26
What Do We Mean By Quality In PCI Institutional Requirements Dr Bernard Prendergast John Radcliffe Hospital, Oxford
| Date post: | 27-Dec-2015 |
| Category: |
Documents |
| Upload: | ronald-mitchell |
| View: | 215 times |
| Download: | 1 times |
What Do We Mean By Quality In PCIInstitutional Requirements
Dr Bernard PrendergastJohn Radcliffe Hospital, Oxford
NO CONFLICT OF INTEREST TO DECLARE
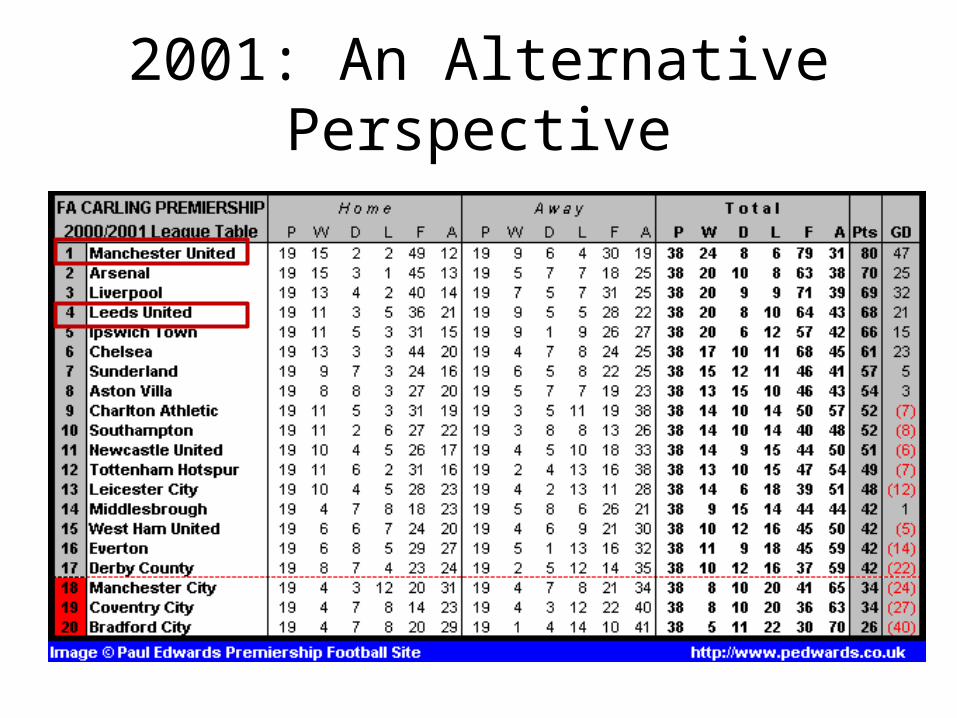
2001: An Alternative Perspective
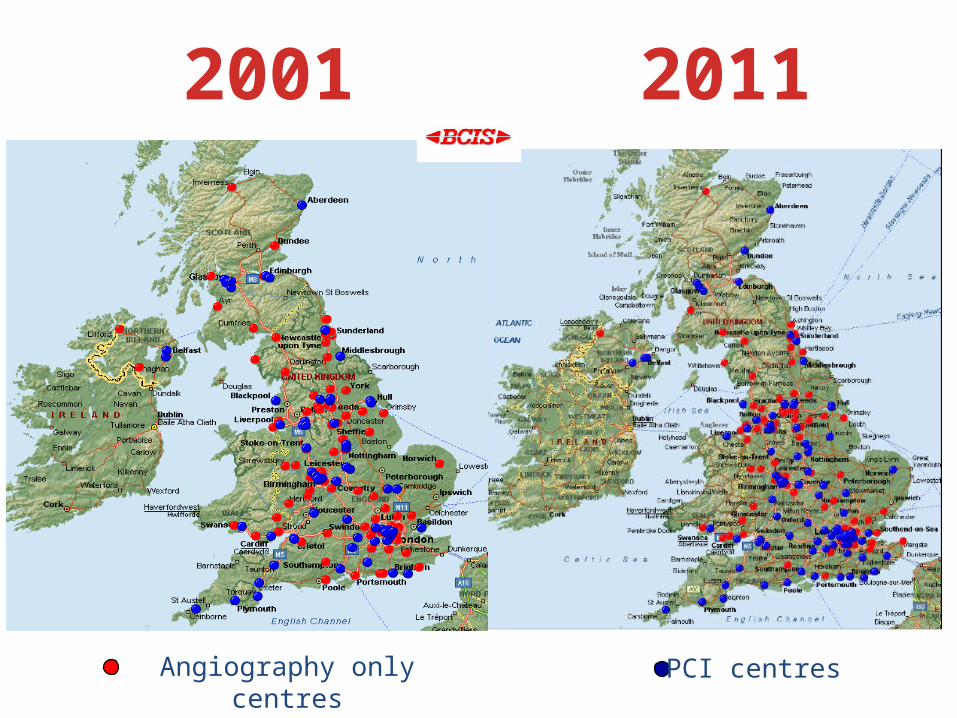
PCI centresAngiography only centres
2001 2011
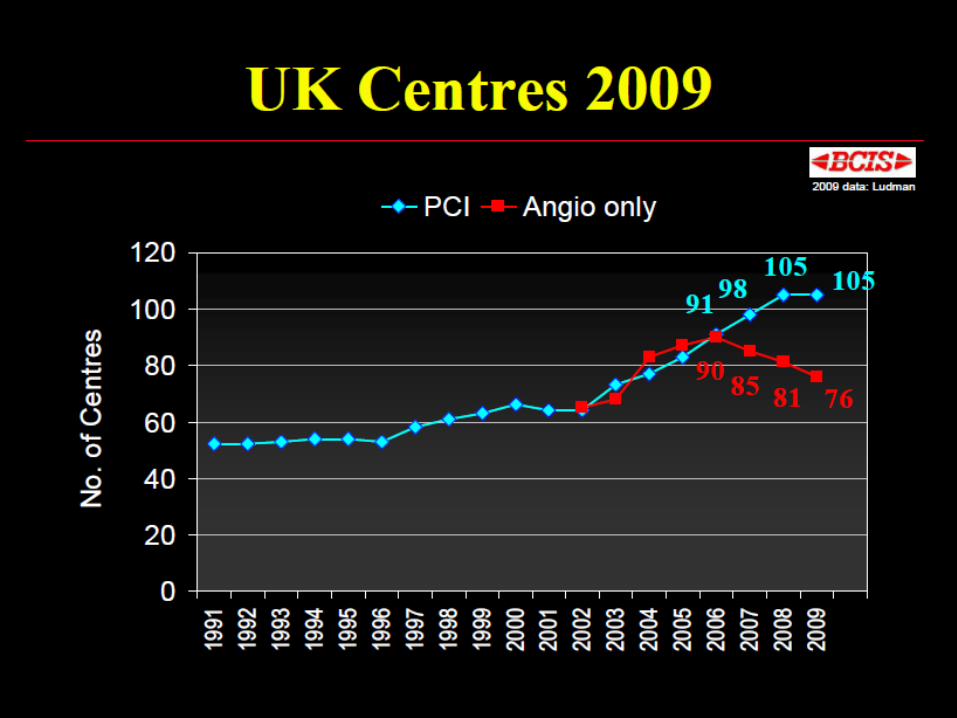
Key Questions 2011
• Do we need any more PCI centres in the UK?
• What should a PCI centre look like?

