World Health Organization Western Pacific Region REVIEW OF THE DISEASE BURDEN OF HAEMOPHILUS INFLUENZAE TYPE B (Hib), AND THE USE AND COST-EFFECTIVENESS OF Hib VACCINATION IN THE WESTERN PACIFIC REGION Manila, Philippines October 2006
Transcript
World Health Organization Western Pacific Region
REVIEW OF THE DISEASE BURDEN OF HAEMOPHILUS INFLUENZAE TYPE B (Hib), AND THE USE AND COST-EFFECTIVENESS OF Hib VACCINATION IN THE
1.1 Sociogeographical context of the Western Pacific Region and the categorization of its countries.......................................................................................................................... 2
2. METHODS ............................................................................................................................... 7 2.1 Literature search.............................................................................................................. 7 2.2 Information abstraction ................................................................................................... 8 2.3 Terminology.................................................................................................................... 8
3. RESULTS ................................................................................................................................. 9 3.1 Disease burden of Hib in the Western Pacific Region.................................................... 9 3.2 Hib vaccination status in the Western Pacific Region ...................................................24 3.3 Impact of Hib vaccination in the Western Pacific Region.............................................27 3.4 Economic evaluation of Hib immunization in the Western Pacific Region...................28
5.1 Recommendations for individual countries ...................................................................39 6. ACKNOWLEDGEMENTS.....................................................................................................39
- iii -
ANNEXES
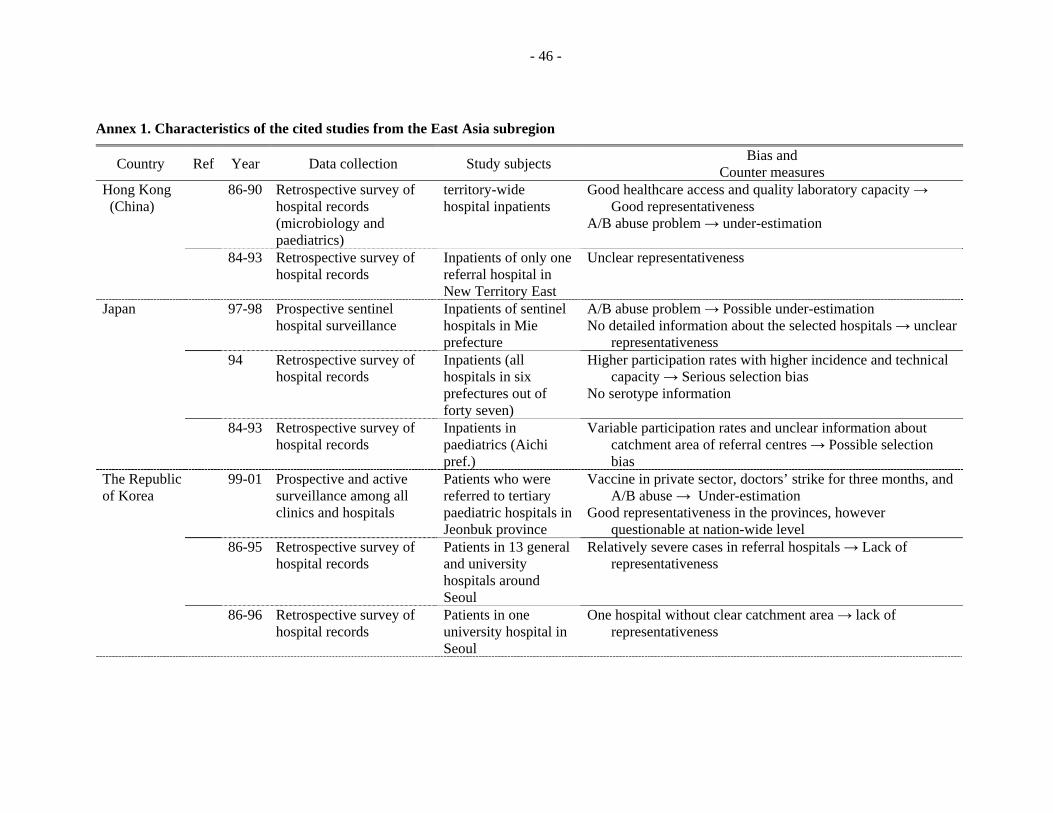
ANNEX 1 - CHARACTERISTICS OF THE CITED STUDIES FROM THE EAST ASIA SUBREGION
ANNEX 2 - CHARACTERISTICS OF THE CITED STUDIES FROM THE OCEANIA SUBREGION
FIGURES
FIGURE 1 - MAP OF THE WESTERN PACIFIC REGION
FIGURE 2 - RELATIONSHIP BETWEEN HIB MENINGITIS AND INFANT MORTAILITY IN THE WESTERN PACIFIC REGION
TABLES
TABLE 1 - SELECTED SOCIODEMOGRAPHIC, HEALTH, IMMUNIZATION COVERAGE AND HIB DATA AVAILABILITY INDICATORS FOR COUNTRIES AND AREAS IN THE WESTERN PACIFIC REGION
TABLE 2 - PRELIMINARY RESULTS OF LITERATURE SEARCH
TABLE 3 - HIB DISEASE BURDEN IN THE EAST ASIA SUBREGION
TABLE 4 - HIB MENINGITIS IN THE OCEANIA REGION
TABLE 5 - HAEMOPHILUS INFLUENZAE TYPE B VACCINES
TABLE 6 - HIB VACCINATION STATUS AND COVERAGE RATE BY COUNTRY
TABLE 7 - KEY LITERATURE ON ECONOMIC EVALUATION OF HIB VACCINE ACROSS WHO REGIONS
TABLE 8 - MAJOR ASSUMPTIONS AND FINDINGS OF MILLER'S MODEL FOR THE WESTERN PACIFIC REGION (UNIT: US$ IN 1997)
TABLE 9 - MAJOR FINDINGS IN AUSTRALIAN STUDIES (UNIT: AUD, 1 US$ = 1.46 AUD IN 1994)
TABLE 10 - MAJOR FINDINGS OF LIMCANGCO'S COST-EFFECTIVENESS MODEL IN THE PHILIPPINES (UNIT: PHP IN 1998, 1 US$ = 35 PHP)
TABLE 11 - MAJOR FINDINGS OF BRINSMEAD'S STUDY IN TONGA (US$ 1 = 2 TOP, 2002)
TABLE 12 - MAJOR FINDINGS OF ECONOMIC EVALUATION FOR HIB IMMUNIZATION ACROSS REGIONS
TABLE 13 - SENSITIVITY ANALYSIS UNDER DIFFERENT ASSUMPTIONS ABOUT HIB INCIDENCE
TABLE 14 - SUMMARY OF COST-BENEFIT ANALYSES ACROSS REGIONS
GAVI Global Alliance for Vaccines and Immunization
GNP gross national product
HbOC Haemophilus b oligosaccharide conjugate vaccine
Hib Haemophilus influenzae type b
NIP National Immunization Programme
NR no response (or no data available)
NNDSS National Notifiable Diseases Surveillance System
PRP polyribosyl ribitol phosphate
PRP-D PRP–diphtheria toxoid conjugated vaccine
PRP-T PRP–tetanus toxoid conjugated vaccine
PRP-OMP PRP–outer membrane protein conjugate vaccine
QALY quality-adjusted life year
RAT rapid assessment tool
SQ sequelae, a morbid condition occurring as a consequence of another condition.
- v -
EXECUTIVE SUMMARY
This study aims to critically review and analyse the disease burden due to Haemophilus influenzae type b (Hib), based on existing studies. It also reviews studies on the impact of the Hib vaccine on child morbidity and mortality, and on the cost-effectiveness of mass vaccination of the eligible population in the Western Pacific Region. In addition, it examines current vaccination policies in the Western Pacific Region for Hib, including the types of vaccines used and vaccination schedules.
Methods used for the review include: (1) review of all published and accessible unpublished literature on Hib, including communications from experts; and (2) comparison of economic evaluation studies across regions and a sensitivity analysis for different disease burden scenarios.
Review of existing studies reveals significant variation in disease burden due to Hib among subregions and countries in the Western Pacific Region. Acknowledging the limited number of studies and their methodological limitations, the incidence of Hib meningitis in the East Asia subregion, comprising 13 countries and areas, is estimated to be lower than 40 per 100 000 under-5 population, except in the Philippines. In the Oceania subregion, comprising 24 countries and areas, Australia, French Polynesia and New Zealand show similar rates of Hib meningitis incidence, at about 30 per 100 000 under-5 population. Data generated from a rapid assessment tool (RAT) in the Pacific island countries and areas suggests a higher incidence, from 50 to 84 per 100 000 under-5 population. Regarding Hib vaccination, 23 out of 37 countries and areas in the Western Pacific Region have introduced the vaccine and 18 countries have incorporated it into their routine immunization programmes, with two more countries planning to do so in 2007. Three countries (Australia, Fiji and New Zealand) with data on the impact of Hib vaccination have reported a dramatic decrease in Hib incidence following introduction of the vaccination. The cost–benefit ratio of universal Hib immunization in the Western Pacific Region seems to be lower than observed in the WHO Region of the Americas or the WHO European Region, mainly because of relatively lower incidence.
Seventeen countries and areas have no data on Hib disease burden, though some have introduced Hib vaccination (e.g. Brunei Darussalam). Many of the available disease burden data in the Region are based on hospital-based or retrospective studies, with only seven out of 40 studies on Hib disease burden being community-based prospective studies. In order to decide whether or not to introduce Hib vaccination, and to evaluate the economic value or impact of immunization, well-designed studies using innovative methodologies should be carried out to assess the Hib disease burden and the cost-effectiveness of vaccination with minimum resources and time.
1. INTRODUCTION
Haemophilus influenzae type b bacteria (Hib) cause invasive diseases such as meningitis, pneumonia, septicaemia, epiglottitis, cellulitis, septic arthritis and osteomyelitis, mainly among children under five years of age. Hib was documented to be a leading cause of morbidity and mortality among children in developed countries in the pre-vaccination era. The introduction of effective Hib conjugate vaccines in national immunization programmes in the early 1990s in many developed countries led to a considerable decline in Hib-related morbidity and mortality in those countries
1.
Yet, despite its demonstrated impact in reducing the burden of Hib disease, conjugate Hib vaccines have not been taken up in all countries. By 1997, 15 years after Hib conjugate vaccines became available, only 25 industrialized countries and a few developing countries (e.g. Chile) were using them. At the end of 2005, 92 countries (out of 192 WHO Member States), accounting for only 20% of the global under-5 population had included the vaccine in their immunization schedules. Only 21 out of 72 of the world’s poorest countries (eligible for Global Alliance for Vaccines and Immunization [GAVI] funding) were using or planning to use Hib vaccine by early 2006. In the Western Pacific Region, as of September 2006, 18 out of the 37 countries and areas, accounting for only 3.4% of the total regional population, had included Hib vaccination in their routine immunization schedules. A disproportionate share of developing countries have yet to adopt Hib immunization into their national infant immunization schedules, partly due to a lack of conclusive evidence on the disease burden and partly due to the relatively high price of the vaccine. In addition, other factors, including the perceived severity of the disease and costs associated with the treatment of the illness play a role in determining the introduction of Hib vaccines
2. WHO currently recommends that Hib conjugate vaccines be included in national
immunization schedules in all countries where resources permit their use, and where justified on the basis of disease burden
3. WHO’s Strategic Advisory Group of Experts, in November 2005,
strongly recommended global implementation of Hib vaccination—unless robust epidemiological evidence exists of low disease burden, lack of benefit or overwhelming impediments to implementation
4.
A review of Hib studies by Bennett and others (2002) illustrates the discrepancy between developed and developing countries regarding Hib data
5. Although several studies have been
completed in developed countries, only limited data are available from developing countries, especially in Africa and Asia, including the Western Pacific Region.
1 Peltola H. Worldwide Haemophilus influenzae type b disease at the beginning of the 21st century: global analysis of
the disease burden 25 years after the use of the polysaccharide vaccine and a decade after the advent of conjugates. Clinical Microbiology Reviews, 2000, 13(2):302-317. 2 Bennett JV, et al. Haemophilus influenzae type b (Hib) meningitis in the pre-vaccine era: a global review of
incidence, age distributions, and case-fatality rates. Geneva, World Health Organization, 2002. 3 WHO position paper on Haemophilus influenzae type b conjugate vaccines. Weekly Epidemiological Record, 1998,
73(10):64-68. 4 World Health Organization. Conclusions and recommendations from the Immunization Strategic Advisory Group.
Weekly Epidemiological Record, 2006:81(1):2-11. 5 Bennett JV, et al. Op cit. Ref 2.
- 2 -
Building on the insights provided by earlier review studies, this study critically reviews and summarizes data from studies conducted in the Western Pacific Region on the Hib disease burden and the impact and cost-effectiveness of vaccination, with particular emphasis on studies conducted between 2000 and 2005. The report is intended to provide policy-makers with background information and evidence on Hib disease and to identify areas where additional data may be needed in their countries in order to guide their decision-making regarding the vaccine.
1.1 Sociogeographical context of the Western Pacific Region and the categorization of its countries
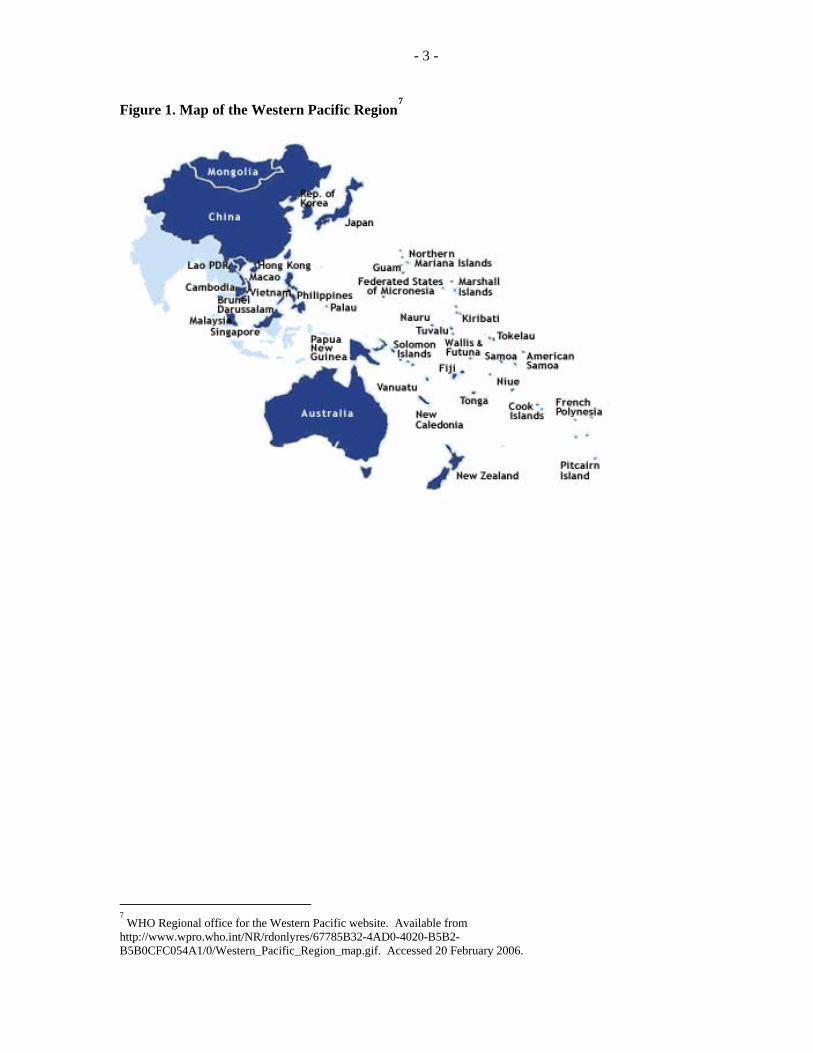
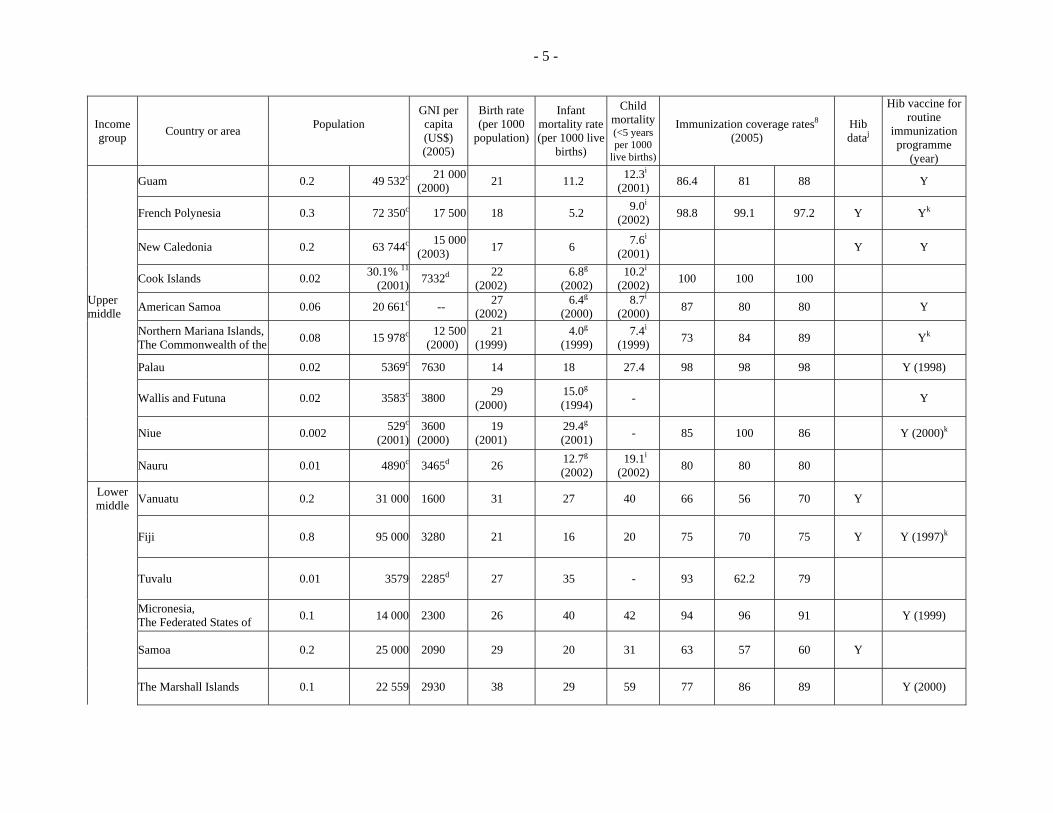
There are 37 countries and areas in the WHO Western Pacific Region (Figure 1), with a total population of more than 1.7 billion, accounting for about 28.7% of the world’s population. The under-5 population ranges from just 13 000 in Tonga to 92.5 million in China. The infant mortality rate, closely associated with level of economic development, ranges from three per 1000 live births in Japan and Singapore to 85 per 1000 in the Lao People’s Democratic Republic. Except for nine countries and areas [Australia, Brunei Darussalam, Hong Kong (China), Japan, Macao (China), Malaysia, New Zealand, the Republic of Korea and Singapore] and some Pacific countries and areas (American Samoa, Guam, French Polynesia, New Caledonia, Northern Marianna Islands and Palau), most countries were categorized as low-income or lower-middle-income countries by the World Bank in 2006
6.
