43
When Trauma and When Trauma and Psychosis Mix Psychosis Mix Presenter: Ron Unger LCSW Presenter: Ron Unger LCSW 541-513-1811 541-513-1811 [email protected] [email protected]
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | ron-unger-lcsw |
| View: | 10,631 times |
| Download: | 5 times |
When Trauma and When Trauma and Psychosis MixPsychosis Mix
Presenter: Ron Unger LCSWPresenter: Ron Unger LCSW541-513-1811541-513-1811
[email protected]@efn.org
Defining Psychological TraumaDefining Psychological Trauma
DSM focuses on perceived physical DSM focuses on perceived physical threatthreat– But this is somewhat arbitraryBut this is somewhat arbitrary
Psychological impact is keyPsychological impact is key– Trauma is created by a combination of Trauma is created by a combination of
sense of overwhelming threat, or terror, sense of overwhelming threat, or terror, with helplessnesswith helplessness
– It’s not a specific type of event, but our It’s not a specific type of event, but our appraisal of the event, which causes appraisal of the event, which causes psychological traumapsychological trauma
Psychosis: the last holdout for Psychosis: the last holdout for those who deny the role of traumathose who deny the role of trauma
In 1975 the Comprehensive In 1975 the Comprehensive Textbook of Psychiatry, a respected Textbook of Psychiatry, a respected source of information, estimated the source of information, estimated the prevalence of incest to be 1 in a prevalence of incest to be 1 in a millionmillion
Since then, a lot has changed Since then, a lot has changed regarding recognition of the regarding recognition of the existence and role of trauma, but not existence and role of trauma, but not for those with psychosis, especially for those with psychosis, especially in the U.S.in the U.S.
From an official “Illness From an official “Illness Management and Recovery” Management and Recovery”
handout:handout: ““What causes schizophrenia?What causes schizophrenia? ““Schizophrenia is nobody’s fault. This Schizophrenia is nobody’s fault. This
means that you did not cause the means that you did not cause the disorder, and neither did your family disorder, and neither did your family members or anyone else. Scientists members or anyone else. Scientists believe that the symptoms of believe that the symptoms of schizophrenia are caused by a schizophrenia are caused by a chemical imbalance in the brain.”chemical imbalance in the brain.”
The Evidence that Trauma can Cause Psychotic Symptoms:
The high incidence of psychotic symptoms in people who have been traumatized
The high incidence of trauma histories in people who have psychotic symptoms
Studies that show the greater the severity of the trauma, the greater likelihood of more, and more intense, psychotic symptoms
Brain changes sometimes linked with psychotic symptoms are also found in many children and adults with PTSD
There are logical and meaningful connections between psychotic symptoms and normal reactions to traumatic experience
Three levels of possible Three levels of possible relationship between trauma and relationship between trauma and
psychosis:psychosis:11 Trauma, especially childhood sexual trauma, can Trauma, especially childhood sexual trauma, can
cause psychosis latercause psychosis later22 Having psychotic symptoms can in itself be Having psychotic symptoms can in itself be
traumatizingtraumatizing33 The response by others to one’s psychosis, such The response by others to one’s psychosis, such
as the response of the mental health system, of as the response of the mental health system, of friends, of family, and of society, can also be friends, of family, and of society, can also be traumatizingtraumatizing
Further trauma can cause more psychosis, in a Further trauma can cause more psychosis, in a vicious circlevicious circle
Trauma (involves
perceived need to reorganize in a radical way.)
Psychosis (disorganization or mistaken way
of being organized.)
Trauma (involves
perceived need to reorganize in a radical way.)
Psychosis (disorganization
or mistaken way of being organized.)
Peter Bulimore’s story Peter Bulimore’s story illustrates all three levels illustrates all three levels of trauma, as well as why of trauma, as well as why it is so important for the it is so important for the mental health system to mental health system to
begin to understand these begin to understand these issues.issues.
What is the impact when the What is the impact when the possible link between trauma & possible link between trauma &
psychosis is denied?psychosis is denied? Trauma is often not even asked Trauma is often not even asked
about, much less discussedabout, much less discussed– Potentially, through decades of Potentially, through decades of
treatmenttreatment Understandable reactions to trauma Understandable reactions to trauma
may be defined as non-may be defined as non-understandableunderstandable
Psychotherapy for trauma is deniedPsychotherapy for trauma is denied Even self-understanding may be Even self-understanding may be
discourageddiscouraged
Why is the role of trauma in causing Why is the role of trauma in causing psychosis commonly denied?psychosis commonly denied?
It is hoped that since some psychosis has It is hoped that since some psychosis has a biological explanation, all of it will prove a biological explanation, all of it will prove to have a biological explanationto have a biological explanation
Evidence of genetic causation is commonly Evidence of genetic causation is commonly exaggeratedexaggerated
Tendency to believe that if biology is Tendency to believe that if biology is involved at all, it must be primaryinvolved at all, it must be primary
If seen as not primarily biological, then If seen as not primarily biological, then power of psychiatrists & pharmaceutical power of psychiatrists & pharmaceutical companies would be reducedcompanies would be reduced
Denial of trauma has lessened overall, but Denial of trauma has lessened overall, but this hasn’t yet reached the field of this hasn’t yet reached the field of psychosispsychosis
Why is the role of trauma in causing Why is the role of trauma in causing psychosis commonly denied? psychosis commonly denied?
