31
We’re All Getting Older! Maria Quintero-Conk, Ph.D. Tri-County Behavioral Healthcare [email protected]

We’re All Getting Older!
Maria Quintero-Conk, Ph.D.
Tri-County Behavioral Healthcare

Who is the Person with Intellectual
Disability?
• Intellectual Disability ▫ Deficits in general mental abilities
In Texas, IQ <70
▫ Impairment in adaptive functioning for the individual’s age
and socio-cultural background
▫ Onset during the developmental period In Texas, before age 18
▫ Severity: Mild, Moderate, Severe, & Profound

Autism Spectrum Disorder • Neurodevelopmental Disorder • Diagnostic criteria:
▫ Persistent deficits in social communication and social interaction across multiple contexts
▫ Restricted, repetitive patterns of behavior, interests, or activities ▫ Symptoms must be present in the early developmental period
(but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life)
▫ Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning
▫ These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay

Related Condition
Note: Some wounded may veterans may be eligible for IDD services

Society has changed… Deinstitutionalization…Normalization
For the first time in history, we’re supporting large
numbers of people with developmental disabilities into their senior years.
Society has changed…
or has it?

What is “Normal” Aging?
• Cardiovascular system
▫ Slower heart rate
▫ Heart enlarges
▫ Blood vessels stiffen, causing heart to work harder
• Bones, joints and muscles
▫ Bones shrink in size and density
▫ Muscles lose strength and flexibility
▫ Coordination and balance are more difficult

What is “Normal” Aging?
• Digestive system ▫ Constipation! Less fluids, less exercise, more medicines
• Bladder and urinary tract ▫ Loss of bladder control Menopause
Prostate enlargement
• Memory ▫ Less efficient ▫ Longer to learn ▫ Remembering familiar words or names

What is “Normal” Aging?
• Skin
▫ Thinner and less elastic Wrinkles
▫ Less sweat and oil Dry skin
▫ Less fat storage under skin Visible bones
• Immune system
▫ Less efficient

What is “Normal” Aging?
• Vision ▫ Dryness ▫ Lens loses focus ▫ Floaters are common
• Hearing ▫ Changes in nerves of hearing and ear structures impair
hearing ▫ Higher frequencies become more difficult to hear
• Smell & taste ▫ Smell diminishes ▫ In some cases, taste is also reduced

What is “Normal” Aging?
• Dental health
▫ Less saliva, resulting in dry mouth and cavities
▫ Receding gums
▫ Teeth become weaker, brittle
• Hair & nails
▫ Drier, causing itching (head) and ridges (nails)
▫ Common fungal infections
What is “Normal” Aging?
• Hormones ▫ Sugar and carbohydrate metabolism changes and can
promote diabetes ▫ Metabolisms of fat, cholesterol, calcium and vitamin D
are common altered ▫ Thyroid malfunction is not unusual ▫ Erectile dysfunction and vaginal dryness
• Sleep ▫ Difficulty going to sleep ▫ More episodes of waking—sleep fragmentation ▫ Overall decline in REM sleep

The top 10 leading causes of death in
the U.S. • Heart disease.
• Cancer (malignant neoplasms)
• Chronic lower respiratory disease.
• Accidents (unintentional injuries)
• Stroke (cerebrovascular diseases)
• Alzheimer's disease.
• Diabetes.
• Influenza and pneumonia.
http://www.medicalnewstoday.com/articles/282929.php

Aging and Developmental Disability
Life Span (U.S.) 78.94 yrs for general population, vs.
50.4-58.7 yrs state intellectual and
developmental disabilities systems
61.2-63.0 yrs in Medicaid data
Cancer Higher proportion of gastrointestinal cancer
Leukemia in children with Down syndrome
Women less likely to be tested for cervical
cancer
Heart Disease Almost half of children with Down syndrome
are affected by heart disease

