72
Why We Should Avoid Transfusions Economics and Quality Care: The Case for Patient Blood Management Irwin Gross, M.D., Medical Director Transfusion Services, Eastern Maine
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | rosemary-melina-hancock |
| View: | 217 times |
| Download: | 2 times |

Why We Should Avoid Transfusions
Economics and Quality Care:The Case for Patient Blood
Management
Irwin Gross, M.D., Medical DirectorTransfusion Services, Eastern Maine Medical Center
Disclosures
• Speakers Bureau – Centocor Ortho Biotech• Medical Advisory Board – Strategic Healthcare Group

Who We Are
• 370 bed community and tertiary care hospital in rural Maine
• Large hospitalist service• High risk obstetrics• Trauma Center, Level 2• Dialysis Center• Family Practice residency • Cardiac surgery program
– Approx. 450 cases/yr.• Active heme/onc service
– 10 oncologists• No transplant surgery
Patient Blood Management (PBM)
The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin concentration, optimize hemostasis and minimize blood loss in an effort to improve patient outcome.

© Axel Hofmann/Shannon Farmer – SHEF Meeting Perth August 2010
Optimize Optimize erythro-erythro-poieispoieis
MinimizeMinimizebleeding bleeding & blood & blood
lossloss
Harness & Harness & optimize optimize
physiologiphysiologic c
tolerance tolerance of anemiaof anemia
What is Patient Blood Management:What is Patient Blood Management:The Three PillarsThe Three Pillars
Can Patient Blood Management Reduce the Need for Transfusions?
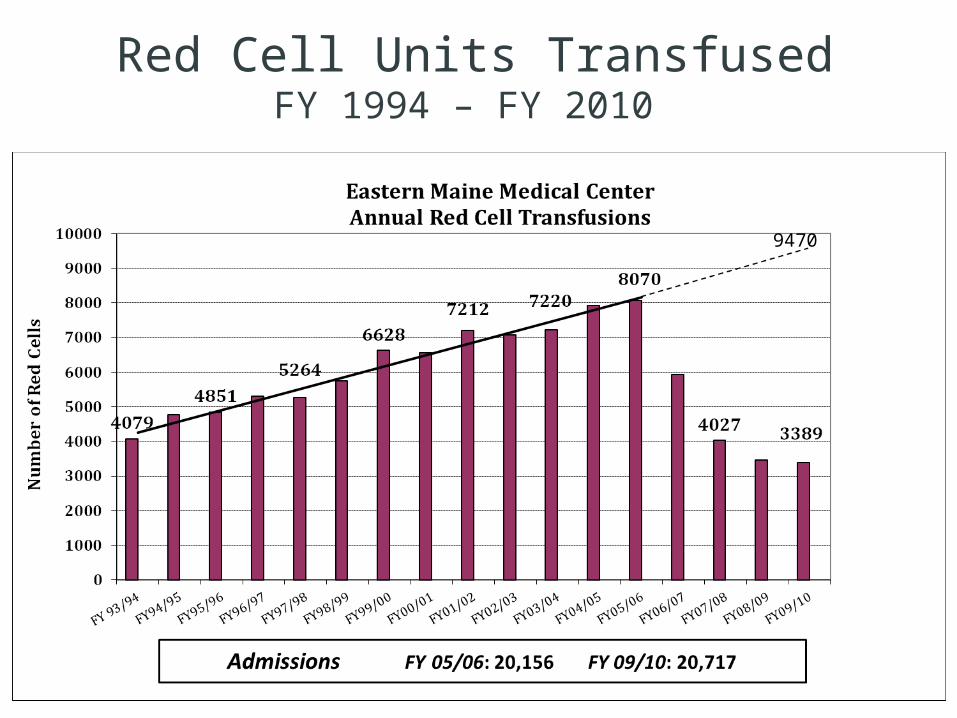
Red Cell Units TransfusedFY 1994 – FY 2010
9470

