72
What Works? in dementia training and education: study findings

What Works? in dementia training and education: study
findings

Background
Health Education England, Skills for Health and Skills for Care: Dementia Core Skill Education and Training Framework
Tier 1 – dementia awareTier 2 – those working regularly, directly with people with dementiaTier 3 – clinical leaders
How do we know what approaches to education and training are effective?

What we did
Three inter-related work packages
WP1: Literature review of research about dementia education and training across all health and social care settingsWP2: National audit of dementia training and survey of staff who have taken dementia trainingWP3: In-depth case studies in up to 12 sites who show signs of good training practice spanning health and social care settings

The study team
Framework for analysis
Kirkpatrick’s 4 levels
1. Reaction – learners’ reaction to and satisfaction with, the programme; 2. Learning - the extent to which this has occurred including staff knowledge and attitudes; 3. Behaviour – extent to which behaviour has changed as a result of the programme; 4. Results – impact of training on outcomes for people with dementia, their families and staff

Work Package 1: summary of findings
Research question
What does existing research evidence indicate are the most effective approaches to the delivery of education and training that can be applied to the dementia care workforce? (Literature review)
Summary
152 papers included in the reviewTraining most likely to be effective:• Includes face-to-face delivery using group-based activities and
discussion• Is tailored to the staff attending so it is relevant to their role
and service setting• Is delivered by an experienced facilitator• Combines theory/knowledge with opportunities to apply
learning through practice/practice-based activities• Is of at least 3 hours duration with longer programmes more
likely to be effective

Work Package 2

WP , Survey 1- Aims & Methods
Survey 1
• How many organisations are providing tier 1-3 education
• What type at what tier?
• How designed and delivered?
• What does it cost?
Online survey distributed nationally using databases of health and social care providers, training providers and training commissioners, opportunities sample via social media.

Dementia Core Skills Education and Training Framework

Survey 1 Design
Questions:
• the number of training packages provided
• the subject(s) and learning outcomes of the training or education (Dementia Core Skills Education and Training Framework)
• design, delivery, target audience, length, level, content, format, numbers of staff trained and frequency of delivery.

Provider Type Organisation Type Number Respondents
Number of Packages
Care Provider Acute Care 60 117
Charitable Care 25 53
Community or Mental health Trust
3862
Domiciliary care 6 9
Primary Care 37 29
Residential Care 47 100
Other Care Provider 24 38
TOTAL CARE PROVIDER 237 408Training Provider Private Training Company 18 52
University 65 117
Charitable Organisation 23 44
Other Training Provider 28 55TOTAL TRAINING PROVIDER
134268
Commissioning Group/Network COMMISIONERS TOTAL 49 42
TOTAL 420 718
Overview of Respondents
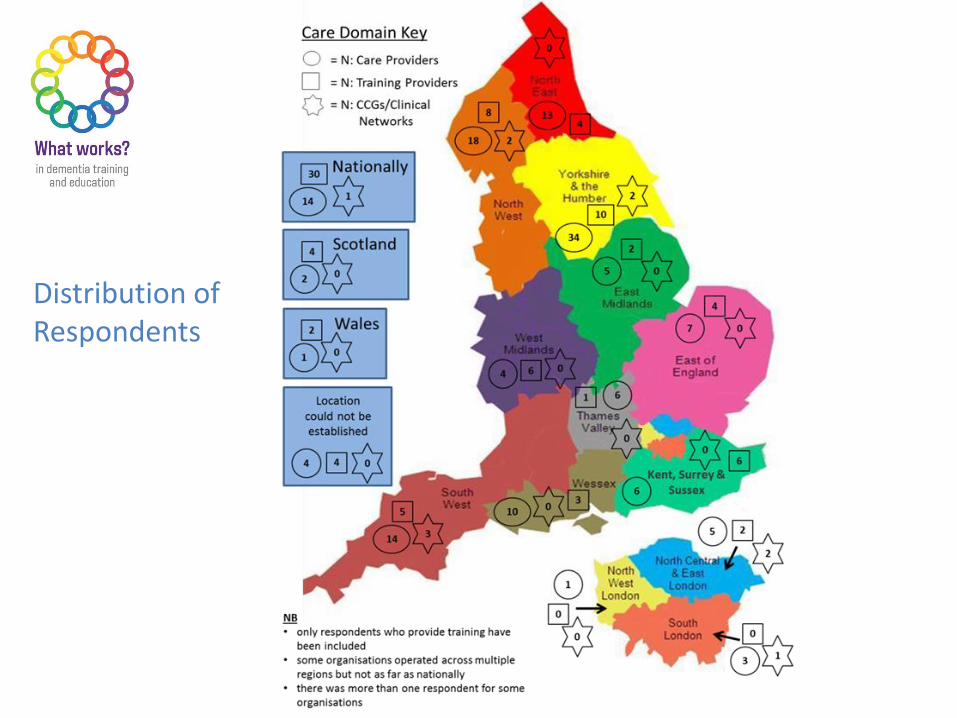
Distribution of Respondents

