The Laryngoscope V C 2010 The American Laryngological, Rhinological and Otological Society, Inc. A Computational Study on the Characteristics of Airflow in Bilateral Abductor Vocal Fold Immobility M. Ku ¨ rs at Go ¨kcan, MD; D. Funda Kurtulus , PhD; Evren U ¨ stu ¨ner, MD; Elif O ¨ zyu ¨ rek, MD; G. Go ¨kc ¸en Kesici, MD; S. Ceyhan Erdem, BSc; Gu ¨rsel Dursun, MD; Cemil Yag ˘ci, MD Objectives/Hypothesis: To evaluate airway suf- ficiency and airflow dynamics in a group of patients who underwent a posterior transverse laser cordot- omy (PTLC) procedure. Study Design: Mixed methods research, univer- sity hospital setting. Methods: Sixteen patients who underwent a PTLC procedure volunteered to be involved in this study. Dyspnea levels, voice, and glottic opening in indirect laryngoscopy were evaluated subjectively. The airway was evaluated objectively by pulmonary function tests, and glottic areas were measured from axial computed tomography (CT) images. The control group consisted of 63 subjects from the tomography archive. For computational fluid dynamics (CFD) analyses, two subjects from the study group were cho- sen on the basis of obstruction level, and a normal female subject was selected from the control group. Cartesian coordinates for airway boundaries were determined from axial CT images, and a three-dimen- sional computational model of the larynx was con- structed. Flow simulations were performed with two different flow conditions during inspiration. Compari- son of velocity, static pressure, turbulence intensity, and wall shear stress distribution values were made between selected cases and control. Results: Pulmonary data varied widely and did not correlate with the size of the glottic area or dysp- nea level. CFD analyses revealed that in addition to obstruction at the glottic level, aerodynamic proper- ties of the larynx are altered due to loss in muscular tonus. Also, the contour of the glottic opening was found to be very important in determining the char- acter of airflow as laminar or turbulent. Conclusions: Patients have considerable differ- ences in their flow patterns and force distributions during respiration. Patient-specific models may help in evaluation and treatment planning. Key Words: Adult, cross-sectional studies, treatment outcome, vocal cord paralysis/ physiopathology, vocal cord paralysis/surgery, voice, computed tomography, computational fluid dynamics. Level of Evidence: 3b Laryngoscope, 120:1808–1818, 2010 INTRODUCTION In cases of bilateral abductor vocal fold immobility (BAVFI), forced inspiration draws vocal folds together and closes off the laryngeal inlet, which may cause severe airway obstruction and require emergency surgi- cal intervention. Tracheotomy was the only available treatment until the beginning of the 20th century. 1,2 Although it is still a highly effective method in relieving obstruction in BAVFI, the invasiveness of the procedure and long-term social problems necessitated development of new and more focused surgical techniques. A wide va- riety of surgical techniques have been developed to date to eliminate the need for tracheotomies with varying degrees of success. 1,2 Surgical procedures involving vocal folds often bring a trade-off between relieving airway obstruction and laryngeal functions such as phonation and deglutition. Therefore, the ideal surgical technique should provide an air passage to prevent vocal fold col- lapse during inspiration but should preserve phonation as much as possible. There are a variety of endoscopic procedures involv- ing the posterior glottis, such as laser arytenoidectomy, laser medial arytenoidectomy, posterior transverse cor- dotomy, or combined arytenoidectomy and cordotomy. 1 Posterior transverse laser cordotomy (PTLC) was first described by Dennis and Kashima 3 as a means of provid- ing an airway at the posterior part of the glottis. This procedure is widely accepted in the treatment of BAVFI From the Department of Otorhinolaryngology, Head and Neck Surgery (M.K.G., G.G.K., G.D.), Department of Radiology (E.U., E.O., C.Y.), Ankara University Medical School, and the Department of Aerospace Engineering (D.F .K., C.E.), Faculty of Engineering, Middle East Technical University, Ankara, Turkey. Editor’s Note: This Manuscript was accepted for publication April 19, 2010. The authors have no funding, financial relationships, or conflicts of interest to disclose. Send correspondence to M. Ku ¨ rs at Go ¨kcan, MD, Koza Sokak Ikizler Sitesi 72B/39, 06700 G.O.P., Ankara, Turkey. E-mail: [email protected]DOI: 10.1002/lary.21003 Laryngoscope 120: September 2010 Go ¨ kcan et al.: Characteristics of Airflow in BAVFI 1808
Transcript
The LaryngoscopeVC 2010 The American Laryngological,Rhinological and Otological Society, Inc.