Patients Transfused:FY 1994 - 2010
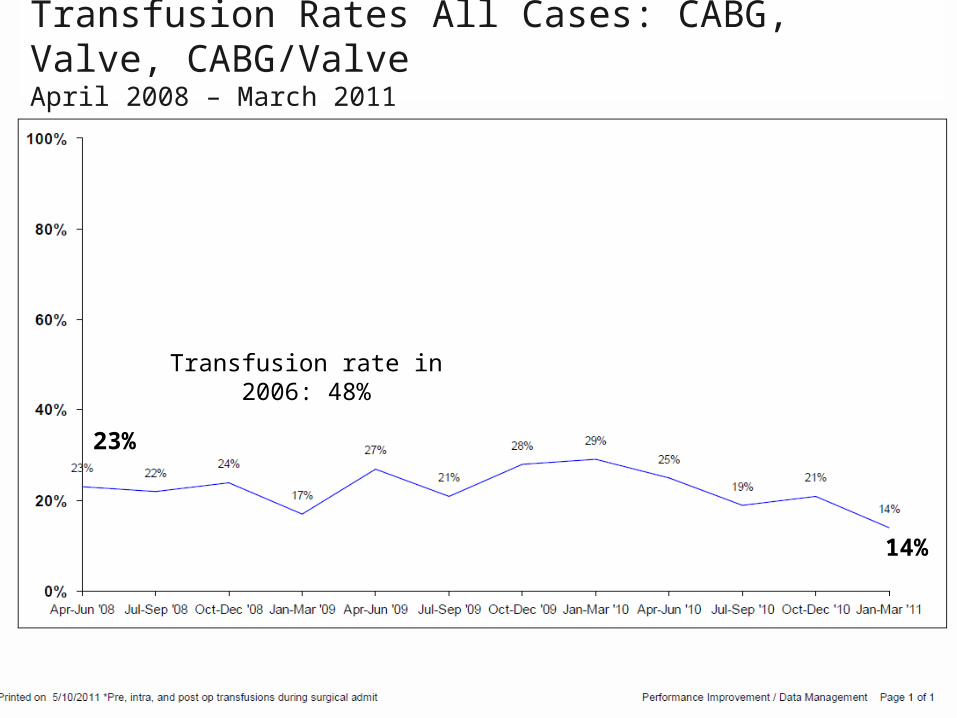
Transfusion Rates All Cases: CABG, Valve, CABG/ValveApril 2008 – March 2011
23%
14%
Transfusion rate in 2006: 48%
Cardiac Surgery and Transfusions
• With reduction in transfusion rate from 48% to approximately 20% , there was a reduction in:– Perioperative AMI– New onset renal failure– Perioperative infection– Stroke– Length of stay– No change in mortality
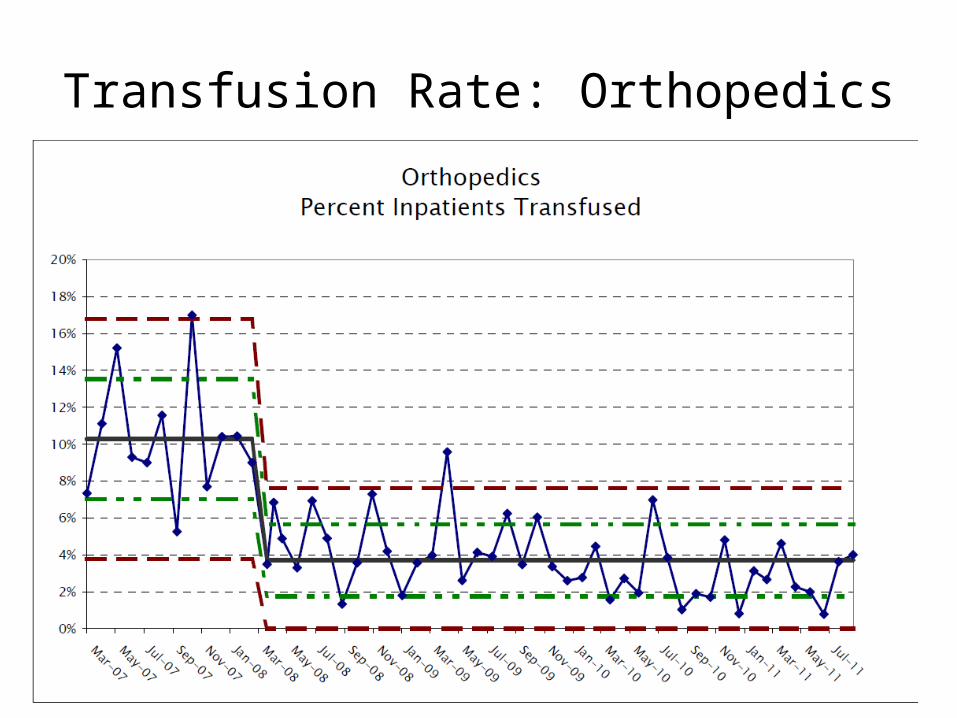
Transfusion Rate: Orthopedics

Blood Transfusion: A Growth Industry
Our Demographic Challenge
• Rapidly increasing percentage of population over the age of 65 and decreasing percentage of population between 17 and 65– Decrease in eligible donors– Increase in population that are transfusion recipients– Demand may exceed supply in the near future

Transfusion is expensive!

Between $832 and $1284per unit in the EMHS System
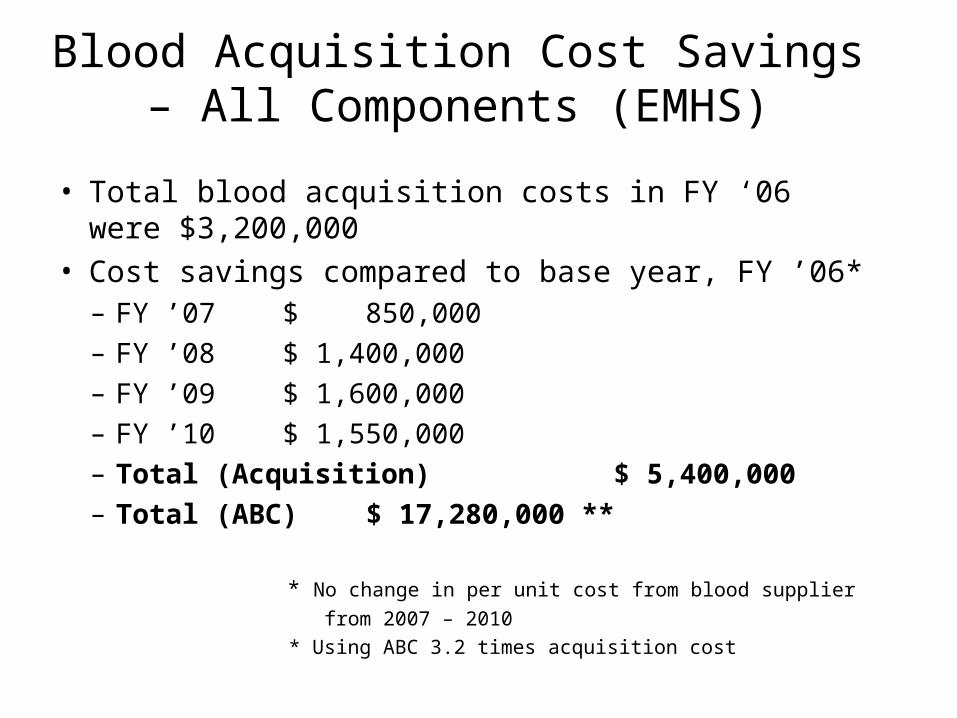
Blood Acquisition Cost Savings – All Components (EMHS)
• Total blood acquisition costs in FY ‘06 were $3,200,000• Cost savings compared to base year, FY ’06*
– FY ’07 $ 850,000– FY ’08 $ 1,400,000– FY ’09 $ 1,600,000– FY ’10 $ 1,550,000– Total (Acquisition) $ 5,400,000– Total (ABC) $ 17,280,000 **
* No change in per unit cost from blood supplier from 2007 – 2010 * Using ABC 3.2 times acquisition cost

