U.S. Department of Justice Office of Justice Programs Office of Juvenile Justice and Delinquency Prevention Youth With Mental Health Disorders: Issues and Emerging Responses Also ◆ Wraparound Milwaukee Program ◆ Suicide Prevention in Juvenile Facilities Volume VII • Number 1
Transcript
U.S. Department of Justice
Office of Justice Programs
Office of Juvenile Justice and Delinquency Prevention
Youth With Mental HealthDisorders: Issues andEmerging Responses
Also◆ Wraparound Milwaukee Program
◆ Suicide Prevention inJuvenile Facilities
Volume VII • Number 1
From the Administrator
If we are to succeed in preventing and reducing juvenile delinquency, we mustaddress not only the offenses that bring certain youth to the attention of the juvenilejustice system but the underlying problems they face, including the mental healthproblems that affect so many youth in the juvenile justice system.
The increased attention recently accorded the mental health needs of youth in thejuvenile justice system, noted by Joseph Cocozza and Kathleen Skowyra, is as wel-come as it is overdue. We need to learn much more about “Youth With MentalHealth Disorders” who are involved with the juvenile justice system so that we mayenhance the quality of the services provided them.
Solving these problems requires designing and implementing effective treatmentmodels. “Wraparound Milwaukee,” as Bruce Kamradt reports, has successfully inte-grated a broad array of services to better serve youth with mental health needs whohave been adjudicated delinquent. I am sure you will find this program and its resultsof interest.
The mental health needs of juveniles in custody is another area of concern to juve-nile justice practitioners that needs to be addressed. Suicide is a particularly disturb-ing manifestation of unmet mental health needs, especially when it occurs duringconfinement. Lindsay Hayes offers constructive recommendations for “Suicide Pre-vention in Juvenile Facilities” and for providing mental health services to the youthconfined in those facilities.
As the above articles illustrate, youth challenged with interrelated mental health dis-orders and delinquent behaviors need our help to get their lives back on track.OJJDP has included a number of initiatives and programs to this end in its Compre-hensive Plan for Fiscal Year 2000, which are described in the journal’s In Brief section.
It is my hope that the knowledge and insights offered by this issue will enlighten ourefforts to assist youth with mental health disorders in the juvenile justice system.
John J. WilsonActing AdministratorOffice of Juvenile Justiceand Delinquency Prevention
Roberta Dorn, DirectorState Relations andAssistance Division
Eileen M. Garry, DirectorInformation Dissemination Unit
Charlotte A. Kerr, Acting DirectorResearch and ProgramDevelopment Division
Ronald Laney, DirectorMissing and Exploited
Children’s Program
Emily Martin, DirectorTraining and Technical
Assistance Division
Executive EditorEileen M. Garry
Managing EditorCatherine Doyle
Senior EditorEarl E. Appleby, Jr.
Production EditorLeila Wieser
Juvenile Justice (ISSN 1524–6647)is published by the Office of Juve-nile Justice and DelinquencyPrevention (OJJDP) to advanceits mandate to disseminate infor-mation regarding juvenile delin-quency and prevention programs(42 U.S.C. 5652).
FEATURESYouth With Mental Health Disorders: Issues and Emerging Responsesby Joseph J. Cocozza and Kathleen Skowyra ................................................... 3
Tragic mass homicides by juveniles, documented cases of neglect and inadequate ser-vices, and Federal policy initiatives focusing on providing systems of care for at-riskjuveniles have propelled mental health issues among juvenile offenders into theheadlines.
Wraparound Milwaukee: Aiding Youth With Mental Health Needsby Bruce Kamradt .............................................................................. 14
Finding effective treatment models for youth in the juvenile justice system who haveserious emotional, mental health, and behavioral needs can be difficult. WraparoundMilwaukee’s innovative, integrated approach offers care that is tailored to each youth.
Suicide Prevention in Juvenile Facilitiesby Lindsay M. Hayes ........................................................................... 24
Youth suicide is recognized as a serious public health problem, but suicide withinjuvenile facilities has not received comparable attention. Collaborative efforts andtechnical assistance training are essential components for suicide prevention withinsecure juvenile facilities.
IN BRIEFJustice Matters
OJJDP-Supported Mental Health Initiatives and Programs ................................ 33Juvenile Suicide in Confinement: A National Survey......................................... 34
PublicationsTreating Serious Anti-Social Behavior in Youth: The MST Approach ............. 36Mental Health Disorders and Substance Abuse Problems Among Juveniles ...... 36Juvenile Offenders and Victims: 1999 National Report ...................................... 37
OJJDP OnlineA Network for Sharing ......................................................................................... 38
ORDER FORM ....................................................................................................... 39
The Office of Juvenile Justice and Delinquency Prevention is a component of the Office of JusticePrograms, which also includes the Bureau of Justice Assistance, the Bureau of Justice Statistics, theNational Institute of Justice, and the Office for Victims of Crime.
Points of view or opinions expressed in this publication are those of the authors and do not necessarilyrepresent the official position or policies of OJJDP or the U.S. Department of Justice.
Youth With Mental Health Disorders: Issues and Emerging Responses
3Volume VII • Number 1
Joseph J. Cocozza, Ph.D., isVice President of Policy ResearchAssociates (PRA) and Directorof the National GAINS Centerfor People with Co-OccurringDisorders in the Justice System.Kathleen R. Skowyra is an AreaManager (Violence and CriminalJustice) for PRA. PRA offerscomprehensive services for theapplication of social scienceresearch methods to crucial policyissues at the Federal, State, andlocal levels.
T
Youth With MentalHealth Disorders:Issues and EmergingResponsesby Joseph J. Cocozza and Kathleen R. Skowyra
ragic mass homicides by juveniles, documented cases of neglectand inadequate services, and Federal policy initiatives focusing on pro-viding systems of care for at-risk juveniles have propelled mental healthissues among juvenile offenders into the headlines.
As the former Administrator of the Of-fice of Juvenile Justice and DelinquencyPrevention (OJJDP) has observed(Bilchik, 1998):
It is crucial that we deal not onlywith the specific behavior or circum-stances that bring them [youth] to ourattention, but also with their underly-ing, often long-term mental healthand substance abuse problems.
Recognition of theMental Health Needsof YouthThe mental health needs of youth in thejuvenile justice system have receivedmore attention at the Federal level inthe past 2 years than in the past threedecades combined. During the past 2years:
◆ The Civil Rights Division of the U.S.Department of Justice undertook a seriesof investigations that documented theconsistent inadequacy of mental healthcare and services in juvenile correctionalfacilities in a number of States(Butterfield, 1998).
◆ The U.S. Department of Health andHuman Services’ Center for MentalHealth Services initiated the first na-tional survey of juvenile justice facili-ties to identify available mental healthservices (Center for Mental HealthServices, 1998).
◆ Congress considered several billsand amendments that mandated com-prehensive mental health and sub-stance abuse screening and treatmentprograms for youth in the juvenile jus-tice system (Manisses CommunicationsGroup, Inc., 1999).
4
Juvenile Justice
The importance of the mental healthissue is also recognized at the Statelevel, for example, in the response givenrecently by the Secretary of the FloridaState Department of Juvenile Justicewhen asked about the most challengingissue facing juvenile corrections at thebeginning of this century. His answerwas not funding, sufficient beds, or secu-rity. Rather, the most challenging issuehe identified was “providing specializedservices such as mental health and sub-stance abuse services within the ju-venile correctional continuum”(Bankhead, 1999).
◆ Growing recognition of the mentalhealth needs of youth in general. Asnoted by a number of authors, children’sand adolescents’ mental health needshave historically been addressed inad-equately in policy, practice, and research(Hartman, 1997; Burns, 1999). Only re-cently have the number of youth withmental illness and their level of unmetneed been recognized (Burns, 1999).Recent estimates place the rate of seriousemotional disturbance among youth inthe general population at 9 to 13 percent(Friedman et al., 1996), much higherthan the 0.5- to 5-percent range previ-ously used by State policymakers (Busi-ness Publishers, Inc., 1996).
◆ Increasing reliance on the justicesystem to care for individuals withmental illness. This trend has beenclearly documented for the adult popula-tion. A report to Congress (Center forMental Health Services, 1995:iii) found:“As jail and prison populations increased,and the number of persons with mentalillness living at the fringe of their com-munities rose, the absolute number ofpersons with mental illness in jails andprisons also increased.” The survey-basedstudy Criminalizing the Seriously MentallyIll (Torrey et al., 1992:iv) also concluded:“Our jails have once again become surro-gate mental hospitals.” Various otherstudies have confirmed that large propor-tions of individuals in the Nation’s jailsand prisons are seriously mentally ill. Forexample, Teplin (1990) reported preva-lence rates of 6.4 percent for male jailinmates and 15 percent for female jailinmates. The most recent study releasedby the U.S. Department of Justice re-ported that 16 percent of State prison-ers were identified as mentally ill(Ditton, 1999). Such findings buttressthe view that “[j]ails and prisons havebecome the nation’s new mental hospi-tals” (Butterfield, 1998a). As suggested
Our jails have once again becomesurrogate mental hospitals.
The current level of concern about themental health needs of youth in the ju-venile justice system stands in stark con-trast to past neglect (Knitzer, 1982). Acomprehensive review of the last severaldecades of research (Cocozza, 1992)concluded:
We still know very little about themental health needs of youth who areinvolved in the juvenile justice sys-tem. There are no good nationalstudies on the number of such youthwho come in contact with the juve-nile justice system. Systematic infor-mation on how services are organizedand delivered across the country, oron how the mental health and juve-nile justice systems coordinate theirefforts, does not exist. Moreover, wehave no adequate information onwhat services are provided, their qual-ity and whether or not they make adifference.
What has led to this dramatic change?A number of different factors are in-volved, including the following:
Youth With Mental Health Disorders: Issues and Emerging Responses
5Volume VII • Number 1
above, policymakers, practitioners, andadvocates now recognize that the sametrends and issues exist in the juvenilejustice system.
◆ Recent changes in the juvenile jus-tice system. The juvenile justice systemhas largely shifted away from treatmentand rehabilitation and toward retributionand punishment as the “get tough” move-ment swept the Nation during the 1990’s.The decade has seen more youth trans-ferred to criminal court, longer sentences,and lower minimum ages at which juve-niles can be prosecuted in the criminaljustice system as if they were adults—allpart of the “adultification” of juvenilejustice (Altschuler, 1999). This trend to-ward criminalizing the juvenile justicesystem has raised questions about its role(Schwartz, 1999). The trend has alsoforced courts and the juvenile correctionssystem to address mental health-relatedissues for youth that had been previouslyrestricted primarily to adults, such as theconstitutional right to mental healthtreatment (Woolard et al., 1992), the ap-plicability of the “not guilty by reason ofinsanity” defense (Heilbrun, Hawk, andTate, 1996), and mental competencyguidelines (Woolard, Reppucci, andRedding, 1996).
Prevalence of MentalHealth DisordersAmong YouthDespite the growing concern, there isa paucity of adequate research on theprevalence and types of mental healthdisorders among youth in the juvenilejustice system. A comprehensive reviewof the research literature (Otto et al.,1992) found the research to be scarceand methodologically flawed. Other re-views have reached similar conclusions(Wierson, Forehand, and Frame, 1992).
Methodological problems include incon-sistent definitions and measurements ofmental illness; use of biased, nonrandomsamples; reliance on retrospective casereport data; and use of nonstandardizedmeasurement instruments.
Despite these problems, some generalconclusions can be drawn:
◆ Youth in the juvenile justice systemexperience substantially higher rates ofmental health disorders than youth inthe general population. This is a majorconclusion drawn from a review of 34studies (Otto et al., 1992) and is alsoconsistent with the finding that mentalillness prevalence rates in adult correc-tions populations are two to four timeshigher than the rates in the general adultpopulation (Teplin, 1990).
There is a paucity of adequate researchon mental health disorders among youthin the juvenile justice system.
◆ A high percentage of youth in thejuvenile justice system have a diagnos-able mental health disorder. One diffi-culty in addressing mental health issuesin the juvenile justice system centersaround the varying uses and definitionsof the terms “mental health disorder” and“mental illness.” One critical distinctionis between youth with a diagnosablemental health disorder and youth with aserious mental health disorder or seriousemotional disturbance (SED). Youthwith a diagnosable mental health disor-der are those that meet the formal crite-ria for any of the disorders listed in theDiagnostic and Statistical Manual of MentalDisorders: Fourth Edition, DSM–IV(American Psychiatric Association,1994) such as psychotic, learning, con-duct, and substance abuse disorders. Theterms “serious mental health disorder”
6
Juvenile Justice
and “SED”—defined and measured in anumber of different ways—are used toidentify youth experiencing more severeconditions that substantially interferewith their functioning. The term “seri-ous mental health disorder” often refersto specific diagnostic categories such asschizophrenia, major depression, andbipolar disorder. “SED,” a term used foryouth, includes those youth with a diag-nosable disorder for whom the disorderhas resulted in functional impairmentaffecting family, school, or communityactivities. With regard to diagnosablemental health disorders in general, re-search has found that most youth in thejuvenile justice system qualify for atleast one diagnosis. It is not uncommonfor 80 percent or more of the juvenilejustice population to be diagnosed withconduct disorder (Otto et al., 1992;Wierson, Forehand, and Frame, 1992;Virginia Policy Design Team, 1994).Given the broad definitional criteria forconduct disorder, Melton and Pagliocca(1992) point out that such a finding isnot surprising, although many of theseyouth qualify for more than one diagno-sis (Virginia Policy Design Team, 1994).
◆ It is safe to estimate that at least oneout of every five youth in the juvenilejustice system has serious mental healthproblems. Estimates of the prevalence ofserious mental health disorders among
these youth are particularly unreliablebecause of the problems with researchand, as mentioned above, the varyingdefinitions and measures of serious men-tal illness. If the prevalence rate of SEDfor youth in the general population is es-timated at 9–13 percent (Friedman et al.,1996) and the prevalence rate of disor-ders for youth in the juvenile justice sys-tem is consistently found to be at leasttwice as high (Otto et al., 1992), onecan reasonably expect the prevalencerate of serious mental health disordersfor youth in contact with the juvenilejustice system to be at least 20 percent.This estimate is consistent with thefindings other researchers have reported(Schultz and Mitchell-Timmons, 1995).A more accurate estimate will requirefurther research. It is clear, however, thatwhile most youth in the juvenile justicesystem have a diagnosable mental illnessand could benefit from some services,there is a sizable group of youth whocritically need access to mental healthservices because they are experiencingserious problems that interfere with theirfunctioning.
