19
| Date post: | 09-Dec-2023 |
| Category: |
Documents |
| Upload: | independent |
| View: | 0 times |
| Download: | 0 times |


American Society for Surgery of the Hand 113
CHAPTER 11Arthroscopic Management of
Unstable TFCC LesionsAndrea Atzei, MD • Riccardo Luchetti, MD
Our understanding of functional anatomy and biomechanics has highlighted the importance of a well-functioning triangular fibrocartilage complex (TFCC) to preserve stability of the ulnar side of the wrist. As outlined by the Palmer classification,1 TFCC disorders may follow a traumatic injury (Class 1) or some degenerative changes developing with ageing (Class 2). After a fall or a violent twisting of the wrist, the TFCC is most often lacerated at its ulnar periphery: the so-called 1B tear.1 The ulnar part of the TFCC is a complex 3-dimensional structure. From an anatomical and functional standpoint, it can be divided into two components, distal and proximal.2,3 The distal component of the TFCC (distal TFCC) is constituted by the distal hammock structure, the meniscus homologue and the surrounding loose ligamentous tissue and the so-called ulnar collateral ligament, though still debated as being either an isolated structure4,5 or a thickening of the floor of the extensor carpi ulnaris (ECU) tendon sheath.6,7 The “proximal component of the TFCC (proximal TFCC) represents the true triangular ligament that stabilizes the distal radioulnar joint (DRUJ).”2,3 It is also described as “ligamentum subcruentum,”8 and is made up of the palmar and dorsal DRUJ ligaments that originate from the ulnar corners of the distal radius to interdigitate and converge onto the fovea and the basi-styloid area of the ulnar head. Biomechanical studies have suggested that the foveal insertions are the most important for stability of the DRUJ.9
Though frequently overlooked, it should be kept in mind that the foveal area also represents the “convergent point” of insertion for the palmar ulnocarpal (UC) ligaments10: ulnolunate and ulnotriquetral ligaments. Recent biomechanical studies have confirmed that UC ligaments are responsible for the stability of the ulnar carpus11: hence the proximal TFCC, taken as a whole, plays a key role in the stability of both the DRUJ and the UC joints.
These anatomical findings yield important clinical and therapeutic implications. Since the traumatic force producing a type 1-B TFC tear may have different directions and
magnitude, the components of the ulnar part of the TFCC may rupture in a variable manner, so that clinical presentation and treatment will differ accordingly.
When only the distal TFCC is ruptured, the ulnar wrist is painful, but joint stability is still preserved. However, when the tear involves the proximal TFCC, the ulnar head becomes unstable and clinical complaints include ulnar-sided pain, reduced grip strength, decreased forearm rotation, and signs of DRUJ and, potentially, ulnocarpal joint (UCJ) instability.
Understanding the anatomical complexity of the TFCC has contributed to a dramatic change from the earlier concept that considered this structure as a simple “hammock” for the ulnar carpus into the novel “iceberg concept” (Fig. 11-1).12 This new model compares the TFCC, as seen during standard radiocarpal (RC) arthroscopy, to an iceberg showing with a small “emerging” tip and a very large “submerged” component that is not visible from a radiocarpal portal. In this new model, the size of these two parts is related to their functional importance. The readily visible part corresponds to the distal TFC functioning as the shock absorber. The submerged part corresponds to the proximal TFCC, made of the foveal insertions of the TFC and UC ligaments, and functioning as the stabilizer of the DRUJ and UCJ. The larger size of the submerged portion of the iceberg correlates to its greater importance in the biomechanics of the ulnar wrist. But the “iceberg concept” also leads to the clue that, in order to assess the proximal TFC, standard RC arthroscopy is not sufficient. Even with an intact TFCC seen upon RC arthroscopy, the ulnar head may still be unstable due to rupture of the foveal ligament insertions. Therefore only the use of DRUJ arthroscopy or special RC arthroscopic tests will reveal the rupture and allow the correct diagnosis. Adopting the “iceberg concept” also necessitates a more in-depth classification of Type 1-B TFC tears, taking joint instability into greater account.
Likewise, recent literature confirms that DRUJ instability is frequently misdiagnosed preoperatively and intraoperatively
Wrist_Ch11.indd 113Wrist_Ch11.indd 113 27/03/13 7:46 PM27/03/13 7:46 PM

Ulnar-Sided Wrist Pain
114 American Society for Surgery of the Hand
when treating TFCC tears and that this is the most common cause of unsatisfactory results and reoperations.
Estrella and colleagues,13 reviewing the clinical and functional outcomes of 35 patients treated by arthroscopic repair of TFCC tears, found that 26% of their patients had an unsatisfactory result, 45% of which related to persistent DRUJ instability. A similar finding regarding persistent DRUJ instability was reported by Anderson and colleagues.14 They compared the clinical results of arthroscopic (36 patients) and open (39 patients) repair of traumatic TFCC tears and did not find any statistically significant difference between the two groups that showed the same rate of reoperation of 26.6%. Out of these, 65% of reoperations (i.e., about 17% of the whole series) were required to address DRUJ instability. The investigators related this finding either to a failure to diagnose true DRUJ instability or to an inadequate TFC repair.14 Implications of these studies are that DRUJ instability is a major issue and should be investigated carefully, unstable TFC tears should be treated differently from stable ones, and there are TFCC tears that cannot heal with simple repair.
In order to obtain reliable guidelines to surgical treatment and improve comparison of the different surgical techniques, there is a need for an improved definition of the spectrum of Type 1-B TFCC tear. The novel classification15 endorsed by the European Wrist Arthroscopy Society (EWAS) may fulfill
these needs (Table 11-1). Based on clinical and arthroscopic findings, this treatment-oriented classification system subdivides the ulnar-sided injuries of the TFCC (1B) into 5 different classes, proposing specific treatment guidelines for each class, and emphasizes the following main concepts:
1. The involvement of the proximal TFC is associated with symptomatic DRUJ instability and should be treated by TFC repair to the fovea ulnaris. Proximal TFC involvement may be present in two clinical forms: Class 2, consisting of a complete laceration of the ulnar TFC involving also the distal TFC, or Class 3, consequence of either an acute isolated avulsion of the proximal TFC from the fovea or a chronic tear in which only the distal TFC has healed spontaneously.
2. TFC tears that cannot be debrided back to healthy tissue (Class 4) are unlikely to heal by direct repair and should be treated by tendon graft reconstruction. Candidates for TFC reconstruction usually have chronic tears, which occur after massive tears or repetitive injury causing ligament fraying or elongation and even local calcium deposition, or following failed repair. Reduction of TFCC vascularity, as it may happen in congenital dysplasia of the styloid and foveal area, may be another factor associated with poor healing potential.
ShockAbsorber
THE ICEBERG CONCEPT
DRUJStabilizer Carpal
Stabilizer
dc-TFCCpc
-TFCC
Figure 11-1 The “iceberg concept” uses an immediate visual representation to summarize the functional importance of the distal component (dc-TFCC) and proximal component (pc-TFCC) of the TFCC as well as the difficulty of achieving a thorough assessment from only a standard radiocarpal arthroscopy. During radiocarpal arthroscopy, the TFCC shows its “emerging” tip (i.e. distal TFCC) that functions as a shock absorber. In analogy with the iceberg’s tip, it represents only the smaller part of the TFCC, compared with the “submerged” part (i.e. proximal TFCC). The larger size of the submerged part corresponds to the greater functional importance of the proximal TFCC as the stabilizer of the DRUJ and of the ulnar carpus. The “submerged” part (i.e. the foveal insertions of the TFCC) cannot be visualized during radiocarpal arthroscopy, but only through DRUJ arthroscopy.
Wrist_Ch11.indd 114Wrist_Ch11.indd 114 27/03/13 7:46 PM27/03/13 7:46 PM

Tab
le 1
1-1
Cla
ssifi
catio
n of
TFC
C P
erip
hera
l Tea
rs M
odifi
ed fr
om A
tzei
15
Cla
ss 1
Rep
aira
ble
Dis
tal T
ear
Cla
ss 2
Rep
aira
ble
Co
mp
lete
Tea
r
Cla
ss 3
Rep
aira
ble
Pro
xim
al T
ear
Cla
ss 4
No
nrep
aira
ble
Tear
Cla
ss 5
Art
hrit
ic D
RU
J
Clin
ical
D
RU
J In
stab
ility
Non
e /
Slig
htM
ild /
Sev
ere
Sev
ere
Mild
/ S
ever
e
Ap
pea
ranc
e of
TF
CC
D
ista
l Com
pon
ent
(RC
Art
hros
cop
y)
Torn
Torn
Inta
ctTo
rn
Varia
ble
Sta
tus
of T
FCC
Pro
xim
al
Com
pon
ent
(Hoo
k te
st /
DR
UJ
arth
rosc
opy)
Inta
ctTo
rnTo
rnTo
rn
Hea
ling
Pot
entia
l of
the
TF
CC
tea
r’s
mar
gins
Goo
dG
ood
Goo
dP
oor
Sta
tus
ofD
RU
J C
artil
age
(DR
UJ
arth
rosc
opy)
Goo
dG
ood
Goo
dG
ood
Poo
r
Trea
tmen
tR
EP
AIR
Sut
ure
(Lig
amen
t-to
-cap
sule
)
RE
PA
IRFo
veal
Ref
ixat
ion
RE
CO
NS
TRU
CTI
ON
Tend
on G
raft
SA
LVA
GE
Art
hrop
last
y or
Join
t R
epla
cem
ent
The
clas
sific
atio
n sy
stem
con
sid
ers
clin
ical
and
art
hros
cop
ic f
ind
ings
. C
linic
al a
sses
smen
t of
DR
UJ
inst
abili
ty i
s p
erfo
rmed
by
the
bal
lott
emen
t te
st.
Rad
ioca
rpal
art
hros
cop
y re
veal
s th
e p
rese
nce
of a
tea
r in
the
dis
tal T
FCC
and
the
qua
lity
of t
he t
ear’s
mar
gins
. Th
e ho
ok t
est
is u
sed
to
asse
ss in
tegr
ity o
f th
e p
roxi
mal
TFC
C.
DR
UJ-
arth
rosc
opy
is r
equi
red
to
excl
ude
chon
dro
mal
acia
, tha
t, w
hen
pre
sent
(Cla
ss 5
), m
ay b
e as
soci
ated
with
var
iab
le T
FCC
find
ings
. Tre
atm
ent
is s
ugge
sted
acc
ord
ing
to t
he d
iffer
ent
Cla
sses
. See
tex
t.
Wrist_Ch11.indd 115Wrist_Ch11.indd 115 27/03/13 7:46 PM27/03/13 7:46 PM
Ulnar-Sided Wrist Pain
116 American Society for Surgery of the Hand
3. DRUJ cartilage loss or degeneration (Class 5), which may occur after an acute injury or chronic instability, is responsible for unsatisfactory results of ligament repair or reconstruction. Arthroplasty or other salvage options should be considered.
