81
Drinking Water Contamination AOEC Teaching Module 2007
Drinking Water Contamination
AOEC Teaching Module2007

This educational module was produced by Michael Greenberg, MD, MPH, Arthur Frank, MD, PhD, and John Curtis, MD for The University of Texas
Health Science Center at San Antonio (UTHSCSA) Environmental Medicine Education Program and South Texas Environmental Education and Research Program (STEER-San Antonio/Laredo/Harlingen,Texas)Administrative support was provided by the Association of Occupational
and Environmental Clinics through funding to UTHSCSA by the Agency forToxic Substances and Disease Registry (ATSDR), U.S. Department of
Health and Human Services.Use of this program must include acknowledgement of the authors,
UTHSCSA and the funding support.For information about other educational modules contact the UTHSCSA
STEER office, Mail Code 7796, 7703 Floyd Curl Drive, San Antonio,Texas 78229-3900,(210)567-7407.

• 2 Introductory case studies
• Examples of specific toxicants– Farm chemicals– Perchlorate– Heavy Metals– Biologicals
• Clinical problem solving
Outline

Objectives
• After completion of this module, the student will be able to:– Describe the importance of the water supply as it
relates to epidemic illness– Identify issues related to water purity as related to
the use of industrial and agricultural chemicals– Demonstrate ability to evaluate illness due to
biological contamination of water

Case Study #1Introduction to the Problem
• From March 23rd to April 5th, 1993 two water treatment facilities in Milwaukee reported record setting turbulence in intake water
• April 5th the Department of Health reported an outbreak of gastrointestinal illness

Southern Water Treatment Plant

Mac Kenzie W et al. N Engl J Med 1994;331:161-167
Maximal Turbidity of Treated Water in the Northern and Southern Water-Treatment Plants of the Milwaukee Water Works from March 1 through April 28, 1993

Mystery GI Illness
• 50% of the population served by the southernmost plant and 25% of those served by the northern plant become ill– Over 400,000 (26% of population) estimated to be
affected• GI illness:
– Watery diarrhea lasting approximately 9 days– Low grade fever– Average 10 lbs. weight loss

Investigation• Cryptosporidium was
identified in over 600 stool samples (30% of those tested)
• No other causative organisms found in greater than 2% of samples
• Later, Cryptosporidium was also found in ice made from water during that period

Cryptosporidium in water• Disease transmitted by
oocysts• Not destroyed by chlorine or
chloramine• Difficult to identify and not
normally screened for by water treatment facilities
• Disease is usually self-limited in immunocompetent hosts
Illustrative Points
• Importance of evaluating air, water, and food supply in epidemic illness
• Relevant history regarding event• Symptoms, evaluations of patients• Impact on water-quality standards• Impact on U.S. public health including
impact on HIV/AIDS awareness
Case Study #2
• In January of 2003, a resident of Hebbronville, TX contacted the Texas Department of Health concerned about elevated arsenic (As) levels in drinking water Hebbronville Library

Hebbronville, TX

Hebbronville• Agency for Toxic Substances and Disease Registry (ATSDR)
conducted an evaluation of local residents and water supply• Water supply:
– Arsenic levels in the drinking water ranged from 43.7 to 52.1 µg/L– Prior to 2006, the maximum contaminant level for As was 50 µg/L
Home of the Hebbronville Longhorns

Evaluation of Population• 2/3 of the 140 people
sampled had urinary inorganic As concentrations > reference concentration of 10 µg/L
• Drinkers of tap water had higher-than-reference range levels
• Drinkers of bottled water had substantially lower levels. Hebbronville Courthouse

Evaluation of Population• According to the ATSDR 91%
of the population described themselves as Hispanic
• Typical regional diet included rice and beans cooked in water - potentially increasing arsenic consumption:– 8-9 µg As per serving of rice– 20-24 µg As per serving of beans (if cooked in water containing 50
µg/L)

Actions Recommended in Hebronnville
• Those with inorganic As levels > 20 µg/g of creatinine to be retested
• Individuals encouraged to discuss their results with a personal health care provider
• Evaluation of other (dietary) sources of As• Efforts to reduce As levels in the public water
system.

Implications
• Unclear what, if any, health effects would be expected
• Possible parallels to areas such as Taiwan and Bangladesh that have experienced high levels of environmental arsenic

Bangladesh
• Borders India and Burma• Local water wells were
commonly contaminated with disease-causing microorganisms

Bangladesh Water Supply
• UNICEF and other international organizations promote the use of “tube wells” for safer water supply in the 1970’s and 1980’s– Thin tubes sunk in ground; usually < 200
meters in depth– Resulted in high levels of arsenic in soil
leached into water, first confirmed in 1993

Quantification of Arsenic Exposure
• In 1980’s first reports of arsenic-related dermatologic disease
• Analysis of water in British Geological Survey showed that >35% of wells contained
> 50 g As/L– In some districts >80% of wells
contained greater than 50 g As/L– 8% had As concentrations of > 300 g/L