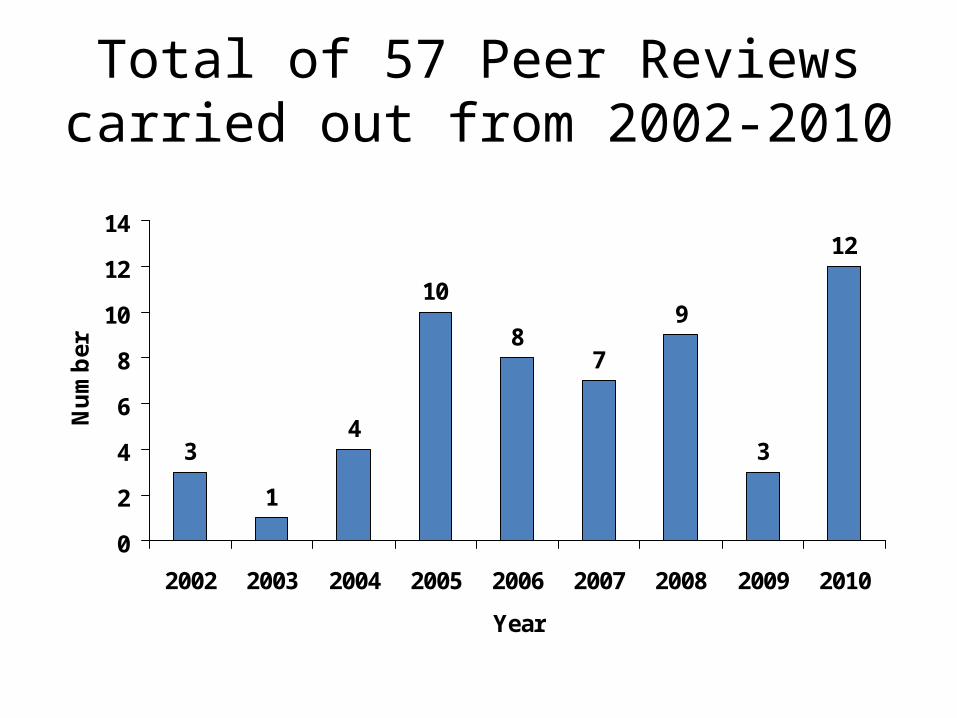
Total of 57 Peer Reviews carried out from 2002-2010
3
1
4
10
87
9
3
12
0
2
4
6
8
10
12
14
2002 2003 2004 2005 2006 2007 2008 2009 2010
Year
Nu
mb
er

“Angioplasty is like riding a bike”
The keepy-uppy argument 2008“The more I practice, the better I get”
The Numbers Debate
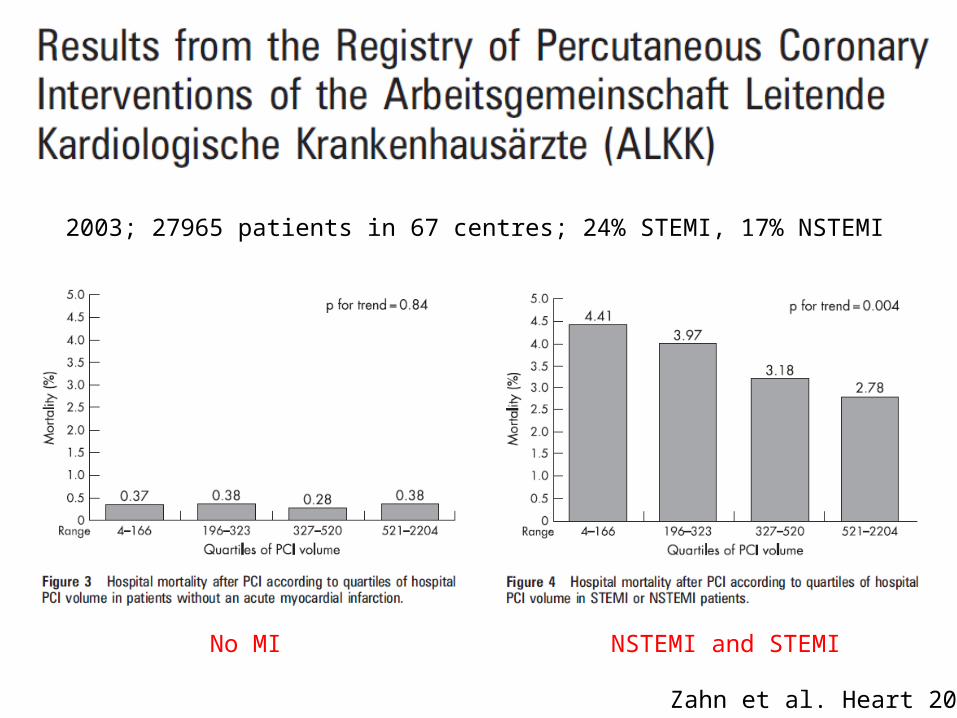
Zahn et al. Heart 2007
NSTEMI and STEMINo MI
2003; 27965 patients in 67 centres; 24% STEMI, 17% NSTEMI
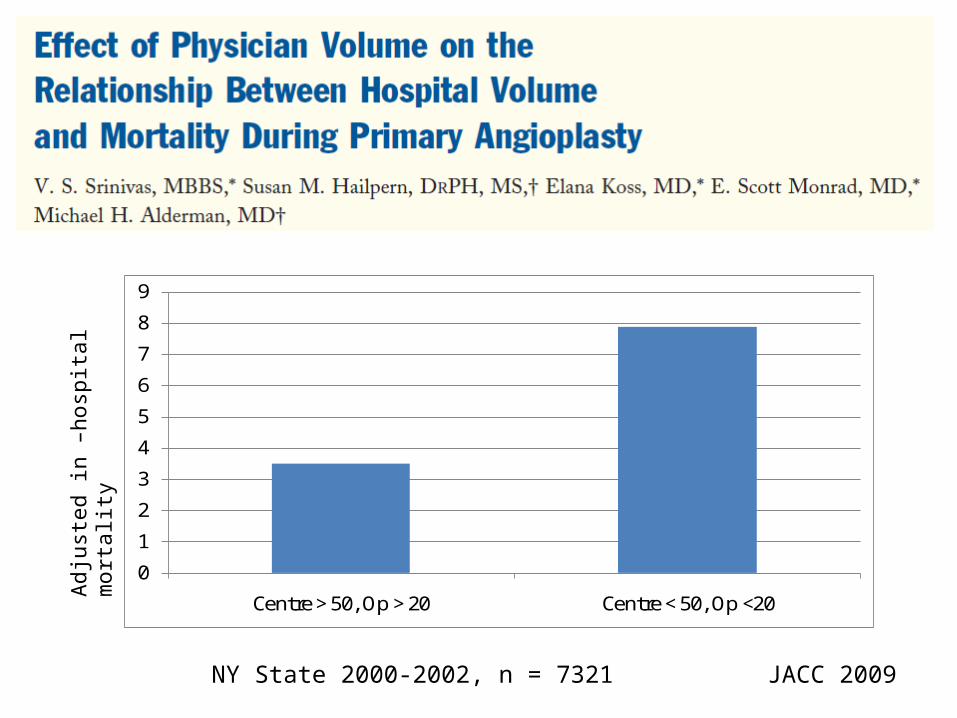
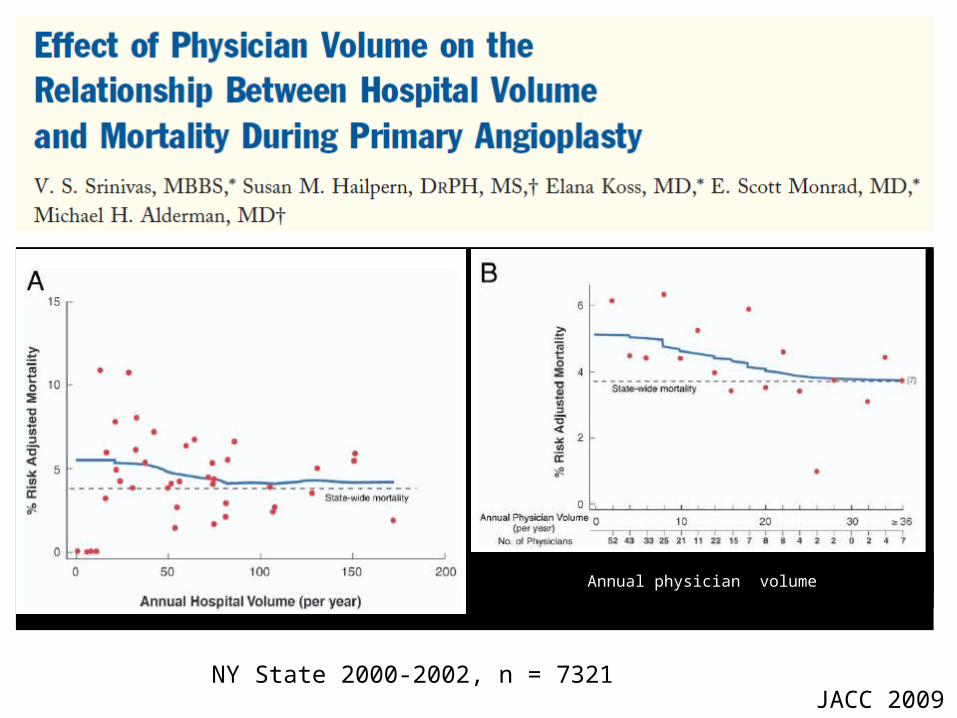
NY State 2000-2002, n = 7321 JACC 2009
