1 of 2 www.wakegov.com Wake County Human Services Board October 25, 2012 AGENDA Human Services Center 220 Swinburne St., 2nd Fl., Rm. 2132 Standing Time: 7:30AM – 10:00AM Dianne Dunning, Chair Pablo Escobar, Vice Chair Purpose: Advocacy, Policy, Advisory, Accountability --James A. Smith, III, MD, (Psychiatrist) - Oct. 2, 2012 - Nov. 14, 2015 8:05 am Elections of 2013 Board Officers 8:15 am Public Health Committee: Mr. Benny Ridout, Chair • Review/Discuss Public Health Quarterly Report (Apr.-Jun 2012) - (#2.4) - Dr. Edith Alfano, Epidemiologist & Ms. Sue Ledford, PH Administrator 8:30 am Board Interviews: 8:30am - John H. Myhre, (Pharmacist) 9:00am - Rosine L. Sanders, (Psychologist) 7:30 am Meeting Called to Order Invocation Approval of Minutes: September 27, 2012 Next Board Meeting: November 15, 2012 (**3rd Thursday) 7:35 am Oath of Office - Commissioner James West 7:40 am Recognition of Departed/Departing Board Members: 1. Kent Earnhardt: Feb. 15, 2010 - Aug. 01, 2012 2. Richard G. Greb: Aug. 02, 2004 - Aug. 01, 2012 3. Jeffrey K. Smith: Mar. 21, 2005 - Aug. 01, 2012 4. Burton A. Horwitz: Nov. 15, 2004 - Nov. 14, 2012 5. Benny Ridout: Jun. 24, 2004 - Nov. 14, 2012 7:55 am Recognition of Dr. Peter Morris Dr. Morris has been appointed Executive Director of Urban Ministries effective December 4, 2012. A Human Services Reception will be held November 30 th , 2:30pm – 4:30pm, Rm. 5032 Regular Agenda
--James A. Smith, III, MD, (Psychiatrist) - Oct. 2, 2012 - Nov. 14, 2015
8:05 am Elections of 2013 Board Officers
8:15 am Public Health Committee: Mr. Benny Ridout, Chair
• Review/Discuss Public Health Quarterly Report (Apr.-Jun 2012) - (#2.4) - Dr. Edith Alfano, Epidemiologist & Ms. Sue Ledford, PH Administrator
8:30 am Board Interviews:
8:30am - John H. Myhre, (Pharmacist) 9:00am - Rosine L. Sanders, (Psychologist)
7:30 am Meeting Called to Order
Invocation
Approval of Minutes: September 27, 2012
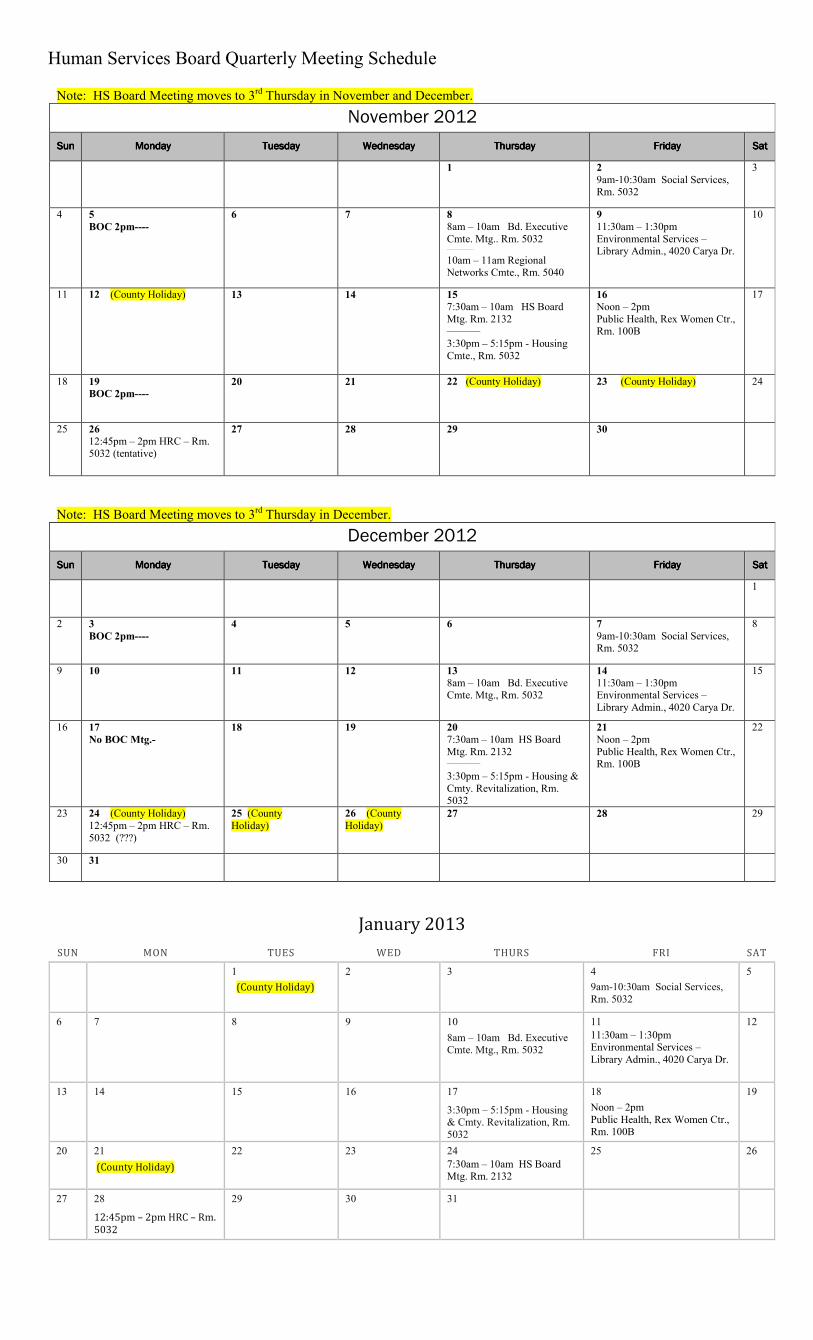
Next Board Meeting: November 15, 2012 (**3rd Thursday)
7:35 am Oath of Office - Commissioner James West
7:40 am Recognition of Departed/Departing Board Members: 1. Kent Earnhardt: Feb. 15, 2010 - Aug. 01, 2012
2. Richard G. Greb: Aug. 02, 2004 - Aug. 01, 2012 3. Jeffrey K. Smith: Mar. 21, 2005 - Aug. 01, 2012 4. Burton A. Horwitz: Nov. 15, 2004 - Nov. 14, 2012 5. Benny Ridout: Jun. 24, 2004 - Nov. 14, 2012
7:55 am Recognition of Dr. Peter Morris Dr. Morris has been appointed Executive Director of Urban Ministries effective December 4, 2012. A Human Services Reception will be held November 30
• Review Example of a Committee Structure. (Collect Feedback from Board and Committees)
Human Services Mission Statement
Wake County Human Services in partnership with the community will anticipate and respond to the public health, behavioral health and the economic and social needs of Wake County residents. We will coordinate and sustain efforts that assure safety, equity, access and well-being for all. - December 2006 _____________________________________________________________________________
Environmental Services Mission Statement
To protect and improve the quality of Wake County’s environmental and ensure a healthy future for its citizens through cooperation, education, management and enforcement. Environmental Services combines:
• water quality
• air quality
• solid waste (recycling, landfills, etc.)
• environmental health and safety (sanitation inspections, pest management, swimming pool regulations, animal control)
Recognition to 2012 Departed/Departing Board Members
1. Kent Earnhardt February 15, 2010 – August 1, 2012 -Consumer & Family Advisory Committee -Human Rights/Consumer Affairs Committee -LME Advisory Committee
2. Richard G. Greb August 2, 2004 – August 1, 2012 -Chair, LME Human Rights Committee -Past Chair, Human Rights/Consumer Affairs Committee
3. Jeffrey K. Smith March 21, 2005 – August 1, 2012 -Consumer & Family Advisory Committee -LME Advisory Committee -Environmental Services Committee
4. Burton A. Horwitz November 15, 2004 – November 14, 2012 -Social Services Committee -Public Health Committee
5. Benny Ridout June 24, 2004 – November 14, 2012 -Chair, Public Health Committee -Regional Networks Committee -Environmental Services Committee -Board Advocacy Workgroup -Board Appeal Hearing Panel
SLATE for
2013 BOARD CHAIR and VICE CHAIR
Wake County Human Services Board (Open Nominations and Vote at the October 25 Board Meeting)
Nominations for Board Chair
Pablo Escobar Mr. Escobar has been nominated for the Office of Board Chair. Mr. Escobar is completing his
second term as Board Vice Chair (2011 and 2012). He is also Chair of the HRC/Consumer
Affairs Committee. He has been a member of the Board since December 2008.
Nominations for Board Vice Chair
Leila Goodwin Ms. Leila Goodwin has been nominated for the office of Board Vice Chair. She has served as
Chair of the Environmental Services Committee since her Board appointment in November
2010.
VOTING PROCESS:
Election of Chair and Vice-Chair will be held at the October 25 Board meeting. After opening
the floor for additional nominations, votes will be taken in open session for each office.
To be elected Chair or Vice-Chair, a candidate must receive a minimum number of votes equal
to a majority of the duly appointed and currently serving members of the Board. If no candidate
for an office receives a majority of the votes, a run-off will then be conducted between the two
candidates receiving the greatest number of votes.
EFFECTIVE DATE:
Terms for Board Officers take effect at the December Board meeting.
HUMAN SERVICES AND ENVIRONMENTAL SERVICES
BOARD AGENDA ITEM
Agenda Date: Executive Committee: October 11, 2012
HS & ES Board: October 25, 2012
Committee/Item: Public Health Committee/Public Health Quarterly Report April –June2012
Specific Action Requested: Receive Public Health Quarterly Report
Item Summary: The Public Health Quarterly Report is published by WCHS Public Health
Division. This report highlights communicable disease data and includes data from the second
quarter of calendar year 2012.
Purpose for Action (Proposed Solutions/Accomplishments):
Public Health Accreditation requires that “The local health department shall analyze and note
reportable events occurring within the community and shall report atypical incidence, if any, to the
Division and the local board of health” (Benchmark 2 Activity 2.4).
Next Steps:
Accept quarterly report and use as needed to inform discussions, decisions and advocacy efforts
related to public health.