Aging and Developmental Disability
Respiratory Illness Hygiene, hands to mouth, increased infection risk
Higher than general population
Dental Health Poor oral hygiene
Lack of dental care
Poor fitting dentures
Increased risk of choking/aspiration
Tongue thrust, mouth breathers
Sensory Health Vision & hearing problems common correlates of
developmental disability
Inability to communicate changes in detail

Aging and Developmental Disability
Physical Health Increased risk of osteoporosis secondary to
medication
History of sedentary lifestyle
Fall risk with lack of understanding , sensory
problems, medications
Identified complications with Cerebral Palsy
Gastrointestinal
Health
Higher incidence of GERD
Higher incidence of bowel obstruction
Greater incontinence, risk of skin effects
Mental Health…
Mental Health As We Age
• Get rid of stereotypes!
• But mental changes do occur ▫ It may take longer to learn new information and
tasks (rate of encoding is slower over time) ▫ Short-term memory changes with age; long-term
memory shows less age-related decline. ▫ Word-finding ability declines with age.

Mental Health As We Age http://www.apa.org/pi/aging/resources/guides/older.aspx
• Dementia presents in between 5 and 7% of adults over age 65 and 30% over age 85.
• 6% of older adults suffer from anxiety disorders
• The highest suicide rate of any age group is in older adults, primarily older Caucasian men who live alone.
• The incidence of sexual dysfunction increases with age for both men and women.
• Sleep problems increase with age, and about 50% of those over age 80 complain of sleep difficulty.

Mental Health As We Age http://www.apa.org/pi/aging/resources/guides/older.aspx
• 10 - 15 % percent of older adults exhibit hypochondriasis
• Prevalence of alcohol abuse and substance dependence among those age 65 and over is 2 to 5% for men and 1% for women, with opioid use sharply rising
• Drug abuse among older adults typically takes the form of prescription medication abuse, and older adults take 25 percent of the medication taken in the United States
• Behavior disorders in those over age 65 can take the form of physical aggression, motor over-activity (wandering), and disruptive verbal outbursts.

Mental Health in People with IDD as
They Age • Dementia risk for certain populations
• Co-occurring mental illness

Alzheimer’s Disease and Down
syndrome • Shared genetic risk
▫ Down syndrome – three chromosome 21 ▫ Chromosome 21 Carries a gene that produces one of the key proteins
involved with changes in the brain caused by Alzheimer’s
Has several genes involved in aging that increase the risk of Alzheimer’s
• Alzheimer’s disease affects about 30% of people with Down syndrome in their 50s. ▫ By their 60s, this number comes closer to 50%

What is Co-Occurring ID/ASD and MI?
“Dual Diagnosis” (the other one)
Substance Abuse
ID or ASD
Mental Illness
The concurrent presence of Intellectual Disability
and /or Autism Spectrum Disorder
And
Mental Illness
And possibly,
Substance Abuse
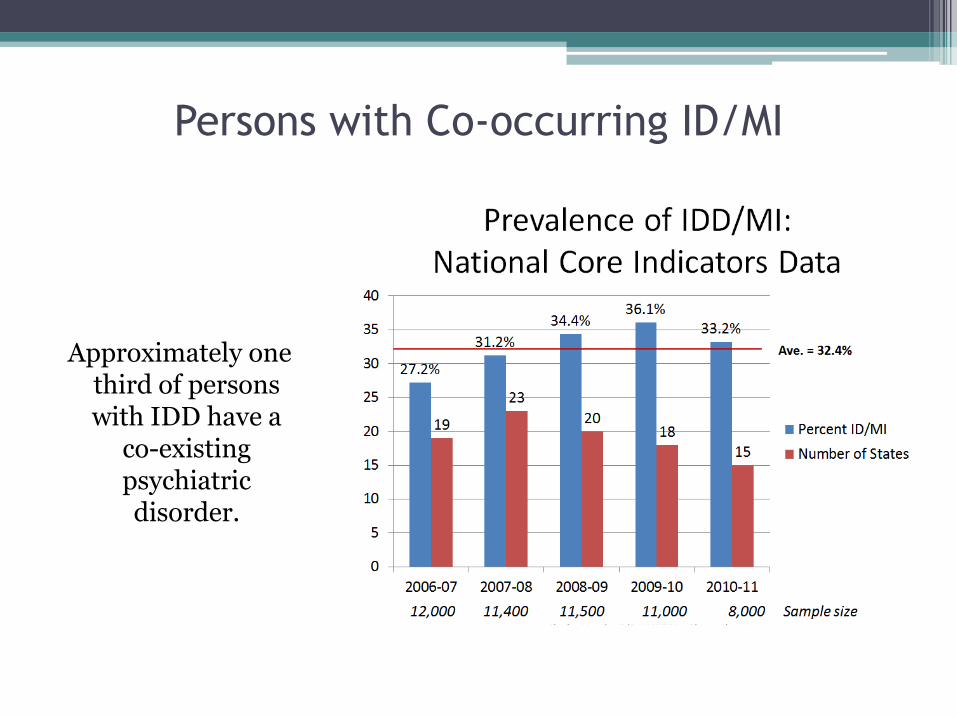
Persons with Co-occurring ID/MI
Approximately one third of persons with IDD have a
co-existing psychiatric disorder.