% of Field-tests positive for As

Chronic Arsenic Toxicity• Approximately 125
million residents drawing from water supply
• In some studies 30-50% of patients had skin lesions due to arsenic– Skin lesions typically
develop after latency of 10 years
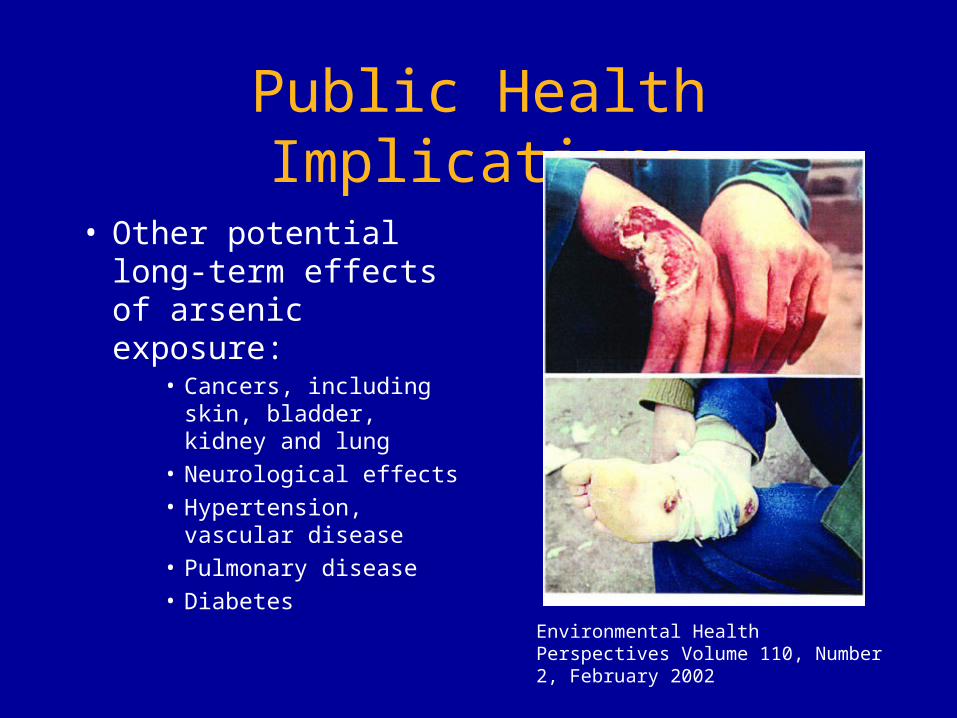
Public Health Implications
• Other potential long-term effects of arsenic exposure:
• Cancers, including skin, bladder, kidney and lung
• Neurological effects• Hypertension,
vascular disease• Pulmonary disease• Diabetes
Environmental Health Perspectives Volume 110, Number 2, February 2002
Public Health Issues - Bangladesh
• How to treat the millions of exposed patients?– Nutritional supplementation?– Infected hyperkeratotic lesions?
• What about tremendous predicted expense from excess cancer morbidity/mortality?
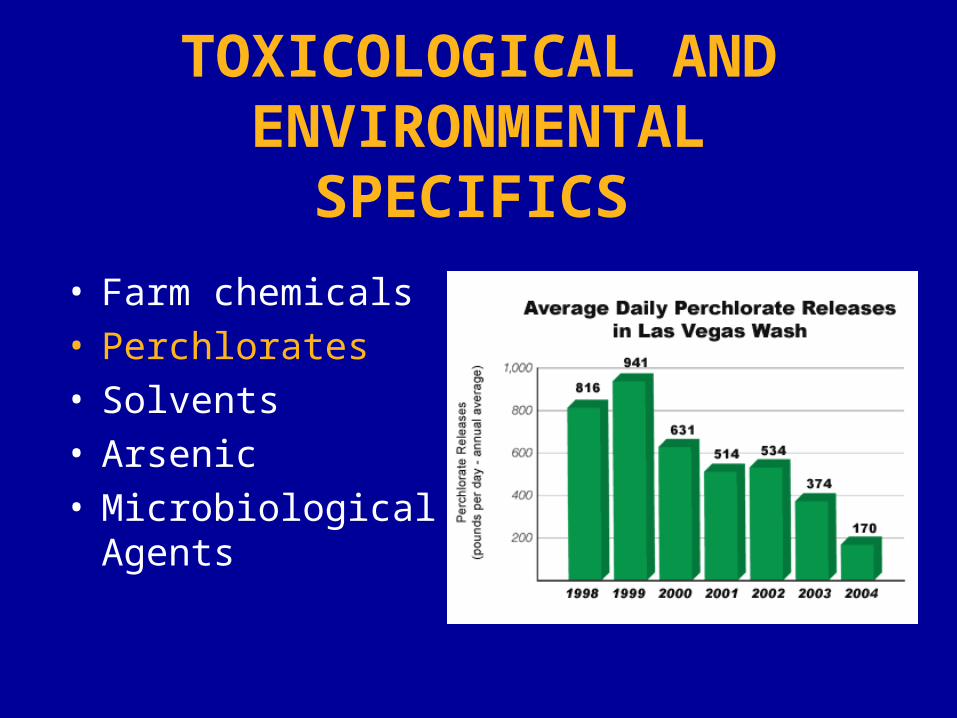
TOXICOLOGICAL AND ENVIRONMENTAL
SPECIFICS • Farm chemicals• Perchlorates• Solvents• Arsenic• Microbiological
Agents

Occurrence of Nitrite/Nitrate• Naturally occurring inorganic ions
– Enter groundwater from fertilizer use, including anhydrous ammonia
– Releases totaled over 110 million pounds– Contamination from septic systems
• Chemical characteristics lead to migration to ground water

Exposure• Groundwater supplies 20% of nitrate intake,
but can be higher in the setting of water contamination
• MCL for nitrates has been set at 10 ppm, and for nitrites at 1 ppm– US Geological survey in 1995 showed >8,000
wells had levels exceeding 10 ppm– 1-2% of population estimated to be exposed to
excessive levels of nitrates• >600,000 homes draw from contaminated
wells and rural wells are not routinely tested

