Welcome to our second newsletter for patients in the ACTIVE trial. For those of you who have recently joined the trial, the first newsletter is on the website under “Your participation” www.active-trial.org.uk We will send out a regular newsletter and would greatly appreciate any of your stories, news or pictures suitable for sharing and helping others with a similar knee problem. Please keep in touch… If your address is going to change please let us know so that we can collect the information which is vital to the trial. A change of address form is enclosed. Most of your assessments are in the first 12 months (pre-op, 2-3, 6 & 12 months, then 3, 5 & 10 years post-op) but we also send you a questionnaire by post at 2, 4, & 6-9 years follow- up. Whether or not your knee is still causing you problems we need to know about it so please attend assessment and complete the forms. Your stories following ACI surgery CHONDROCYTE TRANSPLANTATION / IMPLANTATION VERSUS EXISTING TREATMENTS NEWSLETTER July 2008 The Lee’s knees Lee Williams from Abertillery in South Wales provided these photos of his scar after ACI. Lee’s surgeon here at Oswestry said his knee had healed well though somewhat tethered. I think Lee is trying to show that is gets rapidly better, and not to be too alarmed when you first see it! Thanks Lee for the thought. (Apologies to anyone who’s squeamish!) It takes more than surgery…. In this edition we are featuring the stories of two ACTIVE patients who have shown a great deal of determination. Firstly, Debbie Holmes provides an insight from the perspective of patient, physiotherapist and ACTIVE Trial assessor. Our second story comes from Conor O’Donovan from Ireland who describes his rehabilitation under the guidance of a private physiotherapist. My own knee injury came as a very unwelcome surprise back in 1997. I had always been active in most sports so at the age of 31 I did not consider my injury to be anything particularly serious that would curb my activities for long. And so, while I was limping around at work at the Derbyshire Royal Infirmary (I should perhaps mention that I am a physiotherapist), I was spotted by one of our orthopaedic consultants and sent for urgent tests. When the x-ray revealed nothing, an MRI scan followed but there was still no obvious cause of the huge swelling in my knee. Three days later I was being wheeled into the operating theatre for exploratory surgery, still protesting that I really did not need an operation and that my knee would surely settle down by itself. My surgeon Mr Rowles fortunately knew better. Debbie Holmes He discovered that I had sustained damage to the articular cartilage that covers the end of the femur leaving a hole about the size of a ten pence piece. He had tidied up the area and carried out microfracture to encourage new tissue to grow over the area where the strong articular cartilage was missing. Over the past ten years my activities have been restricted due to the painful area in the knee. There would be periods when the knee would allow me to carry out some sports but to a lesser standard than before injury. Every year or so, I would suffer bouts of swelling and pain which would often continue for a few months before settling again. I was fortunate only to return to theatre once more, whereas I know that many other patients have endured a variety of procedures aimed at trying to improve things.
Transcript
Welcome to our second newsletter for patients in the ACTIVE trial. For those of you who have recently joined the trial, the first newsletter is on the website under “Your participation” www.active-trial.org.uk We will send out a regular newsletter and would greatly appreciate any of your stories, news or pictures suitable for sharing and helping others with a similar knee problem.
Please keep in touch…If your address is going to change please let us know so that we can collect the information which is vital to the trial. A change of address form is enclosed. Most of your assessments are in the first 12 months (pre-op, 2-3, 6 & 12 months, then 3, 5 & 10 years post-op) but we also send you a questionnaire by post at 2, 4, & 6-9 years follow-up. Whether or not your knee is still causing you problems we need to know about it so please attend assessment and complete the forms.
