www.metcardi o.org Giuseppe Biondi Zoccai University of Turin, Turin, Italy METCARDIO, Turin, Italy [email protected]Educational Fellowship in PCI for Young Interventionalists - Certified Training Course (EAPCI, SCAI, GISE) - Bologna, 25/9/2008 – 14:30-17:30 (15’) LEFT MAIN/MULTIVESSEL DISEASE: LEFT MAIN/MULTIVESSEL DISEASE: WHEN PERCUTANEOUS CORONARY WHEN PERCUTANEOUS CORONARY INTERVENTION, WHEN SURGERY? INTERVENTION, WHEN SURGERY?
Transcript
www.metcardio.org
Giuseppe Biondi Zoccai
University of Turin, Turin, ItalyMETCARDIO, Turin, Italy
LEFT MAIN/MULTIVESSEL DISEASE: LEFT MAIN/MULTIVESSEL DISEASE:
WHEN PERCUTANEOUS CORONARY WHEN PERCUTANEOUS CORONARY
INTERVENTION, WHEN SURGERY?INTERVENTION, WHEN SURGERY?
www.metcardio.org
LEARNING GOALS
• Should I bother with left main (LM)/ multivessel disease (MVD)?
• Who is the winner between PCI and CABG in LM/MVD?
• When is surgery appropriate for LM/MVD?
• When is PCI appropriate for LM/MVD?
www.metcardio.org
LEARNING GOALS
• Should I bother with left main (LM)/ multivessel disease (MVD)?
• Who is the winner between PCI and CABG in LM/MVD?
• When is surgery appropriate for LM/MVD?
• When is PCI appropriate for LM/MVD?
www.metcardio.org
PREVALENCE AND PROGNOSIS OF LM/MVD DISEASE
Chaitman et al, Circulation 1981;64:360-367; Yusuf et al, Lancet 1994;344:563-570;
Melidonis et al, Angiology 1999;50:997-1006
• Out of 1000 pts undergoing coronary angio: 30-80 will have unprotected LM, 20-60 protected LM, a total of 300-700 will have MVD
• Unprotected LM has, historically, a 36% 5-year mortality rate with medical Rx only, which is reduced to 12% after CABG (p=0.004)
• Corresponding figures for 3VD are 18% vs 10% (p<0.001), and for 2VD are 12% vs 10% (p=0.45)
• Whenever LV function is abnormal, 5-year mortality with medical Rx only is 25%, which is reduced to 14% after CABG (p=0.02)
