Original J Bras Neurocirur 30 (4): 289-296, 2019 Salle F, Jaume A, Devita A, Spagnuolo E - Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patients Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patients Tumores Bulbomedulares Intra-Axiales. Resultados em una serie de 14 pacientes Federico Salle 1 Alejandra Jaume 2 Andrea Devita 2 Edgardo Spagnuolo 3 ABSTRACT Introduction: Intra-axial cervicomedullary tumors are relatively rare and their surgical management is still controversial. e aim of this study is to present the clinical results in a series of patients mostly composed of adults. Material and methods: We performed a retrospective study on 14 patients who underwent surgical resection of intra-axial medullary or cervicomedullary lesions between July 2016 and August 2018 in four different Uruguayan hospitals. e clinical features, pathological findings, extent of surgical resection, functional outcome and complications were analyzed. Results: Eleven male and 3 female patients were included. Mean age was 33.3 ± 6.8 y.o. A long history of motor weakness or sensory changes was the most common symptoms. A total of 28% of our patients presented with lower cranial nerve dysfunction. Surgical resection was complete in two cases, subtotal in 6 and partial in another 6 patients. Most patients (85%) showed postoperative worsening of their neurological function and six of them required tracheostomy and/or gastrostomy tubes. At long-term follow-up 13 patients have returned to their baseline functional status or improved. ere have been no tumor recurrences or progression. Conclusion: Surgical resection of cervicomedullary tumors can be achieved with good results. Even if morbidity in the immediate postoperative period seems elevated, most patients recover in the long term. Keywords: Cervicomedullary tumors; Outcomes; Surgical management; Complications; Intrinsic brainstem tumors RESUMEN Introducción: los tumores bulbo-medulares intra-axiales son relativamente raros y su manejo quirúrgico es controversial. El objetivo de este estudio es presentar los resultados clínicos en una serie de pacientes principalmente compuesta por adultos. Material y métodos: se realizó un estudio retrospectivo de 14 pacientes sometidos a resección quirúrgica de tumores intra-axiales del bulbo o de la región bulbo-medular entre julio 2016 y agosto 2018 en cuatro hospitales uruguayos. Se analizó la presentación clínica, hallazgos anatomo- patológicos, grado de resección, resultados funcionales y complicaciones. Resultados: se incluyeron 11 pacientes de sexo masculino y 3 de sexo femenino. La edad promedio fue 33.3 ± 6.8 años. Los síntomas más comunes fueron los trastornos sensitivos y déficit motor de lenta evolución. 28% de nuestros pacientes se presentaron con disfunción de pares craneanos bajos. La resección fue completa en 2 casos, subtotal en 6 y parcial en otros 6 pacientes. La mayoría de los pacientes (85%) presentaron peoría de su función neurológica en el postoperatorio y seis de ellos requirieron traqueostomía y/o gastrostomía. En el seguimiento a largo plazo, 13 pacientes han recuperado su estado funcional previo o han mejorado. No se han constatado recidivas o progresión lesional. Conclusión: la resección quirúrgica de tumores bulbo-medulares puede lograrse con buenos resultados. Incluso si la morbilidad inmediata postoperatoria parece elevada, la mayoría de los pacientes se recuperan en la evolución. Palavras-chave: Tumores bulbo-medulares; Resultados; Manejo quirúrgico; Complicaciones; Tumores intrínsecos de tronco 1 MD, MSc, Neurosurgery Department, Hospital Maciel - ASSE, Docent Unit, Universidad de la República, Montevideo, Uruguay. 2 MD, Neurosurgery Department, Hospital Maciel - ASSE, Docent Unit, Universidad de la República, Montevideo, Uruguay. 3 MD, Neurosurgeon, Chairman of Neurosurgery Department, Hospital Maciel - ASSE, Docent Unit, Universidad de la República, Montevideo, Uruguay Received: Accepted:
Transcript
Original
J Bras Neurocirur 30 (4): 289-296, 2019Salle F, Jaume A, Devita A, Spagnuolo E - Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patients
Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patientsTumores Bulbomedulares Intra-Axiales. Resultados em una serie de 14 pacientes
Federico Salle1
Alejandra Jaume2
Andrea Devita2
Edgardo Spagnuolo3
ABSTRACTIntroduction: Intra-axial cervicomedullary tumors are relatively rare and their surgical management is still controversial. The aim of this study is to present the clinical results in a series of patients mostly composed of adults. Material and methods: We performed a retrospective study on 14 patients who underwent surgical resection of intra-axial medullary or cervicomedullary lesions between July 2016 and August 2018 in four different Uruguayan hospitals. The clinical features, pathological findings, extent of surgical resection, functional outcome and complications were analyzed. Results: Eleven male and 3 female patients were included. Mean age was 33.3 ± 6.8 y.o. A long history of motor weakness or sensory changes was the most common symptoms. A total of 28% of our patients presented with lower cranial nerve dysfunction. Surgical resection was complete in two cases, subtotal in 6 and partial in another 6 patients. Most patients (85%) showed postoperative worsening of their neurological function and six of them required tracheostomy and/or gastrostomy tubes. At long-term follow-up 13 patients have returned to their baseline functional status or improved. There have been no tumor recurrences or progression. Conclusion: Surgical resection of cervicomedullary tumors can be achieved with good results. Even if morbidity in the immediate postoperative period seems elevated, most patients recover in the long term.