◆ Many of the youth in the juvenilejustice system with mental illness alsohave a co-occurring substance abusedisorder. Over the past several years,there has been greater recognition anddocumentation of the high level of co-occurring substance abuse disordersamong individuals with mental healthdisorders. Kessler et al. (1996) foundthat 50.9 percent of the general adultpopulation with serious mental healthdisorders have a co-occurring substanceabuse disorder, while Teplin, Abram,and McClelland (1991) found that73 percent of adult jail detainees withserious mental health disorders had aco-occurring substance abuse disorder.Although research has just begun tofocus on youth, Greenbaum, Foster-Johnson, and Petrila (1996:58) foundthat “approximately half of all adolescentsC
Youth With Mental Health Disorders: Issues and Emerging Responses
7Volume VII • Number 1
receiving mental health services” inthe general population are reported ashaving a dual diagnosis. Among thejuvenile justice system population, therates may be even higher (Otto et al.,1992; Milin et al., 1991).
Emerging Strategiesand ModelsGiven these findings, it is not surpris-ing that juvenile justice officials regardthe care of youth with serious mentalhealth problems—and the multiple andcomplex issues surrounding the treat-ment of these youth—as among theirgreatest challenges. Efforts to addressthese problems confront numerous bar-riers, including the following:
◆ The confusion across multiservicedelivery and juvenile justice systems, atboth the policy and practice levels, as towho is responsible for providing serviceto these youth.
◆ Inadequate screening and assessment.
◆ The lack of training, staffing, andprograms necessary to deliver mentalhealth services within the juvenilejustice system.
◆ The lack of funding and clear fundingstreams to support services.
◆ The dearth of research that ad-equately addresses the level and natureof mental health disorders experiencedby these youth and the effectiveness oftreatment models and services.
If one considers other complicatingtrends, such as managed care, theprivatization of services, and the diag-nostic and treatment issues surroundingparticular populations such as youth ofcolor (Issacs, 1992) and girls (Prescott,1997), one quickly gets a sense of howgreat a challenge any change will be.
At the same time, a clear set of compre-hensive strategies that appear to be criticalto any progress is emerging. These strate-gies are consistent with many of the actionsrecommended by leading national experts(Whitbeck, 1992), State officials (VirginiaPolicy Design Team, 1994; Ohio Depart-ment of Rehabilitation and Correction,Youth Services, Mental Health, and Alco-hol and Drug Addiction Services, 1995),and advocates (National Mental HealthAssociation, 1999). They are beingimplemented—often in a less than idealmanner—for a limited number of youthand in only a few locations. Describedbelow are some of these strategies andexamples of supporting policies, pro-grams, and services that are developingacross the Nation as systems and commu-nities begin to better address the needs ofthe growing number of youth with men-tal health disorders entering the juvenilejustice system.
A clear set of comprehensive strategiesis emerging.
Collaborating Across SystemsCross-system collaboration must form thebasis for all solutions. The field is begin-ning to understand that the needs and is-sues surrounding individuals with mentalhealth disorders cannot be placed at thedoorstep of any single agency or system(Steadman, McCarthy, and Morrissey,1989). Systematic efforts to examineand improve the response to these youth,whether at the national (Whitbeck, 1992)or State level (Virginia Policy DesignTeam, 1994), reach the same conclusions.Although an individual system can helpto improve the care and treatment ofyouth with mental illness in the juvenilejustice system, effective solutions requirethat multiple relevant agencies coordinateand integrate strategies and services.
8
Juvenile Justice
Collaborative efforts can include coordi-nated strategic planning, multiagencybudget submissions, implementation ofcomprehensive screening and assessmentcenters, cross-training of staff, and teamapproaches to assessment and case man-agement. Further, such efforts can beemployed at varying points in the juvenilejustice process—from intake through ad-judication, disposition, and aftercare.
At the State level, there also have beenattempts to foster more coordinated ap-proaches. In Ohio, four State agencies—the Ohio Departments of Alcohol andDrug Addiction Services, Mental Health,Rehabilitation and Correction, andYouth Services—allocated funds for theLinkages Project. This project supportslocal efforts to improve the coordinationof the criminal and juvenile justice,mental health, and substance abuseservice systems to reduce incarcerationand improve offender access to mentalhealth services. One funded county,Lorain, used the funds to create theProject for Adolescent Intervention andRehabilitation (PAIR), which targetsyouth placed on probation for the firsttime for any offense. Youth are screenedand assessed for mental health and sub-stance abuse disorders, and individualtreatment plans are developed. Youthare then supervised by probation officers/case managers in conjunction with treat-ment providers. An evaluation of thePAIR program found that it provides animportant service and coordinatingfunction for youth, the courts, and theservice systems involved (Cocozza andStainbrook, 1998).
Diverting Youth From theJuvenile Justice SystemWhenever possible, youth with seriousmental health disorders should be di-verted from the juvenile justice system.Given community concerns about safety,there are youth who, regardless of theirmental health needs, will need to beplaced in the juvenile justice systembecause of their serious and violent of-fenses. For other youth, however, theirpenetration into the juvenile justice sys-tem and placement into juvenile deten-tion and correctional facilities will serveto further increase the number of mentallyill youth in the Nation’s juvenile facilitieswho are receiving inadequate mental
Whenever possible, youth with seriousmental health disorders should bediverted from the juvenile justice system.
At the Federal level, the systems of careconcept developed by the Center forMental Health Services (CMHS) hasencouraged the coordination of servicesfor youth with SED in a number of com-munities across the Nation (Center forMental Health Services, 1996). Mostsites have not focused heavily on thejuvenile justice population, but thosethat have, such as the Wraparound Mil-waukee program, have observed positiveresults. Wraparound Milwaukee is a col-laborative county-operated health main-tenance organization that providescomprehensive care to youth referred fromboth the child welfare and juvenile justicesystems and their families. The programis designed to provide community-basedalternatives to residential treatment andpsychiatric hospitalization (WraparoundMilwaukee, 1998; see Bruce Kamradt’sarticle on Wraparound Milwaukee onpages 14–23). In addition, OJJDP andCMHS have collaborated for the past 2years to increase juvenile justice systeminvolvement in systems of care. Underthis interagency agreement, OJJDP hasprovided funds to the CMHS technicalassistance grantee to promote inclusionof youth with mental health needs in-volved in the juvenile justice system inother systems of care.
Youth With Mental Health Disorders: Issues and Emerging Responses
9Volume VII • Number 1
health services. At the adult level, effortsto stem this tide have begun to focus ondeveloping collaborative programs todivert individuals with serious mentalillness into community-based services(Steadman, Morris, and Dennis, 1995).
Diverting appropriate youth from the ju-venile justice process—whether at firstcontact with law enforcement officials,at intake, or at some other point priorto formal adjudication—can reduce thegrowing number of these youth enteringthe juvenile justice system and reducethe likelihood that their disorders willgo untreated. Diversion to services, how-ever, requires a multidisciplinary partner-ship involving the justice and treatmentsystems and a comprehensive range ofservices to which youth can be diverted.
The Persons in Need of Supervision(PINS) Diversion Program in New Yorkis an example of how to implement sucha diversion initiative. In 1985, the NewYork State PINS Adjustment ServicesAct was enacted on behalf of personsalleged to be in need of supervision inorder to prevent inappropriate or un-necessary court intervention. Countiesparticipating in the PINS DiversionProgram must submit a plan containinginteragency strategies for diverting youthfrom court and providing youth withcommunity-based services. Upon Stateapproval of the plan, the county is autho-rized to deny access to family court andto divert potential PINS and their fami-lies to assessment and adjustment ser-vices. Participating counties are requiredto create a multiagency Designated As-sessment Service (DAS) to provide com-prehensive assessments of the serviceneeds of PINS youth and their familiesand to develop treatment plans based onassessment results. An interagency plan-ning process encourages collaborationamong the local and State agencieswhose programs and resources targetthis population.
Mental Health ScreeningOne of the major obstacles in recognizingand treating youth with mental healthdisorders in the juvenile justice system isthe lack of screening and assessment. Allyouth in contact with the juvenile justicesystem should be screened and, whennecessary, assessed for mental health andsubstance abuse disorders. The screeningshould be brief, easily administered, andused to identify those youth who requirea more comprehensive assessment to fur-ther define the type and nature of thedisorder. The screening also should occurat the youth’s earliest point of contactwith the juvenile justice system andshould be available at all stages of juve-nile justice processing.
A major obstacle has been the absence ofreliable, valid, and easy-to-use screeningtools to help the juvenile justice systemidentify signs of mental illness. Grisso andBarnum (1998), however, recently devel-oped a new tool, the Massachusetts YouthScreening Instrument (MAYSI). It is ashort, easily administered inventory ofquestions that has been normed andtested on a number of juvenile justicepopulations and appears to provide apromising, standardized screen for use injuvenile justice settings (i.e., probationintake, detention, correctional facilities).
Community-BasedAlternativesEffective community-based alternativesshould be used whenever possible. Overthe past decade, a number of community-based approaches have been developedas alternatives to institutional care forchildren with serious mental healthdisorders, which is often more costly.These approaches are designed to keepyouth in their homes, schools, andcommunities while providing a com-prehensive set of services that respondto their mental health needs and re-lated problems.
Appropriate TreatmentIt is critical that youth with mentalhealth disorders who are placed in juve-nile correctional facilities receive appro-priate treatment. Even with greateremphasis on diversion and increasedreliance on community-based alterna-tives, many such youth will be placed injuvenile correctional facilities because ofthe nature and severity of their acts.Clearly, for youth assessed as being seri-ously disordered, it is reasonable to ex-pect that a mental health treatment planwill be developed and implemented byqualified, trained staff. Investigations bythe U.S. Department of Justice’s CivilRights Division, as has been noted, indi-cate that this is not always the case.
With funding from OJJDP, the Councilof Juvenile Correctional Administrators(1998) is developing and testing newperformance-based standards for theseyouth that include treatment guidelinespromulgated by a group of mental healthand substance abuse experts. Thesestandards should provide the field withmeaningful guidance in providing effec-tive mental health services.
Part of the difficulty in providing mentalhealth services to incarcerated youthcenters around larger issues concerningthe relative responsibilities of the juve-nile justice and treatment systems forthese youth. Some jurisdictions haveresponded to the increasing number ofyouth with mental health disorders bymaking more secure beds availablewithin the mental health system andtransferring the more seriously disturbedyouth back and forth between the twosystems. Other jurisdictions have createda continuum of mental health serviceswithin the juvenile corrections systemitself to address the needs of these youth(Underwood, Mullan, and Walter, 1997).
Standards should provide the field withmeaningful guidance in providingeffective mental health services.
A number of communities have imple-mented the systems of care initiativesnoted previously and related efforts suchas Wraparound services (Clark andClarke, 1996). One approach that hasdemonstrated positive outcomes is Multi-systemic Therapy (MST) (Henggeler,1997; Henggeler and Borduin, 1990).Developed by Scott Henggeler andhis colleagues, MST is a family- andcommunity-based treatment model thatprovides services in the home and com-munity settings and addresses a range offamily, peer, school, and community fac-tors. Research, most of which has beenconducted on youth with serious anti-social behavior, has found that MST isa successful and cost-effective clinicalalternative to out-of-home placements.The use of this therapy has resulted inpositive outcomes in a number of dimen-sions, including the prevalence of recidi-vism, psychiatric symptomatology, anddrug use (Henggeler, 1999).
Youth With Mental Health Disorders: Issues and Emerging Responses
11Volume VII • Number 1
Although empirical data on the relativesuccess of different approaches is lacking,a collaborative approach that involvesboth systems in planning, cross-training,and the delivery of services appears to bepreferable. Such an approach builds onthe strengths of each system and helpsto establish connections that are criticalto aftercare and community reintegrationfollowing release. In New York, for ex-ample, Mobile Mental Health TreatmentTeams, supported by State juvenile justiceand mental health agencies, serve youthwith identified mental health needs in ju-venile correctional facilities. Six regionalteams provide onsite assessments, training,counseling, and other clinical servicesto youth in these facilities.
ConclusionThese are just some of the topics and is-sues that are relevant to a discussion onhow to improve the field’s understandingof and response to the mental healthneeds of youth in the juvenile justice sys-tem. There are many more that merit ex-amination. For example, given what thefield is learning about the high prevalenceof co-occurring mental health and sub-stance abuse disorders, emerging direc-tions and strategies should emphasizeapproaches that rely on more integratedmental health and substance abuse treat-ment approaches. Although this reviewhas dealt with youth in the juvenile jus-tice system as a whole, research on varia-tions in prevalence, needs, and types oftreatment services must also consider is-sues surrounding particular populationssuch as minority youth and females in thejuvenile justice system.
Nonetheless, several critical pointsemerge from the preceding review. First,a large number of youth who come incontact with the juvenile justice system
require mental health treatment. Second,there is growing recognition of theseneeds and of the inadequacies of currentassessments and services. Third, a set ofclear strategies and useful models andtools are emerging. Much more isneeded—funding, social and politicalwill, and further research—but the foun-dation of a recognition of the problemand the development of promising prac-tices appears to be in place as we enterthe new millennium.
ReferencesAltschuler, D.M. 1999. Trends and issues in theadultification of juvenile justice. In Research toResults: Effective Community Corrections, edited byP. Harris. Lanham, MD: American CorrectionalAssociation.
American Psychiatric Association. 1994. Diagnos-tic and Statistical Manual of Mental Disorders: FourthEdition, DSM–IV. Washington, DC: AmericanPsychiatric Association.
Bankhead, B. 1999. Q & A: Florida’s BillBankhead. Mobilizing Leadership in JuvenileJustice: Council of Juvenile Correctional Adminis-trators (Newsletter) July(19):6–7.
Bilchik, S. 1998. Mental Health Disorders and Sub-stance Abuse Problems Among Juveniles. Fact Sheet#82. Washington, DC: U.S. Department of Jus-tice, Office of Justice Programs, Office of JuvenileJustice and Delinquency Prevention.
