YWCA Programs for Early Learning and School Age Development 2017-2018 Enrollment Packet Child’s Name: ____________________________________________ Early Learning Center SDOL School Age Care Penn Manor School Age Care Penn Manor Wrap Program ________________ -FOR OFFICE USE ONLY- _____ Registration Form _____ Contracted Schedule Form _____ Emergency Contact form-MUST BE COMPLETE _____ Child Health Report _____ Getting to Know Your Child Form _____ Publicity Release Form _____ CACFP Paperwork (Lime Street Location Only) Payment Information: _____ Funded Caseworker: _____________________ _____ Self-Pay Record Number: ____-_____________ Checked By: __________________ Sibling name for discount __________________________ -FOR OFFICE USE ONLY- $__________ Registration $ __________ Deposit or CCIS Co-pay (Goes toward last week of care with 2 weeks’ notice) $__________ First Week Fee (Only when program already started) $__________ Key Card YWCA Only Lime Street only (1 st $15.00, 2 nd $7.50) Refunded upon return $ __________ Total Receipt Number: ____________________ Cash Check# ________ Money Order#_________ Credit Card # ________ TE #__________ Initials: __________________________ Date: ___________________________ (Registration fee, and deposit are non-refundable) Start Date: ___________________________ Site Notified: __________________________ Data completed ___/____/____ By: ________ H.A./Schedule completed ___/____/____ By: ________ Ledger/Tuition completed ___/____/______ By: ______ Payment Option ___Tuition Express Automatic (Attach form will be processed once file is entered into Pro-Care) ___ Tuition Express Online (Email will be sent with Link and Codeonce file is entered into Pro-Care) 1
Transcript
YWCA Programs for Early Learning and School Age Development 2017-2018 Enrollment Packet
Early Learning Center SDOL School Age Care Penn Manor School Age Care Penn Manor Wrap Program ________________
-FOR OFFICE USE ONLY-
_____ Registration Form _____ Contracted Schedule Form _____ Emergency Contact form-MUST BE COMPLETE _____ Child Health Report _____ Getting to Know Your Child Form _____ Publicity Release Form _____ CACFP Paperwork (Lime Street Location Only)
Payment Option ___Tuition Express Automatic (Attach form will be processed once file is entered into Pro-Care)
___ Tuition Express Online (Email will be sent with Link and Codeonce file is entered into Pro-Care)
1
Registration Form All information must be filled out in order for your child to be enrolled.
__________________________________________________ Start Date Site/Class Name
Please Print
Child’s Full Name ____________________________________________Age_____Birthdate__________Sex_____Race _____Grade Fall 2017______
Address ____________________________________________________________________________________ Home Phone # _________________
Please attach an IEP or IFSP for your child if applicable. Indicate with a check mark one of the following: _____ I am providing a copy of my child’s IEP/IFSP_____ I am not providing a copy of my child’s IEP/IFSP_____ This is not applicable to my child
Primary Guardian Name _____________________________________________________________________________________________________
Home Address_____________________________________________________________________________________________________________ Street City State Zip
Secondary Employer/School____________________________ Employer’s Address _____________________________________________________ Street City State Zip
Social Security #______________________ Date of Birth ___________________________________E-mail __________________________________ Person Responsible for Payment (if different from above, list address & phone): �Self �CCIS �Other _________________________________
At the time of enrollment a deposit/co-pay equal to the amount of one contracted week is required; in addition to the Registration and security card fees (for Lime Street Only). The deposit will be credited for the last week of service assuming a two week (14 days) written notice has been given.These fees are non-refundable. Please call Child Care Information Service at (717) 393-4004 for more information on subsidized care. 1. I understand my bill will be sent weekly via-email to the address I have provided to the YWCA Lancaster. Please provide the
YWCA Lancaster with your current e-mail address. If your e-mail is changed for any reason please provide the YWCA Lancaster with the new e-mail address. It is your responsibility to review all correspondence sent from the YWCA Lancaster. I agree to pay in advance for each week my child is contracted. I understand that payment is due the Thursday before the week service is needed.
