86
What’s new in Clinical Practice Guidelines (CPG) in Critical Care Kuwait, April 11, 2013
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | alexia-mckenzie |
| View: | 214 times |
| Download: | 0 times |

What’s new in Clinical Practice Guidelines (CPG) in Critical Care
Kuwait, April 11, 2013

What is new in CPG in Critical CarePast, Present, Future
1.Process of CPG development (GRADE)
2.Examples of new and / or controversial recommendations
3.Future tasks
4.Allow you to use those guidelines with more satisfaction

New developments in communism
The evolution of power in medicine
• Clinical Experience and pathophysiological knowledge
• RCTs
• Meta-analyses, decision analyses, economic analyses
• Above with recommendation Practice guidelines
In the beginning...
• Early 2000– CPG increasing in importance– Chaos all over the place, especially for
‘generalists’– Need to create order out of chaos


• Step one – What is the question?
• Step two – Find and summarize best evidence
• Step three – Apply judgments (quality of evidence, strength
of recommendations)
Grad
eGRADE: Guideline development process
GRADE defining feature
• Evidence: high or low quality?• quality of evidence: the likelihood that our
estimates of effects are true and adequate to support given recommendation
• Recommendation: weak or strong?• confidence that following the
recommendation will cause more good than harm

strong recommendationsstrong methodsANDbenefits clearly outweigh downsides
weak recommendationsweak methodsORbalance of benefits and downsides unclear
or close
Reco
mm
en
datio
nRecommendations: Weak or strong?

recommendation
Outcome1
Outcome2
Outcome3
Outcome4
Formulate question
Rateimportanceof outcomes
Critical
Important
Critical
Not important
Evidence Profile (GRADEpro)
Pooled estimate of effect for each outcome
Rate overall quality of evidence across outcomes
high low
1. risk of bias2. inconsistency3. indirectness4. imprecision5. publication bias
1. large effect2. dose-response3. antagonistic bias
Quality of evidence for each outcome
Select outcomes
High Moderate Low Very low
Formulate recommendations For or against an action Strong or weak (strength)
Strong or weak: Quality of evidence Balance benefits/downsides Values and preferences Resource use (cost)
Wording “We recommend…” | “Clinicians should…” “We suggest…” | “Clinicians might…”
Systematic Review(outcomes across studies)
action
PICOrate down
RCT observational
rate
up
12
start
High | Moderate | Low | Very low
Guideline panel
unambiguous clear implications for action transparent (values & preferences statement)
systematic review of evidence


Strength of recommendation
degree of confidence that desirable effects of adhering to recommendation outweigh the undesirable effects.
Desirable effects•health benefits•less burden•savings
Undesirable effects•harms•more burden•costs

Strong or Weak Recommendation?
• Quality of the evidence
• Balance between desirable and undesirable effects
• Values and preferences
• Costs (resource allocation, feasibility)

Strenght of Recommendations
• strong recommendation• authors confident that following the
recommendation will cause more good than harm
• weak recommendation (suggestion)• authors believe that following the
recommendation will cause more good than harm, but are less confident

Why Grade Recommendations? Implications
• strong recommendation–one size fits all–expect uniform clinician behavior–use as performance indicator
• weaker recommendation –expect action to vary

Strenght of Recommendations
• do it or don’t do it–strong recommendation
• probably do it, or probably don’t–weaker recommendation

How to present grades?
• words only– recommendations versus suggestions– quality high, moderate, low, very low
• numbers and letters– recommendation 1 and 2– quality A, B, C, D


GRADE pragmatic approach
• If question appropriate, look for meta-analysis (MA)
• If no published MA, identify main studies• If possible, do your own MA• If no MA, describe main studies and their
results• Be explicit about the way you identified and
summarized the evidence• Make sure there is explicit link between
recommendation and evidence