Attachments: Public Health Quarterly Report April – June 2012
Opportunities for Advocacy, Policy or Advisory: (see next steps)
Connections to Other Committees: Environmental Services
W A K E C O U N T Y
H U M A N S E R V I C E S
P U B L I C H E A L T H
Q U A R T E R L Y R E P O R T
S P E C I A L E D I T I O N :
C O M M U N I C A B L E D I S E A S E S
A P R I L — J U N E 2 0 1 2
Wake County Human Services
Public Health Division
10 Sunnybrook Road
P.O. Box 14049
Raleigh, NC 27620-4049
www.wakegov.com
SEPTEMBER 17, 2012
P u b l i c H e a l t h Prevent · Promote · Protect
Ramon Rojano, Human Services Director
Sue Lynn Ledford, Public Health Division Director
Editor-in chief: Edie Alfano–Sobsey, Public Health Epidemiologist
Editorial Staff: Roxanne Deter, Public Health Nurse and
Carla Piedrahita, Public Health Educator
Design and Layout: Michelle Ricci, Public Health Educator
2 2
Table of Contents
Topic Page
Introduction 3
Wake County Communicable Disease Morbidity 2008-2011 4 & 5
Foodborne Illness 6
Tickborne Illness 6
Tuberculosis 7
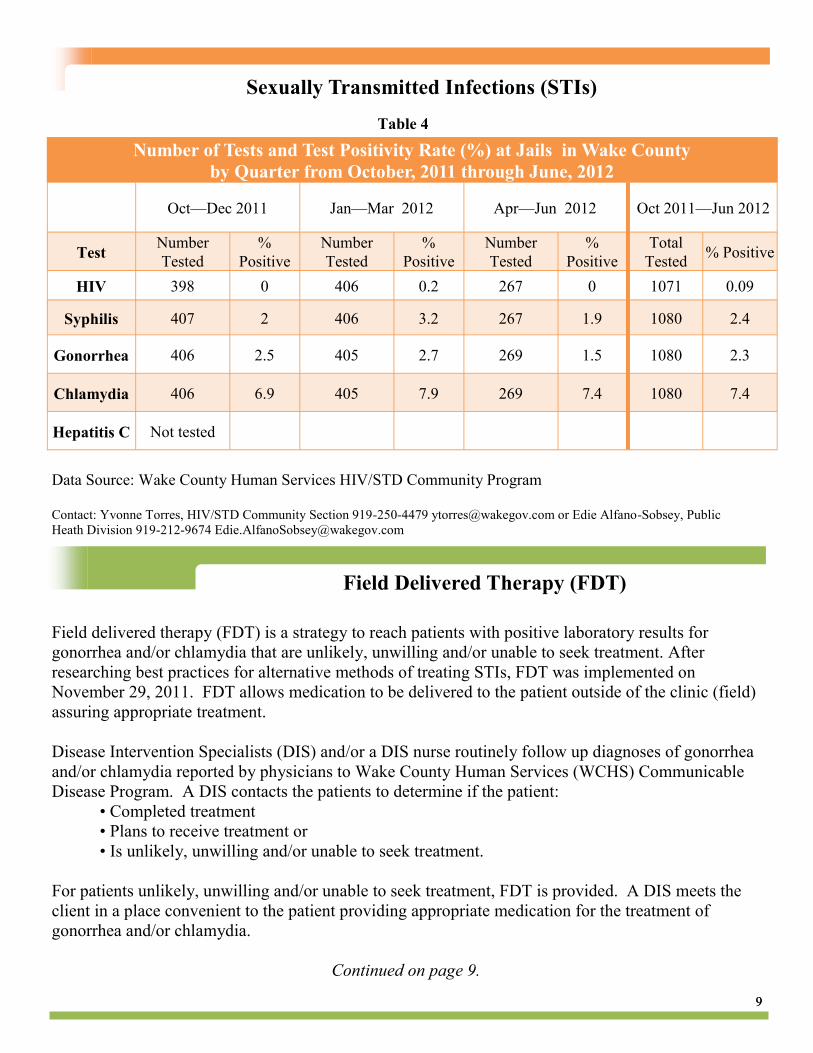
Sexually Transmitted Diseases 8 & 9
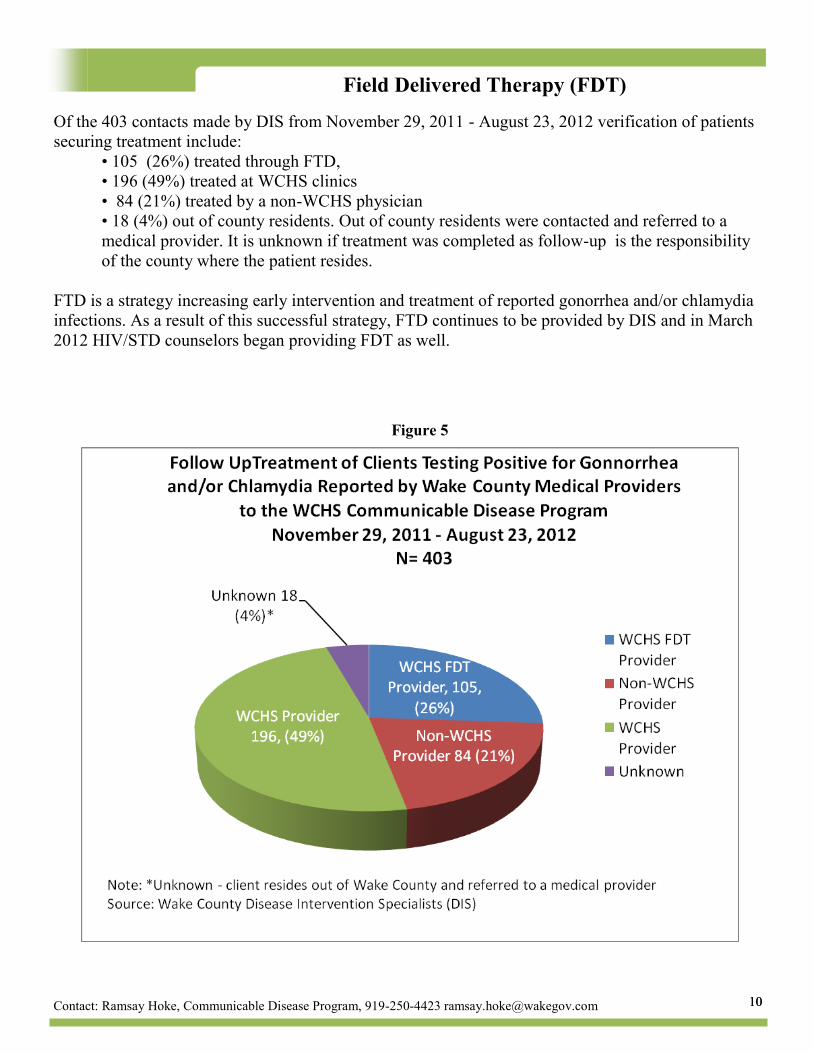
Field Delivered Therapy 9 & 10
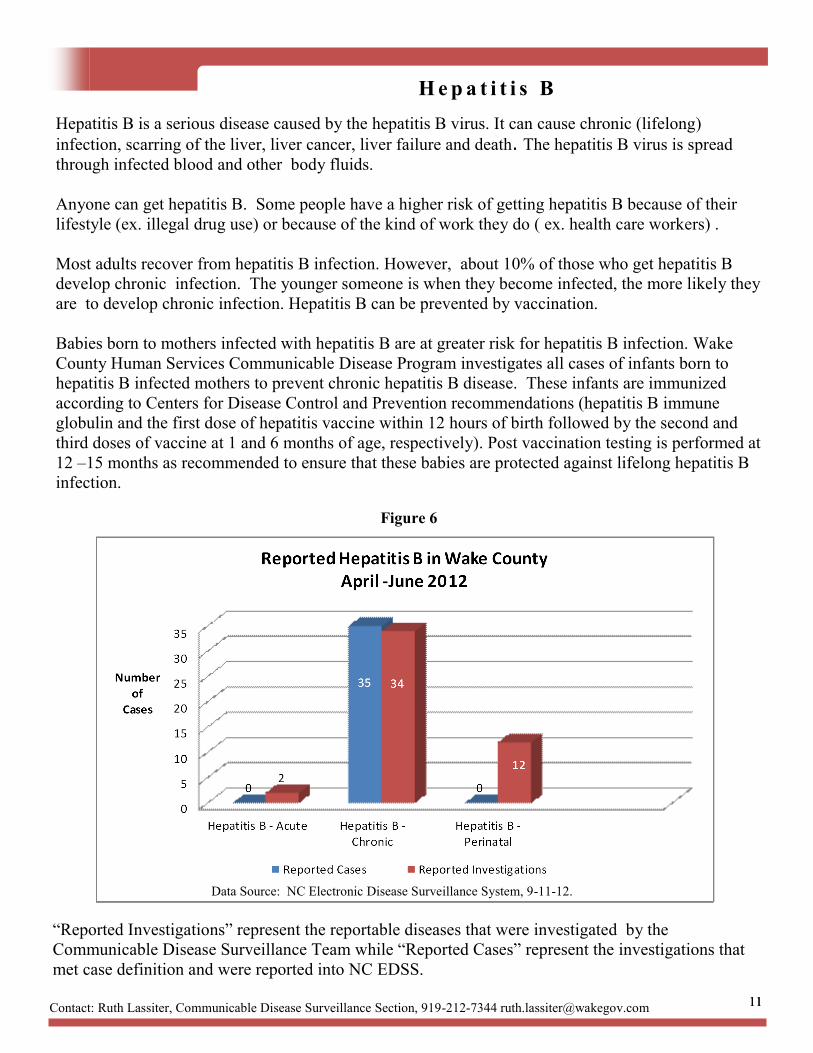
Hepatitis B 11
Acknowledgements 12
3 3
Introduction
Surveillance for Reportable Communicable Diseases in Wake County
Communicable diseases are illnesses caused by infectious agents (bacteria, viruses, parasites, fungi or prions) or their toxins that are transmitted from an infected person, animal, plant or from the environment. Because communicable diseases can have so much impact on populations, they are tracked and information analyzed (called surveillance) so that measures can be put in place for protecting the public's health. Certain communicable diseases are required by law to be reported to local health departments by physicians, school administrators, child care operators, medical facilities and operators of restaurants and other