284
Acuity Systems Dialogueand Patient ClassificationSystem Essentials
Kelle Harper, BSN, RN; Crystal McCully, BSN, RN
Obtaining resources for quality patient care is a major responsibility of nurse leaders and requiresaccurate information in the political world of budgeting. Patient classification systems (PCS) assistnurse managers in controlling cost and improving patient care while appropriately using financialresources. This paper communicates acuity systems development, background, flaws, and com-ponents while discussing a few tools currently available. It also disseminates the developmentof a new acuity tool, the Patient Classification System. The PCS tool, developed in a small ruralhospital, uses 5 broad concepts: (1) medications, (2) complicated procedures, (3) education, (4)psychosocial issues, and (5) complicated intravenous medications. These concepts embrace a 4-tiered scale that differentiates significant patient characteristics and assists in staffing measures forequality in patient staffing and improving quality of care and performance. Data obtained throughuse of the PCS can be used by nurse leaders to effectively and objectively lobby for appropriatepatient care resources. Two questionnaires distributed to registered nurses on a medical-surgicalunit evaluated the nurses’ opinion of the 5 concepts and the importance for establishing patientacuity for in-patient care. Interrater reliability among nurses was 87% with the author’s acuity tool.Key words: acuity, classification, patient care, retention, staffing
MANY ARTICLES have been dedicated tohealthcare issues such as nursing short-
age, higher patient acuities, decreased lengthof hospital stay, and rising healthcare costs.Almeida and Persson1 state that these issueshave become a major concern of consumers,healthcare professionals, providers, and pur-chasers. These changes within the healthcaresystem have led administrators to look for im-proved ways to manage a broken system.
Healthcare managers are constantly tryingto contain cost while still providing excel-lent patient care. The desire to control cost,however, has changed patient care. In thepast, doctors admitted patients the day beforesurgery. This provided ample time for the doc-
From the School of Nursing, University of Texas atArlington.
Corresponding author: Kelle Harper, BSN, RN, ER, Uni-versity of Texas at Arlington, FNP Student (e-mail:[email protected] or [email protected]).
tor and nurse to provide valuable postsurgi-cal and discharge teaching. To contain cost,however, hospital and insurance companiesno longer support this service. This decreasedlength of hospitalization ultimately increasedthe average patient acuity on care units.
Patient acuity is defined as the categoriza-tion of patients according to an assessmentof their nursing care requirements.2 Owing toincreased patient acuity in care units, nursesare taking care of more complex patientsthan in the past. Fagin3 notes that this situa-tion is complicated by the fact that increaseddemands for documentation mean that care-givers can devote fewer hours to direct careand monitoring. To counter these increasingneeds, hospital administrators have used pa-tient classification systems to document pa-tient acuity. These tools aid in gathering in-dividual patient care information, identifyingacuity ratings, determining staffing, and as-signing patient loads. The purpose of this pa-per is to review the literature on acuity tools,discuss the pros and cons of acuity tools,
284
Acuity Systems Dialogue and Patient 285
highlight currently available patient classifica-tion systems, and disseminate the data anddescription of the new Patient ClassificationSystemTM (PCS) acuity tool.
BACKGROUND
A literature search of Medline, Cumula-tive Index for Nursing and Allied Health(CINAHL), and PubMed using the searchterms acuity tools, acuity scales, patient clas-sification systems, and staffing tool identified4 concepts crucial in validating acuity toolsas they relate to patient and hospital man-agement: (1) improvement of patient care/outcomes, (2) proper staffing, (3) budgeting/cost containment, and (4) nurse retention.The next section will define these conceptsand how they relate to acuity tools.
Patient care/outcomes
A variety of issues have led to the inabil-ity to deliver quality healthcare. Nurses areexpected to give competent patient care de-spite a shortage of nurses, increased care re-sponsibilities, and higher patient’s acuities (in-cluding patients with multiple chronicities).Blegen et al highlight the importance of mea-suring and controlling patient acuity, whichthey identified as the “driver” of patientoutcomes.4 Nurses are responsible for provid-ing competent care to decrease the severityof illness and therefore decrease a patient’sacuity level.5 As leaders, nurse managers mustprovide an environment that supports nursesand ensures quality care.6
Proper staffing
Proper nurse staffing is an important part ofthe nurse manager’s job. Low nurse-to-patientratios are related to lower rates of adverse pa-tient outcomes.7 Aiken and colleagues foundthat when nurse-to-patient ratios go from 1:6to 1:4, patient death rates decreased by 2.3per 1000 patients. Cho et al found lower ratesof urinary tract infections, pneumonia, uppergastrointestinal bleeding, and shorter hospi-tal stays for patients in hospitals with low
registered nurse (RN) staffing versus thosewith high RN staffing.8 Hospitals where stan-dards allowed for fewer patients per nursehad lower patient mortality rates. Negativeoutcomes can be minimized or avoided, withcareful attention to managing nurse-to-patientratios.