Indications and ContraindicationsIndications for arthroscopic treatment of unstable lesions of the peripheral TFC are based mainly on an accurate clinical and arthroscopic assessment since imaging techniques are usually of limited value.
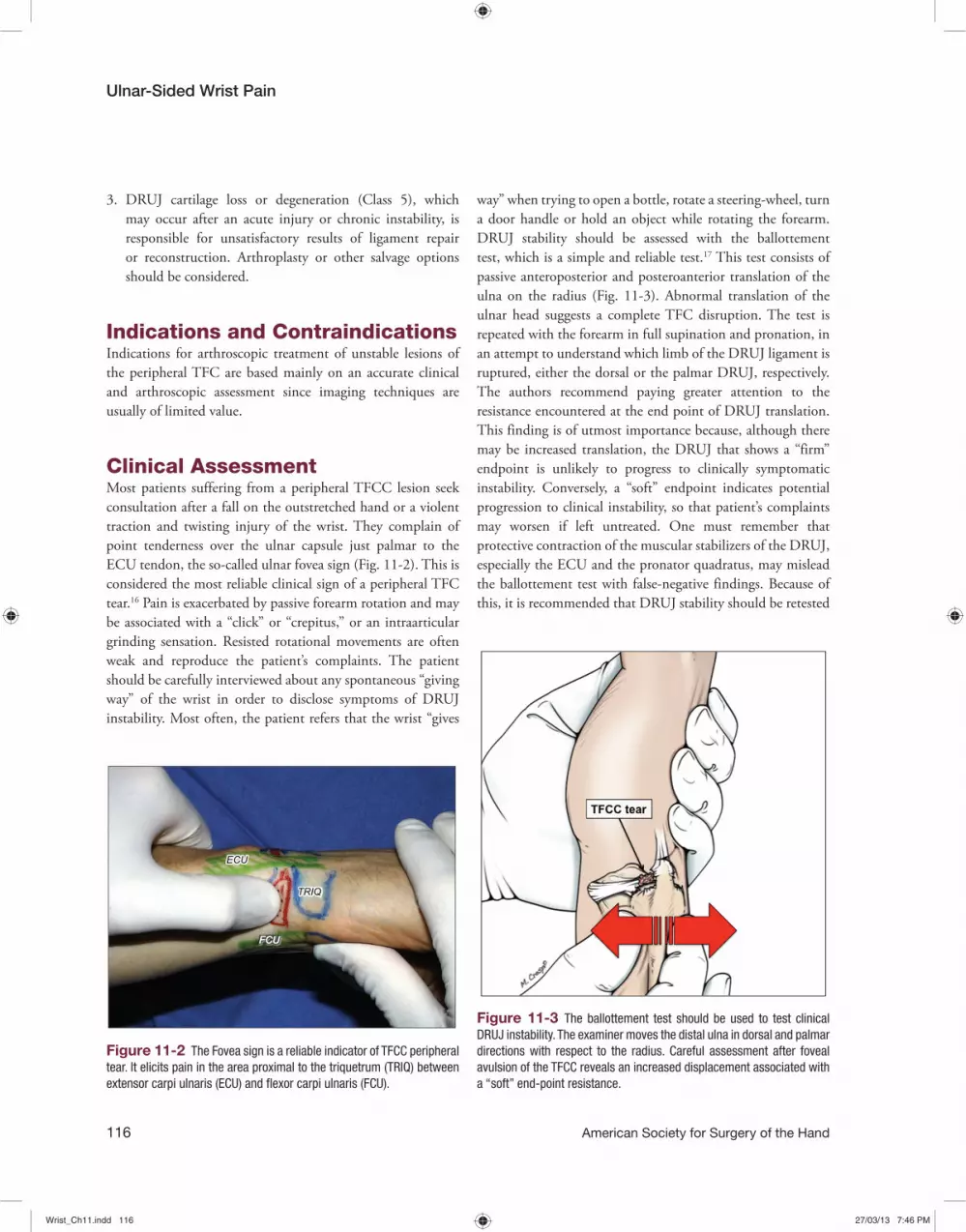
Clinical AssessmentMost patients suffering from a peripheral TFCC lesion seek consultation after a fall on the outstretched hand or a violent traction and twisting injury of the wrist. They complain of point tenderness over the ulnar capsule just palmar to the ECU tendon, the so-called ulnar fovea sign (Fig. 11-2). This is considered the most reliable clinical sign of a peripheral TFC tear.16 Pain is exacerbated by passive forearm rotation and may be associated with a “click” or “crepitus,” or an intraarticular grinding sensation. Resisted rotational movements are often weak and reproduce the patient’s complaints. The patient should be carefully interviewed about any spontaneous “giving way” of the wrist in order to disclose symptoms of DRUJ instability. Most often, the patient refers that the wrist “gives
way” when trying to open a bottle, rotate a steering-wheel, turn a door handle or hold an object while rotating the forearm. DRUJ stability should be assessed with the ballottement test, which is a simple and reliable test.17 This test consists of passive anteroposterior and posteroanterior translation of the ulna on the radius (Fig. 11-3). Abnormal translation of the ulnar head suggests a complete TFC disruption. The test is repeated with the forearm in full supination and pronation, in an attempt to understand which limb of the DRUJ ligament is ruptured, either the dorsal or the palmar DRUJ, respectively. The authors recommend paying greater attention to the resistance encountered at the end point of DRUJ translation. This finding is of utmost importance because, although there may be increased translation, the DRUJ that shows a “firm” endpoint is unlikely to progress to clinically symptomatic instability. Conversely, a “soft” endpoint indicates potential progression to clinical instability, so that patient’s complaints may worsen if left untreated. One must remember that protective contraction of the muscular stabilizers of the DRUJ, especially the ECU and the pronator quadratus, may mislead the ballottement test with false-negative findings. Because of this, it is recommended that DRUJ stability should be retested
Figure 11-2 The Fovea sign is a reliable indicator of TFCC peripheral tear. It elicits pain in the area proximal to the triquetrum (TRIQ) between extensor carpi ulnaris (ECU) and flexor carpi ulnaris (FCU).
Figure 11-3 The ballottement test should be used to test clinical DRUJ instability. The examiner moves the distal ulna in dorsal and palmar directions with respect to the radius. Careful assessment after foveal avulsion of the TFCC reveals an increased displacement associated with a “soft” end-point resistance.
Wrist_Ch11.indd 116Wrist_Ch11.indd 116 27/03/13 7:46 PM27/03/13 7:46 PM

Chapter 11 • Arthroscopic Management of Unstable TFCC Lesions
American Society for Surgery of the Hand 117
when the patient is under regional anesthesia before surgery. In the special case in which the suspicion of a TFC tear is associated with a distal radius fracture, it is strongly recommended that the ballottement test be assessed intraoperatively, after reduction and stable fixation of the fracture.
Imaging AssessmentAll patients presenting with acute or chronic wrist pain should have radiographs taken of the wrist. Usually these are of limited value for diagnosing isolated TFC tears because they can only show indirect signs of DRUJ instability, such as the evidence of distal ulna displacement, DRUJ widening, and/or ulnar styloid fracture. The presence of an ulnar styloid fracture, regardless of the fragment size and displacement, is no longer considered an absolute indicator of TFC rupture, but only a risk factor.18,19 This has been confirmed by several arthroscopic studies20,21 that did not find any predictable correlation between ulnar styloid fractures and a TFC tear. When seen on the radiographs taken for a distal radius fracture, indirect signs of associated TFC tear suggest that a thorough clinical and arthroscopic evaluation should be performed at the time of fracture realignment and fixation, to allow TFC repair at the same time. Likewise when a TFC tear is associated with a distal radius malunion, it is advisable to correct the malunion and then perform the clinical and arthroscopic evaluation to confirm the need of any TFCC repair or reconstruction. TFCC tears are frequently associated with the Galeazzi fracture-subluxation. DRUJ instability is also a common finding when the fracture is located within 7.5 cm
of the distal epiphysis of the radius and should be treated with TFC reattachment to the ulna.22
Usefulness of magnetic resonance imaging (MRI) in the diagnosis of a peripheral TFC tear is still a controversial issue. Whereas an MRI arthrogram may be both sensitive and specific in diagnosing a tear, it has not shown similar accuracy in assessing the tear size and location.23 Studies comparing specificity and sensitivity of arthrography, MRI, and arthroscopy confirm arthroscopic visualization of a TFC tear to be the gold standard for definitive diagnosis.24,25 However, MRI is useful to exclude associated pathologies of the ulnar compartment.
Arthroscopic AssessmentDiagnostic wrist arthroscopy is performed under brachial plexus block and exsanguination with an upper limb tourniquet inflated to 250 mmHg. Vertical traction is arranged using finger traps on the index and ring finger with approximately 3–4 Kg of counterweight traction. A standard dry arthroscopy is conducted.26,27 Standard portals (Fig. 11-4) are established and a 2.7 or 1.9 mm arthroscope is used according to wrist size. Standard arthroscopic assessment starts with RC arthroscopy. The scope is introduced in the 3–4 portal that allows adequate visualization of the distal TFC. Typical type 1B tear is visualized in the dorsoulnar corner of the TFC and may be probed through the 6R portal. As a rule, TFC tension is assessed by the trampoline test,28 which evaluates the TFC resilience (“trampoline effect”) by applying a compressive load
Figure 11-4 Standard portals for radiocarpal (3-4; 6R; 6U), midcarpal (MCR; MCU), and DRUJ (D-DRUJ; DF) arthroscopy.