The Macroeconomic Burden of Transfusion
• Retrospective cohort study by American College of Medical Quality
• Evaluated all 38.7 million hospitalizations in U.S. in 2004
• Adjusted for age, gender, comorbidities, admission type and DRG
• Charges per transfused patient were $17,194 more than charges for non-transfused, matched patient
• Total excess financial burden: $40 billion
Am J Med Qual 2010;25:289-296
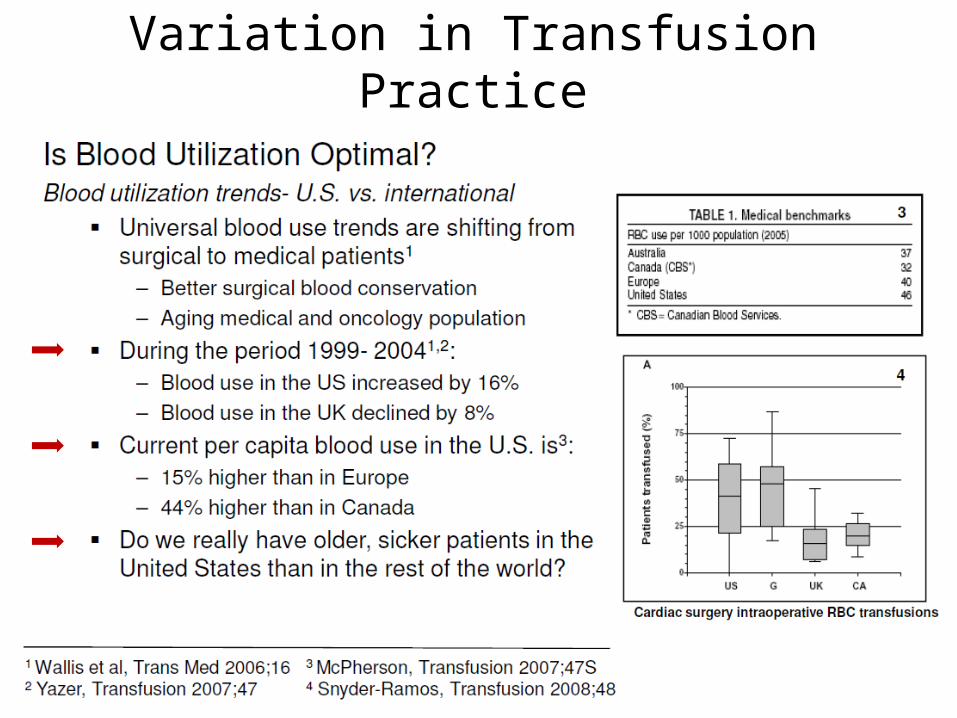
Variation in Transfusion Practice

Observed Variation in Hospital-Specific Transfusion Rates for Primary Isolated CABG Surgery With Cardiopulmonary Bypass
During 2008 (N = 798 Sites)
Bennett-Guerrero, E. et al. JAMA 2010;304:1568-1575.

Are Transfusions Safe: Risk vs. Benefit
• The risks of transfusion are increasingly well defined and extend far beyond concerns about disease transmission (e.g. HIV, hepatitis)
• The benefits of red cell transfusion, except in severe hemorrhage, have never been proven
• While anemia is associated with poorer outcomes, red cell transfusion to treat anemia does not appear to improve outcomes
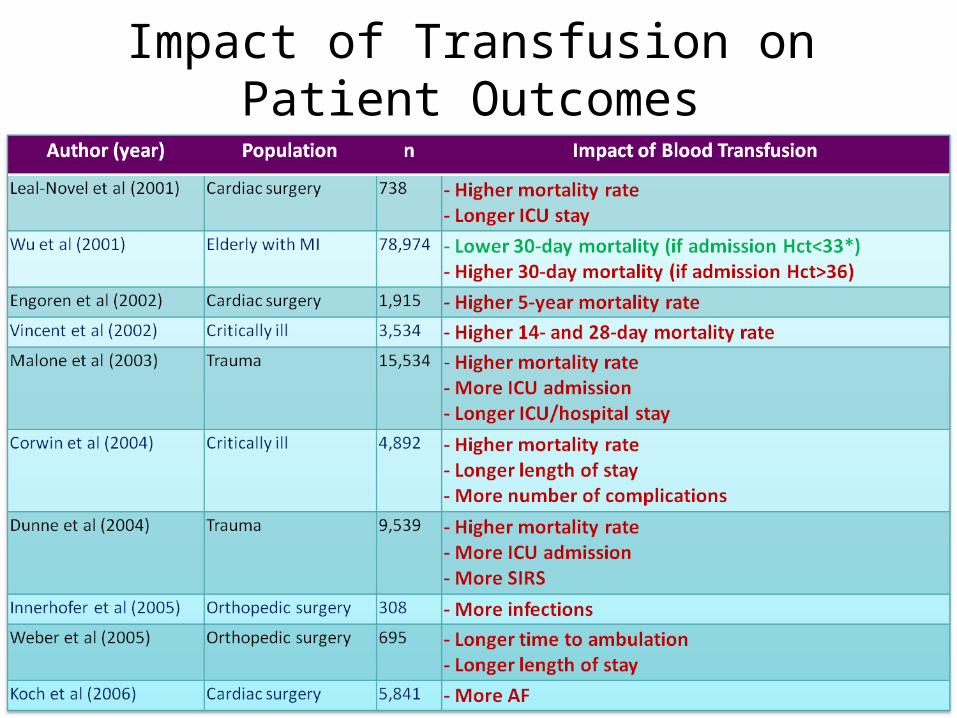
Impact of Transfusion on Patient Outcomes