For the sake of data presentation, the countries and areas are organized into two groups, based on their geographical location:
(1) East Asia (13 countries and areas): Brunei Darussalam, Cambodia, China, Hong Kong (China), Japan, the Lao People’s Democratic Republic, Macao (China), Malaysia, Mongolia, the Philippines, the Republic of Korea, Singapore, and Viet Nam;
(2) Oceania (24 countries and areas): American Samoa, Australia, Cook Islands, Fiji, French Polynesia, Guam, Kiribati, the Marshall Islands, the Federated States of Micronesia, Nauru, New Caledonia, New Zealand, Niue, the Commonwealth of the Northern Mariana Islands, Palau, Papua New Guinea, the Pitcairn Islands, Samoa, Solomon Islands, Tokelau, Tonga, Tuvalu, Vanuatu, and Wallis and Futuna.
In addition, countries are again categorized by the World Country Classification System, which uses 2005 gross national income (GNI) per capita (in US$) calculated using the World Bank Atlas method6: (1) low-income: US$ 875 or less; (2) lower-middle: US$ 876–US$ 3465; (3) upper-middle: US$ 3466–US$ 10 725; (4) high: US$ 10 726 or more. Table 1 presents the basic sociodemographic data for countries and areas in the Western Pacific Region.
6 http://siteresources.worldbank.org/DATASTATISTICS/Resources/CLASS.XLS, as accessed in September 2006.
- 3 -
Figure 1. Map of the Western Pacific Region7
7 WHO Regional office for the Western Pacific website. Available from
http://www.wpro.who.int/NR/rdonlyres/67785B32-4AD0-4020-B5B2-B5B0CFC054A1/0/Western_Pacific_Region_map.gif. Accessed 20 February 2006.
- 4 -
Table 1. Selected sociodemographic, health, immunization coverage, and Hib data availability indicators for countries and areas in the Western Pacific Region, 2006
Income group Country or area Population
GNI per capita (US$)
(2005)
Birth rate (per 1000
population)
Infant mortality rate (per 1000 live
births)
Child mortality(<5 years per 1000
live births)
Immunization coverage rates8
(2005) Hib dataj
Hib vaccine for routine
immunization programme
(year)
East Asia Total
(mid-2006) (million)
0–4 yearsb
(2003) 2005 2005 DPT3 Measles Hepatitis B
High Hong Kong (China) 7.0 953 023c 27 670 8 2.4 3.2i
(2002) 95 95 95 Y
Japan 127.8 5 947 000 38 980 9 2.8 4 Y
Singapore 4.5 242 000 27 490 10 2.1 3 96 96 96 Y
Brunei Darussalam 0.4 39 000 --- 20 9 10.0i
(2002) 107.7 97.4 99.8 Y (2003)
The Republic of Korea 48.5 2 932 000 15 830 9 5 6 96.1 99.9 99 Y
Macao (China) 0.5 83 605c ---- 8 3 1.6i
(2003) 92.2 90.9 87.5
Upper middle Malaysia 26.9 2 714 000 4960 20 10 12 95.3 88.4 91.5 Y Y (2002)
Lower middle China 1311.4 92 555 000 1740 12 27 31 86.5 86.2 84.3 Y
The Philippines 86.3 9 758 000 1300 27 27 34 79 82 44 Y
Sources of Data: Total population, birth rate, infant mortality rate: 2006 World Population Data Sheet. Washington DC, Population reference Bureau. Gross national Income, under-5 mortality: World Development Indicators database. Washington DC, World Bank, Washington DC, 1 July, 2006, except the italicized
figures and data on under-5 population, which are taken from World Factbook, 2005. Washington DC, Central Intelligence Agency (http://www.cia.gov/cia/publications/factbook/, accessed 4 May 2005).
Immunization coverage rates: Joint Reporting Forms, as reported by countries to the WHO Western Pacific Regional Office in April 2006. EDITOR’S NOTE: Where are keys for b and c ?
b WHO vaccine-preventable disease monitoring system, 2004 global summary. Geneva, World Health Organization, WHO, 2004 (http://www.who.int/vaccines-documents/GlobalSummary/GlobalSummary.pdf, accessed 7 March, 2005).
c The World Factbook, 2005 (2005 estimate for 0-14 years). Washington, DC, Central Intelligence Agency (http://www.cia.gov/cia/publications/factbook/, accessed 4 May 2005).
d Social indicators. New York, NY, United Nations Statistical Division, 2003 (http://unstats.un.org/unsd/demographic/products/socind/inc-eco.htm, accessed: 9 March, 2005. e 2003 GNP per capita (US$). Manila, WHO, 2003 (http://www.wpro.who.int, accessed 4 May 2005). f Asia-Pacific in Figures. United Nations Economic and Social Commission for Asia and the Pacific, 2004 (http://www.unescap.org/stat/data/apif/index.asp, accessed 6 March 2005). g Millennium Indicator: Infant mortality rate (0-1 year) per 1,000 live births (UNICEF estimates). New York, NY, United Nations Statistical Division (http://millenniumindicators.un.org/unsd/mi/mi_series_results.asp?rowId=563, accessed 7 March 2005). h Health Indicators. Manila, WHO, 2004 (http://www.wpro.who.int/information_sources/databases/health_indicators/; accessed 4 May 2005). i Mortality rate by age group (under 5 years). (http://kosis.nso.go.kr/cgi-bin/sws_999.cgi, accessed 4 May 2005). j Data availability of Hib disease burden in this study: Y = epidemiologic data available. k Not entire country. l No profile available except total population.
- 7 -
2. METHODS
2.1 Literature search
The PubMed database was used to search studies on “Haemophilus” from 1980 to the end of December 2005. The search covered “all languages” and was categorized by country and subregion (i.e. “Asia” and “Pacific islands”).
The number of articles identified in the search is shown in the upper row of Table 2. After examining the titles and abstracts, the articles that were irrelevant to Hib per se were excluded (N=176), including those dealing with clinical information such as diagnostic methods, antibiotics susceptibility, vaccine development and bacteriology, etc. (see the lower row of Table 2). In order to avoid missing any epidemiological study, the database was searched again using the Mesh Browser with the Mesh Keyword “Haemophilus influenzae type b—epidemiology” under the “all language” option.
After examining all available abstracts, only papers relevant to the Western Pacific Region concerning Hib disease burden, economic analysis, and Hib vaccination impact were selected. In addition, various experts were contacted personally to obtain unpublished information.
Table 2. Preliminary results of literature search Category Medical literature identified in PubMed as of December 2005, ranked by results
(number of papers) Countries a Japan (204)
Australia (159) China (49) Papua New Guinea (36) New Zealand (34) Hong Kong (China) (32) Solomon Islands (32) The Philippines (24) Singapore (17) Korea, Republic of (16) Malaysia (11) Viet Nam (7) Vanuatu (4) Cook Islands (3) French Polynesia (3) Niue (3) Tokelau (3) Fiji (1) New Caledonia (1)
American Samoa (0) Brunei Darussalam (0) Cambodia (0) Guam (0) Kiribati (0) The Lao People’s Democratic Republic (0) Macao (China) (0) The Marshall Islands (0) Micronesia, the Federated States of (0) Mongolia (0) Northern Mariana Islands, The Commonwealth of the (0) Nauru (0) Palau (0) The Pitcairn Islands (0) Samoa (0) Tonga (0) Tuvalu (0) Wallis and Futuna (0) * Asia (463), Pacific islands (60)
a Search condition: "Haemophilus" + the name of country under the option of all languages, and between 1980 and December 2005.
- 8 -
2.2 Information abstraction
The information on Hib disease burden was systematically abstracted by: (1) the time/duration of data collection, (2) study design and setting, (3) incidence, (4) case fatality and sequelae, and (5) other notable information. Whenever available, information regarding the age distribution of Hib disease and the proportion of bacterial meningitis caused by Hib was also extracted.
To examine the economic impact of Hib disease, the authors reviewed published papers as well as one unpublished paper containing data on the cost-effectiveness of Hib vaccination for countries in the Western Pacific Region. Sensitivity analysis on cost-effectiveness was carried out for different disease and vaccine price scenarios. Each study was evaluated for the internal and external validity of the data presented. The quality of the studies is discussed in the discussion section and in Annexes 1 and 2.
2.3 Terminology
“Incidence” is defined as the annual number of Hib meningitis cases per 100 000 children under five years of age, unless and until specified otherwise. The term “case fatality rate” represents the percentage of Hib cases resulting in death due to Hib conditions. The term “sequelae rate” refers to the percentage of Hib cases that develop residual neurological manifestations.
Studies included in the review were classified by the following data collection methods:
(1) Hospital-based (H) or community-based (C): Studies that provided incidence data were classified as community-based (C) even if case detection occurred at the hospital level, but included all hospitals in a given catchment area that might provide care for meningitis patients. However, studies that provided information only on the proportion of meningitis or pneumonia cases due to different etiologies admitted in a particular health facility, with no data on disease incidence, were classified as hospital-based (H).
(2) Prospective (P) or retrospective (R): Studies were further classified as prospective (P) if the study population was enrolled on a prospective basis starting from a point of time forward, or retrospective (R) if the study population was enrolled based on existing hospital records for a specified time period in the past.
Studies using the rapid assessment tool (RAT) were designated as “retrospective”. RAT is an alternative data collection method that provides estimates of Hib disease burden in a relatively short time by analysis of existing retrospective data for the number of meningitis and pneumonia cases and deaths in children under five years of age that may be attributable to Hib infection. RAT uses two different methods: the meningitis incidence rate method and the under-5 mortality rate method. The meningitis incidence rate method uses a local estimate of Hib meningitis incidence based on fresh analysis of retrospective data from a hospital or directly from other local studies conducted in the past to estimate the national burden of total Hib disease. The under-5 mortality rate method uses the proportion of childhood deaths from acute lower respiratory infection (ALRI) attributable to Hib, as calculated by applying a factor of 13% as the percentage of deaths due to Hib to the total number of under-5 deaths due to ALRI, minus the neonatal
- 9 -
deaths unlikely to be due to Hib infection8. Backward calculations are then done to estimate the
total number of Hib pneumonia and meningitis cases based on estimated case fatality rates for Hib meningitis and Hib pneumonia.
Cost-benefit ratio is used as a measure of cost-effectiveness of the vaccination programme and is calculated by dividing total monetary value of benefits of the vaccination programme by the total monetary cost of vaccination.
3. RESULTS
The results are presented in four sections—on disease burden, vaccination status, impact of vaccination programme and the evidence on cost-effectiveness.
3.1 Disease burden of Hib in the Western Pacific Region
Eight countries and areas—Brunei Darussalam, Cambodia, Cook Islands, the Lao People’s Democratic Republic, Macao (China), Nauru, Tokelau and Tuvalu—lack any information on Hib epidemiology (Table 2) In general, the less developed a country, the less likely it is to have any data on Hib disease burden, although there are some exceptions (Table 2).
3.1.1 East Asia subregion
Previous review studies estimated that Hib accounted for an average of 42.4% (39.2%–45.6%) and 34%
9,10 of the total meningitis cases of known etiology at the global level and in
Asia, respectively. Review of individual studies from the Western Pacific Region shows that the proportion of Hib meningitis out of the total bacterial meningitis cases ranges from 18.4% in Singapore to 62% in the Republic of Korea
11,12. Despite several studies pointing out the low rate
of positive culture, partly due to the high levels of antibiotics used prior to taking the sample, almost all studies note Hib to be the dominant organism causing bacterial meningitis among children under five years of age
13,14,15,16,17. This is corroborated by recent studies in Bangladesh,
8 Estimating the local burden of Haemophilus influenzae type b (Hib) disease preventable by vaccination: A rapid
assessment tool. Geneva, World Health Organization, WHO. http://www.who.int/vaccines-documents/. 9 Bennett JV, et al. Op cit. Ref 2.
10 Peltola H. Spectrum and burden of severe Haemophilus influenzae type b diseases in Asia. Bulletin of the World
Health Organization, 1999, 77(11):878-887. 11
Lee YS, et al. Invasive Haemophilus influenzae type b infections in Singapore children: a hospital-based study. Journal of Paediatrics and Child Health, 2000, 36(2):125-127. 12
Lee HJ. Epidemiology of systemic Haemophilus influenzae disease in Korean children. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S185-189. 13
Lee YS, et al. Op cit. Ref. 11. 14
Kim JS et al. Incidence of Haemophilus influenzae type b and other invasive diseases in South Korean children. Vaccine, 2004; 22(29-30):3952-3962. 15
Shao PL, et al. Epidemiology of Haemophilus influenzae type b meningitis in Taiwan, 1997 and 2000. Journal of Microbiology, Immunology, and Infection, 2004, 37(3):164-168. 16
Wang YJ, et al. Relative frequency of Haemophilus influenzae type b pneumonia in Chinese children as evidenced by serology. Pediatric Infectious Disease Journal, 2002,, 21(4):271-277.
- 10 -
Indonesia and other Asian countries that point out that the incidence of Hib meningitis is greater than what can be measured through laboratory-based surveillance because preclinical (delayed contact, use of antibiotics) and clinical (rate of lumbar puncture, specimen handling) factors can affect laboratory-based surveillance sensitivity
18.
Peltola estimated that the overall incidence of Hib meningitis in Asia is 25 per 100 000 under-5 population, and pointed out that there are large variations among Asian countries
19.