Texans with Co-Occurring
ID/ASD & MI
Population of Texas based on 2015 estimates at www.census.gov
27,469,114
Number of persons with ID Texas uses 2.5%
686,728
Number of Texans with co-occurring ID and MI (not including persons with ASD who do not have ID but do have MI)
222,500

General Considerations
The condition of dual diagnosis is often not correctly diagnosed.
MI is overshadowed by ID—by both the MH and ID systems: The presence of IDD masks the possibility of a mental illness.
Misinterpretation of symptoms of mental illness as inappropriate learned behaviors.
Lack of experience in treating persons with dual diagnoses
No specific clinical training; assumption that what works with general population can extend to people with ID/ASD complexity
• Medical issues often precipitate crises
▫ But clinicians and providers do not look for medical causes or communicate effectively across medical, ID and MH systems
• Overuse of medication; undesirable side effects
• High incidence of trauma, often overlooked

Establishing a Baseline:
NTG-EDSD • The National Task Group-Early Detection Screen for Dementia
(NTG-EDSD) ▫ Can be used for the early detection screening of adults with an
intellectual disability who are suspected or may be showing early signs of mild cognitive impairment or dementia.
▫ The NTG-EDSD is not an assessment or diagnostic instrument, but an administrative screen that can be used by staff and family caregivers to note functional decline and health problems and record information useful for further assessment.
▫ Use of the NTG-EDSD is recommended on annual or as indicated basis for people with Down syndrome beginning with age 40, and with other at-risk persons with intellectual or developmental disabilities when suspected of experiencing cognitive change.
• It is important to note that other conditions, such as thyroid disorders and depression, can also manifest with the same symptoms—Medical follow up & neurological assessments are necessary

Google “NTG-EDSD for the assessment instrument and the manual.
Barriers to Care
Aging in America Disability in America
• Stigma
• Lack of clinicians who specialize in aging
• Ageism – anti-aging culture
• Lack of models of care
• Poor reimbursement models
• Stigma
• Lack of clinicians who specialize in disabilities
• Ableism – anti-disability culture
• Lack of models of care
• Poor reimbursement models

http://ucp.org/wp-content/uploads/2013/02/preventive-health-care-screening-guidelines-for-people-aging-with-intellecutal-and-develpmental-disabilities.pdf

Just a few places to start…
• UTHealth - Kathleen Pace Murphy, PhD, MS, GNP-BC, RN
• Eunice Kennedy Shriver Center webinars, http://shriver.umassmed.edu/cdder/aging_idd_education
• Julie Moran, D.O. https://www.youtube.com/watch?v=H_N-yaId71s



