Subjects and Learning Outcomes
Using the Dementia Core Skills Framework:
• Of 718 training packages reported, 387 of the packages reported did not meet any of the learning outcomes identified in Framework
• 127 packages reported covering some of the subject areas identified in the Framework, but did not report learning outcomes for at least one reported subject areas
• 204 packages met at least 1 learning outcome for a reported subject area

Subject
LOs (N)
Av. LOs
per
Package
(N)
Av. LOs
per
Package
(%)
Communication, Interaction & Behaviour in Dementia Care 18 14.4 80
Person Centred Dementia Care 11 8.34 76
Awareness Training 11 8.03 73
Living Well with Dementia & Promoting Independence 17 9.04 53
Health & Wellbeing in Dementia Care 18 8.79 49
Families and Carers as Partners in Dementia Care 18 8.9 49
Equality Diversity & Inclusion in Dementia Care 13 5.26 40
Law, Ethics & Safeguarding in Dementia Care 16 5.44 34
Dementia Identification, Assessment & Diagnosis 19 6.29 33
Leadership in Transforming Dementia Care 10 3.08 31
Dementia Risk Reduction & Prevention 10 2.9 29
End of Life Dementia Care 11 2.5 23
Research & Evidence Based Practice in Dementia Care 9 1.63 18
Total Across All Subjects195 86.91 45

Tiers covered (n=204 packages)
0
10
20
30
40
50
60
70
80
90
100
Tier 1 Tier 2 Tier 3
% LOs covered

Subject Subject covered LOs covered Agreement
Dementia Identification, Assessment & Diagnosis 187 195 8
Awareness Training 298 300 2
Dementia Risk Reduction & Prevention 172 172 0
Leadership in Transforming Dementia Care 110 109 -1
Pharmacological Interventions in Dementia Care 108 103 -5
Health & Wellbeing in Dementia Care 257 238 -19
Law, Ethics & Safeguarding in Dementia Care 159 140 -19
End of Life Dementia Care 132 108 -24
Person Centred Dementia Care 314 289 -25
Families and Carers as Partners in Dementia Care 253 227 -26
Communication, Interaction & Behaviour in Dementia Care
305 285 -30
Equality Diversity & Inclusion in Dementia Care 230 197 -33Living Well with Dementia & Promoting Independence
284 249 -35
Research & Evidence Based Practice in Dementia Care
169 96 -73
Agreement between reported subjects and reported learning outcomes

Mode of Delivery
• Of 718 training packages 369 included mode of delivery - some multiple modes of delivery
• Small group face to face common in University, Acute Care , Residential Care and Private Training Organisations
• E-learning common in Universities and Acute Care
• Acute Care, Universities and Charitable Organisations more likely to use 2+ modes of delivery

Survey 1 - Summary
• Most respondents from care provider organisations - acute care and residential care sectors.
• Most training packages offered by Acute Care and Universities (n=117 each)
• Two thirds of delivery modes used involved face to face teaching
• Variation extent to which the training packages align to the Framework
• Training packages cover 75% of Tier One learning outcomes- more met in the Person Centred Dementia Care and Communication, Interaction & Behaviour in Dementia Care.
• Packages are weaker in covering the learning outcomes associated with Tier three training
• Disagreement between LOs defined by framework and reported packages most pronounced in research and evidence based practice