2. I understand that there is an annual non-refundable registration fee for all Programs. 3. I understand that all Program fees are based on my contracted schedule. 4. I understand that billing is based on the full time or part time enrollment for which I have contracted and not for actual attendance. I
understand I will be billed for the days for which my child is enrolled based on their full time or part time status, even if she/he is absent from the program for any reason including but not limited to illness, vacations, etc. I understand that no fees will be credited to my account if my child is ill or fails to attend.
5. I agree to pay late fees of $1/minute if my child is not picked up by 6:00 pm. I also understand that I may be asked to remove my child from the program if late pick up is habitual.
6. I understand YWCA Lancaster programs cannot exceed staff-child ratios mandated by Department of Human Services. Therefore, unscheduled children will not be accepted.
7. I understand that failure to pay my contracted fees or an unpaid balance will result in my childcare services being interrupted until said balance is addressed. I understand that there is a $25 charge for all returned checks. Checks are to be made payable to YWCA Lancaster. I understand that it is my responsibility to keep statements, receipts or canceled checks for income tax purposes. YWCA Lancaster’s Federal ID number is 23-1352609.
110 North Lime Street Lancaster, PA 17602 [email protected] (717) 393-1735 (717) 396-0513 (fax)
Office use Only Total Days Contracted _____ M T W TH F Weekly Fee:______
____EHS ___ PKC ___SACC
2
8. All designated individuals understand that my child may not be left on school grounds without supervision. I agree to walk my childinto the Program each morning and to be sure a staff member is present before releasing my child. I understand that staff are notprepared to accept my child until 6:30 a.m. I will sign my child in each morning and/or out each evening. Transportation home fromthe program must be provided by a parent or other designated person.
9. I agree to follow all parking procedures mandated by the school when I drop off and/or pick up my child. I understand that failure todo so may affect my child’s enrollment in the program.
10. I understand that all forms required for programs must be completed and on file before my child may attend. These include theregistration form and this contract for services.
11. I understand that staff must release children to all parents unless a court order indicating sole custody is provided to the ProgramDirector at YWCA Lancaster.
12. I understand that I need to give written permission allowing staff to release my child to any individual other than the parent/guardianor those persons listed on Emergency contract/Parental consent form.
13. I understand that I am responsible for any damages resulting from my child’s actions to either YWCA Lancaster or school property.The price of any damaged items will be added to my weekly bill.
14. I understand that no medication is administered unless I fill out the medication log completely. Written instructions from a physicianare required for medication administered for ten or more days, or on an as-needed basis. All medication must be in the originalprescription bottle.
15. Families who wish to have sunscreen/sunblock at the program must complete a sunscreen form.16. I agree to support and reinforce Program rules and procedures that concern the health and safety of the children. I understand that
I must provide a current Health Appraisal, along with a current vaccination record for my child. I understand that my child may notattend the program with any illness that threatens the health of other children, and that the Health Department regulationsgoverning periods of infection are enforced. I will be asked to pick up my child from the program if he/she has a contagious illness.
17. I understand that all YWCA childcare programs are state licensed programs and that all staff are mandated reporters who arerequired to report any evidence of suspected abuse to Childline.
18. I waive any claim for bodily injury or property damage against Penn Manor School District, the City of Lancaster, LancasterTownship, Millersville Borough, Conestoga Township, Washington Boro, Manor Township, Martic Township, Pequea Township andthe YWCA Lancaster while my child is a participant in a YWCA Lancaster program at any location.