Patient classification systems and acuitytools allow managers and administrators topredict staffing needs and more accuratelycontrol nurse-to-patient ratios. Parrinelloshowed that acuity tools allow staffingpredictions based on patient acuity as wellas monitoring nursing productivity andworkload.9 In addition, acuity tools can helpidentify census trends used to schedule staff.For example, if the patient classificationsshow that more postoperative patients returnto the unit on Wednesdays, the nurse managercan schedule more staff at that time to handlethe increased census. Patient classificationsystems can help avoid poor nurse-to-patientratios by allowing managers and nurses tomore accurately reflect staffing patterns andpredict future needs.
Budgeting/cost containment
Budgeting is an important part of the nursemanager’s job. Careful budgeting can be ben-eficial for the nurse, patient, and health-care system. Garretson notes hospital ad-ministrators are constantly reviewing budgetsand patient length of stay to facilitate theirinstitution’s financial security.10 Changes inthe way hospital services are reimbursed byMedicare/Medicaid and other insurance com-panies have forced many healthcare profes-sionals to change the way they manage patientcare.
This has led to focused cost-containmentefforts and a scrutiny of how resources areutilized.11 Nurses comprise the largest popu-lation of hospital employees and expense12;therefore, careful management is imperativein maintaining a balance between patient careand cost-effective budgeting.
One way to manage these complex bud-getary restraints is the use of a patient
classification system that allows managers totrack their expenses in terms of the care pa-tients receive.13 Without such tools, nursemanagers may be bound to external con-straints that may not reflect the needs of theirstaff and patients. Budreau et al stated thatnurse managers must manage their own coststo avoid controls initiated from within theorganization.11 The prudent nurse managercan select a patient acuity classification toolthat addresses the hospital administration’sneeds, but also reflects nurse and patient out-comes on the unit.
Nurse retention
Nurses have the honor of taking care of pa-tients during a time of immense need and lossof control. Nurses serve those who have un-met needs by using their skills and knowledgeto help other people. Why then are so manynurses burnt out, chronically calling-in sick,or leaving nursing altogether? Nurses feel aloss of control within their profession.14 Frus-trated over the lack of control and supportwithin the hospital, nurses are looking for jobsoutside the hospital setting. Reasons includethe physical and emotional stresses of the job,high acuity of patients, a perceived lack ofrespect, and a lack of voice and autonomywithin the workplace.
Nurses need a voice for the patients intheir care. Acuity tools and patient classifica-tion systems allow for such a voice, givingnurses a way to communicate their needs aswell as the needs of their patients. These toolsallow nurses to state the acuity of their pa-tient load, advocating for their patients’ needsand determining the requirements for qualitybedside care; however, the nurses themselvesmust have a role in implementing the acuitytool. “Involving the staff in the developmentof a patient classification system tool leadsto an efficient and staff-valued tool.”15 Thisinvolvement of nurses in determining acuityand staffing can appeal to nursing satisfactionand retention.
Systematic changes within healthcare haveaffected patients, nurses, and managers. The
development of patient classification sys-tems and acuity tools has improved patientcare/outcomes, staffing, budgeting/cost con-tainment, and nurse retention. Appropriatelyused, these tools can help nurses and man-agers create a successful care environment.Therefore, it is beneficial to know their weak-ness and limitations to facilitate better utiliza-tion and implementation of these tools.
DEVELOPMENT OF PATIENT
CLASSIFICATION SYSTEM TOOLS
Although patient classification/acuity toolsare widely used by hospital management, onlymodest research exists on these tools. Fewstudies have been dedicated to establishing re-liability and validity. Furthermore, researchershave failed to determine what makes a qualitypatient classification tool. A review of litera-ture identified key concepts that make a qual-ity acuity tool: the tool involves the nursingprocess, proves adaptable and flexible, andhas credibility (reliability and validity).13,16–20
These concepts are crucial in developinga tool that continues to be relevant tomanagement.
Nursing Process
The nursing process is the “gold standard”by which nurses give prudent patient care;however, many patient classification tools donot accurately measure the social and psy-chological aspects of the nursing process.McNaughton14 writes that patient classifica-tion tools are “task oriented” and do notconsider the professional components of thenursing process. For example, a nurse takingcare of a patient after a total mastectomy willhave various care activities. The activities willprobably include JP drain care, pain control,monitoring blood loss, blood pressure, andurinary catheter care. These are tangible tasksthat can easily be measured on an acuity tool.The emotional aspect of the patient, however,is equally important in the nursing process.The patient must cope with the emotionaloutcomes of the surgery itself, including
Acuity Systems Dialogue and Patient 287
body image disturbances, feelings of inade-quacy, and loss of self-esteem. The nurse hasan important role in the recuperation of thepatient that includes mental health. The nurs-ing process should be an important criterionwhen selecting an acuity tool.
