55
Welcome to the OPQC NAS September 2017 Sustain Period Call Thank you for joining; please sign in the chat box with the names of all webinar participants and your hospital affiliation.
| Date post: | 12-Aug-2018 |
| Category: |
Documents |
| Upload: | hoangquynh |
| View: | 214 times |
| Download: | 0 times |

Welcome to the OPQC NAS
September 2017 Sustain Period Call
Thank you for joining;
please sign in the chat
box with the names of
all webinar participants
and your hospital
affiliation.

Neonatal Abstinence
Syndrome Project
Quarterly Sustain Period Call
Ohio Perinatal Quality Collaborative
September 19, 2017
Welcome!
The OPQC NAS Project is funded by the Ohio Department of Medicaid and administered by the Ohio Colleges of Medicine Government Resource Center. The
views expressed in this presentation are solely those of the authors and do not represent the views of the state of Ohio or federal Medicaid programs.

The line will be placed on
Group Mute
To ask a question:
Click on the Raised Hand icon
You can type your question
in to the Chat Box
You can use 60# to come off of
GROUP MUTE (and 61# to go back on)
3

Time Topic Presenter
3:00 pm Welcome & Agenda Review Susan Ford, MSN, RN
3:05pm Data
• Aggregate Data Overview
• Data Entry Updates
• No babies edits
• Transfer vs Discharge
Moira Crowley, MD
Susan Ford
3:25 pm NAS Care at & After Discharge
• Infant disposition/safety plan at discharge
• f/u clinic at CCHMC
Susan Ford
Jenny McAllister, MD
3:45 pm Questions/Team Discussion Susan Ford
3:55 pm Upcoming Conferences/Next Steps Susan Ford
Agenda
REMEMBER: You
can use 60# to come
off of GROUP MUTE 4