Health Effects
• Nitrites and nitrates cause oxidation
• Nitrates are converted in vivo to nitrites– More potent oxidizers
• Oxidation of iron in hemoglobin results in methemoglobinemia
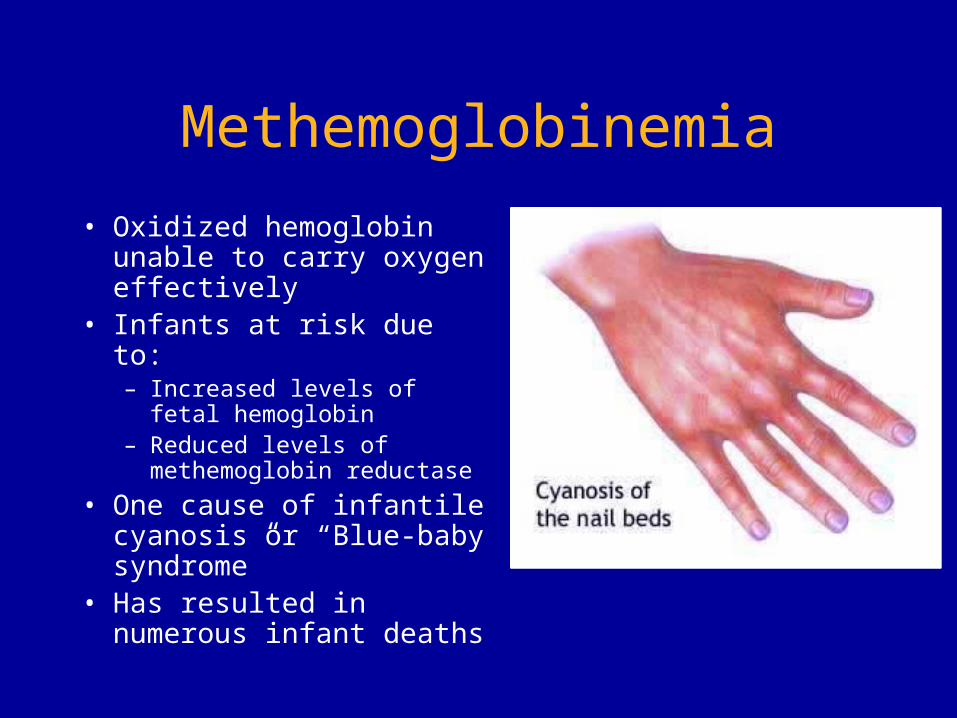
Methemoglobinemia• Oxidized hemoglobin
unable to carry oxygen effectively
• Infants at risk due to:– Increased levels of fetal
hemoglobin– Reduced levels of
methemoglobin reductase• One cause of infantile
cyanosis or “Blue-baby syndrome”
• Has resulted in numerous infant deaths
Methemoglobinemia Treatment
• Supportive care• Removal from exposure• Reducing agents such
as methylene blue• Antioxidants such as
vitamin C
TOXICOLOGICAL AND ENVIRONMENTAL
SPECIFICS • Farm chemicals• Perchlorates• Solvents• Arsenic• Microbiological
Agents

Perchlorates• Naturally occurring (e.g. in
saltpeter deposits)• Magnesium, potassium,
sodium, lithium, ammonium perchlorate are manufactured in large amounts– Uses include: solid rocket
fuel, ammonium perchlorate, explosives

Perchlorates
• Perchlorates are the primary oxidizers in solid rocket fuel
• Perchlorates are also very stable in water
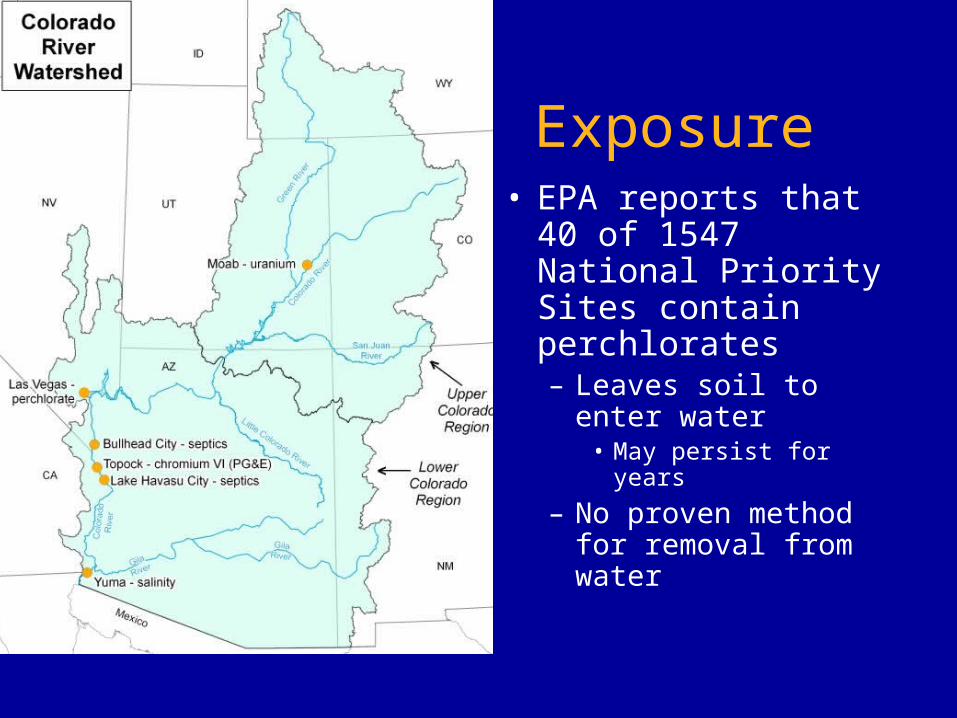
Exposure• EPA reports that 40
of 1547 National Priority Sites contain perchlorates– Leaves soil to enter
water• May persist for years
– No proven method for removal from water

