54
Zygomaticomaxillary complex Fracture Deepak K Gupta
| Date post: | 16-Apr-2017 |
| Category: |
Health & Medicine |
| Upload: | deepak-kumar-gupta |
| View: | 3,671 times |
| Download: | 3 times |

Zygomaticomaxillarycomplex Fracture
Deepak K Gupta

• Zygoma or cheek bone
• Fracture of zygoma is not usually present alone, its find mostly in the conjunction with adjacent structure i.e.
– antrum,
– orbital walls including the infraorbital canal,
– rim
– orbital floor
This structure makes up the zyogmaticomaxillarycomplex
www.facebook.com/notesdental

Applied Anatomy
• Zygomatic bone separated from the craniofacial skeleton. Five articulations are identified:1. Frontal process
2. Zygomaticomaxillarybuttress
3. Infraorbital rim
4. Zygomatic arch
5. Lateral orbital wall
www.facebook.com/notesdental

Frontal process
Zygomaticomaxillary
buttress
Infraorbital rim
Zygomatic arch
Lateral orbital wall
www.facebook.com/notesdental
Rowe’s and Killey classification (1968)
• Type I : no significant displacement• Type II : fracture of zygomatic arch• Type III : rotation arround horizontal axis – inward or
outward displacement• Type IV: rotation around longitudinal axis – medial or
lateral• Type V : displacement of the complex block –
medial/inferior/lateral• Type VI: displacement of orbitoantral partition• Type VII: displacement of orbital rim segment• Type VIII: complex comminuted fracture.
www.facebook.com/notesdental

Axis of rotation
• Vertical axis : Line passing through frontozygomatic suture and first molar tooth
– Medial or lateral movement
• Horizontal Axis : infraorbital foramen and horizontal arch
– Upward or downward movement of broken segment
www.facebook.com/notesdental

Clinical features: Skeletal deformities• Asymmetry of the
midface• Depression/flattening
of the malarprominence
• Flattening, hollowing (bony indentation) or broadening over the zygomatic arch
• Palpable step offs or gap deformities of orbital margins (infraorbital/lateral)
www.facebook.com/notesdental

Clinical features : ocular/opthalmicsypmtoms
• Periorbital edema or hematoma (“monocle hematoma”)
• Pseudoptosis - inability to elevate the eyelid
• Increased scleral show• Downward slant of palpebral
fissure or horizontal lid axis respectively
• Malposition of the lateral canthus• Vertical shortening of the lower
eyelid (ectropion)• Subconjunctival ecchymosis
(temporal/medial)• Chemosis – edema of conjuctiva• pupillary or globe level disparity
(hypoglobus)• Proptosis bulbi www.facebook.com/notesdental

Clinical features : ocular/opthalmicsypmtoms
• Enophthalmos (outward displacement of zygoma)
• Exophthalmos (inward displacement of zygoma)
• Subcutaneous periorbitalair emphysema (skin crepitation)
• Pneumoexophthalmos• Amaurosis - vision loss or
weakness that occurs without an apparent lesion affecting the eye
• Superior orbital fissure syndrome
www.facebook.com/notesdental

Diplopia
• Neurogenicocular motility disorder – classic symptom of ZMC fracture
• Classified
– Monocular: double vision with 1 eye
– Binocular : double vision with both eyes open
– Permanent : paralysis or muscle entrapment
– Temporary : last for 5-7 days
www.facebook.com/notesdental

Diplopia: cause• Haeomotoma or
edema arroundextraoccularmuscle
• Neuromuscular injury
• Disruption of attatchment of inferior rectus or inferior oblique muscle
www.facebook.com/notesdental

Diplopia : test
• Finger Gaze: finger moved in front of eye in all nine direction of gaze at a distance 30 cm. Reporting of double vision – positive.
• Forced duction test: differentiate between permanent and temporary diplopia – carried out under topical LA. – Tendons of inferior rectus muscle is held with
tissue holding forceps and eyeball is rotated superiorly with other movement
– failure to rotate indicates paralysis or entrapment of muscle in fracture
www.facebook.com/notesdental

Forced Duction test
www.facebook.com/notesdental

Clinical feature : Sensory • Sensory deficit
(hypoesthesia, anesthesia) in the distribution of the following nerves:
1. Infraorbital nerve: lower eyelid, upper lip, ala and lateral sidewall of the nose
2. Zygomatiofacial nerve: malar eminence, cheek
3. Zygomaticotemporalnerve: lower lateral orbital rim anterior temporal/lateral/frontal region
1
2
3
www.facebook.com/notesdental