Wrist_Ch11.indd 117Wrist_Ch11.indd 117 27/03/13 7:46 PM27/03/13 7:46 PM
Ulnar-Sided Wrist Pain
118 American Society for Surgery of the Hand
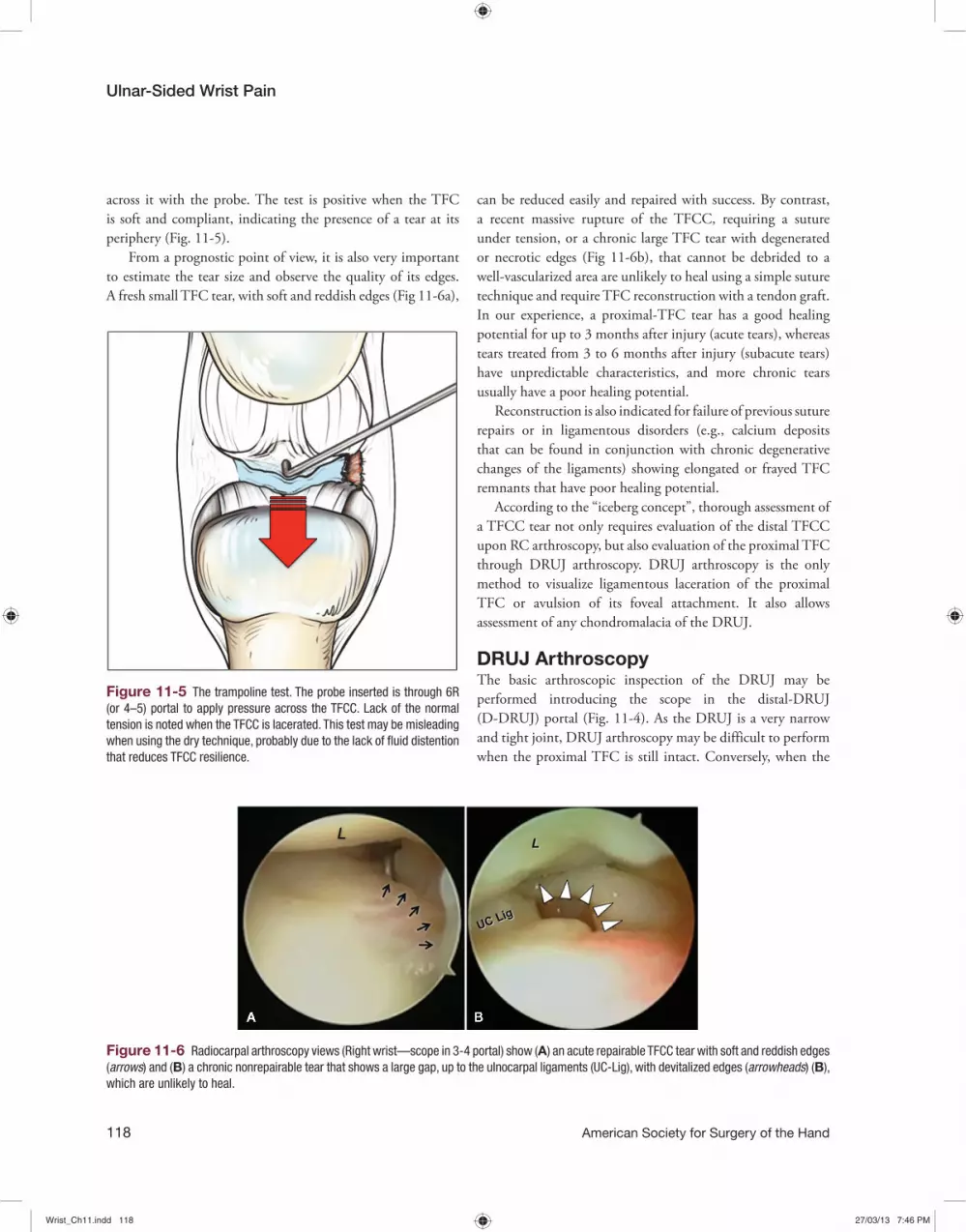
can be reduced easily and repaired with success. By contrast, a recent massive rupture of the TFCC, requiring a suture under tension, or a chronic large TFC tear with degenerated or necrotic edges (Fig 11-6b), that cannot be debrided to a well-vascularized area are unlikely to heal using a simple suture technique and require TFC reconstruction with a tendon graft. In our experience, a proximal-TFC tear has a good healing potential for up to 3 months after injury (acute tears), whereas tears treated from 3 to 6 months after injury (subacute tears) have unpredictable characteristics, and more chronic tears usually have a poor healing potential.
Reconstruction is also indicated for failure of previous suture repairs or in ligamentous disorders (e.g., calcium deposits that can be found in conjunction with chronic degenerative changes of the ligaments) showing elongated or frayed TFC remnants that have poor healing potential.
According to the “iceberg concept”, thorough assessment of a TFCC tear not only requires evaluation of the distal TFCC upon RC arthroscopy, but also evaluation of the proximal TFC through DRUJ arthroscopy. DRUJ arthroscopy is the only method to visualize ligamentous laceration of the proximal TFC or avulsion of its foveal attachment. It also allows assessment of any chondromalacia of the DRUJ.
DRUJ ArthroscopyThe basic arthroscopic inspection of the DRUJ may be performed introducing the scope in the distal-DRUJ (D-DRUJ) portal (Fig. 11-4). As the DRUJ is a very narrow and tight joint, DRUJ arthroscopy may be difficult to perform when the proximal TFC is still intact. Conversely, when the
Figure 11-5 The trampoline test. The probe inserted is through 6R (or 4–5) portal to apply pressure across the TFCC. Lack of the normal tension is noted when the TFCC is lacerated. This test may be misleading when using the dry technique, probably due to the lack of fluid distention that reduces TFCC resilience.
Figure 11-6 Radiocarpal arthroscopy views (Right wrist—scope in 3-4 portal) show (A) an acute repairable TFCC tear with soft and reddish edges (arrows) and (B) a chronic nonrepairable tear that shows a large gap, up to the ulnocarpal ligaments (UC-Lig), with devitalized edges (arrowheads) (B), which are unlikely to heal.
across it with the probe. The test is positive when the TFC is soft and compliant, indicating the presence of a tear at its periphery (Fig. 11-5).
From a prognostic point of view, it is also very important to estimate the tear size and observe the quality of its edges. A fresh small TFC tear, with soft and reddish edges (Fig 11-6a),
Wrist_Ch11.indd 118Wrist_Ch11.indd 118 27/03/13 7:46 PM27/03/13 7:46 PM

Chapter 11 • Arthroscopic Management of Unstable TFCC Lesions
American Society for Surgery of the Hand 119
proximal TFC is torn, the articular disc is loose so that usually there is adequate space available for scope insertion. Holding the forearm supinated and reducing traction may facilitate scope introduction. An 18-gauge hypodermic needle can be inserted percutaneously at about 1 cm proximal to the 6U portal in order to enter the joint close to the fovea. It can be used to lift the articular disc and give provisional assessment of the tautness of the proximal TFC. The needle can be withdrawn to prepare the Direct Foveal (DF) portal that allows introduction of a probe or motorized instrumentation
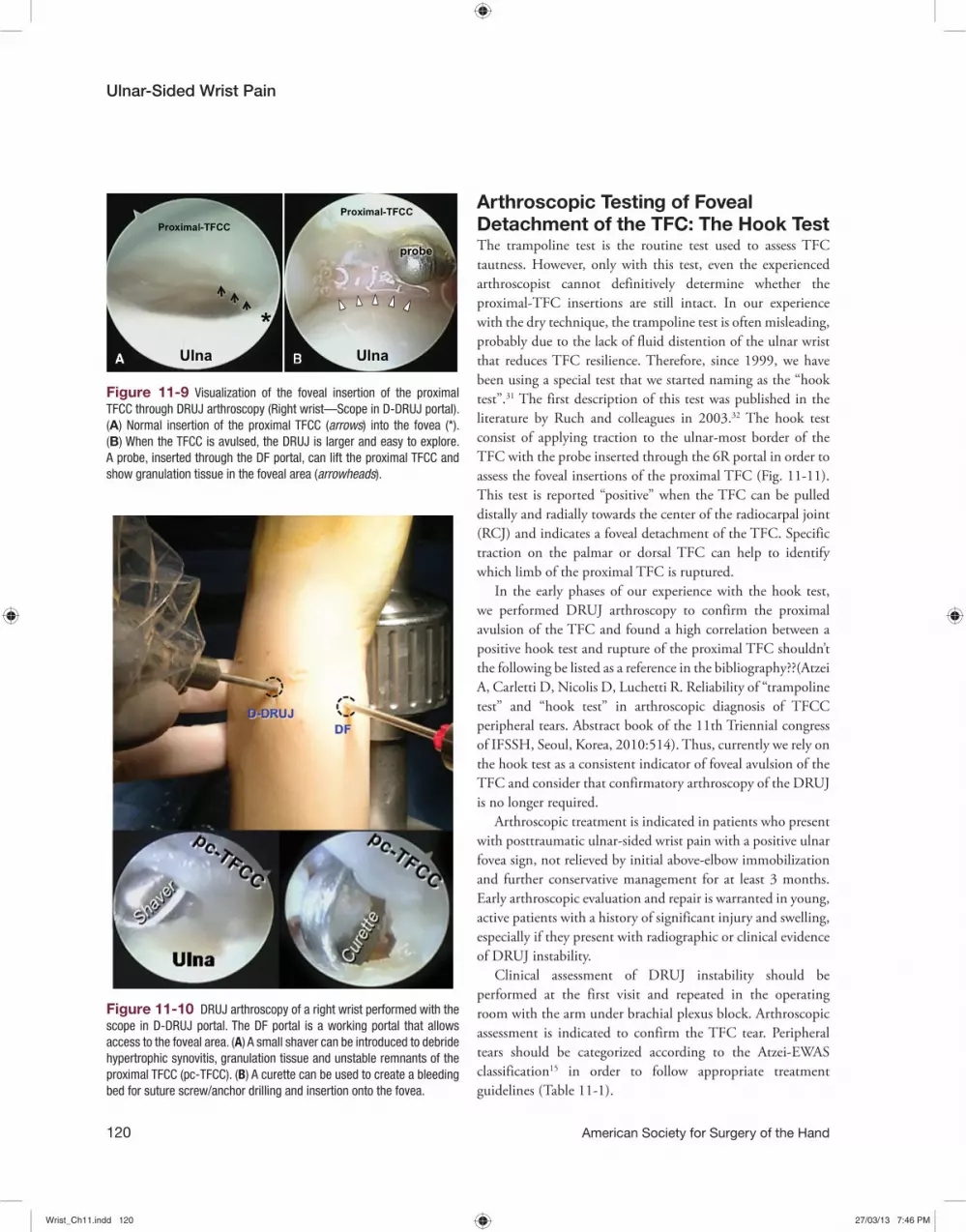
for joint debridement. The DF portal is located about 1 cm proximal to the 6U portal (Fig. 11-7a). During preparation of the DF portal, the dorsal sensory branches of the ulnar nerve (DSBUN) are at potential risk, thus careful blunt dissection using a hemostat and forearm supination are recommended to reduce the risk of damaging the DSBUN. A further attempt to protect the DSBUN is to make a 2 to 2.5 cm longitudinal skin incision proximally to the 6U portal, between the ECU and the FCU, in order to identify the nerve and retract it through this small open incision (Fig. 11-7b). However, laceration of the DSBUN is a rare complication even during arthroscopic training of inexperienced arthroscopists.29 The DF portal is made with the forearm in full supination, so that the ulnar styloid and the ECU tendon displace dorsally and the fovea and the ulnopalmar area of the distal ulna become subcutaneous and can be easily reached (Fig 11-8b). In smaller wrists, a volar ulnar (VU) portal is used.30 The DF portal is less technically demanding than the VU portal, but its use is limited to the introduction of working instruments in the area of the ulnar styloid and fovea.15 The scope through the D-DRUJ portal allows visualization of the foveal insertion of the proximal TFC (Fig. 11-9a) or its avulsion, which can probed through the DF portal (Fig. 11-9b). The DF portal is utilized to perform synovectomies and resect unstable ligamentous remnants, remove intraarticular loose bodies, or to prepare the bone for suture screw/anchor drilling and insertion (Fig. 11-10).
Figure 11-7 (A) The DF portal is located about 1 cm proximal to the 6U portal, on the very lateral aspect of the wrist. (B) Less experienced surgeons may prefer making a 2 to 2.5 cm longitudinal skin incision proximal to the 6U portal in order to identify and protect the dorsal sensory branch of the ulnar nerve (DSBUN) with two small Ragnell retractors.