Work Package 2: Survey 2

What are the most effective education and training approaches for fostering positive attitudes, high levels of
knowledge and self efficacy in health and social care staff?
What are the perceived barriers and facilitators to implement learning?
Aims and objectives

National Survey of Health and Social Care Staff
• Sent survey to 183 organisations who had completed survey 1
• Survey contained questions about:
• Reaction to training• Knowledge tests• Attitudes• Self efficacy
Method

We received feedback for 60 different training packages
553 staff completed the survey for the 18 training packages we included:
DELIVERY MODE14 were delivered face to face in small groups2 packages had e learning components3 training courses were delivered in large face to face to groups3 courses had a mentorship component
Results

• Training packages covered a range of dementia topics• The only topic not to be covered was ‘Pharmacological Interventions in
Dementia Care’
Results

Demographics

Demographics

Demographics
27
42
45
55
60
89
102
87
2915 2
18-24 years
25-29 years
30-34 years
35-39 years
40-44 years
45-49 years
50-54 years
55-59 years
60-64 years
65 plus years
prefer not to say
Most people
were aged 50 years
and above

Demographics
39
108
194
26
65
121Ancillary or clerical
Unqualified clinical orcare staff
Qualified clinical orcare staff
Unit or facilitymanager
Service manager seniormanagement
Other
Most people were
qualified clinical
care staff

Demographics
1545
50
94
141
197
11
less than 1 year
1-2 years
3-4 years
5-9 years
10-19 years
20 plus years
Unknown
Most people had been in their
role for over 10 years
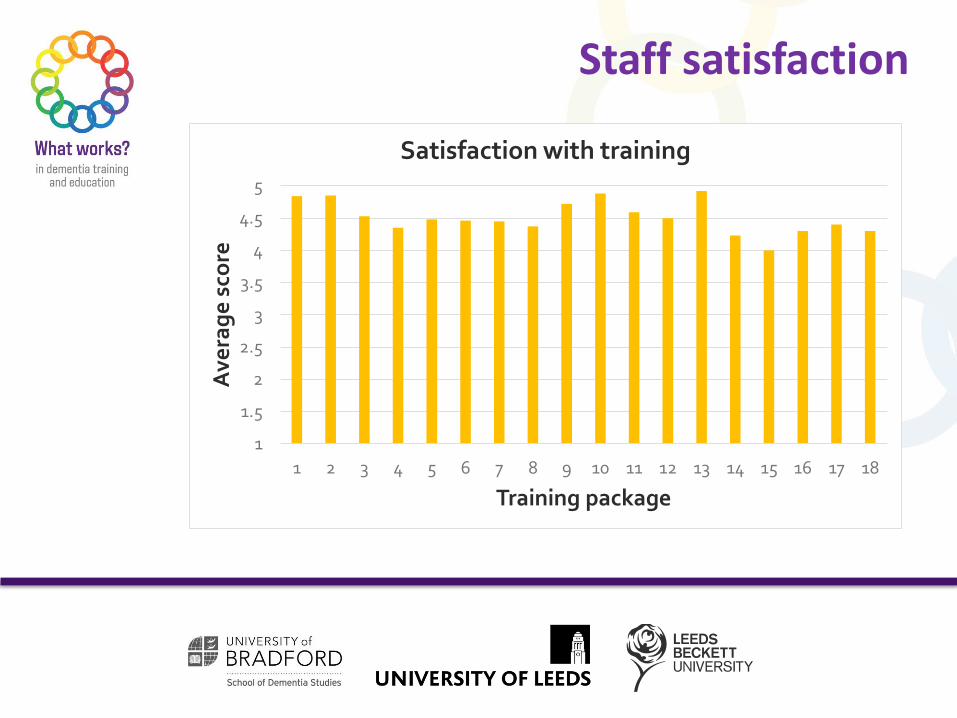
Staff satisfaction
1
1.5
2
2.5
3
3.5
4
4.5
5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Ave
rag
e s
core
Training package
Satisfaction with training