Adaptability and flexibility
The adaptability and flexibility of a patientclassification tool has important ramificationson multidisciplinary use. Rigid tools do nottake into account the uniqueness of differenthospitals, units of care, or patients. An effec-tive tool should be adaptable to different envi-ronments while accomplishing the same acu-ity goals. According to Stilwell and Hawley,lack of flexibility within an acuity tool canhinder staffing; however, acuity tools shouldallow care units to forecast staffing needs,such as new admissions and unexpected dis-charges, rather than simply react to the fluiddemands of staffing.21 The ability to forecastis an important step in the development ofacuity tools, and provides the flexibility andadaptability necessary to predict staffing andbudgeting.
Credibility (reliability and validity)
Modest research exists on validity and re-liability testing for acuity tools. Despite theshortage of research, the lack of a valid andreliable tool was considered an issue for man-agers and nursing staff. Hastings reportedthat a credible ambulatory care patient clas-sification tool was nonexistent.22 The JointNursing Practice Commission and Dumpeldetermined that nurses in California, wherehospitals are required to use acuity tools,are concerned that the tools lack adequatecredibility.23 “Few tools are available andthose cited in the literature tend to report min-imal validity and readability and lack applica-bility to the setting.”24 In addition, the imple-mentation of the tools is dependent upon thenurses using them for accuracy. Nurses havevarying skill and education levels; these dif-ferences are not addressed in current acuitytools.
Although patient classification/acuity toolsare widely used by hospital management, onlyminimal research exists on these tools, par-ticularly regarding the credibility of the tools.Despite these shortcomings, these tools offergreat promise for managers in balancing thecomplex and often difficult demands of man-aging rising costs, shrinking budgets, and di-verse patient loads.
TYPES OF ACUITY TOOLS
Patient classification systems have beenused since the 1960s. These systems wereoriginally designed for the purpose of “fore-casting staffing needs” and to “project andmonitor workload.”23 There are 2 types of pa-tient classification tools recognized in the lit-erature: time/motion studies or a patient carechecklist with assigned acuity scores/ratings.
Acuity tools that are based on time/motionstudies were developed from the industrialmodel of Malloch and Conovaloff25; however,their model does not take into account holis-tic patient care. In addition, time/motion stud-ies do not consider (a) transfers, admissions,or discharges; (b) interruptions in work flu-ency; (c) family dynamics; and (d) ethical,social, or psychological factors. Malloch andConovaloff stated that time and motion stud-ies do not capture nursing multitasking. As aresult, these inefficient acuity tools can leadto overstaffing and budgeting problems.
Patient care checklists with assigned acuityscores/ratings are abundant within the litera-ture. This type of rating system has the care-giver check off each patient’s care needs, ap-ply predetermined point values to each careneed, and add up the points for each pa-tient. This type of acuity tool can be simplya checklist created by the unit manager ora complex computer-based patient classifica-tion program such as the Sunrise Patient Acu-ity (Van Slyck & Associates and Eclypses) orthe Trend Care Systems (Trend Care SystemsPty Ltd).
When nurse managers are designing or se-lecting a classification tool, the subjective or
objective nature of the tool should be consid-ered. Acuity tool subjectivity allows nursingstaff and management to manipulate the re-sults. Skewing results can then lead to frus-trated managers and dissatisfied employees.For example, charge nurses can skew acuitytool data to create a need for more nurseson a particular shift. The nurse manager canalso manipulate data to support an increasedbudget proposal. Malloch and Conovaloff sug-gest complete objectivity is an important con-cept when designing a new acuity tool thoughit will be hard to obtain.26 A computerizedpatient classification tool can achieve objec-tivity by automating patient care documenta-tion during computer charting. The SunrisePatient Acuity Scale (designed by Van Slyck &Associates) is an example of a computerizedprogram that uses this type of programming.The benefits and limitations of subjective ver-sus objective patient classification tools mustbe part of any selection criteria for nurse man-agers considering the implementation of anacuity tool.
As healthcare advances, and the require-ments upon nurses to deal with increas-ingly complex disease processes progress,and higher acuity patients expand, the nurs-ing profession must demand a broader viewof patient acuity than a simple checklist ormodel. The abundance of acuity tools can bedaunting and the distinctions between themcan be pronounced or subtle. Nurse managersmust therefore take the time to determine thedistinctions between tools and implement atool that suits their hospital, nursing staff, andpatient needs.
DEVELOPMENT OF THE PATIENT
CLASSIFICATION SCALE
The Patient Classification Scale (PCS) wasdeveloped because of the need for a more ef-fective acuity scale. The instrument, a patientacuity rating system, is a simplistic, adapt-able, nurse-oriented tool, designed to en-hance communication and productivity whileimproving nurse and patient satisfaction. The
PCS was developed in a small rural hospi-tal where a productivity scale exclusively as-sisted in assigning rooms for new patient ad-missions. The former productivity scale wasbased on a ratio of nurses/patient-care techni-cians to patient census and focused primarilyon the financial burden of providing inpatientcare. As admissions of increasingly ill pop-ulations with multiple morbidities grew, thestaff experienced frustrations from the over-whelming load. Realizing communication be-tween management and staff needed to im-prove, the PCS was developed.