(continued)(continued) Past overly simplistic judgments and Past overly simplistic judgments and
assumptions by some of those who did see assumptions by some of those who did see a role for trauma in causing psychosisa role for trauma in causing psychosis
Biological explanations seem much simplerBiological explanations seem much simpler Biological model is easier for bureaucrats Biological model is easier for bureaucrats
to deal withto deal with Idea that if trauma causes a mental Idea that if trauma causes a mental
problem, it will be PTSDproblem, it will be PTSD
The PTSD model of how trauma The PTSD model of how trauma “makes psychosis worse”“makes psychosis worse”
Argues that “schizophrenia” is a real Argues that “schizophrenia” is a real illness independent of trauma, but illness independent of trauma, but that trauma can make a mild case that trauma can make a mild case much worsemuch worse
Problems of this model:Problems of this model:– Ignores evidence that trauma can cause Ignores evidence that trauma can cause
psychosis, not just make it worse psychosis, not just make it worse – Leads to seeing “schizophrenia” as a a Leads to seeing “schizophrenia” as a a
“thing in itself” separate from the “thing in itself” separate from the response to trauma, when it may not beresponse to trauma, when it may not be
Understanding why trauma causes much more than just
“PTSD” A PTSD diagnosis requires symptoms that can be
identified as revolving around the trauma There must be at least one of the following:
– recurrent recollections, or – distressing dreams that relate to the trauma or– acting or feeling as though it's reoccurring, – or distress at exposure to external or internal cues that
symbolize or resemble the event.
But if a person successfully avoids thinking about or processing the trauma in an obvious way, then there will be no symptoms that clearly revolve around the trauma.
Common factors in PTSD and Common factors in PTSD and psychosis:psychosis:
High arousal & hypervigilanceHigh arousal & hypervigilance Sleep disturbanceSleep disturbance AvoidanceAvoidance Emotional numbingEmotional numbing Selective AttentionSelective Attention Safety behaviorsSafety behaviors Dysfunctional thought control strategiesDysfunctional thought control strategies Expressed emotion causes relapseExpressed emotion causes relapse DissociationDissociation Intrusive phenomena: thoughts, sensory, Intrusive phenomena: thoughts, sensory,
emotions emotions
Is trauma responsible for all psychotic symptoms?
Lots of factors, not just trauma, contribute to vulnerability– Most of these factors, like trauma, have a disorientating
effect Such as drug use, lack of sleep, brain damage for some,
mistaken beliefs, even lack of good social support can be understood to be
disorientating But trauma also contributes to many of the above
factors– Such as a traumatized person is more likely to use
substances, or to lose sleep, or to have damaged support systems
And as vulnerability increases, stresses in the environment become increasingly traumatizing, which is what sends people “over the edge”
Catastrophic Interaction ModelCatastrophic Interaction Model
That there are a number of routes by That there are a number of routes by which severe trauma may tip someone which severe trauma may tip someone toward psychosistoward psychosis– When various processes occur together, then When various processes occur together, then
there is a bifurcation into psychosisthere is a bifurcation into psychosis For example:For example:
– Intrusive trauma memoriesIntrusive trauma memories– Processing biases like overestimation of Processing biases like overestimation of
danger, or jump to conclusionsdanger, or jump to conclusions– Negative opinions about self lead to greater Negative opinions about self lead to greater
distress about hallucinations that occurdistress about hallucinations that occur
How the Stress/Vulnerability model How the Stress/Vulnerability model was hijackedwas hijacked
The idea is that “vulnerable” people, The idea is that “vulnerable” people, when subject to excess stress, when subject to excess stress, become psychoticbecome psychotic– Biological psychiatry quickly adopted Biological psychiatry quickly adopted
this model, with “vulnerability” assumed this model, with “vulnerability” assumed to be always biological, such as genetic to be always biological, such as genetic etc.etc.
But psychological trauma, as well as But psychological trauma, as well as certain other experiences, can also certain other experiences, can also lead to vulnerabilitylead to vulnerability
Why trauma causes problems in Why trauma causes problems in integrating experiencesintegrating experiences
Ordinarily, the hOrdinarily, the hippocampus serves to bind ippocampus serves to bind individual features of incoming information individual features of incoming information into a spatial/temporal contextinto a spatial/temporal context– Then info goes to amygdalaThen info goes to amygdala
But when trauma is too intense, info goes But when trauma is too intense, info goes straight to the amygdalastraight to the amygdala– Resulting in memory fragments that contain Resulting in memory fragments that contain
high affecthigh affect With no contextWith no context
Decontextualized trauma Decontextualized trauma flashbacks can easily become flashbacks can easily become
psychosispsychosis
Psychotic interpretations of the Psychotic interpretations of the activation of trauma memoriesactivation of trauma memories– Like a voice that echoes meanings first Like a voice that echoes meanings first
encountered during traumaencountered during trauma– Or “emotional flashbacks”Or “emotional flashbacks”– Even “body memories”Even “body memories”
Key Difference between a Key Difference between a flashback and a hallucination:flashback and a hallucination:
In a flashback, there is the recognition In a flashback, there is the recognition that what one is experiencing now is that what one is experiencing now is related to the past traumarelated to the past trauma– But when a trauma has been especially But when a trauma has been especially
overwhelming or denied, this recognition itself overwhelming or denied, this recognition itself is blockedis blocked
– A hallucination is often just a “flashback” type A hallucination is often just a “flashback” type of experience where the connection to the past of experience where the connection to the past is overlooked or denied.is overlooked or denied.
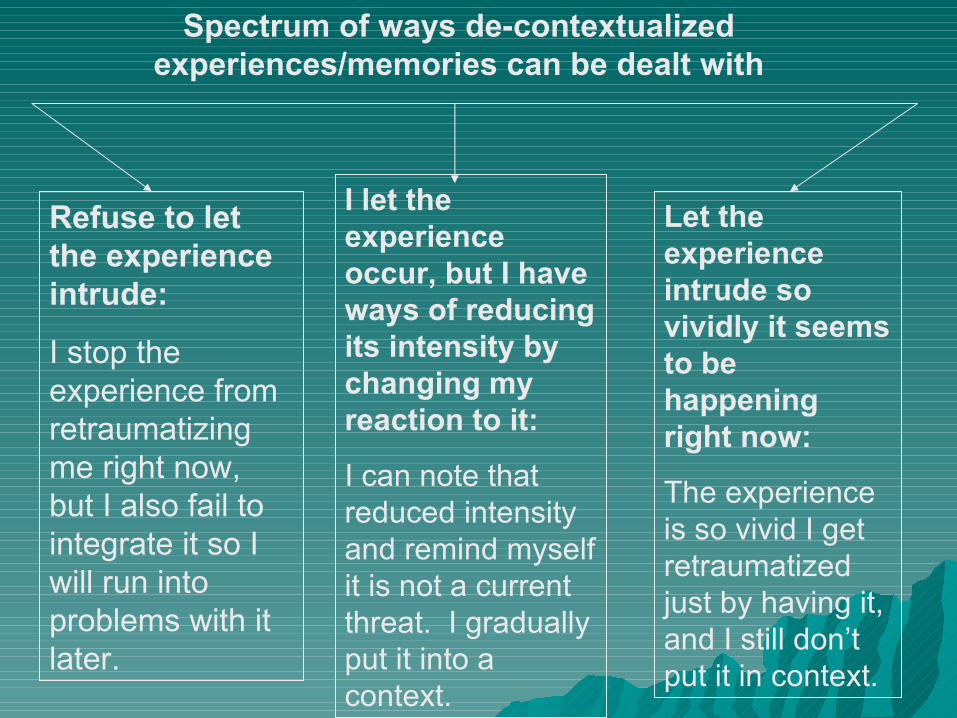
Let the experience intrude so vividly it seems to be happening right now:
The experience is so vivid I get retraumatized just by having it, and I still don’t put it in context.