Figure 11-8 (A) Artist’s rendering of the anatomical relationships of the ulnar wrist in neutral prono-supination, as in the standard arthroscopic setup. (B) With full forearm supination, the ulnar styloid and the ECU tendon displace dorsally so that the foveal area becomes subcutaneous and very easy to access. Full forearm supination is required to create the DF portal.
Wrist_Ch11.indd 119Wrist_Ch11.indd 119 27/03/13 7:46 PM27/03/13 7:46 PM
Ulnar-Sided Wrist Pain
120 American Society for Surgery of the Hand
Arthroscopic Testing of Foveal Detachment of the TFC: The Hook TestThe trampoline test is the routine test used to assess TFC tautness. However, only with this test, even the experienced arthroscopist cannot definitively determine whether the proximal-TFC insertions are still intact. In our experience with the dry technique, the trampoline test is often misleading, probably due to the lack of fluid distention of the ulnar wrist that reduces TFC resilience. Therefore, since 1999, we have been using a special test that we started naming as the “hook test”.31 The first description of this test was published in the literature by Ruch and colleagues in 2003.32 The hook test consist of applying traction to the ulnar-most border of the TFC with the probe inserted through the 6R portal in order to assess the foveal insertions of the proximal TFC (Fig. 11-11). This test is reported “positive” when the TFC can be pulled distally and radially towards the center of the radiocarpal joint (RCJ) and indicates a foveal detachment of the TFC. Specific traction on the palmar or dorsal TFC can help to identify which limb of the proximal TFC is ruptured.
In the early phases of our experience with the hook test, we performed DRUJ arthroscopy to confirm the proximal avulsion of the TFC and found a high correlation between a positive hook test and rupture of the proximal TFC shouldn’t the following be listed as a reference in the bibliography??(Atzei A, Carletti D, Nicolis D, Luchetti R. Reliability of “trampoline test” and “hook test” in arthroscopic diagnosis of TFCC peripheral tears. Abstract book of the 11th Triennial congress of IFSSH, Seoul, Korea, 2010:514). Thus, currently we rely on the hook test as a consistent indicator of foveal avulsion of the TFC and consider that confirmatory arthroscopy of the DRUJ is no longer required.
Arthroscopic treatment is indicated in patients who present with posttraumatic ulnar-sided wrist pain with a positive ulnar fovea sign, not relieved by initial above-elbow immobilization and further conservative management for at least 3 months. Early arthroscopic evaluation and repair is warranted in young, active patients with a history of significant injury and swelling, especially if they present with radiographic or clinical evidence of DRUJ instability.
Clinical assessment of DRUJ instability should be performed at the first visit and repeated in the operating room with the arm under brachial plexus block. Arthroscopic assessment is indicated to confirm the TFC tear. Peripheral tears should be categorized according to the Atzei-EWAS classification15 in order to follow appropriate treatment guidelines (Table 11-1).
Figure 11-10 DRUJ arthroscopy of a right wrist performed with the scope in D-DRUJ portal. The DF portal is a working portal that allows access to the foveal area. (A) A small shaver can be introduced to debride hypertrophic synovitis, granulation tissue and unstable remnants of the proximal TFCC (pc-TFCC). (B) A curette can be used to create a bleeding bed for suture screw/anchor drilling and insertion onto the fovea.
Figure 11-9 Visualization of the foveal insertion of the proximal TFCC through DRUJ arthroscopy (Right wrist—Scope in D-DRUJ portal). (A) Normal insertion of the proximal TFCC (arrows) into the fovea (*). (B) When the TFCC is avulsed, the DRUJ is larger and easy to explore. A probe, inserted through the DF portal, can lift the proximal TFCC and show granulation tissue in the foveal area (arrowheads).
Wrist_Ch11.indd 120Wrist_Ch11.indd 120 27/03/13 7:46 PM27/03/13 7:46 PM

Chapter 11 • Arthroscopic Management of Unstable TFCC Lesions
American Society for Surgery of the Hand 121
Only Class 1 tear (repairable isolated distal tear) shows slight to no instability. These tears can be reattached to the dorsal ulnocarpal joint capsule and/or the ECU tendon subsheath by one of the many arthroscopic suturing techniques described in the literature33–35 with good resolution of symptoms. Class 2 (repairable complete tear) is the typical peripheral tear with DRUJ instability. Also Class 3 (isolated repairable proximal tear) presents with DRUJ instability, but it may be more difficult to diagnose due to the normal appearance of the distal TFC upon RCJ arthroscopy: positive hook test and DRUJ arthroscopy will reveal the rupture of the proximal TFC. Both Class 2 and 3 require foveal reattachment of the TFC. Class 4 (nonrepairable tears) need ligament reconstruction using a tendon graft, either open36 or arthroscopic,15 to restore DRUJ stability. When a TFCC tear is associated with DRUJ arthritis, as in Class 5, neither repair nor reconstruction are indicated: this condition is best treated by salvage procedures, such as resection arthroplasty—open37 or arthroscopic38—or joint replacement.39 Repair is also contraindicated in chronic Essex-Lopresti interosseous membrane injury, previous soft-tissue infection, osteomyelitis or severe osteoporosis of the ulnar head, and low-demand patients who are not healthy enough for surgery. Relative contraindications include carpal chondromalacia, or ulnar positive variance in which concomitant arthroscopic wafer procedure or ulnar shortening osteotomy is required for joint leveling. Hypoplasia of the palmar or dorsal rim of the sigmoid notch, if present, may require osteotomy and bone graft.
Figure 11-11 (A) The hook test evaluates tautness of the foveal insertions of the proximal TFCC through radiocarpal arthroscopy (scope 3-4): the probe inserted through the 6R portal in the prestyloid recessus and applies traction to the ulnar-most border of the TFCC. (B) When the proximal TFCC is torn/avulsed, it can be displaced towards the center of the RCJ and the test is considered positive.
Surgical Technique
Arthroscopic Foveal Reattachment of Repairable TFCC TearsThe wrist is suspended by finger traps using a wrist traction tower in the standard arthroscopic setup, as for diagnostic arthroscopy. Joint distension is usually not required and the use of the dry technique is advisable, since it benefits complex and long-lasting procedures.
A 2.7-mm arthroscope is used routinely. A 1.9-mm arthroscope may be necessary for smaller wrists. The scope is introduced through the 3-4 portal, and tears of the distal component of the TFCC are seen on the dorsal-ulnar aspect. Depending on the delay of treatment, tears are frequently covered by coagulated hematoma or granulation tissue. The 6R portal is used to insert the probe to assess TFC tautness or a shaver in order to debride the tear. The 6U portal is also established to facilitate joint debridement and late TFC suturing.
Arthroscopic reattachment of the foveal insertion of the TFC starts with a DRUJ arthroscopy. It requires preparation of the D-DRUJ portal for DRUJ exploration and the DF portal (see above), as a working portal to provide instrument access to the fovea ulnaris (Fig. 11-7). With forearm supination, the fovea is located palmarly at the base of the ulnar styloid, just lateral to the capsule as an area of soft bone that can be easily pierced with the tip of a probe (Fig. 11-8). After cautious blunt
Wrist_Ch11.indd 121Wrist_Ch11.indd 121 27/03/13 7:46 PM27/03/13 7:46 PM

Ulnar-Sided Wrist Pain
122 American Society for Surgery of the Hand
Figure 11-12 Operative setup for arthroscopic foveal reattachment with suture anchor (right wrist). The technique starts with DRUJ arthroscopy (scope in D-DRUJ). (A) The suture anchor is introduced through the DF portal and drilled into the fovea. (B) Artist’s rendering shows the four strands exiting the DF portal after suture anchor insertion.
Figure 11-13 The needle is loaded with the radial thread of the palmar suture (green) and is introduced from the DF portal through the TFCC to exit in the RCJ. The suture should pierce the TFCC close to its palmar edge, to grasp the palmar limb of the DRUJ ligament and the origin of UC ligaments. Then radial thread of the dorsal suture (blue) is introduced from the DF portal to pierce the dorsal edge of the TFCC, in order to grasp the dorsal limb of the DRUJ ligament. The scope is in the 3-4 portal to ensure correct suture placement.
dissection to avoid damage to the DSBUN, a small shaver or curette is introduced through the DF portal to debride the torn or avulsed ligament and also to prepare a bleeding bone bed for insertion of a suture anchor onto the fovea (Fig. 11-10). The use of a suture anchor with a pair of sutures (4 strands) will produce an increased area of contact for the ligament against the fovea promoting healing.40 The advantage of using two sutures in the anchor is that each limb of the ligament can be repaired independently, in order to re-create a more anatomical repair of the TFCC.