Burns, B.J. 1999. A call for a mental health ser-vices research agenda for youth with serious emo-tional disturbance. Mental Health Services Research1(1):5–20.
Business Publishers, Inc. 1996. CMHS set to re-lease new SED prevalence estimates. MentalHealth Report (Newsletter) (September 18):169.
Butterfield, F. 1998. Prisons replace hospitalsfor the nation’s mentally ill. New York Times(March 5):A1.
Center for Mental Health Services. 1995. DoubleJeopardy: Persons with Mental Illness in the CriminalJustice System. Rockville, MD: U.S. Department ofHealth and Human Services.
Center for Mental Health Services. 1996. Systemsof Care Fact Sheet. Rockville, MD: U.S. Depart-ment of Health and Human Services.
12
Juvenile Justice
Center for Mental Health Services. 1998. 1998Inventory of Mental Health Services in Juvenile Jus-tice Facilities, Halfway Houses and Group Homes.Survey. Rockville, MD: U.S. Department ofHealth and Human Services.
Clark, H.B., and Clarke, R.T. 1996. Research onthe wraparound process and individualized servicesfor children with multi-system needs. Journal ofChild and Family Studies 5(1):1–5.
Cocozza, J.J. 1992. Introduction. In Respondingto the Mental Health Needs of Youth in the JuvenileJustice System, edited by J.J. Cocozza. Seattle, WA:The National Coalition for the Mentally Ill in theCriminal Justice System, pp. 1–6.
Cocozza, J.J., and Stainbrook, K. 1998. The OhioLinkages Project: Final Evaluation Report. Delmar,NY: Policy Research Associates, Inc.
Council of Juvenile Correctional Administrators.1998. CJCA’s performance-based standardsproject update: Implementation visits start in July.Mobilizing Leadership in Juvenile Justice: Council ofJuvenile Correctional Administrators (July)15:8.
Ditton, P.M. 1999. Mental Health and Treatmentof Inmates and Probationers. Special Report. Wash-ington, DC: U.S. Department of Justice, Office ofJustice Programs, Bureau of Justice Statistics.
Friedman, R.M., Katz-Leavy, J.W., Manderscheid,R.W., and Sandheimer, D.L. 1996. Prevalence ofserious emotional disturbances in children andadolescents. In Mental Health, United States, editedby R.W. Manderscheid and M.A. Sonnerschein.Washington, DC: U.S. Department of Health andHuman Services, Substance Abuse and MentalHealth Services Administration, Center for Men-tal Health Services, pp. 71–89.
Greenbaum, P.E., Foster-Johnson, L., and Petrila, J.1996. Co-occurring addictive and mental disordersamong adolescents: Prevalence research and futuredirections. American Journal of Orthopsychiatry66(1):52–60.
Grisso, T., and Barnum, R. 1998. MassachusettsYouth Screening Instrument: Preliminary Manual andTechnical Report. Report. Worcester, MA: Univer-sity of Massachusetts Medical School.
Hartman, L. 1997. Children are left out. Psychiat-ric Services 48(7):953–954.
Heilbrun, K., Hawk, G., and Tate, D.C. 1996.Juvenile competence to stand trial: Researchissues in practice. Law and Human Behavior20(5):573–578.
Henggeler, S.W. 1997. Treating Serious Anti-Social Behavior in Youth: The MST (Multi-systemic Therapy) Approach. Washington, DC:U.S. Department of Justice, Office of JusticePrograms, Office of Juvenile Justice and Delin-quency Prevention.
Henggeler, S.W., and Borduin, C.M. 1990. FamilyTherapy and Beyond: A Multisystemic Approach toTreating the Behavior Problems of Children and Ado-lescents. Pacific Grove, CA: Brooks/Cole.
Isaacs, N.R. 1992. Assessing the mental healthneeds of children and adolescents of color in thejuvenile justice system: Overcoming institutional-ized perceptions and barriers. In Responding to theMental Health Needs of Youth in the Juvenile JusticeSystem, edited by J.J. Cocozza. Seattle, WA: TheNational Coalition for the Mentally Ill in theCriminal Justice System, pp. 141–163.
Kessler, R.C., Nelson, C.B., McGonagle, K.A.,Edlund, M.J., Frank, R.G., and Leaf, P.J. 1996.The epidemiology of co-occurring addictive andmental disorders: Implications for prevention andservice utilization. American Journal of Orthopsy-chiatry 66(1):17–25.
Knitzer, J. 1982. Unclaimed Children: The Failure ofPublic Responsibility to Children and Adolescents inNeed of Mental Health Services. Washington, DC:Children’s Defense Fund.
Manisses Communications Group, Inc. 1999. Ad-vocates win MH amendments to Senate juvenilecrime bill. Children’s Services Report (Newsletter)3(10):1–2.
Melton, G.B., and Pagliocca, P.M. 1992. Treat-ment in the juvenile justice system: Directions forpolicy and practice. In Responding to the MentalHealth Needs of Youth in the Juvenile Justice System,edited by J.J. Cocozza. Seattle, WA: The NationalCoalition for the Mentally Ill in the CriminalJustice System, pp. 107–129.
Milin, R., Halinkas, J.A., Miller, J.E., and Morse, C.1991. Psychopathology among substance abusingjuvenile offenders. Journal of the American Academyof Child and Adolescent Psychiatry 30:569–574.
National Mental Health Association. 1999. JuvenileJustice Initiative: Status Report and Call to Action. Alex-andria, VA: National Mental Health Association.
Ohio Department of Rehabilitation and Correc-tion, Youth Services, Mental Health, and Alcoholand Drug Addiction Services. 1995. Managingmentally ill and substance abusing offenders in thecommunity, demonstration project: A request forconcept papers. State agency correspondence.
Otto, R.K., Greenstein, J.J., Johnson, M.K., andFriedman, R.M. 1992. Prevalence of mental dis-orders among youth in the juvenile justice sys-tem. In Responding to the Mental Health Needsof Youth in the Juvenile Justice System, edited byJ.J. Cocozza. Seattle, WA: The National Coali-tion for the Mentally Ill in the Criminal JusticeSystem, pp. 7–48.
Youth With Mental Health Disorders: Issues and Emerging Responses
13Volume VII • Number 1
Prescott, L. 1997. Adolescent Girls with Co-occurringDisorders in the Juvenile Justice System. Delmar,NY: The National GAINS Center for People withCo-Occurring Disorders in the Justice System.
Schultz, C.S., and Mitchell-Timmons, J. 1995.Prevalence of Mental Disorder in a Juvenile JusticePopulation. Cleveland, OH: Case Western ReserveUniversity School of Medicine, Department ofPsychiatry.
Schwartz, I.M., ed. 1999. The Annals of the Ameri-can Academy of Political and Social Science: Will theJuvenile Court System Survive? Thousand Oaks,CA: Sage Publications, Inc.
Steadman, H.J., McCarthy, D.W., and Morrissey,J.P. 1989. The Mentally Ill in Jail: Planning forEssential Services. New York, NY: The GuilfordPress.
Steadman, H.J., Morris, S.M., and Dennis, D.L.1995. The diversion of mentally ill persons fromjail to community-based services: A profile ofprograms. American Journal of Public Health85(12):1630–1635.
Teplin, L.A. 1990. The prevalence of severe men-tal disorder among male urban jail detainees:Comparison with the epidemiological catchmentarea program. American Journal of Public Health80(6):663–669.
Teplin, L.A., Abram, K.M., and McClelland,G.M. 1991. Psychiatric and Substance Abuse Dis-orders Among Juveniles in Detention: An EmpiricalAssessment. Chicago, IL: Northwestern UniversityMedical School.
Torrey, E.F., Stieber, J., Ezekiel, J., Wolfe, S.M.,Sharfstein, J., Noble, J.H., and Flyn, L.M. 1992.Criminalizing the Seriously Mentally Ill: The Abuseof Jails as Mental Hospitals. Report to the NationalAlliance for the Mentally Ill and Public Citizen’sHealth Research Group.
Underwood, L.A., Mullan, W.C., and Walter,C.L. 1997. We built them and they came: Newinsights for managing Ohio’s aggressive juvenileoffenders with mental illness. Corrections Manage-ment Quarterly 1(4):19–27.
Virginia Policy Design Team. 1994. Mental HealthNeeds of Youth in Virginia’s Juvenile Detention Cen-ter. Richmond, VA: Virginia Policy Design Team.
Whitbeck, J. 1992. The national work session:Issues and recommended actions. In Responding tothe Mental Health Needs of Youth in the Juvenile Jus-tice System, edited by J.J. Cocozza. Seattle, WA:The National Coalition for the Mentally Ill in theCriminal Justice System, pp. 165–180.
Wierson, M., Forehand, R.L., and Frame, C.L.1992. Epidemiology and the treatment of mentalhealth problems in juvenile delinquents. Advancesin Behavior Residential Theory 14:93–120.
Woolard, J.L., Gross, S.L., Mulvey, E.P., andReppucci, N.D. 1992. Legal issues affecting men-tally disordered youth in the juvenile justicesystem. In Responding to the Mental Health Needsof Youth in the Juvenile Justice System, edited byJ.J. Cocozza. Seattle, WA: The National Coalitionfor the Mentally Ill in the Criminal Justice Sys-tem, pp. 91–95.
Woolard, J.L., Reppucci, N.D., and Redding, R.E.1996. Theoretical and methodological issues instudying children’s capacities in legal contexts.Law and Human Behavior 20(3):219–228.
Wraparound Milwaukee. 1998. Annual Report.Milwaukee, WI: Milwaukee County MentalHealth Division, Child and Adolescent ServicesBranch.
14
Juvenile Justice
Bruce Kamradt, MSW, is Directorof the Children’s Mental HealthServices Division for MilwaukeeCounty, the largest public providerand purchaser of children’s mentalhealth services in Milwaukee, WI.Over the past 5 years, the divisionhas focused on a system of care tointegrate mental health, childwelfare, juvenile justice, andeducation services for complex-needs children and their families.
T
WraparoundMilwaukee: AidingYouth With MentalHealth Needsby Bruce Kamradt
he estimated percentage of youth with mental health disorders inthe juvenile justice system varies from study to study. Estimates of diag-nosable mental health disorders among the general population run about20 percent. While there are no reliable national studies of the preva-lence of mental health disorders among juvenile offenders, estimatesfrom existing studies indicate that the rate for mental health disordersamong juvenile offenders may be as high as 60 percent, of which an esti-mated 20 percent have severe mental health disorders (Cocozza, 1992).
Finding effective treatment models foryouth in the juvenile justice system withserious emotional, mental health, and be-havioral needs can be difficult. Systemstend to use more traditional residentialand day treatment programs to serve theseyouth. The traditional categorical ap-proach that the juvenile justice, child wel-fare, and mental health systems often useplaces youth in a “one-size-fits-all” pro-gram, regardless of the youth’s needs.
Wraparound Milwaukee, now in its fifthyear of operation, takes a quite differentapproach to serving youth with mentalhealth needs. The program serves morethan 650 youth, 400 of whom are adjudi-cated delinquent. Created under a Cen-ter for Mental Health Services grant,
Wraparound Milwaukee sustains itself bypooling dollars with its systems partnersand taking an integrated, multiserviceapproach to meeting the needs of youthand their families. This approach, whichis based on the Wraparound philosophyand the managed care model, offers carethat is tailored to each youth. Data indi-cate that the program is achieving posi-tive outcomes.
Process and ApproachThe Wraparound philosophy began withJohn Brown, a Canadian service providerwho developed the idea of placing youthin small group homes with individualizedcare, flexible programming, and a “never
Wraparound Milwaukee: Aiding Youth With Mental Health Needs
15Volume VII • Number 1
give up” philosophy (Behar, 1985). KarlDennis’ Kaleidoscope program in Chi-cago, IL, and John Van Den Berg’sAlaska Youth Initiative adapted theseconcepts. The Kaleidoscope program—the oldest Wraparound initiative in theUnited States—used unconditional careand flexible, integrated services to meetyouth and family needs (Burns andGoldman, 1998). The Alaska YouthInitiative used cross-system collabora-tion and funding and individualizedplanning to bring youth back to thecommunity from out-of-State residentialtreatment placements (Burchard et al.,1993). Dr. Ira Laurie, National Directorof the U.S. Department of Health andHuman Services’ Child and AdolescentServices System Program (CASSP),further conceptualized the process. Hisdescriptions of the values of CASSP intreating children with serious emotionalproblems, including the development ofindividualized, child-centered, family-focused, community-based, and cultur-ally competent services, have beenadopted by Wraparound (Laurie andKaty-Leavy, 1987).
The evolution of Wraparound in systemsdesign was further enhanced by the im-plementation and growth of system ofcare models, developed under demonstra-tion grants from the U.S. Departmentof Health and Human Services’ Centerfor Mental Health Services. This grantprogram incorporated the values, phi-losophy, and approaches of Wraparoundto promote integrated service systems foryouth with serious emotional problemsoperating across the mental health, juve-nile justice, child welfare, and educationsystems.
Although there are many componentsto Wraparound, the following elementshave been of particular importance inworking with children in the juvenilejustice and child welfare systems:
◆ Strength-based approach to childrenand families. Mental health and juvenilejustice systems have focused largely onidentifying a child’s deficits or a family’sproblems. This is not the most effectiveway to engage a child or family in the treat-ment process. Focusing on a family’sstrengths, learning about the family’s cul-ture, and building on the natural supportsthat exist within the family, neighborhood,or community is a much more effective ap-proach. Examples of such supports in-clude peer groups, recreational basketballleagues, parenting classes, and positiverelationships a child may have with grand-parents, uncles, aunts, peers, and others.
Demographics of the Delinquent Populationin Wraparound Milwaukee
◆ Eighty percent are male.
◆ The average age is 14.7.
◆ Sixty-five percent are African American, 28 percent areCaucasian, and 7 percent are Hispanic.
◆ Sixty-five percent are from mother-maintained households.
◆ Fifty-three percent of the population’s families are at orbelow the poverty level.