19. In accordance with applicable Federal and State civil rights laws and regulatory requirements, you and your child, as clients of theYWCA Lancaster, have the right:-To be provided services by YWCA Lancaster and to be referred for services at other facilities without regard to your race, color,sexual orientation, religious creed, disability, ancestry, national origin, age or sex.-Program services shall be made accessible to persons with disabilities through the most practical and economically feasiblemethods available. These methods include, but are not limited to equipment redesign, the provision of aids, and the use ofalternative services delivery locations. Structural modifications shall be considered only as a last resort among available methods.-If you feel you have been discriminated against on the basis of your race, color religious creed, disability, ancestry, national origin,age or sex, complaints of discrimination may be filed with any of the following:
YWCA Lancaster Attention: Deb Sims 110 North Lime Street Lancaster, PA 17602
PA Human Relations Comm. Harrisburg Regional Office 333 Market Street-8th Floor Harrisburg, PA 17101
Department of Human Services Bureau of Equal Opportunity Room 223, Health & Welfare Building P.O. Box 2675 Harrisburg, PA 17105
U.S. Department of Health and Human Services Office for Civil Rights Suite 372, Public Ledger Building 150 S. Independence Mall West Philadelphia, PA 19106
20. I understand that I may be asked to withdraw my child if his/her behavior patterns threaten his/her own health and safety or thehealth and safety of other children. The established discipline procedure will be followed, but severe infractions of the rules mayresult in immediate dismissal from the program.
21. I will notify the YWCA Lancaster of any change on the Registration Form and will verify by signature that all information is correctsemi-annually.
22. I understand that if my CCIS funding is discontinued I am responsible to pay the entire fee. Per CCIS regulations, if I reach 25 daysabsent from the program, I am responsible to pay the Center the daily rate for each day absent after the first 25 days.
_______________________________________ ____________ _________________________ ______________ Primary Parent/Guardian Signature Date YWCA Lancaster Signature Date
________________________________________ __________ Secondary Parent/Guardian Signature (optional) Date
Please sign after January 2018 Annual Review
I have reviewed my child’s registration and made necessary corrections. ____________________________________ _________________ Parent/Guardian Signature Date
3
Financial Information 2017-2018 YWCA Lancaster Rates
Infant, Young Toddlers, Older Toddlers and Pre School Full-Time Rates Infants $210.00 weekly
Young Toddlers $190.00 weekly
Older Toddlers $175.00 weekly
Pre School $210.00 weekly
Pre-K Counts Before and After Care Rates Pre-K Counts (8AM-1PM)
Schedule is based on the SDOL school year calendar.
Pre-K Counts Only Before Care/ASP Care
6:30AM-8AM & 1PM-6PM $100.00 Weekly No extra charge for No School Day
School Year Program (Grade K5)
2017-2018 Minimum
2 days 3 Days 4 Days 5 Days
Before & Wrap & After care
(6:30AM-9AM), (11:30AM-3:30 PM),
(3:30PM-6 PM)
$80.00 $106.00 $130.00 $135.00 No extra charge for No School Day or
Early Dismissal. Must sign-up for day!
Wrap care (11:30AM-3:30 PM) $68.00 $92.00 $102.00 $110.00
No extra charge for No School Day or Early Dismissal.
Must sign-up for day! Before & Wrap care
(6:30AM-9AM), (11:30AM-3:30 PM)
$70.00 $94.00 $114.00 $125.00 No extra charge for No School Day or
Early Dismissal. Must sign-up for day!
Wrap & After care (11:30AM-3:30 PM),
(3:30PM-6 PM) $70.00 $94.00 $114.00 $125.00
No extra charge for No School Day or Early Dismissal.
Must sign-up for day!
4
CCIS Clients
CCIS clients will be charged the daily rate for days of absence after the 25th absence, starting the 26thday of absence.
CCIS Rates Full-time per day Part-time per day
Infants $42.00 $35.00
Young Toddlers $38.00 $32.00
Older Toddlers $35.00 $30.00
Pre School/Pre-K Counts $31.00 $26.00
School Age Students 31.00 BSP/ASP 15.50 ASP
School Year Program (Grade 1-6th)
Before Care (6:30AM-9AM) $31.00 $41.00 $49.00 $55.00 May not add After school or Early
Dismissal day.