0
1
2
3
4
5
6
7
8
9
Centre > 50, Op > 20 Centre < 50, Op <20
3.5% vs. 7.9%, P = 0.01
Adj
uste
d in
–ho
spita
l mor
talit
y

NY State 2000-2002, n = 7321JACC 2009
01234567
>10/yr <10 yr
High Volume Centres (>50 PPCI/yr)
3.8 vs. 6.5%, OR 0.6 (CI 0.4 – 0.9)
Adj
uste
d in
–ho
spita
l mor
talit
y
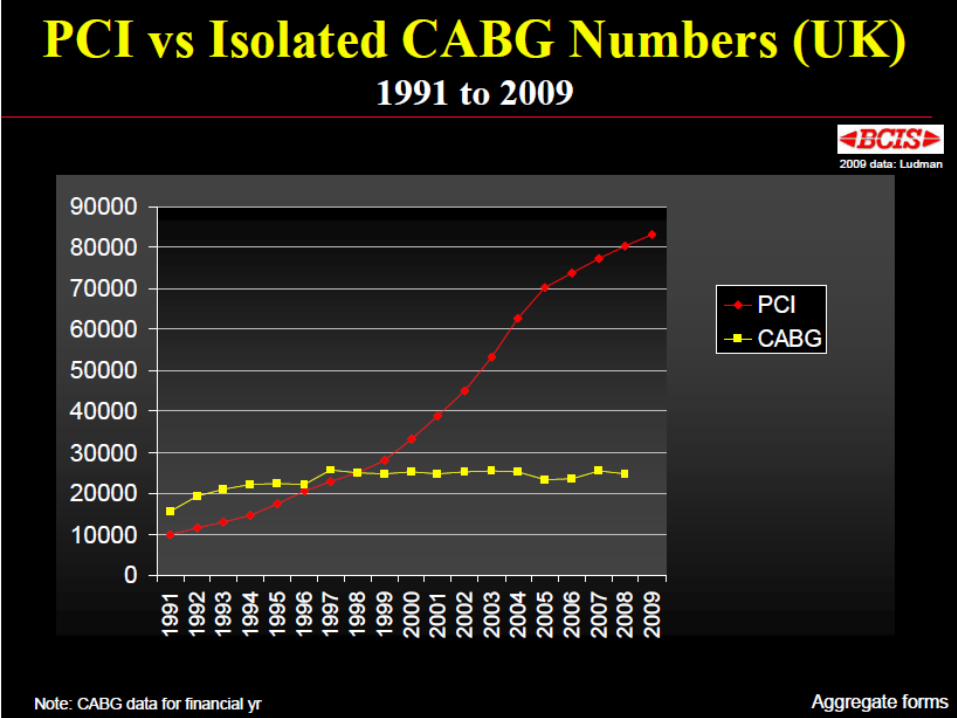
Expansion of PCI in the UK
“BCIS should show more teeth”PPCI Consensus meeting, London, September 2008
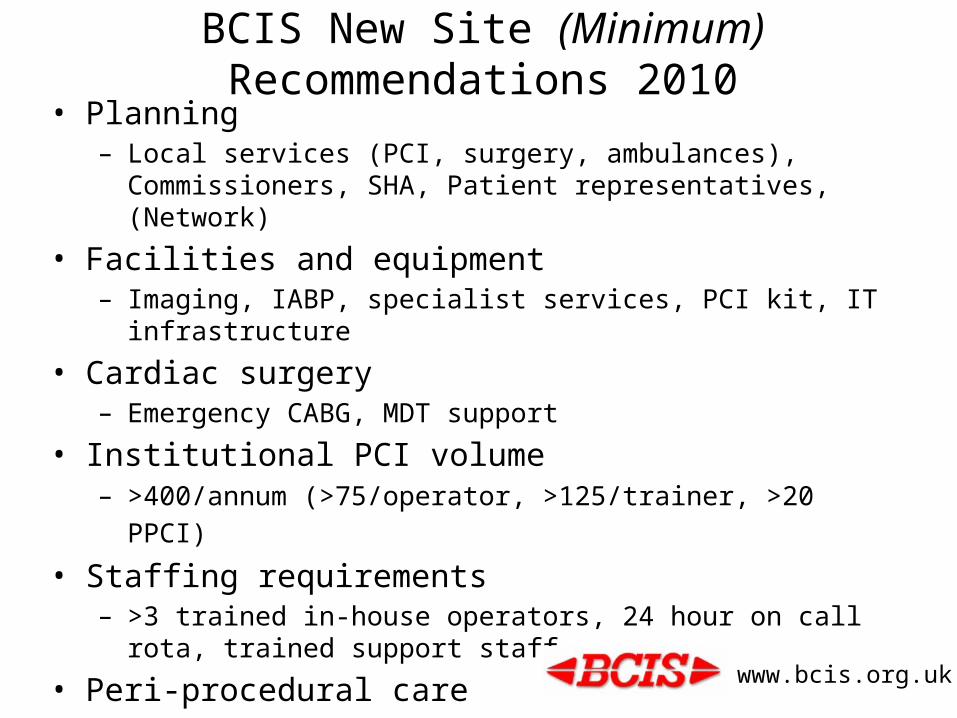
BCIS New Site (Minimum) Recommendations 2010• Planning
– Local services (PCI, surgery, ambulances), Commissioners, SHA, Patient representatives, (Network)
• Facilities and equipment– Imaging, IABP, specialist services, PCI kit, IT infrastructure
• Cardiac surgery– Emergency CABG, MDT support
• Institutional PCI volume– >400/annum (>75/operator, >125/trainer, >20 PPCI)
• Staffing requirements– >3 trained in-house operators, 24 hour on call rota, trained support staff
• Peri-procedural care• Consent• Audit
www.bcis.org.uk
The BCIS Site Visit Process 2001-2011Some Personal Observations (n=57)
• Some new centres set up with no BCIS visit• Inadequate business case/procedural numbers• Competition with neighbouring small units/surgical centre
– underused facilities & expertise
• No support from Network/surgical centre• Consultant numbers (n=2)• Ad hoc Consultant training/retraining (some not on Specialist Register) • Discontented, undertrained support staff (radiographers, nurses)• Outdated equipment (IABP/imaging)• Morning only PCI• No out of hours cover (including high volume and PPCI centres)• No progress over time – numbers/service development (impending revisits)• Treat and return – is post procedural care the same?