Keywords: Cervicomedullary tumors; Outcomes; Surgical management; Complications; Intrinsic brainstem tumors RESUMENIntroducción: los tumores bulbo-medulares intra-axiales son relativamente raros y su manejo quirúrgico es controversial. El objetivo de este estudio es presentar los resultados clínicos en una serie de pacientes principalmente compuesta por adultos. Material y métodos: se realizó un estudio retrospectivo de 14 pacientes sometidos a resección quirúrgica de tumores intra-axiales del bulbo o de la región bulbo-medular entre julio 2016 y agosto 2018 en cuatro hospitales uruguayos. Se analizó la presentación clínica, hallazgos anatomo-patológicos, grado de resección, resultados funcionales y complicaciones. Resultados: se incluyeron 11 pacientes de sexo masculino y 3 de sexo femenino. La edad promedio fue 33.3 ± 6.8 años. Los síntomas más comunes fueron los trastornos sensitivos y déficit motor de lenta evolución. 28% de nuestros pacientes se presentaron con disfunción de pares craneanos bajos. La resección fue completa en 2 casos, subtotal en 6 y parcial en otros 6 pacientes. La mayoría de los pacientes (85%) presentaron peoría de su función neurológica en el postoperatorio y seis de ellos requirieron traqueostomía y/o gastrostomía. En el seguimiento a largo plazo, 13 pacientes han recuperado su estado funcional previo o han mejorado. No se han constatado recidivas o progresión lesional. Conclusión: la resección quirúrgica de tumores bulbo-medulares puede lograrse con buenos resultados. Incluso si la morbilidad inmediata postoperatoria parece elevada, la mayoría de los pacientes se recuperan en la evolución. Palavras-chave: Tumores bulbo-medulares; Resultados; Manejo quirúrgico; Complicaciones; Tumores intrínsecos de tronco
1 MD, MSc, Neurosurgery Department, Hospital Maciel - ASSE, Docent Unit, Universidad de la República, Montevideo, Uruguay. 2 MD, Neurosurgery Department, Hospital Maciel - ASSE, Docent Unit, Universidad de la República, Montevideo, Uruguay. 3 MD, Neurosurgeon, Chairman of Neurosurgery Department, Hospital Maciel - ASSE, Docent Unit, Universidad de la República, Montevideo, Uruguay
Received: Accepted:
J Bras Neurocirur 30 (4): 289-296, 2019Salle F, Jaume A, Devita A, Spagnuolo E - Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patients
Original
Brainstem tumors have a low incidence. In the pediatric age they constitute approximately 10-15% of all primary CNS tumors, and tend to be benign, low grade lesions1. In adults, they account for 2% of all CNS tumors, and both low and high grade lesions can be equally found2.
These tumors can affect the midbrain, pons or medulla oblongata. Although medullary and cervicomedullary tumors are relatively rare, they present distinctive characteristics that require special consideration3.
Unlike diffuse pontine gliomas that are generally managed medically, cervico-medullary lesions are often focal and/or exophytic, and can be amenable to surgery with a good prognosis4. Their localization, and sometimes their infiltrative nature make surgery challenging and with elevated risk of morbidity5. This is why some authors in the past recommended avoiding aggressive surgical management.
Recent advances in neurophysiological monitoring and microsurgical techniques make it possible to operate on these lesions with good results6. Nevertheless, most publications refer to pediatric populations and the largest series report on patients that underwent surgery more than two decades ago.
The aim of this study is to present the clinico-pathological findings, surgical strategies, outcomes and complications in an updated series of 14 patients, mostly composed of adults.
The authors performed a retrospective study on 14 patients who underwent surgical resection of intra-axial medullary or cervicomedullary lesions between July 2016 and August 2018. All of the patients were operated on by the same
surgeon, the senior author of this paper (ES), in four different Uruguayan hospitals, with the same team of anesthesiologists and neurophysiologists. The study was approved by the ethics committee of our institution.