After Care (3:30PM-6PM)
$31.00 $41.00 $49.00 $55.00 You must be contracted for the day that the Early Dismissal occurs in
order to attend.
No School Day charge (6:30AM-6PM) $20.00
This fee is for those who sign up for NSD on their regularly contracted day of care. Must sign-up for day!
$62.00 $82.00 $98.00 $110.00 All Early dismissal and/or NSD fees for contracted days are included.
5
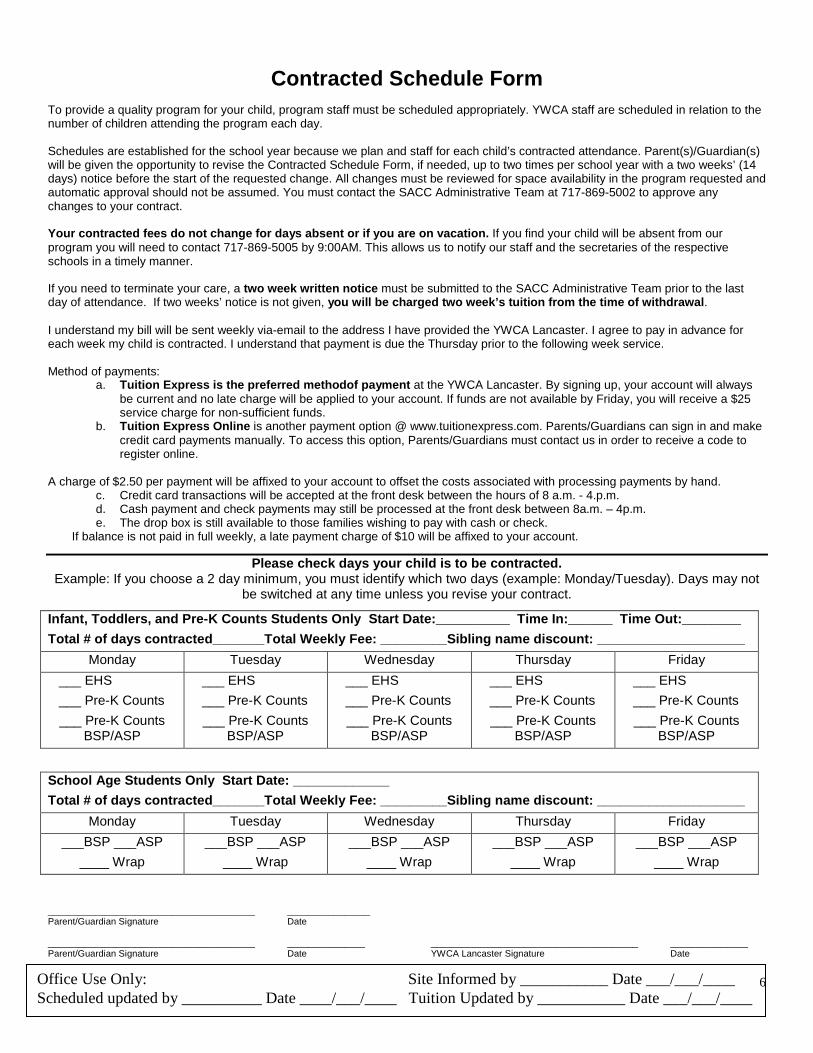
Contracted Schedule Form
To provide a quality program for your child, program staff must be scheduled appropriately. YWCA staff are scheduled in relation to the number of children attending the program each day. Schedules are established for the school year because we plan and staff for each child’s contracted attendance. Parent(s)/Guardian(s) will be given the opportunity to revise the Contracted Schedule Form, if needed, up to two times per school year with a two weeks’ (14 days) notice before the start of the requested change. All changes must be reviewed for space availability in the program requested and automatic approval should not be assumed. You must contact the SACC Administrative Team at 717-869-5002 to approve any changes to your contract. Your contracted fees do not change for days absent or if you are on vacation. If you find your child will be absent from our program you will need to contact 717-869-5005 by 9:00AM. This allows us to notify our staff and the secretaries of the respective schools in a timely manner. If you need to terminate your care, a two week written notice must be submitted to the SACC Administrative Team prior to the last day of attendance. If two weeks’ notice is not given, you will be charged two week’s tuition from the time of withdrawal. I understand my bill will be sent weekly via-email to the address I have provided the YWCA Lancaster. I agree to pay in advance for each week my child is contracted. I understand that payment is due the Thursday prior to the following week service. Method of payments:
a. Tuition Express is the preferred methodof payment at the YWCA Lancaster. By signing up, your account will always be current and no late charge will be applied to your account. If funds are not available by Friday, you will receive a $25 service charge for non-sufficient funds.