Refuse to let the experience intrude:
I stop the experience from retraumatizing me right now, but I also fail to integrate it so I will run into problems with it later.
I let the experience occur, but I have ways of reducing its intensity by changing my reaction to it:
I can note that reduced intensity and remind myself it is not a current threat. I gradually put it into a context.
Spectrum of ways de-contextualized experiences/memories can be dealt with
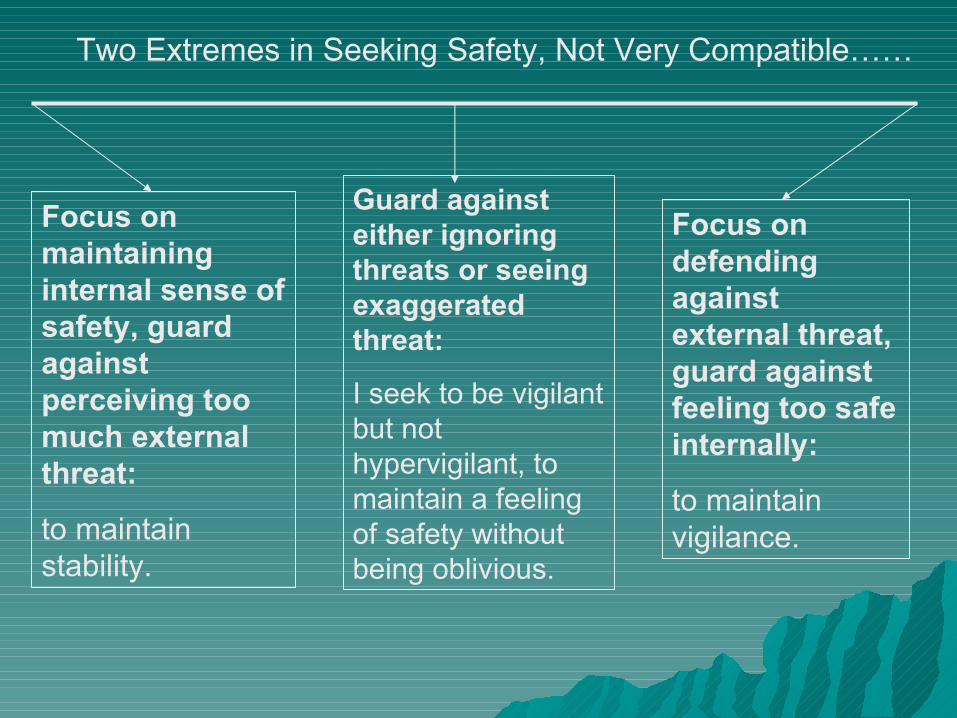
Focus on defending against external threat, guard against feeling too safe internally:
to maintain vigilance.
Focus on maintaining internal sense of safety, guard against perceiving too much external threat:
to maintain stability.
Guard against either ignoring threats or seeing exaggerated threat:
I seek to be vigilant but not hypervigilant, to maintain a feeling of safety without being oblivious.
Two Extremes in Seeking Safety, Not Very Compatible……
Two types of hallucinations and/or delusions:
Those whose function is to get the person to see the danger that they may have been blocking out– These are on a spectrum with “flashbacks” that
are common after trauma Those whose function is to protect the
person from being overwhelmed by what they are afraid of– These are on a spectrum with dissociation, the
ability to separate from experience that is overwhelming All types of grandiosity can be understood as having
a protective function
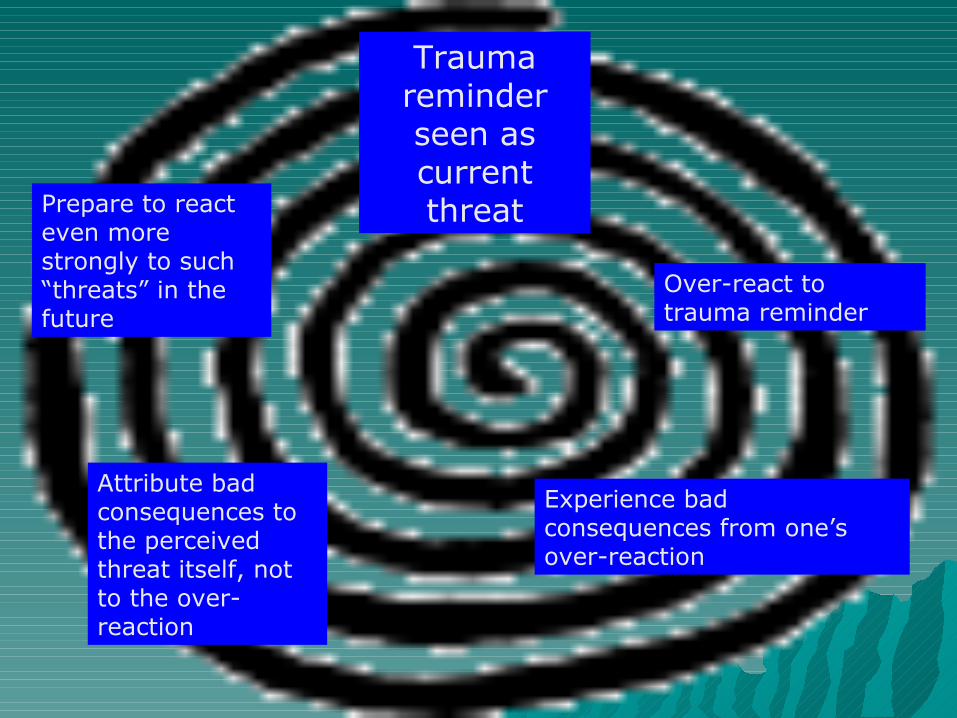
Trauma reminder seen as current threat
Over-react to trauma reminder
Experience bad consequences from one’s over-reaction
Prepare to react even more strongly to such “threats” in the future
Attribute bad consequences to the perceived threat itself, not to the over-reaction
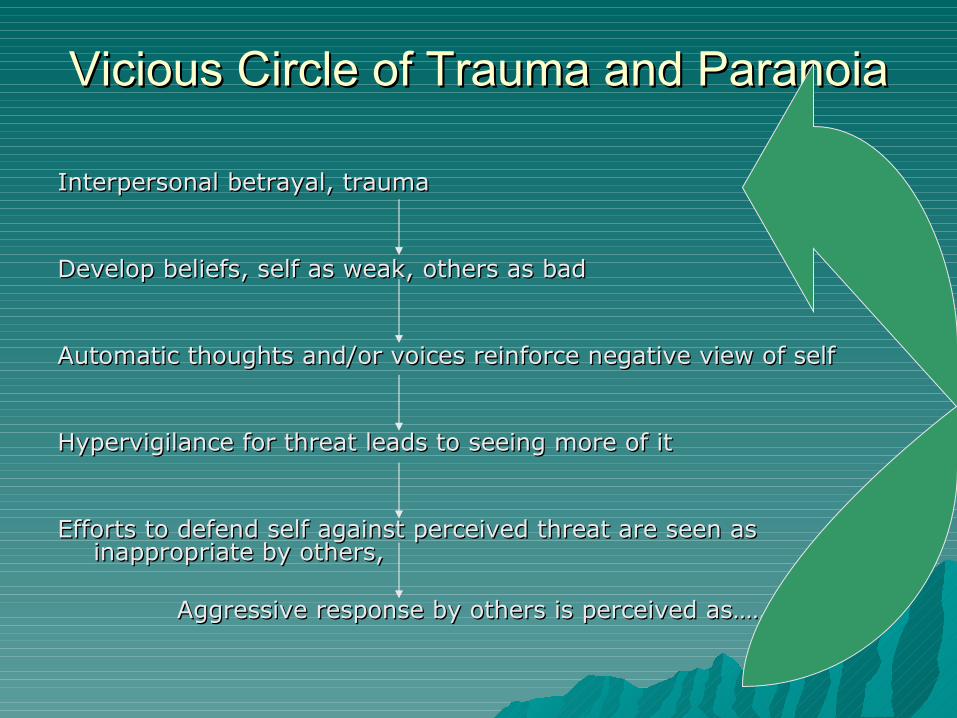
Vicious Circle of Trauma and ParanoiaVicious Circle of Trauma and Paranoia
Interpersonal betrayal, traumaInterpersonal betrayal, trauma