Eleven male and 3 female patients were included. Ages ranged from 21 to 44 years old (mean 33.3±6.8 y.o), and there was only one pediatric case of a 1-year-old boy.
The clinical features, pathological findings, extent of surgical resection, functional outcome and complications were analyzed.
The extent of resection was classified as gross total removal (GTR) if there was no evidence of remnant lesion on postoperative MRI, subtotal resection (STR) if at least 80% of the tumor was removed, and partial resection (PR) if less than 80% of the lesion was excised.
Functional status was assessed with the modified McCormick grading scale preoperatively and at long term follow-up. Follow-up ranged from 4 to 24 months (mean 14.8 mo). We considered that the outcome was good if the patient improved his/her neurological function or remained stable without any new deficits. Otherwise, the outcome was considered as poor.
Surgical ProceduresAll of the patients underwent a standard sub-occipital midline approach with high cervical laminectomy in a semi-sitting position, except for the pediatric case who underwent surgery in park-bench position through a far-lateral approach.
After opening the dura mater, stimulation of the dorsal aspect of the medulla or the spinal cord was performed in order to find a safe place for the initial myelotomy. Lesions were removed with careful microsurgical dissection, sometimes with ultrasonic aspirator. Intraoperative monitoring of somatosensory and motor evoked potentials was applied in all cases to prevent neurological deficits. Surgery was stopped if the potentials were lost or if their amplitude diminished significantly without recovery after 5 minutes.
INTRODUCTION
MATERIAL AND METHODS
Original
J Bras Neurocirur 30 (4): 289-296, 2019Salle F, Jaume A, Devita A, Spagnuolo E - Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patients
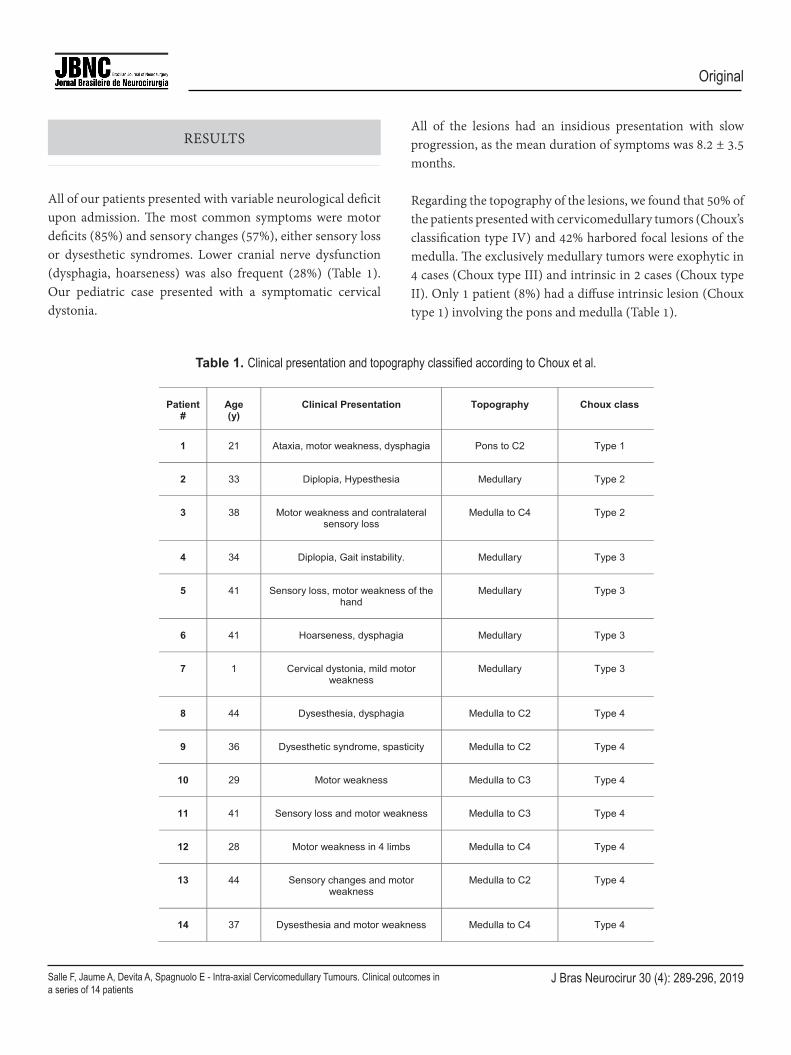
All of our patients presented with variable neurological deficit upon admission. The most common symptoms were motor deficits (85%) and sensory changes (57%), either sensory loss or dysesthetic syndromes. Lower cranial nerve dysfunction (dysphagia, hoarseness) was also frequent (28%) (Table 1). Our pediatric case presented with a symptomatic cervical dystonia.