Surviving Sepsis Campaign
• New or controversial recommendations
• 68 international authors• 30 international organizations• 19 reviewers• Attention to COI• GRADE system• Emphasis on meta-analyses (636
references)– If you can't dazzle them with brilliance,
baffle them with bs

recommendation
Outcome1
Outcome2
Outcome3
Outcome4
Formulate question
Rateimportanceof outcomes
Critical
Important
Critical
Not important
Evidence Profile (GRADEpro)
Pooled estimate of effect for each outcome
Rate overall quality of evidence across outcomes
high low
1. risk of bias2. inconsistency3. indirectness4. imprecision5. publication bias
1. large effect2. dose-response3. antagonistic bias
Quality of evidence for each outcome
Select outcomes
High Moderate Low Very low
Formulate recommendations For or against an action Strong or weak (strength)
Strong or weak: Quality of evidence Balance benefits/downsides Values and preferences Resource use (cost)
Wording “We recommend…” | “Clinicians should…” “We suggest…” | “Clinicians might…”
Systematic Review(outcomes across studies)
action
PICOrate down
RCT observational
rate
up
12
start
High | Moderate | Low | Very low
Guideline panel
unambiguous clear implications for action transparent (values & preferences statement)
systematic review of evidence

Importance of team work!

Controversies and changes – team work
• Sepsis management requires a multidisciplinary team (physicians, nurses, pharmacy, respiratory, dieticians, and administration) and multispecialty collaboration (medicine, surgery, and emergency medicine) to maximize the chance for success.

Calibrating the level of your enthusiasm
• There will be one week of extra paid vacation for all attending this conference
• Kuwait and UAE meet in the opening match of the World Cup in Qatar 2022
• New personal income tax is introduced to pay the football team players for winning more games
Controversies and changes (plus some gossiping)
• The administration of effective intravenous antimicrobials within the first hour of recognition of septic shock (grade 1B) and severe sepsis without septic shock (grade 1C) should be the goal of therapy.
• Remark: Although the weight of the evidence supports prompt administration of antibiotics following the recognition of severe sepsis and septic shock, the feasibility with which clinicians may achieve this ideal state has not been scientifically evaluated.

Controversies and changes (plus some gossiping)
• The administration of effective intravenous antimicrobials within the first hour of recognition of septic shock (grade 1B) and severe sepsis without septic shock (grade 1C) should be the goal of therapy.
• Remark: Although the weight of the evidence supports prompt administration of antibiotics following the recognition of severe sepsis and septic shock, the feasibility with which clinicians may achieve this ideal state has not been scientifically evaluated.

survivingpatients
[%]
time from onset of hypotension [hours]

Importance of team work!

Controversies and changes (plus some gossiping)
• The administration of effective intravenous antimicrobials within the first hour of recognition of septic shock (grade 1B) and severe sepsis without septic shock (grade 1C) should be the goal of therapy.
• Remark: Although the weight of the evidence supports prompt administration of antibiotics following the recognition of severe sepsis and septic shock, the feasibility with which clinicians may achieve this ideal state has not been scientifically evaluated.

Controversies and changes – protocolized care
• EGDT (targets BP, CVP, UO, Scvo2) with the use of fluids, pressors, transfusion, dobutamine (1C)
– CVP too low (high PEEP)– one protocol versus another– Transfusion and dobutamine

Another protocol

JAMA Feb 24, 2010 (Jan 2007-Jan 2009)
17% mortality 23% mortality

Controversies and changes – new protocol
• We suggest targeting resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion (grade 2C)
• Text: If Scvo2 is not available, lactate normalization may be a feasible option in the patient with severe sepsis-induced tissue hypoperfusion. Scvo2 and lactate normalization may also be used as a combined endpoint when both are available.
Controversies and changes – new diagnostic possibilities (plus gossiping)
• We suggest the use of low procalcitonin levels or similar biomarkers to assist the clinician in the discontinuation of empiric antibiotics in patients who appeared septic, but have no subsequent evidence of infection (grade 2C).


Vasopressors and inotrops – positive thinking

Controversies and changes - vasopressors
• We recommend norepinephrine as the first-choice vasopressor (grade 1B).
• We suggest epinephrine (added to and potentially substituted for norepinephrine) when an additional agent is needed to maintain adequate blood pressure (grade 2B).
• We suggest dopamine as an alternative vasopressor agent to norepinephrine only in highly selected patients (eg, patients with low risk of tachyarrhythmias and absolute or relative bradycardia) (grade 2C).
• A trial of dobutamine infusion up to 20 mcg/kg/min be administered or added to vasopressor (if in use) in the presence of (a) myocardial dysfunction as suggested by elevated cardiac filling pressures and low cardiac output, or (b) ongoing signs of hypoperfusion, despite achieving adequate intravascular volume and adequate MAP (grade 1C)