With the forearm in full supination, the anchor is inserted through the DF portal so that the sutures exit the DF portal from under the TFC (Fig. 11-12). It is important to recognize that one suture is palmar and the other one more dorsal, and that each suture has a radial and an ulnar strand. The end of each suture strand is loaded into the tip of a 25-G hypodermic or Tuohy needle using the so-called suture loop technique.15
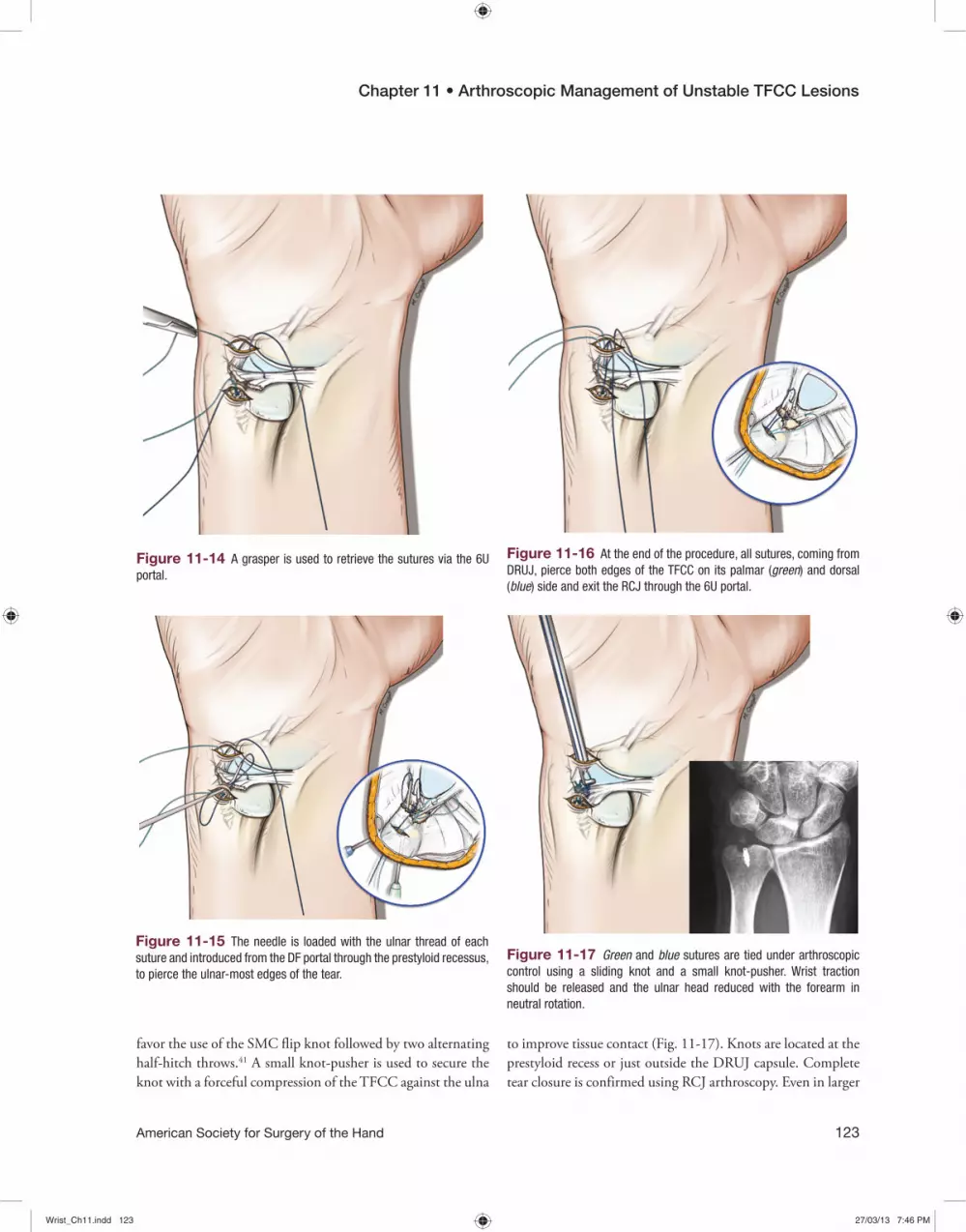
The radial strand of the palmar suture is introduced from the DF portal through the TFC to exit in the RCJ. Then the scope is shifted to the 3-4 portal (Fig. 11-13) to ensure correct placement of the radial thread of the palmar suture across the TFC’s palmar edge. This corresponds to the palmar limb of the DRUJ ligament and the origin of the UC ligaments. The suture is retrieved with a grasper through the 6U portal (Fig. 11-14). Then the end of the ulnar thread of the same suture is introduced from the DF portal through the prestyloid recess and retrieved through the same 6U portal (Fig. 11-15). The same procedure is performed to pass the radial thread of the dorsal suture across the dorsal edge of the TFC to hold the dorsal limb of the DRUJ ligament and its ulnar thread through the pre-styloid recess, and both strands are retrieved through the 6U portal (Fig. 11-16). All sutures are retrieved from the 6U portal and should be identified and cleared from interposed soft tissue, in order to prepare for knot tying. Wrist traction is released and an assistant maintains the ulnar head in a reduced position with the forearm in neutral rotation. The sutures are tied under arthroscopic vision using a sliding knot. Due to the ease of knot placement and reduced bulkiness, we
Wrist_Ch11.indd 122Wrist_Ch11.indd 122 27/03/13 7:46 PM27/03/13 7:46 PM
Chapter 11 • Arthroscopic Management of Unstable TFCC Lesions
American Society for Surgery of the Hand 123
favor the use of the SMC flip knot followed by two alternating half-hitch throws.41 A small knot-pusher is used to secure the knot with a forceful compression of the TFCC against the ulna
Figure 11-14 A grasper is used to retrieve the sutures via the 6U portal.
Figure 11-15 The needle is loaded with the ulnar thread of each suture and introduced from the DF portal through the prestyloid recessus, to pierce the ulnar-most edges of the tear.
Figure 11-16 At the end of the procedure, all sutures, coming from DRUJ, pierce both edges of the TFCC on its palmar (green) and dorsal (blue) side and exit the RCJ through the 6U portal.
Figure 11-17 Green and blue sutures are tied under arthroscopic control using a sliding knot and a small knot-pusher. Wrist traction should be released and the ulnar head reduced with the forearm in neutral rotation.
to improve tissue contact (Fig. 11-17). Knots are located at the prestyloid recess or just outside the DRUJ capsule. Complete tear closure is confirmed using RCJ arthroscopy. Even in larger
Wrist_Ch11.indd 123Wrist_Ch11.indd 123 27/03/13 7:46 PM27/03/13 7:46 PM

Ulnar-Sided Wrist Pain
124 American Society for Surgery of the Hand
Class 2 TFC peripheral tears, further ligament-to-capsule sutures are seldom necessary to repair the distal component of the TFC. The DRUJ is assessed for range of forearm rotation and residual laxity.
RehabilitationDuring the first week postoperatively, the patient is placed in a long arm splint in neutral forearm rotation. A Münster-type thermoplastic splint, which allows elbow flexion and extension but restricts forearm rotation, is worn for another 3 weeks. Unrestricted wrist flexion/extension is started at 3 weeks. During the first week of rehabilitation, progressive forearm rotation is allowed, but the splint is still worn between exercises. During the next 6 weeks, resisted movements are not permitted. Progressive resisted wrist and hand strengthening exercises begin after the sixth week, until the patient is able to bear weight on the operated wrist. Sport and heavy work tasks are allowed only after 3 months, according to the recovery of the forearm muscle strength and endurance.
Arthroscopic Tendon Graft Reconstruction of Nonrepairable TFCC TearsThe operative setup is the same as for a standard dry wrist arthroscopy. The 3-4 portal is used for the arthroscope and 6R, 4-5, and 6U portals are used as accessory portals for instrumentation. When standard diagnostic wrist arthroscopy reveals a nonrepairable (Class 4) TFC peripheral tear, arthroscopic reconstruction with a tendon graft is indicated, which is a modification of the open procedure using a palmaris longus (PL) tendon graft.36 In addition to the arthroscopic portals, it is necessary to prepare two limited open approaches to the palmar and dorsal distal radius (Fig. 11-18). A 2.5 cm palmar longitudinal incision is made from the proximal wrist crease in order to expose the palmar aspect of the distal radius and to harvest the distal part of the Palmaris Longus (PL) tendon. The PL tendon is divided proximally through a 1 cm transverse incision over the musculotendinous junction. When PL is absent, the flexor digitorum superficialis tendon of the ring finger, or a strip of the FCR may be harvested. The ulnar part of the palmar aspect of the distal radius is accessed in the interval between the ulnar neurovascular bundle and the finger flexor tendons. Special care is taken to free and protect the ulnar neurovascular bundle from any adhesions over the palmar aspect of the ulnar carpus, to avoid damage during passage of the tendon graft. The palmar carpal arch that anastomoses between the radial artery
and the anterior interosseous artery and courses volar to the pronator quadratus is coagulated, and the pronator quadratus is retracted proximally to allow sub-periosteal dissection of the ulnar corner of the palmar radius.
On the dorsal aspect of the wrist, the skin incision for the 4-5 portal is extended 2–3 cm proximally, the extensor retinaculum is incised, the posterior interosseous nerve is preserved to spare wrist proprioceptive input and it is retracted radially, and the dorsoulnar corner of the distal radius is exposed by sub-periosteal dissection. Fluoroscopic control is used to allow for precise positioning of a guide-wire for cannulated drilling of the distal radius through the floor of the 4th extensor compartment (Fig. 11-19). Care is taken to prevent fracture of the subchondral bone during drilling. A 2.4-mm cannulated drill bit is driven over the guide-wire through the radius, just a few millimeters proximal to the articular surface of the lunate fossa and radial to the sigmoid notch. The tunnel is progressively enlarged to 3.4–4 mm with standard drill bits according to the size of the graft.
Figure 11-18 Artist’s rendering and intraoperative views of the dorsal and palmar aspect of a right wrist showing the portals and skin incisions required for arthroscopic reconstruction of the TFCC.
Wrist_Ch11.indd 124Wrist_Ch11.indd 124 27/03/13 7:46 PM27/03/13 7:46 PM
Chapter 11 • Arthroscopic Management of Unstable TFCC Lesions
American Society for Surgery of the Hand 125
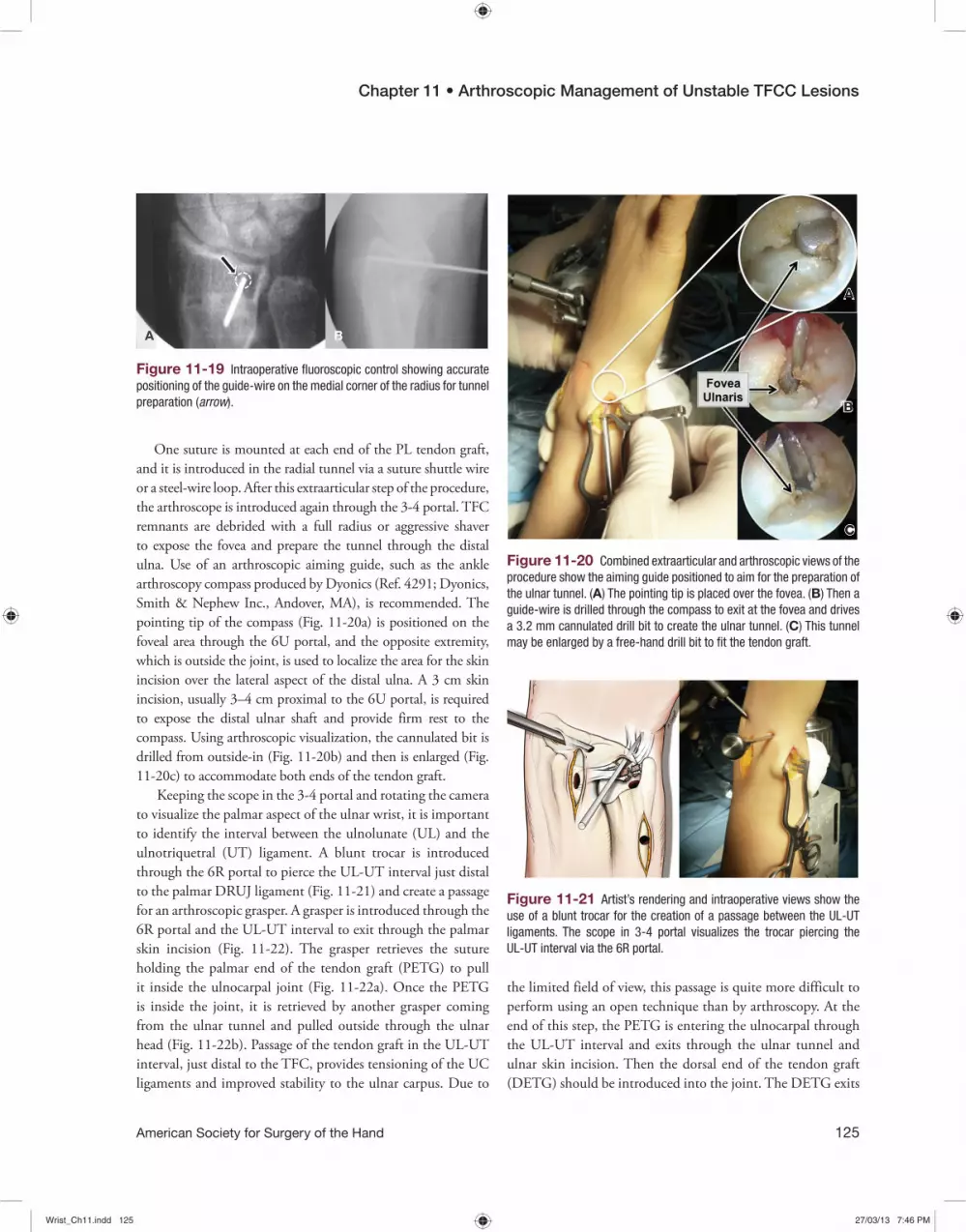
One suture is mounted at each end of the PL tendon graft, and it is introduced in the radial tunnel via a suture shuttle wire or a steel-wire loop. After this extraarticular step of the procedure, the arthroscope is introduced again through the 3-4 portal. TFC remnants are debrided with a full radius or aggressive shaver to expose the fovea and prepare the tunnel through the distal ulna. Use of an arthroscopic aiming guide, such as the ankle arthroscopy compass produced by Dyonics (Ref. 4291; Dyonics, Smith & Nephew Inc., Andover, MA), is recommended. The pointing tip of the compass (Fig. 11-20a) is positioned on the foveal area through the 6U portal, and the opposite extremity, which is outside the joint, is used to localize the area for the skin incision over the lateral aspect of the distal ulna. A 3 cm skin incision, usually 3–4 cm proximal to the 6U portal, is required to expose the distal ulnar shaft and provide firm rest to the compass. Using arthroscopic visualization, the cannulated bit is drilled from outside-in (Fig. 11-20b) and then is enlarged (Fig. 11-20c) to accommodate both ends of the tendon graft.