A Computational Study on theCharacteristics of Airflow in BilateralAbductor Vocal Fold Immobility
M. Kurs�at Gokcan, MD; D. Funda Kurtulus�, PhD; Evren Ustuner, MD; Elif Ozyurek, MD;
G. Gokcen Kesici, MD; S. Ceyhan Erdem, BSc; Gursel Dursun, MD; Cemil Yagci, MD
Objectives/Hypothesis: To evaluate airway suf-ficiency and airflow dynamics in a group of patientswho underwent a posterior transverse laser cordot-omy (PTLC) procedure.
Study Design: Mixed methods research, univer-sity hospital setting.
Methods: Sixteen patients who underwent aPTLC procedure volunteered to be involved in thisstudy. Dyspnea levels, voice, and glottic opening inindirect laryngoscopy were evaluated subjectively.The airway was evaluated objectively by pulmonaryfunction tests, and glottic areas were measured fromaxial computed tomography (CT) images. The controlgroup consisted of 63 subjects from the tomographyarchive. For computational fluid dynamics (CFD)analyses, two subjects from the study group were cho-sen on the basis of obstruction level, and a normalfemale subject was selected from the control group.Cartesian coordinates for airway boundaries weredetermined from axial CT images, and a three-dimen-sional computational model of the larynx was con-structed. Flow simulations were performed with twodifferent flow conditions during inspiration. Compari-son of velocity, static pressure, turbulence intensity,and wall shear stress distribution values were madebetween selected cases and control.
Results: Pulmonary data varied widely and didnot correlate with the size of the glottic area or dysp-nea level. CFD analyses revealed that in addition toobstruction at the glottic level, aerodynamic proper-ties of the larynx are altered due to loss in muscular
tonus. Also, the contour of the glottic opening wasfound to be very important in determining the char-acter of airflow as laminar or turbulent.
Conclusions: Patients have considerable differ-ences in their flow patterns and force distributionsduring respiration. Patient-specific models may helpin evaluation and treatment planning.
Level of Evidence: 3bLaryngoscope, 120:1808–1818, 2010
INTRODUCTIONIn cases of bilateral abductor vocal fold immobility
(BAVFI), forced inspiration draws vocal folds togetherand closes off the laryngeal inlet, which may causesevere airway obstruction and require emergency surgi-cal intervention. Tracheotomy was the only availabletreatment until the beginning of the 20th century.1,2
Although it is still a highly effective method in relievingobstruction in BAVFI, the invasiveness of the procedureand long-term social problems necessitated developmentof new and more focused surgical techniques. A wide va-riety of surgical techniques have been developed to dateto eliminate the need for tracheotomies with varyingdegrees of success.1,2 Surgical procedures involving vocalfolds often bring a trade-off between relieving airwayobstruction and laryngeal functions such as phonationand deglutition. Therefore, the ideal surgical techniqueshould provide an air passage to prevent vocal fold col-lapse during inspiration but should preserve phonationas much as possible.
There are a variety of endoscopic procedures involv-ing the posterior glottis, such as laser arytenoidectomy,laser medial arytenoidectomy, posterior transverse cor-dotomy, or combined arytenoidectomy and cordotomy.1
Posterior transverse laser cordotomy (PTLC) was firstdescribed by Dennis and Kashima3 as a means of provid-ing an airway at the posterior part of the glottis. Thisprocedure is widely accepted in the treatment of BAVFI
From the Department of Otorhinolaryngology, Head and NeckSurgery (M.K.G., G.G.K., G.D.), Department of Radiology (E.U., E.O., C.Y.),Ankara University Medical School, and the Department of AerospaceEngineering (D.F.K., C.E.), Faculty of Engineering, Middle East TechnicalUniversity, Ankara, Turkey.