Staff Understanding
1
1.5
2
2.5
3
3.5
4
4.5
5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Ave
rag
e s
core
s
Training package
Understanding of information

Relevance of training
1
1.5
2
2.5
3
3.5
4
4.5
5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Ave
rag
e s
core
Training package
Relevance of training

Likelihood of recommending training?
1
1.5
2
2.5
3
3.5
4
4.5
5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Ave
rag
e s
core
Training package
Recommendation of training

Staff Knowledge
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Ave
rag
e s
core
Training package
Average knowledge score
• Training package 1, 2, 4, 5, 7, 12, 15, 17 & 18

Staff attitude: knowledge
0
10
20
30
40
50
60
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Ave
rag
e s
core
Training package
Average attitude: knowledge score
• Training package 1, 2, 3, 4, 5, 6, 8, 9, 10, 12, 13, 14, 15, 17 and 18

Staff attitude: comfort
0
10
20
30
40
50
60
70
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Ave
rag
e s
core
Training package
Average attitude: comfort score

Self efficacy
0
5
10
15
20
25
30
35
40
45
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Ave
rag
e s
core
Training package
Average self-efficacy score
Training package 1, 4, 10, 13, 18
To summarise
• 18 training packages were completed between the 553 health care staff. • Training was delivered mainly in small groups• Staff in general were very positive about training. • Specific training packages not associated with greater staff comfort levels,
BUT greater number of courses attended was positively associated with higher levels of comfort.
• This suggests building of expertise via training is important in enabling staff to feel more comfortable when providing care to people living with dementia.

To summarise
• Training packages 1, 4 and 18 were found to have a significant positive impact on staff knowledge and confidence.
• These training packages covered fewer subjects in comparison to others. • All three were delivered in small face to face groups. • Training package 4 had an additional e-learning component and training
package 18 also involved mentorship for staff. • This suggests that focusing on fewer subjects and delivering via face to face
small group work, enables training to have a more significant impact on staff knowledge and self-confidence.
• Lack of contact with people living with dementia• Lack of time to reflect on learning and also to put into practice• Lack of resources such as financial, staff shortages and trained staff• Not having protected time to plan how to implement learning• Changes in the team with new staff joining and trained staff leaving• The attitude and unwillingness of other colleagues• Having a heavy workload• Operational systems within the NHS (for example bed shortages and the need to move people with dementia regularly led to poor care being delivered)
Staff barriers to implementing their
training

• Supportive colleagues• High level managerial support• Working in an already dementia friendly environment• Respondents being personally motivated to create change• Regular opportunities to engage with people living with dementia• Opportunities to practice learning and refresh learning• Self-confidence and enthusiasm.
Facilitators

• The survey had a very low response rate • Many had completed training which was not included in the evaluation
and this may have had an impact. • It was not possible to control for all possible factors due to a small sample
size and a large number of factors we needed to consider.• The main limitation of the evaluation is we were unable to obtain pre and
post measures and therefore it is not possible to determine whether respondent’s scores were due to their training.
• The results are not generalisable due to respondents being mainly older white British female clinical staff.
Methodological limitations