Keeping the scope in the 3-4 portal and rotating the camera to visualize the palmar aspect of the ulnar wrist, it is important to identify the interval between the ulnolunate (UL) and the ulnotriquetral (UT) ligament. A blunt trocar is introduced through the 6R portal to pierce the UL-UT interval just distal to the palmar DRUJ ligament (Fig. 11-21) and create a passage for an arthroscopic grasper. A grasper is introduced through the 6R portal and the UL-UT interval to exit through the palmar skin incision (Fig. 11-22). The grasper retrieves the suture holding the palmar end of the tendon graft (PETG) to pull it inside the ulnocarpal joint (Fig. 11-22a). Once the PETG is inside the joint, it is retrieved by another grasper coming from the ulnar tunnel and pulled outside through the ulnar head (Fig. 11-22b). Passage of the tendon graft in the UL-UT interval, just distal to the TFC, provides tensioning of the UC ligaments and improved stability to the ulnar carpus. Due to
Figure 11-19 Intraoperative fluoroscopic control showing accurate positioning of the guide-wire on the medial corner of the radius for tunnel preparation (arrow).
Figure 11-20 Combined extraarticular and arthroscopic views of the procedure show the aiming guide positioned to aim for the preparation of the ulnar tunnel. (A) The pointing tip is placed over the fovea. (B) Then a guide-wire is drilled through the compass to exit at the fovea and drives a 3.2 mm cannulated drill bit to create the ulnar tunnel. (C) This tunnel may be enlarged by a free-hand drill bit to fit the tendon graft.
the limited field of view, this passage is quite more difficult to perform using an open technique than by arthroscopy. At the end of this step, the PETG is entering the ulnocarpal through the UL-UT interval and exits through the ulnar tunnel and ulnar skin incision. Then the dorsal end of the tendon graft (DETG) should be introduced into the joint. The DETG exits
Figure 11-21 Artist’s rendering and intraoperative views show the use of a blunt trocar for the creation of a passage between the UL-UT ligaments. The scope in 3-4 portal visualizes the trocar piercing the UL-UT interval via the 6R portal.
Wrist_Ch11.indd 125Wrist_Ch11.indd 125 27/03/13 7:46 PM27/03/13 7:46 PM
Ulnar-Sided Wrist Pain
126 American Society for Surgery of the Hand
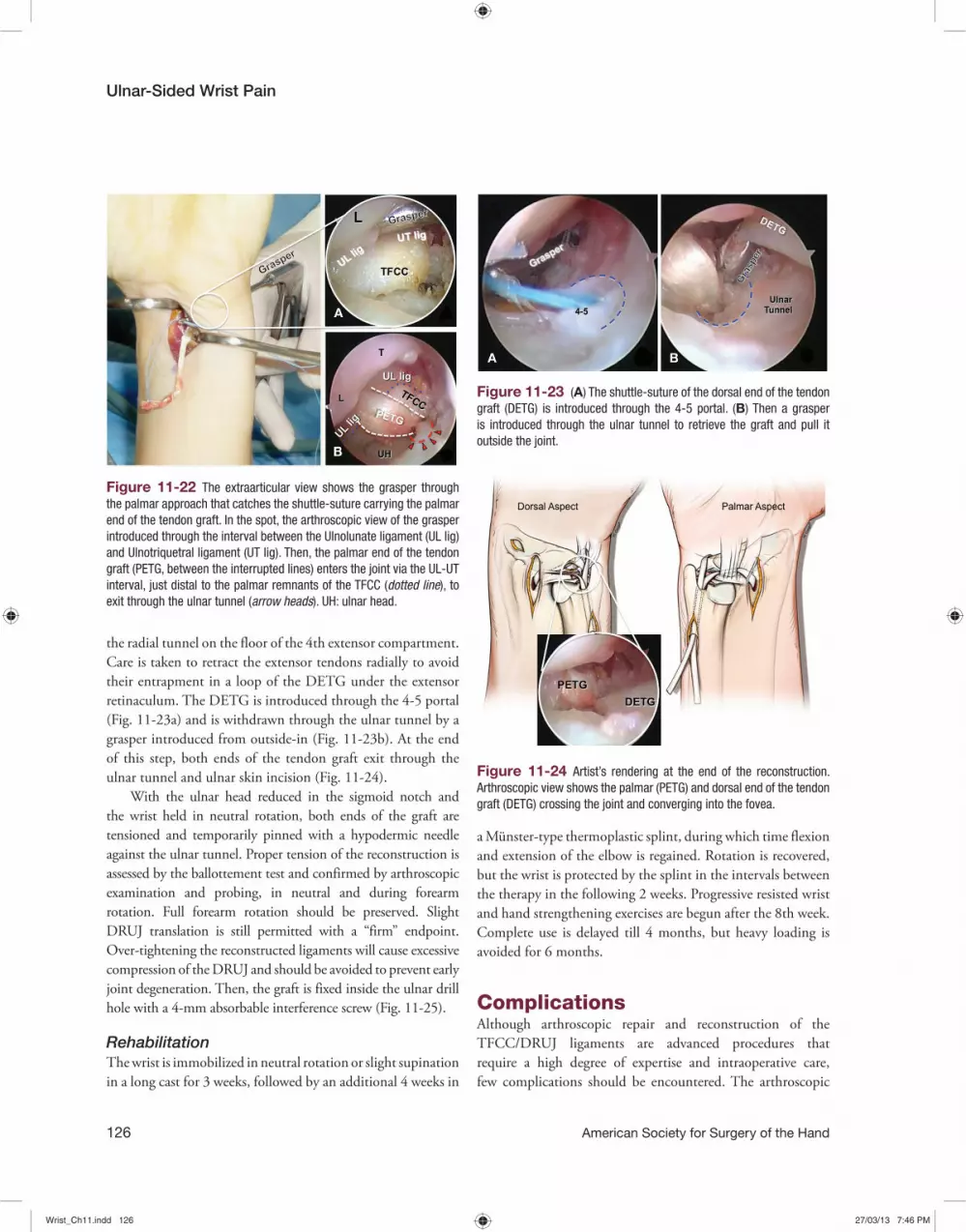
Figure 11-22 The extraarticular view shows the grasper through the palmar approach that catches the shuttle-suture carrying the palmar end of the tendon graft. In the spot, the arthroscopic view of the grasper introduced through the interval between the Ulnolunate ligament (UL lig) and Ulnotriquetral ligament (UT lig). Then, the palmar end of the tendon graft (PETG, between the interrupted lines) enters the joint via the UL-UT interval, just distal to the palmar remnants of the TFCC (dotted line), to exit through the ulnar tunnel (arrow heads). UH: ulnar head.
Figure 11-23 (A) The shuttle-suture of the dorsal end of the tendon graft (DETG) is introduced through the 4-5 portal. (B) Then a grasper is introduced through the ulnar tunnel to retrieve the graft and pull it outside the joint.
Figure 11-24 Artist’s rendering at the end of the reconstruction. Arthroscopic view shows the palmar (PETG) and dorsal end of the tendon graft (DETG) crossing the joint and converging into the fovea.
the radial tunnel on the floor of the 4th extensor compartment. Care is taken to retract the extensor tendons radially to avoid their entrapment in a loop of the DETG under the extensor retinaculum. The DETG is introduced through the 4-5 portal (Fig. 11-23a) and is withdrawn through the ulnar tunnel by a grasper introduced from outside-in (Fig. 11-23b). At the end of this step, both ends of the tendon graft exit through the ulnar tunnel and ulnar skin incision (Fig. 11-24).
