19
WANDERING SPLEEN – COURSE OF EVENTS ABSTRACT ID: 1154
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | egbert-bryant |
| View: | 216 times |
| Download: | 0 times |

WANDERING SPLEEN – COURSE OF EVENTS
ABSTRACT ID: 1154

OBJECTIVES
•To determine the role of imaging studies in diagnosing wandering spleen, a rare condition with common clinical presentation like abdominal pain.
•To identify the location, vascular status for appropriate management.

• The spleen develops from the mesoderm in the dorsal mesogastrium. It lies in the left hypochondrium behind the stomach, and is about 12 × 7 cm
• The spleen is fixed in position by the lieno-renal and gastro-splenic ligaments; the phrenico-colic ligament provides additional support.
•Wandering spleen also called ectopic spleen, is a rare clinical occurrence with fewer than 500 cases reported in literature

• Wandering spleen is defined as a mobile spleen that is attached only by an elongated vascular pedicle, allowing it to migrate to any part of the abdomen or pelvis.
• It is a result of congenital anomalies in the development of the dorsal mesogastrium and the absence or malformation of normal splenic suspensory ligament.
• However, acquired anomalies have been described and are attributed to laxity of the ligaments due to weakness of the abdominal wall, multiple pregnancies, hormonal changes, or increase in the size in the spleen.
•Clinical presentation is variable. Patients can be asymptomatic or may have chronic vague abdominal pain.
•They may present as acute abdomen when there is infarction due to torsion of pedicle.

Case history
•A 19 yr old female presented with chronic lower abdominal pain. Her routine blood investigations were inconclusive.
•She was referred for Ultrasonography. •Ultrasound of abdomen showed absence
of spleen in left hypochondrium. A well-defined, homogenous hypoechoic mass measuring 17x 8 cm seen in the pelvis on left side extending to midline.

oThe mass is seen to compress the bladder and pushing the uterus.
oHilar vessels were made out ,and showed mild color flow on doppler evaluation. However the spleen looked congestive.
oOther abdominal organs showed no significant abnormality.
oA diagnosis of wandering spleen with possible partial torsion of vascular pedicle was given.

USG images showing spleen in pelvis, ectopic location.
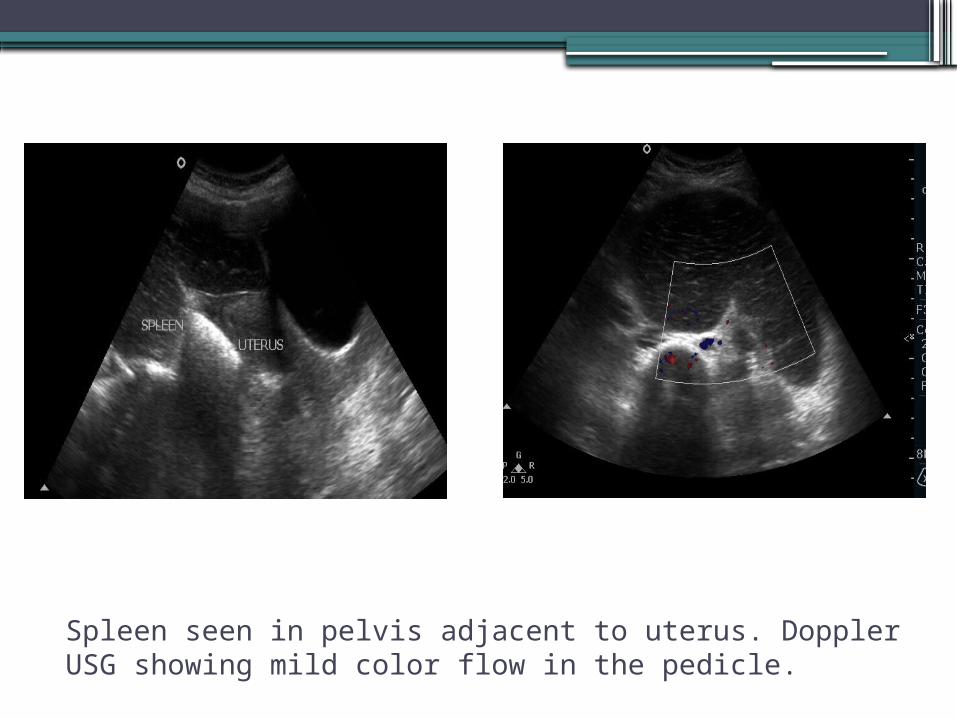
Spleen seen in pelvis adjacent to uterus. Doppler USG showing mild color flow in the pedicle.

CECT ABDOMEN• Four days later the patient presented with acute
abdominal pain.• Computed tomography of abdomen was done
which showed enlarged spleen in pelvis with a long vascular pedicle attached to pancreatic tail.
• On contrast study the spleen showed no enhancement. The vascular pedicle was seen twisted just above the level of pelvis causing vascular compromise and infarction of spleen.
• The pancreatic tail was normally enhancing.• There were no other areas of infarction.

CECT Axial images. A. Spleen not seen in left hypochondrium. B. Spleen seen in ectopic location ,pelvis.
A B

CECT: a. Axial and b. Coronal reformatted images showing non-enhancing pedicle and spleen.
a b

a. sagittal, b. coronal reformatted images showing enhancing vascular pedicle upto the level of twisting.
a b

TO
RS
ION
OF W
AN
DER
ING
S
PLEEN
CURVED MPR showing the vascular pedicle twisted causing infarction of spleen.

TORSION OF PEDICLE
Video clip of sequential CECT images showing twisted oedicle.
•Diagnosis of wandering spleen with torsion was given.
•Patient underwent laporotomy.•Spleen along with a part of vascular
pedicle were removed.

Per operative images showing pedicle, spleen
CONCLUSION Though rare, wandering spleen should be considered
as a part of differential diagnosis in patients presenting with lower abdominal pain, palpable mass etc., and when not seen in usual position.
Only treatment for wandering spleen is surgery, which will be either splenopexy [salvaging] or splenectomy.
Imaging by ultrasound, computed tomography confirms the diagnosis. More importantly the vascular supply, and thus helps in appropriate management avoiding the complications like gangrene, pancreatic tail infarction etc.,

REFERENCES• Sharma and Salerno Journal of Medical Case
Reports 2014, 8:133• Alawi MH, Khalifa A, Bana H. Wandering
spleen: a challenging diagnosis. Pak J Med Sci 2005;21(4):482–4.
• Taori K, Ghonge N, Prakash A. Wandering spleen with torsion of vascular pedicle. Abdom Imaging 2004; 29:479–481.
• Danaci M, Belet U, Yalin T. Power Doppler sonographic diagnosis of torsion in a wandering spleen. J Clin Ultrasound 2001; 28:246–248

