16
Juvenile Justice
◆ Family involvement in the treatmentprocess. Families are the most importantresource in any youth’s life. Juvenile jus-tice, child welfare, and mental healthpractitioners often have been too quickto identify families as the source of theyouth’s problems. The tendency is to re-move youth from the home and institu-tionalize them in order to “fix” them.Youth, however, usually prefer to live withtheir families. Whenever possible, serviceproviders should engage families in thetreatment process. Accordingly, it is im-portant that providers view families ascapable and knowledgeable about theirchildren’s needs and enhance families’abilities to parent their troubled children.
typical needs of persons of like age, gen-der, or culture. These can involve livingsituations; legal status; and medical,health, and psychological needs.
◆ Outcome-focused approach. TheWraparound process does not rely on sub-jective assessments of what does or doesnot work. Clear goals for the youth andfamily—established by the youth and fam-ily in partnership with the professionals—are continually measured and evaluated.The key to this approach is to manage theprocess to ensure desired outcomes.
ImplementationWraparound Milwaukee adapted theWraparound process to its system of carein some very unique ways. In Milwaukee,the multiple needs of youth who cross ju-venile justice, child welfare, and mentalhealth system lines are coordinatedthrough a public managed care organiza-tion. Youth and families are offered en-rollment in a type of social/medical healthmaintenance organization (HMO) witha comprehensive benefit plan that offersmore than 60 services. These services areindividualized for each youth and family,based on their identified needs.
HistoryWraparound Milwaukee is part of theMilwaukee County Human ServicesDepartment, Milwaukee County MentalHealth Division, which provides juvenileprobation and child welfare services.In 1994, Milwaukee County received a5-year Federal grant from the Center forMental Health Services to initiate systemreform in the community. Although Wrap-around Milwaukee experienced initial suc-cess in providing services to youth andfamilies in the mental health system, it wasnot until it targeted youth in the child wel-fare and juvenile justice systems that itdemonstrated the effectiveness of the
Treatment plans that are tailored toaddress the unique needs of each childwork best.
◆ Needs-based service planning anddelivery. If families are to be involvedas active partners, it is essential to listento their assessment of their needs. Juve-nile justice, child welfare, and mentalhealth practitioners tend to assume thatas “experts” they are best equipped to de-cide the programs and services youthneed. If, for example, a youth and familyhave identified a need for respite care, atutor, or a mentor to serve as a positiverole model, why do some practitionersinsist on providing outpatient therapy,day treatment, or residential care? Thefailure to listen to what a child and fam-ily identify as their needs, and to addressthose needs, can cause programs and ser-vices to fail.
◆ Individualized service plans. Treat-ment plans that are tailored to addressthe unique needs of each child and fam-ily work best. Individualized plans foryouth, particularly those involved in thejuvenile justice system, must address the
Wraparound Milwaukee: Aiding Youth With Mental Health Needs
17Volume VII • Number 1
Wraparound approach with youth whohave multiple needs.
In May 1996, Wraparound Milwaukeeinitiated a pilot project, The 25 KidProject, to use Wraparound philosophywith both delinquent and nondelinquentyouth placed in residential treatment cen-ters. Prior to this project, child welfare andjuvenile justice placements had reachedrecord proportions—more than 360 youthwere in placement on an average day at acost of more than $18 million per year.Wraparound Milwaukee targeted 25 youthin residential treatment centers, identifiedby child welfare and juvenile justice profes-sionals, who had no immediate dischargeplans. The goal was to demonstrate thatby using a Wraparound model most ofthese youth could be returned home orto community-based foster or kinship care,that they could be maintained safely inthose settings, and that it would cost lessthan a residential placement. Within 90days, Wraparound Milwaukee returned 17of the youth to the community. Eventually,24 of the 25 youth were placed in the com-munity. Seven youth entered foster homes;the remaining 17 successfully returned totheir families.
Key ComponentsThe structural and design aspects of Wrap-around incorporate components of carethat are integrated to meet the specificneeds of each child and family. The follow-ing components are essential to the successof the project:
◆ Care coordination. Care coordinatorsare the cornerstone of the system. Theyperform strength-based assessments, as-semble the Child and Family Team,conduct plan-of-care meetings, helpdetermine needs and resources with theyouth and family, assist the team in iden-tifying services to meet those needs, ar-range for community agencies to providespecific services, and monitor the imple-
Mental Health Issuesof the Population inWraparound Milwaukee◆ Predominant diagnoses when
using the Diagnostic andStatistical Manual of MentalDisorders: Fourth Edition,DSM–IV (American Psychiat-ric Association, 1994). Ninety-seven percent conduct disorder/oppositional defiant, 58 percentdepression, 44 percent attentiondeficit, and 42 percent seriousalcohol and substance abuseproblems.
◆ Primary identified concerns atintake for youth. Fifty-twopercent school/community, 40percent acting out, 37 percentalcohol and substance abuse, and33 percent severe aggressiveness.
◆ Attempted suicide. One ineight youth.
◆ Primary family concerns at in-take. Fifty percent of parentshave significant abuse issues, 33percent of parents have a historyof domestic abuse, 24 percent ofparents have been incarcerated,and 22 percent of families havedocumented mental illness.
mentation of the case plan. Care coordi-nators in the Wraparound MilwaukeeProject typically work with small case-loads (a ratio of one worker to eightfamilies), which provides more time forthe personal contact needed to workwith youth with complex needs.
◆ The Child and Family Team. Wrap-around plans are family driven. The carecoordinator asks the family to identify allthose who are providing support to thefamily. With this information, the care
18
Juvenile Justice
coordinator assembles the family mem-bers; the family’s natural supports such asrelatives, church members, and friends;and systems people, including probationor child welfare workers. These individu-als form the core of the support systemfor the child and family.
◆ A mobile crisis team. To meet theneeds of youth and families when acare coordinator might not be available,24-hour crisis intervention services areavailable through the Mobile UrgentTreatment Team. The team consists ofpsychologists and social workers trainedin intervening in family crisis situationsthat might otherwise result in the removalof youth from their home, school, or com-munity. Youth participating in Wrap-around are automatically enrolled in thiscrisis service, and their care plans includea crisis safety plan that the team can im-mediately access. The Mobile UrgentTreatment Team reviews all requests forinpatient psychiatric hospital admissionsand operates two 8-bed group homes thatprovide short-term (up to 14 days) crisisstabilization. The crisis team and care co-ordinator work with the family to returnthe child to the community. Because ofthe crisis team’s availability, WraparoundMilwaukee has nearly eliminated the useof inpatient psychiatric care for mostyouth in the project.
◆ A provider network. WraparoundMilwaukee has an array of services and re-sources to respond to the multiple needsidentified by families. This enables the pro-gram to move beyond the few categoricalservices historically prescribed for youthand families. As a result, Wraparound hasexpanded its portfolio of services from 20to 60. Practitioners provide services on afee-for-service basis, with Wraparound set-ting the price of each category of service.Rather than creating fixed-price contracts,vendors apply to provide one or more ofthe services as part of a provider network.The provider network now includes more
than 170 agencies, a number that allows fora diverse list of providers and increases thechoices families have when selecting agen-cies in the network from which to receiveservices.
Managed Care andBlended FundingBecause Wraparound Milwaukee blendssystem funds, it can provide a flexible andcomprehensive array of services to delin-quent youth and their families. Wrap-around Milwaukee pools funds throughcase rates paid by the child welfare andjuvenile justice systems, receives amonthly capitation payment for eachMedicaid child enrolled, and coordi-nates other insurance and SupplementalSecurity Income payments to form atype of insurance pool. In 1999, Wrap-around Milwaukee received more than$26 million in pooled funds. The childwelfare and juvenile justice systems fundWraparound at $3,300 per month perchild. Prior to Wraparound, these fundswere used entirely for residential treat-ment care for which the systems paid$5,000 or more per month per child.The $1,542 per month per child capita-tion payment from Medicaid covers theprojected cost for all mental health andsubstance abuse services and is based onpre-Wraparound actuarial costs for ser-vices for these youth.
After all funds are pooled and decategorized,Wraparound Milwaukee can use them tocover any services that families need.Wraparound offers the same range of ser-vices to all enrolled families and covers anycosts that exceed the pooled funds. Table 1lists a number of the services offered in theWraparound Milwaukee benefit plan.
Informal ServicesWhile Wraparound Milwaukee offersan array of formal services to youth and
Wraparound Milwaukee: Aiding Youth With Mental Health Needs
19Volume VII • Number 1
their families, informal services that thecare coordinator and Child and FamilyTeam identify through strengths assess-ment are often even more effective. TheWraparound care plan, therefore, shoulduse a mix of formal and informal services.One family may identify a friend or relativewhose positive relationship with the youthindicates suitability as a mentor. Anotherfamily may identify a relative to providerespite care to the parent. These supportswill remain with the family beyond theirenrollment in Wraparound Milwaukee.Other examples of informal supports are aneighbor who provides transportation, alocal church with a peer support group, ora YMCA program that offers recreationand summer camp programs. These services
often can be mobilized at little cost andoffer the advantage of always beingthere for the youth and family in theirown community.
OutcomesOutcomes for youth participating in Wrap-around Milwaukee have been encourag-ing. The use of residential treatment hasdecreased 60 percent since WraparoundMilwaukee was initiated (from an averagedaily census of 364 youth in placement tofewer than 140 youth). Inpatient psychiat-ric hospitalization has dropped by 80 per-cent; in 1998, only 322 days of care wereprovided. As mentioned above, the aver-age overall cost of care per child has
Services in the Wraparound Milwaukee Benefit Plan
◆ Care Coordination
◆ In-Home Therapy
◆ Medication Management
◆ Outpatient—Individual FamilyTherapy
◆ Alcohol/Substance AbuseCounseling
◆ Psychiatric Assessment
◆ Psychological Evaluation
◆ Housing Assistance
◆ Mental Health Assessment/Evaluation
◆ Mentoring
◆ Parent Aide
◆ Group Home Care
◆ Respite Care
◆ Child Care for Parent
◆ Tutor
◆ Specialized Camps
◆ Emergency Food Pantry
◆ Crisis Home Care
◆ Treatment Foster Care
◆ Residential Treatment
◆ Foster Care
◆ Day Treatment/AlternativeSchool
◆ Nursing Assessment/Management
◆ Job Development/Placement
◆ Kinship Care
◆ Transportation Services
◆ Supervision/Observation inHome
◆ Afterschool Programming
◆ Recreation/Child-OrientedActivities
◆ Discretionary Funds/FlexibleFunds
◆ Housekeeping/Chore Services
◆ Independent Living Support
◆ Psychiatric Inpatient Hospital
20
Juvenile Justice
dropped from more than $5,000 permonth to less than $3,300 per month.Because the savings have been reinvestedinto serving more youth, the project nowserves 650 youth with the same fixedchild welfare/juvenile justice monies thatpreviously served 360 youth placed inresidential treatment centers.
Clinical outcomes, as measured by theChild and Adolescent Functional Assess-ment Scale (CAFAS) (Hodges, 1994),have improved significantly for delin-quent youth. CAFAS is used in allChildren’s Mental Health Servicesprograms to measure changes in theyouth’s functioning at home, at school,and in the community. With CAFAS,a lower score indicates the youth isfunctioning more adequately. For agroup of 300 delinquent youth enrolledin Wraparound Milwaukee, the averagescore at the time of enrollment was 74,which is considered in the high range ofimpairment. By 6 months after enroll-ment, the average score decreased to 56,
in the moderate range of impairment.One year after enrollment, the averagescore was 48, again a moderate level ofimpairment.
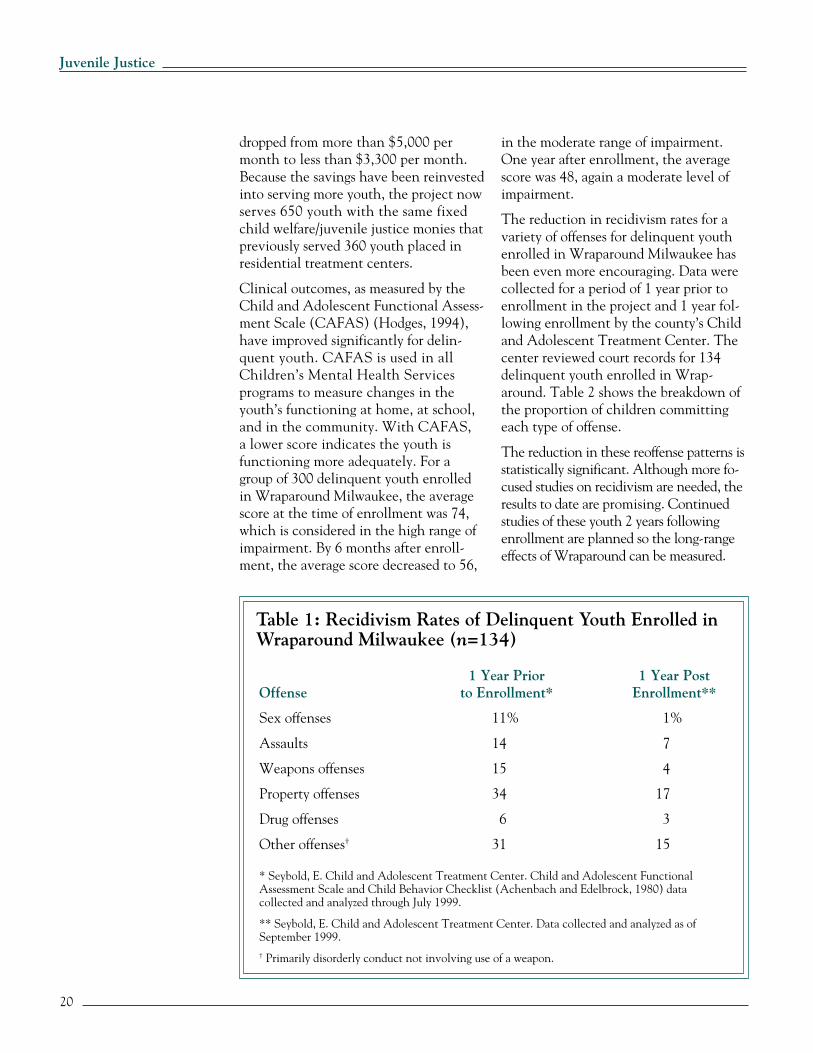
The reduction in recidivism rates for avariety of offenses for delinquent youthenrolled in Wraparound Milwaukee hasbeen even more encouraging. Data werecollected for a period of 1 year prior toenrollment in the project and 1 year fol-lowing enrollment by the county’s Childand Adolescent Treatment Center. Thecenter reviewed court records for 134delinquent youth enrolled in Wrap-around. Table 2 shows the breakdown ofthe proportion of children committingeach type of offense.
