23
Morocco Rounds
| Date post: | 26-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | sparks92 |
| View: | 64 times |
| Download: | 0 times |

Morocco Rounds

The colitis mule
Ruth Cranston

• History: 1 year old foal presented on Monday with 3 day history of colic. Owner reported that it had not eaten, drunk or defecated for 3 days.
• Presentation: pyrexia (38.8 deg C.), shivering, tachycardia (80), seemed painful
• Rectal exam: NAD but soft slightly watery faeces was found.
• Haematology: NAD

• Initial plan: Treat as colitis suspect parasitic: 4ml flunixin I.V. (one off dose), Metronidazole TID, Fenbendazole SID for 5 days, Biosponge BID
• Day 2: pyrexia had resolved, DUDE. Tachycardia was still present (72bpm). Suspect babesia +/- parasites (e.g. Cyathostomins). Coproscopy: FEC 0epg. Smear: no babesia seen.
• Still tahcycardic...



Colic Mule - Justine
• Presented Mon 19th Jan• Hadn’t eaten for 4 days• On presentation had a stretched stance and heart rate of
56bpm. • PCV 30 TP 6.7• Rectal exam- gas distension of large intestine• Ultrasound- small intestines all motile, no free peritoneal
fluid, colon and caecum were fluid filled.• Gastric reflux- none• CBC- BUN slightly high, otherwise unmerarkable• Impaction or RDD?

Treatment
• Flunixin 1.1mg/kg• MgSO4 1g/kg• 1 litre nasogatric fluids q 2hours• Started refluxing so changed to IV fluids 2xM• U/S and rectal exam again- results as previous day• Fluids increased to 3xM• Walk 3x daily• Pain became poorly responsive to butorphanol and
detomidine so was euthanised

Post Mortem


Swollen Limb Mule - Rachel
• Presented 21/01/15 with 7 day history of swollen limb following trauma.
• Problems: Grade 4 heart murmur, bilateral nasal discharge, crackles heard on lung auscultation, HR = 100, very pale mm, swollen limb.
• Procedures: Accidentally burst abscess, flushed abscess, rebreathing test, lung ultrasound, abdominal ultrasound, radiographs of swollen limb, PCV = 8, TP = 6.6, smear=negative, slide agglutination test=negative.


Treatment:Flunixin, buscopan and x4 imidocarb.Nebulisation with 3ml Gentamicin x4 daily.Penicillin and GentamicinFlunixin BIDMetronidazole TIDIvermectin

Becky’s Colicking Donkey
• Presented Monday; 3 day history colic and shock• Proximal Enteritis and Ileus (rectal, ultrasound
and abdominocentesis)• Inflammation of duodenum and upper jejunum• Refluxed every 2 hours • IVFT spiked with lidocaine and calcium; and oral
fluids• Flunixin, Metronidazole and Omeprazole

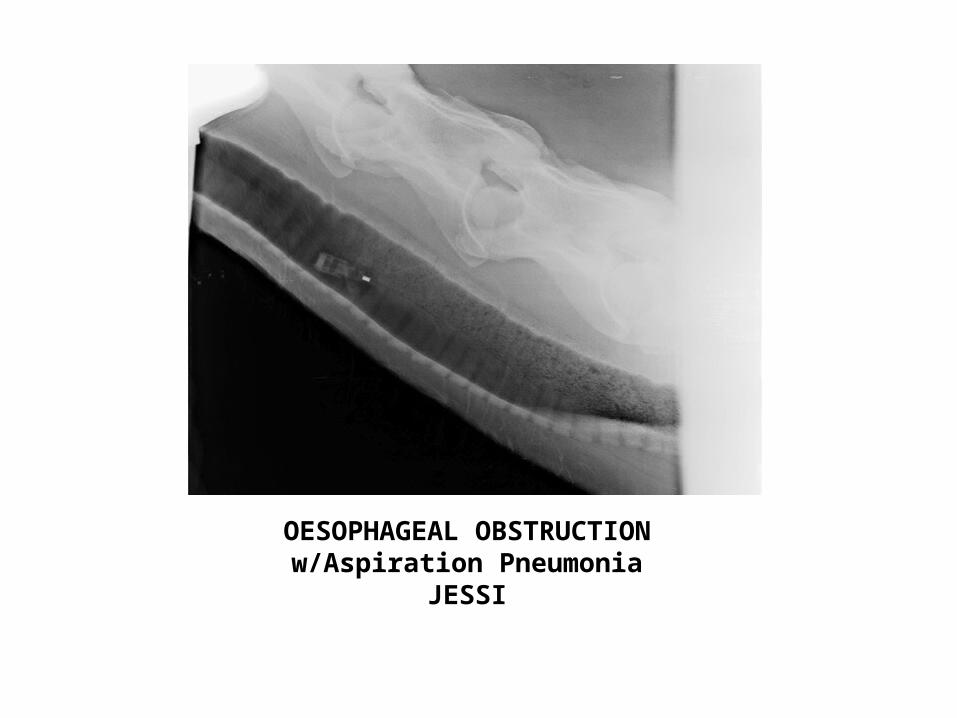
OESOPHAGEAL OBSTRUCTION w/Aspiration Pneumonia
JESSI