To develop a new tool, the problem areasneeded to be determined. Answers to ques-tions such as, “What takes a nurse so longat the bedside?” and “What is needed to staffeffectively and maintain patient safety whileproducing desirable patient outcomes?” wereconsolidated into five broad concepts for thedevelopment of a useful new tool: (1). medi-cations, (2) complicated procedures, (3) edu-cation, (4) psychosocial issues, and (5) com-plicated intravenous medications.
In consideration of these concepts, the bur-den of providing holistic care in an inpatienthospital setting needs to be succinctly andsimply conveyed from the nurse at patientbedside to the managers performing bed as-signments. The PCS was developed to simplyand accurately perform that task. With thatgoal in mind, these task-oriented, time-takingduties became the key concepts for the PCStool.
Concepts and variables
The concepts of the PCS define a patient’sacuity status by balancing patient hospitalneeds along with nursing tasks. The conceptsalso distinctively address patients’ educationalneeds as well as the underlying emotional orpsychosocial needs for holistic healing. Theconceptual map (Fig 1) demonstrates howeach of these inpatient concepts interlink, in-fluencing each other while continuously re-volving around the patient. A bedside nursemust consider each of these patient conceptswhile also addressing the patient’s illness.
Acuity Systems Dialogue and Patient 289
Figure 1. Patient Classification System concepts.
Each concept addressed in the PCS has auniquely definitive measure of nursing careprovided at the bedside. Specific variablescommon to most nursing unit populationswere used to formulate these concepts. Adraft of the envisioned PCS was presented toa group of 12 medical-surgical nurses and the5 proposed categories were unanimously sup-ported. Conceptual definitions are listed inTable 1.
Table 1. Patient Classification System conceptual definitions
Medications The number of medications a patient receives during a 12-h nursing
shift that must be verified against a medical doctor’s order and
based on standards of medication delivery.
Complicated Procedures Task- and time-oriented procedures carried out to perform
competent patient care in management of disease process and
prevention of complications.
Education Requirements for complex patient care encompassing teaching
about disease processes, procedures, preventive measures, and
standard facility protocols.
Psychosocial Nursing tasks related to monitoring and intervention correlating
with mental disabilities, end-of-life care, palliative care, and
including personal or family dynamics.
Complicated IntravenousMedications
Task- and time-oriented distribution and monitoring of intravenous
medications, blood or blood products, or hemodynamic
monitoring of vascular access.
Once the concepts were identified, vari-ables relevant for each concept were listedand ranked from 1 to 4. A higher level indi-cates a higher patient acuity. For example, thevariable “tube feeding”ranked a level 4 in theComplicated Intravenous Medications cate-gory since it takes more time than the variable“blood sugar monitoring”ranked a level 1. Un-like the previously mentioned 5 concepts, thevariables have the ability to change according
Table 2. Patient Classification System variable examples
Rural medical- Urban short stay Urban medical-
surgical unit overflow unit surgical unit
Medications Based on number of
medications
distributed per shift
Based on number of
medications
distributed per shift
Based on number of
medications
distributed per shift
ComplicatedProcedures
Pediatric case
Continuous bladder
irrigation
Chest tube monitoring
Wound care
Telemetry monitoring
Bariatric monitoring
Ileostomy/colostomy
Education Ranged from basic
education to
disease-specific
education; also
included monitored
indicators
Ranged from basic
education to
disease-specific
education; also
included monitored
indicators
Ranged from basic
education to
disease-specific
education; also
included monitored
indicators
Psychosocial Remained same Remained same Remained same
Complicated IVsandMedications
IDDM/sugar monitor
Heparin
Cardiac drip
Potassium rider
PICC/central line
Tube feedings
to the unit and environment utilizing the tool.Examples of the different variables chosen byeach specific unit piloting the PCS are listed inTable 2. The arrangement of variables definesthe accurate acuity level of the patient.
Medications were scored on a level of 1 to4 depending on the number of medicationsthe nurse was responsible for giving and accu-rately checking for each patient. The variablesfor Education remained the same from unitto unit, primarily focusing on basic educationfor common diseases such as congestive heartfailure, diabetes, and smoking cessation. Edu-cation also included consideration for multi-ple chronicities, as well as the pre and postprocedures of monitoring and preparation.The Psychosocial category reflected illnessessuch as depression, bipolar disorder, and pal-liative care. This category also included familydynamics in the highest acuity ranking. Theability to allow each unit to choose variablessuited for their specific population and spe-cialty concerns not only defined their acuitybut also enhanced communication about spe-cific patient requirements.
Besides using the PCS as an acuity measurefor patient placement, the rural unit also used
the PCS tool as a means of giving report fromshift to shift. This not only ensured shift up-dates regarding the acuity level of patients butalso ensured accurate information exchangebetween staff, interdisciplinary departments,and middle management positions.