Key Driver DiagramProject Name: OPQC Neonatal NAS Leader: Walsh
SMART AIM
KEY DRIVERS INTERVENTIONS
By increasing identification of and
compassionate withdrawal treatment for full-term infants born with
Neonatal Abstinence Syndrome (NAS), we will
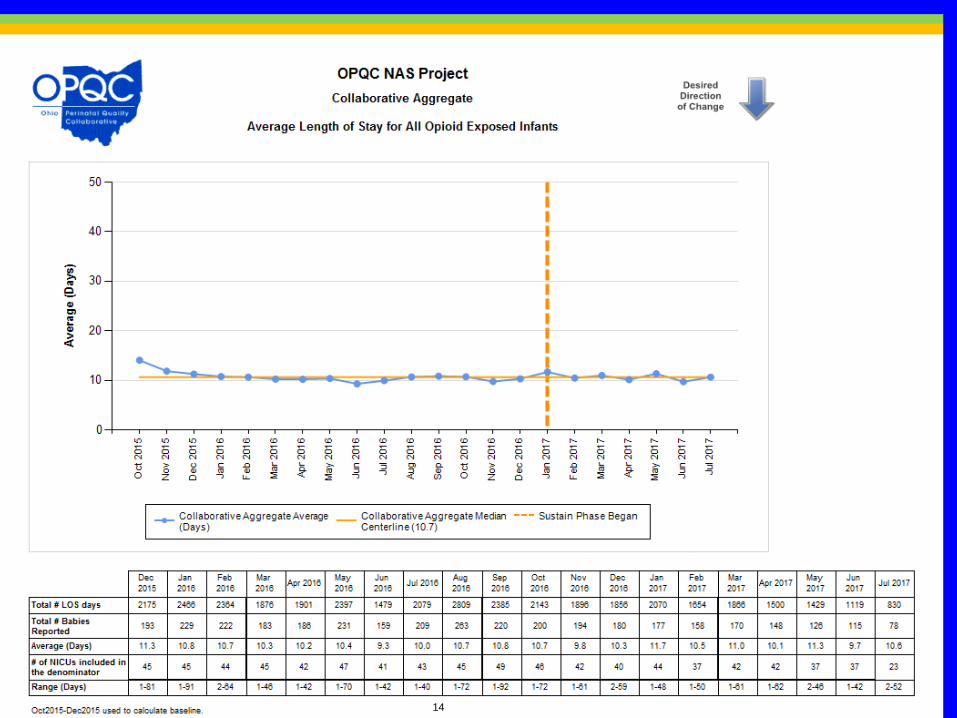
reduce length of stay by 1 day across participating sites by June 30, 2016.
Improve recognition and non-judgmental support for Narcotic
addicted women and infants
Connect with outpatient support and treatment program prior to
discharge
Standardize NAS Treatment Protocol
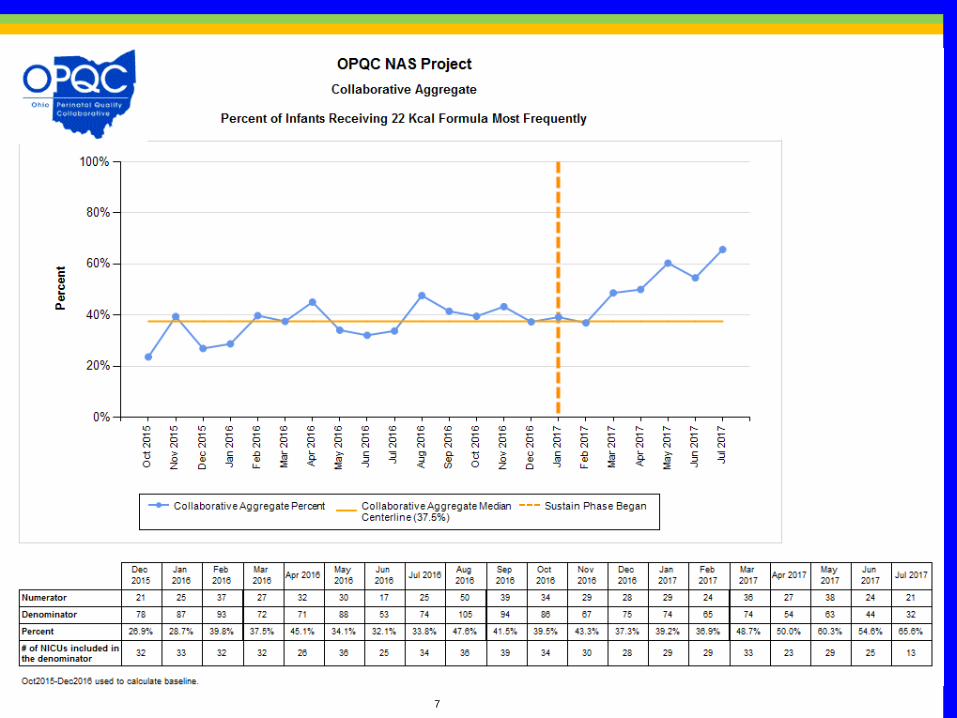
Optimize Non-Pharmacologic Rx Bundle
Initiate Rx If NAS score > 8 twice. Stabilization/ Escalation Phase Wean when stable for 48 hrs by 10%
daily.
Swaddling, low stimulation. Encourage kangaroo care Feed on demand- MBM if appropriate
or lactose free, 22 cal formula
All MD and RN staff to view “Nurture the Mother- Nurture the Child”
Monthly education on addiction care
Attain high reliability in NAS scoring by nursing staff
Partner with Families to Establish Safety Plan for Infant
• Fulltime RN staff at Level 2 and 3 to complete D’Apolito NAS scoring training video and achieve 90% reliability.
Establish agreement with outpatient program and/or Mental Health
Utilize Early Intervention Services
Collaborate with DHS/ CPS to ensure infant safety.
Prenatal Identification of MomImplement Optimal Med Rx Program
Engage families in Safety Planning. Partner with other stakeholders to influence policy and primary
prevention. Provide primary prevention materials to sites.
To reduce the number of moms and babies with narcotic exposure, and
reduce the need for treatment of NAS.
GLOBAL AIM
5

6
7

8

9
10

11

12

13
14

15

Same chart; different y axis
(ability to see greater detail)
16

17

Data Updates
• No Babies
– Please open a New Form each month
– Do NOT edit a previous month’s submission
of “no babies” for a new month
18