Expert by experience group involvement

Who we are
• Group of people living with dementia and current and former carers
• During the lifetime of the project 23 people contributed in some way
• We have a wide range of experience and expertise including but also wider than dementia
• One member (Alison Dennison) was a co-applicant on the study
• Two members were part of the project’s independent advisory group
What we did
• We met at 2-3 month intervals - 15 times - during the study
• We inputted into how the study was delivered• We turned our experiences of good and poor care into
practice scenarios for use in the case study focus groups• We suggested these were also presented as storyboards• As part of the case study analysis we read some of the
focus group transcripts and suggested findings
Scenario 1: Day, residential or intermediate care
It is 11 am and Christine and Ella, two women living with dementia, are sitting next to each other in the dayroom. No-one else is sitting nearby. For most of the following hour Ella is lifting the fabric of her skirt and looking at it in a puzzled way, while Christine seems to be having a conversation with someone who isn’t actually there. At times Christine replies to herself in a different, deeper tone of voice, and she often mentions someone called Bob. She talks mainly about a time when she was injured and had to have stitches in her leg. Her hearing aid is in upside down. Ella doesn’t talk much, but every now and then she will try to start a conversation with Christine by asking a polite question, such as ‘When did that happen?’ Whenever Ella does this Christine’s face takes on an angry expression and she replies in a harsh voice. Ella looks as though she is about to cry. A passing member of staff says, ‘Play nicely, girls.’ Ella says that she wants to go home, and that everything was better back home, when she used to help out at the mission. At 12 o’clock another member of staff tells Christine and Ella that they can have either shepherd’s pie or fish and chips for lunch. ‘You don’t like fish’, the staff member tells Ella. Ella replies ‘I like saltfish. I just don’t like your white fish.’ • What problems can you identify here relating to each of the people involved? • What suggestions do you have for things you might try to improve the situation
for Christine and Ella?

Storyboard – a picture is worth a thousand words
Artwork by Kate Clark

Data analysis
• Themes we identified in the focus group transcripts as barriers to training
• Lack of time for training
• Lack of resources for training
• Lack of management support
• Challenges in putting training into practice

Key insights and contributions
• We moved to a more informal setting in someone’s house for our meetings
• We brought high levels of personal insights
• We will use our connections to disseminate to a wide range of groups, e.g. Memory Tree
• We have felt pleased to ‘give something back’

Work Package 3

Aim of the case studies
• To derive models of good practice regarding the design and implementation of dementia education and training
• To make recommendations for establishing the right setting conditions for dementia education and training

How?
Through in-depth case studies of organisations, paying attention to:
• Four levels of impact (Reaction; Learning; Behaviour in practice; Quality of care experience)
• Context and culture of the organisation• Design and facilitation of the training• What blocks positive impact?• What helps positive impact?

Where?
10 sites:
• 1 Primary Care organisation• 3 Mental Health Trusts• 3 Acute Hospital Trusts• 3 Care Home groups

Why those sites?
• Responded to survey 1• Training covered a high proportion of
learning outcomes from the Framework• Training met quality criteria derived from
the literature review

At each site, we involved:• Training leads• Trainers/facilitators• Unit/home/ward managers• Staff who had been trained• People receiving care• Family or friends
Who was involved?

What did we do at each site?
• Interviews• Focus groups including scenario discussions• Questionnaires• Analysis of training materials• Observation of training • Observation of care• Satisfaction cards with people living with dementia, family,
friends• Brief interviews with people living with dementia, family,
friends
Analysis by source
Analysis by site
Integration across settings
Integration across all sites
Description then...
…. then drew out recommendations for good practice
How did we analyse our findings?

Overall findings - reaction
Positive reaction when:• Content was relevant to staff roles, and materials were accessible
and clear• Delivery was interactive, e.g. discussions, learning activities,
videos, scenarios- not didactic• Learning was face-to-face in small groups – not self-directed• Simulation was accompanied by theory, and support and
debriefing was offered
Just hearing first-hand accounts from people can be quite profound, quite poignant. I think it invites a degree of empathy, which is more difficult if you are sitting and staring at a screen (Staff member, Acute Trust-048)
I find personally I understand
things better when it’s in a training
setting, there is a group of you,
when you know, giving ideas and
all talking together about it rather
than a question on a page (Staff
member, Care Home site -042)

Overall findings - learningIn all settings:
• Staff gained knowledge of what it is like to live with dementia • Staff gained understanding of the person-centred perspective• Staff attitudes became more empathic
In social care and acute care:• Some gained skills/practical ideas (e.g. how to provide aids/ activities)
In mental health trusts:• Experienced staff gained valuable reflection and refreshment time
BUT• Inconsistent evidence of positive attitudes, knowledge & understanding
of dementia among staff during DCM observations and focus groups
It kind of brought it to your mind and it was –
you retained that knowledge and you
understand it. So for me to go back into
procurement and into finance – having done
that simulation training I could relate to a
patient with dementia” (staff member, Acute
Trust-044).
It made me re-evaluate the way I look at people who have dementia… when people come into hospital it is pre-packaged, somebody in an awful situation that is presenting with behaviour that is probably very unlike them…” (Manager, MHT-029)