b. Tuition Express Online is another payment option @ www.tuitionexpress.com. Parents/Guardians can sign in and make credit card payments manually. To access this option, Parents/Guardians must contact us in order to receive a code to register online.
A charge of $2.50 per payment will be affixed to your account to offset the costs associated with processing payments by hand. c. Credit card transactions will be accepted at the front desk between the hours of 8 a.m. - 4.p.m. d. Cash payment and check payments may still be processed at the front desk between 8a.m. – 4p.m. e. The drop box is still available to those families wishing to pay with cash or check.
If balance is not paid in full weekly, a late payment charge of $10 will be affixed to your account.
Please check days your child is to be contracted. Example: If you choose a 2 day minimum, you must identify which two days (example: Monday/Tuesday). Days may not
be switched at any time unless you revise your contract.
________________________________________ ________________ Parent/Guardian Signature Date ________________________________________ _______________ ________________________________________ _______________ Parent/Guardian Signature Date YWCA Lancaster Signature Date
School Age Students Only Start Date: _____________ Total # of days contracted_______Total Weekly Fee: _________Sibling name discount: ____________________
Infant, Toddlers, and Pre-K Counts Students Only Start Date:__________ Time In:______ Time Out:________ Total # of days contracted_______Total Weekly Fee: _________Sibling name discount: ____________________
Office Use Only: Site Informed by ___________ Date ___/___/____ Scheduled updated by __________ Date ____/___/____ Tuition Updated by ___________ Date ___/___/____
6
Questionnaire for Parents How did you find out about YWCA Lancaster Program’s?
o Newspaper Addo Magazineo Onlineo Returning familyo By friends or familieso Other please indicate _______________________________________________________________________
GETTING TO KNOW YOU FORMBasic Information Child’s Name: ____________________________________________________________Birthdate:_________________
What time do you expect to drop off/pick up?_____________________________________________________________
Illness or Injury Contact If your child becomes ill, who would you prefer us to call?