Data Updates
• Transfer vs Discharge
– Do NOT enter data on NAS infant if he/she is
being transferred to another site for NAS
treatment. That will result in duplicate
submissions for one infant. The treating site will
enter data on that infant after discharge.
Response if “other” is chosen for infant disposition
Level 3
transferred to XXX hospital
Transferred to XXX Hospital
Transferred to XXX per parent request for medication treatment
transfer to XXX for treatment
Transfer to XXX for pharmacologic treatment
19

20

Aggregate Safety Plan/Social Work
replies from OQPC database
Answer to Safety Plan/Social Work
Questionn (%)
Yes 637 (64.0%)
No 313 (31.4%)
Can't Determine 46 (4.6%)
21

Answer to Disposition Question on NAS Sustain Form
n (%)
Discharged with mother743
(74.6%)
Discharged with other family member (other than mother)
98(9.8%)
Discharged with foster/adoptive care135
(13.6%)
Other20
(2.0%)
Aggregate Infant Disposition
from OQPC database
22

From the American Academy of Pediatrics
During follow-up, infants with NAS particularly require
(1) neurodevelopmental assessments to identify motor deficits, cognitive delays, or
relative microcephaly
(2) psycho-behavioral assessments to identify hyperactivity, impulsivity, and
attention-deficit in preschool-aged children, as well as school absence, school failure,
and other behavioral problems in school-aged children
(3) ophthalmologic assessment to identify nystagmus, strabismus, refractive errors,
and other visual defects
(4) growth and nutritional assessment to identify failure to thrive and short stature
(5) family support assessments to exclude continuous maternal substance abuse and
child abuse.
Parents need to be educated about sudden infant deaths as well as complications
due to perinatal infections. The complexity and challenging nature of the home
atmosphere should never be underestimated in these situations. The importance of
an optimal home environment for the global development of these children should be
emphasized to all parents.
http://pediatrics.aappublications.org/content/134/2/e54723

Follow Up Care of NAS Infants
Neonatal Abstinence Follow Up ClinicCincinnati Children’s Hospital Medical Center
Jennifer McAllister, MD
24

NAS Clinic
• Since 2012 we have been following babies
with NAS who were discharged home on
phenobarbital in NICU follow up clinic at
CCHMC
– This arose from a need to have expertise in
weaning these babies from phenobarbital as
well as understanding the NAS patient
– Infants were scheduled among other NICU
follow up babies including former preemies,
surgical babies, and other infants with complex
medical needs
25

NAS Clinic
• In 2015, we opened a specialized clinic under our current NICU follow-up clinic dedicated specifically to babies treated for NAS
• Mission Statement:– It is our goal that NAS Clinic is a unique,
comprehensive, collaborative clinic in which we provide care for those infants exposed to opioids prenatally and infants treated for NAS after discharge. We will provide support for parents and caregivers, and we will establish a foundation for long term research on the effects of in utero opioid exposure.
26