Develop beliefs, self as weak, others as badDevelop beliefs, self as weak, others as bad
Automatic thoughts and/or voices reinforce negative view of selfAutomatic thoughts and/or voices reinforce negative view of self
Hypervigilance for threat leads to seeing more of itHypervigilance for threat leads to seeing more of it
Efforts to defend self against perceived threat are seen as Efforts to defend self against perceived threat are seen as inappropriate by others, inappropriate by others,
Aggressive response by others is perceived as…….Aggressive response by others is perceived as…….
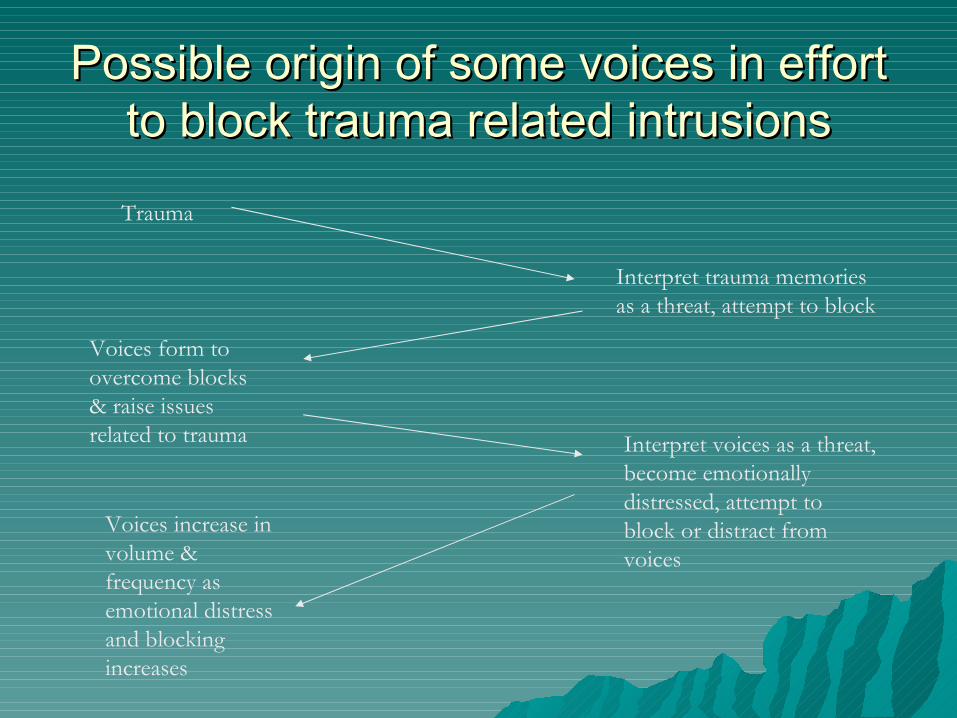
Possible origin of some voices in effort Possible origin of some voices in effort to block trauma related intrusionsto block trauma related intrusions
Trauma
Interpret trauma memories as a threat, attempt to block
Voices form to overcome blocks & raise issues related to trauma Interpret voices as a threat,
become emotionally distressed, attempt to block or distract from voices
Voices increase in volume & frequency as emotional distress and blocking increases
It is the “blocking” itself that gives It is the “blocking” itself that gives an intrusion its poweran intrusion its power
Trying to get rid of the “madness” is Trying to get rid of the “madness” is actually part of the madnessactually part of the madness
““The way out of hell is through the The way out of hell is through the center”center”– Just accepting the trauma, just Just accepting the trauma, just
accepting the intrusion or unwanted accepting the intrusion or unwanted “psychotic” experience, allows us to put “psychotic” experience, allows us to put it into perspective for what it isit into perspective for what it is
– And it’s putting it into perspective, into And it’s putting it into perspective, into context, that allows us to move oncontext, that allows us to move on
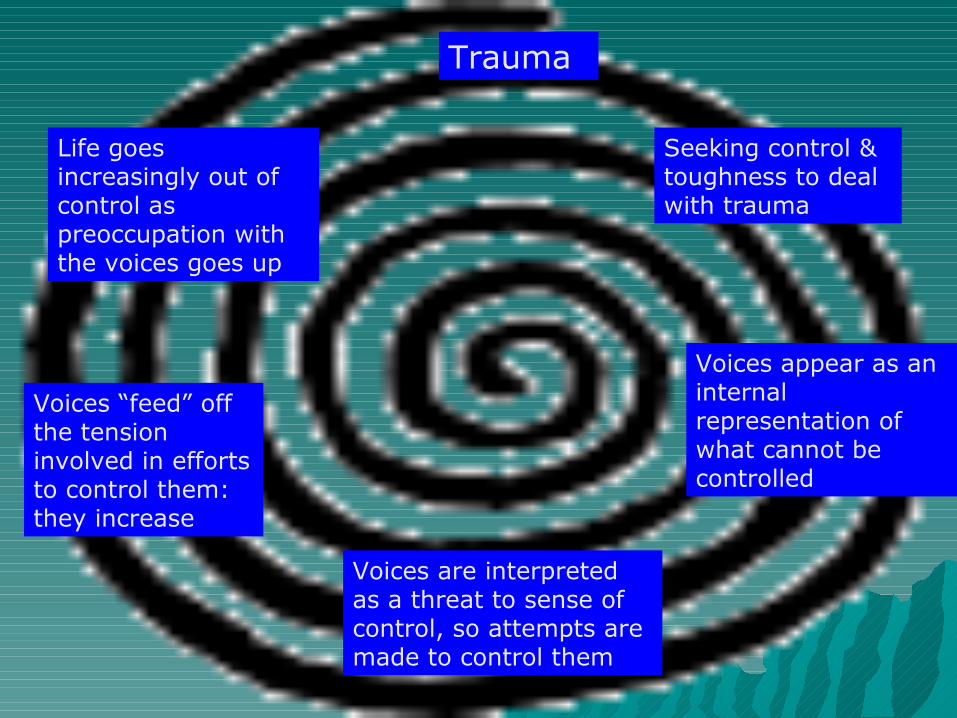