All of the lesions had an insidious presentation with slow progression, as the mean duration of symptoms was 8.2 ± 3.5 months.
Regarding the topography of the lesions, we found that 50% of the patients presented with cervicomedullary tumors (Choux’s classification type IV) and 42% harbored focal lesions of the medulla. The exclusively medullary tumors were exophytic in 4 cases (Choux type III) and intrinsic in 2 cases (Choux type II). Only 1 patient (8%) had a diffuse intrinsic lesion (Choux type 1) involving the pons and medulla (Table 1).
RESULTS
Patient#
Age(y)
Clinical Presentation Topography Choux class
1 21 Ataxia, motor weakness, dysphagia Pons to C2 Type 1
2 33 Diplopia, Hypesthesia Medullary Type 2
3 38 Motor weakness and contralateralsensory loss
Medulla to C4 Type 2
4 34 Diplopia, Gait instability. Medullary Type 3
5 41 Sensory loss, motor weakness of thehand
Medullary Type 3
6 41 Hoarseness, dysphagia Medullary Type 3
7 1 Cervical dystonia, mild motorweakness
Medullary Type 3
8 44 Dysesthesia, dysphagia Medulla to C2 Type 4
9 36 Dysesthetic syndrome, spasticity Medulla to C2 Type 4
10 29 Motor weakness Medulla to C3 Type 4
11 41 Sensory loss and motor weakness Medulla to C3 Type 4
12 28 Motor weakness in 4 limbs Medulla to C4 Type 4
13 44 Sensory changes and motorweakness
Medulla to C2 Type 4
14 37 Dysesthesia and motor weakness Medulla to C4 Type 4
Assessment of functional status revealed that 4 patients (28.6%) had mild symptoms
preoperatively and still performed their professional activities with moderate discomfort (Mc
Cormick grade 1b). The rest of the patients had either moderate or severe neurological deficits
6
Table 1. Clinical presentation and topography classified according to Choux et al.
J Bras Neurocirur 30 (4): 289-296, 2019Salle F, Jaume A, Devita A, Spagnuolo E - Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patients
Original
Assessment of functional status revealed that 4 patients (28.6%) had mild symptoms preoperatively and still performed their professional activities with moderate discomfort (McCormick grade 1b). Th e rest of the patients had either moderate or severe neurological defi cits requiring assistance to walk. A total of 28.6% was classifi ed as McCormick grade II (still independent) and 42.8% were grade III.
Gross total removal was achieved in 2 cases (Figures 1 and 2). Subtotal resection was performed in 6 patients and partial resection in another 6 cases.
Except for one patient that had a cavernous angioma, histopathological examination of all the other lesions revealed astrocytomas (8 patients) or ependymomas (5 patients) of diff erent grades.
Th ere were 6 low grade tumors (WHO grade I or II) and 7 anaplastic tumors (WHO grade III).
Figure 1. A. Preoperative sagittal T2-weighted magnetic resonance image showing the upper-cervical tumor. B. Operative exposure and resection of the tumor. C. Postoperative sagittal T2-weighted MRI showing removal of the lesion.
Figure 2. A. Preoperative sagittal T1-weighted MRI image showing an ependymoma of the medulla oblongata. B. Operative exposure of the tumor. C. Postoperative sagittal T1-weighted MRI image showing removal of the lesion.
requiring assistance to walk. A total of 28.6% was classified as McCormick grade II (still
independent) and 42.8% were grade III.
Gross total removal was achieved in 2 cases (Figures 1 and 2). Subtotal resection was performed
in 6 patients and partial resection in another 6 cases.
Except for one patient that had a cavernous angioma, histopathological examination of all the
other lesions revealed astrocytomas (8 patients) or ependymomas (5 patients) of different grades.
There were 6 low grade tumors (WHO grade I or II) and 7 anaplastic tumors (WHO grade III).
Fig.1 A. Preoperative sagittal T2-weighted magnetic resonance image showing the upper-cervicaltumor. B. Operative exposure and resection of the tumor. C. Postoperative sagittal T2-weightedMRI showing removal of the lesion.
A B C
7
Original
J Bras Neurocirur 30 (4): 289-296, 2019Salle F, Jaume A, Devita A, Spagnuolo E - Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patients
In the immediate postoperative period, all of the patients spent at least 48 hours intubated in the intensive care unit. Removal of the orotracheal tube was performed only if considered safe after assessment by an otorhinolaryngologist.