Studies in high-income countries have found a lower incidence of Hib meningitis, ranging from 1.1 cases per 100 000 under-5 population in Hong Kong (China)
20 to 6.1 per 100 000 under-5
population in Japan21
. These estimates are much lower than for Europe or for the United States of America in the pre-vaccine era (23 and 53 per 100 000 under-5 population, respectively). However, studies from middle- and low-income countries in East Asia show relatively higher incidence rates. The incidence rate for Hib meningitis was estimated to be 38 per 100 000 under-5 population in Malaysia
22; and 32 per 100 000 under-5 population in Mongolia
23.
One study in Manila, the capital city of the Philippines, estimated Hib meningitis incidence to be as high as 95 per 100 000 under-5 population (95% CI: 76.5%-106.3%)
24. Given this wide range
of Hib meningitis incidence in countries of East Asia, it is difficult and impractical to make a single estimate for Hib disease burden or to make recommendations for Hib vaccine for the subregion as a whole.
Case fatality rate and sequelae rate
At the global level, the case fatality rate of Hib meningitis is estimated to be 28%, with wide differentials between developed (5%) and developing regions (30%)
25. A review of Hib
meningitis data from 14 countries in Asia, including six countries and areas in the Western Pacific Region concluded that the case fatality rate was 25%, with a residual sequelae rate of 30%
26. In this review of studies, the case fatality rate ranged from 0% in Taiwan (China) to
44.4% in Malaysia, with relatively lower case fatality rates in high-income countries.
17
Yang Y, et al. Study on Haemophilus influenzae type b diseases in China: the past, present and future. Pediatric Infectious Disease Journal , 1998, 17(9 Suppl):S159-165. 18
Review panel on Haemophilius influenzae type b disease burden in Bangladesh, Indonesia, and other Asian countries, Bangkok, 28-29 January 2004. Weekly Epidemiological Record. Geneva, World Health Organization, 2004, 79(18):173-180. Available from: http://www.who.int/wer. 19
Peltola H. Op cit Ref 1. 20
Sung RY et al. Meningitis in Hong Kong children, with special reference to the infrequency of haemophilus and meningococcal infection. Journal of Paediatrics and Child Health, 1997, 33(4):296-299. 21
Nakano T, et al. Incidence of Haemophilus influenzae type b meningitis in Mie prefecture, Japan. Pediatrics International, 2001, 43(3):323-324. 22
Hussain IHMI, et al. Haemophilus influenzae meningitis in Malaysia. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S189-190. 23
unpublished data on Mongolia. 24
Limcangco MR, et al. Cost-benefit analysis of a Haemophilus Influenzae Type B Meningitis Prevention Programme in The Philippines. Pediatric Infectious Disease Journal, 2001, 19(4):391-400. 25
Peltola H. Op cit. Ref 1. 26
Peltola H. Op cit. Ref. 1
- 11 -
Hib disease burden by individual country
Out of the 13 countries and areas in the East Asia subregion, no disease burden data were available in four countries and areas (Brunei Darussalam, Cambodia, the Lao People’s Democratic Republic, and Macao [China]). However, Brunei Darussalam introduced the Hib vaccine in 2003, following its introduction in Malaysia in 2002.
China
China lacks nationwide estimates of the Hib disease burden. To date, there has been only one hospital-based surveillance study conducted in Beijing between November 1988 and December 1989, followed by a community-based prospective surveillance study in Hefei city between January 1990 and December 1992
27. From the Hefei community survey,
which used both culture and capsular polysaccharides antigen detection methods to diagnose Hib, the annual incidence of Hib meningitis among children under five years of age was estimated to be 10.4 per 100 000 under-5 population (the overall incidence of acute bacterial meningitis in the same age group was 19.2) with a case fatality rate of 9.3%. Hib was estimated to account for 30%–50% of all bacterial meningitis cases. The study also tried to estimate the role of Hib in paediatric pneumonia. It was estimated that, from 1991 to 1993, the average pneumonia mortality rate among children under five years of age was 1563 per 100 000, and one-fourth to one-third of cases of pneumonia might be caused by Hib. Even though the annual incidence of Hib meningitis in China, based on the limited studies in Beijing and Hefei, was much higher compared with the rates in Hong Kong (China) or Taiwan (China), it was lower than in other developing countries in Asia, and in Europe and North America (see Table 3). However, a more recent study, using WHO generic protocol for population-based surveillance of Hib in Guangxi Zhuang autonomous Region between 2000 and 2002, estimated the annual incidence of Hib meningitis at 1.2 per 100 000 under-5 population, almost similar to that observed in Hong Kong (China) or Taiwan (China)
28.
Another study conducted in Beijing and Hefei between November 1997 and May 1998 reported that Hib was the second most common micro-organism in bacterial pneumonia, accounting for 10% of pneumonia cases with proven bacterial cause, which in turn accounted for about 37% of all pneumonia cases
29. The studies pointed out the problem of
antibiotics abuse, so the estimates from bacteriological evidence might be lower. In fact, one study showed much higher odds of positive nasopharyngeal cultures for Hib or pneumococcus in clinically or radiologically confirmed pneumonia cases than in age-matched control patients with diarrhoea or dermatitis
30. However, the same study found
much lower nasopharyngeal colonization rates (~2%) with Hib among the control population compared with colonization rates of 3%-6% in Western developed countries in the pre-vaccination era.
27
Yang Y, et al. Op cit. Ref 17. 28
WHO. Review panel of Haemophilus influenzae type b (Hib) disease burden in Bangladesh, Indonesia and other Asian countries. Op cit. Ref.18 29
Wang YJ, et al. Op cit. Ref 16. 30
Levine OS, et al. Haemophilus influenzae type b and Streptococcus pneumoniae as causes of pneumonia among children in Beijing, China. Emerging Infectious Diseases, 2000, 6(2):165-170.
- 12 -
Taiwan (China)
In Taiwan (China), the annual incidence of invasive Hib disease was estimated at 1.9 per 100 000 under-5 population based on a review of hospital records between 1992 and 1994
31. Meningitis accounted for 70% of all invasive Hib disease, and Hib was estimated
to cause about 20.7% of all bacterial meningitis. The case fatality and neurologic sequelae amounted to 13% and 27%, respectively. A hospital-based active surveillance study between January 1996 and April 1997 estimated Hib invasive disease incidence at 1.6 per 100 000 under-5 population, almost similar to the previous study
32. However, a recent
study using the National Health Insurance Research Database reported the annual incidence of Hib meningitis to be 5.6 per 100 000 under-5 population in 1997, and 3.2 per 100 000 under-5 population in 2000
33. The study attributed the decline in incidence from 1997 to
2000 to the possible impact of the introduction of a client-paid Hib vaccine in Taiwan (China) starting in 1993 (though the study done earlier between 1992 and 1994 also pointed to relatively lower incidence). Most of the Hib cases were among children aged six to twelve months. The estimates could be considered representative because the dataset covered almost all paediatric patients in the area. However, there still remains the possibility of underestimation of the disease burden due to antibiotic abuse and vaccine use in the private sector since 1993 (Table 3).
Hong Kong (China)
A retrospective study, based on a review of records of children hospitalized because of meningitis between 1984 and 1993 at the teaching hospital in New Territory East region, estimated annual Hib meningitis incidence at 1.1 (95% CI: 0.43-2.2) per 100 000 under-5 population among the Chinese population
34. Another five-year, territorywide retrospective
survey of children hospitalized between 1986 and 1990 estimated annual Hib meningitis incidence at 1.75 (95% CI: 1.21-2.44) per 100 000 under-5 population, with the incidence of overall invasive Hib disease, including meningitis, pneumonia, and septicaemia, at 2.7 (95% CI: 2.0-3.5) per 100 000 under-5 population
35,36. Both studies found a much higher
incidence rate among Vietnamese refugees: 5.2 (95% CI: 1.63-18.8) per 100 000 under-5 population of Hib meningitis
37 and 42.7 (95% CI: 17.2-87.9) per 100 000 under-5
population with invasive Hib disease38
. The high incidence rates for refugees was explained partly by the crowded living conditions for Vietnamese refugees, resulting in a higher probability of exposure to the micro-organism, and partly by lower access to local clinics, resulting in delayed use of antibiotics with consequent increased likelihood of a
31
Wang CH, Lin TY. Invasive Haemophilus influenzae diseases and purulent meningitis in Taiwan. Journal of the Formosan Medical Association, 1996, 95(8):599-604. 32
Chen MK, et al. Prospective surveillance of children with invasive Haemophilus influenzae disease in Taiwan. Journal of Microbiology, Immunology, and Infection, 1999, 32(4):257-260. 33
Shao PL, et al. Op cit. Ref. 15. 34
Sung RY, et al. Op cit. Ref 20. 35
Lau YL, et al. Invasive Haemophilus influenzae type b infections in children hospitalized in Hong Kong, 1986-1990. Hong Kong Hib Study Group. Acta Paediatrica, 1995, 84(2):173-176. 36
Lau YL, et al. Haemophilus influenzae type b infections in Hong Kong. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S165-169. 37
Sung RY, et al. Op cit. Ref 20. 38
Lau YL, et al. Op cit. Ref. 35.
- 13 -
positive culture. Both studies were conducted in a high-quality laboratory with representative samples, and the estimates are likely to reflect real conditions. However, the possibility of underestimation due to antibiotics abuse, leading to low culture positivity, cannot be ruled out completely, especially among the local Chinese population (see Table 3).
Japan
Three studies published in international journals were reviewed. A hospital-based retrospective survey conducted in Aichi prefecture between 1984 and 1993 estimated Hib meningitis incidence at 2.53 per 100 000 under-5 population, with a 3.2% case fatality rate and a 15% neurological sequelae rate
39. Hib meningitis accounted for 35% of all bacterial
meningitis. The authors argued that the findings reflected actual conditions in Japan, although the possibility of underestimation due to underreporting to hospitals cannot be ruled out. The second study, conducted in 1994 and based on a retrospective voluntary survey of all the 876 hospitals in six prefectures through a structured questionnaire (only 363 [41.4%] hospitals returned the complete questionnaire), estimated the mean annual incidence of Hib meningitis at 4.7 (ranging from 3.4 in Hokkaido prefecture to 9.9 in Mie perfecture) per 100 000 under-5 population, with a 3% fatality rate and an 18% sequelae rate
40. However, the study noted that technical difficulties in culturing Hib, in addition to
lower hospital participation rates in prefectures with higher estimated rates, may have led to underestimation of incidence. In that study, 40% of Hib cases were among children under one year of age. Hib was the most common cause of bacterial meningitis (43%), followed by S. pneumoniae (13%). The most recent study, carried out in 1997-98 and based on community-based surveillance in Mie prefecture, reported a higher incidence of meningitis, at 6.1 per 100 000 under-5 population. However, the study location and data collection methods differed from the earlier studies
41. In fact, the estimates of invasive Hib
diseases cited in domestic journals ranged from 2.9 to 6.2 per 100 000 under-5 population. However, even the highest estimates were lower than those estimated in Western developed countries in the pre-vaccine era (see Table 3).
Republic of Korea
One study collected medical records, including culture-proven bacterial meningitis, between 1986 and 1995 from 13 general and university hospitals around Seoul
42. The most
common causative organism for meningitis among children under five years of age was Hib (40.4%), followed by S. pneumoniae (28.1%). In addition, 95.8% of the Hib cases were among children under five years of age. The fatality rate was reported to be 16.7%. Another study, based on one university hospital’s records from 1986 to 1996, reported that
39
Ishikawa T, et al. Epidemiology of bacterial meningitis in children: Aichi Prefecture, Japan, 1984-1993. Pediatric Neurology, 1996, 14(3):244-250. 40
Kamiya H, et al. Childhood bacterial meningitis in Japan. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S183-185. 41
Nakano T, et al. Op cit. Ref. 21. 42
Kim KH, Sohn YM, Kang JH, et al. The causative organisms of bacterial meningitis in Korean children, 1986-1995. Journal of Korean Medical Science 1998; 13(1):60-64.
- 14 -
Hib accounted for 62% of bacterial meningitis, and that 92% of Hib cases developed in children under five years of age
43.
The first incidence study using prospective community-based surveillance was conducted between 1999 and 2001 in the province of Jeonbuk
44. The annual incidence of Hib
meningitis was estimated at 6.0 (95% CI: 2.9-12.4) per 100 000 under-5 population, with a 7% case-fatality rate and a 36% neurologic sequelae rate, although the results cannot be generalized to national level. The authors pointed out that the incidence might have been underestimated due to treatment with antibiotics before specimen collection and because of the introduction of the Hib vaccine in the private sector. In fact, although Hib was the most common organism of bacterial meningitis, only 14 out of 214 probable cases of bacterial meningitis were Hib culture-proven cases. At any rate, it seems that Hib meningitis rates in the Republic of Korea are much lower than in developing countries (see Table 3).
Malaysia
One study retrospectively collected medical records between 1985 and 1987 from a tertiary hospital in the eastern Malaysian state of Kelantan. The study noted that Hib accounted for 53.7% (29/54) of bacterial meningitis cases among children under five years of age, and all Hib cases occurring in children under five
45. Case fatality amounted to 44.4%.
Another study, also conducted in Kelantan, between 1985 and 1994, reported that 89.1% of invasive Hib diseases occurred in children under two years of age, and the fatality rate amounted to 12.3%, with a 41.5% rate of long-term complications from Hib meningitis
46.
However, those results may not be generalized to the national level due to their narrow geographical focus. A retrospective review of medical records in five paediatric departments during 1995 estimated the annual incidence of Hib meningitis at 38 per 100 000 under-5 population, with a 12.5% case fatality rate and a 30% sequelae rate
47. About 76% of cases
had occurred in children under one year of age. Even although those estimates may be on the low side, as the lumbar puncture rate was only 16.3% for local cultural reasons, they are relatively high compared with other countries in the East Asia subregion, but comparable to rates in Western developed countries in the pre-vaccine era (see Table 3). Conjugate Hib vaccine was introduced into the routine immunization schedule in July 2002.
Mongolia
The Ministry of Health has been conducting hospital-based sentinel surveillance in two national hospitals and four district hospitals in the capital city of Ulaanbaatar since February 2002. Based on surveillance results from 2002 to December 2004, the annual incidence of Hib meningitis was estimated at 16 per 100 000 under-5 population with a 22.2% case fatality rate in 2002, 38 per 100 000 under-5 population with a 20% case fatality rate in 2003, and 39 per 100 000 under-5 population in 2004. With an adjustment
43
Lee HJ. Op cit Ref. 12.. 44
Kim JS, et al. Op cit. Ref. 14.. 45
Choo KE, Ariffin WA, Ahmad T, Lim WL, Gururaj AK. Pyogenic meningitis in hospitalized children in Kelantan, Malaysia. Annals of Tropical Paediatrics 1990; 10(1):89-98. 46
Khairulddin NY, Choo KE, Johari MR. Epidemiology of Haemophilus influenzae invasive disease in hospitalised Kelantanese children, 1985-1994. Singapore Medical Journal 1999; 40(2):96-100. 47
Hussain IH, et al. Op cit. Ref. 22.
- 15 -
for the low rate of specimen collection and pre-admission death, the overall incidence was estimated to be 36 per 100 000 under-5 population (unpublished report).
Hib was identified as the most common cause of bacterial meningitis (24.5%, 59/241 cases) between 2002 and 2004. Mongolia introduced conjugate vaccine (diphtheria-pertussis-tetanus [DPT]-Hepb-Hib) into the national immunization programme with GAVI support in January 2005, covering approximately 25% of the total population in Phase I. The total number of suspected bacterial meningitis decreased sharply in 2005 with the introduction of the vaccine, from 66 cases in 2004 to 47 in 2005. Only 12.8% (six cases) of all meningitis cases were identified as being due to Hib in 2005, compared with 37.9% in 2004.
The Philippines
One study, using prospective hospital-based surveillance between April 1994 and December 1996 in Tagbilaran city in Bohol Province, estimated the annual incidence of laboratory-confirmed invasive Hib diseases at 28 per 100 000 under-5 population
48. All
cases of invasive Hib diseases occurred in children under one year of age, with an incidence rate of 71 (95% CI: 21-120) (see Table 3). The study suggested that Hib may not be an important etiological agent of pneumonia in children in the Philippines, which would be in contrast to its inferred 21% role in Gambia. However, the authors noted that the common practice of prescribing preadmission antibiotics may have led to underestimation of the true incidence.