Clinical feature: Oral symptoms
• Ecchymosis of the gingivobuccal maxillary sulcus • Subjective occlusal disorder due to altered
sensation of the maxillary premolars/ molars and gingiva, no objective malocclusion
• Palpable contour disturbance of zygomaticomaxillary buttress
• Restriction of mandibular opening (trismus) or closing– blockage of temporal muscle or coronoid process
• impacted zygomatic arch • retrodisplaced zygoma
www.facebook.com/notesdental

Clinical feature : Nasal symptoms
• Ipsilateral epistaxis
• Ipsilateral hematosinus
www.facebook.com/notesdental

Investigation
• Conventional plain x-rays in combination with a detailed clinical examination in absence of CT scan
• high-resolution CT scans in axial, coronal, and sagittal reconstructions provide complete radiological visualization of the fracture sections with bone and soft-tissue windows
www.facebook.com/notesdental

The apex of the V-shaped fracture is indented toward the coronoid mandibular process
www.facebook.com/notesdental

Surgical Approach• Extra-oral approach
– Bicoronal or hemicoronal– Gillies : Temporal – Superolateral
• Supraorbital approach : lateral eyebrow• Upper eyelid
– Lower eyelid• Infraorbital• Subtarsal• Subcilliary/infracilliary : lower blepheroplasty
– Transconjuctival– Percutaneous
• Intra-oral approach• Transoral : maxillary vestibular• Endoscopic transantral
www.facebook.com/notesdental

Bicoronal or hemicoronal
• The coronal or bi-temporal approach is used to expose the anterior cranial vault, the forehead, and the upper and middle regions of the facial skeleton
www.facebook.com/notesdental