The reduction in these reoffense patterns isstatistically significant. Although more fo-cused studies on recidivism are needed, theresults to date are promising. Continuedstudies of these youth 2 years followingenrollment are planned so the long-rangeeffects of Wraparound can be measured.
1 Year Prior 1 Year PostOffense to Enrollment* Enrollment**
Sex offenses 11% 1%
Assaults 14 7
Weapons offenses 15 4
Property offenses 34 17
Drug offenses 6 3
Other offenses† 31 15
* Seybold, E. Child and Adolescent Treatment Center. Child and Adolescent FunctionalAssessment Scale and Child Behavior Checklist (Achenbach and Edelbrock, 1980) datacollected and analyzed through July 1999.
** Seybold, E. Child and Adolescent Treatment Center. Data collected and analyzed as ofSeptember 1999.† Primarily disorderly conduct not involving use of a weapon.
Wraparound Milwaukee: Aiding Youth With Mental Health Needs
21Volume VII • Number 1
Wraparound Milwaukee Case Studies
Michael, a 15-year-old Hispanic, was referred to Wraparound Milwaukee as theresult of delinquency charges of party to a crime and attempted arson of a schoolbuilding. As a result of the charges, Michael was expelled from a Milwaukeepublic school, and the Probation Department was ready to recommend residen-tial treatment.
Michael is cognitively delayed and has received special education services. At onepoint, he had a substance abuse problem and was diagnosed with depression.
Michael’s Child and Family Team included his mother, grandmother, a mentor,a teacher, a probation worker, and an alcoholism treatment counselor. The teamworked on Michael’s identified academic needs. They learned that he had poorvision, which contributed to his school problems. Michael enrolled in a special-ized learning center to develop his academic skills. Initial testing by the learningcenter revealed that Michael tested at only a first- and second-grade level in En-glish, mathematics, and reading. After 4 months, he improved his academic per-formance by two grades.
Michael’s mentor introduced him to recreational and other activities and becamea positive role model and father figure. Michael’s grandmother provided respitecare to Michael’s mother once a week. Informal service providers included theCouncil for the Spanish Speaking, which provides substance abuse counseling,and Milwaukee Christian Center and Journey House, which offers neighborhoodrecreation activities.
After 1 year in Wraparound, Michael has been readmitted to his Milwaukee publicschool as a freshman and placed in a special education program. He now tests at afifth- and sixth-grade level in English, mathematics, and reading—an extraordinaryimprovement. Michael has had no further delinquencies.
Anthony, a 15-year-old African American, originally was placed in WraparoundMilwaukee because of multiple counts of criminal damage to property. He wasdiagnosed with attention deficit disorder and major depression. Anthony’s familystrengths included his parents’ desire to keep him at home, the number of aunts anduncles who were interested in being resources for him in times of family stress, andhis family’s motivation for change. Anthony’s personal strengths included his out-going nature, affection for his siblings, desire to find a job, and love for his parents.
His Child and Family Team included his mother, stepfather, aunt, a sibling, an in-home therapist, a probation worker, a volunteer mentor, and his care coordinator.Formal services he received through Wraparound included in-home treatment,day treatment, mentoring, and job coaching. Anthony’s aunt provided informalservices—Anthony would stay with her during some of his crisis periods.
Anthony has been in Wraparound for 2 years. He has had no further law viola-tions and has been an honor student in the alternative school program. He isreturning to a Milwaukee public high school. He is also working with an employ-ment agency in the provider network to obtain a part-time job.
22
Juvenile Justice
ChallengesWraparound Milwaukee is provingto be an effective model that can bereplicated in other communities. It isimportant, however, to note the chal-lenges to system collaboration thatcare coordinators and case managersface. Table 3 outlines these challengesand the solutions that these profession-als implement when working acrosssystems.
Wraparound’s FutureThe future of Wraparound Milwaukeeas an effective approach to meeting theneeds of youth with serious emotional,behavioral, and health issues in thejuvenile justice or child welfare systemsremains positive.
Milwaukee’s community has adoptedthe model designed for early interven-tion services for abused and neglectedchildren in the child welfare system.
Table 2: Challenges to System Collaboration
Challenge Solution
Operating with different ◆ Cross train.terminology (juvenile court ◆ Share each other’s turf.and mental health system).
Defining roles (Who’s ◆ Conduct team development training.in charge?). ◆ Conduct job shadowing sessions.
◆ Share myths and realities.
Sharing information. ◆ Set up a common database.◆ Share organization charts and phone lists.◆ Share paperwork.◆ Promote flexibility in schedules to
support attendance at meetings.
Addressing issues of ◆ Document safety plans.community safety. ◆ Develop protocol for high-risk youth.
◆ Demonstrate adherence to court orders.◆ Communicate with district attorneys
and public defenders.
Keeping the stakeholders ◆ Track and report outcomes.informed. ◆ Share literature.
◆ Conduct workshops.
Sharing the value base. ◆ Reinforce Wraparound values in allmeetings.
◆ Conduct strength-based cross training.◆ Include parents in joint meetings.
Wraparound Milwaukee: Aiding Youth With Mental Health Needs
23Volume VII • Number 1
This model is being considered foryouth coming out of State juvenilecorrectional facilities.
Nationally, several States and communi-ties have incorporated aspects of the pro-gram into their own systems of care. TheCenter for Mental Health Services de-scribes Wraparound Milwaukee as a mostpromising practice in children’s mentalhealth.
The initial results are encouraging.Wraparound Milwaukee offers an inno-vative and cost-effective approach andan alternative to punitive approaches tojuvenile violence and delinquency.
ReferencesAchenbach, T.M., and Edelbrock, C. 1980. ChildBehavior Checklist. Burlington, VT: University ofVermont, Department of Psychiatry.
American Psychiatric Association. 1994. Diagnos-tic and Statistical Manual of Mental Disorders: Fourth
Behar, L. 1985. Changing patterns of State re-sponsibility: A case study in North Carolina. Jour-nal of Clinical Psychology 14:88–195.
Burchard, J., Burchard, S., Sewell, R., and VanDen Berg, J. 1993. One Kid at a Time: EvaluativeCase Studies and Description of the Alaska YouthInitiative Demonstration Project. Washington, DC:Georgetown University Child DevelopmentCenter.
Burns, B., and Goldman, S. 1998. PromisingPractices in Wraparound for Children With SeriousEmotional Disturbance and Their Families. Vol. 4.Rockville, MD: Child and Adolescent ServicesBranch, Center for Mental Health Services, p. 82.
Cocozza, J.J., ed. 1992. Responding to the MentalHealth Needs of Youth in the Juvenile Justice System.Seattle, WA: The National Coalition for theMentally Ill in the Criminal Justice System.
Hodges, K. 1994. Child and Adolescent FunctionalAssessment Scale. Ypsilanti, MI: Eastern MichiganUniversity, Department of Psychology.
Laurie, I., and Katy-Leavy, J. 1987. In ChronicallyMentally Ill Patient, Vol. 2, edited by L. Mennegerand G. Hannah. Washington, DC: AmericanPsychological Press.
24
Juvenile Justice
Lindsay M. Hayes, M.S., isAssistant Director of the NationalCenter on Institutions andAlternatives. He has conductedresearch, provided technicalassistance and training, andserved as an expert witness in thearea of jail, prison, and juvenilesuicide for the past 20 years.
N
Suicide Prevention inJuvenile Facilitiesby Lindsay M. Hayes
elson, a 16-year-old American Indian, was committed to theValley Youth Correctional Facility in May 1996 as a disposition for asexual assault.1 At an early age he had been physically abused by familymembers and sexually abused by neighborhood youth. Although he hadnever attempted suicide, Nelson had an extensive history of suicidalthoughts and tendencies. Psychiatric evaluation led to a diagnosis ofconduct disorder and attention deficit hyperactivity disorder. Thefacility’s psychiatrist saw him regularly and prescribed psychotropicmedication. In October 1996, Nelson was placed on suicide watch afterhe had scratched his arms following an altercation with another youth.Nelson told the counselor that he often got depressed and mutilatedhimself after getting into trouble. Suicide precautions were discontinuedseveral days later.
In June 1997, Nelson was placed in aquiet room for several hours after he wasjudged a risk to himself because he hadinflicted superficial scratches on his armsand a risk to others because he threat-ened his peers. He later told unit staffthat placement in the quiet room dimin-ished his need to abuse himself (some-times he would punch the walls to relievehis tension and anger). In July 1997,Nelson was again housed in a quiet roomand placed on suicide precautions afterthreatening suicide. In December 1997,cottage staff referred him to a counseloras they were concerned about his depres-sion and his questioning whether “lifewas worth living anymore.” He was
reportedly upset by the likelihood of be-ing transferred to another facility becauseof his noncompliance with the treatmentprogram. The situation was exacerbatedby his mother’s decision to stop visitinghim in order to encourage his participa-tion in treatment. The counselor be-lieved that suicide precautions wereunnecessary, and Nelson agreed to notifystaff should he feel suicidal again.
On January 12, 1998, at approximately5:30 p.m., Nelson was placed in a quietroom as a discipline for flashing gang signsin the dining room and making sexualcomments about female cottage staff. Cot-tage staff returned Nelson—who appearedquiet and lonely to his peers—to his hous-ing cottage at approximately 6:50 p.m.At approximately 10:30 p.m., cottage stafffound Nelson in his room hanging from a
1 To ensure confidentiality, the names of thevictim and facility have been changed.
25Volume VII • Number 1
Suicide Prevention in Juvenile Facilities
ceiling vent by a sheet. Staff initiated car-diopulmonary resuscitation and called foran ambulance. Paramedics arrived shortlythereafter, continued lifesaving measures,and transported the youth to a local hos-pital where he died a few days later as aresult of his injuries.
PrevalenceNelson’s death is one of an undeterminednumber of suicides that occur each yearin public and private juvenile facilitiesthroughout the Nation. According to theCenters for Disease Control and Preven-tion (CDC), the suicide rate of adoles-cents ages 15 to 19 has quadrupled from2.7 suicides per 100,000 in 1950 to 11suicides per 100,000 in 1994 (Centers forDisease Control and Prevention, 1995).CDC also reported that more teenagersdied of suicide during 1994 than of can-cer, heart disease, acquired immune defi-ciency syndrome, birth defects, stroke,pneumonia and influenza, and chroniclung disease combined.
Several national studies have examinedthe extent and nature of suicide in jailand prison facilities (Hayes, 1989, 1995),but there has been little comparable na-tional research regarding juvenile suicidein secure detention or confinement. Theonly national survey of juvenile suicidesin secure custody (Flaherty, 1980) re-flected a problematic calculation of sui-cide rates. Reanalysis of suicide rates inthat study found that youth suicide injuvenile detention and correctional fa-cilities was more than four times greaterthan youth suicide in the general popula-tion (Memory, 1989). Accurate data onthe total scope and rate of juvenile sui-cide in custody are still lacking.
The U.S. Bureau of the Census has beencollecting data on the number of deathsof juveniles in custody since 1989. In thefirst year of the survey, juvenile officials
self-reported 17 suicides in public deten-tion centers, reception and diagnosticcenters, and training schools during 1988(Krisberg et al., 1991). Fourteen such sui-cides were reported during 1993 (Austinet al., 1995). Given the epidemiologicaldata regarding adolescent suicide, coupledwith the increased risk factors associatedwith detained and confined youth, thereported number of suicides in custodyappears low. The National Center forHealth Statistics, however, reported that30,903 persons committed suicide in theUnited States in 1996. Of these, approxi-mately 7 percent (2,119) were youth age19 or younger. For youth younger than age15, suicides increased 113 percent between1980 and 1996 (Snyder and Sickmund,1999). Because of statistics like these, manyjuvenile justice experts and practitionersbelieve that suicides are underreported. Todate, no comprehensive study of deaths incustody has been undertaken.
Suicide in juvenile detention andcorrectional facilities was more than fourtimes greater than youth suicide overall.
Risk FactorsBrent (1995) identified mental healthdisorder and substance abuse as the mostimportant set of risk factors for adoles-cent suicide. Other risk factors includeimpulsive aggression, parental depressionand substance abuse, family discord andabuse, and poor family support. Life stres-sors, specifically interpersonal conflictand loss and legal and disciplinary prob-lems, were also associated with suicidalbehavior in adolescents, particularly sub-stance abusers. Many of these risk factorsare prevalent in youth confined in ju-venile facilities (Alessi et al., 1984;Rohde, Seeley, and Mace, 1997).
26
Juvenile Justice
Although there are insufficient nationaldata regarding the incidence of youthsuicide in custody, information suggestsa high prevalence of suicidal behavior injuvenile correctional facilities. Accordingto a study funded by the Office of JuvenileJustice and Delinquency Prevention, morethan 11,000 juveniles engage in morethan 17,000 incidents of suicidal behaviorin juvenile facilities each year (Parent etal., 1994). In addition, the limited re-search on juvenile suicide in custody sug-gests that confined youth may be morevulnerable to suicidal behavior based oncurrent or prior suicidal ideation (i.e.,thoughts and/or ideas of hurting or killingoneself). For example, one study foundthat incarcerated youth with either majoraffective disorders or borderline personal-ity disorders had a higher degree of sui-cidal ideation and more suicide attemptsthan comparable adolescents in the gen-eral population (Alessi et al., 1984).
American Indian youth confined injuvenile facilities.
Conditions ofConfinementIn August 1994, the Office of JuvenileJustice and Delinquency Preventionpublished Conditions of Confinement:Juvenile Detention and Corrections Facilities(Parent et al., 1994). The study describedin that Report investigated several con-ditions of confinement within juvenilefacilities, including suicide preventionpractices. Using four specific assessmentcriteria to evaluate suicide preventionpractices—written procedures, intakescreening, staff training, and closeobservation—the study found thefollowing:
◆ Only 25 percent of confined juvenileswere in facilities that conformed to all foursuicide prevention assessment criteria.
◆ Facilities that conducted suicidescreening at admission and trained staff insuicide prevention had fewer incidents ofsuicidal behavior among their residents.
◆ Suicidal behavior increased for youthhoused in isolation.