During this period, 10 patients (71%) presented a new motor deficit or worsening of their previous deficit. We found a similar rate of new or worsened sensory deficit (64%). Half of the patients showed worsening of their previous lower cranial nerve dysfunction or new deficit. Six patients required tracheostomy and gastrostomy tubes in the immediate postoperative period.
In summary, 12 out of 14 operated patients showed an immediate worsening of their neurological status, meaning an 85% morbidity rate.
One patient died 4 months after surgery because of aspiration pneumonia, directly related to lower cranial nerve dysfunction. This patient presented severe motor deficit preoperatively, and she could not walk unaided. She worsened her deficit in the postoperative period and never recovered.
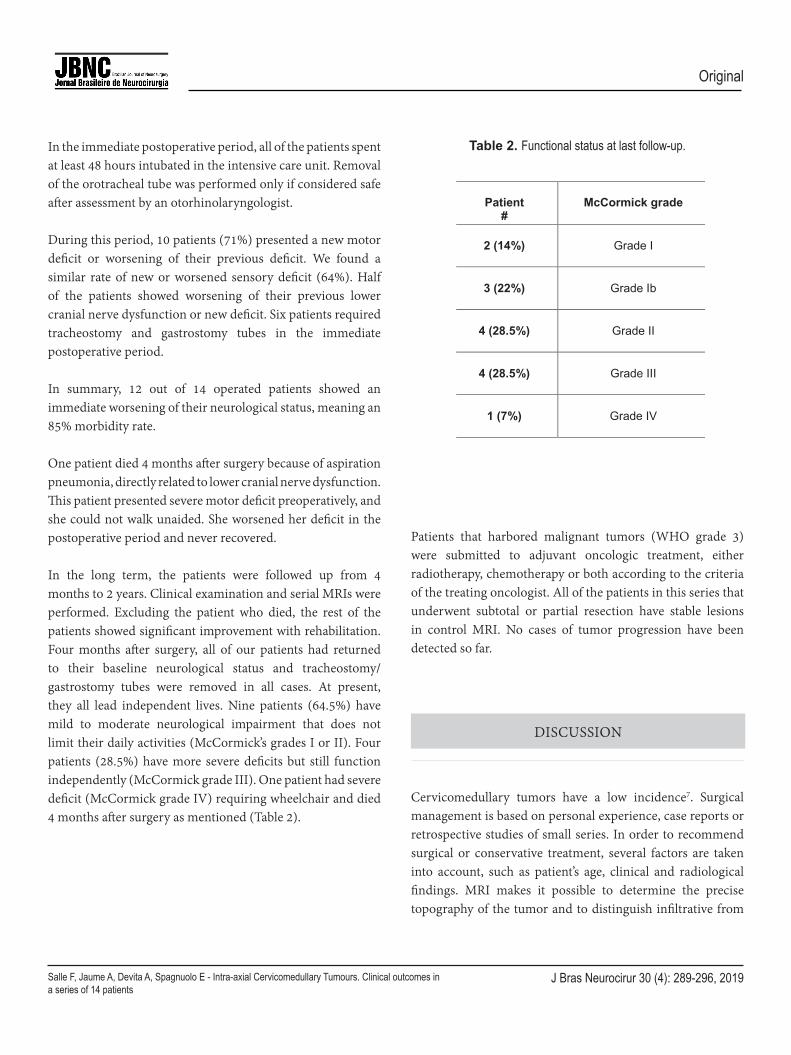
In the long term, the patients were followed up from 4 months to 2 years. Clinical examination and serial MRIs were performed. Excluding the patient who died, the rest of the patients showed significant improvement with rehabilitation. Four months after surgery, all of our patients had returned to their baseline neurological status and tracheostomy/gastrostomy tubes were removed in all cases. At present, they all lead independent lives. Nine patients (64.5%) have mild to moderate neurological impairment that does not limit their daily activities (McCormick’s grades I or II). Four patients (28.5%) have more severe deficits but still function independently (McCormick grade III). One patient had severe deficit (McCormick grade IV) requiring wheelchair and died 4 months after surgery as mentioned (Table 2).
Patients that harbored malignant tumors (WHO grade 3) were submitted to adjuvant oncologic treatment, either radiotherapy, chemotherapy or both according to the criteria of the treating oncologist. All of the patients in this series that underwent subtotal or partial resection have stable lesions in control MRI. No cases of tumor progression have been detected so far.