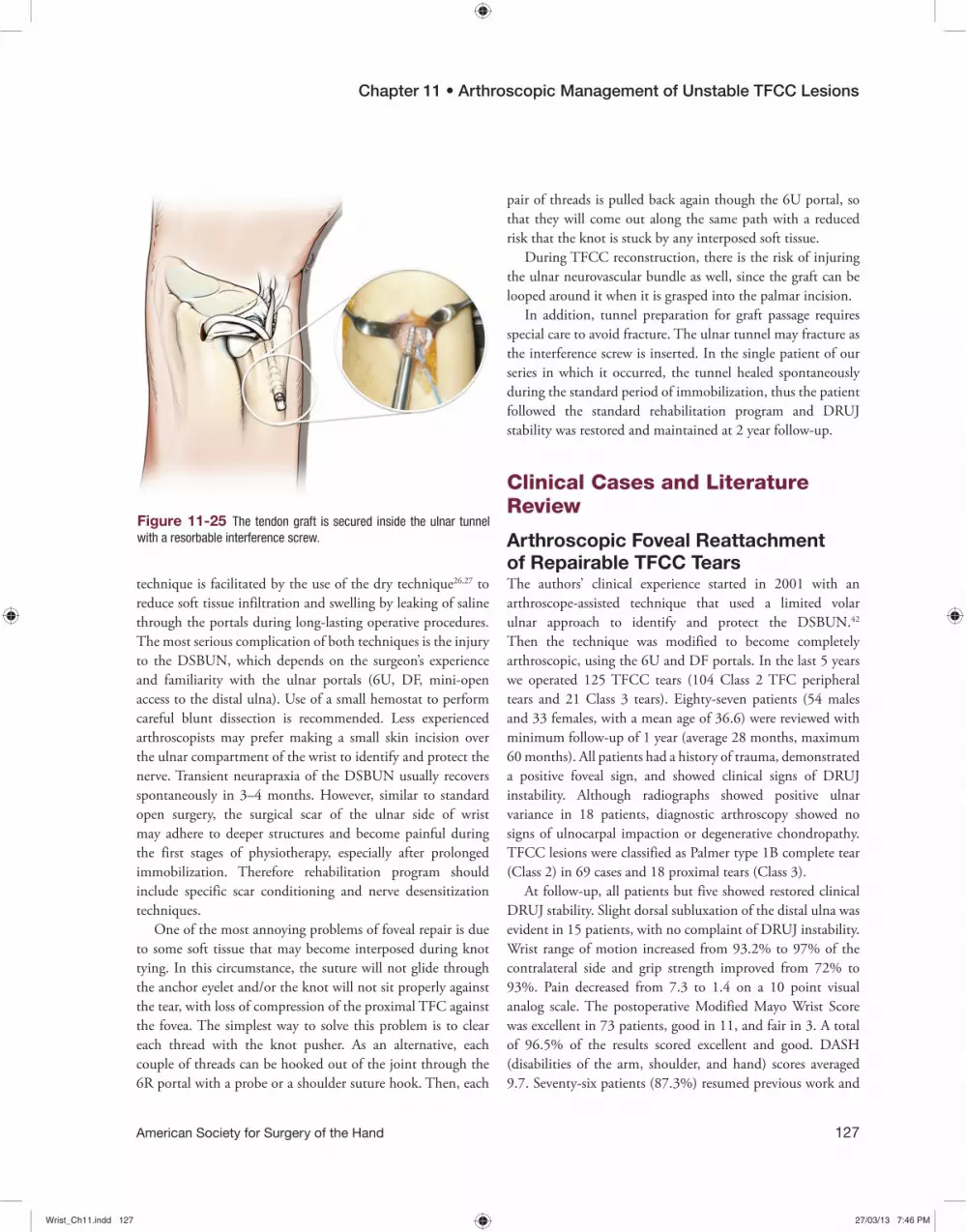
With the ulnar head reduced in the sigmoid notch and the wrist held in neutral rotation, both ends of the graft are tensioned and temporarily pinned with a hypodermic needle against the ulnar tunnel. Proper tension of the reconstruction is assessed by the ballottement test and confirmed by arthroscopic examination and probing, in neutral and during forearm rotation. Full forearm rotation should be preserved. Slight DRUJ translation is still permitted with a “firm” endpoint. Over-tightening the reconstructed ligaments will cause excessive compression of the DRUJ and should be avoided to prevent early joint degeneration. Then, the graft is fixed inside the ulnar drill hole with a 4-mm absorbable interference screw (Fig. 11-25).
RehabilitationThe wrist is immobilized in neutral rotation or slight supination in a long cast for 3 weeks, followed by an additional 4 weeks in
a Münster-type thermoplastic splint, during which time flexion and extension of the elbow is regained. Rotation is recovered, but the wrist is protected by the splint in the intervals between the therapy in the following 2 weeks. Progressive resisted wrist and hand strengthening exercises are begun after the 8th week. Complete use is delayed till 4 months, but heavy loading is avoided for 6 months.
ComplicationsAlthough arthroscopic repair and reconstruction of the TFCC/DRUJ ligaments are advanced procedures that require a high degree of expertise and intraoperative care, few complications should be encountered. The arthroscopic
Wrist_Ch11.indd 126Wrist_Ch11.indd 126 27/03/13 7:46 PM27/03/13 7:46 PM
Chapter 11 • Arthroscopic Management of Unstable TFCC Lesions
American Society for Surgery of the Hand 127
technique is facilitated by the use of the dry technique26,27 to reduce soft tissue infiltration and swelling by leaking of saline through the portals during long-lasting operative procedures. The most serious complication of both techniques is the injury to the DSBUN, which depends on the surgeon’s experience and familiarity with the ulnar portals (6U, DF, mini-open access to the distal ulna). Use of a small hemostat to perform careful blunt dissection is recommended. Less experienced arthroscopists may prefer making a small skin incision over the ulnar compartment of the wrist to identify and protect the nerve. Transient neurapraxia of the DSBUN usually recovers spontaneously in 3–4 months. However, similar to standard open surgery, the surgical scar of the ulnar side of wrist may adhere to deeper structures and become painful during the first stages of physiotherapy, especially after prolonged immobilization. Therefore rehabilitation program should include specific scar conditioning and nerve desensitization techniques.
One of the most annoying problems of foveal repair is due to some soft tissue that may become interposed during knot tying. In this circumstance, the suture will not glide through the anchor eyelet and/or the knot will not sit properly against the tear, with loss of compression of the proximal TFC against the fovea. The simplest way to solve this problem is to clear each thread with the knot pusher. As an alternative, each couple of threads can be hooked out of the joint through the 6R portal with a probe or a shoulder suture hook. Then, each
Figure 11-25 The tendon graft is secured inside the ulnar tunnel with a resorbable interference screw.
pair of threads is pulled back again though the 6U portal, so that they will come out along the same path with a reduced risk that the knot is stuck by any interposed soft tissue.
During TFCC reconstruction, there is the risk of injuring the ulnar neurovascular bundle as well, since the graft can be looped around it when it is grasped into the palmar incision.
In addition, tunnel preparation for graft passage requires special care to avoid fracture. The ulnar tunnel may fracture as the interference screw is inserted. In the single patient of our series in which it occurred, the tunnel healed spontaneously during the standard period of immobilization, thus the patient followed the standard rehabilitation program and DRUJ stability was restored and maintained at 2 year follow-up.
Clinical Cases and Literature Review
Arthroscopic Foveal Reattachment of Repairable TFCC TearsThe authors’ clinical experience started in 2001 with an arthroscope-assisted technique that used a limited volar ulnar approach to identify and protect the DSBUN.42 Then the technique was modified to become completely arthroscopic, using the 6U and DF portals. In the last 5 years we operated 125 TFCC tears (104 Class 2 TFC peripheral tears and 21 Class 3 tears). Eighty-seven patients (54 males and 33 females, with a mean age of 36.6) were reviewed with minimum follow-up of 1 year (average 28 months, maximum 60 months). All patients had a history of trauma, demonstrated a positive foveal sign, and showed clinical signs of DRUJ instability. Although radiographs showed positive ulnar variance in 18 patients, diagnostic arthroscopy showed no signs of ulnocarpal impaction or degenerative chondropathy. TFCC lesions were classified as Palmer type 1B complete tear (Class 2) in 69 cases and 18 proximal tears (Class 3).
At follow-up, all patients but five showed restored clinical DRUJ stability. Slight dorsal subluxation of the distal ulna was evident in 15 patients, with no complaint of DRUJ instability. Wrist range of motion increased from 93.2% to 97% of the contralateral side and grip strength improved from 72% to 93%. Pain decreased from 7.3 to 1.4 on a 10 point visual analog scale. The postoperative Modified Mayo Wrist Score was excellent in 73 patients, good in 11, and fair in 3. A total of 96.5% of the results scored excellent and good. DASH (disabilities of the arm, shoulder, and hand) scores averaged 9.7. Seventy-six patients (87.3%) resumed previous work and
Wrist_Ch11.indd 127Wrist_Ch11.indd 127 27/03/13 7:46 PM27/03/13 7:46 PM

Ulnar-Sided Wrist Pain
128 American Society for Surgery of the Hand
recreational activities, and 11 patients (12.7%) returned to restricted employment.
Although responsible for disabling DRUJ instability, rupture of the foveal attachment of the TFC is often underdiagnosed by wrist arthroscopy. As the foveal fibers cannot be visualized using the standard RCJ arthroscopy, many surgeons consider that foveal repair of the TFC should be performed by open techniques3 and arthroscopy should be limited to simple mending procedures similar to the meniscal suture in the knee. Routine use of the preoperative ballottement test, the hook test, and DRUJ arthroscopy facilitates the diagnosis. Increased expertise and the introduction of new DRUJ portals, such as the DF portal, make it possible to restore the foveal attachments of the proximal TFC to the bone by arthroscopic techniques, as well. Standard open techniques rely on transosseous tunnels for refixation43 because this repair is considered stronger and more resistant against shear forces compared to anchor fixation. However, Chou44 has demonstrated that there is no difference between the techniques and that the anchor technique is easier and quicker to perform, with a reduced risk of anchor pull out. These results are confirmed by our experience with our arthroscopic technique that showed very satisfactory results. Furthermore, arthroscopy allows a better intraarticular view and more accurate suturing of both limbs of the DRUJ ligament, especially the palmar DRUJ ligament that would be very difficult to reach by open approach. Moreover, since only a small incision of the joint capsule is required, the innervation of the capsule and its proprioceptive character are preserved,45 the postoperative pain is also of reduced intensity, so that the functional recovery is potentially easier and quicker than after an open procedure.
Arthroscopic Tendon Graft Reconstruction of Nonrepairable TFCC TearsThe authors’ experience with this technique started in 200546 and since then 11 patients underwent arthroscopic reconstruction of the TFCC. Four patients (all males, mean age 28 years) were reviewed with a minimum follow-up of 1 year (average 22 months, maximum 34 months).
References 1. Palmer AK. Triangular fibrocartilage complex lesions: a classification.
J Hand Surg Am. 1989;14:594–606. 2. Nakamura T, Yabe Y, Horiuchi Y. Functional anatomy of the triangular
fibrocartilage complex. Hand Surg. 1996;21:581–586.
3. Nakamura T, Makita A. The proximal ligamentous component of the triangular fibrocartilage complex: functional anatomy and three-dimensional changes in length of the radioulnar ligament during pronation-supination. J Hand Surg Br. 2000;25:479–486.
Three patients complained of severe DRUJ instability following distal radius fracture and one patient had instability due to calcium deposits on chronic degenerative changes of DRUJ ligaments. The ulnar styloid was ununited in two. In all patients, arthroscopy revealed a nonrepairable Palmer Type 1B ulnar avulsion (Class 4). One patient had associated luno-triquetral instability (Geissler stage 3. Geissler testing may be performed on lunate-triquetral (LT) joint so that the same staging may be applied, and it is readily understandable).
At follow-up, DRUJ stability was restored in all. The range of motion increased from 85% to 95% of the contra-lateral side and grip strength increased from 65% to 87%. Pain decreased from 8.7 to 1.7 on a 10 point visual analog scale. Modified Mayo Wrist Score was excellent in 3 patients and good in 1. All patients were satisfied with the results of the procedure, 3 resumed manual activities and previous work and 1 changed work for unrelated reasons.
The arthroscopic classification of TFCC tears (Table 11-1) helps the surgeon to recognize those cases that cannot be treated by direct TFCC repair and choose the best treatment.
Compared to the open technique,36 the primary advantage of the arthroscopic technique is that it is minimally invasive, protects ligaments and its proprioceptive innervation, and allows for a limited scar adhesion and joint stiffness so that postoperative pain is reduced and rehabilitation is quicker. Moreover, complete intraarticular visualization and magnification of the operating field provides an improved level of surgical precision, especially in the foveal placement of the ulnar tunnel and in the passage of the graft through the interval between the palmar ulnocarpal ligaments.