Conclusions• The debate concerning PCI centres is nothing to do with:
– 399 versus 401 per annum– Surgical versus non-surgical centres– Old guard versus young turks
• But is all about:– Consistent national standards– Quality care 24/7, 365 days per annum– Treatment that you would wish for your own family
• The BCIS new site guidance is as applicable to established centres as to newcomers
• Take a look – does your service measure up?


BCIS Guidance on Development of new PCI sites 2002
1. PCI activity should increase 2. The development of new PCI sites should be
planned and coordinated and not occur on an ad hoc basis
3. All PCI sites should adhere to agreed technical, professional and practical standards
4. New sites should undergo a peer review visit through BCIS prior to starting PCI activity (as requested by the National Director for Heart Disease)
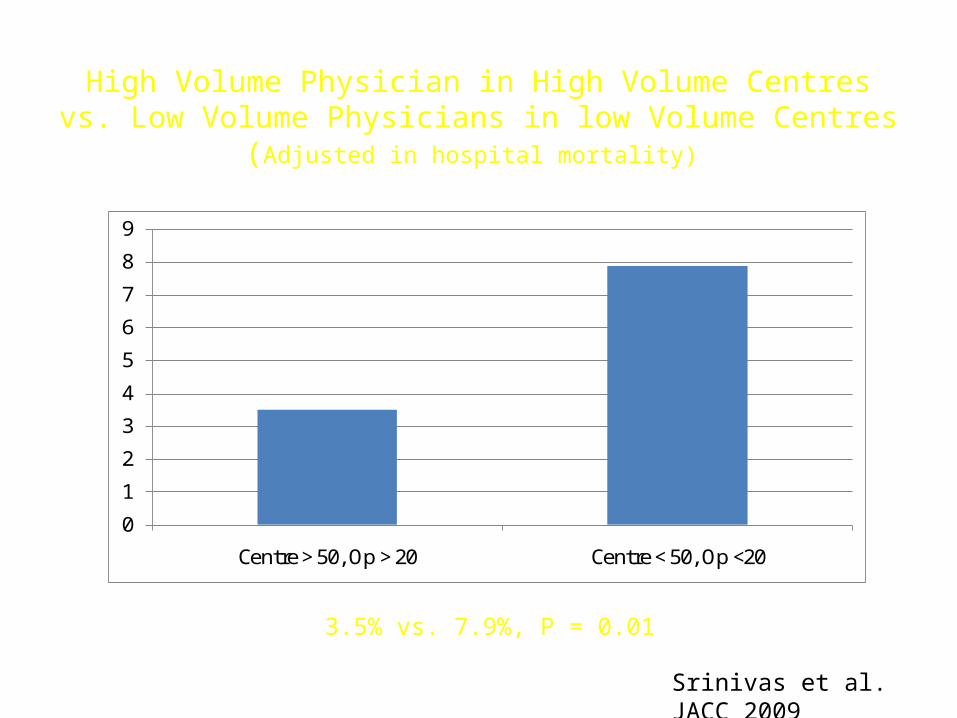
High Volume Physician in High Volume Centres vs. Low Volume Physicians in low Volume Centres
(Adjusted in hospital mortality)
0
1
2
3
4
5
6
7
8
9
Centre > 50, Op > 20 Centre < 50, Op <20
3.5% vs. 7.9%, P = 0.01
Srinivas et al. JACC 2009
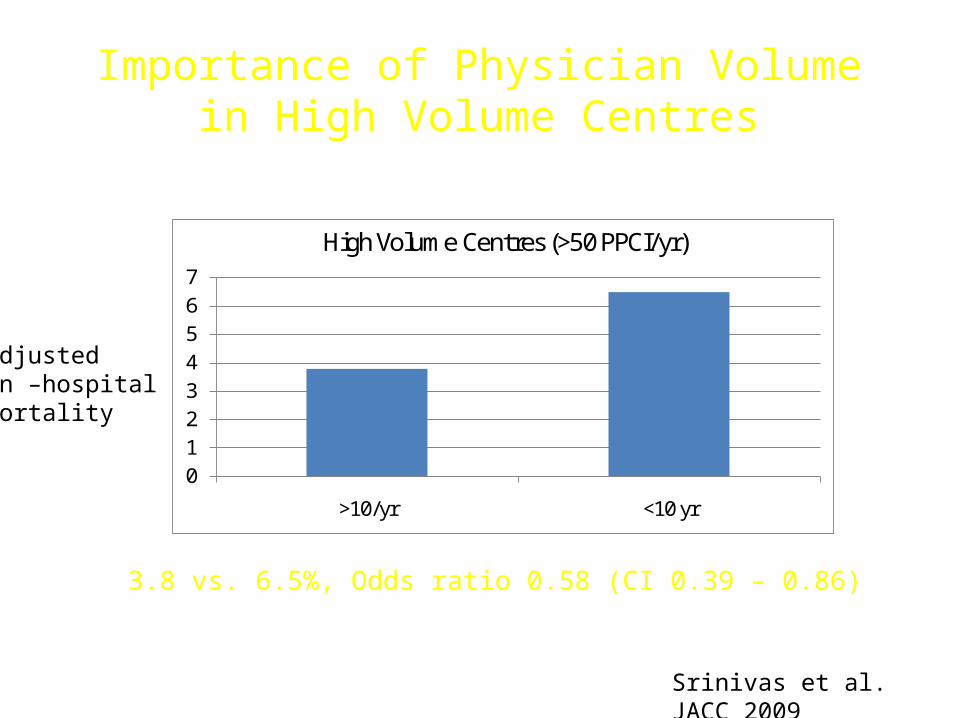
Importance of Physician Volume in High Volume Centres
01234567
>10/yr <10 yr
High Volume Centres (>50 PPCI/yr)
3.8 vs. 6.5%, Odds ratio 0.58 (CI 0.39 – 0.86)
Adjustedin –hospitalmortality
Srinivas et al. JACC 2009
Annual physician volume
NY State 2000-2002, n = 7321JACC 2009
AHA Guidelines:PPCI Operator and Centre Volumes
Elective PCI should be performed by operators with acceptable annual volume (at least 75 procedures) at high-volume centers (more than 400 procedures).
Primary PCI for STEMI should be performed by experienced operators who perform more than 75 elective PCI procedures per year and, ideally, at least 11 PCI procedures for STEMI per year. Ideally, these procedures should be performed in institutions thatperform more than 400 elective PCIs per year and more than 36 primary PCI procedures for STEMI per year.