Editor’s Note: This Manuscript was accepted for publication April19, 2010.
The authors have no funding, financial relationships, or conflictsof interest to disclose.
Send correspondence to M. Kurs�at Gokcan, MD, Koza SokakIkizler Sitesi 72B/39, 06700 G.O.P., Ankara, Turkey.E-mail: [email protected]
DOI: 10.1002/lary.21003
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI
1808
because it is minimally invasive and can be applied inemergency cases; therefore, the requirement for trache-otomy could be reduced.2 Effectiveness of the procedurehas been evaluated in terms of laryngoscopic findings,decannulation rates, aerodynamic parameters (pulmo-nary function tests and/or body plethysmography),subjective dyspnea indices, or quality-of-life question-naires.1–5 However, there are certain questions that stillneed to be answered: 1) How much tissue should bevaporized or resected in the posterior glottis? Consider-ing that the healing tissue scars over the surgical areawith time, what is the proportion of provided glottic areawhen compared with the normal larynx in the longterm? 2) What are the physiologic and aerodynamicproperties of this new airway? How efficient is the proce-dure in meeting the patient’s demands on forcedinspiration?
Thus, we designed a case-control study in a groupof BAVFI patients who were treated with PTLC to findout the answers to some of these questions. There weretwo main objectives in this study. The first was to evalu-ate the long-term results of PTLC using objective andsubjective measures of breathing and voice quality. Thesecond was to create a realistic model of an airway afterthe PTLC procedure and to simulate a forced respirationto determine the efficiency of the procedure in the longterm.
MATERIALS AND METHODS
Study and Control GroupsThe study protocol was approved by the ethics committee
of Ankara University Medical School. The hospital records data-base search yielded 65 adult patients who were diagnosed withBAVFI (with history, laryngoscopy with or without laryngealelectromyography) and underwent PTLC between 1998 and2007. Patients were reached by phone, and 16 patients (15female, 1 male) who were nonsmokers and otherwise healthyvolunteered to participate in this study and provided theirsigned informed consent.
The control group consisted of 63 subjects from the tomog-raphy archive who underwent multidetector computedtomography (MDCT) imaging of the neck for other reasonsbetween January 2008 and April 2009. Studies mostly includedcomputed tomography (CT) angiography or neck vertebrateimaging CTs; subjects who had any pathology involving, neigh-boring, or affecting the airway were not included. Also, studieswith motion artifacts induced by involuntary movements associ-
ated with deglutition, respiration, and throat clearing were notincluded.
As there was only one male case in study group, male sub-jects were excluded from both study and control groups, andstatistical analyses were carried out with 15 study and 38 con-trol female subjects.
Airway AssessmentThe study group was evaluated with videolaryngostrobo-
scopy using a 90� rigid telescope (model 8707DJ; Storz,Tuttlingen, Germany) for subjective evaluation of the airwayand vocal folds. Patients were asked to grade their dyspnealevel and compare it with preoperative status according to afive-level subjective dyspnea scale that classifies dyspnea inrelation to the limitation in daily activity and to the level of re-spiratory difficulty (Table I). Phonation quality was evaluatedsubjectively with a standard Turkish text (the equivalent of theRainbow Passage).
Pulmonary function tests (PFTs) were performed by a sin-gle operator using a spirometer device (Sensormedics; VIASYSHealthcare Inc., San Diego, CA). Full calibration and verifica-tion of equipment was carried out prior to each set of tests. Thevalues for forced vital capacity (FVC), forced expiratory volumeat 1 second (FEV1), FEV1/FVC ratio, and peak expiratory flowrate (PEF) of patients were measured, and percentage ofexpected values for these parameters were calculated accordingto sex, age, and height.