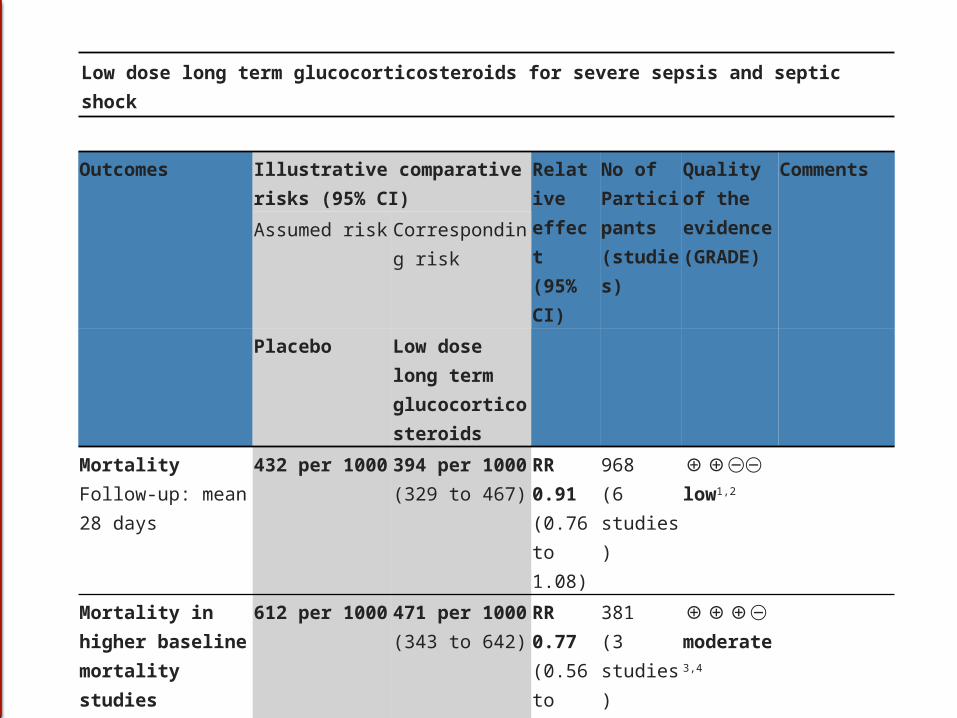
Low dose long term glucocorticosteroids for severe sepsis and septic shock
Outcomes Illustrative comparative risks (95% CI)
Relative effect(95% CI)
No of Participants(studies)
Quality of the evidence(GRADE)
Comments
Assumed risk Corresponding risk
Placebo Low dose long term glucocorticosteroids
MortalityFollow-up: mean 28 days
432 per 1000 394 per 1000(329 to 467)
RR 0.91 (0.76 to 1.08)
968(6 studies)
⊕⊕⊝⊝low1,2
Mortality in higher baseline mortality studiesFollow-up: mean 28 days
612 per 1000 471 per 1000(343 to 642)
RR 0.77 (0.56 to 1.05)
381(3 studies)
⊕⊕⊕⊝moderate3,
4
Mortality in lower baseline mortality studies Follow-up: mean 28 days
317 per 1000 336 per 1000(270 to 425)
RR 1.06 (0.85 to 1.34)
587(3 studies)
⊕⊕⊕⊝moderate5
Controversies and changes
2008: We suggest that intravenous hydrocortisone be given only to adult septic shock patients after it has been confirmed that their blood pressure is poorly responsive to fluid resuscitation and vasopressor therapy (grade 2C)
2012: We suggest not using intravenous hydrocortisone as a treatment of adult septic shock patients if adequate fluid resuscitation and vasopressor therapy are able to restore hemodynamic stability. If this is not achievable, we suggest intravenous hydrocortisone alone at a dose of 200 mg per day (grade 2C)

ARDS

Controversies and changes - ARDS
• We recommend target a tidal volume of 6 mL/kg predicted body weight in patients with sepsis-induced ARDS (grade 1A vs. 12 mL/kg).
• We suggest strategies based on higher rather than lower levels of PEEP for patients with sepsis-induced moderate to severe ARDS (grade 2C).
• We suggest recruitment maneuvers in sepsis patients with severe refractory hypoxemia due to ARDS (grade 2C).
• We suggest a short course of NMBA of not greater than 48 hours for patients with early sepsis-induced ARDS and a Pao2/Fio2 < 150 mm Hg (grade 2C).
• We suggest prone positioning be used in sepsis-induced ARDS patients with a Pao2/Fio2 ratio ≤ 100 mm Hg in facilities that have experience with such practices (grade 2B).
Sedation

Controversies and changes – less sedation
• We recommend that either continuous or intermittent sedation be minimized in mechanically ventilated sepsis patients, targeting specific titration endpoints (grade 1B).