Another hospital-based retrospective study conducted during the same period in Central Manila
49 reported the annual incidence of Hib meningitis at 95 (95% CI: 76.5 to 106.3) per
100 000 under-5 population, with an 11% case fatality rate and a 15% sequelae rate.50
The incidence in infants less than six months of age was estimated to be 412 (95% CI: 358-466) per 100 000. The study, however, does not provide information on total cases of probable bacterial meningitis admitted to the study hospitals during the study period. It was almost three times the estimates from a Tagbilaran city study (28 per 100 000 for overall invasive Hib disease), conducted at almost the same time. It was also one of the highest estimates ever reported in the East Asia subregion. Although the very different results obtained from the two studies may reflect true geographical differences in Hib incidence, it may also be due to overestimation of the numerator in the Manila study in calculation of the incidence rate, as the study site, being a capital city, may attract seriously ill patients from other parts of the country as well (though residency criteria was applied for inclusion in the study—it would be hard to verify addresses in a retrospective study). Although the results cannot be generalized to the whole country, the findings suggest that the Hib disease burden could be much larger than expected in Asia (see Table 3).
48
Lupisan SP, et al. Incidence of invasive Haemophilus influenzae type b infections in Filipino children. Pediatric Infectious Disease Journal, 2000, 19(10):1020-1022. 49
Central Manila comprises of the districts of Paco, Ermita, San Andres and Malate, with a total population of 3 415 000. 50
Limcangco MR, Salole EG, Armour CL. Epidemiology of Haemophilus influenzae type b meningitis in Manila, Philippines, 1994 to 1996. Pediatric Infectious Disease Journal, 2000, 19(1):7-11.
- 16 -
Singapore
The only study, based on a retrospective hospital survey between 1990 and 1995, estimated the annual incidence of invasive Hib diseases at 3.3 (95% CI: 2.6-3.5) per 100 000 children under five years of age
51. Hib was estimated to account for 18%–41% of all bacterial
meningitis cases (see Table 3).
Viet Nam
Tram and others examined the etiology of bacterial pneumonia and meningitis by recruiting children of one month to 59 months presenting with symptoms and signs of bacterial pneumonia and meningitis between May 1995 and November 1996 in Pediatric Hospital No. 1 in Ho Chi Minh City in South Viet Nam
52. Based on cerebrospinal fluid
(CSF) culture and latex agglutination, among 86 probable bacterial meningitis cases recruited, Hib, pneumococci and other bacterial organisms accounted for 34.9%, 26.7% and 13.6%, respectively. The remaining 21 cases (24%) had pleocytosis and elevated albumin concentrations, but no evidence of bacterial etiology by culture or latex agglutination of CSF. About 90% of Hib meningitis cases occurred in children under one year of age. Among probable bacterial pneumonia cases (n=300), S. pneumoniae, Hib and other organisms were identified in 92.5%, 1% and 6.6% of cases, respectively. A more recent study, using the WHO generic protocol for population-based surveillance of Hib in urban Ha Noi between March 2000 and February 2002, estimated the annual incidence of confirmed and probable Hib meningitis based on culture and Hib PCR at 12 per 100 000 under-5 population, with a 4% case fatality rate and a 10% sequelae rate
53. Confirmed or
probable Hib meningitis accounted for 14% of all probable meningitis cases among children under five years of age. However, if probable meningitis cases in the neonatal period are excluded from the denominator, then the proportion of Hib meningitis cases rises to 20.5%, lower than the 35% estimated in the study conducted in Ho Chi Minh City. No cases were detected among children older than two years of age. The estimates were much lower than for other developing countries in East Asia including Malaysia, Mongolia and the Philippines (see Table 3).
51
Lee YS, et al. Op cit. Ref. 11. 52
Tran TT, et al. The etiology of bacterial pneumonia and meningitis in Vietnam. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S192-194. 53
Anh D, et al, and the Vietnam Invasive Bacterial Disease Surveillance Network. Haemophilus influenzae type b meningitis among children in Ha Noi, Viet Nam: epidemiologic patterns and estimates of H. Influenzae type b disease burden. American Journal of Tropical Medicine and Hygiene, Mar 2006, 74: 509-515.
- 17 -
Table 3. Hib disease burden the East Asia subregion Income group Country Ref Year Design Incidence a Case fatality and
meningitis and 53% of confirmed bacterial meningitis and 1% of pneumonia.
Low
Viet Nam
53 00-02 C-P (Hanoi) 12 4.3% (sq 10%) The incidence includes both culture proven and probable Hib meningitis diagnosed with PCR. Hib meningitis accounted for 20.5% of all probable bacterial meningitis.
In general, the annual incidence of Hib meningitis in the Oceania subregion is much higher than in the East Asia subregion, ranging from 29 per 100 000 under-5 population in French Polynesia to 84 per 100 000 under-5 population in Fiji and Samoa, as estimated using RAT
54,55. The RAT estimates of Hib disease burden from each of these countries were found to
be consistently lower using the childhood mortality rate method than using the meningitis incidence rate method.
The case fatality rate ranged from 10% to 28%, comparable to estimates for developing regions at the global level (see Table 4)
56.
Country-level data
No disease burden data were available from Nauru, Tuvalu and Tokelau.
Australia
Before the introduction of the publicly-funded Hib immunization programme in 1993, Hib was one of the most important causes of morbidity and mortality among children in Australia (Table 2). Several studies were conducted, mainly between 1984 and 1990, in various regions, including Victoria
57, Northern Territory
58, Western Australia
59, Australia
Capital Territory60
and Sydney61
to estimate the burden of Hib disease. Those studies showed that the annual incidence of Hib meningitis among children under five years of age ranged from 20 to 63.2 per 100 000 under-5 population, with a 0%–4% case fatality rate, while among Aboriginal children, the annual incidence ranged from 150 to 159 per 100 000 under-5 population, with a 8%–10% fatality rate (see Table 4).
One study, examining the impact of the immunization programme based on the national communicable disease surveillance system, reported that the number of invasive Hib cases among children under five years of age declined by 87% between 1993 and 2000; the overall incidence of invasive Hib disease decreased from 15 to 1.2 per 100 000 under-
54
Russell FM, et al. High incidence of Haemophilus influenzae type b infection in children in Pacific island countries. Clinical Infectious Diseases, 2003, 37(12):1593-1599. 55
Wilson N, et al. Estimating the Haemophilus influenzae type b (Hib) disease burden and the impact of Hib vaccine in Fiji. Vaccine, 2003, 21(17-18):1907-1912. 56
Peltola H. Op cit. Ref 1. 57
Gilbert GL, Clements DA, Broughton SJ. Haemophilus influenzae type b infections in Victoria, Australia, 1985 to 1987. Pediatric Infectious Disease Journal, 1990, 9(4):252-277. 58
Hanna JN. The epidemiology of invasive Haemophilus influenzae infections in children under five years of age in the Northern Territory: a three-year study. Medical Journal of Australia, 1990, 152(5):234-236, 238, 240. 59
Hanna JN, Wild BE. Bacterial meningitis in children under five years of age in Western Australia. Medical Journal of Australia,1991, 155(3):160-164. 60
McGregor AR, et al. Invasive Haemophilus influenzae infection in the Australian Capital Territory region. Medical Journal of Australia, 1992, 156(8):569-571. 61
McIntyre PB, Leeder SR, Irwig LM. Invasive Haemophilus influenzae type b disease in Sydney children 1985-1987: a population-based study. Medical Journal of Australia,1991, 154(12):832-837.
- 20 -
5 population62
. However, the relative proportion of cases among Aboriginal children or among children under six months of age increased during the same period (see Table 4).
Fiji
Fiji is among the lower-middle-income economies in the Region, with a relatively large population compared with other countries in the Pacific (95 000 children under five years of age). The conjugate vaccine was introduced in mid-1994, but was only integrated with the national immunization programme in 1997 (see Table 1).
A study using the RAT method estimated the annual incidence of Hib meningitis between 1992 and 1994 at 84 and 70 per 100 000 under-5 population by meningitis incidence and childhood mortality rate method, respectively.
63 On the other hand, through a backward
calculation from the post-vaccine decline in the hospitalization rate, the annual incidence of Hib meningitis was estimated at 56–66 per 100 000 under-5 population. The authors concluded that, although the estimates were different depending on the calculation methods used, the true estimate of the pre-vaccine Hib meningitis burden was likely to be at least 50 per 100 000 under-5 population.
French Polynesia
An overseas territory of France, French Polynesia is among the high-income economies in the Region, with relatively low infant and child mortality rates.
Although there is no published data about the Hib disease burden, Russell and colleagues estimated the annual incidence of Hib meningitis at 29 per 100 000 under-5 population, with a 40% fatality rate, based on personal communication with an expert
64. That rate is
much lower than those in other Pacific island countries and areas, and is comparable to the global estimates for developing regions. However, the country has already introduced Hib vaccine into its national immunization programme.
Kiribati, Samoa, Solomon Islands and Tonga
Except for Solomon Islands, which is a low-income country, the other three countries are among the lower-middle-income economies in the Region. Only Tonga has introduced the Hib vaccine, in 2005. No data on disease burden were available until a recent survey using the WHO RAT was conducted with support of the WHO Western Pacific Regional Office between 2000 and 2002
65.
In that study, the Hib disease burden was estimated using three different methods: (1) enumeration of culture-proven Hib meningitis, (2) RAT meningitis incidence rate method, and (3) RAT under-5 mortality rate method. The three methods yielded varying results. For Kiribati, using the first two methods, the annual incidence of Hib meningitis
62
Horby P, et al. Progress towards eliminating Hib in Australia: An evaluation of Haemophilus influenzae type b prevention in Australia, 1 July 1993 to 30 June 2000. Communicable Diseases Intelligence, 2003, 27(3):324-341. 63
Wilson N, et al. Op cit. Ref. 55. 64
Russell FM, et al. Op cit. Ref 54. 65
Russell FM, et al. Op cit. Ref. 54.
- 21 -
was estimated at 11 (95% CI: 0-60) and 60 per 100 000 under-5 population, respectively. In Samoa, estimates using the three methods, respectively, were 25 (95% CI: 13-42), 84 and 49 per 100 000 under-5 population, in Solomon Islands, 33 (95% CI: 19-53), 84 and 49 per 100 000 under-5 population, and in Tonga, 52 (95% CI: 27-88), 70 and 14 per 100 000 under-5 population. The estimates were much higher than those for the other East Asia countries and higher than the global estimates for developing regions. However, the disease burden varied considerably, depending on assumptions about the Hib pneumonia/meningitis ratio. For example, when applying the assumption of a 5:1 ratio, the number of estimated cases and deaths in Samoa was 122 and 8 per 100 000 under-5 population, respectively; however, using the 1:1 assumption, the corresponding figures for estimated cases and deaths were 40 and 4.8, respectively.
New Caledonia
A territory of France, New Caledonia is among the high-income economies, with relatively low infant and child mortality rates, and provides the Hib vaccine through its national immunization programme.
Based on a retrospective review of medical records from one hospital with the only paediatrics unit in the country, the annual incidence of invasive Haemophilus infection was estimated at 54.6 per 100 000 under-5 population
66. However, the review was not
specific for serotype b or for meningitis. Even considering that limitation, the estimate was higher than that of French Polynesia, another French territory with similar conditions, and much lower than in neighbouring countries and areas with poor economic conditions. Notably, the burden differed significantly between ethnic groups: 94 per 100 000 under-5 population for Melanesians, and 13.8 for Caucasians.
New Zealand
New Zealand is among the high-income economies in the Region, with low infant and child mortality rates. Similar to Australia, Hib was the most common cause of life-threatening bacterial infection among children in the pre-vaccine era. A study that retrospectively collected hospital data in Auckland from 1981 to 1987 estimated the annual incidence of invasive Hib disease to be 41 per 100 000 under-5 population
67.
About 64% of the cases occurred among children under two years of age, and 63% were meningitis.
However, since the conjugate vaccine was integrated into the national immunization programme in 1994, morbidity and mortality from Hib have declined dramatically. Wilson and others evaluated the beneficial impact of the Hib vaccine in New Zealand based on medical records and mortality data
68. They found that Hib meningitis declined
by 92% from 1988-1993 to 1995-2000, and estimated the annual incidence of Hib meningitis at two per 100 000 under-5 population in the post-vaccination era. Although
66
Anglaret X, et al. Invasive Haemophilus influenzae disease of Melanesian and Caucasian children in New Caledonia. Pediatric Infectious Disease Journal, 1993, 12(10):888-889. 67
Voss L, Lennon D, Gillies M. Haemophilus influenzae type b disease in Auckland children 1981-87. New Zealand
Medical Journal, 1989, 102(865):149-151. 68
Wilson N, et al. The beneficial impact of Hib vaccine on disease rates in New Zealand children. New Zealand Medical Journal, 2002, 115(1159):1-7.
- 22 -
the incidence among Maori children also decreased to three per 100 000 under-5 population, the relative proportion of cases increased from 23% to 40%.
Papua New Guinea
Papua New Guinea is among the lower-middle-income economies, with high infant and child mortality rates. It has a relatively large population for the region, with 833 000 children under five years of age.
One study, based on a retrospective hospital survey between 1978 and 1987, reported that pneumococci and Hib were the main etiologies of invasive infectious disease in childhood; the two organisms were responsible for 73% of lung aspirates, 82% of blood, and 92% of CSF
69. However, the report did not provide the disease burden caused by
Hib. Another study also used hospital records between 1980 and 1984 and reported the case fatality of Hib at 30%, lower than the 46% for pneumococci
70.
A more recent study based on a prospective hospital survey between 1989 and 1992 reported that Hib accounted for 44% of blood culture and antigen-proven bacterial meningitis cases
71. However, Hib accounted for 28% of organisms isolated from CSF in
meningitis patients, while pneumococci were the most common organisms for 61%. Those figures are a little lower than reported in previous studies, which can be explained by prior use of antibiotics. The authors estimated the annual incidence of Hib meningitis (using population census data) at 63 per 100 000 under-5 population and 278 per 100 000 under-1 population. That estimate seems comparable to numbers from other Pacific island countries and areas with lower-income economies.
Vanuatu
Vanuatu is among the lower-middle-income economies, with relatively high infant and child mortality rates. A prospective three-year community-based hospital study (August 1988 to July 1991) estimated the annual incidence of Hib meningitis at 68.5 per 100 000 under-5 population, with a 29% case fatality rate, comparable to estimates from other poor Pacific island countries.
72
69
Gratten M, Montgomery J. The bacteriology of acute pneumonia and meningitis in children in Papua New Guinea: assumptions, facts and technical strategies. Papua New Guinea Medical Journal, 1991, 34(3):185-198. 70
Gratten M, et al. The etiology of purulent meningitis in highland children: a bacteriological study. Papua New Guinea Medical Journal, 1985, 28(4):233-240. 71
Lehmann D, et al. Etiology and clinical signs of bacterial meningitis in children admitted to Goroka Base
Hospital, Papua New Guinea, 1989-1992. Annals of Tropical Paediatrics, 1999, 19(1):21-32. 72
Carroll K, Carroll C. The epidemiology of bacterial meningitis occurring in a Pacific Island population. Papua
New Guinea Medical Journal 1993; 36(3):234-242.