◆ Written policies to provide close ob-servation of suicidal residents did not ap-pear to significantly reduce the rate ofsuicidal behavior. Because these policiesare typically implemented after the riskor attempt is recognized, however, theymay reduce the number of suicides.
Critical Componentsof a Suicide PreventionPolicyThe American Correctional Association(ACA), the National Commission onCorrectional Health Care (NCCHC), theNational Juvenile Detention Association
Policies to provide close observation ofsuicidal residents did not appear tosignificantly reduce suicidal behavior.
Other studies found that a high percent-age of detained youth reported a historyof suicide attempts (Dembo et al., 1990)and psychiatric hospitalization (Waite,1992) and current and active suicidalbehavior (Davis et al., 1991). Two re-cent studies of youth confined in a ju-venile detention facility found thatsuicidal behavior in males was associ-ated with depression and decreased so-cial connection, while suicidal behaviorin females was associated with impulsiv-ity and instability (Mace, Rohde, andGnau, 1997; Rhode, Seely, and Mace,1997). Finally, other researchers foundhigh rates of suicidal behavior (Duclos,LeBeau, and Elias, 1994) and psychiatricdisorders (Duclos et al., 1998) among
27Volume VII • Number 1
Suicide Prevention in Juvenile Facilities
(NJDA), and other national organizationshave long advocated comprehensive sui-cide prevention programming. ACA andNCCHC have promulgated national de-tention and corrections standards thatare adaptable to individual juvenile facili-ties. While the ACA standards are morewidely recognized, the NCCHC standardsoffer more comprehensive guidance regard-ing suicide prevention and identify therecommended ingredients for a suicide pre-vention plan: identification, training, as-sessment, monitoring, housing, referral,communication, intervention, notification,reporting, review, and critical incident de-briefing (National Commission on Correc-tional Health Care, 1999). NJDA hasdeveloped a suicide prevention curriculumthat is incorporated into its detention staffbasic training course. Using a combinationof ACA and NCCHC standards, the au-thor has developed a comprehensive sui-cide prevention plan for juvenile facilitiesthat addresses the following key compo-nents: staff training, intake screening andongoing assessment, communication, hous-ing, levels of supervision, intervention, re-porting, and followup/mortality review.These components form a continuum ofcare intended to minimize suicidal behav-ior within secure juvenile detention andcorrectional facilities.
Staff TrainingThe essential component of a successfulsuicide prevention program is properlytrained staff—the backbone of any ju-venile facility. Mental health, medical,or other program staff prevent few sui-cides because juveniles usually attemptsuicides in housing units during lateevening hours or on weekends, whenprogram staff are absent. Accordingly,suicide attempts must be thwarted bydirect-care staff who have been trainedin suicide prevention and have devel-oped an intuitive sense about the youthunder their care.
All direct-care, medical, and mentalhealth personnel, in addition to anystaff who have regular contact withyouth, should receive 8 hours of initialsuicide-prevention training, followedby 2 hours of refresher training eachyear. The initial training should addressthe reasons the environments of juve-nile facilities are conducive to suicidalbehavior, factors that may predisposeyouth to suicide, high-risk suicideperiods, warning signs and symptoms,components of the facility’s suicide pre-vention policy, and liability issues asso-ciated with juvenile suicide. The 2-hourrefresher training should review the pre-disposing risk factors, warning signs andsymptoms, and any changes to thefacility’s suicide prevention plan anddiscuss any recent suicides or suicideattempts in the facility.
Intake Screening andOngoing AssessmentIntake screening and ongoing assessmentof all confined youth are critical to a juve-nile facility’s suicide-prevention efforts.Although youth can become suicidal atany point during their confinement, thefollowing periods are considered timesof high risk (National Commission onCorrectional Health Care, 1999):
◆ On return to the facility from courtafter adjudication.
◆ Following receipt of bad news orafter suffering any type of humiliationor rejection.
◆ During confinement in isolation orsegregation.
◆ Following a prolonged stay in thefacility.
◆ Does the youth express helplessness orhopelessness and feel there is nothing tolook forward to in the immediate future?
◆ Is the youth thinking of hurting orkilling himself or herself?
To make a thorough and complete assess-ment, the intake process should also in-clude procedures for referring youth tomental health or medical personnel.Following the intake process, a procedureshould be in place that requires staff totake immediate action in case of anemergency. If staff hear a youth verbalizea desire or intent to commit suicide, ob-serve a youth engaging in self-harm, orotherwise believe a youth is at risk forsuicide, they should constantly observethe youth until appropriate medical,mental health, or supervisory assistancecan be obtained.
CommunicationCertain behavioral signs exhibited byyouth may indicate suicidal behavior.Detection and communication of thesesigns to others can reduce the likelihoodof suicide. Direct-care staff who establishtrust and rapport with youth, gather per-tinent information, and take action canprevent many juvenile suicides (Roush,1996). There are three paths of commu-nication in preventing juvenile suicides:between the arresting or transporting of-ficer and direct-care staff; between andamong facility staff (including directcare, medical, and mental health person-nel); and between facility staff and thesuicidal youth.
In many ways, suicide prevention beginsat the point of arrest. Close observationof what youth say and how they behaveduring arrest, transport to the facility,and intake are crucial in detecting sui-cidal behavior. The scene of arrest isoften the most volatile and emotionaltime, so arresting officers should pay
Suicide prevention begins at the pointof arrest.
Intake screening for suicide risk may beincluded in the medical screening formor on a separate form. The screening pro-cess should obtain answers to the follow-ing questions:
◆ Was the youth considered a medical,mental health, or suicide risk during anyprevious contact or confinement withinthis facility?
◆ Does the arresting or transporting of-ficer have any information (e.g., from ob-served behavior, documentation from thesending agency or facility, conversationwith a family member or guardian) thatindicates the youth should currently beconsidered a medical, mental health, orsuicide risk?
◆ Has the youth ever attempted suicide?
◆ Has the youth ever considered suicide?
◆ Has the youth ever been or is theyouth currently being treated for mentalhealth or emotional problems?
◆ Has the youth recently experienced asignificant loss (e.g., job, relationship,death of a family member or close friend)?
◆ Has a family member or close friendever attempted or committed suicide?
29Volume VII • Number 1
Suicide Prevention in Juvenile Facilities
particular attention to youth during thistime: The anxiety or hopelessness of thesituation can provoke suicidal behavior,and onlookers such as family members,guardians, and friends can provide infor-mation on any previous suicidal behav-ior. The arresting or transporting officershould communicate any pertinent infor-mation regarding the well-being of theyouth to direct-care staff. It is also criti-cal for direct-care staff to maintain openlines of communication with parents orguardians, who often have pertinent in-formation regarding the mental healthstatus of residents.
During intake and screening, effectivemanagement of suicidal youth is based oncommunication between direct-care per-sonnel and other professional staff in thefacility. Because youth can become sui-cidal at any point during confinement,direct-care staff should be alert, share in-formation, and make appropriate referralsto mental health and medical staff. Thefacility’s shift supervisor should ensurethat direct-care staff are properly in-formed of the status of each youth desig-nated for suicide precautions and shouldsimilarly brief the incoming shift supervi-sor. Interdisciplinary team meetings todiscuss the status of youth designated for
suicide precautions should occur on aregular basis and include direct-care,medical, and mental health personnel.Finally, the authorization for suicide pre-cautions, any changes in these precau-tions, and the observations made ofyouth designated for precautions shouldbe documented on specific forms anddistributed to appropriate staff.
HousingWhen determining the most appropriatehousing location for a suicidal youth, ju-venile facility officials often physicallyisolate and restrain the individual withthe concurrence of medical or mentalhealth staff. These responses may provedetrimental to the youth. Isolation in-creases the sense of alienation and furtherremoves the individual from proper staffsupervision (Parent et al., 1994). Housingassignments should maximize staff inter-action with the youth and avoid height-ening the depersonalizing aspects ofconfinement. Suicidal youth should behoused in the general population, mentalhealth unit, or medical infirmary, wherethe youth is close to staff. Removing ayouth’s clothing (with the exception ofbelts and shoelaces) and using physicalrestraints should be done only as a lastresort when the youth is physicallyengaging in self-destructive behavior.
Rooms designated to house suicidal youthshould be suicide-resistant, free of signifi-cant protrusions, and provide full visibility(including room doors with clear panelslarge enough to provide staff with unob-structed interior views). Finally, eachhousing unit in the facility should containemergency equipment, including a first-aid kit, pocket mask or face shield, Ambu-bag, and a rescue tool that cuts throughfibrous material. Direct-care staff shouldensure, on a daily basis, that such equip-ment is in working order.C
SupervisionPromptness of response to suicide at-tempts in juvenile facilities is often drivenby the level of supervision. Medical evi-dence suggests that brain damage fromstrangulation caused by a suicide attemptcan occur within 4 minutes and death canoccur within 5 to 6 minutes (AmericanHeart Association, Emergency CardiacCare Committee and Subcommittees,1992). Two levels of supervision are rec-ommended for suicidal youth: close obser-vation and constant observation. Closeobservation is reserved for youth who arenot actively suicidal but express suicidalthoughts (e.g., expressing a wish to diewithout a specific threat or plan) or havea recent history of self-destructive behav-ior. Staff should observe such youth atstaggered intervals not to exceed 15 min-utes. Constant observation is reserved foryouth who are actively suicidal—eitherthreatening or engaging in suicidal behav-ior. Staff should observe such youth on acontinuous, uninterrupted basis. Somejurisdictions use an intermediate level ofsupervision with observation at staggeredintervals that do not exceed 5 minutes.Other aids (e.g., closed-circuit televisionand roommates) can be used as a supple-ment to, but never as a substitute for,these observation levels. Finally, mentalhealth staff should assess and interactwith—not just observe—suicidal youthon a daily basis. A careful assessmentshould be made of the youth’s underlyingmental health needs, and a plan shouldbe developed to address those needs.
InterventionThe manner and promptness of the staff ’sintervention after a suicide attempt oftendetermine whether the victim will sur-vive. Providing competent training andestablishing an effective system of com-munication can facilitate this interven-tion process. First, all staff who come into
contact with youth should be trained infirst-aid procedures and cardiopulmonaryresuscitation (CPR). Second, any staffmember who discovers a youth engagingin self-harm should immediately surveythe scene to assess the severity of theemergency, alert other staff to call formedical personnel, if necessary, and be-gin first aid or CPR. Third, staff shouldnever presume that the youth is dead;rather, they should initiate and continueappropriate life-saving measures untilthey are relieved by arriving medical per-sonnel. In addition, medical personnelshould ensure daily that equipment usedin responding to an emergency withinthe facility is in working order. Finally,although not all suicide attempts requireemergency medical intervention, mentalhealth staff should intervene and assessall suicide attempts.
ReportingIn the event of a suicide attempt or sui-cide, appropriate officials should be noti-fied through the appropriate chain ofcommand. Following the incident, thevictim’s family and appropriate outsideauthorities should be notified immedi-ately. Staff who came into contact withthe victim before the incident shouldsubmit a statement that details theirknowledge of the youth and the incident.
FollowupA juvenile suicide is extremely stressfulfor staff and residents. Staff may feel os-tracized by fellow personnel and admin-istration officials; the direct-care workermay display misplaced guilt, wondering“What if I had made my room checkearlier?”; and residents are often trauma-tized by critical events occurring withina facility. When crises occur, staff andresidents should be offered immediateassistance. One form of assistance isCritical Incident Stress Debriefing
31Volume VII • Number 1
Suicide Prevention in Juvenile Facilities
(CISD). A CISD team, comprisingprofessionals trained in crisis interven-tion and traumatic stress awareness(e.g., police officers, paramedics,firefighters, clergy, and mental healthpersonnel), provides affected staff andresidents an opportunity to process theirfeelings about the incident, develop anunderstanding of critical stress symp-toms, and develop ways of dealing withthem (Meehan, 1997; Mitchell andEverly, 1996). For maximum effective-ness, the CISD process or other appro-priate support services should occurwithin 24 to 72 hours of the criticalincident.
Every suicide and serious suicide attempt(i.e., attempts requiring medical treat-ment or hospitalization) should be exam-ined through a mortality review process.If resources permit, clinical review of sui-cide through a psychological autopsy—a retrospective reconstruction of thevictim’s life—is also recommended(Sanchez, 1999). Ideally, the mortalityreview should be coordinated by an out-side agency to ensure impartiality andshould be separate from other formal in-vestigations that may be required to de-termine the cause of death. The reviewshould include a critical inquiry of thefollowing aspects of the case:
◆ Circumstances surrounding theincident.
◆ Facility procedures relevant to theincident.
◆ All relevant training received byinvolved staff.
◆ Pertinent medical and mental healthservices and reports involving the victim.
◆ Recommendations, if any, for changesin policy, training, physical plant, medi-cal or mental health services, and opera-tional procedures.
Conclusion“For every two youth (ages 0–19) mur-dered in 1996, one youth committedsuicide” (Snyder and Sickmund,1999:24). Youth suicide is recognized as aserious public health problem, but suicidewithin juvenile facilities has not receivedcomparable attention, and the extentand nature of these deaths remain un-known. Collaborative efforts amongchild-serving agencies and technical as-sistance training for juvenile facility staffare just two of the components that areessential for suicide prevention withinsecure juvenile detention and correc-tional facilities. Now is the time to focusadditional attention and resources onpreventing suicide within these facilities.
ReferencesAlessi, N.E., McManus, M., Brickman, A., andGrapentine, L. 1984. Suicidal behavior amongserious juvenile offenders. American Journal ofPsychiatry 141(2):286–287.
American Heart Association, Emergency CardiacCare Committee and Subcommittees. 1992.Guidelines for cardiopulmonary resuscitation andemergency cardiac care. Journal of the AmericanMedical Association 268:2172–2183.
Austin, J., Krisberg, B., DeComo, R., Rydenstine,S., and Del Rosario, D. 1995. Juveniles Taken IntoCustody: Fiscal Year 1993. Report. Washington,DC: U.S. Department of Justice, Office of JusticePrograms, Office of Juvenile Justice and Delin-quency Prevention.
Brent, D.A. 1995. Risk factors for adolescent sui-cide and suicidal behavior: Mental and substanceabuse disorders, family environmental factors, andlife stress. Suicide and Life-Threatening Behavior 25(Supplement):52–63.