food or drink establishments (G.S. § 130A-135 through 130A-139). There are 71 “reportable” diseases specified in the N.C. Administrative Code rule 10A NCAC 41A .0101 (http://epi.publichealth.nc.gov/cd/index.html). After initial notification about a case or cases of a communicable disease, an investigation begins to collect details such as demographic, clinical, and epidemiological information. After verifying that a reported case meets the reporting requirements in the standardized case definitions, it is reported electronically to the N.C. Division of Public Health via the North Carolina Electronic Disease Surveillance System (NC EDSS) and then to the Centers for Disease Control and Prevention’s (CDC) National Notifiable Diseases Surveillance System. This report focuses on all reportable diseases that have been detected in Wake County during 2011 and information about selected reportable communicable diseases of public health significance for Wake County detected during 2012. Other diseases of public health significance for which reporting is not required except during outbreaks, for example norovirus infection, are not included in this report.
Wake County Human Services (WCHS), an
accredited health department, continues to strive
to perform the three core functions of assessment,
policy development and assurance and the 10
public health essential services (see Figure 1).
This report helps fulfill public health essential
services:
Number 1: Monitor health status to
identify community health problems
and
Number 3: Inform, educate, and
empower people about health issues.
Information is provided on a quarterly basis about
health and safety trends for Wake County
residents, providers, policy makers and
community partners to better inform decision
making. Strategies used by WCHS Public Health
programs and services to improve health
outcomes are also featured in these reports. For
additional information, point of contact
information is provided for each area.