- 23 -
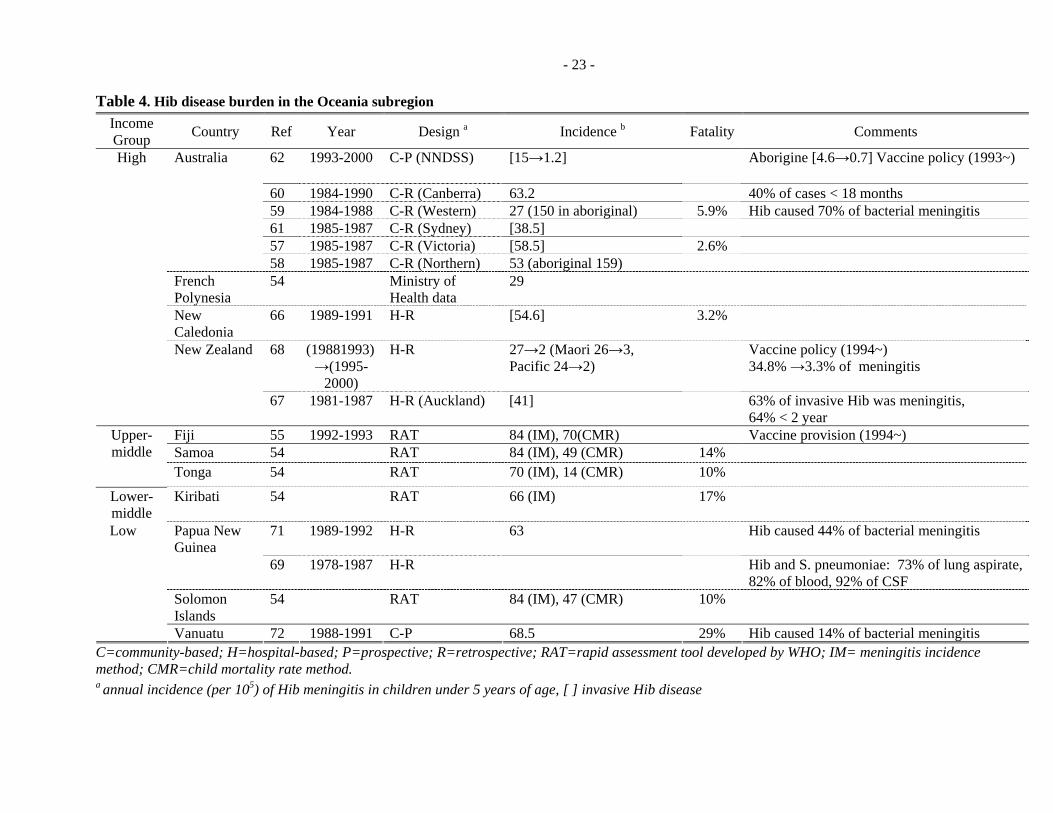
Table 4. Hib disease burden in the Oceania subregion Income Group Country Ref Year Design a Incidence b Fatality Comments
58 1985-1987 C-R (Northern) 53 (aboriginal 159) French Polynesia
54 Ministry of Health data
29
New Caledonia
66 1989-1991 H-R [54.6] 3.2%
68 (19881993) →(1995-
2000)
H-R 27→2 (Maori 26→3, Pacific 24→2)
Vaccine policy (1994~) 34.8% →3.3% of meningitis
High
New Zealand
67 1981-1987 H-R (Auckland) [41] 63% of invasive Hib was meningitis, 64% < 2 year
Fiji 55 1992-1993 RAT 84 (IM), 70(CMR) Vaccine provision (1994~) Samoa 54 RAT 84 (IM), 49 (CMR) 14%
Upper- middle
Tonga 54 RAT 70 (IM), 14 (CMR) 10%
Lower- middle
Kiribati 54 RAT 66 (IM) 17%
71 1989-1992 H-R 63 Hib caused 44% of bacterial meningitis Papua New Guinea
69 1978-1987 H-R Hib and S. pneumoniae: 73% of lung aspirate, 82% of blood, 92% of CSF
Solomon Islands
54 RAT 84 (IM), 47 (CMR) 10%
Low
Vanuatu 72 1988-1991 C-P 68.5 29% Hib caused 14% of bacterial meningitis C=community-based; H=hospital-based; P=prospective; R=retrospective; RAT=rapid assessment tool developed by WHO; IM= meningitis incidence method; CMR=child mortality rate method. a annual incidence (per 105) of Hib meningitis in children under 5 years of age, [ ] invasive Hib disease
- 24 -
3.2 Hib vaccination status in the Western Pacific Region
3.2.1 Haemophilus influenzae type b vaccines
The first Hib vaccine, a pure polysaccharide vaccine (polyribosyl ribitol phosphate [PRP]), was licensed for use in the United States of America in 1985. However, the vaccine was not effective in infants and was consequently discontinued. The first Hib conjugate vaccine (PRP–diphtheria toxoid conjugated vaccine [PRP-D]) was licensed for use in December 1987; however, that vaccine was found to be inconsistently immunogenic in children under 18 months of age, and was not recommended for use in infants. Since 1990, three additional immunologically distinct conjugate Hib vaccines (Haemophilus b oligosaccharide conjugate vaccine [HbOC], PRP–tetanus toxoid conjugated vaccine [PRP-T], and PRP–outer membrane protein conjugate vaccine [PRP-OMP]) have been licensed for use in infants.
The schedule for primary immunization of infants varies according to the product and country, depending on policy and budgeting. PRP-OMP is administered in two primary doses at ages two and four months, with a booster dose at 12-15 months; HbOC and PRP-T are administered in three primary doses at ages two, four, and six months, with a booster dose at 15 months. There are many different combination vaccines that contain Hib conjugate vaccine (see Table 5). All conjugate Hib vaccines are interchangeable for the primary series and the booster dose. The number of doses a child needs to complete the series depends on the child’s age. Unvaccinated children of seven months and older may not require a full series of three or four doses. All children of 15 to 59 months need at least one dose. No vaccination is recommended for children of five years or older.
The prices of vaccines vary according to the type of vaccine and the market, from US$ 3.10 to US$ 21.38. The United Nations Children's Fund price for diphtheria-tetanus-whole cell pertussis vaccine (DTwP)-Hib-HepB vaccine in 2000 was US$ 3.50 per dose.
Table 5. Haemophilus influenzae type b vaccines
Vaccine Trade Name Manufacturer Date licensed
Routine vaccination schedule (months)
Polysaccharide vaccine (no longer in use) b-CAPSA 1 Praxis 1985 24-59 Hib-VAX Connaught Labs 18-24 PRP Hib-Imune Lederle
HepB Infanrix hexa GlaxoSmithKline 2000 2, 4, 6 and 15-18
Hib(PRP-OMP)-HepB COMVAXb Merck & Co., Inc. 1996 2, 4 and 12-18
a TriHIB and other vaccines with accellular pertussis antigens are not approved for the primary series at 2, 4, or 6 months of age, but are approved for the fourth dose of the DTaP and Hib series only. b COMVAX should not be used in infants under 6 weeks of age. Not licensed for use if mother is HBsAg+.
3.2.2 Hib vaccination status and coverage rate by country
Among the 37 countries and areas in the Western Pacific Region, Hib vaccine is available in 23. Of those 23 countries and areas, 17 have introduced Hib vaccine into their routine childhood immunization programmes, and six (China, Hong Kong [China], the Philippines, the Republic of Korea, Singapore and Viet Nam) have made conjugate Hib vaccines available to parents for purchase at private or government clinics. In the East Asia subregion, three out of 13 countries (Brunei Darussalam, Malaysia and Mongolia) have introduced the Hib vaccine into their national immunization programmes. While Hib vaccination was introduced with financing from domestic public resources in Brunei Darussalam and Malaysia, its introduction in Mongolia was facilitated by financing from GAVI. Macao (China) is also planning to introduce the Hib vaccine in 2007, based on a favourable cost-effectiveness analysis for Hib vaccine introduction
- 26 -
vis-à-vis introduction of inactivated polio vaccine (IPV)73
. Hong Kong (China), Japan, the Republic of Korea and Singapore are among the high-income countries and areas that have not introduced the Hib vaccine, as most available data suggest low disease burdens.
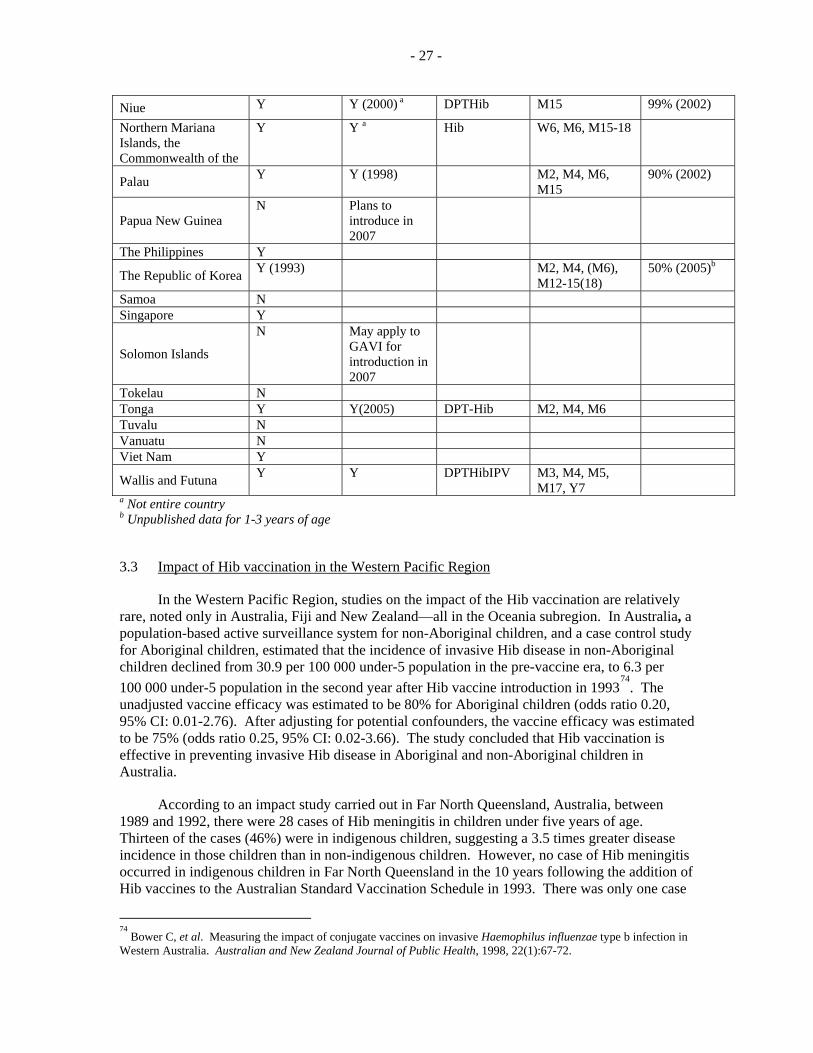
In Oceania, 14 out of 24 countries have adopted the Hib vaccine into their national immunization programmes (NIP); two high-income countries (Australia and New Zealand); the Pacific islands associated with the United States of America (American Samoa, Guam, the Marshall Islands, the Federated States of Micronesia, the Commonwealth of the Northern Mariana Islands and Palau); those associated with France (French Polynesia, New Caledonia, and Wallis and Futuna); Fiji; Niue; and Tonga. Papua New Guinea is planning to introduce the Hib vaccine as DPT-Hib with GAVI support in 2007.
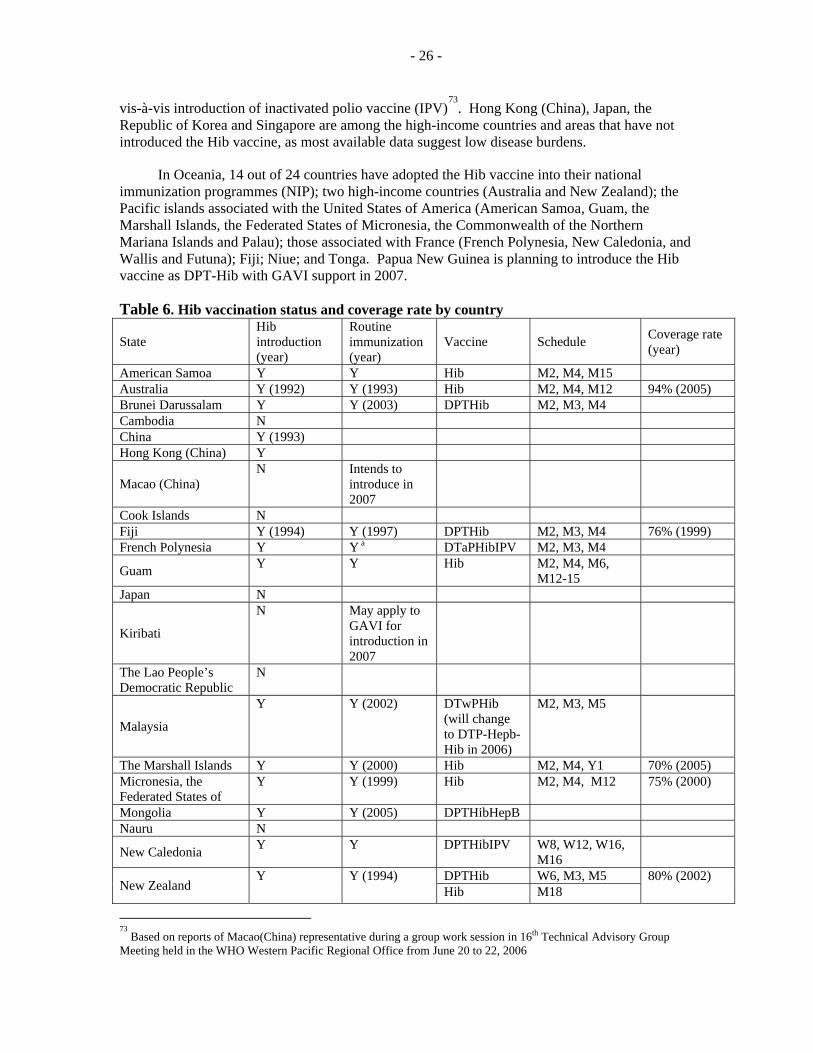
Table 6. Hib vaccination status and coverage rate by country
State Hib introduction (year)
Routine immunization (year)
Vaccine Schedule Coverage rate (year)
American Samoa Y Y Hib M2, M4, M15 Australia Y (1992) Y (1993) Hib M2, M4, M12 94% (2005) Brunei Darussalam Y Y (2003) DPTHib M2, M3, M4 Cambodia N China Y (1993) Hong Kong (China) Y
Macao (China) N Intends to
introduce in 2007
Cook Islands N Fiji Y (1994) Y (1997) DPTHib M2, M3, M4 76% (1999) French Polynesia Y Y a DTaPHibIPV M2, M3, M4
Guam Y Y Hib M2, M4, M6, M12-15
Japan N
Kiribati
N May apply to GAVI for introduction in 2007
The Lao People’s Democratic Republic
N
Malaysia
Y Y (2002) DTwPHib (will change to DTP-Hepb-Hib in 2006)
M2, M3, M5
The Marshall Islands Y Y (2000) Hib M2, M4, Y1 70% (2005) Micronesia, the Federated States of
Y Y (1999) Hib M2, M4, M12 75% (2000)
Mongolia Y Y (2005) DPTHibHepB Nauru N
New Caledonia Y Y DPTHibIPV W8, W12, W16, M16
DPTHib W6, M3, M5 New Zealand
Y Y (1994) Hib M18
80% (2002)
73
Based on reports of Macao(China) representative during a group work session in 16th Technical Advisory Group Meeting held in the WHO Western Pacific Regional Office from June 20 to 22, 2006
- 27 -
Niue Y Y (2000) a DPTHib M15 99% (2002)
Northern Mariana Islands, the Commonwealth of the
Y Y a Hib W6, M6, M15-18
Palau Y Y (1998) M2, M4, M6, M15
90% (2002)
Papua New Guinea N Plans to
introduce in 2007
The Philippines Y
The Republic of Korea Y (1993) M2, M4, (M6), M12-15(18)
50% (2005)b
Samoa N Singapore Y
Solomon Islands
N May apply to GAVI for introduction in 2007
Tokelau N Tonga Y Y(2005) DPT-Hib M2, M4, M6 Tuvalu N Vanuatu N Viet Nam Y
Wallis and Futuna Y Y DPTHibIPV M3, M4, M5, M17, Y7
a Not entire country b Unpublished data for 1-3 years of age
3.3 Impact of Hib vaccination in the Western Pacific Region
In the Western Pacific Region, studies on the impact of the Hib vaccination are relatively rare, noted only in Australia, Fiji and New Zealand—all in the Oceania subregion. In Australia, a population-based active surveillance system for non-Aboriginal children, and a case control study for Aboriginal children, estimated that the incidence of invasive Hib disease in non-Aboriginal children declined from 30.9 per 100 000 under-5 population in the pre-vaccine era, to 6.3 per 100 000 under-5 population in the second year after Hib vaccine introduction in 1993
74. The
unadjusted vaccine efficacy was estimated to be 80% for Aboriginal children (odds ratio 0.20, 95% CI: 0.01-2.76). After adjusting for potential confounders, the vaccine efficacy was estimated to be 75% (odds ratio 0.25, 95% CI: 0.02-3.66). The study concluded that Hib vaccination is effective in preventing invasive Hib disease in Aboriginal and non-Aboriginal children in Australia.
According to an impact study carried out in Far North Queensland, Australia, between 1989 and 1992, there were 28 cases of Hib meningitis in children under five years of age. Thirteen of the cases (46%) were in indigenous children, suggesting a 3.5 times greater disease incidence in those children than in non-indigenous children. However, no case of Hib meningitis occurred in indigenous children in Far North Queensland in the 10 years following the addition of Hib vaccines to the Australian Standard Vaccination Schedule in 1993. There was only one case
74
Bower C, et al. Measuring the impact of conjugate vaccines on invasive Haemophilus influenzae type b infection in Western Australia. Australian and New Zealand Journal of Public Health, 1998, 22(1):67-72.