Exposure
• Exposure pathways may include:– Drinking
contaminated water– Also may occur
through tobacco use– Proximity to
industrial use of perchlorates
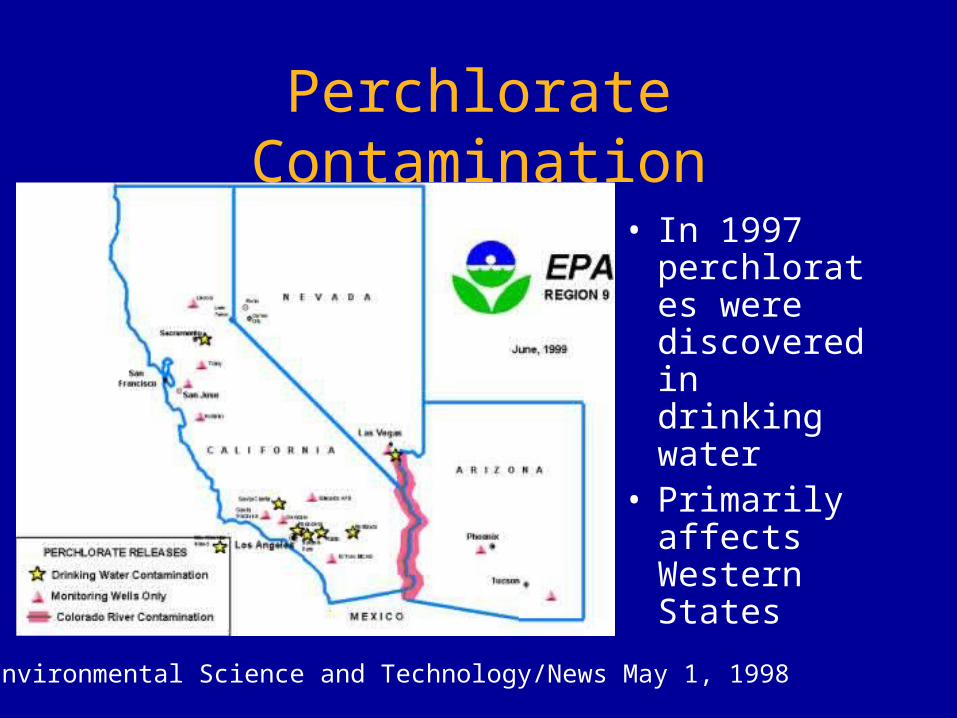
Perchlorate Contamination
• In 1997 perchlorates were discovered in drinking water
• Primarily affects Western States
Environmental Science and Technology/News May 1, 1998
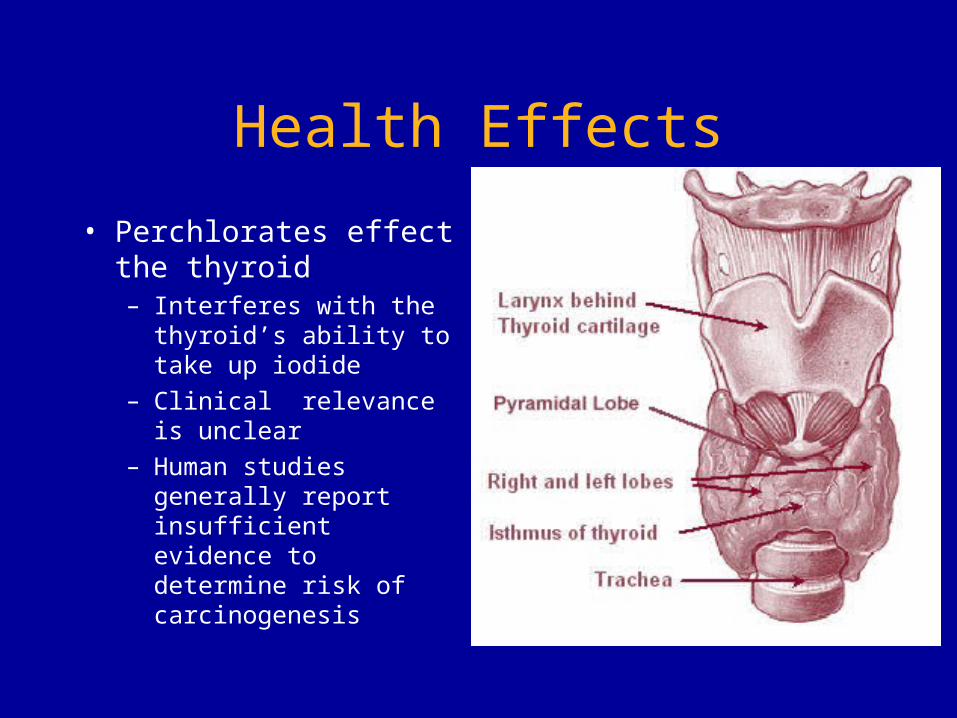
Health Effects
• Perchlorates effect the thyroid– Interferes with the
thyroid’s ability to take up iodide
– Clinical relevance is unclear
– Human studies generally report insufficient evidence to determine risk of carcinogenesis

TOXICOLOGICAL AND ENVIRONMENTAL
SPECIFICS • Farm chemicals• Perchlorates• Solvents• Arsenic• Microbiological Agents
Solvents - including MTBE• Methyl-t-butyl-ether
– Manufactured by reaction of methanol and isobutylene
– Flammable liquid with disagreeable odor
– Evaporates quickly– Added (like ethanol) to
gasoline as an oxygenator to decrease carbon monoxide emissions.