• Presented in shock with Hx of NPO x 3 days with intermittent severe cough and
bilateral nasal d/c
• T=36.6 P=76 R=8, mm= congested, CRT= 2s, reduced gut sounds all 4 quadrants
• PCV= 42, TP=9.0
• Radiographs= large, 30cm impaction in middle third of oesophagus.
• NG tube passed to just past pharynx
• Multiple attempts to flush impaction with water and Coca-Cola= partial
reduction achieved

• Initial Therapy and Plan: – Penicillin, 28ml IM – Gentamycin, 36ml IV SID– Flunixin, 7ml IV BID– Demosedan, 1ml – Oxytocin, 5ml then 6ml, then 6 ml– IVFT, 12L NaCl bolus
• Plan to repeat PCV/TP then based on values can administer another 12L IVFT over 6 hours and then IVFT at 1.5 x Maintenance (3 drops/sec).
• 5 hrs later: PCV= 22, TP=5

Ongoing Management
• 20 hours after initial presentation and multiple attempts to flush later = complete removal of obstruction.
• Started on Electrolyte/Juice cocktail orally – Not taking in enough oral fluids or ‘mash’ as needed, so…
• Back out to grass for 1 hour within 24 hrs of presentation. • Concerned about possible oesophageal stricture post
obstruction–> discussed Omeprazole and Sucralfate preventative therapy BUT Omeprazole only available as capsules (28 capsule dose expensive and this is less efficacious) and Sulcralfate unable to be obtained at this time.
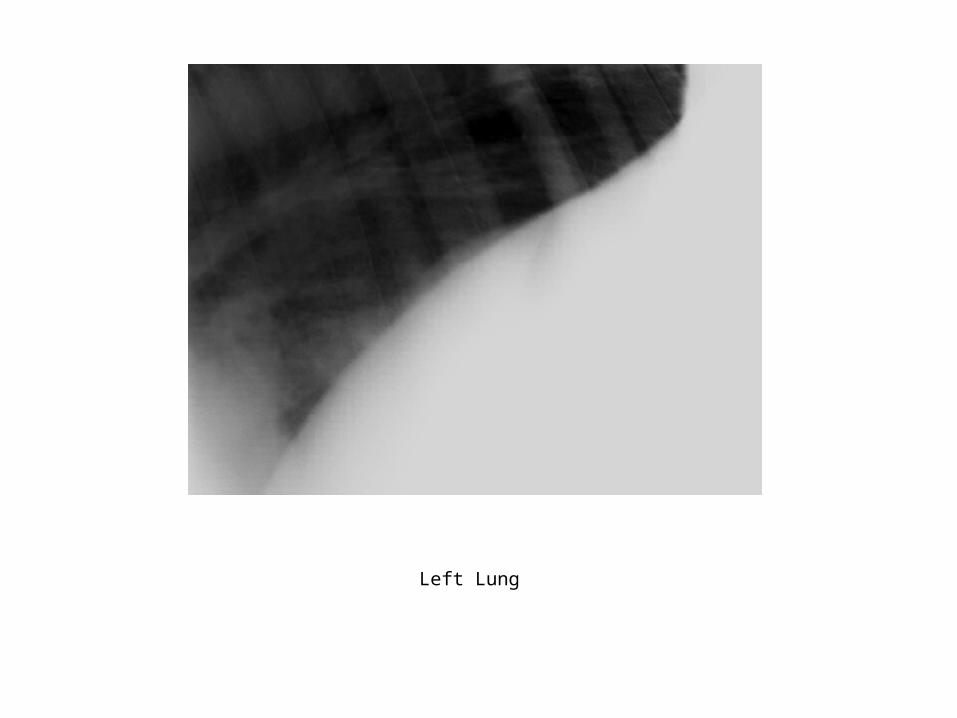
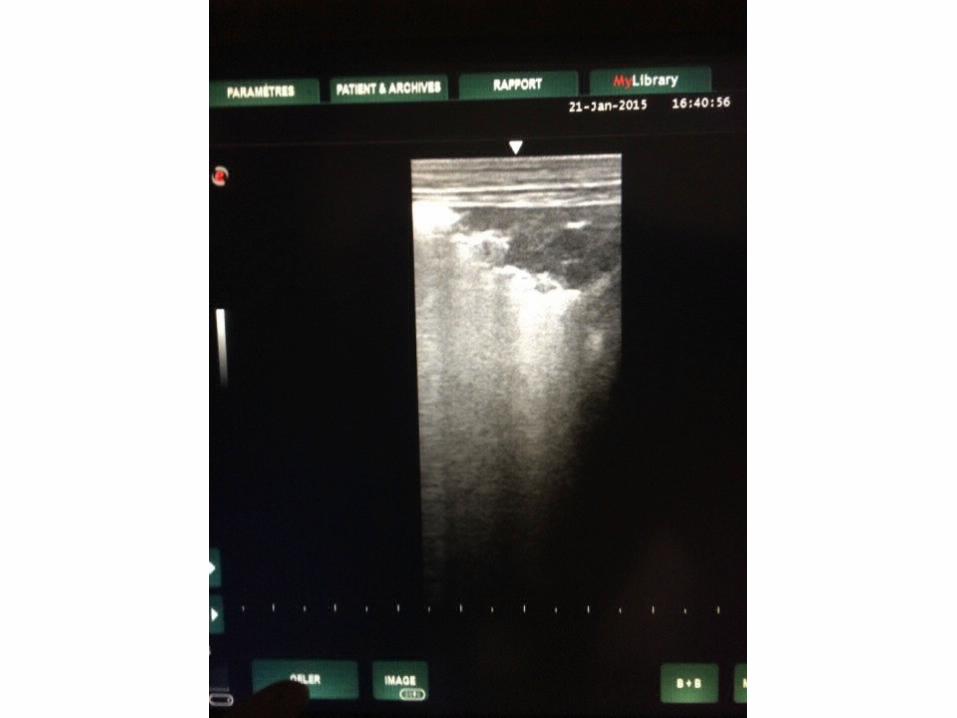
Left Lung

• Aspiration Pneumonia Concerns – Crackles heard on lung auscultation bilaterally – Continuing to have coughing intermittently, ADR on 20/1– Ultrasound shows ‘comet tails’ bilaterally and small abscesses
on RHS– Medications:
• Penicillin BID x 7 days (IV x 5 days, then IM x 2); now changed to Ceftiofur after repeat U/S showed minimal improvement yesterday.
• Gentamycin IV SID x 4 days, stopped 2 days, now restarted• Metronidazole rectally x 4 days (bc now head shy and cannot give
oral meds), stopped x 2 days, now restarted • Nebulisation started yesterday (w/Gentamycin) BID
• Working Management Plan: • Grass ad lib• Soaked hay ad lib • Water ad lib • Continue to treat aspiration pneumonia with
broad spectrum abx therapy• Once recovered, plan to sedate for oral exam
and dental float prn.

