When do you wish to be informed on a minor injury or illness (i.e. scratch, headache, etc) o Immediately by phoneo At pick upo Other:_____________________________________________________________________________________
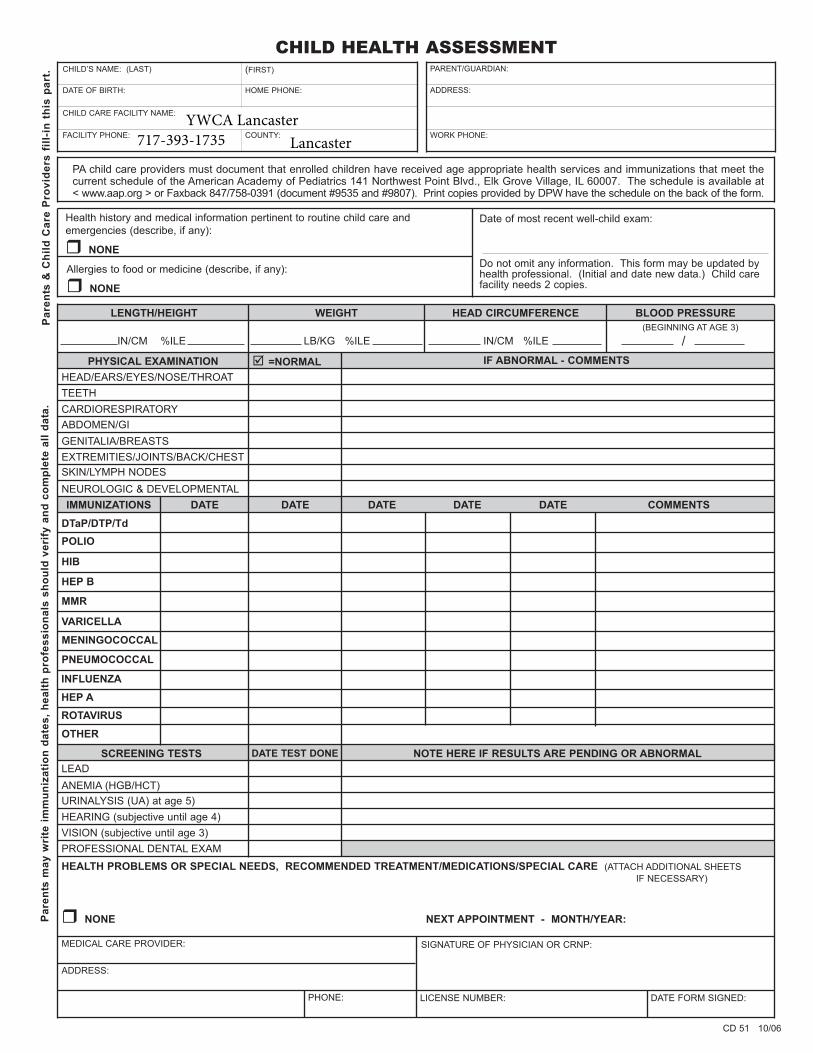
PA child care providers must document that enrolled children have received age appropriate health services and immunizations that meet the current schedule of the American Academy of Pediatrics 141 Northwest Point Blvd., Elk Grove Village, IL 60007. The schedule is available at < www.aap.org > or Faxback 847/758-0391 (document #9535 and #9807). Print copies provided by DPW have the schedule on the back of the form.
Health history and medical information pertinent to routine child care and
emergencies (describe, if any):
� NONE
Date of most recent well-child exam:
Allergies to food or medicine (describe, if any):
� NONE
Do not omit any information. This form may be updated byhealth professional. (Initial and date new data.) Child care facility needs 2 copies.
LENGTH/HEIGHT WEIGHT HEAD CIRCUMFERENCE BLOOD PRESSURE
IN/CM %ILE LB/KG %ILE IN/CM %ILE / (BEGINNING AT AGE 3)
PHYSICAL EXAMINATION =NORMAL� IF ABNORMAL - COMMENTS
HEAD/EARS/EYES/NOSE/THROAT
TEETH
CARDIORESPIRATORY
ABDOMEN/GI
GENITALIA/BREASTS
EXTREMITIES/JOINTS/BACK/CHEST
SKIN/LYMPH NODES
NEUROLOGIC & DEVELOPMENTAL
IMMUNIZATIONS DATE DATE DATE DATE DATE COMMENTS
DTaP/DTP/Td
POLIO
HIB
HEP B
MMR
VARICELLA
MENINGOCOCCAL
PNEUMOCOCCAL
INFLUENZA
HEP A
ROTAVIRUS
OTHER
SCREENING TESTS DATE TEST DONE NOTE HERE IF RESULTS ARE PENDING OR ABNORMAL
LEAD
ANEMIA (HGB/HCT)
URINALYSIS (UA) at age 5)
HEARING (subjective until age 4)
VISION (subjective until age 3)
PROFESSIONAL DENTAL EXAM
HEALTH PROBLEMS OR SPECIAL NEEDS, RECOMMENDED TREATMENT/MEDICATIONS/SPECIAL CARE (ATTACH ADDITIONAL SHEETS
IF NECESSARY)
� NONE NEXT APPOINTMENT - MONTH/YEAR:
MEDICAL CARE PROVIDER:
ADDRESS:
PHONE:
SIGNATURE OF PHYSICIAN OR CRNP:
LICENSE NUMBER: DATE FORM SIGNED:
CD 51 10/06
YWCA Lancaster717-393-1735 Lancaster
YWCA Lancaster
CHILD'S NAME BIRTHDATE
ADDRESS
MOTHER'S NAME/LEGAL GUARDIAN HOME TELEPHONE NUMBER
ADDRESS
BUSINESS NAME BUSINESS TELEPHONE NUMBER
ADDRESS
FATHER'S NAME/LEGAL GUARDIAN HOME TELEPHONE NUMBER
ADDRESS
BUSINESS NAME BUSINESS TELEPHONE NUMBER
ADDRESS
EMERGENCY CONTACT PERSON(S) NAME TELEPHONE NUMBER WHEN CHILD IS IN CARE
PERSON(S) TO WHOM CHILD MAY BE RELEASED NAME ADDRESS TELEPHONE NUMBER WHEN CHILD IS IN CARE
NAME OF CHILD'S PHYSICIAN/MEDICAL CARE PROVIDER TELEPHONE NUMBER
ADDRESS
SPECIAL DISABILITIES (IF ANY) ALLERGIES (INCLUDING MEDICATION REACTION)