For objective evaluation of the airway, MDCT scans of thewhole airway from nasopharynx to thoracic inlet were obtainedfrom study group with a 64-channel CT scanner (Aquilion 64;Toshiba Medical Systems, Tokyo, Japan), which enables acquisi-tion of 64 simultaneous slices of 0.5 mm—the thinnestavailable—with a rotation time of 0.5 seconds. Imaging was per-formed without administration of intravenous contrast materialwhile patients were in a supine position during normal calm in-spiration with the following parameters: 120 kV, 100 mAs, 64 �0.5 mm collimation, reconstruction interval of 0.5 mm, helicalpitch of 53, pitch factor of 0.83, and 512 � 512 pixels matrix.Axial images were screened by radiologists (C.Y., E.U., E.O.) forany airway pathology that might obscure PFT or airway analy-ses. Acquired images in axial sections were then transferredinto a workstation that uses the manufacturer’s supplied soft-ware (Vitrea 4.0; Vital Images Inc., Minnetonka, MN) andstored in digital imaging and communication in medicineformat.
The MDCT images of both groups were processed withimage processor software (Vitrea 4.0) to obtain multiplanarreformats and virtual endoscopy of the airway. The area of theglottis was measured from the axial slices, passing through thevocal folds, using imaging software. Axial and virtual laryngos-copy images of the widest glottic opening were stored.
Computational Fluid Dynamics AnalysesTo analyze the efficiency of the PTLC procedure, two sub-
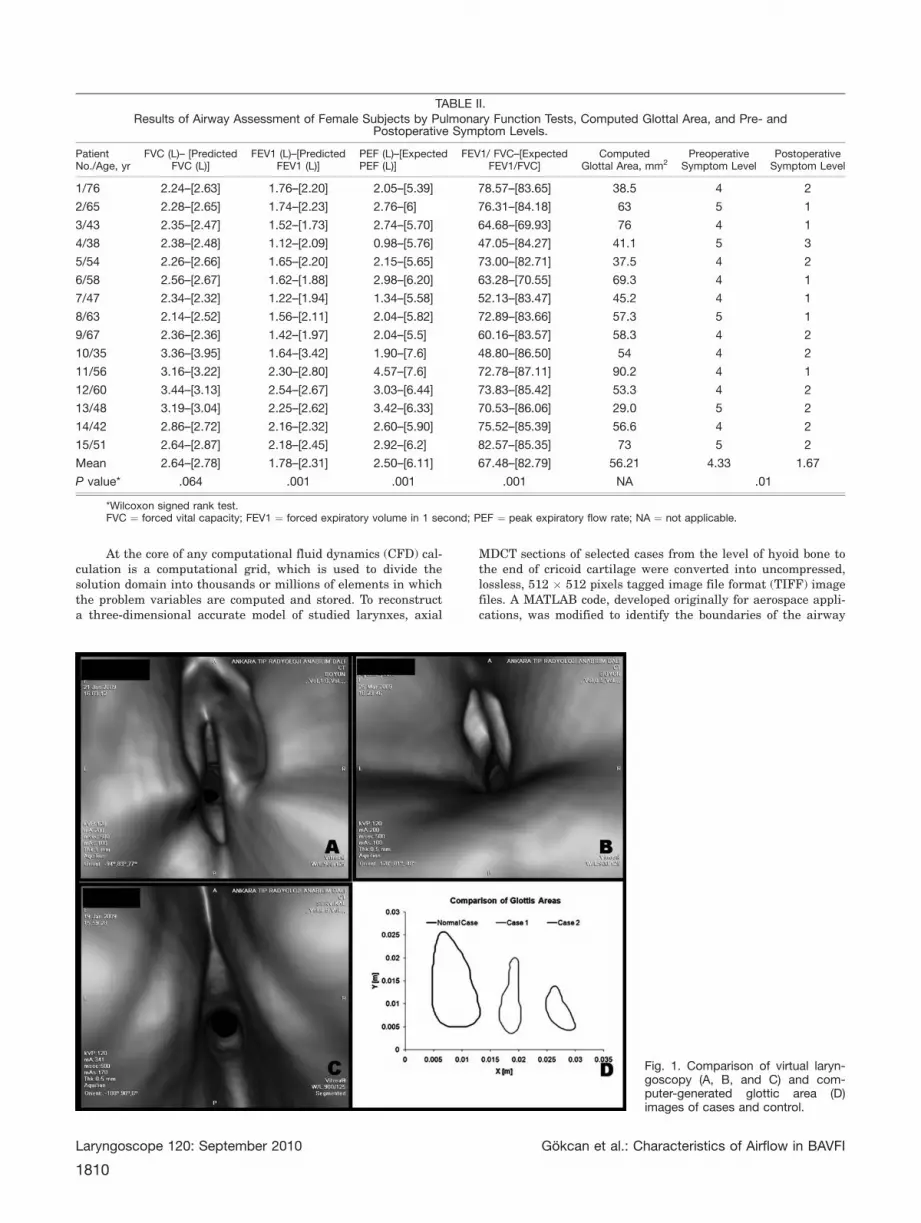
jects from the study group were chosen on the basis ofobstruction level in PFT and measured glottic area. Subject 4(case 1) had the worst FEV1/FVC and PEF values (47.05 and0.98 L, respectively) for provided glottic area (41.1 mm2), andsubject 13 (case 2) had the best of those values (70.53 and 3.42L, respectively) for provided glottic area (29 mm2) (Table II). Anormal female subject (control) with a glottic area of 125 mm2