Controversies and changes
• 2008: We recommend that stress ulcer prophylaxis using H2 blocker (grade 1A) or proton pump inhibitor (grade 1B) be given to patients with severe sepsis to prevent upper gastrointestinal (GI) bleed.
• 2012: We recommend that stress ulcer prophylaxis using H2 blocker or proton pump inhibitor be given to patients with severe sepsis/septic shock who have bleeding risk factors (grade 1B).
• When stress ulcer prophylaxis is used, we suggest the use of proton pump inhibitors rather than H2 receptor antagonists (H2RA) (grade 2C).
• We suggest that patients without risk factors should not receive prophylaxis (grade 2B).
Stress ulcer prophylaxis
• The balance of benefits and risks may thus depend on the individual patient’s characteristics (including the presence of enteral feeding) as well as on the local epidemiology of VAP and C. difficile infections.

Controversies and changes – DVT
• We recommend that patients with severe sepsis receive daily pharmacoprophylaxis against VTE (grade 1B).
• We recommend that this be accomplished with daily subcutaneous LMWH (grade 1B versus UFH twice daily and grade 2C versus UFH given thrice daily).
2008: • We recommend that
patients with severe sepsis receive DVT prophylaxis with either a) low dose UFH administered twice or three times per day; or b) daily LMWH unless there are contraindications (grade 1A).
• We suggest that in patients at very high risk, LMWH be used rather than UFH as LMWH is proven superior in other high-risk patients (grade 2C).

Sweet is good!

Controversies and changes – sweet is good!
• A protocolized approach to blood glucose management in ICU patients with severe sepsis commencing insulin dosing when 2 consecutive blood glucose levels are >180 mg/dL.
• This protocolized approach should target an upper blood glucose ≤180 mg/dL rather than an upper target blood glucose ≤ 110 mg/dL (grade 1A).
• 2008
We suggest use of a validated protocol for insulin dose adjustments and targeting glucose levels to the 150 mg/dL range (grade 2C).

Controversies and changes - platelets
• 2012: In patients with severe sepsis, we suggest that platelets be administered prophylactically when counts are ≤ 10,000/ mm3 (10 × 109/L) in the absence of apparent bleeding, as well when counts are ≤ 20,000/mm3 (20 × 109/L) if the patient has a significant risk of bleeding. Higher platelet counts (≥ 50,000/mm3 [50 × 109/L]) are advised for active bleeding, surgery, or invasive procedures (grade 2D).
• 2008: In patients with severe sepsis, we suggest that platelets be administered when counts are 5000/mm3 (5x109/L) regardless of apparent bleeding.
• Platelet transfusion may be considered when counts are 5000–30,000/mm3 (5–30 109/L) and there is a significant risk of bleeding. Higher platelet counts (50,000/mm3 [50 109/L]) are typically required for surgery or invasive procedures (grade 2D).

Nutrition

Controversies and changes – don’t push calories...
• 1. We suggest administering oral or enteral (if necessary) feedings, as tolerated, rather than either complete fasting or provision of only intravenous glucose within the first 48 hrs after a diagnosis of severe sepsis/septic shock (grade 2C).
• 2. We suggest avoiding mandatory full caloric feeding in the first week, but rather suggest low-dose feeding (eg, up to 500 kcal per day), advancing only as tolerated (grade 2B).
• 3. We suggest using intravenous glucose and enteral nutrition rather than total parenteral nutrition (TPN) alone or parenteral nutrition in conjunction with enteral feeding in the first 7 days after a diagnosis of severe sepsis/septic shock (grade 2B).
• 4. We suggest using nutrition with no specific immunomodulating supplementation in patients with severe sepsis (grade 2C).
• Translation: Atempt feeding as patient tolerates, don’t push full caloric intake for its own sake, underfeeding (2/3) / trophic feeding (up to 500 kcal) is OK/even better (but may increase it if fast recovery), don’t use TPN early, do not use supplements (all 2C)

Controversies and changes - Communication
2012Setting Goals of Care
• 1. We recommend that goals of care and prognosis be discussed with patients and families (grade 1B).
• 2. We recommend that the goals of care be incorporated into treatment and end-of-life care planning, utilizing palliative care principles where appropriate (grade 1B).
• 3. We suggest that goals of care be addressed as early as feasible, but no later than within 72 hrs of ICU admission (grade 2C).
2008 Consideration for
Limitationof Support
• 1. We recommend that advance care planning, including the communication of likely outcomes and realistic goals of treatment, be discussed with patients and families (grade 1D).