Centers for Disease Control and Prevention. 1995.Suicide among children, adolescents and youngadults—United States, 1980–1992. Morbidity andMortality Weekly Review 44:289–291.
Davis, D.L., Bean, G.L., Schumacher, J.E., andStringer, T.L. 1991. Prevalence of emotional dis-orders in a juvenile justice institutional popula-tion. American Journal of Forensic Psychology9:1–13.
32
Juvenile Justice
Dembo, R., Williams, L., Wish, E.D., Berry, E.,Getreu, A.M., Washburn, M., and Schmeidler, J.1990. Examination of the relationships amongdrug use, emotional/psychological problems, andcrime among youths entering a juvenile detentioncenter. The International Journal of the Addictions25:1301–1340.
Duclos, C.W., Beals, J., Novins, D.K., Martin, C.,Jewett, C.S., and Manson, S.M. 1998. Prevalenceof common psychiatric disorders among AmericanIndian adolescent detainees. Journal of the Ameri-can Academy of Child and Adolescent Psychiatry37(8):866–873.
Duclos, C.W., LeBeau, W., and Elias, G. 1994.American Indian suicidal behavior in detentionenvironments: Cause for continued basic andapplied research. Jail Suicide Update 5(4):4–9.
Flaherty, M. 1980. An Assessment of the NationalIncidence of Juvenile Suicides in Adult Jails, Lockups,and Juvenile Detention Centers. Champaign, IL:Community Research Forum.
Hayes, L.M. 1989. National study of jail suicides:Seven years later. Psychiatric Quarterly 60(1):7–29.
Hayes, L.M. 1994. Juvenile suicide in confine-ment: An overview and summary of one system’sapproach. Juvenile and Family Court Journal45(2):65–75.
Hayes, L.M. 1995. Prison suicide: An overviewand a guide to prevention. The Prison Journal75(4):431–455.
Krisberg, B., DeComo, R., Herrera, N.C.,Steketee, M., and Roberts, S. 1991. JuvenilesTaken Into Custody: Fiscal Year 1990 Report.Washington, DC: U.S. Department of Justice,Office of Justice Programs, Office of JuvenileJustice and Delinquency Prevention.
Mace, D., Rohde, P., and Gnau, V. 1997. Psycho-logical patterns of depression and suicidal behav-ior of adolescents in a juvenile detention facility.Journal of Juvenile Justice and Detention Services12(1):18–23.
Meehan, B. 1997. Critical incident stress debriefingwithin the jail environment. Jail Suicide/MentalHealth Update 7(1):1–5.
Memory, J. 1989. Juvenile suicides in secure de-tention facilities: Correction of published rates.Death Studies 13:455–463.
Mitchell, J.T., and Everly, G.S. 1996. Critical Inci-dent Stress Debriefing: An Operations Manual for thePrevention of Traumatic Stress Among EmergencyServices and Disaster Workers, 2d ed. Ellicott City,MD: Chevron Publishing.
National Commission on Correctional HealthCare. 1999. Standards for Health Services in JuvenileDetention and Confinement Facilities. Chicago, IL:National Commission on Correctional HealthCare.
Parent, D.G., Leiter, V., Kennedy, S., Livens, L.,Wentworth, D., and Wilcox, S. 1994. Conditionsof Confinement: Juvenile Detention and CorrectionsFacilities. Washington, DC: U.S. Department ofJustice, Office of Justice Programs, Office of Juve-nile Justice and Delinquency Prevention.
Rohde, P., Seeley, J.R., and Mace, D.E. 1997. Cor-relates of suicidal behavior in a juvenile detentionpopulation. Suicide and Life-Threatening Behavior27(2):164–175.
Roush, D.W. 1996. Desktop Guide to Good JuvenileDetention Practice. Washington, DC: U.S. Depart-ment of Justice, Office of Justice Programs, Officeof Juvenile Justice and Delinquency Prevention.
Sanchez, H.G. 1999. Inmate suicide and the psy-chological autopsy process. Jail Suicide/MentalHealth Update 8(3):3–9.
Snyder, H.N., and Sickmund, M. 1999. JuvenileOffenders and Victims: 1999 National Report.Washington, DC: U.S. Department of Justice,Office of Justice Programs, Office of JuvenileJustice and Delinquency Prevention.
Waite, D. 1992. Unpublished data. Richmond,VA: Virginia Department of Youth and FamilyServices.
JUSTICE MATTERSIN BRIEF
33Volume VII • Number 1
OJJDP-Supported Mental HealthInitiatives and ProgramsThe following OJJDP-supported ini-tiatives and programs target youthwith mental health disorders in thejuvenile justice system.
Assessing Alcohol, Drug,and Mental HealthDisorders Among JuvenileDetaineesThis program, implemented byNorthwestern University, supple-ments an ongoing National Insti-tute of Mental Health longitudinalstudy assessing alcohol, drug, andmental health disorders among ju-veniles in detention in CookCounty, IL. The program, whichOJJDP began funding in FY 1998,has three goals:
◆ To determine how alcohol, drug,and mental disorders among juve-nile detainees develop over time.
◆ To investigate whether juveniledetainees receive needed psychiatricservices after their cases reach dis-position and they are back in thecommunity or serving sentences.
◆ To study how risk behaviors as-sociated with violence, drug use,and HIV/AIDS develop over time,what the antecedents of these be-haviors are, and how these behav-iors are interrelated.
This project is unique because of itslarge sample size. It includes 1,833youth from Chicago, IL, who were
arrested and then interviewed be-tween 1996 and 1998. The sample isstratified by gender, race (AfricanAmerican, non-Hispanic white,Hispanic), and age (10–13, 14–17).Investigators have completed initialinterviews and have collected ex-tensive archival data (e.g., arrestand incarceration history, healthand/or mental health treatments)on each subject. They have beentracking the whereabouts of subjectsand are beginning to reinterviewthese adolescents. The large samplesize provides sufficient statisticalpower to study rare disorders, pat-terns of drug use, and risky, life-threatening behaviors.
Center for Students WithDisabilities in the JuvenileJustice SystemIn FY 1999, OJJDP undertook a jointinitiative with the U.S. Departmentof Education’s Office of Special Edu-cation and Rehabilitative Servicesto establish the Center for StudentsWith Disabilities in the JuvenileJustice System. The Attorney Gen-eral and the Secretary of Educationexpect this project to significantlyenhance juvenile justice system ser-vices for students with disabilities.Based on a combination of research,training, and technical assistance,these enhancements in prevention,educational services, and reintegra-tion will improve results for children
and youth with disabilities. TheCenter, implemented by the Univer-sity of Maryland, provides guidanceand assistance—based on research-validated practices—to States,schools, justice programs, families,and communities to design, imple-ment, and evaluate comprehensiveeducational programs for studentswith disabilities who are within thejuvenile justice system.
Circles of Care ProgramIn FY 1998, the Center for MentalHealth Services (CMHS) initiatedthe Circles of Care Program to buildthe capacity of selected AmericanIndian tribes to plan and developa continuum of care for AmericanIndian youth at risk of mentalhealth, substance abuse, and delin-quency problems. As part of multi-year joint efforts with CMHS,OJJDP entered into a 3-year inter-agency agreement to support theprogram, and in FY 1998 andFY 1999, OJJDP transferred fundsto CMHS to support one of nineselected tribal sites.
Communities In Schools,Inc.—Federal InteragencyPartnershipThis program continues an ongoingnational school dropout preventionmodel developed and implementedby Communities In Schools, Inc.
34
JUSTICE MATTERSIN BRIEF
(CIS). CIS provides training andtechnical assistance in adapting andimplementing the CIS model inStates and local communities. Thedropout prevention model bringssocial, employment, mental health,drug prevention, entrepreneurial,and other resources to high-riskyouth and their families in theschool setting. During the FederalInteragency Partnership, CIS Stateorganizations assume primary re-sponsibility for local program repli-cation. The partnership is basedon enhancing the following:
◆ CIS’s training and technicalassistance capabilities.
◆ CIS’s capability to introduceselected initiatives for youth at thelocal level.
Juvenile Suicide in Confinement: A National SurveyThe Office of Juvenile Justice andDelinquency Prevention recentlyawarded the National Center onInstitutions and Alternatives(NCIA) a contract to conduct anational survey on the prevalenceof juvenile suicide in confinement.
The project—initiated in August1999 and supported by the NationalJuvenile Detention Association andCouncil of Juvenile CorrectionalAdministrators—will for the firsttime determine the extent and dis-tribution of suicides in approxi-mately 3,400 public and privatejuvenile detention centers, trainingschools, reception/diagnostic cen-ters, ranches, camps, and farmsthroughout the Nation.
Answers to the survey questionswill allow NCIA staff to gatherdescriptive data on demographiccharacteristics of suicide victims,characteristics of the incidents,and characteristics of the facilitiesin which the suicides occurred. Areport of the findings will be avail-able as a resource tool for both ju-venile justice practitioners inexpanding their knowledge baseand juvenile correctional adminis-trators in creating and/or revisingpolicies and training curriculumson suicide prevention.
All juvenile facilities in which asuicide occurred during the 5-yearperiod of 1995–99 are stronglyencouraged to participate in the
study. Data provided will be codedand held in the strictest confi-dence. Results of the study willbe presented in summary fashion;therefore, victim and facility nameswill not appear in any report.
For more information on theJuvenile Suicide in ConfinementProject, contact:
Lindsay M. Hayes, Project DirectorNational Center on Institutions
and Alternatives40 Lantern LaneMansfield, MA 02048
◆ CIS’s capability to network withFederal agencies on behalf of Stateand local CIS programs.
With OJJDP’s support, CIS focuseson family strengthening initiativesthat benefit both youth and theirfamilies.
Comprehensive Childrenand Families MentalHealth Training andTechnical AssistanceUnder an FY 1999 3-year inter-agency agreement, OJJDP trans-ferred funds to the Center forMental Health Services (CMHS) to
support training and technical assis-tance for the CMHS-funded Com-prehensive Mental Health sites.These funds will enhance the in-volvement of the juvenile justicesystem in the systems of care beingdeveloped in each of the CMHS-funded sites.
Multisite, MultimodalTreatment Study of ChildrenWith Attention Deficit/Hyperactivity DisorderIn 1992, the National Institute ofMental Health (NIMH) began astudy of the long-term efficacy ofstimulant medication and intensivebehavioral and educational treat-ment for children with attention
JUSTICE MATTERSIN BRIEF
35Volume VII • Number 1
deficit/hyperactivity disorder(ADHD). Under an interagencyagreement with NIMH, OJJDP hastransferred funds to support this re-search, funded principally byNIMH. The study will continuethrough 2000, following the familieswith ADHD children identified in1992 and a comparison group.OJJDP’s participation, which beganin FY 1998, allows investigators tostudy the subjects’ delinquent be-havior and any contact with the le-gal system, including arrests andcourt referrals.
Strengthening Servicesfor Chemically InvolvedChildren, Youth, andFamiliesThis program, jointly supported bythe U.S. Departments of Justice andHealth and Human Services (HHS),provides services to children affectedby parental substance use or abuse.OJJDP administers this training andtechnical assistance program, whichbegan in FY 1998, with funds trans-ferred to OJJDP by HHS’s SubstanceAbuse and Mental Health ServicesAdministration, through a coopera-tive agreement with the Child Wel-fare League of America (CWLA), anonprofit organization. CWLA,which implements the program, hasidentified five residential child welfaresites, one in each of the CWLA’s fiveregions, to demonstrate the effective-
ness of integrating AOD prevention/treatment strategies into existingchild welfare and juvenile justice pro-grams and services. The goals of thisintegration of strategies are to educatestaff and to improve outcomes for
adolescents participating in the pro-grams. CWLA also provides technicalassistance to other member agenciesreplicating the various program mod-els identified through their evalua-tions of the programs.
For Further InformationAdditional sources of information on programs for children with disabilitiesand their parents are provided below:
Center for Effective Collaborationand Practice
American Institutes for Research1000 Thomas Jefferson Street NW.Suite 400Washington, DC 20007800–457–1551202–944–5454 (fax)E-mail: [email protected]: www.air.org/cecp
Federation of Families forChildren’s Mental Health
1021 Prince StreetAlexandria, VA 22314703–684–7710703–836–1040 (fax)E-mail: [email protected]: www.ffcmh.org
National Mental Health AssociationOffice of Prevention and Children’s
Mental Health ServicesJuvenile Justice and Mental Health1021 Prince StreetAlexandria, VA 22314–2971800–969–6642703–684–7722703–684–5968 (fax)E-mail: [email protected]: www.nmha.org
Northwestern Human Services620 Germantown PikeLafayette Hill, PA 19444610–260–4600Internet: www.nhsonline.org
Youth & Family Centered Services1705 Capital of Texas Highway SouthSuite 500Austin, TX 78746512–327–1119512–327–4576 (fax)E-mail: [email protected]: www.yfcs.com
36
IN BRIEF
Treating Serious Anti-Social Behavior in Youth:The MST Approach
Traditional mentalhealth approachesfor serious, violent,and chronic juve-nile offendershave all too oftenfailed to yieldsuccessful re-
sults. Adolescent drug andsubstance abuse is remarkably resis-tant to treatment.
The Multisystemic Therapy (MST)approach to the treatment of seri-ous antisocial behavior in adoles-cents represents a significantdeparture from more traditionalstrategies. MST is a home-basedservices approach developed in re-sponse to the lack of scientificallyproven, cost-effective treatmentoptions for this population.
Treating Serious Anti-Social Behavior inYouth: The MST Approach, an OJJDPBulletin released in May 1997, pro-vides an overview of the MST ap-proach and features evaluations ofprograms that have implemented it.The Bulletin is available online atwww.ojjdp.ncjrs.org/pubs/delinq.htmlor can be ordered from OJJDP’s Juve-nile Justice Clearinghouse (see theorder form).
Mental Health Disorders and SubstanceAbuse Problems Among Juveniles
An OJJDP Fact Sheetreleased in July 1998,Mental Health Disor-ders and SubstanceAbuse ProblemsAmong Juveniles,describes stepsthat OJJDP is tak-
ing with government andprivate organizations to address spe-cific behavior or circumstances thatbring juveniles into the justice sys-
tem and discusses the underlying,often long-term mental health andsubstance abuse problems of youthin the juvenile justice system.