was selected from the control group. Figure 1 shows virtual lar-yngoscopy and computer generated glottic area images of casesand control.
TABLE I.Five-Level Symptom Scale for Severity of Dyspnea.
Severity Score
None 1 No symptoms
Mild 2 Dyspnea with no limitationsin daily activity
Moderate 3 Dyspnea with mild limitations indaily activity, no stridor
Severe 4 Dyspnea with significant limitationsin daily activity, with stridor
Very severe 5 Respiratory difficulty requiringtracheotomy
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI
1809
At the core of any computational fluid dynamics (CFD) cal-culation is a computational grid, which is used to divide thesolution domain into thousands or millions of elements in whichthe problem variables are computed and stored. To reconstructa three-dimensional accurate model of studied larynxes, axial
MDCT sections of selected cases from the level of hyoid bone tothe end of cricoid cartilage were converted into uncompressed,lossless, 512 � 512 pixels tagged image file format (TIFF) imagefiles. A MATLAB code, developed originally for aerospace appli-cations, was modified to identify the boundaries of the airway
TABLE II.Results of Airway Assessment of Female Subjects by Pulmonary Function Tests, Computed Glottal Area, and Pre- and
Mean 2.64–[2.78] 1.78–[2.31] 2.50–[6.11] 67.48–[82.79] 56.21 4.33 1.67
P value* .064 .001 .001 .001 NA .01
*Wilcoxon signed rank test.FVC ¼ forced vital capacity; FEV1 ¼ forced expiratory volume in 1 second; PEF ¼ peak expiratory flow rate; NA ¼ not applicable.
Fig. 1. Comparison of virtual laryn-goscopy (A, B, and C) and com-puter-generated glottic area (D)images of cases and control.