www.metcardio.org
LEARNING GOALS
• Should I bother with left main (LM)/ multivessel disease (MVD)?
• Who is the winner between PCI and CABG in LM/MVD?
• When is surgery appropriate for LM/MVD?
• When is PCI appropriate for LM/MVD?
www.metcardio.org
WHO’S THE WINNER BETWEEN PCI AND SURGERY IN LM-MVD?
www.metcardio.org
ARE THEY ENEMIES OR FRIENDS?
www.metcardio.org
LET’S LOOK AT THE PAST…
www.metcardio.org
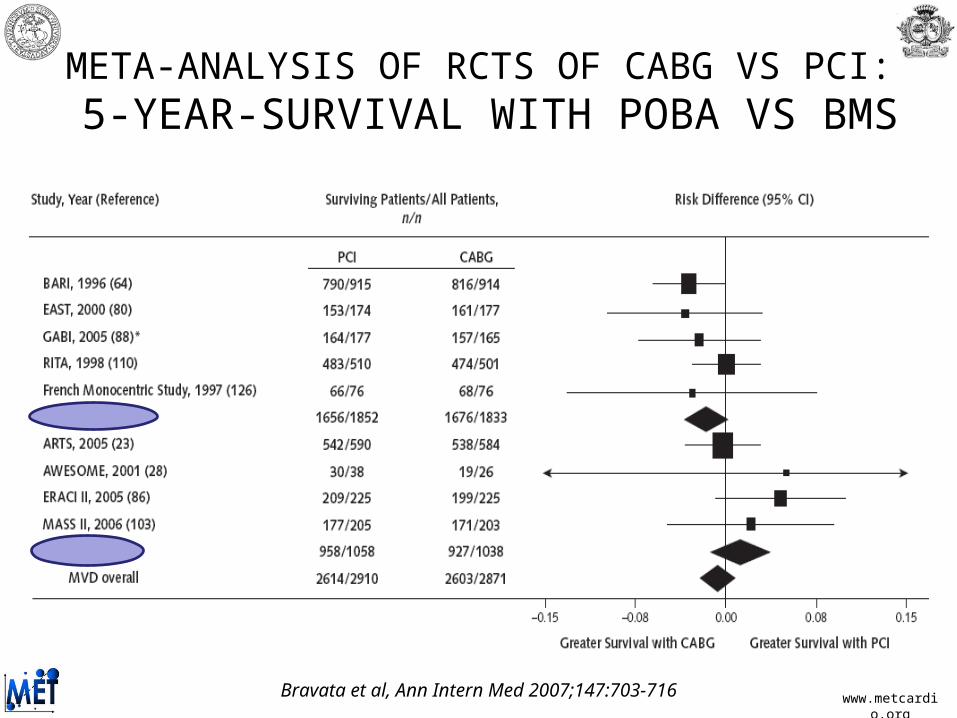
META-ANALYSIS OF RCTS OF CABG VS PCI: 5-YEAR-SURVIVAL WITH POBA VS BMS
Bravata et al, Ann Intern Med 2007;147:703-716
www.metcardio.org
META-ANALYSIS OF RCTS OF CABG VS PCI: 5-YEAR-SURVIVAL WITH POBA VS BMS
Bravata et al, Ann Intern Med 2007;147:703-716
www.metcardio.org
META-ANALYSIS OF RCTS OF CABG VS PCI: 5-YEAR-SURVIVAL IN DIABETICS
Bravata et al, Ann Intern Med 2007;147:703-716
www.metcardio.org
HOWEVER, PCI WITH BMS WAS INFERIOR TO CABG FOR THE
RISK OF REPEAT PCI/CABG
Biondi-Zoccai et al, Ital Heart J 2003;4:271-280
www.metcardio.org
WHAT ABOUT THE PRESENT…
www.metcardio.org
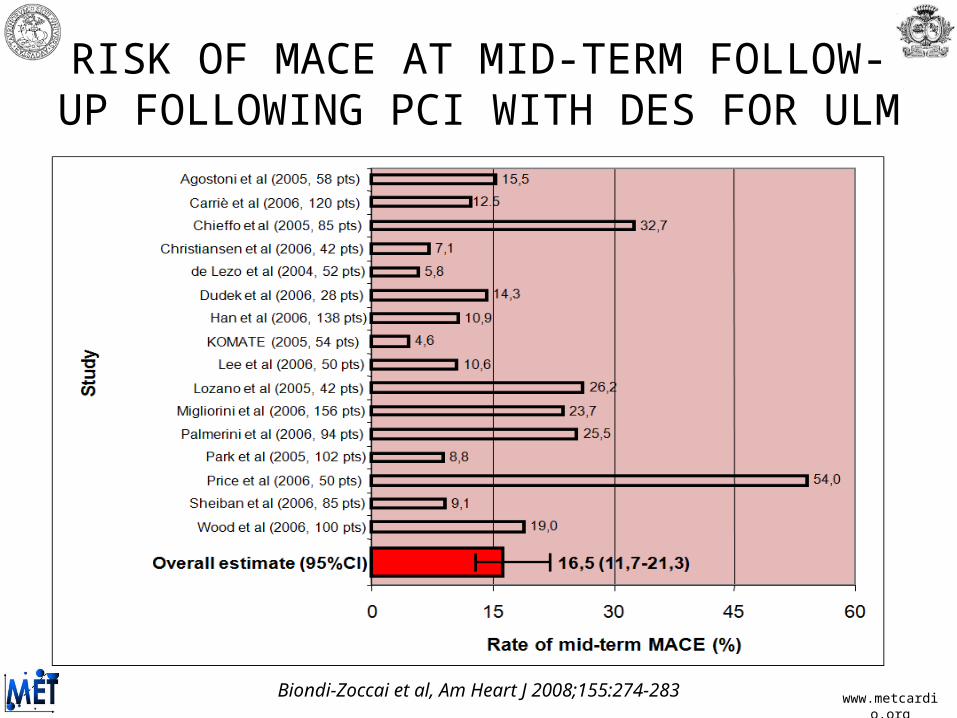
RISK OF MACE AT MID-TERM FOLLOW-UP FOLLOWING PCI WITH DES FOR ULM
Biondi-Zoccai et al, Am Heart J 2008;155:274-283
www.metcardio.org
IMPACT OF LESION LOCATION AND PATIENT RISK FEATURES ON OUTCOMES OF ULM PCI
Biondi-Zoccai et al, Am Heart J 2008;155:274-283
www.metcardio.org
SYNTAX REGISTRIES
Mohr et al, ESC 2008
PCI REGISTRY (N=192) CABG REGISTRY (N=644)
www.metcardio.org
SYNTAX TRIAL: 12-MONTH RESULTS
Serruys et al, ESC 2008
%
P=0.37 P=0.11 P=0.003
P<0.001
P=0.0015
P=0.89
www.metcardio.org
SYNTAX TRIAL: 12-MONTH MACES
Serruys et al, ESC 2008
www.metcardio.org
SYNTAX TRIAL: DM VS NON-DM
Serruys et al, ESC 2008
www.metcardio.org
LEARNING GOALS
• Should I bother with left main (LM)/ multivessel disease (MVD)?