Impact of Transfusion on Patient Outcomes
Transfusion and Outcomes
• Following transfusion:– In all of the studies, Hb increased– In 79% of the studies, DO2 increased– In 16% of the studies, VO2 increased
– In none of the studies, did ischemia (as measured by lactate) improve
– In all of the studies, transfused patients had poorer outcomes
Efficacy of RBC Transfusion in the Critically Ill
• Meta-analysis - 45 observational studies of 272,596 patients
• Included surgical (trauma, general, ortho, neuro, and cardiac) and general ICU patients
• 42 of 45 studies: risks outweighed benefits of transfusion; risk neutral in 2 studies
• Transfusion a risk factor for increased:• Mortality• Infection• Multi-organ dysfunction• ARDS
Marik, et al CCM 2008;36:2667-2675
Adverse Effects of Allogeneic Blood
• Storage Lesion• TRIM• TRALI: 1 in 2,000 transfusions; primarily
plasma rich products; up to 20% mortality • Hemolytic transfusion rxns: (1:4,000)• Bacterial contamination (Plts.-1:75,000)• HIV, HCV, HBV• Febrile and allergic reactions: 1-2%• Other: ARDS, TA-GVH, SIRS, TACO,TAHA,
unknown viruses
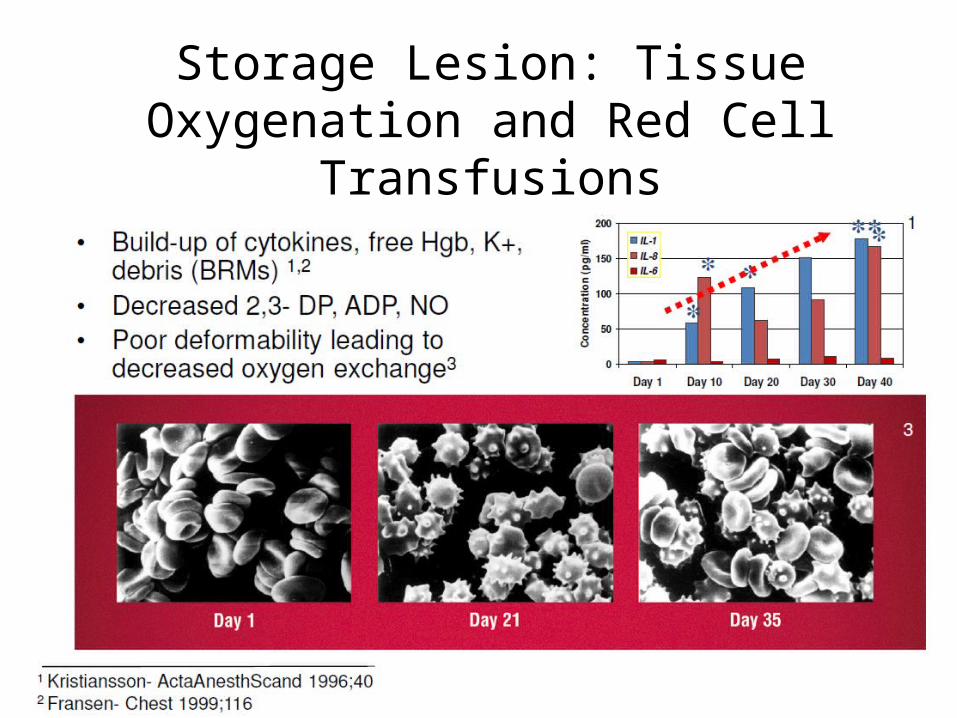
Storage Lesion: Tissue Oxygenation and Red Cell Transfusions

RCTs to Evaluate Red Cell Storage
• Age of Blood Evaluation (ABLE): comparing 8 day old blood vs. standard issue (2-42 days) in ICU patients– Outcome: 90 day all-cause mortality
• Age of Red Blood Cells in Premature Infants (ARIPI): 8 day old blood vs. standard issue– Outcome: 90 day all-cause mortality and organ dysfunction
• Red Cell Storage and Duration and Outcomes in Cardiac Surgery: < 14 day vs. > 20 day old blood– Outcome: Post-op mortality
• Red Cell Storage Duration Study (RECESS): Cardiac surgery patients randomized to < 10 days vs. > 21 day old blood– Outcome: Change in Composite Multi-organ Dysfunction Score
(MODS)
Adverse Effects of Allogeneic Blood
• “Stored RBCs resulted in significantly malperfused and underoxygenated microvasculature “
• May contribute to multi-organ failure• Applies to stored autologous blood
Tsai, A.G. et al. Transfusion 2004;44:1626-34