Overall findings – behaviour change
• Key area – improved communication• Taking time to understand• Responding with greater patience• Trying to find positive solutions
• Also more activity and individualised care• Some felt behaviour change from training alone was
difficult to achieve and this requires additional support from leaders
They are no longer focussed on, they
have to do this for this time, and the
individual gets lost. So I think we’re
breaking that down … everybody is not
sitting at a dining table at eight in the
morning. (Training Lead, Care home-
040)
It has to come from the top. You can have
the best carers in the world, but it makes
no difference if the people at the top don’t
want to actually give people time to learn,
to give people the resources that they need
to learn. (Dementia Lead, Care Home-042)

Overall findings – behaviour change using Dementia Care Mapping
• Mapping took place in 9 out of 10 sites• Care varied between staff, across units and across
sites– it was not universally of high quality• For example, some staff were skilled at creating a
positive atmosphere and using each interaction as an opportunity to engage participants, but not all staff showed this level of skill

Overall findings – behaviour change using Dementia Care Mapping
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
Quality of staff interactions (average per mapping hour)
Highly Detracting Detracting Enhancing Highly Enhancing
Overall findings – outcomes for people living with dementia
• Increased well-being resulting from more person-centred care• Better satisfaction among relatives as a result of better
communication• In some cases, increased staff knowledge and confidence led
to specific practice changes• Aside from training, other changes may have contributed (i.e.
improvements to environment)
They help in a quiet way without
making a fuss about the fact I can’t
walk very well. (Person with
dementia, care home-040)
Although staff are really good.
There’s not enough staff working
on the ward and they are so busy
with other things. More volunteers
on the ward would help. (Relative,
Acute Trust-044)
Staff have been excellent
and care couldn’t be better
(Person with dementia,
MHT-068)

Barriers to training
• Lack of resources (time, staff, funding)• Adjusting to learning was hard for some staff for various
reasons• Reliance on written word and self-directed learning was
off-putting to many learners• Being unable to include agency staff• Care environment may not be suitable when putting
some aspects of training into practice

Facilitators to training• Skilled training delivery by staff with both clinical and
training experience• Creative, memorable delivery methods such as
interactive learning• Learning in small groups with opportunities for peer
support• Motivated staff – topics should be relevant and framed
at an appropriate level• Commitment from the top of the organisation, and an
organisation-wide culture of person-centred care• A whole systems approach connecting trainers, learners
and managers - Joint work between managers and trainers is essential

Models of good practice
Each context is different. Dementia care vision, and training strategies, need to consider the specific barriers to be overcome and the facilitators to be built upon (context, culture, design, delivery and implementation) to achieve positive change.
Nonetheless we have been able to identify key ingredients to produce effective training at:
• Organisation level• Training design and delivery level• Implementation level
Details can be found in our full report.
Summary
• Through training, staff can gain a combination of knowledge and attitude leading to person-centred understanding of dementia
• It was not always clear whether and which behaviours had been affected by training, though we heard strong and convincing accounts of changes in practice linked to training and education.
• The key area of behaviour influenced by dementia education and training was improved communication.
• There was striking variation between staff, across units and across organisations in quality of care – some excellent but also some poor practice
• From the case studies we have produced evidence-based models of good practice for effective dementia training and education.

Dissemination of study findings

Published outputs

Training audit tool and learning outcomes mapping document

The report is based on independent research commissioned and funded by the NIHR Policy Research Programme(Understanding Effective Dementia Workforce Education and Training: A Formative Evaluation (DeWET Evaluation), PR-R10-0514-12006). The views expressed in the publication are those of the author(s) and not necessarily those of the NHS, the NIHR, the Department of Health, ‘arms’ length bodies or other government departments.
Web-site address &Funding acknowledgement
www.leedsbeckett.ac.uk/whatworks

