Cervicomedullary tumors have a low incidence7. Surgical management is based on personal experience, case reports or retrospective studies of small series. In order to recommend surgical or conservative treatment, several factors are taken into account, such as patient’s age, clinical and radiological findings. MRI makes it possible to determine the precise topography of the tumor and to distinguish infiltrative from
neurological impairment that does not limit their daily activities (McCormick’s grades I or II). Four
patients (28.5%) have more severe deficits but still function independently (McCormick grade III).
1 patient had severe deficit (McCormick grade IV) requiring wheelchair and died 4 months after
surgery as mentioned (Table 2).
Table 2. Functional status at last follow-up.
Patient#
McCormick grade
2 (14%) Grade I
3 (22%) Grade Ib
4 (28.5%) Grade II
4 (28.5%) Grade III
1 (7%) Grade IV
Patients that harbored malignant tumors (WHO grade 3) were submitted to adjuvant oncologic
treatment, either radiotherapy, chemotherapy or both according to the criteria of the treating
oncologist. All of the patients in this series that underwent subtotal or partial resection have stable
lesions in control MRI. No cases of tumor progression have been detected so far.
DISCUSSION
Cervicomedullary tumors have a low incidence7. Surgical management is based on personal
experience, case reports or retrospective studies of small series. In order to recommend surgical
or conservative treatment, several factors are taken into account, such as patient’s age, clinical
and radiological findings. MRI makes it possible to determine the precise topography of the tumor
and to distinguish infiltrative from expansive lesions8. This last characteristic is very important to
9
Table 2. Functional status at last follow-up.
DISCUSSION
J Bras Neurocirur 30 (4): 289-296, 2019Salle F, Jaume A, Devita A, Spagnuolo E - Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patients
Original
expansive lesions8. This last characteristic is very important to determine the surgical strategy and risk of recurrence, as lesions with ill-defined borders are associated with partial resections2,9.
In our series, we present 13 adult cases of cervicomedullary tumors that underwent surgery. Pediatric cases have different clinical presentations, management strategies and prognosis10. In adults, these tumors produce insidious and slowly progressive clinical symptoms that make prompt diagnosis difficult. This is reported in the literature1, 11 and is consistent with our findings.
More severe neurological impairment at the moment of diagnosis is related to a poor outcome12. Epstein et al. (1987) found, in their study of 20 cervicomedullary tumors, that patients who were severely disabled preoperatively were much more likely to sustain a neurological injury as a result of the surgical procedure8. In this series, 50% of the patients developed new postoperative sensitive or motor deficits with one case of quadriplegia.
Weiner et al. (1997) also found a strong correlation, between preoperative functional status and surgical outcome. In their series of 39 cervicomedullary tumors, only 16% of the patients classified as McCormick’s grade I were worse after surgery, at the time of last follow-up. This rate increased to 31% for grade II patients, and 55% for grade III. In our series, almost half of the patients (42.8%) presented with significant disability before surgery (McCormick’s grade III). This probably explains the elevated rate of immediate postoperative neurological worsening (85%). Early surgical intervention is therefore warranted prior to neurological deterioration.
Even though we had an elevated morbidity rate at discharge, most patients returned to baseline or reached an even better functional status in the long term. A total of 64.5% of our patients were classified as McCormick’s grades I or II at follow-up, and only 28.5% remained as grade III. Other authors also report that many immediate postoperative deficits are transient or tend to get better with time2,8.
In our series, we found that six patients (43%) required postoperative tracheostomy and gastrostomy tubes. Three of them had preoperative symptoms of lower cranial nerve dysfunction. In the study by Abbot et al. (1996), nine of their 24 cases required feeding gastrostomies and six patients needed prolonged ventilatory support. Factors associated with this postoperative complication were preoperative symptoms of upper respiratory tract infection, previous pneumonia, voice changes or dysphagia3. Jallo et al. (2005) report similar rates of postoperative tracheostomy and/or gastrostomy need. In their series of 41 cervicomedullary tumors, 19 patients (46%) presented this complication. Of note, they all had preoperative symptoms of lower cranial nerve dysfunction (choking, previous pneumonia or hoarseness)13. At last follow-up, 65% of the patients had undergone removal of their tracheostomies, in a mean time of 20.3 months. Gastrostomies could be removed in 68% of the cases in a mean time of 21.5 months. In our series, none of the patients retain tracheostomies or feeding tubes in place and they could all be removed within 4 months after surgery.
Tracheostomy and gastrostomy can be considered beneficial in order to diminish the risk of respiratory infections16. The need for mechanical ventilation is shorter with tracheostomy as well. Feeding tubes keep the patient in a good nutritional status. We did not perform any prophylactic tracheostomies or gastrostomies before surgery, because they are not always needed and, if they are, they can be quickly performed with minimally invasive procedures at the intensive care unit. We did not have any preoperative complications related to this decision, shared by other authors.