Transfusion RelatedImmunomodulation (TRIM)
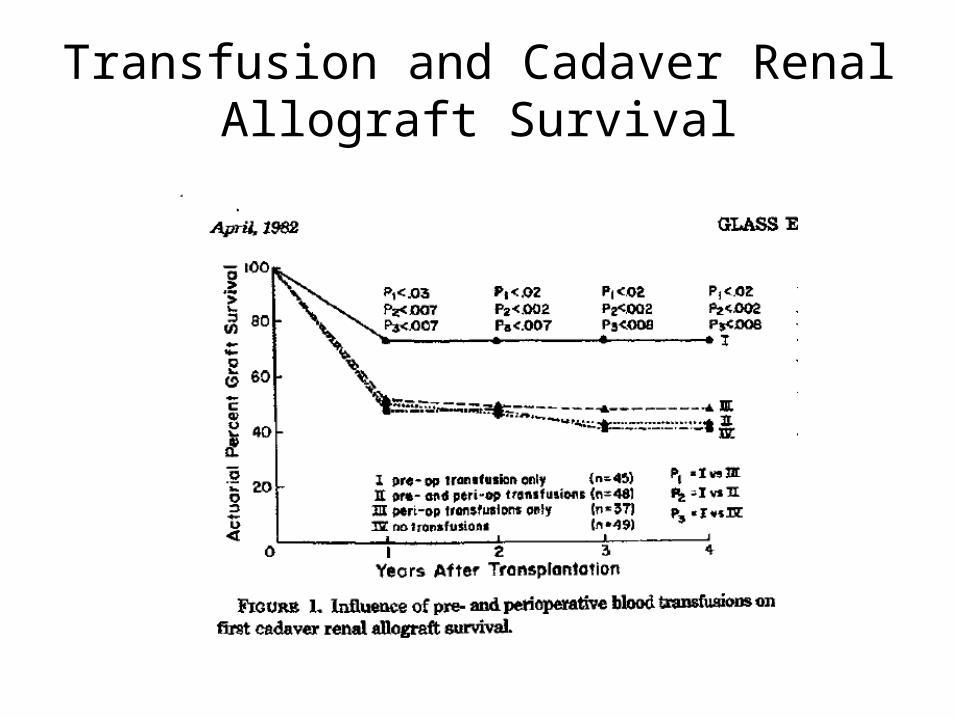
Transfusion and Cadaver Renal Allograft Survival

Transfusion RelatedImmunomodulation (TRIM)
• Improved renal allograft survival
• Increase in nosocomial infection rates leading to increased LOS, resource consumption, total hospital costs
• Increased cancer recurrence rates in transfused patients • Increased long-term mortality in CABG
• A linear dose-response curve of adverse clinical effects is well documented in large studies using multivariate analysis
Nosocomial InfectionsAnd Transfusion

Nosocomial Infection Rates inCritically Ill Patients
7.5
14.3
5.8
0
4
8
12
16
All Patients
Transfused Patients
Non-transfused Patients
Perc
en
t of
Pati
ents
157/2,085 61/428 96/1,657
P < .0001
Taylor RW, et al. Crit Care Med. 2006;34:2302-08.
• Prospective cohort study
• Patients stratified by probability of survival into quartiles
• Lowest quartile for survival: transfusion had no impact on infections
• Highest quartile for survival: transfusion resulted in significant increase on infections

Small Amounts of Intraoperative Blood Loss Heralds Worse Postoperative Outcome
• Database study of NSQIP data with propensity–score matching
• 8728 nonvascular thoracic operations• 6.6 % received one or two units during surgery• After propensity adjustment
– Increased pulmonary complications and LOS– Increased systemic sepsis and wound infections– Composite morbidity 43% vs.32%
Ferraris, et al. Ann Thorac Surg 2011

S. aureus and Iron Surface Determinant (IsdB) .
Lowy FD. N Engl J Med 2011;364:1987-1990.

Transfusion and Mortality

Association Between Blood Transfusion and Risk of Death
Marik, et al CCM 2008;36:2667-2675

Transfusion and Mortality in CABG
• Retrospective study of long-term outcome in 1,915 patients after primary CABG
• Excluded patients who died within 30 days of surgery
• Transfused patients (546) were matched by propensity score (age, gender, size, LOS, perfusion time and STS risk) with pts. not transfused and 5-year mortality compared
• Adjusted 5-year mortality 70% higher in transfused group (p<0.001)
Engoren et al, Ann Thorac Surg 2002;74:1180-6
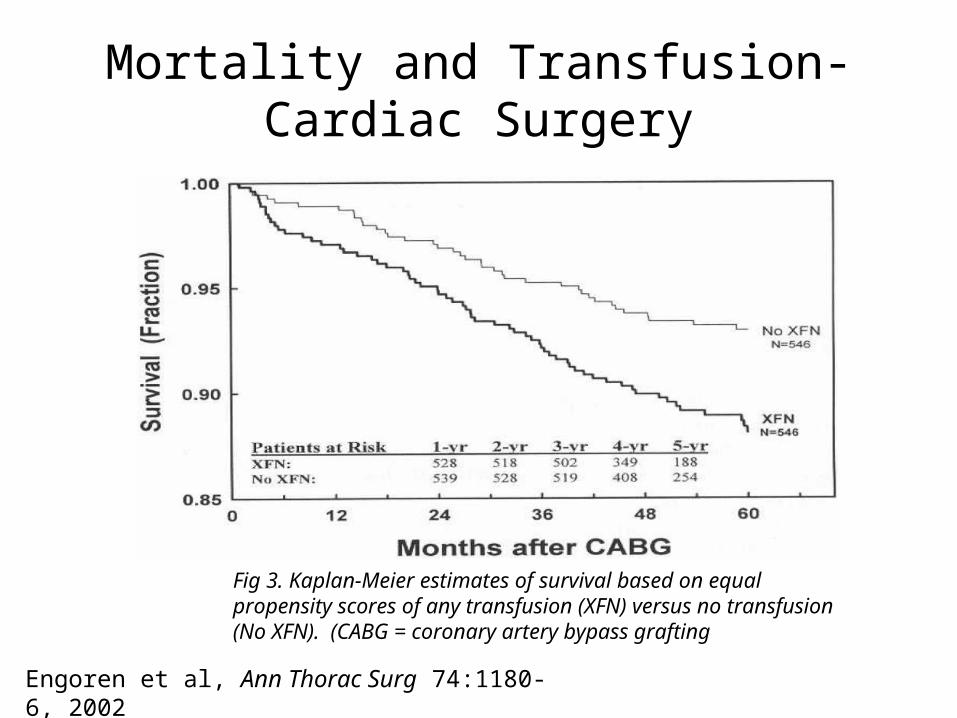
Mortality and Transfusion-Cardiac Surgery
Fig 3. Kaplan-Meier estimates of survival based on equal propensity scores of any transfusion (XFN) versus no transfusion (No XFN). (CABG = coronary artery bypass grafting
Engoren et al, Ann Thorac Surg 74:1180-6, 2002