Referrals
• Our referral base consists of 14 level II and III hospitals in the Greater Cincinnati, Northern Kentucky, Dayton area
• All infants treated for NAS are referred to our clinic
– If they are >32 weeks without other complex medical issues they are seen in NAS clinic
– Otherwise we follow them in regular NICU follow up clinic
27
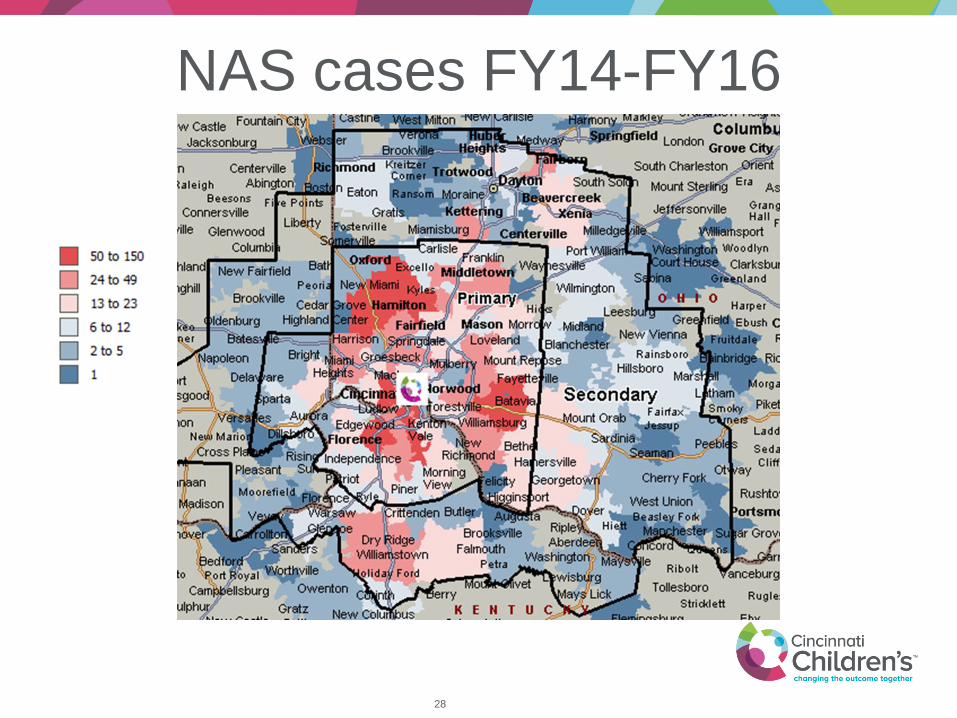
NAS cases FY14-FY16
28

Clinic Patients
• We receive 20-25 referrals for new visits
each month
• We see approximately 500 new visits per
year
• We follow from birth until age 2-3 years
29

Discharge Disposition
• In a study of NAS follow-up patients, 25% went home with mother, 30% went home with kinship care, 45% went to foster/adoptive families
• At 2 year follow up, 20% with mothers, 35% with kinship care, 45% foster/adoptive families
• Currently, in JFS, 70% of all babies in care are due to substance use
30

Services Provided
• Educational information and NAS Clinic Brochure for parents prior to discharge from the hospital
• Appointment scheduled prior to discharge
• Monitoring of ongoing NAS symptoms after hospital discharge
• Weaning instructions for infants on home NAS medications including phenobarbital, clonidine, and gabapentin
• Nutrition counseling and assessment of growth
• Standardized developmental testing and evaluation
• Social services and referrals to community programs
31

Our Team
• Clinic visits
– MD/NNP
– OT
– SW
– RD via phone/sometimes in person
• Office Staffing
– M-F, 9-5 RNs field phone calls, referrals, and perform pre-clinic planning
– MD on call 24/7
32

Scheduling
• NAS clinic is 1-2 half-days/week at both
Main Campus and Liberty Campus
• First clinic visit within 2 weeks of hospital
discharge
• Subsequent visits every 4-6 months
depending on severity of issues
33

NAS Follow Up Clinic
First clinic visit scheduled within 2 weeks of d/c OT and SW evaluation at each new visit
Evaluate home formula and caloric concentration
Next visit in 1 mos
Next visit at 4-6 mos with ASQ-SE• Refer to Ophthalmology if strabismus
present or reported• Vision screening if >6 months• Refer to PT if torticollis present
Next visit at 9-12 mos with ASQ-SE • Refer for Audiology evaluation at 1 year• Vision screening if not previously performed
Next visit at 15-18 mos with ASQ-SE• Schedule Bayley• Hep C testing if recommended• Vision screen if >1 year since last screen
Next visit at 22-26 mos after Bayley performed
• Consider Child Behavior Checklist• Refer to DDBP if needed
• Visits can be scheduled more frequently if necessary
• OT should evaluate any baby with tone issues, developmental concerns, or any child with abnormal ASQ- SE
• Use .NASNOTE template
• Common diagnoses:• Neonatal abstinence syndrome P96.1 (0-28 days only)• Other long term drug therapy (list drug) - if still on medication Z79.899 • Personal history of other drug therapy (list drugs) - if off of meds Z92.29• Perinatal Hepatitis C exposure Z20.5• Screening for developmental handicaps in early childhood Z13.4• Vision screen with abnormal findings Z01.01, without abnormal findings
Z01.00• Abnormal posture, hypertonia• Torticollis, positional plagiocephaly• Diaper rash, thrush
NoHome on adjunct therapy?
Suggested Wean:• No/mild symptoms: cut dose by
50% x1 week, then d/c• Moderate symptoms, cut dose by
25% each week until d/c• Severe symptoms: continue current
dose and re-evaluate at next visit
Yes
34