- 28 -
of Hib meningitis, in a (vaccinated) non-indigenous child, between 1994 and 2003. The study concluded that Hib immunization prevented about 70 cases of Hib meningitis, five deaths and 12 cases with neurological sequelae in children in Far North Queensland between 1994 and 2003
75.
In Fiji, a study that collected laboratory data (meningitis) and hospitalization and mortality data (pneumonia and meningitis) before and after the Hib vaccine introduction, estimated that the Hib vaccine led to a 32% decline in meningitis hospitalizations (95% CI; 11–48), and a 78% decline in mortality due to meningitis (95% CI; 22–94) for all children under five years of age
76.
However, there was no similar consistent decline in pneumonia hospitalizations or in deaths after Hib vaccine introduction, except for a statistically significant reduction in pneumonia mortality in children under one year of age.
According to one study in New Zealand that used national mortality, hospitalization, laboratory and notification data, the introduction of the Hib vaccine in 1994 led to a 92% decline (95% CI: 89-94) in the hospitalization rate due to Hib meningitis among children under five years of age from 27 per 100 000 under-5 population in 1988-1993 to 2 per 100 000 under-5 population in 1995-2000
77. The epiglottitis hospitalizations also declined by 94% (95% CI: 89-96). In
absolute terms, the Hib vaccination appears to be preventing at least 80 cases of meningitis and 30 cases of epiglottitis every year in children under five years of age in New Zealand. Even although Hib meningitis declined in all ethnic groups (e.g. down to three per 100 000 under-5 population among the Maori—the ethnic minority group with highest disease burden), the share of Maori children out of the total children hospitalized with Hib meningitis increased from 23% to 40%. However, the beneficial impact of Hib vaccination has been less for the Maori people and so there is a need for further improvements in immunization coverage in high-risk populations who endure the highest disease burdens.
3.4 Economic evaluation of Hib immunization in the Western Pacific Region
The cost-effectiveness evaluation of proposed new vaccine introductions has become an increasingly important area of research and is regarded as a prerequisite for new vaccine introduction policy in some countries. In this section, the literature on economic evaluations of Hib vaccine in the Western Pacific Region is presented and compared with results from Europe and the United States of America.
There are fewer studies available concerning the economic evaluation of the Hib vaccine in the Western Pacific Region than in the United States of America or in European countries. Most economic evaluation studies have been conducted in the United States of America, Australia and Sweden.
75
Hanna JN. Impact of Haemophilus influenzae type b (Hib) vaccination on Hib meningitis in children in Far North Queensland, 1989 to 2003. Communicable diseases intelligence, 2004, 28(2):255-257. 76
Wilson, et al. Op cit. Ref. 55. 77
Wilson, et al. Op cit. Ref. 68.
- 29 -
Table 7. Key literature on economic evaluation of Hib vaccine across WHO regions
Western Pacific (37 countries)
Americas (35 countries)
Europe (52 countries)
Africa (46 countries)
Eastern Mediterranean (21 countries)
South-East Asia
(11 countries)Brinsmead et al. (2003)
78
Limcangco et al. (2001)
79
Hussain et al. (1999)
80
Miller (1998)81
Harris et al. (1994)
82
McIntyre et al. (1994)
83
Zhou et al. (2002)
84
Midani et al. (1995)
85
Levine et al. (1993)
86
Hay and Daum (1990)
87
Cochi et al. (1985)
88
Hay and Daum (1987)
89
Pokorn et al. (2001)90
Jiménez, et al. (1999)
91
Garpenholt et al. (1998)
92
Livartowski et al. (1996)
93
Trollfors (1994)94
Ginsberg et al. (1993)
95
Hussey et al. (1995)
96
Miller (1998)
97
78
Brinsmead R, Hill S, Walker D. Are economic evaluations of vaccines useful to decision-makers? Case study of Haemophilus influenzae type b vaccines. Pediatric Infectious Disease Journal, 2004; 23(1):32-37. 79
Limangco, et al. Op cit. Ref. 24. 80
Hussain IHMI, et al. Cost-Benefit analysis of Haemophilus influenzae vaccination programme in Malaysia. Buletin Kasiharan Masyakat Jilid, 1999, 5:79-89. 81
Miller MA. An assessment of the value of Haemophilus influenzae type b conjugate vaccine in Asia. Pediatric Infectious Disease Journal,1998, 17(9 Suppl):S152-159. 82
Harris A, et al. The burden of Haemophilus influenzae type b disease in Australia and an economic appraisal of the vaccine PRP-OMP. Medical Journal of Australia, 1994, 160(8):483-488. 83
McIntyre P, Hall J, Leeder S. An economic analysis of alternatives for childhood immunisation against Haemophilus influenzae type b disease. Australian Journal of Public Health, 1994, 18(4):394-400. 84
Zhou F, et al. Impact of universal Haemophilus influenza type b vaccination starting at 2 months of age in the United States: an economic analysis. Pediatrics, 2002, 110(4):653-661. 85
Midani S, Ayoub E, Rathore M. Cost-effectiveness of Haemophilus influenza type b conjugate vaccine programme in Florida. Journal of the Florida Medical Association, 1995, 82(6):401-402. 86
Levine OS, et al. Cost-benefit analysis for the use of Haemophilus influenzae type b conjugate vaccine in Santiago, Chile. American Journal of Epidemiology, 1993, 137(11):1221-1228. 87
Hay JW, Daum RS. Cost-benefit analysis of Haemophilus influenzae type b prevention: conjugate vaccination at eighteen months of age. Pediatric Infectious Disease Journal, 1990, 9(4):246-252. 88
Cochi SL, Broome CV, Hightower AW. Immunization of US children with Hemophilus influenzae type b polysaccharide vaccine. A cost-effectiveness model of strategy assessement. Journal of the American Medical Association, 1985, 253(4):521-529 89
Hay JW, Daum RS. Cost-benefit analysis of two strategies for prevention of Haemophilus influenzae type b infection. Pediatrics,1987, 80(3); 319-329. 90
Pokorn M, et al. Economic evaluation of Haemophilus influenzae type b vaccination in Slovenia. Vaccine, 2001, 19:3600-3605. 91
Jiménez FJ, et al. Cost-benefit analysis of Haemophilus influenzae type b vaccination in children in Spain. Pharmoeconomics, 1999, 15(1):75-83. 92
Garpenholt O, Silfversal S-A, Levin L-A. Economic Evaluation of General Childhood Vaccination against Haemophilus influenzae type b in Sweden. Scandinavian Journal of Infectious Disease, 1998, 30:5-10. 93
Livartowski A, et al. Cost-effectiveness evaluation of vaccination against Haemophilus influenzae invasive diseases in France. Vaccine, 1996, 14(6):495-500. 94
Trollfors B. Cost-benefit analysis of general vaccination against Haemophilus influenzae type b in Sweden. Scandinavian Journal of Infectious Disease, 1994, 611-614.
- 30 -
3.4.1 Literature on the economic evaluation of Hib vaccine in the Western Pacific Region
Miller modelled the cost per death prevented and cost per disability-adjusted life year (DALY) and the net cost of a Hib vaccination programme in 23 Asian countries (13 from the Western Pacific Region) based on several epidemiological and economic assumptions on the Hib disease burden and the cost of Hib vaccination and disease treatment, and noticed large differences in the results of economic evaluations of Hib vaccination across countries, with variations in the overall economic development and Hib disease burden
98.
In the absence of local data, the Hib meningitis incidence in the countries included in the study was assumed to be comparable to that observed in countries in other regions at a similar level of economic development. The pneumonia incidence was assumed to be five times that of meningitis, except in high-income countries, where no Hib pneumonia was assumed. The case fatality rate for pneumonia was assumed to be one-half that of meningitis. For calculation of Hib vaccination programme costs, the cost per dose of vaccine was assumed to be US$ 1.5 in lower-income countries rising to US$ 4.50 in high-income countries, with vaccine administration costs per dose ranging from US$ 0.18 to US$ 13.97. On the other hand, for calculation of cost-savings from treatment of prevented Hib disease, the treatment cost per day was assumed to vary from US$ 7.00 in China to US$ 21.00 in lower-income countries to US$ 784.00 in high-income countries for inpatient treatment costs; and from US$ 2.00 in China to US$ 5.00 in lower-income countries to US$ 50.00 in high-income countries for outpatient treatment. No inputs were made for the cost of treatment of long-term sequelae. The author classified an intervention in which a DALY costs less than the per capita gross national product (GNP) as cost-effective, but noted that even if the introduction of the Hib vaccine is found to be cost-effective (see Table 8), there still remains the issue of affordability; most low-income countries with a probable high disease burden due to Hib and other infectious agents cannot afford the vaccine without donor assistance.
Miller’s model has some limitations: a failure to offer information on treatment-seeking behaviour; the application of different assumptions about medical service utilization rates (50%-90%) across countries; and a failure to consider the long-term costs due to sequelae. In addition, the price of vaccine considered was too low, with current prices, even for low-income countries, ranging from US$ 3.00 per dose and up. Also, the assumptions about the ratio of pneumonia to meningitis cases and assumptions regarding cost of treatment are questionable. Hence, although the model provides an overall rough idea about the cost-effectiveness of Hib vaccine, further, country-specific evaluations are required.
95
Ginsberg G, Kassis I, Dagan R. Cost benefit analysis of Haemophilus influenzae type b vaccination programme in Israel. Journal of Epidemiology and Community Health, 1993, 43:485-490. 96
Hussey GD, Lasser ML, Reekie WD. The costs and benefits of a vaccination programme for Haemophilus influenzae type b disease. South African Medical Journal, 1995, 85(1):20-25. 97
Miller MA. Op cit. Ref. 81. 98
Miller MA. Op cit. Ref 81.
- 31 -
Table 8. Major assumptions and findings of Miller’s model for the Western Pacific Region(unit: US$ in 1997)
In Australia, Harris and others evaluated the cost and impact of the immunization schedule (second, fourth and twelfth month) of the PRP-OMP vaccine
99. It was estimated that the
Hib incidence among children under five years of age is 53 per 100 000 under-5 population among non-Aboriginal and 460 per 100 000 under-5 population among Aboriginal peoples. Based on those estimates, at least 630 children were expected to contract Hib annually, resulting in up to 19 deaths and 46 children with residual neurological sequelae. From their study, the authors considered Hib immunization to be more cost-effective than other preventive medical interventions, such as mammography. However, the cost per life per year saved cannot be an appropriate basis for decision-making, especially when there are substantial inequities in disease burden distribution. If the conjugate vaccine is given only to Aboriginal children, the cost savings could be much larger, since immunization may have a proportionately larger impact among that minority group. McIntyre and colleagues studied the cost-benefit and cost-utility analysis of Hib immunization based on a hypothetical birth cohort of 250 000 non-Aboriginal children
100. The model predicted that,
without immunization, 625 cases of invasive Hib disease would occur among children under five years of age. The study showed that the assumptions about Hib incidence, age distribution of disability, and administrative cost of immunization played an important role in the results of the economic evaluation. However, neither study considered the indirect benefits of prevention of disability and death due to Hib.
Table 9. Key findings in Australian studies (unit :AUD, 1 US$ = 1.46 AUD in 1994) Estimates
Cost/case prevented - AUD 5431 (=US$ 3720) QALY, quality adjusted life year
Malaysia
In Malaysia, a cross-sectional study involving five public hospitals was undertaken to examine the cost-benefit ratio of universal childhood immunization against Hib
103. Costs
were calculated from a societal point of view and included the cost of acute care for Hib meningitis (RM 3.8 million), the cost to families in terms of lost wages during hospitalization of the children (RM 2.04 million) and the cost of long-term care of children with residual neurological deficits (RM 29.2 million). Assuming the Hib vaccine will be introduced as DPT-Hib, which will simply replace existing DPT vaccine, no incremental cost except the cost of the vaccine were assumed to the total cost of routine immunization. The total cost of new vaccine at a rate of RM 19.55 per dose was calculated to be RM 32.3 million. Results suggested a cost–benefit ratio of 1.09 with a net benefit of
99
Harris, et al. Op cit. Ref 82. 100
McIntyre PB, et al. Op cit. Ref 83. 101
Harris, et al. Op cit. Ref 82. 102
McIntyre PB, et al. Op cit. Ref 83. 103
Hussain IHMI, et al. Op cit. Ref 80.
- 33 -
RM 2.89 million. However, the researchers used many assumptions in their calculations (e.g. it is assumed that 1.2% of all paediatric admissions are due to meningitis and 30% of these meningitis cases are due to Hib) due to the lack of empirical data. Continuous revisions using actual data are needed.
The Philippines
Limcangco and others evaluated the cost-benefit of a three-dose Hib immunization schedule in Manila, the Philippines, in a hypothetical birth cohort of 100 000 children
104.
Their model, similar to the Malaysian one, focused only on Hib meningitis and did not include costs associated with other invasive infections associated with Hib. Hib meningitis incidence was computed at 95 per 100 000, as observed in a study in Central Manila, although it was almost three times the total Hib disease incidence calculated in another study carried out at the same time in another city in the Philippines. Costs included hospital treatment cost (inpatient as well as intensive care); marginal cost for special education of disabled children; annual cost of residential care for severely disabled children; cost of hearing aids for children with hearing impairment; annual salary loss to the parent who had to stay home to take care of the sick/disabled child. The vaccination costs were estimated to be US$ 13.4 at 1998 exchange rates, assuming a 33% wastage rate and use of the DTP-Hib formulation. The results of the study indicate that the costs generated by Hib meningitis from a societal perspective would exceed the costs associated with a vaccination programme. The incidence of Hib meningitis in the Philippines (95 per 100 000 under-5 population) taken into account for the study, however, is at least twice that of other countries where other invasive infections associated with the Hib organism, such as pneumonia, epiglottitis and cellulites, are included.
Table 10. Key findings of Limcangco’s cost-effectiveness model in the Philippines (Unit: PHP, 1 US$ = 35 PHP in 1998)
Parameters Estimates Cases/sequelae/deaths prevented per year 553/74/61 Cost per case prevented PHP 14 400 (=US$ 411.43) Cost per sequelae prevented PHP 108 200 (=US$ 3091.43) Cost per death prevented PHP 131 200 (=US$ 3748.57)
Tonga
Brinsmead examined the cost and benefit of Hib immunization in Tonga in terms of savings to the public sector rather than from the societal perspective, which, accordingly, resulted in an overestimation of cost and an underestimation of benefit
105. Nevertheless,
although the economic and intangible costs for affected children and their families were not considered, the Hib vaccination was found to be cost-effective (see
104
Limcangco, et al. Op cit. Ref. 24. 105
Brinsmead R. Economic evaluation of the introduction of Haemophilus influenzae type b(Hib) and rubella vaccine to the kingdom of Tonga. 2003. (unpublished paper).
- 34 -
Table 11). It is plausible to extrapolate the results to other Pacific islands under the assumption of identical epidemiologic parameters, although local estimates of Hib incidence, ratio of Hib pneumonia to meningitis and case fatality should be applied.
Table 11. Key findings of Brinsmead’s study in Tonga (US$ 1 = 2 TOP in 2002)
Tonga and other Pacific islands*
Incremental cost-effectiveness ratio (ICER) (TOP) (US$) Incremental cost per extra case prevented 1181 591 Incremental cost per life saved 17 722 8894 Incremental cost per extra undiscounted life year gained 176 88 Incremental cost per extra discounted life year gained 477 239 * Based on the results of sensitivity analysis, as well as discussions with health care workers in Tonga and Fiji, it appears feasible to develop a “generic” model of the cost-effectiveness of Hib vaccine in the Pacific islands.