Due to the limited space in the ulnar carpus, this surgical step is rather difficult to perform during open surgery, however it is very important to achieve complete stabilization of the ulnar carpus and DRUJ.
Treatment of DRUJ instability by arthroscopic TFC foveal repair or reconstruction represents an exciting frontier in wrist surgery that may overcome the difficulties of open surgery.
These complex procedures demand a steep learning curve. However, once the technique is mastered, the numerous advantages over open surgery will give good reason for the specific competence and arthroscopic skills required.
Wrist_Ch11.indd 128Wrist_Ch11.indd 128 27/03/13 7:47 PM27/03/13 7:47 PM

Chapter 11 • Arthroscopic Management of Unstable TFCC Lesions
American Society for Surgery of the Hand 129
4. Adams BD, Holley KA. Strains in the articular disk of the triangular fibrocartilage complex: a biomechanical study. J Hand Surg Am. 1993;18:919–925.
5. Palmer AK, Werner FW. The triangular fibrocartilage complex of the wrist: anatomy and function. J Hand Surg Am. 1981;6:153–162.
6. Benjamin M, Evans EJ, Pemberton DJ. Histological studies on the triangular fibrocartilage complex of the wrist. J Anat. 1990;172:59–67.
7. Kauer JMG. The distal radioulnar joint: anatomic and functional considerations. Clin Orthop Relat R. 1992;275:37–45.
8. Kleinman WB. Stability of the distal radioulnar joint: biomechanics, pathophysiology, physical diagnosis and restoration of function. What we have learned in 25 years. J Hand Surg Am. 2007;32:1087–1106.
9. Haugstvedt JR, Berger RA, Nakamura T, Neale P, Berglund L, An KN. Relative contributions of the ulnar attachments of the triangular fibrocartilage complex to the dynamic stability of the distal radioulnar joint. J Hand Surg Am. 2006;31:445-451.
10. Moritomo H, Murase T, Arimitsu S, Oka K. Change in the length of the ulnocarpal ligaments during radiocarpal motion: possible impact on triangular fibrocartilage complex foveal tears. J Hand Surg Am. 2008;33:1278–1286.
11. Dy CJ, Ouellette EA, Makowski AL, Milne E, Latta LL. Peripheral triangular fibrocartilage complex tears cause ulnocarpal instability: a biomechanical pilot study. Clin Orthop Relat Res. 2012;470(10):2771-2775.
12. Atzei A, Luchetti R. Foveal TFCC tear: classification and treatment. Hand Clin. 2011;27:263–272.
13. Estrella EP, Hung LK, Ho PC, et al. Arthroscopic repair of triangular fibrocartilage complex tears. Arthroscopy. 2007;23:729–737.
14. Anderson ML, Larson N, Moran S, Cooney WP, Amrami KK, Berger RA. Clinical comparison of arthroscopic versus open repair of triangular fibrocartilage complex tears. J Hand Surg Am. 2008;33:675-682.
15. Atzei A. New trends in arthroscopic management of type 1-B TFCC injuries with DRUJ instability. J Hand Surg Eur Vol. 2009;34:582–591.
16. Tay SC, Tomita K, Berger RA. The “ulnar fovea sign” for defining ulnar wrist pain: an analysis of sensitivity and specificity. J Hand Surg Am. 2007;32:438–444.
17. Moriya T, Aoki M, Iba K, et al. Effect of triangular ligament tears on distal radioulnar joint instability and evaluation of three clinical tests: a biomechanical study. J Hand Surg Eur Vol. 2009;34:219–223.
18. Lindau T, Adlercreutz C, Aspenberg P. Peripheral tears of the triangular fibrocartilage complex cause distal radioulnar joint instability after distal radial fractures. J Hand Surg Am. 2000;25:464–468.
19. May MM, Lawton JN, Blazar PE. Ulnar styloid fractures associated with distal radius fractures: incidence and implications for distal radioulnar joint instability. J Hand Surg Am. 2002;27:965–971.
20. Richards RS, Bennett JD, Roth JH, et al. Arthroscopic diagnosis of intraarticular soft tissue injuries associated with distal radial fractures. J Hand Surg Am. 1997;22:772–776.
21. Lindau T. Treatment of injuries to the ulnar side of the wrist occurring with distal radial fractures. Hand Clin. 2005;21:417–425.
22. Rettig ME, Raskin KB. Galeazzi fracture dislocation: a new treatment-oriented classification. J Hand Surg Am. 2001;26:228–235.
23. Zanetti M, Bram J, Hodler J. Triangular fibrocartilage and intercarpal ligaments of the wrist: does MR arthrography improve standard MRI? J Magn Reson Imaging. 1997;7:590–594.
24. Fulcher S, Poehling G. The role of operative arthroscopy for the diagnosis and treatment of lesions about the distal ulna. Hand Clin. 1998;14:285–296.
25. Pederzini L, Luchetti R, Soragni O, et al. Evaluation of the triangular fibrocartilage complex tears by arthroscopy, arthrography, and magnetic resonance imaging. Arthroscopy. 1992;8:191–197.
26. Atzei A, Luchetti R, Sgarbossa A, Carità E, Llusà M. Setup, portals and normal exploration in wrist arthroscopy. Chir de la Main. 2006;25(Suppl.):S131–S144.
27. del Piñal F, García-Bernal FJ, Pisani D, Regalado J, Ayala H, Studer A. Dry arthroscopy of the wrist: surgical technique. J Hand Surg Am. 2007;32:119–123.
28. Hermansdorfer JD, Kleinman WB. Management of chronic peripheral tears of the triangular fibrocartilage complex. J Hand Surg Am. 1991;16:340–346.
29. Poublon AR, Kleinrensink G-J, Coert JH. Which portal related complications occur during a wrist arthroscopy workshop? J Hand Surg. 2012;37E(Suppl.).
30. Slutsky DJ. Distal radioulnar joint arthroscopy and the volar ulnar portal. Tech Hand Up Extrem Surg. 2007;11:38–44.
31. Atzei A, Rizzo A, Luchetti R, et al. Arthroscopic foveal repair of triangular fibrocartilage complex peripheral lesion with distal radioulnar joint instability. Tech Hand Up Extrem Surg. 2008;12:226–235.
32. Ruch DS, Yang CC, Smith BP. Results of acute arthroscopically repaired triangular fibrocartilage complex injuries associated with intra-articular distal radius fractures. Arthroscopy. 2003;19:511-516.
33. Whipple TL, Geissler WB. Arthroscopic management of wrist triangular fibrocartilage complex injuries in the athlete. Orthopedics. 1993;16:1061–1067.
34. Poehling GP, Chabon SJ, Siegel DB. Diagnostic and operative arthroscopy. In: Gelberman RH, ed. The Wrist: Master Techniques in Orthopedic Surgery. New York, NY: Raven Press, 1994:21–25.
35. del Piñal F, García-Bernal FJ, Cagigal L, Studer A, Regalado J, Thams C. A technique for arthroscopic all-inside suturing in the wrist. J Hand Surg Eur Vol. 2010;35:475–479.
36. Adams BD, Berger RA. An anatomic reconstruction of the distal radioulnar ligaments for posttraumatic distal radioulnar joint instability. J Hand Surg Am. 2002;27:243–251.
37. Sauvé L, Kapandji M. Nouvelle technique de traitement chirurgical des luxations recidivantes isolées de l’extrémité inferieure du cubitus. J Chir. 1936;47:589–594 [in French].
38. Luchetti R, Khanchandani P, Da Rin F, et al. Arthroscopically assisted Sauvé-Kapandji procedure: an advanced technique for distal radioulnar joint arthritis. Tech Hand Up Extrem Surg. 2008;12:216–220.
39. Laurentin-Perez LA, Goodwin AN, Babb BA, et al. A study of functional outcomes following implantation of a total distal radioulnar joint prosthesis. J Hand Surg Eur Vol. 2008;33:18–28.
40. Lo IKY, Burkhart SS. Double-row arthroscopic rotator cuff repair: re-establishing the footprint of the rotator cuff. Arthroscopy. 2003;19:1035–1042.
41. Kim SH, Ha KI. The SMC knot–a new slipknot with locking mechanism. Arthroscopy. 2000;16:563–565.
42. Atzei A, Rizzo A, Luchetti R, Fairplay T. Arthroscopic foveal repair of triangular fibrocartilage complex peripheral lesion with distal radioulnar joint instability. Tech Hand Up Extrem Surgery. 2008;12:226–235.
43. Garcia-Elias M, Smith DE, Llusa M. Surgical approach to the triangular fibrocartilage complex. Tech Hand Up Extrem Surg. 2003;7:134-140.
44. Chou KH, Sarris IK, Sotereanos DG. Suture anchor repair of ulnar-sided triangular fibrocartilage complex tears. J Hand Surg Br. 2003;28:546-550.
45. Hagert E. Wrist ligaments – innervation patterns and ligamento-muscular reflexes. [thesis for doctor degree (PhD)]. Stockholm: Karolinska Institutet; 2008.
46. Atzei A, Luchetti R, Borelli PP, Sgarbossa A, Cugola L. Arthroscopic TFCC reconstruction by tendon graft. Rivista di Chirurgia della Mano. 2006;43:370–376.
Wrist_Ch11.indd 129Wrist_Ch11.indd 129 27/03/13 7:47 PM27/03/13 7:47 PM

Ulnar-Sided Wrist Pain
130 American Society for Surgery of the Hand
Key Points• Consider the TFCC as an iceberg. With the scope in the 3-4 portal you are only looking at its tip. However, the
functionally most important part of the iceberg/TFCC is “submerged”: use the hook test and/or DRUJ arthroscopy to assess it.
• Assess DRUJ laxity/instability with the ballottement test also after anesthesia, which eliminates muscular protection.• Positive ballottement test and hook test suggest unstable TFCC tears.• Consider that TFCC repairability depends on tear size and on the viability of its margins.• Unstable TFCC tears require foveal refixation. The DF portal allows easy access to the fovea.• Optimal healing of the TFCC to the fovea requires: (1) strong suture material/device and (2) good bleeding opposing
surfaces. Always freshen TFCC margins and create a bleeding bony bed for TFCC fixation.• Repair the TFCC with a pair of sutures: it will reproduce a more anatomical tensioning of the DRUJ and UC ligaments
and provide a larger footprint for a faster and stronger healing.• Nonrepairable TFCC tears require tendon graft reconstruction of the DRUJ and UC ligaments. Passing the tendon graft
through the UC interval enhances ulnar carpus stability. • The complex and long-lasting reconstructive procedures benefit from the use of dry arthroscopy. • Arthroscopy improves accuracy of foveal positioning of the sutures or graft, which restores ligament isometricity and
allows earlier rehabilitation and better long-term results.
Wrist_Ch11.indd 130Wrist_Ch11.indd 130 27/03/13 7:47 PM27/03/13 7:47 PM

