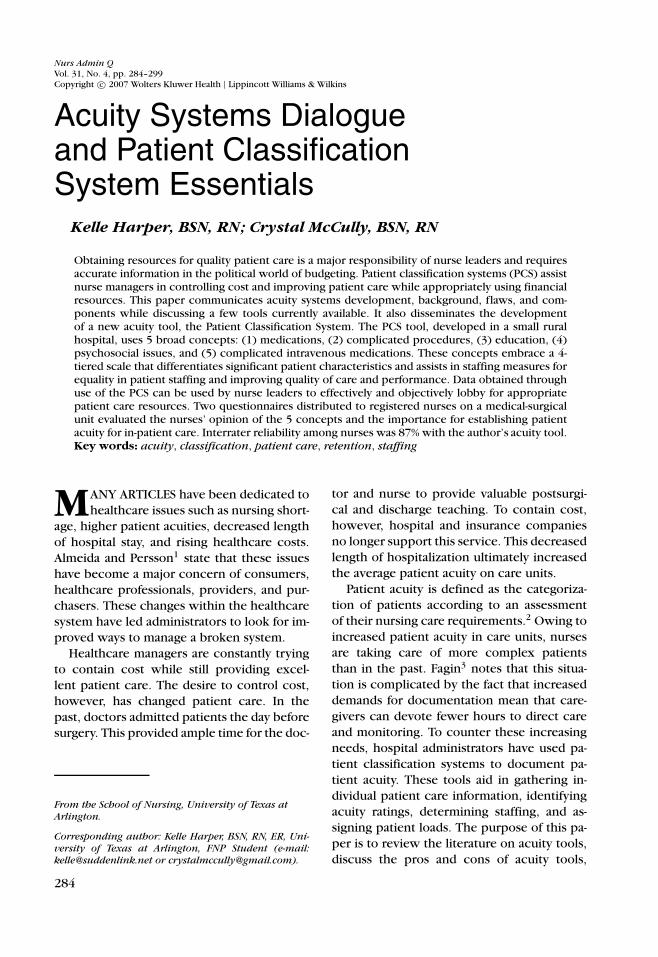
Acuity ranking
The simplicity of the PCS is found in the lay-out (Fig 2). The nurse begins ranking the pa-tient with the highest classification, column 4.If the patient met the criteria set by the vari-ables for the fourth category, the nurse’s ob-jective is fulfilled. A 4 is placed in the scorecolumn of that particular concept and thisprocess continues until each concept row hasbeen scored. Once a total sum of all conceptsis achieved, it is divided by 5, the number thatreflects the 5 major concepts. The final num-ber becomes the patient’s acuity rating. Sinceoften the final number is not a whole num-ber, nurses must round to the nearest wholenumber.
Reliability and validity
In the test studies, this tool was well re-ceived. Participants particularly liked that the
Acuity Systems Dialogue and Patient 291
Figure 2. Patient Classification System. Copyright 2003, K. Harper.
development started with the bedside nursewho developed variables that reflected nurs-ing concerns and demands. A multimodal pro-cess was used to validate the PCS tool. Partici-pation was strictly voluntary and anonymous.
Two questionnaires were distributed forevaluation to RNs working on a medical-surgical unit as either staff, middle manage-ment as charge or coordinators, or an educa-tional specialist. Nurses had an opportunity to
look at the PCS, read an explanation of howto use it, and then apply the tool to a patient.Once the tool was used, nurses could com-plete the questionnaires to evaluate the PCS.
The first questionnaire was an 8-item Lik-ert scale questionnaire with 6 questions,each having a 5-item response. The responsesranged from “extremely effective” to “very in-effective.” The last 2 questions allowed forprofessional opinions on the strengths and
weaknesses of the tool. These opinions are re-ported later.
The second questionnaire, a relevance-rating tool, assessed the nurse evaluator’s ex-pert opinion of the 5 concepts of the PCS tooland the concept’s perceived importance forestablishing patient acuity for inpatient care.After a 2-week period, 14 effectiveness ques-tionnaires, 10 relevance questionnaires, and31 completed “practice” tools were availablefor analysis. Any questionnaire with missingratings was not used for data analysis.
In addition to these data sets, 15 PCS toolswere completed to help establish interraterreliability. These 15 tools rated 5 patientswho were each evaluated by 3 nurses duringthe same 12-hour shift. The nurses were in-structed not to collaborate on patient ratings.The charge nurse of each shift was also madeaware of this process and helped to facilitatethe effort to collect accurate data.
Effectiveness
Nursing opinion of the effectiveness of thePCS tool as evaluated via the first question-naire is depicted in Figure 3. Effectiveness wasdetermined by a rating greater than “neutral.”The bullets below summarize the findings.
• Seventy-seven percent (n = 12) rated thetool effective in its ability to serve as anurse’s voice about the patient’s care.