MEDICAL or DIETARY INFORMATION NECESSARY IN AN EMERGENCY SITUATION MEDICATION, SPECIAL CONDITIONS
ADDITIONAL INFORMATION ON SPECIAL NEEDS OF CHILD
HEALTH INSURANCE COVERAGE FOR CHILD or MEDICAL ASSISTANCE BENEFITS POLICY NUMBER (REQUIRED)
OBTAINING EMERGENCY MEDICAL CARE ADMIN. OF MINOR FIRST - AID PROCEUDURES
WALKS AND TRIPS SWIMMING
TRANSPORTATION BY THE FACILITY WADING
PERIODIC REVIEW
PARENT'S SIGNATURE IS REQUIRED FOR EACH ITEM BELOW TO INDICATE PARENTAL CONSENT
We are excited to offer the safety, convenience and ease of Tuition Express® – a payment processing system that allows secure, on-time tuition and fee payments to be made from either your bank account or credit card.
ELECTRONIC FUNDS TRANSFER AUTHORIZATION FOR BANK ACCOUNT and CREDIT CARD
I (we) hereby authorize (business name) ____________________________________________ to initiate credit card charges to the below referenced credit card account (Section A) OR, initiate debit entries to my (our) Checking or Savings Account, indicated below (Section B). To properly affect the cancellation of this agreement, I (we) are required to give 10 days written notice. Credit Union Members: Please contact your Credit Union to verify account and routing numbers for automatic payments. Check with the center for accepted credit card types.
COMPLETE ONE SECTION ONLY
SECTION A (Credit Card)
_______________________________________________________________________________________________________Cardholder Name Phone #
_______________________________________________________________________________________________________Cardholder Address City State Zip _______________________________________________________________________________________________________Account Number Expiration Date
_________________________________________________________________________________________________________________________________ Cardholder Signature Date
SECTION B (Bank Account)
_______________________________________________________________________________________________________Your Name Phone #
_______________________________________________________________________________________________________Address City State Zip
_______________________________________________________________________________________________________Bank or Credit Union Name
_______________________________________________________________________________________________________Bank or Credit Union Address City State Zip
_______________________________________________________________________________________________________Routing Transit Number (see sample below) Account Number (see sample below)