Bicoronal : AccessThe following areas can be exposed:
–Entire calvarial vault–Anterior and lateral skull base
–Frontal sinus/Ethmoid–Zygoma–Zygomatic arch–Orbit (lateral/cranial/medial–Nasal dorsum–Temporomandibularjoint (TMJ)
–Condyle and subcondylar region
www.facebook.com/notesdental
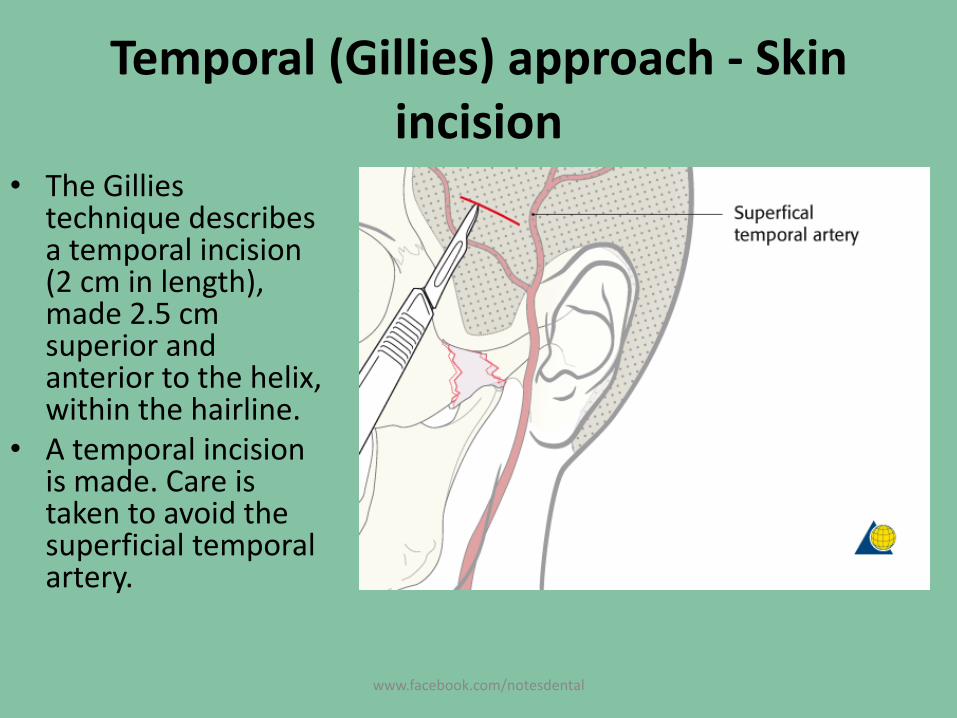
Temporal (Gillies) approach - Skin incision
• The Gilliestechnique describes a temporal incision (2 cm in length), made 2.5 cm superior and anterior to the helix, within the hairline.
• A temporal incision is made. Care is taken to avoid the superficial temporal artery.
www.facebook.com/notesdental
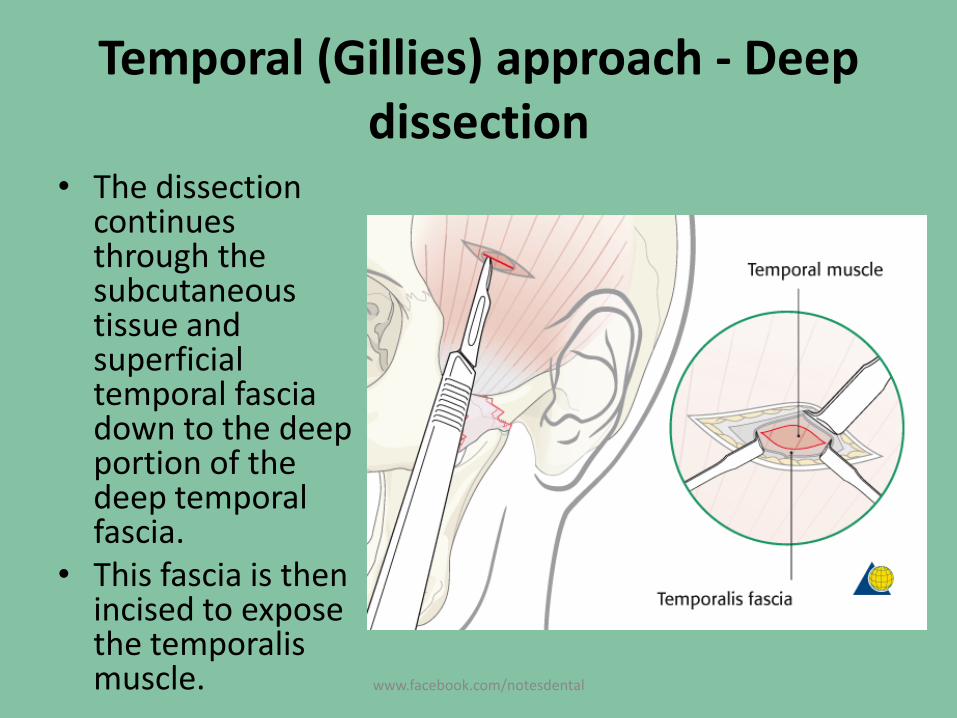
Temporal (Gillies) approach - Deep dissection
• The dissection continues through the subcutaneous tissue and superficial temporal fascia down to the deep portion of the deep temporal fascia.
• This fascia is then incised to expose the temporalismuscle. www.facebook.com/notesdental
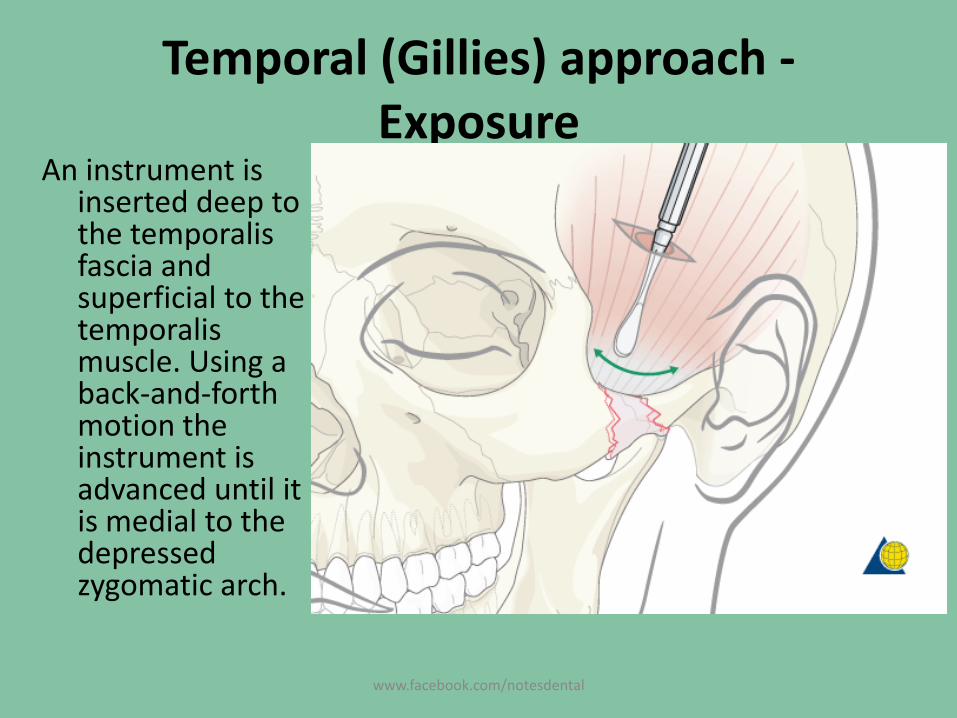
Temporal (Gillies) approach -Exposure
An instrument is inserted deep to the temporalisfascia and superficial to the temporalismuscle. Using a back-and-forth motion the instrument is advanced until it is medial to the depressed zygomatic arch.
www.facebook.com/notesdental