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI
1810
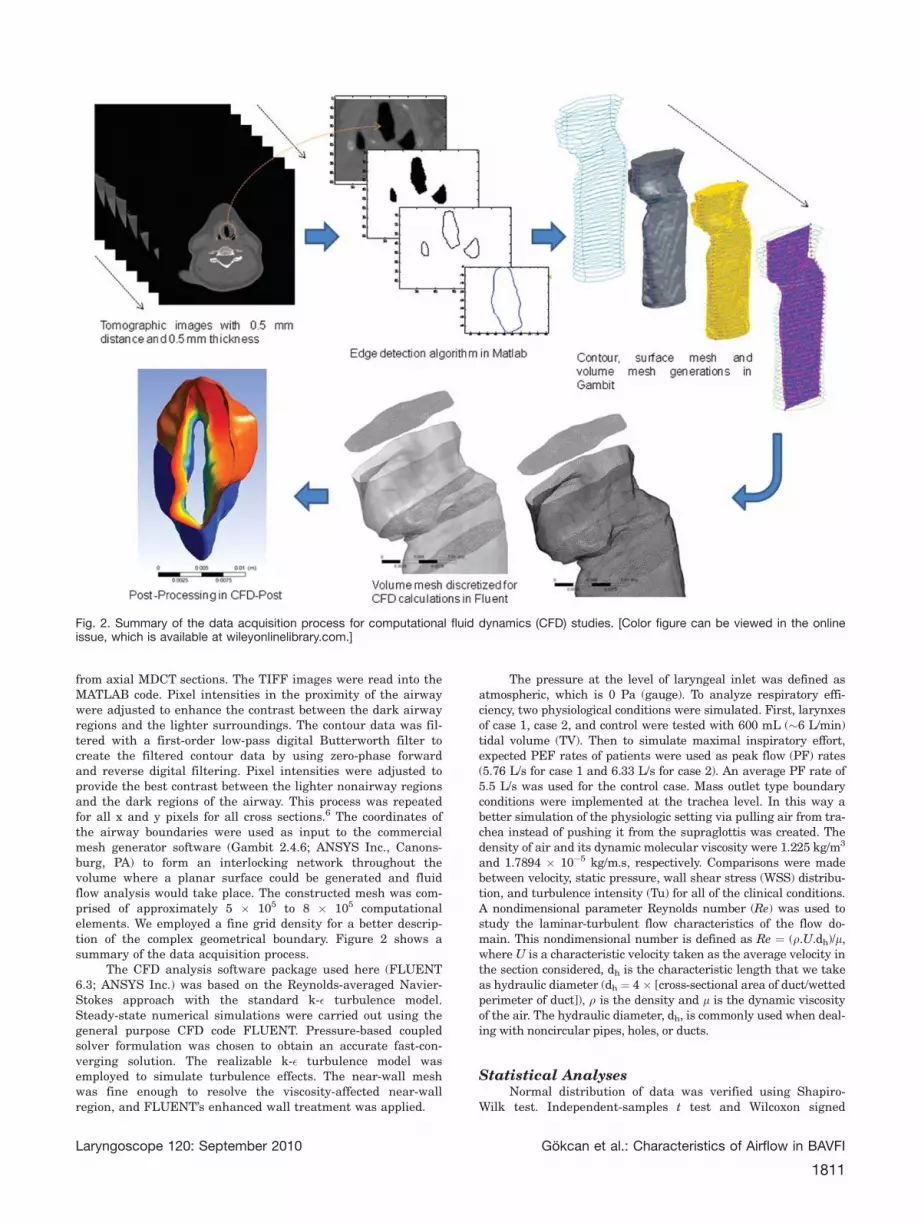
from axial MDCT sections. The TIFF images were read into theMATLAB code. Pixel intensities in the proximity of the airwaywere adjusted to enhance the contrast between the dark airwayregions and the lighter surroundings. The contour data was fil-tered with a first-order low-pass digital Butterworth filter tocreate the filtered contour data by using zero-phase forwardand reverse digital filtering. Pixel intensities were adjusted toprovide the best contrast between the lighter nonairway regionsand the dark regions of the airway. This process was repeatedfor all x and y pixels for all cross sections.6 The coordinates ofthe airway boundaries were used as input to the commercialmesh generator software (Gambit 2.4.6; ANSYS Inc., Canons-burg, PA) to form an interlocking network throughout thevolume where a planar surface could be generated and fluidflow analysis would take place. The constructed mesh was com-prised of approximately 5 � 105 to 8 � 105 computationalelements. We employed a fine grid density for a better descrip-tion of the complex geometrical boundary. Figure 2 shows asummary of the data acquisition process.
The CFD analysis software package used here (FLUENT6.3; ANSYS Inc.) was based on the Reynolds-averaged Navier-Stokes approach with the standard k-� turbulence model.Steady-state numerical simulations were carried out using thegeneral purpose CFD code FLUENT. Pressure-based coupledsolver formulation was chosen to obtain an accurate fast-con-verging solution. The realizable k-� turbulence model wasemployed to simulate turbulence effects. The near-wall meshwas fine enough to resolve the viscosity-affected near-wallregion, and FLUENT’s enhanced wall treatment was applied.