Figure 1
4 4
Wake County Communicable Disease Morbidity 2008—2011
Wake County Communicable Disease Morbidity 2008-2011
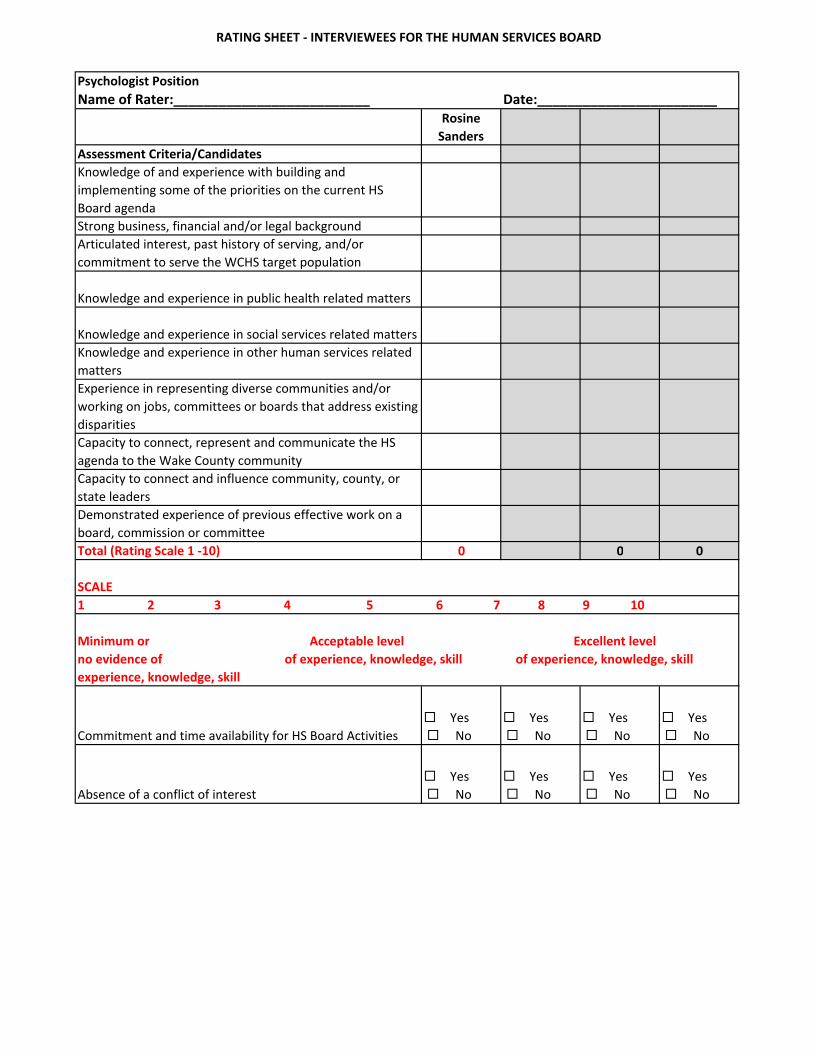
Articulated interest, past history of serving, and/or
commitment to serve the WCHS target population
Knowledge and experience in public health related matters
Knowledge and experience in social services related matters
Knowledge and experience in other human services related
matters
Experience in representing diverse communities and/or
working on jobs, committees or boards that address existing
disparities
Capacity to connect, represent and communicate the HS
agenda to the Wake County community
Capacity to connect and influence community, county, or
state leaders
Demonstrated experience of previous effective work on a
board, commission or committee
Total (Rating Scale 1 -10) 0 0 0 0
SCALE
Commitment and time availability for HS Board Activities
� Yes
� No
� Yes
� No
� Yes
� No
� Yes
� No
Absence of a conflict of interest
� Yes
� No
� Yes
� No
� Yes
� No
� Yes
� No
Date:________________________Name of Rater:__________________________
1 2 3 4 5 6 7 8 9 10
Minimum or Acceptable level Excellent level
no evidence of of experience, knowledge, skill of experience, knowledge, skill
experience, knowledge, skill
Wake County Human Services Board
Summary of Statutory Information
North Carolina General Statutes § 153 A 77
Functions and Authority of the Wake County Human Services
Board
153A-77: Authority of Board of Commissioners in certain counties over commissions, boards, agencies, etc.over commissions, boards, agencies, etc.
Except as otherwise provided, the consolidated human services board
shall have the powers and duties conferred by law upon a board of
health and a social services board….
Summary of Statutory Information
Public Health:
Health authorities tend to rule making; oversight, administration and enforcement;
and direct service provision and coordination with other agencies.
Board functions can be organized to address the ten essential public health
services, mandated services, and “typical” services. Or, they can be considered
public health or environmental health.
Wake County Human Services Board
North Carolina General Statutes § 130A-34 Provision of local public health
services
A county shall provide public health services.
A county shall operate a county health department, establish a consolidated
human services agency pursuant to G.S. 153A-77, participate in a district health
department, or contract with the State for the provision of public health services.
North Carolina General Statutes § 130A-1.1
Public Health Mission and essential services
(a) The General Assembly recognizes that unified purpose and direction of the public
health system is necessary to ensure that all citizens in the State have equal
access to essential public health services. The General Assembly declares that
the mission of the public health system is to promote and contribute to the
highest level of health possible for the people of North Carolina by:
(1) Preventing health risks and disease;
(2) Identifying and reducing health risks in the community;
(3) Detecting, investigating, and preventing the spread of disease;
(4) Promoting healthy lifestyles;
(5) Promoting a safe and healthful environment;
(6) Promoting the availability and accessibility of quality health care services through
the private sector; and
(7) Providing health care services when not otherwise available.
North Carolina General Statutes
FUNCTIONS OF A LOCAL HEALTH DEPARTMENT
SECTION 4. G.S. 130A-1.1(b) reads as rewritten: "(b) A local health department shall ensure that the following 10 essential public health services are available and accessible to the population in each county served by the local health department:
(1) Monitoring health status to identify community health problems.
(2) Diagnosing and investigating health hazards in the community.
(3) Informing, educating, and empowering people about health issues.
(4) Mobilizing community partnerships to identify and solve health problems.(4) Mobilizing community partnerships to identify and solve health problems.
(5) Developing policies and plans that support individual and community health efforts.
(6) Enforcing laws and regulations that protect health and ensure safety.