Temporal (Gillies) approach
• A Rowe zygomaticelevator is inserted just deep to the depressed zygomaticarch and an outward force is applied.
www.facebook.com/notesdental

Superolateral orbital rim Approaches
• There are two periorbitalapproaches:A. Lateral eyebrow
approach : supraorbitaleyebrow approach
B. Upper-eyelid approach : upper blepharoplastyor supratarsalfold approach
www.facebook.com/notesdental

lateral eyebrow approach
•gives rather limited access to zygomaticofrontalprocess and the immediate vicinity of suture line (superolateralorbital rim).• brow skin is thick and the wound edge
www.facebook.com/notesdental

The upper-eyelid or upper blepharoplasty approach
• greater versatility and enhanced accessibility to the superolateralrim compared to the lateral eyebrow approach.
• upper lid are thin, resilient
www.facebook.com/notesdental

Lower eyelid approaches
A. Subciliary : lower blepharoplasty
B. Subtarsal : lower or mideyelid
C. Infraorbital : inferior orbital rim
D. The subciliaryapproach can be extended laterally to gain access to the lateral orbital rim
www.facebook.com/notesdental

www.facebook.com/notesdental

Accessible area with a, b, c, approach
• lower circumference of the orbital cavity and/or for the subperiostealelevation of the upper midfaceand release of the cheek area
www.facebook.com/notesdental

Accessible area with (d) approach
• With a lateral extension of the subciliary incision however, the entire lateral rim- with heavy traction even beyond the level of the zygomaticofrontalsuture, as well the lateral orbital wall back to the zygomaticosphenoidsuture become accessible
www.facebook.com/notesdental

Transconjunctival
• Transconjunctival lower-eyelid approaches are performed in several ways.A. Transconjunctival (inferio
r fornix transconjunctivalusing a retroseptal or preseptal route)
B. Transcaruncular (=medial transconjunctival)
C. Transconjunctival with lateral skin extension(lateral canthotomy/swinging eyelid
D. Combination of (A) and (B)
E. C-shaped incision: Combination (a), (b), (c)
www.facebook.com/notesdental

Transconjunctival : Acess areathe floor of the orbit and infraorbital rim as well as the upper edge of the anterior maxilla(A).Via a pre- or transcaruncular incision, the medial wall of the orbit behind the posterior lacrimal crest can be exposed (B).The combination of the lower fornix and the medial transconjunctival approach provides access to both previously mentioned areas at a time.
www.facebook.com/notesdental
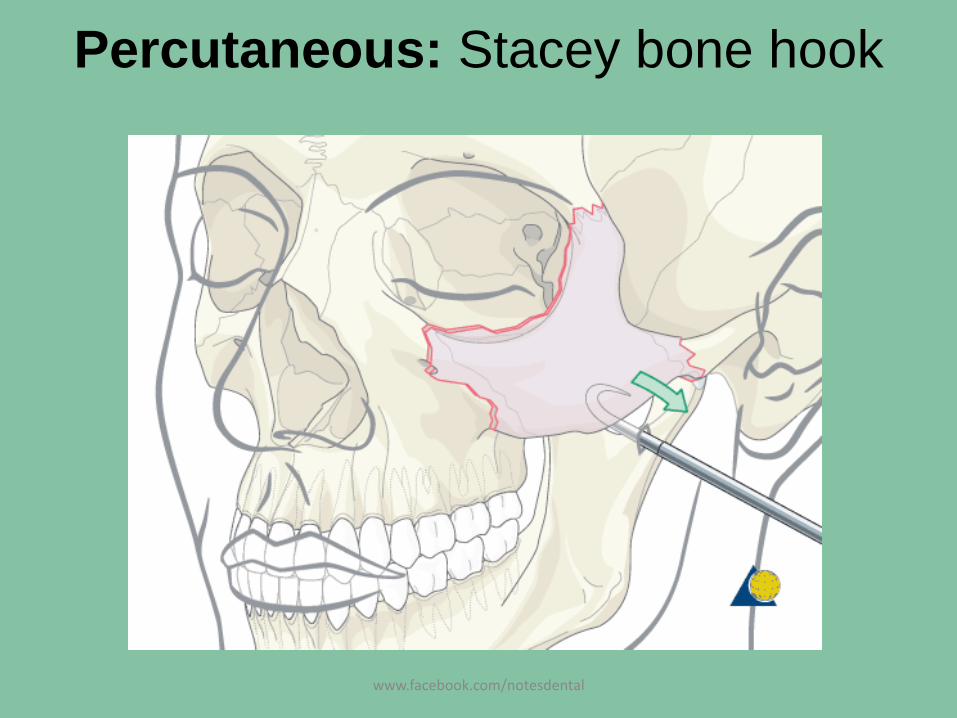
Percutaneous: Stacey bone hook
www.facebook.com/notesdental