3.4.2 Comparison of the studies on economic evaluation across regions
The different epidemiological assumptions and economic inputs used across different studies on cost-effectiveness make comparison difficult. Nevertheless, the cost–benefit ratio in the Western Pacific Region seems to be relatively lower than in the Americas and in Europe (see Table 12). Table 12. Major findings of economic evaluation for Hib immunization across regions Western Pacific Americas and Europe
Incremental cost per QALY Australia: US$ 1572 , US$ 5544
Cost/life saved * The Philippines: US$ 3749 South Korea*: US$ 5619 Brunei Darussalam*: US$ 2 854 897
USA: US$ 743 209 Israel: US$ 896 200
Cost/life year saved Australia: US$ 2518 USA: US$ 17 577
Israel: US$ 11.382 France: US$ 9834
Cost/case prevented The Philippines: US$ 411.4 Australia: US$ 4345
USA: US$ 28 073 Israel: US$ 16 516
* Cost/life saved (US$) with treatment 106
Cochi S, Broome C, Hightower A. Op cit. Ref 88. 107
Pokorn M, et al. Op cit. Ref. 90. 108
Jiménez FJ, et al. Op cit. Ref. 91. 109
Ginsberg G, et al. Op cit. Ref. 95. 110
Levine OS, et al. Op cit. Ref. 86. 111
Limcango, et al. Op cit. Ref .24. 112
Trollfors B. Op cit. Ref. 94.
- 35 -
3.4.3 Sensitivity analysis
The authors performed a sensitivity analysis under different Hib incidence scenarios with published data. As expected, the cost–benefit ratio increased as the Hib incidence increased in all countries (see Table 13) and with a decrease in vaccine price at the same incidence rate. The effect of the decline in the vaccine price was higher than the effect of the increase in incidence of Hib on the cost–benefit ratio.
Table 13. Sensitivity analysis under different assumptions about Hib incidence
Country Assumption for sensitivity analysis cost–benefit ratio
Meningitis incidence: 1025/year 1.09 Incidence increase by 25% (1281/year) 1.36 Incidence increase by 50% (1538/year) 1.63 Incidence increase by 25%, decrease of vaccine price by 25% 1.8
Malaysia (meningitis)
Incidence increase by 50%, decrease of vaccine price by 50% 3.2 Base case 5.4 Pre-vaccine incidence is assumed to be 50% of the base cases 1.7 Pre-vaccine incidence is assumed to be 200% of the base cases 6.9
USA
Post-vaccine incidence is assumed to be 200% of the base cases 3.4 Incidence for base case: 15/100 000 0.89 Incidence for low limit: 10/100 000 0.60 Spain Incidence for high limit: 30/100 000 1.79 Incidence at the baseline: 22.9/100 000 1.66 High incidence: 45.8/100 000 3.31 Chile
(meningitis) US incidence: 60/100 000 4.22
4. DISCUSSION
The Western Pacific Region consists of 37 diverse countries and areas varying in their levels of economic development, population, health care systems and general health status. Therefore, making aggregate estimates and general recommendations for the Region as a whole is not justified. The incidence of Hib meningitis in many East Asian countries is less than 40 per 100 000 under-5 population. In China, Hong Kong (China), Japan, the Republic of Korea and Singapore, incidence has been estimated to be less than or equal to 10 per 100 000 under-5 population. However, one study in the Philippines showed an incidence of 95 per 100 000 under-5 population, although another study from the Philippines estimated the incidence at 28 per 100 000 under-5 population. In the Oceania subregion, the incidence has been estimated to be 27–63 in Australia, 29 in French Polynesia and 27 in New Zealand. Other islands that have data generated using the RAT method show a high incidence of 50–84 per 100 000 under-5 population.
However, one important issue currently being discussed is whether the low Hib disease burden reported from many East Asian countries is real or the consequence of high antibiotic abuse prior to admission and the low sensitivity of laboratory testing. This is now being
- 36 -
highlighted more often since the results of a vaccine probe study in Lombok, Indonesia, demonstrated that incidence of purulent meningitis prevented by vaccination is much higher than the meningitis diagnosed as being due to Hib by laboratory testing. Hence, many researchers are now recommending the use of new study methods rather than just relying on laboratory-based hospital surveillance. Although underestimation of the Hib disease burden is a real possibility, it is difficult to explain why studies should detect a high disease burden with standard laboratory testing in Africa or Papua New Guinea, but not in China and Viet Nam, as both groups are likely to have similar levels of prior antibiotic use and laboratory quality. Another issue worth noting is that the prevalence of overall purulent meningitis is low in East Asia, with much lower overall infant and post-neonatal mortality rates.
113
Figure 2 shows the most recent and the highest annual incidence of Hib meningitis with the infant mortality, an indicator of the overall health status of children. In general, the East Asia subregion (on the left side) shows a lower incidence of meningitis compared with the Oceania subregion (on the right side). No consistent relationship pattern can be seen between Hib disease burden, level of economic development and infant mortality rates.
Figure 2. Relationship between Hib meningitis and infant mortality in the Western Pacific Region
01020304050
60708090
100
Hon
g K
ong,
SA
R
Japa
n
Kor
ea
Mal
aysi
a
Taiw
an, C
hina
Mon
golia
Vie
t Nam
Phi
lippi
nes
Chi
na
Fren
ch P
olyn
esia Fiji
Van
uatu
Sam
oa
Tong
a
Kiri
bati
Pap
ua N
ew G
uine
a
Sol
omon
Isla
nd
inci
denc
e (/1
0000
0)
0
10
20
30
40
50
60
70
mor
talit
y (/1
000)
Hib meningitis
Infant mortality
It was difficult to find the incidence rate of other diseases caused by Hib (i.e. bacterial pneumonia, cellulites, septic arthritis and epiglottitis) in the Western Pacific Region, except in Australia and New Zealand. Hib is known to be one of the most important causes of pneumonia in Papua New Guinea. In China, Hib is estimated to be the second most common etiological agent for pneumonia among children, after S. pneumoniae.
113
Hib does not cause morbidity and mortality in the neonatal period.
- 37 -
Among the 37 countries and areas in the Western Pacific Region, 22 have introduced Hib vaccination and 17 have introduced it into their routine childhood immunization programmes, with two countries (Macao [China] and Papua New Guinea) planning to introduce it in 2007.
The impact assessment studies of Hib vaccination in Australia report vaccine efficacy of more than 70%. Fiji and New Zealand reported a 32% and a 92% decrease, respectively, of Hib meningitis hospitalization of children under five years of age after Hib vaccination. Most studies on the economic evaluation of Hib immunization show that the benefits exceed the costs; however, the cost–benefit ratio is relatively small compared with other immunization programmes. There is even a study from Spain that reports the cost–benefit ratio to be less than one.
Reliable information required for economic evaluation is still lacking in the Western Pacific Region. However, available information suggests relatively low Hib incidence, low medical costs, and a low valuation placed on life, resulting in less favourable economic evaluation estimates. On the other hand, relatively higher fatalities and lower administrative costs are likely to contribute to a higher cost-benefit ratio. However, it should be kept in mind that, generally, economic evaluation puts more weight on incidence than on the other parameters in a study. One study from the United States of America points out that, when incidence during the pre-vaccine era is assumed to be half the base case, the cost-benefit ratio declines from 5.4 to 1.7. Another study from Spain also found that the cost–benefit ratio declined from 0.89 to 0.6 as the presumed incidence changed from 15 to 10 per 100 000 under-5 population (see Error! Reference source not found.)
114
Table 14. Summary of cost–benefit analyses across regions Western Pacific Region Others
Parameters Estimates Impact on
cost/benefit Estimates Impact on cost/benefit
Incidence Low decrease high increase Fatality High increase /? low decrease /? Medical cost Low decrease high increase Benefit
Life value Generally low (with large variation across countries) decrease high increase
In summary, the cost–benefit ratio of Hib immunization in the WHO Western Pacific Region seems to be lower than in either the WHO Region for the Americas or the WHO European Region. However, this may be due to potential underestimation of Hib incidence in the Western Pacific. In addition, the status of economic development varies substantially across countries, affecting the results of economic evaluation of Hib immunization considerably.
114
Jiménez FJ, et al. Ref. 91.
- 38 -
Finally, cost-benefit analysis is not the only way to set priorities among various health issues, especially in settings with many competing priorities (e.g. a high disease burden due to tuberculosis or diarrhoea) for scarce resources. Therefore, in order to decide whether or not to introduce the conjugate vaccine, priority-setting based on a comparison of the disease burden from varying causes, and on the cost-effectiveness of available interventions, should be considered by individual countries.
5. RECOMMENDATIONS
Countries and areas that have already introduced the Hib vaccine should evaluate the impact of its introduction. This may be needed especially in those countries and areas that introduced the vaccine with external support, in order to sustain the external support and to mobilize domestic financial support for continuation of the vaccination programme. Introduction of Hib vaccine in other countries will depend on the Hib disease burden, the availability of internal or external financial resources, and the functioning of routine immunization services, as measured by three doses of diphtheria-pertussis-tetanus (DPT3) coverage rates. GAVI requires at least a 50% DPT3 coverage rate as a criterion for funding a new vaccine. The coverage level of DPT3 may serve as an indicator of programme management, the capacity of a programme to handle increasing complexity in terms of logistics management and the need for an increased number of contacts with children. The current wastage rates in some national programmes (e.g. Cambodia, the Lao People's Democratic Republic and the Philippines) are very high, due both to poor vaccine logistics management and to undue reliance on outreach visits for service delivery. It is important that programmes are able to deliver the vaccine with minimum wastage rates when considering the introduction of an expensive vaccine such as Hib. In addition, in settings with less than 50% coverage for DPT3 or measles vaccine, increasing coverage with existing vaccines will usually prevent more morbidity than adding a new vaccine, although that fact in no way justifies denial of Hib vaccine where the disease burden is clearly demonstrated to be very high. The addition of a new vaccine for a disease perceived to be a major health problem by communities may improve the credibility of the immunization programme and may potentially increase the demand for and coverage of other vaccines as well.
The results of economic analyses of Western countries were used to derive the incidence level at which vaccine introduction would be cost-effective and justified. Spain showed the lowest cost-benefit ratio, at a relatively low incidence of Hib meningitis of 15 per 100 000 under-5 population.
115 It has been assumed that introduction of the vaccine might not be cost-effective if
the incidence of Hib meningitis were less than 15 per 100 000 under-5 population, however, each country-case should be evaluated independently, taking into account its economic status, the treatment cost, its population’s treatment-seeking behaviour and the cost of long-term sequalae. Also, future studies should include the impact on childhood pneumonia—a major killer of children in the Region, while carrying out an economic evaluation of Hib vaccines. If a country lacks data on its Hib disease burden, it can first begin a hospital-based study for Hib. For countries with a small population (<100 000 for zero to four years) and no disease burden data, the incidence of neighbouring countries could be applied. Thus Macao (China) might be similar to Hong Kong (China); and Cook Islands, Nauru, Tokelau and Tuvalu might be similar to other Pacific island countries and areas.
115
Jiménez FJ, et al. Ref. 91.
- 39 -
Countries with poorly performing NIPs and with no disease burden data could simultaneously work to improve immunization programmes and perform Hib disease burden studies to reduce the time lost in introducing the vaccines.
5.1 Recommendations for individual countries
Hong Kong (China), Japan, the Republic of Korea and Singapore need to perform independent economic evaluation analyses to make an informed decision about introducing Hib vaccine in their NIP. The disease burdens need to be further clarified in China, the Philippines and Viet Nam, using innovative study methods. Disease burden data should be used along with cost-effectiveness analyses to guide the decision regarding introduction of the Hib vaccine in these three large countries.
Kiribati, Nauru, Samoa, Solomon Islands and Tuvalu should introduce Hib vaccination into their NIP if sufficient funds can be mobilized, either from external or internal sources. For example, Kiribati and Solomon Islands are eligible to receive financial assistance from GAVI to introduce the Hib vaccine, but did not avail of it in Phase I. Both these countries should exploit the opportunity provided by GAVI Phase II to introduce the vaccine.
Cambodia and the Lao People's Democratic Republic do not have any disease burden data and have relatively low DPT immunization coverage rates. These countries need to strengthen their NIPs and begin disease burden studies on Hib, preferably in combination with other disease surveillance studies (e.g. for Japanese encephalitis).
Papua New Guinea, the Philippines and Vanuatu seem to have relatively high incidences of Hib disease and low DPT vaccination rates; they need to strengthen their NIP systems and include Hib vaccination in their NIPs if the necessary resources can be mobilized.
Although Niue, a self-governing state in free association with New Zealand, introduced the Hib vaccine in 2000, Cook Islands, another state in free association with New Zealand, and Tokelau, a New Zealand territory—with potentially similar Hib disease burdens as Niue—are yet to do so. Advocacy should be carried out with relevant stakeholders to mobilize sufficient resources to help introduce the vaccine in these countries.
6. ACKNOWLEDGEMENTS
This report was prepared and finalized under the overall supervision and guidance of Dr Manju Rani, Scientist, WHO Western Pacific Regional Office.
The Regional Office would like to express sincere thanks to Dr Ki Moran who prepared the first draft, and greatly appreciates the efforts of Zhenyu Quan, lecturer at Yanbian University, China, in assisting Dr Moran in summarizing the findings from literature in Chinese language. Ooi Wei Ming (Melbourne University, Australia) provided an excellent review of the literature on Haemophilus influenzae type b in Asia and of a study undertaken in southern Malaysia evaluating the impact of Hib vaccine introduction. The Regional Office is also grateful to Paul E Kilgore, International Vaccine Institute, for helping with Hib literature and recent research information, as well as for reviewing the paper; to Batmunkh Nyambat, International Vaccine Institute, for
- 40 -
providing useful information about Mongolia; and to Ms Valerie Begley for providing excellent editorial support.
7. BIBLIOGRAPHY BY TOPIC AND COUNTRY
Hib disease burden
American Samoa: No studies
Australia
Gilbert GL, Clements DA, Broughton SJ. Haemophilus influenzae type b infections in Victoria, Australia, 1985 to 1987. Pediatric Infectious Disease Journal, 1990, 9(4):252-277.
Hanna JN. The epidemiology of invasive Haemophilus influenzae infections in children under five years of age in the Northern Territory: a three-year study. Medical Journal of Australia, 1990, 152(5):234-6, 238, 240.
Hanna JN, Wild BE. Bacterial meningitis in children under five years of age in Western Australia. Medical Journal of Australia, 1991, 155(3):160-164.
Horby P, et al. Progress towards eliminating Hib in Australia: An evaluation of Haemophilus influenzae type b prevention in Australia, 1 July 1993 to 30 June 2000. Communicable Diseases Intelligence,2003, 27(3):324-341.
McGregor AR, et al. Invasive Haemophilus influenzae infection in the Australian Capital Territory region. Medical Journal of Australia, 1992, 156(8):569-571.
McIntyre PB, Leeder SR, Irwig LM. Invasive Haemophilus influenzae type b disease in Sydney children 1985-1987: a population-based study. Medical Journal of Australia, 1991, 154(12):832-837.
Brunei Darussalam: No studies
Cambodia: No studies
China
Levine OS, et al. Haemophilus influenzae type b and Streptococcus pneumoniae as causes of pneumonia among children in Beijing, China. Emerging Infectious Diseases, 2000, 6(2):165-170.
Wang YJ, et al. Relative frequency of Haemophilus influenzae type b pneumonia in Chinese children as evidenced by serology. Pediatric Infectious Disease Journal, 2002, 21(4):271-277.
Yang Y, et al. Study on Haemophilus influenzae type b diseases in China: the past, present and future. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S159-165.
Yang Y, et al. Seroetiology of acute lower respiratory infections among hospitalized children in Beijing. Pediatric Infectious Disease Journal, 2001, 20(1):52-58.
Yang Y, et al. Acute bacterial meningitis in children in Hefei, China 1990-1992. Chinese Medical Journal (English edition), 1996,109(5):385-388.
- 41 -
China (Taiwan)
Wang CH, Lin TY. Invasive Haemophilus influenzae diseases and purulent meningitis in Taiwan. Journal of the Formosan Medical Association, 1996, 95(8):599-604.
Chen MK, et al. Prospective surveillance of children with invasive Haemophilus influenzae disease in Taiwan. Journal of Microbiology, Immunology, and Infection, 1999, 32(4):257-260.
Shao PL, et al. Epidemiology of Haemophilus influenzae type b meningitis in Taiwan, 1997 and 2000. Journal of Microbiology, Immunology, and Infection, 2004, 37(3):164-168.
Hong Kong (China)
Lau YL, et al. Invasive Haemophilus influenzae type b infections in children hospitalized in Hong Kong, 1986-1990. Hong Kong Hib Study Group. Acta Paediatrica, 1995, 84(2):173-176.
Lau YL, et al. Haemophilus influenzae type b infections in Hong Kong. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S165-169.
Sung RY, et al. Meningitis in Hong Kong children, with special reference to the infrequency of haemophilus and meningococcal infection. Journal of Paediatrics and Child Health, 1997, 33(4):296-299.