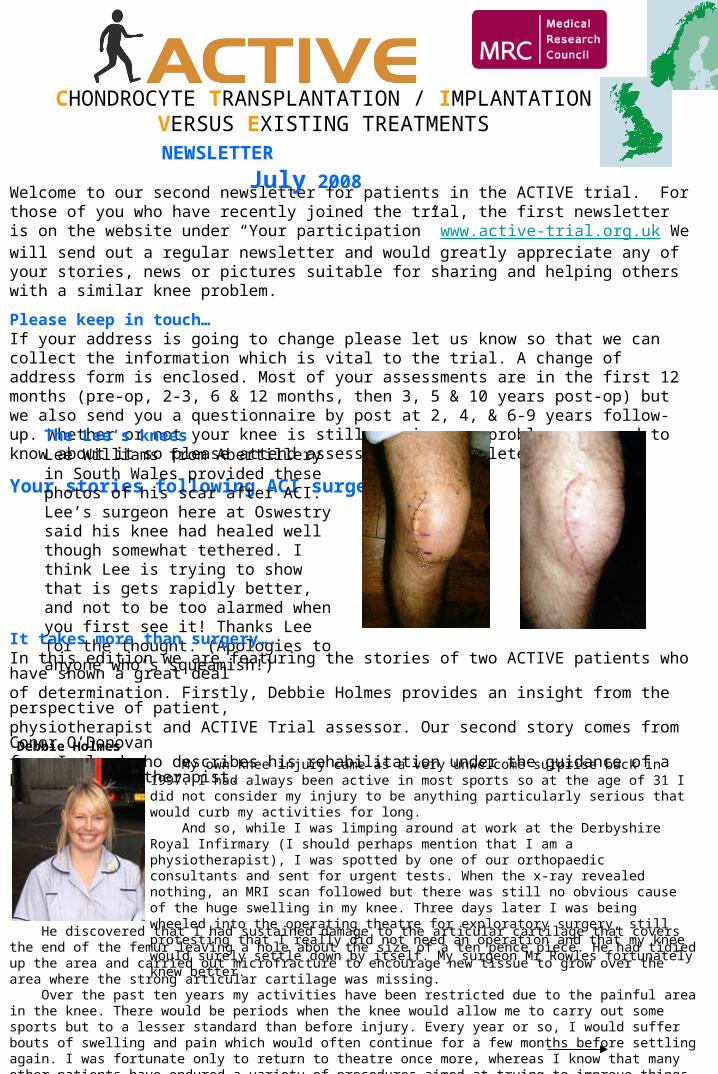
The Lee’s kneesLee Williams from Abertillery in South Wales provided these photos of his scar after ACI. Lee’s surgeon here at Oswestry said his knee had healed well though somewhat tethered. I think Lee is trying to show that is gets rapidly better, and not to be too alarmed when you first see it! Thanks Lee for the thought. (Apologies to anyone who’s squeamish!)
It takes more than surgery….In this edition we are featuring the stories of two ACTIVE patients who have shown a great dealof determination. Firstly, Debbie Holmes provides an insight from the perspective of patient, physiotherapist and ACTIVE Trial assessor. Our second story comes from Conor O’Donovan from Ireland who describes his rehabilitation under the guidance of a private physiotherapist.
My own knee injury came as a very unwelcome surprise back in 1997. I had always been active in most sports so at the age of 31 I did not consider my injury to be anything particularly serious that would curb my activities for long. And so, while I was limping around at work at the Derbyshire Royal Infirmary (I should perhaps mention that I am a physiotherapist), I was spotted by one of our orthopaedic consultants and sent for urgent tests. When the x-ray revealed nothing, an MRI scan followed but there was still no obvious cause of the huge swelling in my knee. Three days later I was being wheeled into the operating theatre for exploratory surgery, still protesting that I really did not need an operation and that my knee would surely settle down by itself. My surgeon Mr Rowles fortunately knew better.
Debbie Holmes
He discovered that I had sustained damage to the articular cartilage that covers the end of the femur leaving a hole about the size of a ten pence piece. He had tidied up the area and carried out microfracture to encourage new tissue to grow over the area where the strong articular cartilage was missing. Over the past ten years my activities have been restricted due to the painful area in the knee. There would be periods when the knee would allow me to carry out some sports but to a lesser standard than before injury. Every year or so, I would suffer bouts of swelling and pain which would often continue for a few months before settling again. I was fortunate only to return to theatre once more, whereas I know that many other patients have endured a variety of procedures aimed at trying to improve things.