Sepsis bundles: Converting guidelinesinto meaningful change in behavior
Controversies and changes - Fluids
2008 We recommend fluid resuscitation with either natural/artificial colloids or crystalloids (1B)
2011 We recommend not using ‘200 starch’ (Grade 1A) and suggest not using 130 starches (2B)

Albumin versus other fluids for sepsis
Patient or population: Patients with sepsisSettings: Intensive care unitIntervention: Albumin versus other fluids.
Outcomes Illustrative comparative risks (95% CI)
Relative effect(95% CI)
No of Participants(studies)
Quality of the evidence(GRADE)
Comments
Assumed risk Corresponding risk
Other fluids (may be crystalloid or colloid)
Albumin
Short term mortality
Study population RR 0.84 (0.73 to 0.97)
1683(11 studies)
⊕⊕⊕⊝moderate342 per 1000 287 per 1000
(249 to 332)
Short term mortality(albumin vs crystalloids)
444 per 1000 377 per 1000(324 t o440)
RR 0.85(0.73 to 0.98)
1402 (4 studies)
⊕⊕⊕⊝moderate1
Short term mortality(albumin vs other colloids)
342 per 1000 195 per 1000(249 to 396)
RR 0.81(0.57 to 1.16)
281(7 studies)
⊕⊕⊕⊝moderate1
*The assumed risk is the control group risk across studies. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).CI: Confidence interval; RR: Risk ratio
Grade reduced for imprecision.

Controversies and changes fluids
2011 We suggest to include some albumin over crystalloids alone in the initial fluid resuscitation regimen(2B) and recommend albumin be combined with crystalloids in the initial fluid resuscitation regimen when serum albumin concentration is known to be low (1B)
In the initial volume management of septic patients we suggest crystalloids with supplemental discretionary use of albumin over other management strategies (2B)

Controversies and changes - fluids
2012 We recommend crystalloids be used as the initial fluid of choice in the resuscitation (1B)
2012 We recommend against the use of hydroxyethyl starches (HES) for fluid resuscitation (grade 1B).
2012 We suggest the use of albumin in the fluid resuscitation of severe sepsis and septic shock when patients require substantial amounts of crystalloids (grade 2C)

Controversies and changes - fluids
2013 administration of saline should be limited in septic shock (2C) (proposal)

PAD guideliens

PAD guidelines

PAD guideliness
• Process– 20 people– 6 year long work– Developing questions,
review/evaluate/sumarize evidence– Develop descriptive statements and
actionable recomendation– Evaluated and compared pain,
agitation/sedation and delirium measurement tools

PAD guideliness
• Differences from previous 2002 guidelines:– Use of GRADE (connecting evidence with
recommendations)
– Use of professional librarian (19,000 papers, 472 references)
– Scope (Pain, Agitation, Sedation, Delirium)
– Anonymous pooling of opinions and assessments
– Multidisciplinary approach (MD (9), RN (6), pharmacy (2), geriatrics)
PAD guidelines
Descriptive statement
• Adult medical, surgical, and trauma ICU patients routinely experience pain, both at rest and with routine ICU care (B)
• Pre-procedural analgesia used in about 20% (B)
• All available IV opioids, when titrated to similar pain intensity endpoints, are equally effective (C).
Actionable recommendation
• We recommend that pain be routinely monitored in all adult ICU patients (+1B)
• We recommend that IV opioids be considered as the first-line drug class of choice to treat non-neuropathic pain in critically ill patients (+1C)
• We suggest that analgesia-first sedation be used in mechanically ventilated adult ICU patients (+2B)

Pain
PAD guidelines - Pain
• Pain frequent (especially in cardiac surgery, especially in women) (B)
• All opioids, when titrated, are equally effective (C)
• Preemptive analgesis prior to chest tube removal (1C)
• Opioids first class of drugs (1C)• The Behavioral Pain Scale (BPS) and the
Critical-Care Pain Observation Tool (CPOT) are the most valid and reliable behavioral pain scales (B).