The extent of resection achieved when operating on these tumors is highly variable in the literature. Ge et al. (2017) report high rates (75%) of gross total removal in their series of 28 patients2, but they were all diagnosed with cervicomedullary ependymomas, which classically have a better plane of separation from neural tissue. Abbot reported only two cases of total removal and 16 subtotal resections (67%) in his series of 24 patients15. On the other hand, Weiner published a 30% rate of total removal1.
Original
J Bras Neurocirur 30 (4): 289-296, 2019Salle F, Jaume A, Devita A, Spagnuolo E - Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patients
In our series, we could achieve gross total removal of the tumor in only a minority of cases (14%), and subtotal resection in six patients (43%). This can probably be explained by the fact that more than 50% of our cases were diagnosed with astrocytomas, and there was a high proportion of malignant infiltrating tumors. We did not find any correlation between the extent of resection and postoperative neurological deficits, as in other publications2,15.
Regarding the surgical technique, it should be highlighted that the surgeon must have laboratory training and microsurgical experience. Trained neuro-anesthesiologists should be in charge and neurophysiological monitoring of motor and somatosensory evoked potentials is mandatory.
Anatomical knowledge of the region allows surgical exposure of the lesions without any difficulties. A suboccipital approach is generally adequate, although some lateral tumors might require a far lateral approach15.
Neurophysiological monitoring before starting surgical resection of the tumor provides information about the integrity or degree of compromise of neural pathways and cranial nerves. Once the medulla and upper cervical spinal cord are exposed, direct electrical stimulation will help localizing a safe entry zone18. Even for exophytic lesions, there is always a layer of neural tissue surrounding them, so electrical stimulation is still important. In our experience, this entry zone is usually no bigger than 2 to 3mm long. During resection, neurophysiological monitoring will act as a guidance to continue in depth or to stop. The surgeon cannot rely on anatomical landmarks only, as the anatomy is often distorted and the lesions might be of infiltrative nature. If a decrease in the amplitude of evoked potentials is detected, the resection should be halted for some minutes. If the amplitude returns to baseline, resection can be resumed, usually in a different region of the surgical bed. If potentials decrease again or if they are lost without recovery, surgery should be definitively aborted.
Use of ultrasonic aspirator can be helpful for debulking large lesions. However, when reaching the margins of the lesion, we recommend to replace this type of aspirator by more delicate conventional aspirators and dissectors.
We also recommend avoiding the use of bipolar coagulation during resection. Most cervicomedullary tumors are poorly vascularized, so irrigation with saline solution and applying hemostatic materials should be enough to stop the bleeding. Bipolar coagulation may damage healthy surrounding tissue and provoke permanent neurological deficits.
Upon completion of surgical resection all of our patients were transferred to intensive care under mechanical ventilation. We strongly recommend to keep the patients intubated during the first 24 to 48 hours, until an otorhinolaryngologist can confirm with endoscopy that the vocal cords and glottis closure are functioning normally. If not, the need for tracheostomy should be considered. Jallo and Epstein, also recommend 48 to 72 hours of artificial ventilation. They attempt extubation if the patient has adequate O2-CO2 levels, good respiratory drive and an intact gag reflex, obviating the need for endoscopy. Trained personnel in neurological intensive care is extremely important, as the outcome of these patients depends on a trained multidisciplinary team working together20.
Cervicomedullary tumors affect children and young adults that present with a long history of spinal deficits or lower cranial nerve dysfunction in most cases. Surgical treatment is challenging but possible with a careful microsurgical technique and guidance of neurophysiological monitoring. In our experience, even if there might be a high morbidity rate in the immediate postoperative period, most patients recover in the long term and are able to live an independent life.
1. Weiner HL, Freed D, Woo HH, Rezai AR, Kim R, Epstein FJ. Intra-axial tumors of the cervicomedullary junction: surgical results and long-term outcome. Pediatr Neurosurg. 1997;27(1):12-8. doi: 10.1159/000121219.
CONCLUSION
REFERENCES
J Bras Neurocirur 30 (4): 289-296, 2019Salle F, Jaume A, Devita A, Spagnuolo E - Intra-axial Cervicomedullary Tumours. Clinical outcomes in a series of 14 patients
Original
2. Ge X, Wu Z, Zhang J, Zhang L. Surgical Strategies and Functional Outcome of Intramedullary Cervicomedullary Ependymoma. Turk Neurosurg. 2017;27(4):563-572. doi: 10.5137/1019-5149.JTN.17104-16.2.