China (Macao): No studies
Cook Islands: No studies
Fiji
Wilson N, et al. Estimating the Haemophilus influenzae type b (Hib) disease burden and the impact of Hib vaccine in Fiji. Vaccine, 2003, 21(17-18):1907-1912.
French Polynesia
Russell FM, et al. High incidence of Haemophilus influenzae type b infection in children in Pacific island countries. Clinical Infectious Diseases, 2003, 37(12):1593-1599.
Guam: No studies
Japan
Ishikawa T, et al. Epidemiology of bacterial meningitis in children: Aichi Prefecture, Japan, 1984-1993. Pediatric Neurology, 1996, 14(3):244-250.
Kamiya H, et al. Childhood bacterial meningitis in Japan. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S183-185.
Nakano T, et al. Incidence of Haemophilus influenzae type b meningitis in Mie prefecture, Japan. Pediatrics International, 2001, 43(3):323-324.
Kiribati
- 42 -
Russell FM, et al. High incidence of Haemophilus influenzae type b infection in children in Pacific island countries. Clinical Infectious Diseases, 2003, 37(12):1593-1599.
The Lao People’s Democratic Republic: No studies
Malaysia
Choo KE, et al. Pyogenic meningitis in hospitalized children in Kelantan, Malaysia. Annals of Tropical Paediatrics, 1990, 10(1):89-98.
Hussain IHMI, et al. Haemophilus influenzae meningitis in Malaysia. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S189-1990.
Khairulddin NY, Choo KE, Johari MR. Epidemiology of Haemophilus influenzae invasive disease in hospitalised Kelantanese children, 1985-1994. Singapore Medical Journal, 1999, 40(2):96-100.
The Marshall Islands: No studies
Micronesia, the Federated States of: No studies
Mongolia: Personal communication
Commonwealth of the Northern Mariana Islands: No studies
Nauru: No studies
New Caledonia
Anglaret X, et al. Invasive Haemophilus influenzae disease of Melanesian and Caucasian children in New Caledonia. Pediatric Infectious Disease Journal, 1993, 12(10):888-889.
New Zealand
Voss L, Lennon D, Gillies M. Haemophilus influenzae type b disease in Auckland children 1981-87. New Zealand Medical Journal, 1989, 102(865):149-151.
Wilson N, et al. The beneficial impact of Hib vaccine on disease rates in New Zealand children. New Zealand Medical Journal, 2002, 115(1159):1-7.
Niue: No studies
Palau: No studies
Papua New Guinea
Gratten M, et al. The etiology of purulent meningitis in highland children: a bacteriological study. Papua New Guinea Medical Journal, 1985, 28(4):233-240.
Gratten M, Montgomery J. The bacteriology of acute pneumonia and meningitis in children in Papua New Guinea: assumptions, facts and technical strategies. Papua New Guinea Medical Journal, 1991, 34(3):185-198.
- 43 -
Lehmann D, et al. Etiology and clinical signs of bacterial meningitis in children admitted to Goroka Base Hospital, Papua New Guinea, 1989-1992. Annals of Tropical Paediatrics, 1999, 19(1):21-32.
Lehmann D. Epidemiology of acute respiratory tract infections, especially those due to Haemophilus influenzae, in Papua New Guinean children. Review. The Journal of Infectious Diseases, 1992, 165 Suppl 1:S20-25.
Duke T. Haemophillus influenzae type b meningitis: how much better is prevention than cure? Papua New Guinea Medical Journal, 2002 Sept-Dec, 45(3-4):213-218.
The Philippines
Reyes ER. Suppurative bacterial meningitis: a 6-year study. Philippine Journal of Microbiology and Infectious Disease, 1986, 15:73-76.
Santana RT, et al. Clinical and laboratory profile of bacterial meningitis in Filipinos: a six year review. Journal of Tropical and Geographical Neurology, 1992, 2:151-156.
Santana-Arciaga R, et al. The epidemiology of invasive Haemophilus influenzae disease among Filipinos. Philippine Journal of Microbiology and Infectious Diseases, 1994, 23(2):52-59.
Limcangco MR, Salole EG, Armour CL. Epidemiology of Haemophilus influenzae type b meningitis in Manila, Philippines, 1994 to 1996. Pediatric Infectious Disease Journal, 2000, 19(1):7-11.
Lupisan SP, et al. Incidence of invasive Haemophilus influenzae type b infections in Filipino children. Pediatric Infectious Disease Journal, 2000, 19(10):1020-1022.
The Republic of Korea
Kim JS, et al. Incidence of Haemophilus influenzae type b and other invasive diseases in South Korean children. Vaccine, 2004, 22(29-30):3952-3962.
Kim KH, et al. The causative organisms of bacterial meningitis in Korean children, 1986-1995. Journal of Korean Medical Science, 1998, 13(1):60-64.
Lee HJ. Epidemiology of systemic Haemophilus influenzae disease in Korean children. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S185-189.
The Pitcairn Islands: No studies
- 44 -
Samoa
Russell FM, et al. High incidence of Haemophilus influenzae type b infection in children in Pacific island countries. Clinical Infectious Diseases, 2003, 37(12):1593-1599.
Singapore
Lee YS, et al. Invasive Haemophilus influenzae type b infections in Singapore children: a hospital-based study. Journal of Paediatrics and Child Health, 2000, 36(2):125-127.
Solomon Islands
Russell FM, et al. High incidence of Haemophilus influenzae type b infection in children in Pacific island countries. Clinical Infectious Diseases, 2003, 37(12):1593-1599.
Tokelau: No studies
Tonga
Russell FM, et al. High incidence of Haemophilus influenzae type b infection in children in Pacific island countries. Clinical Infectious Diseases, 2003, 37(12):1593-1599.
Tuvalu: No studies
Vanuatu
Carroll K, Carroll C. The epidemiology of bacterial meningitis occurring in a Pacific Island population. Papua New Guinea Medical Journal, 1993, 36(3):234-242.
Viet Nam
Tran TT, et al. The etiology of bacterial pneumonia and meningitis in Vietnam. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S192-194.
Anh D, et al and the Vietnam Invasive Bacterial Disease Surveillance Network. Haemophilus influenzae type b meningitis among children in hanoi, vietnam: epidemiologic patterns and estimates of h. Influenzae type b disease burden. American Journal of Tropical Medicine and Hygiene, Mar 2006, 74: 509-515.
Wallis and Futuna: No studies
Hib vaccination impact
Australia
Bower C, et al. Measuring the impact of conjugate vaccines on invasive Haemophilus influenzae type b infection in Western Australia. Australian and New Zealand Journal of Public Health, 1998, 22(1):67-72.
Hanna JN. Impact of Haemophilus influenzae type b (Hib) vaccination on Hib meningitis in children in Far North Queensland, 1989 to 2003. Communicable diseases intelligence, 2004, 28(2):255-257.
- 45 -
Fiji
Wilson N, et al. Estimating the Haemophilus influenzae type b (Hib) disease burden and the impact of Hib vaccine in Fiji. Vaccine, 2003, 21(17-18):1907-1912.
New Zealand
Wilson N, et al. The beneficial impact of Hib vaccine on disease rates in New Zealand children. New Zealand Medical Journal, 2002, 115(1159):1-7.
Economic evaluation
Asia
Miller MA. An assessment of the value of Haemophilus influenzae type b conjugate vaccine in Asia. Pediatric Infectious Disease Journal, 1998, 17(9 Suppl):S152-159.
Australia
Harris A, et al. The burden of Haemophilus influenzae type b disease in Australia and an economic appraisal of the vaccine PRP-OMP. Medical Journal of Australia, 1994, 160(8):483-488.
McIntyre P, Hall J, Leeder S. An economic analysis of alternatives for childhood immunisation against Haemophilus influenzae type b disease. Australian Journal of Public Health, 1994, 18(4):394-400.
Malaysia
Hussain IHMI, et al. Cost-Benefit analysis of Haemophilus influenzae vaccination programme in Malaysia. Buletin Kasiharan Masyakat Jilid, 1999, 5:79-89.
The Philippines
Limcangco MR, et al. Cost-benefit analysis of a Haemophilus influenzae type b meningitis prevention programme in The Philippines. Pediatric Infectious Disease Journal, 2001, 19(4):391-400.
Tonga
Brinsmead R. Economic evaluation of the introduction of Haemophilus influenzae type b(Hib) and rubella vaccine to the kingdom of Tonga. 2003 (unpublished paper).
- 46 -
Annex 1. Characteristics of the cited studies from the East Asia subregion
Country Ref Year Data collection Study subjects Bias and Counter measures
86-90 Retrospective survey of hospital records (microbiology and paediatrics)
territory-wide hospital inpatients
Good healthcare access and quality laboratory capacity → Good representativeness
A/B abuse problem → under-estimation
Hong Kong (China)
84-93 Retrospective survey of hospital records
Inpatients of only one referral hospital in New Territory East
Unclear representativeness
97-98 Prospective sentinel hospital surveillance
Inpatients of sentinel hospitals in Mie prefecture
A/B abuse problem → Possible under-estimation No detailed information about the selected hospitals → unclear
representativeness 94 Retrospective survey of
hospital records Inpatients (all hospitals in six prefectures out of forty seven)
Higher participation rates with higher incidence and technical capacity → Serious selection bias
No serotype information
Japan
84-93 Retrospective survey of hospital records
Inpatients in paediatrics (Aichi pref.)
Variable participation rates and unclear information about catchment area of referral centres → Possible selection bias
99-01 Prospective and active surveillance among all clinics and hospitals
Patients who were referred to tertiary paediatric hospitals in Jeonbuk province
Vaccine in private sector, doctors’ strike for three months, and A/B abuse → Under-estimation
Good representativeness in the provinces, however questionable at nation-wide level
86-95 Retrospective survey of hospital records
Patients in 13 general and university hospitals around Seoul
Relatively severe cases in referral hospitals → Lack of representativeness
The Republic of Korea
86-96 Retrospective survey of hospital records
Patients in one university hospital in Seoul
One hospital without clear catchment area → lack of representativeness
- 47 -
Singapore 90-95 Retrospective survey of hospital records (bacteriological records + clinical information)
Patients of the National University Hospital
No mention of representativeness
97→00
Retrieval of the National Health Insurance Research Data (systematic sampling of one-twentieth of all impatient medical care records of every hospital) and medical center database (inpatients + outpatients)
Province-wide inpatients
Coverage of national health insurance > 96% → good representativeness
A/B abuse → possibility of under-estimation, however, extrapolation based on the medical centre records (outpatient + inpatient information)
96-97 (abstracts only)
Taiwan (China)
92-94 Retrospective survey of hospital records
Almost all inpatients in Taiwan (China)
Good representativeness A/B abuse & variability of laboratory ability→ possibility of
under-estimation 95 Retrospective survey of
hospital records Patients of 5 paediatric departments in 5 states of 13 states
lower rates of lumbar puncture due to cultural issues and no mention of representativeness of sampled hospitals → selection bias
85-94 Retrospective survey of hospital records (microbiology)
Inpatients of one tertiary hospital (out of two) in Kelantan state
Infrequent specimen sampling, lower quality of laboratory and A/B abuse → possibility of under-estimation
No mention of representativeness
Malaysia
85-87 Retrospective survey of hospital records
Inpatients of one tertiary hospital in Kelantan state
No mention of methodological limitation Problem in representativeness
- 48 -
China 88-89 90-92
Prospective hospital surveillance
Inpatients of Beijing Children’s Hospital and all paediatric clinics in Hefei
Hospital survey in the best facility in China → possibility of selection bias
All paediatric clinics in Hefei → representativeness (corresponding to community-wide survey)
Under-detection due to A/B → adoption of immunochemical methods (for capsular polysaccharides)
94-96 Retrospective survey of
hospital records Inpatients in tertiary hospitals in Manila
Selection due to inclusion of only tertiary hospital patients →→ check thorough referral from primary or secondary hospitals by interview with administrators
Low retention rate (63%) of admission records and A/B abuse → possibility of under-estimation
The Philippines
94-96 Prospective hospital surveillance
Patients in one government referral hospital in Tagbiliran city
Unclear catchment area → possibility of selection bias Consideration of taking charge of patients in catchment A/B abuse → possibility of under-estimation
Good representativeness and training for surveillance staffs
00-02 Prospective population based study
Urban Hanoi Viet Nam
95-96 Retrospective survey of hospital records
Inpatients in one hospital in Ho Chi Mihn City
One central hospital & unclear catchment area→ possibility of selection bias (especially, in term of relative exclusion of rural population)
* Personal communication
- 49 -
Annex 2. Characteristics of the cited studies from the Oceania subregion
Country Ref Year Data collection Study subjects Bias and countermeasures
93-00 National Notifiable Disease Surveillance System + Hib case surveillance scheme
All patients from the regions starting NNDSS in 1991
Differences in adoption of NNDSS across states → Possibility of under-estimation
84-90 Retrospective survey of hospital records
Inpatient of central hospital in Capital Territory
Good representativeness (i.e., low possibility of underestimation due to missed cases by private clinics)
84-88 Retrospective survey: hospital data from Health Department + mortality data from Registrar General + microbiology data at only one specialty + notification system in Health Department
Western Australia No mention of methodology but may be good representativeness, minimal under-estimation
85-87 Retrospective survey: all 21 hospitals + 17 laboratories (86% coverage) + discharge records from the three largest hospitals (48% coverage) + death data
Sydney Low possibility of under-estimation (low culture-negative rate, comparable case-fatality)
Good representativeness
Australia
85-87 Retrospective survey of medical records from Royal Children’s Hospital (with only paediatric intensive care unit) + questionnaire survey for all regional paediatricians, lab, and medical record departments with paediatric units
Victoria Good representativeness
- 50 -
85-87 Retrospective survey of hospital records
Inpatients of five regional hospitals in Northern Territory
No mention of methodology
French Polynesia
Ministry of health data (secondary citation)
New Caledonia
89-91 Retrospective survey of hospital records
Inpatients in only paediatrics (all laboratory work done in France)
Representativeness No serotyping
(88-93) →(95-00)
Retrieval of national mortality data and national hospitalization data + national reference laboratory
Inpatients or deceased from Hib throughout the country
Hib designated as notifiable disease in 1996 and A/B abuse → possibility of under-estimation (but, robust trend)
New Zealand
81-87 Retrospective survey of hospital records
Inpatients of one central children’s hospital in Auckland
Possibility of underestimation of epiglotttis
Fiji 92-93 RAT (hospitalization, mortality data)
Inpatients or deceased throughout the country
Reasonable reliability of data source
Kiribati RAT (hospitalization, mortality data)
Inpatients or deceased throughout the country
Consideration of the proportion of lumbar puncture and culture negativity
Unlikely healthcare access problem (low child mortality)
Pneumonia: meningitis ratio assumption → sensitivity analysis
Samoa RAT (hospitalization, mortality data)
Inpatients or deceased throughout the country
No serotyping → assumption of the proportion of Hib (95%)
Consideration of the proportion of lumbar puncture and culture negativity
Unlikely healthcare access problem (low child mortality)
Pneumonia: meningitis ratio assumption → sensitivity analysis
- 51 -
Tonga RAT (hospitalization, mortality data)
Inpatients or deceased throughout the country
No serotyping → assumption of the proportion of Hib (95%)
Consideration of the proportion of lumbar puncture and culture negativity
Unlikely healthcare access problem (low child mortality)
Pneumonia: meningitis ratio assumption → sensitivity analysis
Vanuatu 88-91 C-P All cases of bacterial meningitis admitted to a single hospital in Tanna Island during study period, with a total population of 20 705
(abstracts)
89-92 Prospective survey of paediatrics clinic
Inpatients of one hospital in Goroka town, Eastern Highlands Province
specimen collection problem and prior A/B treatment → possibility of under-estimation
no mention of representativeness
Papua New Guinea
78-87 H-R (abstracts) Solomon Island
RAT (hospitalization, mortality data)
Inpatients or deceased throughout the country
No serotyping → assumption of the proportion of Hib (95%)
Consideration of the proportion of lumbar puncture and culture negativity
Unlikely healthcare access problem (low child mortality)
Pneumonia: meningitis ratio assumption → sensitivity analysis
Note : a. C=community-based, H=hospital-based, P=prospective, Recommended=retrospective; RAT Rapid Assessment Tool developed by
WHO. IM=meningitis incidence method, CMR=child mortality rate method. b. annual incidence (per 105) of Hib meningitis in children under 5 years of age, [ ] invasive Hib disease.