Trauma
Seeking control & toughness to deal with trauma
Voices appear as an internal representation of what cannot be controlled
Voices are interpreted as a threat to sense of control, so attempts are made to control them
Voices “feed” off the tension involved in efforts to control them: they increase
Life goes increasingly out of control as preoccupation with the voices goes up
Effect of dissociation on self-Effect of dissociation on self-organization of dissociated contentorganization of dissociated content Whatever is not integrated in some Whatever is not integrated in some
way may take on a life of its ownway may take on a life of its own Content not yet integrated may be Content not yet integrated may be
simple or complexsimple or complex– From automatic thoughts, emotions, From automatic thoughts, emotions,
memory fragmentsmemory fragments– To mood states, perspectives, voicesTo mood states, perspectives, voices– To complex identity states seen as To complex identity states seen as
“alternate personalities” or alien entities“alternate personalities” or alien entities
Comparing “dissociative voices” Comparing “dissociative voices” with “psychotic voices”with “psychotic voices”
No significant reliable differences No significant reliable differences have been found between the voices have been found between the voices of those diagnosed with of those diagnosed with “schizophrenia” and discussions “schizophrenia” and discussions between alters in those diagnosed between alters in those diagnosed with dissociative identity disorder with dissociative identity disorder
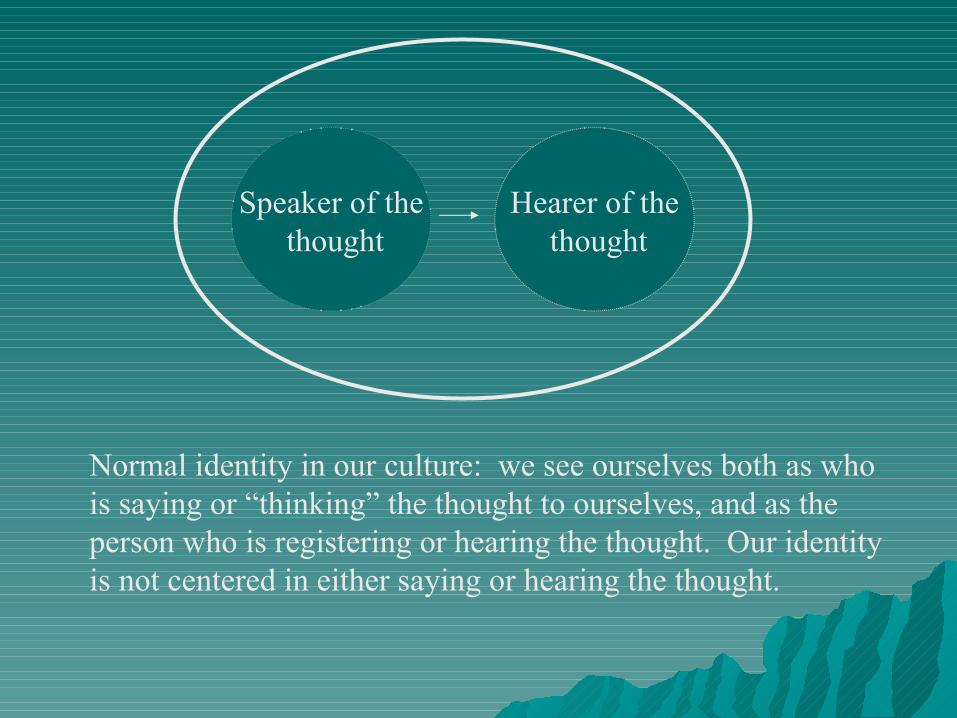
Hearer of the thought
Speaker of the thought
Normal identity in our culture: we see ourselves both as who is saying or “thinking” the thought to ourselves, and as the person who is registering or hearing the thought. Our identity is not centered in either saying or hearing the thought.