Transfusion and ARDS
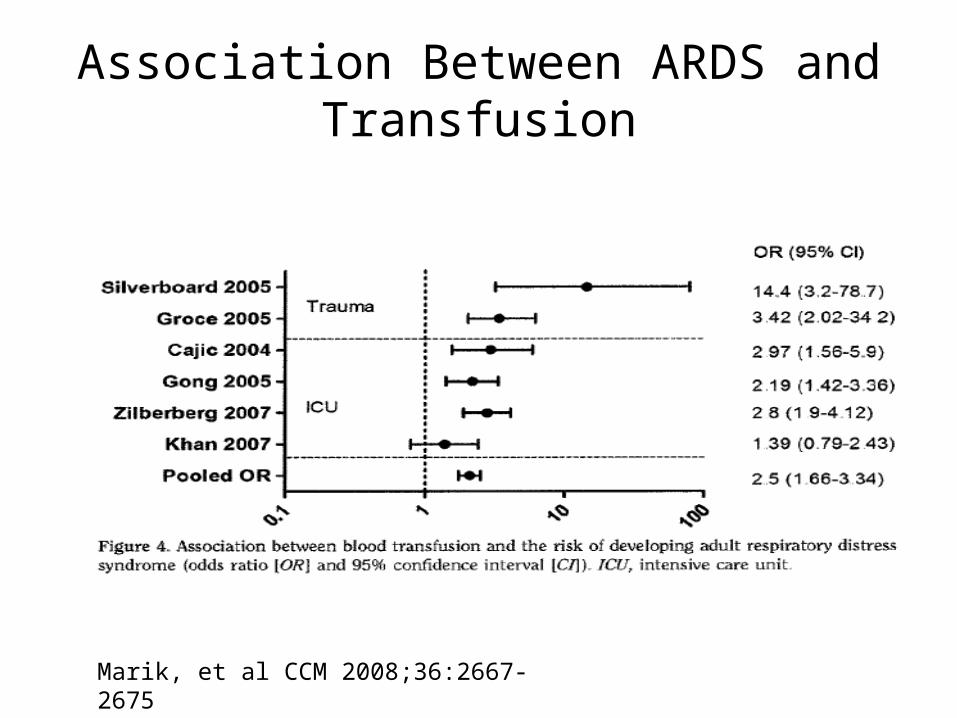
Association Between ARDS and Transfusion
Marik, et al CCM 2008;36:2667-2675

Transfusions in Acute Coronary Syndrome
Blood Transfusion and Clinical Outcomes in Patients with ACS
• Retrospective analysis of 24,112 patients from GUSTO IIb, PURSUIT, and PARAGON B trials
• Main outcome: 30 day mortality• Data adjusted for baseline
characteristics: bleeding, transfusion propensity, nadir hematocrit
• Transfusion was associated with a hazard ratio for death of 3.94 (3.26 – 4.25)
Rao, et al. JAMA, Oct. 6, 2004, Vol 292, No. 13. pp. 1555 -1562

Transfusion and Cancer Survival
Influence of Transfusion on Outcome in Pancreatic Cancer
• 67 patients underwent pancreaticoduodenectomy for cure
• 25 patients received > 3 units• No difference in tumor size, stage,
histology compared to group receiving < 2 units
• Median and cumulative 3 year and 5 year survival worse with > 3 units– 5 year survival 68.9% vs. 30.2% World J Surg, 2008
Influence of Transfusion on Colorectal Cancer Recurrence
• Cochrane meta-analysis involving 12,127 patients
• Evaluated role of transfusion in colorectal cancer recurrence
• Overall OR for recurrence was 1.41 (95% CI 1.20-1.67) in transfused patients
Amato, A, et al. Cochrane Database System Rev 2006;(1): CD005033

Lymphoma and Transfusion
• Meta-analysis of 14 studies– Case control and cohort studies– Outcome reported as relative risk (RR)
• Previous RBC transfusion associated with later development of non-Hodgkin lymphoma, RR 1.2 (95%CI 1.07-1.35, P< .01)
• In subset analysis, risk greatest for development of chronic lymphocytic leukemia/small lymphocytic lymphoma
Castillo, JJ, et al. Blood. 2010;116(16):2897-2907)

Risk vs. Benefit
“The issue (no longer) is whether or not blood transfusion is harmful, but the inflection point at which it is associated with more
harm than benefit.”
-Rao et al, JAMA 2005;292(13)

Blood Product Transfusions
The Traditional Concept• Blood products are an effective
therapeutic intervention
The New Concept• Transfusion of blood products is an
undesirable outcome to be avoided
Goodnough L.T.

“Primum non nocere”(First, Do No Harm)
The accumulating evidence suggests that, when we fail to prevent an avoidable transfusion, we are harming patients.

When to Transfused Red Cells: The Transfusion Threshold


Survival in Patients with Profound Anemia in the Absence of Transfusion
Ford, et al, Blood 2005 106: Abstract 949
Hb Level (gm/dL) Survival
2.5-3.0 6/7 (85.7%)
3.1-4.0 9/11 (81.8%)
4.1-5.0 29/32 (90.6%)
5.1-6.0 30/30 (100%)
6.1-7.0 48/48 (100%)
Overall 122/128 (95.3%)
A prospective, randomized trial comparing a restrictive red cell transfusion strategy vs. a
liberal transfusion strategy
Transfusion in Critical Care: TRICC Trial
Transfusion in Critical Care
• 838 critically ill patients randomized to a restrictive (7-9 g/dl) or liberal (10-12 g/dl) transfusion strategy
• Overall 30 day mortality similar (no transfusion benefit in liberal transfusion group)
• Mortality rates significantly lower in restrictive transfusion group for those with APACHE score < 20 and those < age 55
• No difference in patients with clinically significant heart disease
Hebert. NEJM 1999;340:409-17