♥ The relationship between procedural volume and outcome in contemporary PCI practice is controversial..........The available evidence suggests that the volume-outcome relationship is stronger for patients at higher risk of adverse outcomes, including patients with non-ST and ST-elevation acute coronary syndromes.
♥ Services carrying out at least 50 primary PCI procedures per annum (and operators doing at least 20 primary PCI procedures per annum) have lower in-hospital mortality than services (and operators) carrying out fewer primary PCI procedures. Moreover, high total institutional PCI volume (more than 400 PCI cases per annum) has been associated with short door to balloon times and lower hospital mortality for patients undergoing primary PCI.
♥ It is not possible to make definitive statements about optimal institutional or operator primary PCI volume. Nevertheless, primary PCI services are unlikely to be sustainable with fewer than five operators, and to optimise outcomes it is therefore recommended that PCI services doing primary PCI should carry out a minimum of 100 such procedures per annum.
♥ In the United Kingdom there are approximately 500 reperfusion-eligible myocardial infarction patients per million population per annum. To achieve the minimum recommended number of primary PCI procedures per annum, a PCI centre would need to serve a population of at least 200 000 if the service is available 24/7, and a population of at least 500 000 if the service is available only during normal working hours (for example Monday to Friday, 9am to 5pm).
New Site Guidance 2009Awaiting website release

BCIS Peer Review - Outcome
2002-2008 37 30 ‘approved’ 7 ‘concerns expressed’
1 closed because low
volume
2008-2010 20 7 ‘compliant’ 8 ‘not fully compliant’5 reports in
progress
1 abandoned

















