Water distribution Intracellular 28L (66%) Extracellular 14L (33%) Plasma 3.5 L (8%) Interstitial 10.5 L (25%) Cell membrane Osmotic pressure Osm i (K + ) = Osm o (Na + ) Capillary w Colloid osmotic pressure (albumin) vs. Hydrostatic pressure
Transcript
Water distribution
Intracellular 28L
(66%)
Extracellular 14L
(33%)
Plasma
3.5 L
(8%)
Interstitial
10.5 L
(25%)
Cell membrane
Osmotic pressure
Osmi (K+) = Osmo (Na+)
Capillary wall
Colloid osmotic pressure
(albumin)
vs.
Hydrostatic pressure
Water Balance
INTAKE OUTPUT
Unregulated: food & social drink Insensible and obligate loss
Regulated: thirst AVP modulated water output
Thirst
Hyperosmolar stimulus hypothalamic osmoreceptors threshold 1 to 4% above basal
Hypovolaemic stimulus baroreceptors threshold 10 - 15% ? absent in man (inconvenient with postural change!)
Normally inactive as unregulated input is in excess
AVP secretion
Synthesized in hypothalamic supraoptic and paraventricular nuclei
Stored and released from posterior pituitary (> 1 week store!)
Interacts via V2 receptors to insert aquaporin-2 water channels
0
2
4
6
8
10
270 280 290 300 310
Plasma osmolality (mOsm/Kg)
Pla
sma
AV
P (
pm
ol/L
)
0
100
Su
bje
ctiv
e th
irst
(an
alo
gu
e sc
ale)
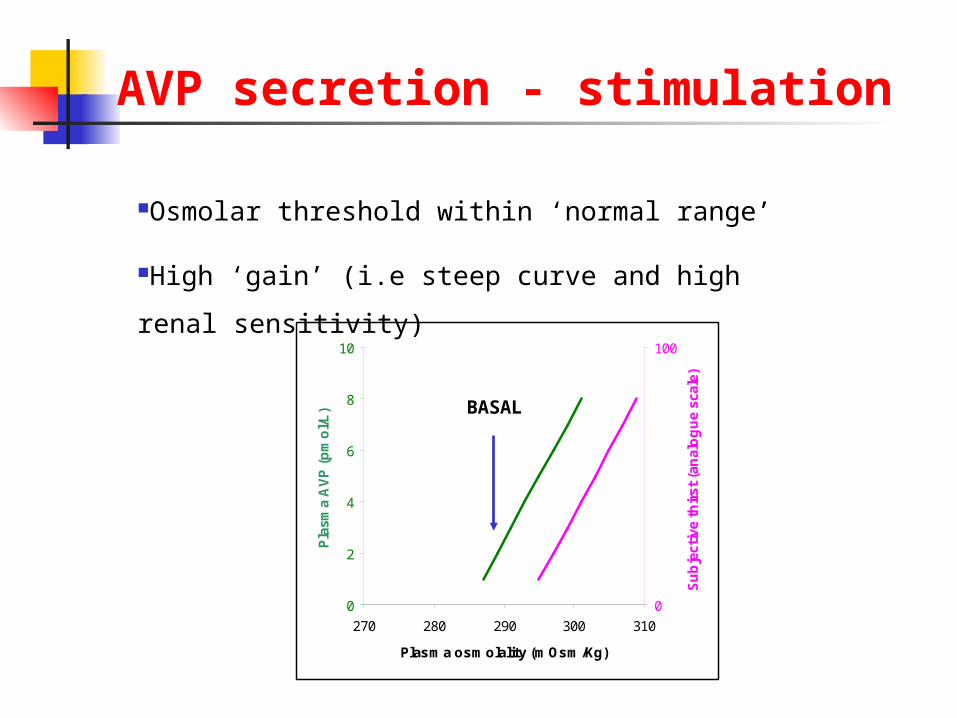
BASAL
AVP secretion - stimulation
Osmolar threshold within ‘normal range’
High ‘gain’ (i.e steep curve and high renal
sensitivity)
AVP secretion - stimulation
Osmotic stimulus high sensitivity
Hypovolaemic stimulus high threshold (>10% depletion)
AVP secretion - stimulation
Osmotic stimulus high sensitivity
Hypovolaemic stimulus high threshold (>10%)
Nausea most powerful known
stimulus
Stress e.g. post-operative
Drugs ‘SIADH’
Integration of thirst and AVP
Unregulated water intake supplies water in excess of need
Excess water is excreted
AVP secretion regulates free water clearance
AVP maintains osmolality within narrow limits
This avoids ‘inconvenient’ thirst and water-seeking behaviour
Thirst kicks-in when deficiency reaches harmful levels
A 17-year old woman was seen in outpatients with a two month history of increasing lethargy and giddiness. She was found to be hyperpigmented and had postural hypotension
Miscellaneous Acute psychosis Post-operative state AIDS Glucocorticoid deficiency Severe hypothyroidism Idiopathic
Patterns of AVP release in SIADH
Diagnosis of SIADH
Essential criteria True plasma hypo-osmolality (<275 mOsm/Kg) Inappropriate urine osmolality (>~100 mOsm/Kg) Euvolaemia; no oedema, ascites or intravascular hypovolaemia Urine sodium not low (>30 mmol/L during normal intake) Normal renal, adrenal, and thyroid function
Supplemental criteria Low serum urea and urate Unable to excrete >80% of water load (20mL/Kg) in 4h and/or failure to
achieve urine osmolality <100 mOsm/Kg No significant rise in serum [Na] after volume expansion but
improvement with fluid restriction
Treatment of SIADH
Identification and treatment of underlying cause
Clearance of excess water not necessary in asymptomatic chronic hyponatraemia fluid restriction to 500 - 1000 mL/24h Demeclocycline
600 to 1,200 mg daily may take three weeks to reach maximal effect caution in renal or hepatic insufficiency
Specific V2 receptor antagonists (OPC-31260)
Treatment of SIADH
Hypertonic saline Only if significantly symptomatic
Calculate sodium required
Na+ req. (mmol) = (125 – [Na+]) x 0.6 x body weight (kg)
A 53-year old bachelor was brought to the A&E department having been found semi-comatose. He was known to be a heavy drinker of alcohol. On examination he was jaundiced. His abdomen was distended; there was hepatomegaly and evidence of ascites. He had ankle oedema.