Figure 3. RN opinion of effectiveness of PCS tool.
patients, showing its usefulness instaffing considerations.
• More than 55% (n = 7) believe the cat-egories represent the patient accurately,while 45% (n = 6) rated this question inthe neutral response.
• Fifty-eight percent (n = 10) stated thetool could be completed in a timelymanner.
Relevance
Figure 4 shows the analysis of the ratingsof the 10 “relevance” questionnaires. Of the10 RNs evaluating the tool, 3 were nurseeducators, 2 were clinical coordinators orcharge nurses, and 5 were staff nurses in ametropolitan hospital on a medical-surgicalfloor. All agreed that the concept of medi-cation administration must be consideredin acuity standards. In contrast, complicatedintravenous (IV) medications and psychoso-cial issues were the only conceptual cate-gories to be ranked in the “not relevant cat-egory,”though only 10% (n = 1) ranked thesecategories in this manner (ie, only 1 of 10 ex-perts considered these concepts irrelevant).No explanations of ratings were shared by theRN. The conceptual categories of educationand complicated procedures were ranked byone RN as “unable to determine relevance.”
Overall, the 5 conceptual categories in thePCS tool maintained an “effective” contentvalidity index.27 the index is determined by
Acuity Systems Dialogue and Patient 293
Figure 4. RN opinion of PCS relevance.
comparing the number of experts ranking themeasure in the “relevant” or “extremely rele-vant”category to the “greater than”or “major-ity rankings.” This is an opinion-based analy-sis using the expertise of professionals in theirspecific field. In this analysis, only 1 reviewerranked 4 of the 5 categories below the “rele-vant” rating. Therefore, the majority opinionof each category achieves the measure of “rel-evant”and “succinct.”
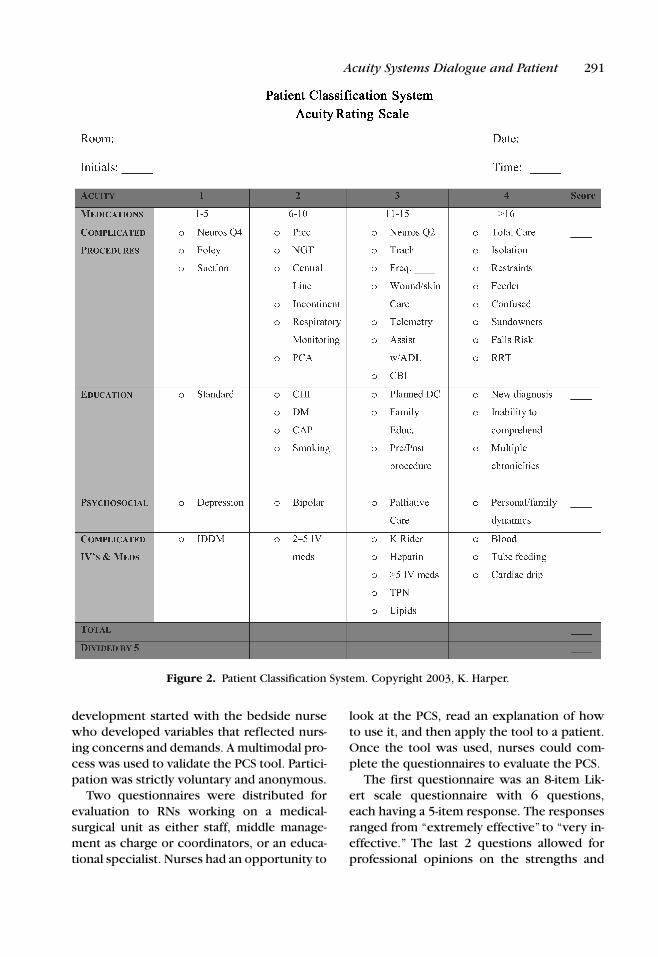
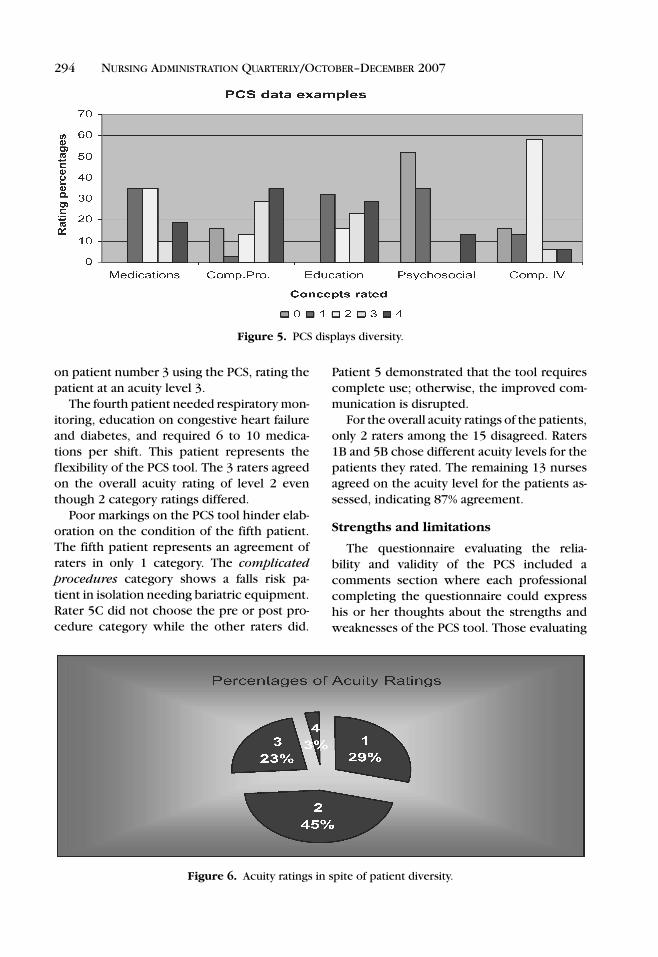
The 2 charts in Figures 5 and 6 show therating results of the 31 sample tools used bynurses to rank their patients during the pilotperiod. Figure 5 reflects the diversity of pa-tient care captured by the PCS tool.