Short and Long Term Issues in the
NAS Patient
35

Continued Symptoms of NAS
• Most commonly noted symptoms at follow-
up:
– Periodic fast breathing
– Nasal stuffiness/congestion
– Reflux, spitting up
– Tremors
– Crying spells, irritability
– Mottling
– Hypertonia
36

Continued Symptoms of NAS
• Recommendations:
– non-pharmacologic treatment (swaddling, skin to skin, low stimulus environment)
– Calming strategies• 5 S’s
– Overall assessment of functioning: eat, sleep, console
– Stretches, range of motion
– Positions for play
– Tummy time
37
Diaper Rash
• Have had babies evaluated in the ED after
hospital discharge due to diaper rash
• Diaper rash recommendations:
– Criticaid and Cavilon if severe and broken
down
– Assess for yeast
38

Feeding and Growth• Transition from hospital formula to WIC formula
– Have seen good results with Gerber Soothe
– WIC will allow Enfamil Gentlease with a diagnosis of NAS
– If continued GI distress, we have had success with Alimentum
• We advise 20kcal formula– In clinic, volumes reported are quite high and if
remains on higher calorie, have seen increase weight gain
• Many NAS babies with reflux– Consider treatment if having difficulties with feeding
secondary to reflux
– Consider smaller, frequent feedings
39

Breastfeeding• Breastfeeding should be encouraged if
mother’s are in a stable treatment program
• Babies are not at risk for withdrawal as mother’s wean from breastfeeding, little methadone or buprenorphine excreted in breastmilk
• May increase compliance with medication assisted treatment
• Mothers need help after discharge– As many as 60% of those who initiate
breastfeeding stop after 6 days
40

Hepatitis C
• Risk of transmission from mother to baby is about 5%
• Transmission depends on concentration of HCV RNA in the mother’s blood– If mother’s have undetectable viral load, risk of transmission very low
– 15-20% of people will spontaneously clear infection and will only have positive antibody
– Up to 10-20% transmission with co-infection with HIV
• HCV RNA testing can be performed as early at 2 months, but is not accurate and would need to be repeated (false negatives)
• Recommendation is HCV antibody testing at 18 months
• Breastfeeding is safe with HCV, mothers should consider pumping if nipples are cracked/bleeding until healed
• Important to receive Hepatitis A and B vaccines for this population
41

Torticollis• Incidence of positional/postural torticollis on the rise
since “back to sleep” with associated plagiocephaly
• In the NAS population, we have seen a 6x higher incidence of torticollis than in the general population (11% of infants seen in clinic)
• 2/3 of these infants also have plagiocephaly
• About 1/3 received services through HMG or KY First Steps
• Over 50% required additional Physical Therapy
• Prevention is key, early diagnosis helpful in resolution– Refer to PT if present
42

Social Emotional Problems
• At each visit, we are performing Ages and
Stages Social Emotional Questionnaire
• If concerned, consider referral for family
counseling, psychiatry, behavioral pediatrics
– At CCHMC we have Baby TIP (Therapeutic
Interagency Program)
• Early Head Start
• Weekly mental health treatment of child and
parent/guardian
43

Sensory Processing Difficulties• Over responders
– Dislike textures in fabric, food, brushing hair, hugging, cuddling, poor sleepers
• Under responders– Lack of awareness to pain, people, “selective hearing,”
poor potty-trainers
• Sensory seekers– Fidgeting, climbing, jumping, “no fear,” impulsive,
making loud noises, sucking, biting
• In NAS clinic, OT will perform sensory profile– Usual recommendation is outpatient
occupational therapy
45