(7) Linking people to needed personal health care services and assuring the provision of health care when otherwise unavailable.
(8) Assuring a competent public health workforce and personal health care workforce.
(9) Evaluating effectiveness, accessibility, and quality of personal and population-based health services.
(10) Conducting research.
North Carolina General Statutes
Chapter 108A. Social Services. Article 1. County Administration.
Part 1. County Boards of Social Services.
§ 108A-1. Creation.
Every county shall have a board of social services or a consolidated
Wake County Human Services Board
Every county shall have a board of social services or a consolidated
human services board created pursuant to G.S. 153A-77(b) which shall
establish county policies for the programs established by this Chapter in
conformity with the rules and regulations of the Social Services
Commission and under the supervision of the Department of Health and
Human Services
Summary of Statutory Information
Social Services:
Board functions can be organized to address public assistance programs
and service programs. They can be considered economic services and
child/adult welfare services.
Statutory Functions
Wake County Human Services Board
Statutory Functions
To advise county and municipal authorities in developing policies and
plans to improve the social conditions of the community;
To consult with the director of social services about problems relating to
his office;
Such other duties and responsibilities as the general assembly, state
Department of Health and Human Services, the Social Services
Commission, or the County Commissioners may assign
North Carolina General Statutes
§ 108A-14.
Responsibilities of a Social Services Department
• To administer the programs of public assistance and social services
• To administer funds provided by the board of commissioners for the care of indigent persons
• To act as agent of the Social Services Commission and Department of Health and Human Services
• To investigate cases for adoption and to supervise adoptive placements;
• To issue employment certificates to children under the regulations of the State Department of Labor;
• To supervise adult care homes under the rules and regulations of the Medical Care Commission;
• To assess reports of child abuse and neglect and to take appropriate action to protect such children pursuant to the Child Abuse Reporting Law;
• To accept children for placement in foster homes and to supervise placements for so long as such children require foster home care;
• To respond by investigation to notification of a proposed adoptive placement , and
• To receive and evaluate reports of abuse, neglect, or exploitation of disabled adults and to take appropriate action as required by the Protection of the Abused, Neglected, or Exploited Disabled Adults
Responsibilities of the Human Services Board Members
BASIC FUNCTIONS:
Function effectively within the context of a Consolidated Human Services
Agency, serving simultaneously as a Public Health and Social Services board
member.
Play an active role in helping to meet the Public Health and Social Services Play an active role in helping to meet the Public Health and Social Services
statutory functions.
Perform necessary reviews of documents and other important materials to be
well prepared to provide sound advice and decision-making.
Attend at least 75% of scheduled meetings
Responsibilities of the Human Services Board
OVERSIGHT
• Monitor compliance will all mandates.
• Ensure that a high quality administrative structure is in place.
• Ensure that consumers are served with appropriate quantity and quality of
services.
• Ensure that a strong financial management system is in place.
• Ensure that consumers are treated with dignity, that customer services are
of high quality and that Human Rights are always honored.
•
REGULATORY
Perform statutory regulatory functions of the Board of Health and the Social
Services Board.
Responsibilities of the Human Services Board
PUBLIC RELATIONS AND ADVOCACY:
• Develop an on-going relationship with County Manager office and Board
of County Commissioners keeping them informed and abreast of Human
Services related matters and contributing to the development of mandates
for all important HS programs and projects.
• Work with legislators promoting and/or supporting state laws beneficial to
Wake County residents.Wake County residents.
• Educate the Wake County community about the needs and the
importance of Human Services.
• Represent and advocate for the department at various venues as needed.
• Identify and advocate for resources needed to carry out the department’s
mission.
• Attend events and represent the HS Board at various venues as
requested
North Carolina General Statutes
Article 5. Administration.
Part 1. Organization and Reorganization of County Government.
§ 153A-76. Board of commissioners to organize county government.The board of commissioners may create, change, abolish, and consolidate offices, positions, departments, boards, commissions, and agencies of the county government, may impose ex officio the duties of more than one office on a single officer, may change the composition and manner of selection of boards, commissions, and agencies, and may generally organize and reorganize the county government in order to promote orderly and efficient administration of county affairs, subject to the following limitations:
(1) The board may not abolish an office, position, department, board, commission, or (1) The board may not abolish an office, position, department, board, commission, or agency established or required by law.
(2) The board may not combine offices or confer certain duties on the same officer when this action is specifically forbidden by law.
(3) The board may not discontinue or assign elsewhere a function or duty assigned by law to a particular office, position, department, board, commission, or agency.
(4) The board may not change the composition or manner of selection of a local board of education, the board of health, the board of social services, the board of elections, or the board of alcoholic beverage control. (1973, c. 822, s. 1.)
North Carolina General Statutes § 130A-39 Powers and duties of a local board of health
(a) A local board of health shall have the responsibility to protect and promote the public health. The board shall have the
authority to adopt rules necessary for that purpose.
(b) A local board of health may adopt a more stringent rule in an area regulated by the Commission for Public Health or
the Environmental Management Commission where, in the opinion of the local board of health, a more stringent rule is
required to protect the public health;
(c) The rules of a local board of health shall apply to all municipalities within the local board's jurisdiction.
(d) Not less than 10 days before the adoption, amendment or repeal of any local board of health rule, the proposed rule
shall be made available at the office of each county clerk within the board's jurisdiction, and a notice shall be published in
a newspaper having general circulation within the area of the board's jurisdiction.
(e) Copies of all rules shall be filed with the secretary of the local board of health.(e) Copies of all rules shall be filed with the secretary of the local board of health.
(f) A local board of health may, in its rules, adopt by reference any code, standard, rule or regulation which has been
adopted by any agency of this State, another state, any agency of the United States or by a generally recognized
association.