PAD guidelines - Pain
Goal – 5 or less; 6 or more not acceptable

PAD guidelines – Agitation and Sedation
• Maintaining light levels of sedation :– is associated with shorter duration of MV and a shorter ICU
LOS [B) – increases the physiologic stress response, but not myocardial
ischemia (B) – its association with psychological stress remains unclear (C).
• We recommend that sedative medications be titrated to maintain a light rather than a deep level of sedation in adult ICU patients, unless clinically contraindicated (+1B).– RASS and SAS (Richmond Sedation Agitation Scale and Reiker
SAS) are valid sedation assesment tools (B)

PAD guidelines – Agitation and Sedation

PAD guidelines – Agitation and sedation
• Prompt identification and treatment of possible underlying causes of agitation, such as pain, delirium, hypoxemia, hypoglycemia, hypotension, or withdrawal from alcohol and other drugs, are important
• Maintenance of patient comfort, provision of adequate analgesia, frequent reorientation, and optimization of the environment to maintain normal sleep patterns, should be attempted before administering sedatives

PAD guidelines – Agitation and Sedation
• We suggest that sedation strategies using nonbenzodiazepine sedatives (either propofol or dexmedetomidine) may be preferred over sedation with benzodiazepines (either midazolam or lorazepam) to improve clinical outcomes in mechanically ventilated adult ICU patients (+2B).

PAD guidelines – Agitation and Sedation

Delirium
PAD guidelines – Delirium
• Delirium:– syndrome of acute onset of cerebral dysfunction with
change or fluctuation in baseline mental status– disorganized thinking or an altered level of consciousness – inattention, inability to sustain or shift attention– reduced awareness of the environment– perceptual disturbance (i.e., hallucinations, delusions)
are frequent but neither required for diagnosis– Other symptoms : sleep disturbances, emotional
disturbances (i.e., fear, anxiety, anger, depression, apathy, euphoria)
– may be agitated (hyperactive delirium), calm or lethargic (hypoactive delirium), or may fluctuate between the two subtypes.

PAD guidelines – Delirium
Delirium is associated with:– increased mortality (A) – prolonged LOS (A)– development of post-ICU cognitive impairment
(B)– Risk factors (baseline): dementia, hypertension,
alkoholism, severity of ilness (B)– Risk factors (later): coma, benzodiazepine use
(in comparison to dex) (B)– Confusion Assesment Method (CAM-ICU) and
Intensive Care Delirium Screening Checklist most valid for monitoring (A)
– We recommend routine monitoring for delirium in adult ICU patients (+1B)

PAD guidelines – Delirium
• Delirium prevention:– early mobilization (1B)
• Delirium treatment:– No evidence to support haloperidol (0)– Atypical may reduce duration (in comparison to
placebo (all patients on haloperidol) (C)– Against ryvastigmine (1B)– Early mobilization (+1B)– If sedation required (and no benzos or alkohol
withdrawal), suggest dexmedetomidine vs. benzos (2B)
– No magic bullet drug, more in way of delivering care
PAD guidelines – Management Strategies
• Strategies for management:– Measure PAD– Analgesia first sedation (2B)– Daily sedation interruption OR light target sedation
(with sedation only if required and goal to allow responsiveness and awarness) (1B)
– Promoting and protecting sleep cycles (1C)– We recommend using an interdisciplinary ICU team
approach that includes provider education, preprinted and/or computerized protocols and order forms, and quality ICU rounds checklists to facilitate the use of pain, agitation, and delirium management guidelines or protocols in adult ICUs (+1B)

Future challenges for method center
• training of GRADE resource individuals;
• training of content area experts in GRADE methodology (rise and usefulness of webinars);
• planning for the future updates and reiterations (succession plans);
• continuous struggle to link the recommendation to evidence;

Proton Pump Inhibitors Versus Histamine 2 Receptor Antagonists for Stress Ulcer Prophylaxis in Critically Ill Patients: A Systematic Review and Meta-Analysis.Waleed Alhazzani, Farhan Alenezi, et al
Neuromuscular blocking agents in acute respiratory distress syndrome: a systematic review and meta-analysis of randomized controlled trials.Alhazzani W, Alshahrani M, et al
The Effect of Selenium Therapy on Mortality in Patients With Sepsis Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Waleed Alhazzani, et al

النهاية.لك .شكرا


