Potential Exposure Pathways• Possible ingestion of MTBE in water
• Concentration dependant
• Dermal exposure while showering or swimming– Medically important systemic absorption is unlikely
MTBE - possible health effects
• Any adverse effects are expected to be a function of exposure and dose
• Vapor exposure (at high concentration for prolonged periods) may have mild but reversible effects
• Ingestion– Potential cancer risk is unproven
• Not classified by the IARC• Only weak evidence of carcinogenicity in some
animal studies

Water Purity Standards
• EPA recommends < 4 mg MTBE/Liter• State-specific limits exist• Taste/odor threshold is 20-40 ppb

TOXICOLOGICAL AND ENVIRONMENTAL
SPECIFICS • Farm chemicals• Perchlorates• Solvents• Arsenic/Heavy Metals• Microbiological Agents
Heavy Metal Occurrence
• Mostly natural– Mineral deposits– Natural soil constituents
• Increased levels may exist at some industrial sites

Potential Exposure Pathways
• Contaminated water supply• Food grown in contaminated soil or with
contaminated water
Potential Health Effects - Arsenic
• Acute– Possible GI illness, neuropathy– Uncommon from environmental exposure– Intentional exposures
• Suicidal• Homicidal
• Chronic– Dermatologic, vascular and malignant disease– Environmental exposure
• Bangladesh

Treatment for Arsenic/Metals
• For chronic exposure the treatment is REMOVAL FROM EXPOSURE
• For acute exposure, consultation with a Poison Control Center or medical toxicologist is advisable– Chelation may be considered in some
extreme cases

TOXICOLOGICAL AND ENVIRONMENTAL
SPECIFICS • Farm chemicals• Perchlorates• Solvents• Arsenic• Microbiological Agents

Microbiological Water Contamination
• Several broad categories, including:– Bacterial– Protozoa– Viruses
Bacterial Contamination
• Traveller’s diarrhea– Up to 50% of international travelers may be
afflicted depending on region• Approximately 10 million people
– High-risk areas• Latin/Central America• Africa• Middle-East• Asia

Traveller’s Diarrhea
• Caused by infectious agents– Primarily Escherichia
coli• Produces
enterotoxins
– Watery diarrhea lasting several days
E.coli 0157:H7
Traveller’s Diarrhea
• Prevention:– Avoidance of local waters and ice– Bottled water for consumption– Daily bismuth (e.g.Pepto-Bismol)
preparations– Avoidance of strong antacids (PPIs)– Possibly prophylactic antibiotics for select
patients

Treatment
• Usually self-limited• Only symptomatic treatment usually
required• Antibiotics (sulfa drugs, quinolones)
may slightly reduce duration of illness

Dysentery
• Enteroinvasive disease caused by any of several organisms– Salmonella, Shigella,
Campylobacter
• Bloody mucoid diarrhea with fever, fecal leukocytes
• Antibiotic treatment recommendedSalmonella infantis
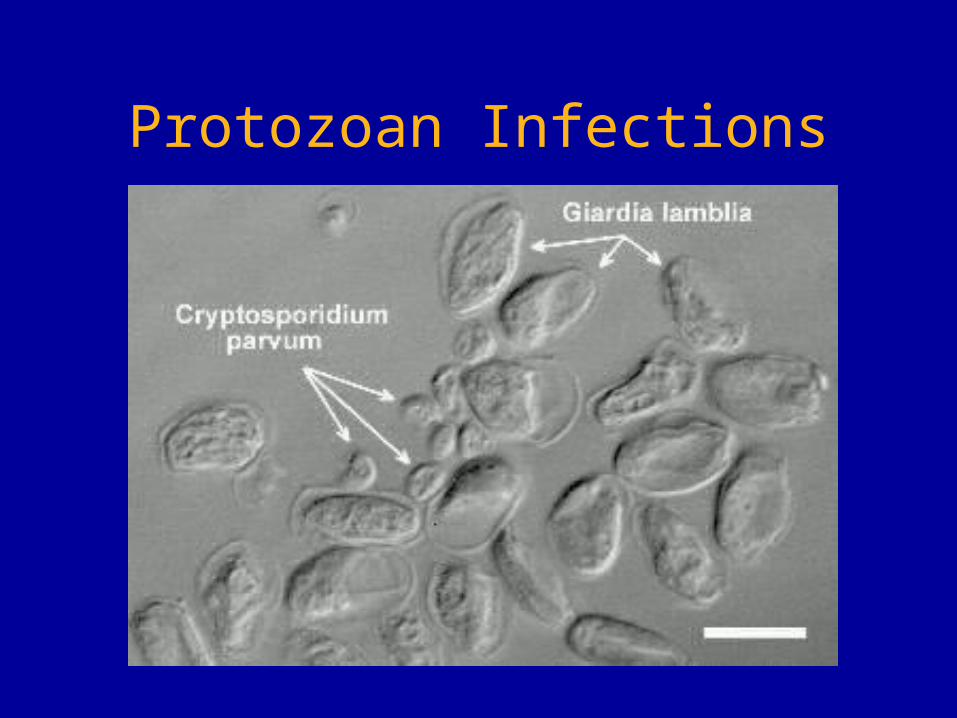
Protozoan Infections
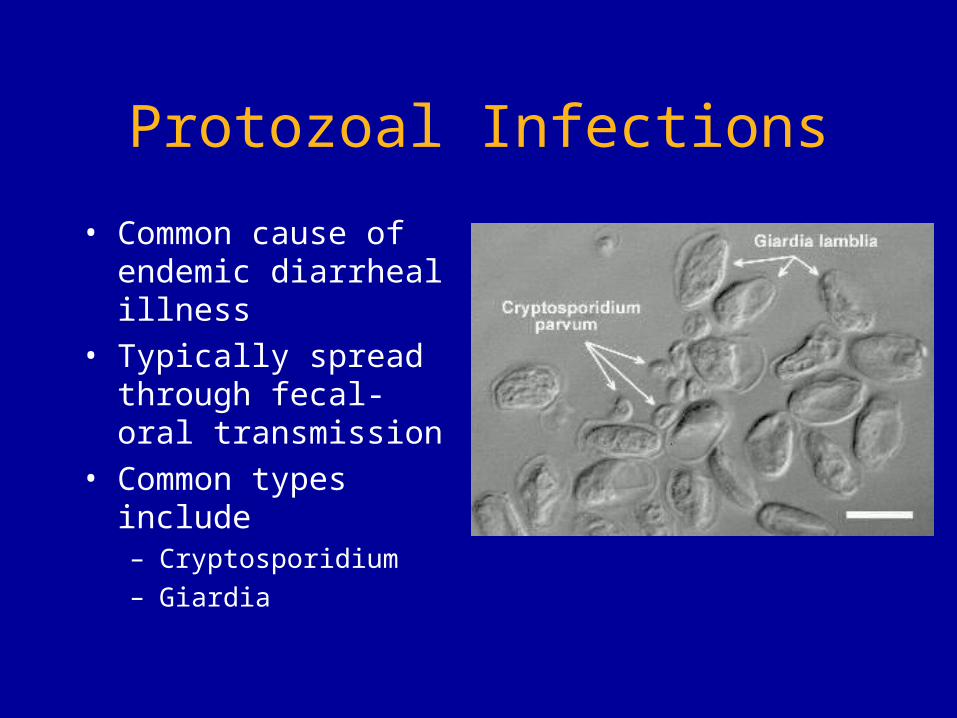
Protozoal Infections
• Common cause of endemic diarrheal illness
• Typically spread through fecal-oral transmission
• Common types include– Cryptosporidium– Giardia