Visual Issues
• Nystagmus
• Strabismus
• Reduced acuity
• Delayed visual maturation
• Refractive errors
• Cerebral visual impairment
• Recommend visual screen starting at 6 months– We perform vision screen with Welch Allyn Spot Vision screener
at 6 months and then annually afterwards
– Any nystagmus warrants referral at the time of diagnosis
– If strabismus still present at 4 months would refer at that time
46
Behavioral Problems
• Inattention/hyperactivity ADHD
– Up to 20% greater risk, recognized in
preschool age
• Sleep disturbances
• Oppositional/defiant
• Wide range of behavioral issues
47

Anesthesia Effects
• May have increased tolerance to opiate
pain medication and anesthesia
• Difficulties with pain/anesthesia control
during surgery and dental procedures
• When performing pre-surgery physicals,
make sure history of in utero opioid
exposure is documented
48

Developmental Delays
• In our recent study, we looked at Bayley
exam scores on our NAS patients at 2
years
– We found lower scores for NAS patients
compared to normal infants
49
Cognitive, Learning, Memory
• Many studies show poor learning and memory
– Deficits in spatial learning
• Lower scores for intelligence and school readiness
• Large national study in Australia >2000 infants with NAS matched for gestation, socioeconomic status, gender
– Mean test scores in grade 3 significantly lower
– Progressive worsening
– By grade 7, NAS children scored lower than matched children in grade 5
50

Future Directions
• Expand to include some exposed but not
treated infants
• Follow patients until age 5 or longer
• Continued research projects
51
Resources
• Help Me Grow
• Every Child Succeeds
• Early Head Start
• OT/PT
• Developmental and Behavioral Pediatrics
• Child Psychiatry
• Local agencies in your community
52

Questions/Discussion
REMEMBER: You
can use 60# to come
off of GROUP MUTE 53

Upcoming Conferences of Interest
• American Academy of Pediatrics–Ohio Chapter, October 27-28th
– AAP Ohio Annual Meeting
– Register at http://ohioaap.org/AnnualMeeting
– Panel Discussion: Opiate Crisis in Ohio
• Sean Loudin, MD, FAAP, Marshall University
• Scott Wexelblatt, MD, FAAP, CCHMC
• Sarah Adams, MD, FAAP, Akron Children’s Hospital
• Denise Strimple, NAS Newborn Foster Parent
• Cincinnati Children’s Hospital Medical Center, Friday November 7th
– Changing the Future of Children of Addicted Parents
– Register at https://cchmc.cloud-cme.com/aph.aspx?P=5&EID=20811
– NAS related Breakout Sessions include:
• Neonatal Abstinence Syndrome; Jonathon Davis, MD, Tufts Medical Center
• Medical Care for the Neonatal Abstinence Syndrome (NAS) Patient;
Jennifer McAllister, MD CCHMC
• Navigating Family Involvement with Children’s Services and the Court
System: A Panel Discussion
54

Next Steps
• Please continue to submit Data for 2017 (under Sustain tab on SharePoint)
• February: 1 site has not yet submitted any monthly data
• March: 1 site has not yet submitted any monthly data
• April: 1 site has not yet submitted any monthly data
• May: 6 sites have not yet submitted any monthly data
• June: 8 sites have not yet submitted any monthly data
• July: 22 sites have not yet submitted any monthly data
• August: 31 sites have not yet submitted monthly data
• Next Quarterly Sustain Phase Call will be December 19th
REMEMBER: You
can use 60# to come
off of GROUP MUTE 55

It takes a village…







![[XLS] · Web viewS/o Rangappa,Anajanapura,Shikaripura Tq Latha-13/NAS/14/2013-14 W/o Hanumanthappa.S,Nittakki, Dyavanahalli Post,,Soraba Tq, Maharudrappa -13/NAS/13/13-14 S/o Chandrappa,Devangada,Anjanapura](https://static.documents.pub/doc/80x56/5adb63b77f8b9a52528e204e/xls-viewso-rangappaanajanapurashikaripura-tq-latha-13nas142013-14-wo-hanumanthappasnittakki.jpg)