The “10/30 Rule” Should be Banished(also the 9/27 rule and 8/24 rule)
No single hemoglobin threshold should be used to make a transfusion decision
No rigid “transfusion trigger” based on hemoglobin alone
But…for most patients, consideration of red cell transfusion should begin at hemoglobin of 7 gm/dl (hematocrit of 21%)
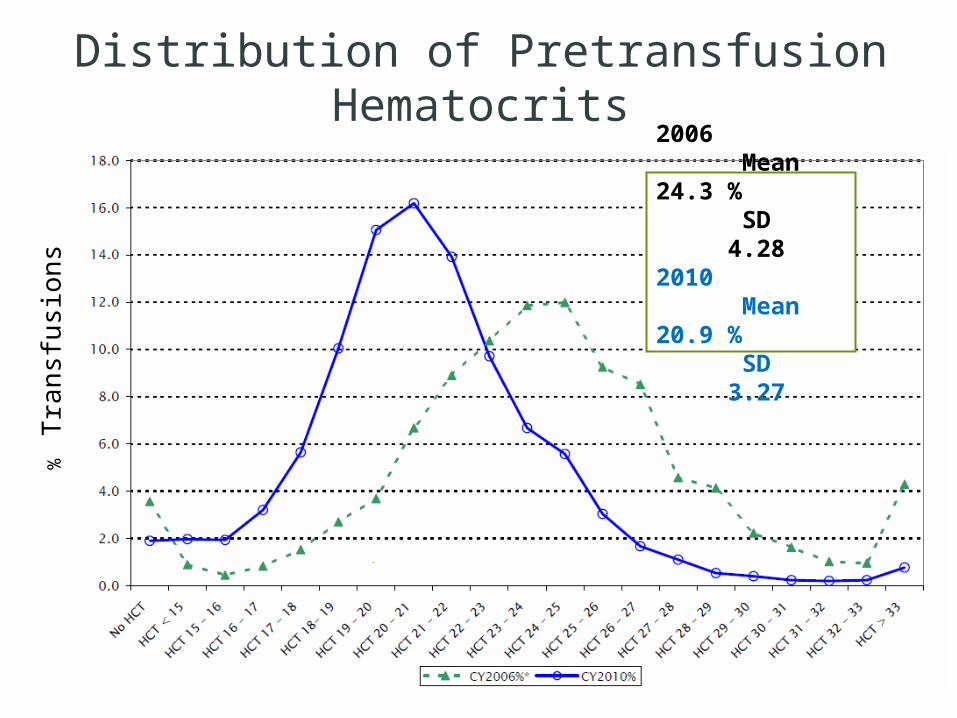
Distribution of Pretransfusion Hematocrits%
Tra
nsfu
sion
s
2006 Mean 24.3 % SD 4.282010 Mean 20.9 % SD 3.27
Red Cells Should Not be Ordered in “Pairs”
For Red Cells:
• Think of a standard dose in the stable patient as one unit
• Each unit should be an independent clinical decision
• Each unit represents an incremental increase in adverse consequences
• Remember: transfusion of red cells may NOT increase oxygen delivery at a tissue level

• Meticulous surgical hemostasis• Meticulous hemostasis with
“bedside” procedures• Minimize phlebotomy blood loss
– Only necessary labs– Smallest sample practical
Reduce Phlebotomy and Procedure-related Blood Losses