Cryptosporidium parvum
• Worldwide presence in water supply– Not effectively killed by
chemical purification methods
• Prevention through– Boiling of drinking water– Water filtration with 1
micron pores

Chen X et al. N Engl J Med 2002;346:1723-1731
Life Cycle of Cryptosporidium and Infection of Host Epithelial Cells

Cryptosporidium - Health Effects
• Watery diarrhea lasting 1-2 weeks in normal hosts
• May result in dehydration, weight-loss• Usually self-limited, but may be severe
in immunocompromised hosts– Treatment includes anti-retrovirals for
those with HIV– Possible role for nitrazoxanide
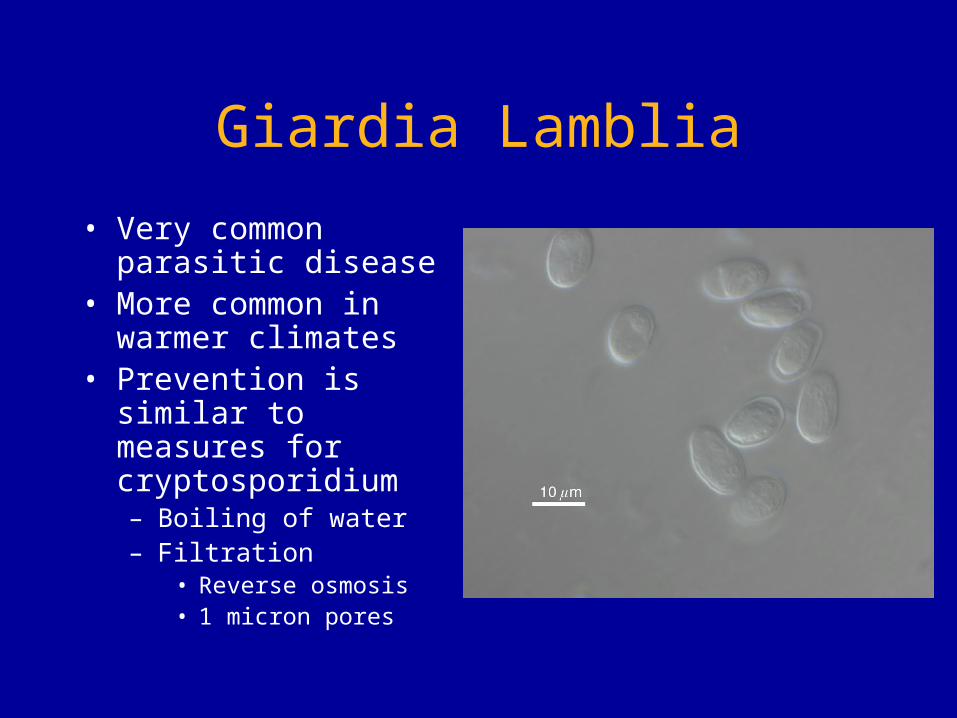
Giardia Lamblia• Very common parasitic
disease• More common in
warmer climates• Prevention is similar to
measures for cryptosporidium– Boiling of water– Filtration
• Reverse osmosis• 1 micron pores