4. Wisoff JH, Epstein FJ. Management of pediatric brain tumors; in Morantz RA, Walsh JW (eds). Brain Tumors: A Comprehensive Text. New York: Dekker, 1993, pp 581–611.
5. Aghakhani N, David P, Parker F, Lacroix C, Benoudiba F, Tadie M. Intramedullary spinal ependymomas: analysis of a consecutive series of 82 adult cases with particular attention to patients with no preoperative neurological deficit. Neurosurgery. 2008;62(6):1279-85. doi: 10.1227/01.neu.0000333299.26566.15.
6. Ahyai A, Woerner U, Markakis E. Surgical treatment of intramedullary tumors (spinal cord and medulla oblongata). Analysis of 16 cases. Neurosurg Rev. 1990;13(1):45-52. doi: 10.1007/BF00638893.
7. Jallo G, Kothbauer K, Epstein F. Surgical Management of Cervicomedullary and Dorsally Exophytic Brain Stem Tumors. Operative Techniques in Neurosurgery. 2000;3(2):131-136. Doi: 10.1053/oy.2000.6565.
8. Epstein F, Wisoff J. Intra-axial tumors of the cervicomedullary junction. J Neurosurg. 1987;67(4):483-7. doi: 10.3171/jns.1987.67.4.0483.
9. Choux M, Lena G. Brainstem Tumors. In: Choux M, Di Rocco C, Hockley Ad, et al (eds). Pediatric Neurosurgery. New York: Churchill Livingstone, 1999, pp 471-491.
10. Hsu W, Pradilla G, Constantini S, Jallo GI. Surgical considerations of spinal ependymomas in the pediatric population. Childs Nerv Syst 25:1253-1259, 2009. Doi: 10.1007/s00381-009-0882-y.
11. Hoffman HJ, Becker L, Craven MA. A clinically and pathologically distinct group of benign brain stem gliomas. Neurosurgery. 1980 Sep;7(3):243-8. doi: 10.1227/00006123-198009000-00007.
12. Jenkinson MD, Simpson C, Nicholas RS, Miles J, Findlay GF, Pigott TJ. Outcome predictors and complications in the management of intradural spinal tumours. Eur Spine J. 2006;15(2):203-10. doi: 10.1007/s00586-005-0902-x.
13. Jallo GI, Shiminski-Maher T, Velazquez L, Abbott R, Wisoff J, Epstein F. Recovery of lower cranial nerve function after surgery for medullary brainstem tumors. Neurosurgery. 2005;56(1):74-17. doi: 10.1227/01.neu.0000144782.39430.12.
14. Schwartz TH, McCormick PC. Intramedullary ependymomas: clinical presentation, surgical treatment strategies and prognosis. J Neurooncol. 2000;47(3):211-8. doi: 10.1023/a:1006414405305. 15. Abbott R, Shiminski-Maher T, Epstein FJ. Intrinsic tumors of the medulla: predicting outcome after surgery. Pediatr Neurosurg. 1996;25(1):41-4. doi: 10.1159/000121095.
16. Wang G, Zhang J, Sun M, Wang C, Long DM. Surgical management of brainstem mass lesions: Respiratory insufficiency
occurrence and recovery. Neurosurgery Quarterly, 11(4), 302-313. Doi: 10.1097/00013414-200112000-00006.
17. Rodríguez D, Cheung MC, Housri N, Quinones-Hinojosa A, Camphausen K, Koniaris LG. Outcomes of malignant CNS ependymomas: an examination of 2408 cases through the Surveillance, Epidemiology, and End Results (SEER) database (1973-2005). J Surg Res. 2009 Oct;156(2):340-51. doi: 10.1016/j.jss.2009.04.024.
18. Albright AL, Sclabassi RJ. Use of the Cavitron ultrasonic surgical aspirator and evoked potentials for the treatment of thalamic and brain stem tumors in children. Neurosurgery. 1985;17(4):564-8. doi: 10.1227/00006123-198510000-00005.
20. Nagasawa DT, Smith ZA, Cremer N, Fong C, Lu DC, Yang I. Complications associated with the treatment for spinal ependymomas. Neurosurg Focus. 2011 Oct;31(4):E13. doi: 10.3171/2011.7.FOCUS11158.
Federico Salle, MD, MScNeurosurgery DepartmentHospital Maciel – ASSEDocent Unit, Universidad de la RepúblicaMontevideo, UruguayE-mail: [email protected]













![[Tumours of testis]](https://static.documents.pub/doc/80x56/635022e42630aed50008c845/tumours-of-testis.jpg)