(g) A local board of health may impose a fee for services to be rendered by a local health department, except where the
imposition of a fee is prohibited by statute or where an employee of the local health department is performing the services
as an agent of the State.
……..Fees shall be based upon a plan recommended by the local health director and approved by the local board of
health and the appropriate county board or boards of commissioners. The fees collected under the authority of this
subsection are to be deposited to the account of the local health department so that they may be expended for public
health purposes in accordance with the provisions of the Local Government Budget and Fiscal Control Act
Example of a Structure of the New Human Services Board - Fall 2013
HS Board Goals:
• Comply With the Law and Perform Statutory Social Services and Public Health Functions
• Incorporate Feedback from Board Members
• Maintain/Enhance Community Participation
• Strengthen Relationships with BOC and Management• Strengthen Relationships with BOC and Management
• Align Board Work with WCHS Strategic Plan
• Provide Board Members Opportunities to Work on Areas of Their Choice
• Provide Venues to Carry Necessary Activities
• Manage Time Effectively and Prevent Burnout
Board Structure Example
Wake County Human Services Board
Statutory Committees Advisory Groups Ad-Hoc & Work Groups
Social
ServicesPublic
Health
• Child & Family Matters
Consumer Rights
Housing
Board Operations
Functions: To plan and organize Board ActivitiesReplaces Executive Committee. Includes Chair and Co-Chair & Director and Board Staff – Other Board
• Child & Family Matters
• Youth Development
• Aging Services
• Adult Protection
• Safety Net
• Crisis Assistance
• Self-Sufficiency
• Child Protection
• Foster Care
• Adoption
• Child Support
• Employment
• Transportation
• Human Capital Dev.
• 10 PH Essential Services
• Communicable Diseases
• Immunization
• Health Care Access
• Epidemiology
• Environmental Health
• PH Preparedness
• HIV-AIDS
• Maternal & Child Health
• Pre-Natal Care
• Women’s Health
• Nutrition
• Health SafetyAdvisory Groups Functions:
Provide Advise to Administration
Quarterly Reports Presented to the
HS Board
Include 1-2 Board Members and
Community members
Housing
Regional Networks
Environmental
Services
Advocacy Group
Issue-Specific
Workgroups
Functions: Assist the Board in the Performance of its statutory
Social Services & Public Health Functions. Review critical issues
and bring recommendations to the full board. Meets Monthly
Include at least 6 Board Members who are Voting Members
Can include non-voting community members as needed
Workgroups Functions: Linked to strategic plan. Staff responsible to work on specific indicators. E.g. Obesity- Child Abuse
Includes staff and PartnersOptional 1-2 Board MembersBi-Annual reports presented to the Board
Director and Board Staff – Other Board members optional. Meets Monthly
Functions: To plan advocacy activitiesIncludes 2-3 Board membersMeets as needed. Presents reports to the full Board
WCHS Board –Example of Structure with Potential Assignments
HS
Board
Statutory
Committees
Advisory to Administration Ad-Hoc Groups Work
Groups
Others
Meeting- HS Board
Meeting
Social
Services
Public
Health
Environme
ntal Health
Housing Consumer
Rights
Board
Planning
Advocacy Issue
Specific
Meeting
Manager
BOC NCGA,
Others
Total
Date 1 x month Varies Varies 1 x month Varies
Duration
1 Member 1 x x x x x 5
2 Member 2 x x x 3
3 Member 3 x x 2
4 Member 4 x x 2
5 Member 5 x x 2
6 Member 6 x x 2
7 Member 7 x x 2
8 Member 8 x x 2
9 Member 9 x x 2
10 Member 10 x x 2
11 Member 11 x x 2
12 Member 12 x x 2
13 Member 13 x x 2
14 Member 14 x x 2
15 Member 15 x x 2
16 Member 16 x x 2
17 Member 17 x x 2
18 Member 18 x x 2
19 Member 19 x x 2
Total 19 6 6 2 2 2 1 2 4
1 Ramon Rojano x x x x x
2 Jonica Hinton x x
3 Regina Petteway x x
4 Jos. Threadcraft x x Description
Regular
Meeting
Statutory
Group
Statutory
Group
2 Board
members-
&Volunteers
2 Board
members- &
Volunteers
2 Board
members- &
Volunteers
Replaces
Executive
Committee
To Advocate
for HS
Optional
Upon
interest-
Chair & Vice-
Chair
Chair, Vice-
Chair & Lead
Advocate
WCHS Board Existing Structure and Assignments- September 2012 – MONTHLY RESPONSIBILITIES
Note: the 4 ORANGE shaded members are schedule to leave November-December 2012
Meeting- HS Board
Meeting
Executive
Committee
Social
Services
Public
Health
Environm-
ental Health
Housing Consumer
Rights
Regional
Networks
Advo-
cacy
Meeting
Director
Meeting
Manager
Other
Functions
Total
Date 1 x
month
1 x month Varies
Duration 2.5 hr 2 2 2 2 2 2 1.5 1 1 1
1 Dianne Dunning X X X X X XX 6
2 Pablo Escobar X X X X X XX 7
3 Leila Goodwin X X X 3
4 Frank Eagles X X X X 4
5 Sharon Foster X X X X 4
6 Julian Smith X X X 3
7 Osama Said X X 2
8 Paul Norman X X X 3
9 Burton Horwitz X X X 3
10 Benny Ridout X X X X X X 5
11 James West X 1
12 Marg Raynor X NEW
13 Tomeeko Piggee x NEW Soc Worker
14 James Smith x NEW Psychiatry
15 McKinl Wooten x NEW Consumer
16 Psychologist To be Recruited
17 General Public To be Recruited
18 Consumer To be Recruited
19 Consumer To be Recruited
Total 19 7 3 3 5 2 2 2 2 2