Viral Diseases
• Multiple viral pathogens– Rotaviruses– Hepatitis A– Enteroviruses
• Most common epidemic (not endemic) diarrheal illnesses
• No specific treatment
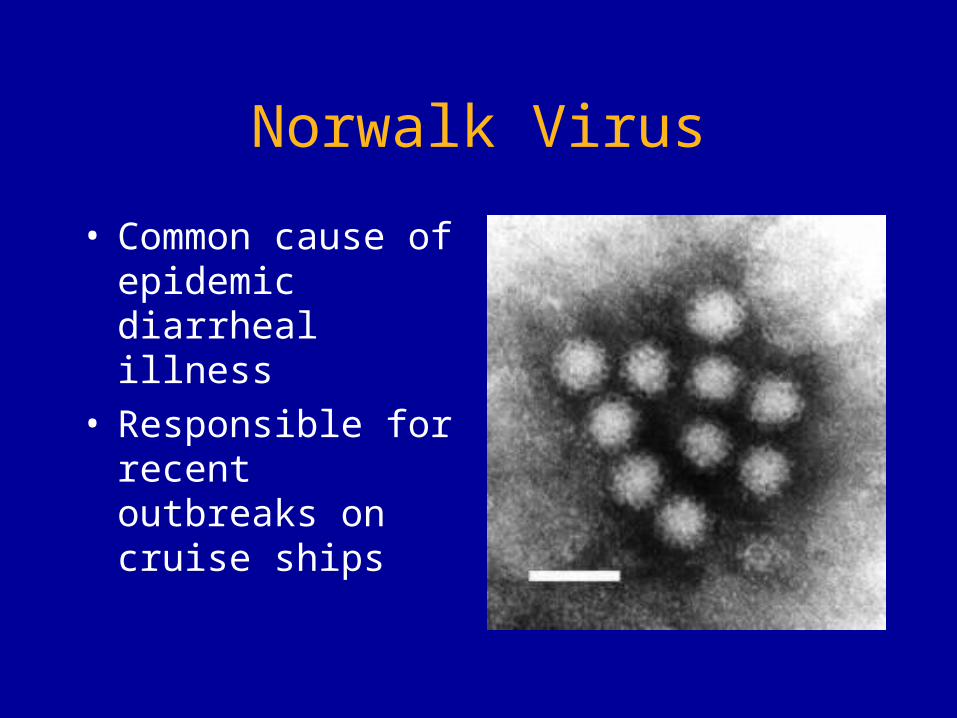
Norwalk Virus
• Common cause of epidemic diarrheal illness
• Responsible for recent outbreaks on cruise ships
Prevention
• Hygiene– Reduce fecal-oral
transmission– Hand-washing– Sanitization of
surfaces• Vaccination
– Effective for hepatitis A prevention

Reported Cases of Hepatitis A, United States
0
5
10
15
20
25
30
35
40
45
52 56 60 64 68 72 76 80 84 88 92 96 2002Year
Rat
e pe
r 100
,000
1995: Vaccine Licensed1996: ACIP recommendations
1999 ACIP recommendations
Source: NNDSS, CDC
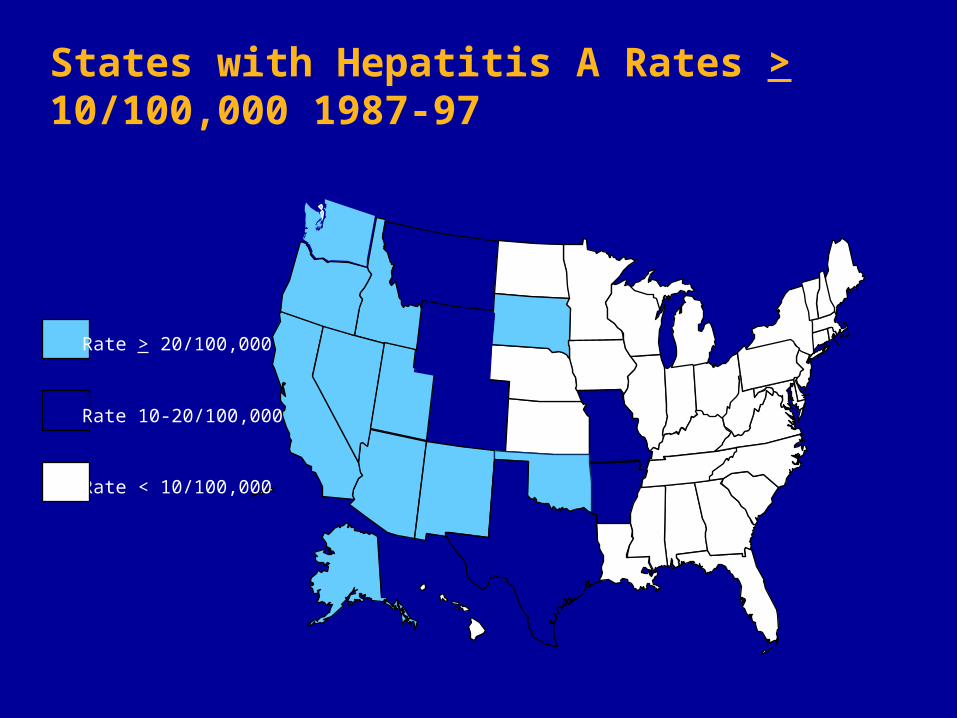
Rate > 20/100,000
Rate 10-20/100,000
Rate < 10/100,000
States with Hepatitis A Rates > 10/100,000 1987-97
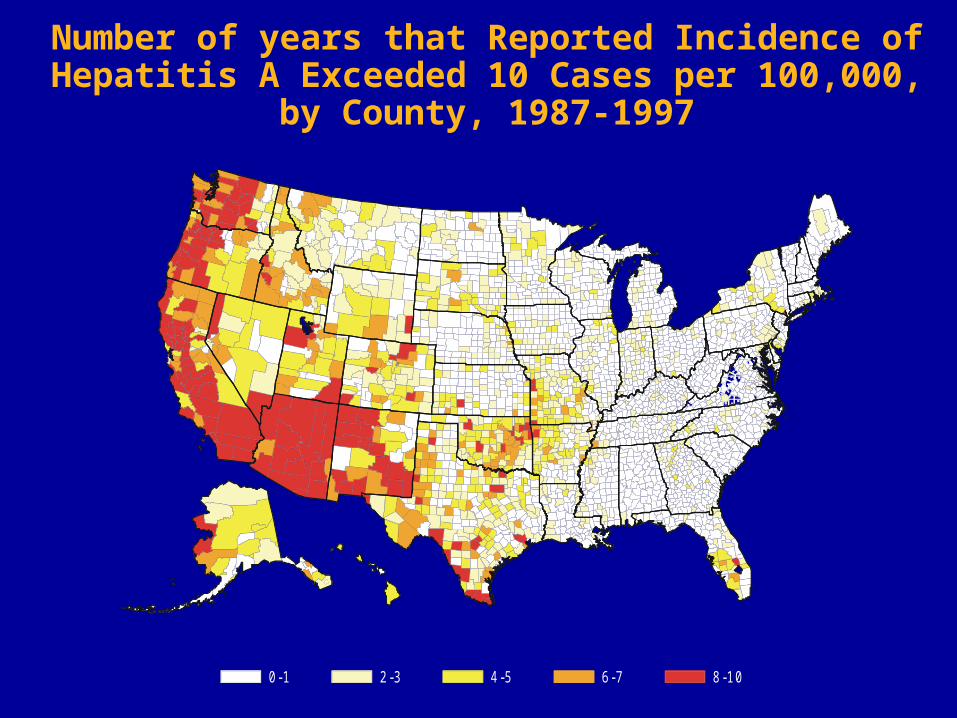
0-1 2-3 4-5 6-7 8-10
Number of years that Reported Incidence of Hepatitis A Exceeded 10 Cases per 100,000,
by County, 1987-1997