Role of Intravenous Iron in Inpatients
• Most inpatients have inflammation and functional iron deficiency (FID)– Chronic inflammatory diseases– Malignancy– Perioperative– Trauma
• Oral iron is poorly tolerated, poorly absorbed, and not bioavailable
• Intravenous iron sucrose may play a role in improving erythropoiesis– There may also be a limited role for ESAs in
inpatients
Conclusions
• Red cell transfusions in patients who are not bleeding and have hemoglobin levels greater than 6-7 g/dL are generally associated with worse outcomes
• The best way to optimize oxygen delivery to the tissues is not by transfusing stored RBCs; instead:– Optimize oxygenation – Optimize hemodynamics
Conclusions
• Even mild anemia contributes to all cause morbidity and mortality and should be evaluated and treated, when possible– Anemia management before elective surgery
helps decrease transfusion rates
• Intravenous iron replacement may be effective at increasing hemoglobin in patients with anemia of chronic inflammation and in patients with an acute inflammatory process
• Limited role for ESAs in inpatients
© Axel Hofmann/Shannon Farmer – SHEF Meeting Perth August 2010
Triad ofIndependent Risk Factors
forAdverse
Outcomes
Triad ofIndependent Risk Factors
forAdverse
Outcomes
Anemia
Blood loss &
bleeding
Transfusion
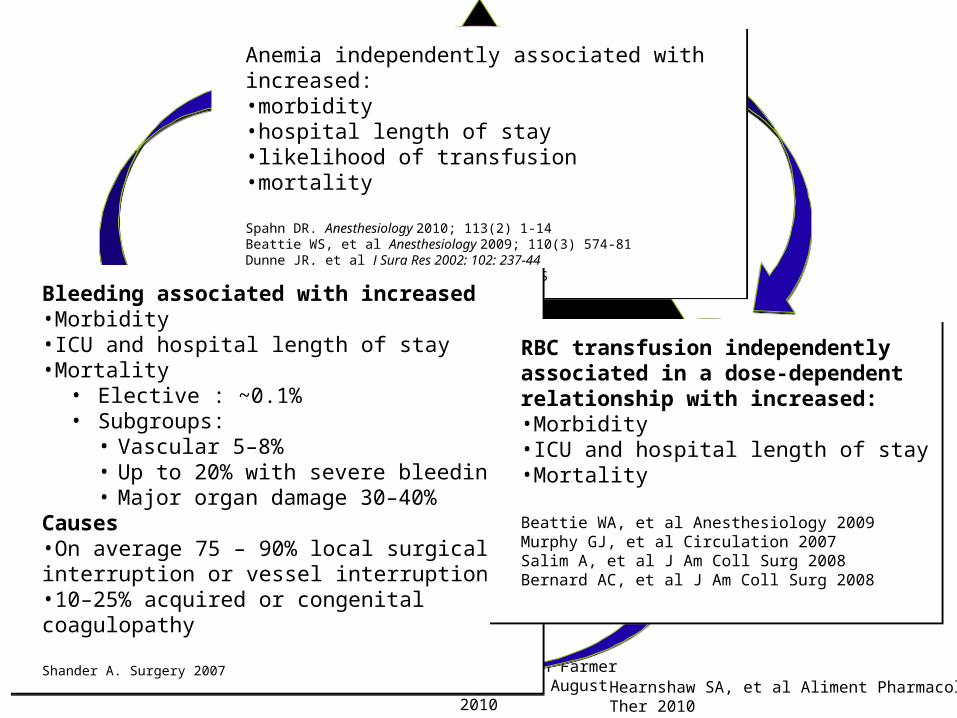
Anemia independently associated with increased: •morbidity •hospital length of stay •likelihood of transfusion •mortality
Spahn DR. Anesthesiology 2010; 113(2) 1-14Beattie WS, et al Anesthesiology 2009; 110(3) 574-81Dunne JR, et al J Surg Res 2002; 102: 237-44Shander A. Am J Med 2004; 116(7A) 58S-69S
Anemia independently associated with increased: •morbidity •hospital length of stay •likelihood of transfusion •mortality
Spahn DR. Anesthesiology 2010; 113(2) 1-14Beattie WS, et al Anesthesiology 2009; 110(3) 574-81Dunne JR, et al J Surg Res 2002; 102: 237-44Shander A. Am J Med 2004; 116(7A) 58S-69S
Bleeding associated with increased•Morbidity•ICU and hospital length of stay•Mortality
• Elective : ~0.1%• Subgroups:
• Vascular 5–8%• Up to 20% with severe bleeding• Major organ damage 30–40%
Causes•On average 75 – 90% local surgical interruption or vessel interruption•10–25% acquired or congenital coagulopathy
Shander A. Surgery 2007
Bleeding associated with increased•Morbidity•ICU and hospital length of stay•Mortality
• Elective : ~0.1%• Subgroups:
• Vascular 5–8%• Up to 20% with severe bleeding• Major organ damage 30–40%
Causes•On average 75 – 90% local surgical interruption or vessel interruption•10–25% acquired or congenital coagulopathy
Shander A. Surgery 2007
RBC transfusion independently associated in a dose-dependent relationship with increased:•Morbidity•ICU and hospital length of stay•Mortality
Beattie WA, et al Anesthesiology 2009Murphy GJ, et al Circulation 2007Salim A, et al J Am Coll Surg 2008Bernard AC, et al J Am Coll Surg 2008
RBC transfusion independently associated in a dose-dependent relationship with increased:•Morbidity•ICU and hospital length of stay•Mortality
Beattie WA, et al Anesthesiology 2009Murphy GJ, et al Circulation 2007Salim A, et al J Am Coll Surg 2008Bernard AC, et al J Am Coll Surg 2008
Hearnshaw SA, et al Aliment Pharmacol Ther 2010Blair SD, et al Br J Surg 1986
So Why Practice Patient Blood Management?
• Higher quality and safety: better patient care
• Lower costs
•“Stewardship” of the blood supply
– Optimal use of blood– Efficient use of resources

© Axel Hofmann/Shannon Farmer – SHEF Meeting Perth August 2010
Optimize Optimize erythro-erythro-poieispoieis
MinimizeMinimizebleeding bleeding & blood & blood
lossloss
Harness & Harness & optimize optimize
physiologiphysiologic c
tolerance tolerance of anemiaof anemia
Patient Blood Management:Patient Blood Management:The Three PillarsThe Three Pillars
• Pre-op anemia screening
• Refer for further evaluation if necessary
• ESAs• Intravenous Iron• Note: anemia is a
contraindication for elective surgery
• Identify and manage bleeding risk and anticoagulants
• ANH• Cell Salvage• DDAVP• TXA, Amicar• Topical hemostatics• Meticulous surgical
hemostasis• Avoid secondary
hemorrhage• Minimize
phlebotomy
• Optimize hemodynamics
• Optimize ventilation and oxygenation
• Low hemoglobin threshold for transfusion
• Minimize oxygen consumption
• Avoid/treat infections promptly

Before I go, a topic for another time
• There is a substantial LACK of evidence that an increased PT/INR (at least < 2.0) can or should be used to make clinical decisions re: benefit of pre-procedure frozen plasma
• Avoid prophylactic plasma transfusions– No proven clinical benefit– Substantial risk of acute pulmonary reactions

“Levels” of Evidence
Thank You!

Patient Blood Management (PBM) is the timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin concentration,
optimize hemostasis and minimize blood loss in an effort to improve patient
outcome.
Please join the Society for the Advancement of Blood Management
SABM.org


Figure 1. A, ORs for TE (396 cases, 1581 controls) and ICH (164 cases, 656 controls) by INR level in adults with nonvalvular AF, with 8 INR categories using INR 2.0 to 2.5 as the referent.
Singer D E et al. Circ Cardiovasc Qual Outcomes 2009;2:297-304
Copyright © American Heart Association






![Traceability of Blood Transfusions and Reporting of ...downloads.hindawi.com/journals/ah/2018/7938130.pdf · delayed transfusion reactions and transfusion-transmitted infectionsfortherecipient[].erefore,itisnecessaryfor](https://static.documents.pub/doc/80x56/601aea8dd1735d5b275f22d0/traceability-of-blood-transfusions-and-reporting-of-delayed-transfusion-reactions.jpg)