Percutaneous: screw and traction method
www.facebook.com/notesdental

Percutaneous : Carroll-Girard screw
www.facebook.com/notesdental

Transoral (Keen) approach – lateral maxillary vestibular incision
• The transoral (Keen) approach provides the most direct access to the zygomatic arch.
• A 2 cm lateral maxillary vestibular incision (upper gingival buccalincision) is made with a scalpel or a cauterydevice just at the base of the zygomaticomaxillarybuttress. The incision is made through mucosa only.
www.facebook.com/notesdental

Transoral (Keen) approach - Exposure
• Because of the direct proximity of the incision to the arch,
– an instrument can easily be placed deep to the fractures to allow elevation of a depressed zygomatic arch.
– the depressed arch can often be palpated and elevated with a digital exam.
www.facebook.com/notesdental

Transoral (Keen) approach - Exposure
• An instrument is inserted deep to the temporalisfascia and superficial to the temporalis muscle. Using a back-and-forth motion the instrument is advanced until it is medial to the depressed zygomatic arch.
www.facebook.com/notesdental

Reduction
Indirect method
1. Gillies temporal fossa approach
2. Transverse maxillary buccal sulcus incision : Keen’s or Balasubramanyam approach
3. Percutaneus approach
Direct method
Done through various approaches as explained earlier
www.facebook.com/notesdental

Fixation
• It can be done in 4 methods depending on severity of fracture
– 1 point fixation
– 2 point fixation
– 3 point fixation
– 4 point fixation
www.facebook.com/notesdental

1 point fixation• Indication
– simple noncomminuted ZMC– patients where CT has
revealed no separation at the fracture of the zygomaticofrontal suture,
– and with good intraoperativevisualization, and reduction of the lateral maxillary buttress and the inferior orbital rim,
– 1-point fixation with a plate between the maxilla and zygoma may be adequate.
www.facebook.com/notesdental

2 point fixation
• When zygoma is not adequately reduced by visualizing only through a single approach
• a second point of exposure can help determine if the zygomatic complex has been properly reduced.
• bone plates placed across the frontozygomaticsuture and the zygomaticomaxillarybuttress provide stable internal fixation.
www.facebook.com/notesdental