The next chart, however, shows how thedifferences of patient diversity will not skewthe patient acuity ratings. Although the manydifferent ratings occur, 45%, almost half of thepatient population remained within acuitylevel 2 and 29% ranked in level 1. If the ma-jority of patient acuity remains within levels 1or 2, then the higher acuity patients, those re-quiring more complex care, can be dispersedequally among the staff. This promotesbetter harmony with equal patient loads. Inaddition, this approach better disseminatesvaluable information about patient careamong staff, while also allowing middle man-
agement to catch a glimpse of the demandsof patient care.
Interrater reliability
Fifteen of the completed PCS tools com-pared the ability of 3 nurses to rate 1 patientthe same way without collaboration dur-ing the same 12-hour shift. Figure 7 demon-strates the evaluators’ ratings for the 5patients. The first patient had multiplechronicities including atrial fibrillation, di-abetes, high blood pressure, and multiplemyeloma as well as reverse isolation. Raters1A and 1C both ranked the patient at anacuity level 4. Rater 1B ranked the patient,however, at an acuity level 2.
The second patient who had sundownerssyndrome was at risk for a fall. Needs includededucation about multiple chronicities, chal-lenging personal and family dynamics, and fre-quent insulin monitoring. The 3 raters rankedthe second patient identically. This patientwas an acuity level 3, with 1 to 5 medicationsdistributed per shift and requiring wound carefor more than 10 minutes.
The third patient required low wall suctionof a nasogastric tube, dressing changes, infu-sion of total parenteral nutrition (TPN), andwas considered a falls risk. The 3 raters agreed
on patient number 3 using the PCS, rating thepatient at an acuity level 3.
The fourth patient needed respiratory mon-itoring, education on congestive heart failureand diabetes, and required 6 to 10 medica-tions per shift. This patient represents theflexibility of the PCS tool. The 3 raters agreedon the overall acuity rating of level 2 eventhough 2 category ratings differed.
Poor markings on the PCS tool hinder elab-oration on the condition of the fifth patient.The fifth patient represents an agreement ofraters in only 1 category. The complicatedprocedures category shows a falls risk pa-tient in isolation needing bariatric equipment.Rater 5C did not choose the pre or post pro-cedure category while the other raters did.
Figure 6. Acuity ratings in spite of patient diversity.
Patient 5 demonstrated that the tool requirescomplete use; otherwise, the improved com-munication is disrupted.
For the overall acuity ratings of the patients,only 2 raters among the 15 disagreed. Raters1B and 5B chose different acuity levels for thepatients they rated. The remaining 13 nursesagreed on the acuity level for the patients as-sessed, indicating 87% agreement.
Strengths and limitations
The questionnaire evaluating the relia-bility and validity of the PCS included acomments section where each professionalcompleting the questionnaire could expresshis or her thoughts about the strengths andweaknesses of the PCS tool. Those evaluating
Acuity Systems Dialogue and Patient 295
the PCS also offered suggestions for enhanc-ing the program. Comments are listed inTable 3.
A limitation noted during the pilot periodwas the need for education on appropriatelycompleting the tool, as evidenced by 32%(n = 5) rating the tool ineffective in beinguser friendly. Two RNs suggested an in-servicewould better help in understanding the tool.The PCS was also developed for manual com-pletion and has not been tested in a comput-erized setting.
Figure 7. Patient 1 through patient 5. (continues)
Finally, the PCS has been tested in only 3nursing specialty settings, 2 medical surgicalfloors, and an overflow unit. Further studieswould help highlight any issues for validity ofthe tool in other nursing settings.