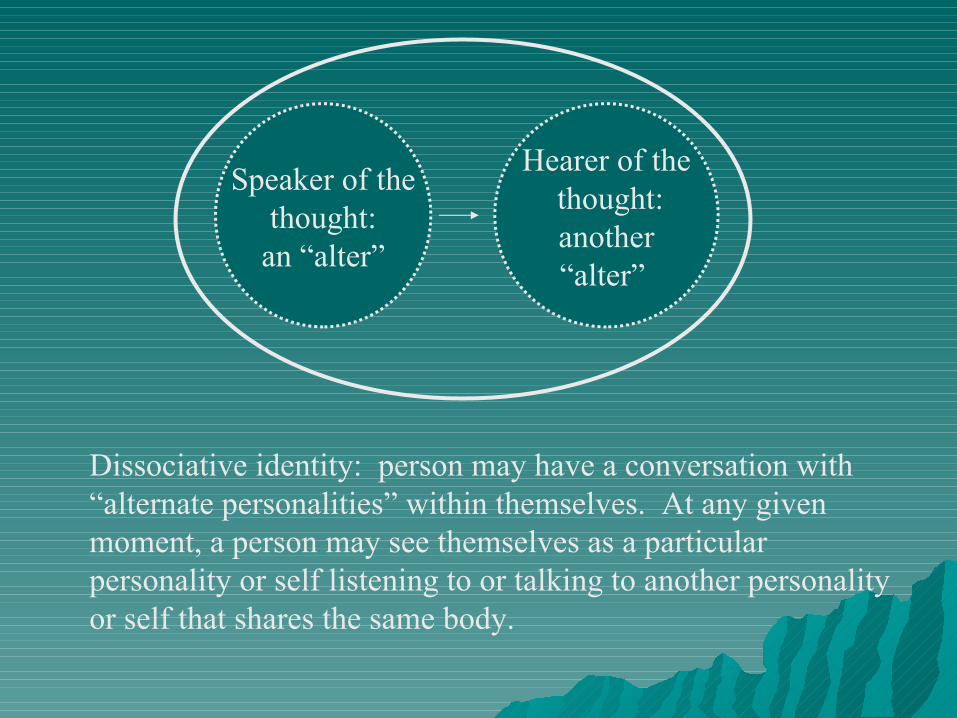
Hearer of the thought:another“alter”
Speaker of the thought: an “alter”
Dissociative identity: person may have a conversation with “alternate personalities” within themselves. At any given moment, a person may see themselves as a particular personality or self listening to or talking to another personality or self that shares the same body.
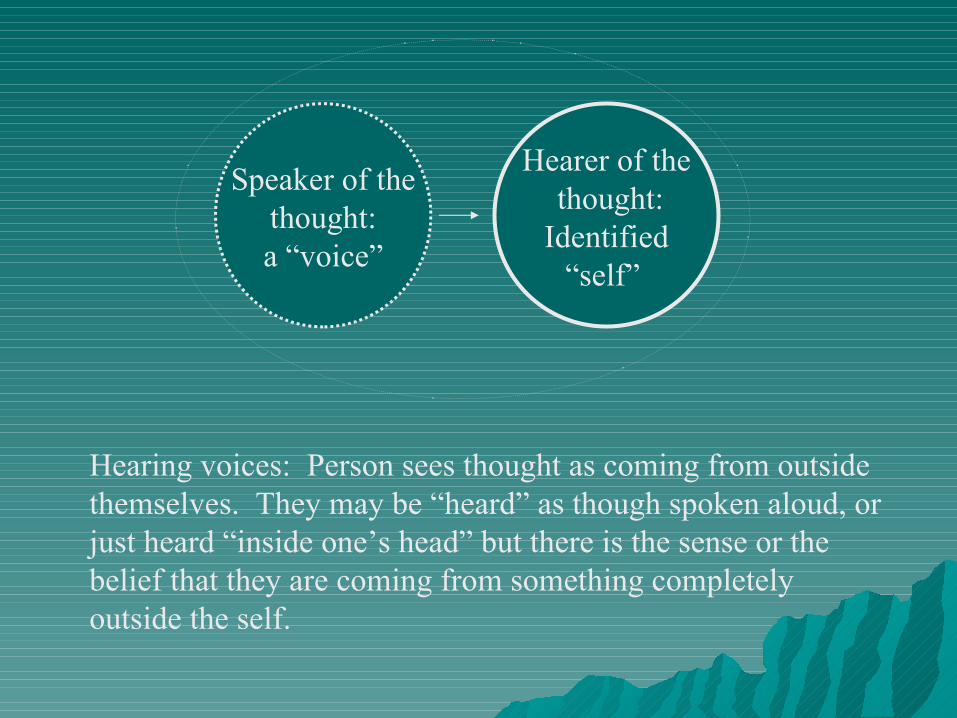
Hearer of the thought:Identified
“self”
Speaker of the thought: a “voice”
Hearing voices: Person sees thought as coming from outside themselves. They may be “heard” as though spoken aloud, or just heard “inside one’s head” but there is the sense or the belief that they are coming from something completely outside the self.