Hepatitis A Incidence, United States
rate per 100,000 0-4 5-9 10-19>=20
DC
NYC
rate per 100,000 0-4 5-9 10-19>=20
DC
NYC
2002 incidence
1987-97 average incidence
> = 2010 - 19 5 - 9 0 - 4
Rate per 100,000

Thielman N and Guerrant R. N Engl J Med 2004;350:38-47
Approach to the Evaluation and Management of Infectious Diarrhea
Water as a Terrorist Target
• Watersheds and reservoirs contain a centralized depot of an essential resource for large numbers of people
• Often inadequately protected• Impossible to monitor for all possible
pathogens at all times

Prevention of Water Terrorism
• Certain chemical properties of water are monitored continuously
• Very large volume of water– Would require very large amounts of toxins
to reach harmful levels– Attractive terrorism agents would have to
be extraordinarily potent to be effective (such as botulinum toxin)

Clinical Problem Solving
• 40 patients present over a 2-3 day period with GI illness– Watery diarrhea– Crampy abdominal pain– No fever/vomiting
• No occupational, social, or family connection between most patients

Key Physician Actions
• Recognize cluster of illnesses• Try to find shared exposure
– Attendance at a gathering• Family/workplace picnic etc.
– Eating at same restaurant or similar unusual foods
– Face-to-face contact (same school, workplace)
Observations
• Some hospitals receive many more patients than others
• Most patients come from same geographic area
• No particular meals, restaurants, or workplaces occur with greater than expected frequency

Investigation
• Comparing geographical distribution of patients to water distribution plans reveals that areas affected all receive water from same reservoir and treatment plant.

Role of Community Physician
• Physicians are on the “front-line”• They are the interface between the
public and the public health agencies• Therefore, physicians must treat not
only individual patients, but be vigilant to protect and treat their entire community

Key Physician Actions
• Recognition of illness cluster• Recognition of probable environmental
illness• Development of rational evaluation and
treatment options• Reporting responsibilities
– Contact the CDC and local public health officials

Treatment and Disposition of Patients
• Evaluate and resuscitate as necessary– Identify and treat dehydration– Check stool for blood and/or fecal
leukocytes to screen for enteroinvasive disease (dysentery)
– Symptomatic treatment• Obtain stool cultures, send stool for
evaluation for ova and parasites

References
• http://www.atsdr.cdc.gov/hac/pha/hebbronville/hae_p1.html#sum
• Agency for Toxic Substances and Disease Registry. 2001. Case studies in environmental medicine: taking an exposure history. Atlanta: US Department of Health and Human Services
References
• American Academy of Pediatrics. 1970. Policy statement. Infant methemoglobinemia: the role of dietary nitrate. Pediatrics 46(3):475-8
References• U.S. EPA. Integrated Risk Information System:
Perchlorate and Perchlorate Salts. 2/18/2005• U.S. EPA. Assessment Guidance for
Perchlorate. January 26, 2006• Chen X.-M. et al. Current Concepts:
Cryptosporidiosis. N Engl J Med 2002; 346:1723-1731, May 30, 2002.
• Thielman NM, Guerrant RL. Acute Infectious Diarrhea. N Engl J Med 2004; 350:38-47, Jan 1, 2004

