The OJJDP steps described in thisFact Sheet include supporting re-search and data collection thatprovide a clearer picture of the in-cidence and prevalence of mentalhealth and substance abuse disordersamong juveniles, assessing juveniles
when they first come in contact withthe system, increasing the numberof high-quality treatment programsin the community and in juvenile in-stitutions, and focusing on juvenileswho are at risk for delinquency ratherthan those already in the juvenile jus-tice system. This Fact Sheet is avail-able online at www.ojjdp.ncjrs.org/pubs/fact.html or can be ordered fromOJJDP’s Juvenile Justice Clearing-house (see the order form).
Volume VII • Number 1 37
IN BRIEF
Juvenile Offenders and Victims:1999 National Report
OJJDP’s JuvenileOffenders andVictims: 1999National Reportbrings togetherthe most recentstatistics on avariety of top-ics related to
the problems of juve-nile crime, violence, and victimiza-tion. Readers will find extensivebaseline information on juvenilepopulation characteristics; patternsof offending and victimization; andthe structure, procedures, and activi-ties of the juvenile justice system.The information is presented in nu-merous tables, graphs, and maps, ac-companied by analyses written inclear, nontechnical language.
The National Report covers severaltopics of particular interest to readersconcerned with mental health issues:
◆ Drug abuse: juvenile arrests fordrug abuse offenses, patterns of deviantbehavior (including marijuana use)among youth ages 12–16, illicit druguse among high school seniors, andsocietal costs of juvenile drug abuse.
◆ Child abuse and neglect: inci-dence and characteristics, includingdata on psychological and emo-tional abuse.
◆ Suicide: long-range trends inyouth suicide, and data by agegroup, race, and sex.
◆ Violence: extensive data on in-cidence and characteristics of juve-
Call for MaterialsThe mental health needs of youth is a vastly growing topic of interest toprofessionals and researchers in the juvenile justice system. The Office ofJuvenile Justice and Delinquency Prevention (OJJDP) wants to assist youand your colleagues in learning about this topic via publications and otherinformation resources. OJJDP’s Juvenile Justice Clearinghouse and the Na-tional Criminal Justice Reference Service (NCJRS) offer an extensive li-brary collection covering all aspects of criminal and juvenile justice anddrug policy. Contribute to the NCJRS library and abstracts database(www.ncjrs.org/database.htm) by sending material related to mental healthand youth. Contributions should be a minimum of four pages in lengthand must have been published within the past 5 years. Materials will bereviewed to determine eligibility, and they cannot be returned. Send mate-rials or information to:
National Criminal JusticeReference Service
c/o Patricia Cronin, Collection Development2277 Research Boulevard, MS 2A
Rockville, MD 20850
nile arrests for violent crimes andpatterns of violent behavior amongyouth.
This Report is available onlineat www.ojjdp.ncjrs.org/pubs/violvict.html or can be ordered inhard copy or CD–ROM format fromOJJDP’s Juvenile Justice Clearing-house (see the order form).
38
IN BRIEF
OJJDP ONLINE
A Network for Sharing
The new Web site includes the following sections:
Visit the Web site at: www.childrenwithdisabilities.ncjrs.org.
Children With Disabilities: An Online Guide toResources for Parents and Children
◆ Federal Resources. Learn about Federal agenciesand their funded and supported initiatives, informa-tion, and resources.
◆ State/Local Resources. Discover informationabout agencies, organizations, and programs in yourarea by State, Territory, or federally recognized tribe.
◆ National Resources. Access national organiza-tions and associations that offer programs, informa-tion, and other resources.
◆ Calendar of Events. Visit the calendar for up-coming disability-related conferences and communityevents.
◆ Grants & Funding. Explore funding, grant, andother opportunities for Federal or private financialassistance.
◆ Research & Statistics. Secure the most up-to-dateresearch and statistics along with a keyword list andtips for searching using the Children With Disabilitiessearch engine.
◆ Youth to Youth. Share experiences, stories, andideas with other children and participate in games,activities, and a moderated online bulletin board.
◆ Highlights. Find out about the latest news andmost recent additions to the Web site.
Juvenile Justice Order FormVolume VII • Number I April 2000
International SubscribersAirmail Postage ScheduleAll documents ordered by Canadian and other international usersare sent airmail. Postage is included in the cost of fee items butmust be paid separately for free items. Use the schedule belowto compute the postage cost for your free items.
No. of free items Canada Other countries1–2 $ 6.30 $ 5.753–4 6.85 11.505–6 7.40 17.257–8 7.95 23.00
For more than 20 items, write JJC, P.O. Box 6000, Rockville, MD20849–6000, or call 301–519–5500.
To order other publications listed on the inside backcover, please complete the following:
Qty. NCJ No. Title Price
____________________________________________
____________________________________________
____________________________________________
____________________________________________
____________________________________________
Total $ ___________
Enclose payment or provide account number.
All payments must be in U.S. dollars and drawn ona U.S. bank.
❑ Check or money order enclosed, payable toJuvenile Justice Clearinghouse.
❑ Deduct the total from my NCJRS Deposit Account.
Acct. No. ____________________________________
Charge my ❑ MasterCard ❑ VISA
Card No. _____________________________________
Exp. Date ____________________________________
Signature_____________________________________
✄
PUBLICATIONS AVAILABLE FREE.
Single copies are available free. There is a nominal fee forbulk orders to cover postage and handling. Contact theClearinghouse for specific information.
❑ America’s Children: Key National Indicators of Well-Being, 1999 (Report). NCJ 171150.
❑ Causes and Correlates of Delinquency Program (FactSheet). FS 99100.
❑ Families and Schools Together: Building Relationships(Bulletin). NCJ 173423.
❑ NEW Juvenile Offenders and Victims: 1999 NationalReport (Report). NCJ 178257.
❑ NEW Juvenile Arrests 1998 (Bulletin). NCJ 179064.
❑ Mental Health Disorders and Substance Abuse ProblemsAmong Juveniles (Fact Sheet). FS 9882.
❑ Relationship Between Mental Health and SubstanceAbuse Among Adolescents. NCJ 177685.
❑ NEW Reporting Crimes Against Juveniles (Bulletin).NCJ 178887.
❑ Check this boxif the information onyour address label isincorrect and makecorrections on yourmailing label.
Publications From OJJDP
OJJDP produces a variety of publications—FactSheets, Bulletins, Summaries, Reports, and theJuvenile Justice journal—along with video-tapes, including broadcasts from the juvenilejustice telecommunications initiative. ThroughOJJDP’s Juvenile Justice Clearinghouse (JJC),these publications and other resources are asclose as your phone, fax, computer, or mailbox.Phone:800–638–8736(Monday–Friday, 8:30 a.m.–7 p.m. ET)Fax:301–519–5600Online:
Mail:Juvenile Justice Clearinghouse/NCJRSP.O. Box 6000, Rockville, MD 20849–6000Fact Sheets and Bulletins are also availablethrough fax on demand.Fax on Demand:800–638–8736, select option 1, select option 2,and listen for instructions.To ensure timely notice of new publications,subscribe to JUVJUST, OJJDP’s electronicmailing list.JUVJUST Mailing List:e-mail to [email protected] the subject line blanktype subscribe juvjust your nameIn addition, JJC, through the National CriminalJustice Reference Service (NCJRS), is the re-pository for tens of thousands of criminal andjuvenile justice publications and resourcesfrom around the world. They are abstractedand placed in a database, which is searchableonline (www.ncjrs.org/database.htm). You arealso welcome to submit materials to JJC forinclusion in the database.The following list highlights popular and re-cently published OJJDP documents and video-tapes, grouped by topical areas.The OJJDP Publications List (BC000115) offersa complete list of OJJDP publications and isalso available online.In addition, the OJJDP Fact Sheet Flier(LT000333) offers a complete list of OJJDPFact Sheets and is available online.OJJDP also sponsors a teleconference initia-tive, and a flier (LT116) offers a complete list ofvideos available from these broadcasts.
Corrections and DetentionBeyond the Walls: Improving Conditions ofConfinement for Youth in Custody. 1998,NCJ 164727 (116 pp.).Disproportionate Minority Confinement: 1997Update. 1998, NCJ 170606 (12 pp.).Disproportionate Minority Confinement:Lessons Learned From Five States. 1998,NCJ 173420 (12 pp.).
CourtsGuide for Implementing the Balanced and Re-storative Justice Model. 1998. NCJ 167887(112 pp.).Innovative Approaches to Juvenile IndigentDefense. 1998, NCJ 171151 (8 pp.).Juvenile Court Statistics 1996. 1999,NCJ 168963 (113 pp.).Offenders in Juvenile Court, 1996. 1999,NCJ 175719 (12 pp.).RESTTA National Directory of Restitutionand Community Service Programs. 1998,NCJ 166365 (500 pp.), $33.50.Trying Juveniles as Adults in Criminal Court:An Analysis of State Transfer Provisions. 1998,NCJ 172836 (112 pp.).Youth Courts: A National Movement Teleconfer-ence (Video). 1998, NCJ 171149 (120 min.), $17.
Delinquency Prevention1998 Report to Congress: Juvenile MentoringProgram (JUMP). 1999, NCJ 173424 (65 pp.).1998 Report to Congress: Title V IncentiveGrants for Local Delinquency Prevention Pro-grams. 1999, NCJ 176342 (58 pp.).Combating Violence and Delinquency: TheNational Juvenile Justice Action Plan (Report).1996, NCJ 157106 (200 pp.).Combating Violence and Delinquency: TheNational Juvenile Justice Action Plan(Summary). 1996, NCJ 157105 (36 pp.).Effective Family Strengthening Interventions.1998, NCJ 171121 (16 pp.).Juvenile Accountability Incentive Block GrantsStrategic Planning Guide. 1999, NCJ 172846(62 pp.).Parents Anonymous: Strengthening America’sFamilies. 1999, NCJ 171120 (12 pp.).Prenatal and Early Childhood Nurse HomeVisitation. 1998, NCJ 172875 (8 pp.).Treatment Foster Care. 1999, NCJ 173421(12 pp.).
Gangs1996 National Youth Gang Survey. 1999,NCJ 173964 (96 pp.).Gang Members on the Move. 1998,NCJ 171153 (12 pp.).Youth Gangs: An Overview. 1998, NCJ 167249(20 pp.).The Youth Gangs, Drugs, and Violence Con-nection. 1999, NCJ 171152 (12 pp.).Youth Gangs in America Teleconference(Video). 1997, NCJ 164937 (120 min.), $17.
General Juvenile JusticeComprehensive Juvenile Justice in StateLegislatures Teleconference (Video). 1998,NCJ 169593 (120 min.), $17.Guidelines for the Screening of Persons Work-ing With Children, the Elderly, and IndividualsWith Disabilities in Need of Support. 1998,NCJ 167248 (52 pp.).Juvenile Justice, Volume V, Number 1. 1998,NCJ 170025 (32 pp.).
A Juvenile Justice System for the 21st Century.1998, NCJ 169726 (8 pp.).Juvenile Offenders and Victims: 1999 NationalReport. 1999, NCJ 178257 (232 pp.).OJJDP Research: Making a Difference forJuveniles. 1999, NCJ 177602 (52 pp.).Promising Strategies To Reduce Gun Violence.1999, NCJ 173950 (253 pp.).Sharing Information: A Guide to the FamilyEducational Rights and Privacy Act andParticipation in Juvenile Justice Programs.1997, NCJ 163705 (52 pp.).
Missing and Exploited ChildrenPortable Guides to Investigating Child Abuse(13-title series).Protecting Children Online Teleconference(Video). 1998, NCJ 170023 (120 min.), $17.When Your Child Is Missing: A Family SurvivalGuide. 1998, NCJ 170022 (96 pp.).
Substance AbuseThe Coach’s Playbook Against Drugs. 1998,NCJ 173393 (20 pp.).Drug Identification and Testing in the JuvenileJustice System. 1998, NCJ 167889 (92 pp.).Preparing for the Drug Free Years. 1999,NCJ 173408 (12 pp.).
Violence and VictimizationCombating Fear and Restoring Safety inSchools. 1998, NCJ 167888 (16 pp.).Guide for Implementing the ComprehensiveStrategy for Serious, Violent, and ChronicJuvenile Offenders. 1995, NCJ 153681(255 pp.).Report to Congress on Juvenile ViolenceResearch. 1999, NCJ 176976 (44 pp.)Serious and Violent Juvenile Offenders. 1998,NCJ 170027 (8 pp.).Serious and Violent Juvenile Offenders: RiskFactors and Successful Interventions Teleconfer-ence (Video). 1998, NCJ 171286 (120 min.), $17.State Legislative Responses to Violent JuvenileCrime: 1996–97 Update. 1998, NCJ 172835(16 pp.).White House Conference on School Safety:Causes and Prevention of Youth ViolenceTeleconference (Video). 1998, NCJ 173399(240 min.), $17.
Youth in ActionCommunity Cleanup. 1999, NCJ 171690 (6 pp.).Cross-Age Teaching. 1999, NCJ 171688 (8 pp.).Make a Friend—Be a Peer Mentor. 1999,NCJ 171691 (8 pp.).Plan a Special Event. 1999, NCJ 171689(8 pp.).Planning a Successful Crime PreventionProject. 1998, NCJ 170024 (28 pp.).Stand Up and Start a School Crime Watch.1998, NCJ 171123 (8 pp.)Two Generations—Partners in Prevention.1999, NCJ 171687 (8 pp.).Wipe Out Vandalism and Graffiti. 1998,NCJ 171122 (8 pp.).Youth Preventing Drug Abuse. 1998,NCJ 171124 (8 pp.).
Revised 3/24/00
NCJ 178256
PRESORTED STANDARDPOSTAGE & FEES PAID
DOJ/OJJDPPERMIT NO. G–91
U.S. Department of Justice
Office of Justice Programs
Office of Juvenile Justice and Delinquency Prevention
Washington, DC 20531
Official BusinessPenalty for Private Use $300
The Children With Disabilitiesonline guide is a new initiative by the
Coordinating Council on Juvenile Justiceand Delinquency Prevention to make
available a wide array of Federal, State,local, and national resources to children
with disabilities and their parents. Visit theChildren With Disabilities Web site at
www.childrenwithdisabilities.ncjrs.org,and join the network for sharing.