Bizarre delusions, such as thought Bizarre delusions, such as thought withdrawal and/or insertion, withdrawal and/or insertion,
& delusions of control& delusions of control These sort of “delusions” occur in These sort of “delusions” occur in
one-third to two-thirds of individuals one-third to two-thirds of individuals diagnosed with Dissociative Identity diagnosed with Dissociative Identity DisorderDisorder
Can easily be understood in terms of Can easily be understood in terms of interactions between “alters” or interactions between “alters” or subsystems created by dissociationsubsystems created by dissociation
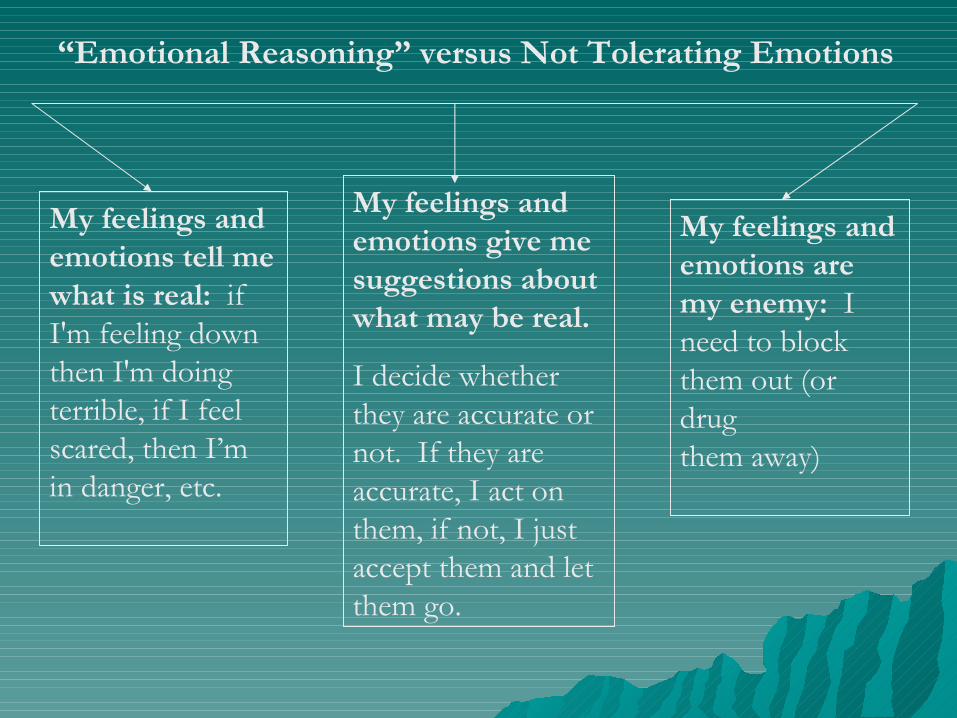
My feelings and emotions tell me what is real: if I'm feeling down then I'm doing terrible, if I feel scared, then I’m in danger, etc.
My feelings and emotions are my enemy: I need to block them out (or drugthem away)
My feelings and emotions give me suggestions about what may be real.
I decide whether they are accurate or not. If they are accurate, I act on them, if not, I just accept them and let them go.
“Emotional Reasoning” versus Not Tolerating Emotions
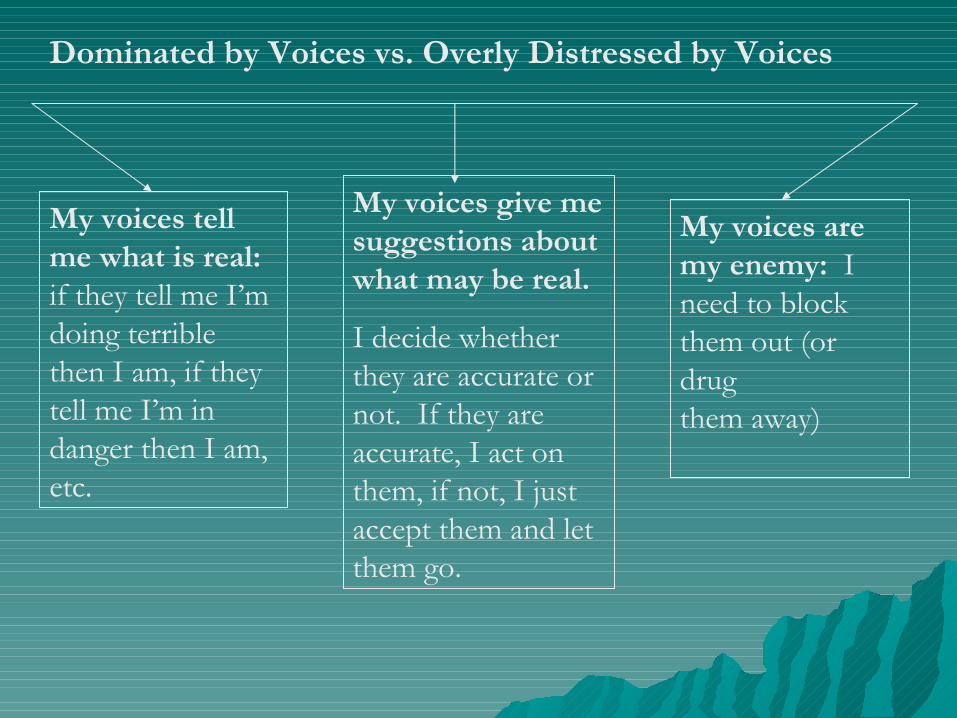
My voices tell me what is real: if they tell me I’m doing terrible then I am, if they tell me I’m in danger then I am, etc.
My voices are my enemy: I need to block them out (or drugthem away)
My voices give me suggestions about what may be real.
I decide whether they are accurate or not. If they are accurate, I act on them, if not, I just accept them and let them go.