There were periods of devastation as I was often unable to do the things I loved. Working as a physiotherapist is very difficult when you are on crutches more often than your patients. There were often spells when I would be confined to deskwork; always with the underlying fear that I could lose the job that I loved should the hospital declare me unfit to fulfil the role. Fun activities with my young family were often impossible or frustrating and I have to confess that I was probably not all that easy to live with at times. It was during one painful flare-up that I began to look into the current work being done on chondral injuries. Some of the operations that are being tried and tested throughout the world are not available on the NHS as there is not yet sufficient evidence to prove their effectiveness. This was certainly the case at my own local hospital where I had a surgeon willing to try a different procedure but no funds available from the local authorities to pay for it. My only option was to seek treatment from a centre that had funding to carry out the surgery as partof a research trial. I discovered that such a trial was about to start at the RJAH Orthopaedic Hospital nearOswestry and was delighted when they agreed to see me and accepted me into their ACTIVE trial. I was informed a few weeks before my surgery that I would be having Autologous Chondrocyte Implantation. This procedure involves two operations, one to harvest the cartilage cells for growing in the laboratory and then a larger operation three weeks later to insert the new cells into the knee under a membrane. I underwent surgery in May of 2006, my knee swollen from a flare-up that had lasted the previous seven months and had shown no signs of settling. I was more than ready to surrender to any surgery that might provide some relief. It is now two years since my operation and I am progressing well. I do walk with a slight limp due tosome minor discomfort but I have not had swelling or a flare up since the operation. I have not returned tomany high impact sports but I am able to walk unlimited distances and participate in high energy cyclingclasses at the gym. I think in terms of sport my priorities have changed and I am no longer prepared to riskfurther devastating injury when I can at least keep fit by doing lower impact sports. More importantly, I am back at work and carrying out my full duties on the wards. This is not to saythat the process has been an easy one. Autologous Chondrocyte Implantation has a difficult and lengthyrecovery period requiring hard work and patience. I am fortunate to have a sympathetic employer who afforded me all the time I needed to recover and has graded my return to work so that I do not endanger my knee. It is thought that it takes as long as 12 to 24 months for the new cells to mature and reach their maximum potential. Other procedures have a quicker recovery but until the much-needed research is complete there are many unanswered questions as to the most effective way to treat these injuries.
Conor O’Donovan’s story Ever since I can remember I played all kind of sports - golf, soccer, rugby, badminton, Gaelic football and hurling. As I got older I began to concentrate more on hurling which is a contact sport played in Ireland and is the fastest field game in the world. During my hurling career I injured my right knee three times. On each occasion I was able to resume playing hurling following several weeks of rest and rehabilitation without having to undergo surgery. My knee would have a tendency to feel a little bit uncomfortable at times, especially during the close season. I continued playing hurling until 2003. During that year though for no obvious reason my knee began swelling each time I played, even though I didn’t experience any pain. In 2003 I had keyhole surgery and the surgeon told me there was considerable wear and tear to the cartilage. It was not possible for him to do any real repair work and all that he could really do was a tidying up job. Then his next remark metaphorically pulled the rug from under my feet when he said that I probably would require a knee replacement in ten to fifteen years time. I was gutted. Even though I was 41 at that time I had hoped to continue to be active well into my later years. But this news brought my hopes to a shuddering halt. A year or so later I returned to light, low stress sports activities such as jogging, swimming, golf and cycling just to be active. Then on one occasion as I was playing a fun game of tennis I had to reach for the ball. In doing so my weight transferred onto my bent knee and a searing bolt of pain shot through the knee joint. It was obvious to me then that there really was a serious problem with my knee. To continue to stress the knee joint in this manner would be detrimental to its condition and would mean that a replacement knee would be inevitable. Around this time I became aware of a procedure which involved a knee cartilage transplant and wondered could this work for me? My surgeon informed me that this type of surgery was not carried out in Ireland but he gave me the name of the RJAH, Oswestry where Autologous Chondrocyte Implantation (ACI) was carried out. During my consultation with Professor Richardson I was asked if I would consider participating in the ACTIVE trial. I was delighted to accept this invitation and was later informed that I was randomly selected for ACI.