• Who is the winner between PCI and CABG in LM/MVD?
• When is surgery appropriate for LM/MVD?
• When is PCI appropriate for LM/MVD?
www.metcardio.org
ESC 2005 GUIDELINES
Silber et al, Eur Heart J 2005;26:804-847
www.metcardio.org
ESC 2005 GUIDELINES
Silber et al, Eur Heart J 2005;26:804-847
THUS CABG IS RECOMMENDED INSTEAD OF PCI IN MOST CASES OF CAD IN
DIABETICS, IN MOST CASES OF MVD, AND ALL BUT A FEW CASES OF ULM…however, the guidelines are based mainly on
differences in repeat revascularization rate
www.metcardio.org
MY SURGICAL MUST DOs• Concomitant compelling indication to
cardiothoracic surgery (eg MR)
• Absolute contraindications to antiplatelet therapy
• Previous failed PCI attempts (especially LAD)
• Multivessel CTO or CTO
involving proximal-mid LAD
• Very high SYNTAX score (?!)
www.metcardio.org
WHAT ABOUT ITALIAN INTERVENTIONISTS?
Sheiban et al, Int J Cardiol 2008 – in press
Results of run-in survey for the RITMO Study on the management of unprotected left main disease in Italy (data limited to 2006)
RESPONDERSRESPONDERS NON-RESPONDERSNON-RESPONDERSNumber of centers 45 195Total coronary angiographies 61,370 198,906Coronary angiographies per center 1363±866 1036±630Total PTCA 31,699 92,392PTCA per center 704±479 499±308Total multivessel PTCA 7,870 19,947Multivessel PTCA per center 183±163 109±106Total PTCA with stenting 28,961 85,732PTCA with stenting per center 673±428 465±288Total PTCA with drug-eluting stenting 18,357 46,498PTCA with drug-eluting stenting per center 426±350 261±200ULM diagnosed at angiography per center, of total angio 5.0% (1.9-15.8) -ULM treated with CABG per center, out of total ULM at angio 50.0% (9.3-99.1) -ULM treated with PTCA per center, out of total ULM at angio 20.0% (0-80.8) -
www.metcardio.org
LEARNING GOALS
• Should I bother with left main (LM)/ multivessel disease (MVD)?
• Who is the winner between PCI and CABG in LM/MVD?
• When is surgery appropriate for LM/MVD?
• When is PCI appropriate for LM/MVD?
www.metcardio.org
CAN WE CAN DO WHATEVER THE SURGEON DOES?
www.metcardio.org
CAN YOU DO IT?
85-year-old 85-year-old ♂ with with non-STEMI and non-STEMI and true trifurcational true trifurcational unprotected LM unprotected LM disease, high disease, high
surgical risk and surgical risk and LVEF 45%LVEF 45%
www.metcardio.org
ACTUALLY, IT CAN BE DONE,
BUT SHOULD I DO IT?
BEFORE PCIBEFORE PCI AFTER PCI WITH AFTER PCI WITH 4 STENTS4 STENTS
Sheiban et al, Catheter Cardiovasc Interv 2008 – in press
www.metcardio.org
ESC 2005 GUIDELINES
Silber et al, Eur Heart J 2005;26:804-847
www.metcardio.org
ESC 2005 GUIDELINES
Silber et al, Eur Heart J 2005;26:804-847
THUS THE ROLE OF PCI IS LIMITED IN MOST CASES OF CAD IN DIABETICS, IN MOST CASES OF MVD, AND ALL BUT A FEW CASES OF ULM
…however, the guidelines are based mainly on differences in repeat revascularization rates
www.metcardio.org
MY PCI MUST DOs• Previous CABG (especially if redo already
• Ongoing STEACS with culprit lesion amenable to primary PCI
• Patients refuses CABG (?!)