Dominated by Voices vs. Overly Distressed by Voices
Excess focus on conflict:
I am always ready to do battle with the voices, my goal is to drive them out of existence.
Excess focus on appeasement:
It’s better to give in to the voices, even when they are unreasonable, rather than risk upsetting them.
Focus on living a good life:
I don’t waste energy opposing the voices just for the sake of conflict, but if they push for something that will harm my life, I will stand firm against it.
Excess focus on conflict vs. excess focus on appeasement
How can understanding the How can understanding the relationship between trauma & relationship between trauma & psychosis inform treatment?psychosis inform treatment?
Cognitive therapy for psychosis is an Cognitive therapy for psychosis is an evidence based approach that helps evidence based approach that helps clients appreciate the impact of clients appreciate the impact of stressful events, including trauma, stressful events, including trauma, on their mental stateon their mental state– This provides an alternative to either This provides an alternative to either
psychotic explanations or strictly psychotic explanations or strictly medical model explanations that may medical model explanations that may induce helplessnessinduce helplessness
Other trauma therapies can be Other trauma therapies can be integrated with CBT for psychosisintegrated with CBT for psychosis
First use CBT for psychosis to First use CBT for psychosis to provide an alternative to psychotic provide an alternative to psychotic interpretationsinterpretations
Then introduce a cognitive approach Then introduce a cognitive approach to trauma, to provide a framework to trauma, to provide a framework for understandingfor understanding
Then proceed to more experiential or Then proceed to more experiential or desensitizing approachesdesensitizing approaches– Proceeding cautiously, being willing to Proceeding cautiously, being willing to
go back to earlier stages when go back to earlier stages when necessarynecessary
When desensitization is effective:When desensitization is effective:
Trauma flashbacks and/or psychotic Trauma flashbacks and/or psychotic intrusions become simply memories intrusions become simply memories or thoughtsor thoughts– That are put into an understandable and That are put into an understandable and
manageable contextmanageable context– That are neither avoided nor overly That are neither avoided nor overly
attended toattended to Once they are put into context no Once they are put into context no
“illness” remains“illness” remains
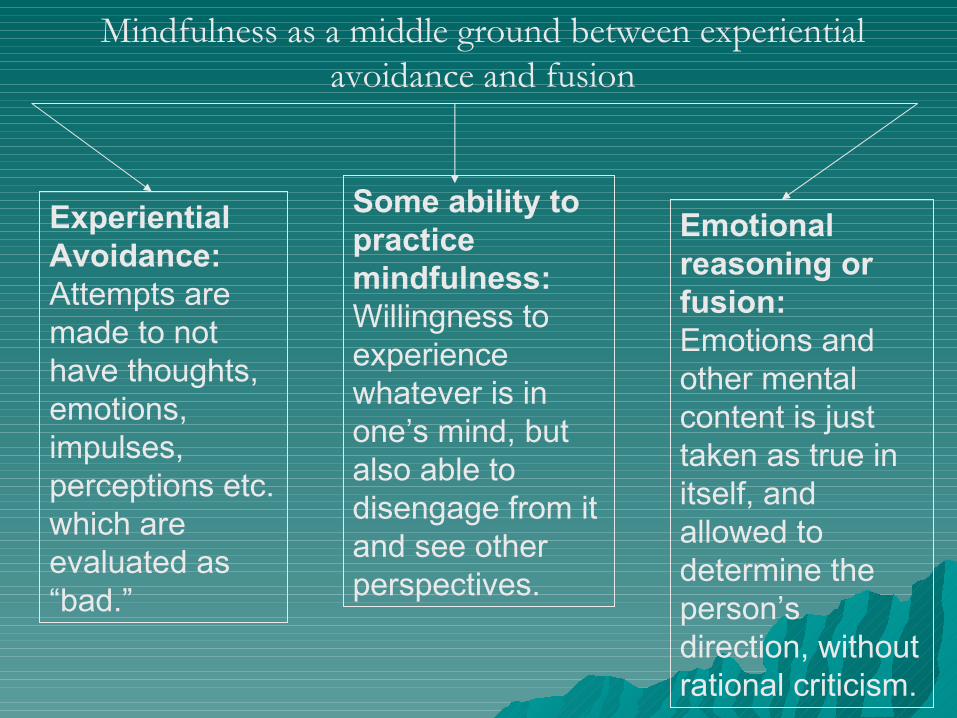
Experiential Avoidance: Attempts are made to not have thoughts, emotions, impulses, perceptions etc. which are evaluated as “bad.”
Emotional reasoning or fusion: Emotions and other mental content is just taken as true in itself, and allowed to determine the person’s direction, without rational criticism.
Some ability to practice mindfulness: Willingness to experience whatever is in one’s mind, but also able to disengage from it and see other perspectives.
Mindfulness as a middle ground between experiential avoidance and fusion
Temptation: to join conscious self in Temptation: to join conscious self in attempt to eliminate “the symptom”attempt to eliminate “the symptom”
This applies to voices, alters, unwanted This applies to voices, alters, unwanted emotions, thoughts, and impulsesemotions, thoughts, and impulses
Integration, rather than elimination, is a Integration, rather than elimination, is a better goalbetter goal– Though once integrated, “symptoms” can seem Though once integrated, “symptoms” can seem
to “disappear”to “disappear” To start with, join with conscious self To start with, join with conscious self
around goal of reducing distressaround goal of reducing distress– Then you can evaluate elimination versus Then you can evaluate elimination versus
integration as two possible strategiesintegration as two possible strategies Notice which is more helpfulNotice which is more helpful
The bottom line:The bottom line:
We need to study, rather than deny, We need to study, rather than deny, the connection between trauma and the connection between trauma and psychosispsychosis
We need to recognize that there is We need to recognize that there is generally a story to how people came generally a story to how people came to be mentally troubledto be mentally troubled
Then we can join with them in Then we can join with them in creating a story of recovery, rather creating a story of recovery, rather than retraumatization and chronic than retraumatization and chronic “illness”“illness”

