The ACI treatment is a two stage surgical procedure. In January 2007 I had the first stage which was keyhole surgery in my right knee to extract some healthy cartilage tissue from which new cartilage cells were then grown in the laboratory over the following three weeks. The following month I had open knee surgery when the newly grown cartilage cells were implanted into the defect in my right knee. The cells were sealed in by a patch over the defect made from a strip of membrane taken from my shin bone, called periosteum.
After my discharge from the hospital I knew I was facing a lengthy period of rehabilitation. I learnt that it is vitally important to have a good physiotherapist, that you fully adhere to the rehabilitation protocol set out for your recovery, and that you have good support at home.
Continued on next page
My first physiotherapy appointment was in March, a week after arriving home from the operation. I was very fortunate that this particular physiotherapist had previously treated a patient who had ACI surgery in Australia and was familiar with the rehabilitation requirements.
From March to May I attended the physiotherapist on a weekly basis, dropping down to every other week from June - July, then every three weeks with my final session in November 2007. During this period my physiotherapist adapted the rehabilitation protocol to enable me to do all the necessary exercises in the comfort of my own home (with the exception of going to the swimming pool).
With the benefit of hindsight I could have been more proactive in planning my recovery as this would have enabled me to manage it a lot better. I should have contacted my physiotherapist a couple of weeks prior to my surgery and put him in the picture. That way a post-operative management plan could have been devised in advance of my surgery. The first part of that plan would have been to have my first post-operative physiotherapy session already pre-booked rather than waiting until after the surgery to book it. Also by informing him well in advance the physiotherapist would have had time to compile a list of items I would need to assist me through the rehabilitation period and that I could have these items already in place prior to my surgery.
The following is a list of items I ended up acquiring during my recovery period to assist with my rehabilitation: •KNEEHAB (this is an electrical muscle stimulation product to treat thigh muscle wastage)•Inflatable Roller Ball•Medical Stocking to reduce swelling in foot and calf muscle•Bio Oil to help the surgical scar to heal.•Exercise Bike•Cryo-Cuff (to help reduce knee swelling)•Ankle Weights•Step-up block•Aqua Belt (for jogging in swimming pool)•Air Disc/Wobble Air Cushion•Mini Trampoline
At various stages during a long physically and mentally demanding recovery period I used each of the above items. Each item played a vital part in the recovery process. However it would have been much more convenient if I already had them in place prior to the commencement of my rehabilitation programme. My wife was a great support and she did a lot of running about the place getting things for me.
While the recovery was slow and demanding almost every day brought some degree of improvement. Because I work in an office I was able to return to work in April 2007, nine weeks after stage 2. Another milestone was April 19th when I finally discontinued using the crutches. The 19th July 2007 was a significant milestone in my recovery as I played my first round of golf following my surgery.
It is now sixteen months since I had the ACI surgery. During this time I have been able to resume all forms of normal activities including quite an amount of heavy lifting, owing to renovations to our house. I am playing golf on a regular basis without any pain or problems in my knee. It is also satisfying to be able to draw a kick at my son’s football when I feel like it. I have done some light running without any pain or problems. But the ‘litmus’ test is in being able to put my weight on the bent knee without pain.
In order to reap the full benefits of the ACI surgery it is vitally important that one commits to doing the rehabilitation work in a serious and dedicated manner. I still need to do a little bit of maintenance work once or twice a week in order to keep the knee strong. It is very likely that I will have to continue indefinitely with this maintenance work. However, it will be a very small price to pay if it prevents my needing a new knee in the future.
ACTIVE Trial Office, ARC, RJAH Orthopaedic Hospital, Oswestry. SY10 7AG
Thanks Debbie and Conor for your stories. I’m sure there are many more stories we can feature so please contact me if you’d like to share yours. In particular, we’d like to include stories from patients who have had microfracture or one of the other non-ACI treatments in the trial. We could also have a helpful tips column where you can share little snippets of information to help other patients, or to help staff working on the trial. I look forward to hearing from you. Best wishes,