but provided patient and referring colleagues are consenting!
www.metcardio.org
MY EQUIPOISE• Non-bifurcational ULM with high surgical risk
• Multivessel but focal disease with only A-B2 lesions, or non-challenging C lesions
• Good LV function
• Very young or very old
• Depending also on need for and likelihood of completeness of revascularization
but still provided patient and referring colleagues are consenting!
www.metcardio.org
TAKE HOME MESSAGES
www.metcardio.org
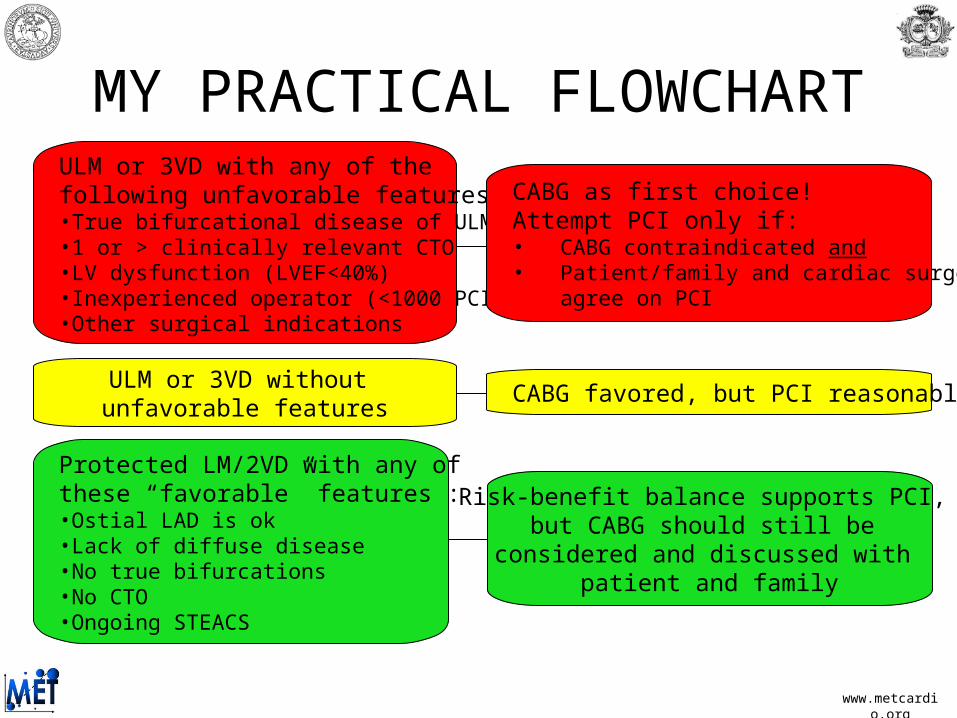
MY PRACTICAL FLOWCHARTULM or 3VD with any of the following unfavorable features:•True bifurcational disease of ULM•1 or > clinically relevant CTO•LV dysfunction (LVEF<40%)•Inexperienced operator (<1000 PCI)•Other surgical indications
CABG as first choice! Attempt PCI only if:• CABG contraindicated and• Patient/family and cardiac surgeon
agree on PCI
CABG favored, but PCI reasonableULM or 3VD without unfavorable features
Risk-benefit balance supports PCI, but CABG should still be
considered and discussed with patient and family
Protected LM/2VD with any of these “favorable” features :•Ostial LAD is ok•Lack of diffuse disease•No true bifurcations•No CTO•Ongoing STEACS
www.metcardio.org
A. 1ST STEP IN CRISIS MANAGEMENT IS PREVENTING THE CRISIS: FOLLOW
GUIDELINES UNLESS YOU ARE JUSTIFIED …
www.metcardio.org
B. COLLABORATIVE DECISON-MAKING IN ALL BUT CLEAR-CUT CASES: INVOLVE OTHER INTERVENTIONAL COLLEAGUES, NON-INVASIVE CARDIOLOGISTS, AND SURGEONS
www.metcardio.org
C. NEVER FORCE TOO MUCH…EITHER INDICATIONS, DEVICES, TECHNIQUES, OR ANCILLARY THERAPY (EG ANTI-THROMBOTIC RX)
www.metcardio.org
For further slides on these topics please feel free to visit the