3 Point Fixation
Indication
–Comminution of the zygomaticomaxillarybuttress and/or the frontozygomaticregion, making assessment of reduction difficult.
–reconstruction of the internal orbit
www.facebook.com/notesdental
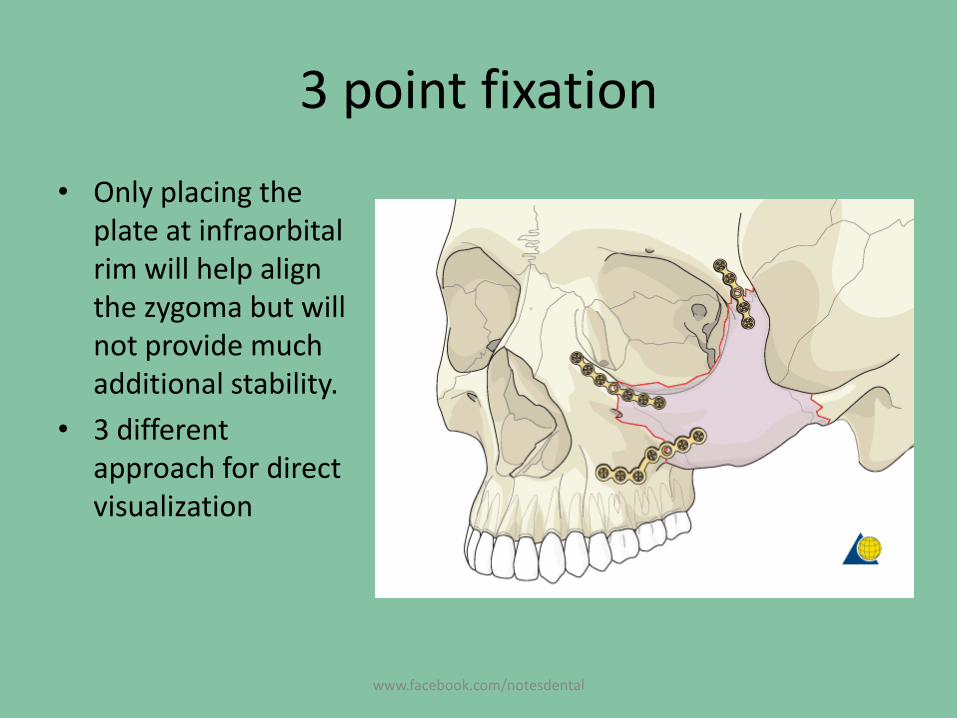
3 point fixation
• Only placing the plate at infraorbitalrim will help align the zygoma but will not provide much additional stability.
• 3 different approach for direct visualization
www.facebook.com/notesdental

4 point Fixation
• complex fracture of the zygoma and uncertainty as to adequate reduction of the fracture.– Zygomaticofrontal suture– Infraorbital rim– Zygomaticomaxillary buttress, – Zygomatic arch
• It require cornoal incision which has its own complication– scar alopecia– injury to the temporal branch of the facial nerve– temporal hollowing : depression within the soft tissues
overlying the temporal fossa
www.facebook.com/notesdental

4 point Fixation
But its absolutely indicated in patient with multiple fractures • frontal sinus
fractures• NOE fractures• Necessity to
harvest split calvarial bone graft
www.facebook.com/notesdental

Zygomatic arch fracture
• Isolated Zygomatic arch fracture may be effectively reduced by closed reduction by Gillies or Keen’s approach
• No need for rigid internal fixation : temporalisand masster muscle and fascia along soft with soft tissue splint the arch sufficiently to stabilize the fragments
www.facebook.com/notesdental

Aftercare
• Evaluation of vision– as soon as they are awakened from anesthesia– regular intervals until they are discharged from the
hospital
• Postoperative positioning : upright position - improve periorbital edema and pain
• Nose-blowing: avoided for 10 days - orbital emphysema
• Medication : Nasal decongestant, Antibiotics, Analgesia, Steroids, Ophthalmic ointment excluding NSAID’S and aspirin
• Ophthalmological examination• Postoperative imaging: 3-D imaging (CT, cone beam)
www.facebook.com/notesdental

Afercare• Wound care: suture removal within 5 days, ice packs, avoid sun
exposure• Diet
• Soft diet: after healing of the maxillary vestibular incision.• Intranasal feeding: oral bone exposure and soft-tissue defects.• liquid diet : Patients in MMF
• Clinical follow-up: complexity of the surgery• Eye movement exercises• Oral hygiene : use of soft tooth brush and oral rinse tds• MMF: duration of MMF is controversial and is dependent on
– Fracture morphology– Type and stability of fixation (including palatal splints)– Dentition– Coexistence of mandibular fractures– Premorbid occlusion
www.facebook.com/notesdental

Post operative complication
• Retrobulbar haemorrhage• Malar assymetry• Visual disturbance• Loss of vision• Persisten diplopia• Orbital dystopia• Enopthalmos• Sensory deifict• Persitant occular-cardiac reflex• Compromised occular function
www.facebook.com/notesdental

Refrences
• Principles of Internal Fixation of the CraniomaxillofacialSkeleton - Trauma and Orthognathic Surgery by AO foundation
• Textbook of oral and maxillofacial surgery 2nd edition: S M Balaji
• Text book of oral and maxillofacial surgery 3rd edition_neelima Mallik
• Contemporary oral and maxillofacial surgery _hupp_ellis_tucker
• clinical handbook of oral and maxillofacial surgery_lashkins
• Netter’s Atlas version 5.1
www.facebook.com/notesdental

THANKS……Feedback if any : [email protected]
Like, share and comment on https://www.facebook.com/notesdental
www.facebook.com/notesdental

