WCHS Board Previous Structure and Assignments- June 2011 – MONTHLY RESPONSIBILITIES
Meeting- HS Board
Meeting
Executive
Committee
Social
Services
Public
Health
Environm-
ental Health
LME
Committee
Housing Consumer
Rights
Regional
Networks
Advo-
cacy
Meeting
Director
Meeting
Manager
Others Total
Date 1 1 Varies
Duration 2.5 hr 2 2 2 2 2 2 1.5 1 1 1
1 Dianne Dunning X X X X X XX 6
2 Pablo Escobar X X X X X X XX 7
3 Leila Goodwin X X X 3
4 Frank Eagles X X X X 4
5 Sharon Foster X X X X 4
6 Julian Smith X X X 3
7 Osama Said X X 2
8 Paul Norman X X X 3
9 Burton Horwitz X X X 3
10 Benny Ridout X X X X X X 5
11 Melissa Jemison X X X X X 5
12 Steph Treadway X X X 3
13 Rich Greb X X 2
14 Jeff Smith X X 2
15 Jim Edgerton X X X X X 5
16 George Corvin X X X 3
17 Dave Filpowski X X 2
18 Jim Mebane X X X X 4
19 Bill Stanford X X X X 4
20 Kent Earnhardt, X X X 2
21 Alexand Herring X X 2
22 C. James West X 1
23 Lena Mehta X X 2
24 Vacant
25 Vacant
Total 22 10 3 5 5 8 2 5 3 4 2 2
WCHS Board Previous Structure and Assignments- May 2007 – MONTHLY RESPONSIBILITIES
Meeting- HS Board
Meeting
Executive
Committee
Success-
ful HS
Children
Comm-
Public
Health
Environment
Services
Watershed
Continuum
of Care
Afforda-
ble
Housing
Human
Rights
Regional
Networks
CFAC Meeting
Director
Meeting
Manager
Others Total
Date 1 1 Varies
Duration 2.5 hr 2 2 2 2 2 2 2 1.5 1 1 1
1 Dave Filipowski X X X X X - 5
2 Jim Mebane X X X X - 4
3 Bill Stanford X X X X X 5
4 Dianne Dunning X X X X 4
5 Sharon Foster X X 2
6 Ann Ackland X X X X 3
7 Lou Mitchell X X X 3
8 Benny Ridout X X X X 4
9 Paul Norman X X 2
10 Burton Horwitz X X X 3
11 Seth Tabb X X X 3
12 Buck Kennedy X X X 3
13 Rich Greb X X X 3
14 Jeff Smith X X 2
15 Kent Goddard X X 2
16 John Key X X X X 4
17 Charles King X X 2
18 Octavia Rainey X X 2
19 Leena Mehta X X 2
20 Susan O’Dell X X 2
21 Vacant X
22 Vacant X
23 Vacant
24 Vacant
25 Vacant
Total 22 9 3 6 4 5 2 4 4 n/a
Staff
Meeting- HS Board
Meeting
Executive
Committee
Social
Services
Public
Health
Environmen-
tal Health
Housing Consumer
Rights
Regional
Networks
Meeting
Director
Meeting
Manager
Other
Functions
Total
Date 1 x month 1 x month Varies
Duration
1 Ramon Rojano
2 Jonica Hinton
3 Regina Petteway
4 Sue Ledford
5 Michelle Ricci
6 Katherine Williams
7 Annemarie Maio-
Jos. Threadcraft
Joe Durham
David Cooke
Historic Information – June 2011 September 2012 Executive Committee: 10 Members 7 Members LME Committee : 8 Members N/A Environmental Committee: 5 Members 5 Members Public Health: 5 Members 3 Members Consumer Rights: 5 Members 2 Members Advocacy: 4 Members 2 Members Social Services: 4 Members 3 Members Regional Networks: 3 Members 2 Members Housing: 2 Members ? Members
WAKE COUNTY HUMAN SERVICES BOARD
INFORMATION ITEM
Agenda Date: October 25, 2012
Committee/Item: Human Rights-Consumer Affairs/Research Proposal
Specific Action Requested: Information Item Only. The Committee is reporting the
participation of the WCHS Foster Care services in a multi-site study that focuses on the
relationships between agency staff and foster parents. Participation did not require HS Board
approval, but is being reported as an information item for the benefit of the Board.
Item Summary: Foster Care services will be participating in a Duke Endowment funded effort
known as Together Facing the Challenge (TFC). The project seeks to maximize the support to
foster parents, and to identify key systemic factors that lead to enhanced support.
Purpose for Action: Information Item Only
Attachments: Summary of the proposal
Opportunities for Advocacy, Policy or Advisory: None at this time.
Connections to Other Committees: Social Services
Information Item
Human Research Proposal in Foster Care
This project is funded by the Duke Endowment and carried out by Duke
University. The project seeks to evaluate effectiveness of different approaches to
providing foster care. For most of a decade this project has worked to develop,
test (random trial published in 2010), and apply a hybrid approach to working
with foster care families and agency staff called Together Facing the Challenge
(TFC) at 14 sites across NC.
This study concentrates on how supervisors work with the treatment parents. The
TFC approach provides tools for supervisors that help them support and guide
foster parents. The approach is to focus on training and consultation with
supervisors, focus on systematic evaluation and monitoring of progress, and to
use group supervision with foster parents to increase connectedness and
professionalism of TFC practitioners.
No foster children are interviewed or directly observed at any time in any way.
Supervisors and foster parents complete questionnaires and are observed
working together. Confidentiality is protected through the use of unique numeric
identifiers secured by the chief researcher. Parents or legal guardians must give
consent, though, since the child will be discussed in the interviews.
The sole risk associated with the proposal is loss of confidentiality, and the study
procedures call for use of unique numeric identifiers maintained by the principal
investigator to guard against that risk. No additional institutional review is
mandated, therefore the planned participation of WCHS foster care is being