Comparison with other tools
There are many differences between thePCS and other acuity tools. A primary ob-jective of the PCS tool is to incorporatetime-oriented nursing tasks. Most nurses
Figure 7. (Continued) Patient 1 through patient 5.
Acuity Systems Dialogue and Patient 297
Table 3. Reported strengths and weakness of the Patient Classification Scale
Strengths “A start to classifying patients concretely”
“It should help with making fair assignments”
“Good categories”
“Working at the number of medications given during the shift is great”
“User friendly, very uncomplicated tool”
“Includes psychosocial and education”
“Includes education and psychosocial considerations”
“The strength is in the acuity measurements”
“Great baseline and guide for assignments and helpful quick reference”
“It shows what is really wrong with the patient”
“It evaluates the time and frequency required for interventions”
Weaknesses “Not sure if all information is effectively captured”
“When adding up the score and dividing by 5, I don’t believe the scale is accurate at all”
“Confused about the standard of medication”
“It is somewhat confusing at the beginning”
“How would you go about making patient assignments with the acuity numbers?
“How do you avoid one nurse being assigned a higher acuity”
“Not sure how the tool is used for assignments or the total assignments a nurse has”
“Must have unit-specific information, which could be biased. Unit consensus may be
difficult to obtain. Suggest to give more information on staffing ratios”
“May need more variables to each concept”
“It takes too long”
agree the time taken at the bedside to givecompetent nursing care is an effective reflec-tion of patient acuity. While time managementis considered in all conceptual fields, medica-tion distribution, performance of nursing pro-cedures, and management of complicated IVmedications demand the highest priority intime management.
The primary focus of the PCS tool is the pa-tient, not the financial priorities of an institu-tion. However, use of the PCS to documentactual care provides data for nurse leaders touse in making a case to fund appropriate re-sources for patient care. Communication ofpatient acuity begins at the bedside with thefirst inpatient nurse who assesses the patient.The acuity level is then reevaluated everyshift using the PCS. The tool accommodateschanges that patients experience throughouta hospitalized illness episode. Because thetool as currently designed is paper based andnot computer based, it does not have to bea permanent part of the chart and as suchcan be used as a “kardex.” Along with the fo-
cus on nurse-patient needs, the PCS tool in-cludes patient education and psychosocial is-sues needed for holistic care. Finally, the PCStool can be used as a means of report, for in-terdisciplinary communication, and to makeappropriate assignment of those patients be-ing admitted to the unit.
Implications for nursing managers
The simplistic nature of the PCS tool, hav-ing only 4 levels for acuity, makes this acuitysystem unique. The tool’s ability to differen-tiate significant patient characteristics allowsfor equality in patient dispersal among staff.Differentiating patient characteristics makesmanaging patient care easier since all level4 patients will not be cared for by the samenurse.
The education component provides an ad-ditional use beyond addressing education ofillness and disease process. The trial hospi-tals chose to place their critical nursing indica-tors for patient outcome measurements in the
education category, which ensured patientswere easily identified who needed to receiveeducation on a particular topic. This helpedto remind nurses to perform particular taskssuch as giving smoking cessation packets or adaily weight refrigerator grid to patients withcongestive heart failure.
One manager hopes to utilize the tool asa means of discussion, giving light to yet an-other use of the PCS tool. At times the man-ager has found the numbers of nurses orpatient care technicians exceed the allottedstaffing productivity numbers. The PCS willbe used as a source to justify the need for theextra staff by objectively describing the pa-tient load and burden of care placed on staffto meet each patient’s specific needs.
CONCLUSIONS
In conclusion, the PCS tool serves as a re-port tool, education reminder, holistic per-spective of patient needs, and voice for man-agers when rebuttal is needed for overstretch-ing productivity numbers. The tool can alsobe a nurse’s voice about the rigorous de-mands and time-consuming tasks that mustbe performed for varied hospitalized popula-tions and serves as a means of communica-tion to others not at the bedside. Systematicevaluation of this tool revealed that with ad-equate education about the tool’s applicationand more user-friendly instruction, the PCS isa major asset for nursing management, staff,and, most important, the patient.
REFERENCES
1. Almeida RT, Persson J. The use of and need for pa-
tient classification systems in Swedish neonatal care.
Scand J Caring Sci. 1998;12:11–17.
2. Lazerowich V . Development of a patient classifica-
tion system for a home based hospice program. JCommunity Health Nurs. 1995;12(2):121–126.
3. Fagin CM . When Care Becomes a Burden: Dimin-ishing Access to Adequate Nursing. New York: Mil-
bank Memorial Fund; 2001.
4. Blegan MA, Goode CJ, Reed L. Nurse staffing and pa-
tient outcomes. Nurs Resour. 1998;47:43–50.
5. Van Slyck A, Johnson KR. Using patient acuity data to
manage patient care outcomes and patient care costs.
Outcomes Manag Nurs Pract. 2001;5(1):36–40.
6. Disch J, Beilmann G, Ingbar D. Medical directors
as partners in creating healthy work environments.