The pressure at the level of laryngeal inlet was defined asatmospheric, which is 0 Pa (gauge). To analyze respiratory effi-ciency, two physiological conditions were simulated. First, larynxesof case 1, case 2, and control were tested with 600 mL (�6 L/min)tidal volume (TV). Then to simulate maximal inspiratory effort,expected PEF rates of patients were used as peak flow (PF) rates(5.76 L/s for case 1 and 6.33 L/s for case 2). An average PF rate of5.5 L/s was used for the control case. Mass outlet type boundaryconditions were implemented at the trachea level. In this way abetter simulation of the physiologic setting via pulling air from tra-chea instead of pushing it from the supraglottis was created. Thedensity of air and its dynamic molecular viscosity were 1.225 kg/m3
and 1.7894 � 10�5 kg/m.s, respectively. Comparisons were madebetween velocity, static pressure, wall shear stress (WSS) distribu-tion, and turbulence intensity (Tu) for all of the clinical conditions.A nondimensional parameter Reynolds number (Re) was used tostudy the laminar-turbulent flow characteristics of the flow do-main. This nondimensional number is defined as Re ¼ (q.U.dh)/l,where U is a characteristic velocity taken as the average velocity inthe section considered, dh is the characteristic length that we takeas hydraulic diameter (dh ¼ 4 � [cross-sectional area of duct/wettedperimeter of duct]), q is the density and l is the dynamic viscosityof the air. The hydraulic diameter, dh, is commonly used when deal-ing with noncircular pipes, holes, or ducts.
Statistical AnalysesNormal distribution of data was verified using Shapiro-
Wilk test. Independent-samples t test and Wilcoxon signed
Fig. 2. Summary of the data acquisition process for computational fluid dynamics (CFD) studies. [Color figure can be viewed in the onlineissue, which is available at wileyonlinelibrary.com.]
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI
1811
ranks test were conducted to compare means of the glottic areameasurements, pulmonary function tests, and symptom scores.Pearson coefficient and Spearman tests were used for correla-tion analysis. Analyzes were carried out using a commercialsoftware (Statistical Package for Social Sciences, version 15;SPSS Inc., Chicago, IL).
RESULTSThis study included 15 female BAVFI patients aged
between 35 and 76 years (mean, 53.5 years) and 38female control subject aged between 22 and 85 years(mean, 51.3 years). An overview of patient characteris-tics and previous interventions were given in Table III.The etiologies of BAVFI included recurrent laryngealnerve paralysis after thyroidectomy in the majority ofpatients (13 patients), development of bilateral cricoary-tenoid joint immobility after intubation in one patient,and the etiology of BAVFI was unknown in one patient.All patients were treated with unilateral (7/16) or bilat-eral (8/16) PTLC. Details of the procedure weredescribed previously.2
glottic airway in all patients; there were no granulomasor adhesions renarrowing the airway. There were mini-mal vocal fold movements in six patients with nosignificant abduction during respiration. Residual muco-sal waves could be seen in the remaining vocal foldsduring phonation.
The functional result of the operation was deemed asuccess if a stable airway was achieved with acceptablevoice quality and no aspiration. Successful results wereobtained at the first trial in 73.3% of patients (11/15) fol-lowing PTLC (Table III). Four patients needed revisionendoscopic laser procedures due to excess granulation
tissue formation. Aspiration was not encountered; allpatients resumed normal swallowing after their opera-tion. Neither pain (requiring narcotic analgesics) norinfection ensued as a complication in the postoperativeperiod. All patients experienced significant hoarsenessin immediate postoperative period; however, changes inthe patients’ quality of speech reached an acceptablelevel within 4 to 5 postoperative months.
Patients had significant dyspnea with limitation indaily activity and/or required tracheotomy (level 4 or 5)before the procedure (Table III). After the procedure,some patients experienced varying degrees of dyspneaduring moderate physical activity or required revisionendoscopic procedures, but none required tracheotomy inthe peri- or postoperative period, and five patients whohad a tracheotomy before the procedure were decannu-lated in the long term.
Computation of the glottic area (GA) during calmrespiration was carried out using MDCT image proces-sor. The mean GA of the study group (56.21 6 4.24 mm2
[range, 29.0–90.20 mm2]) was significantly lower thanthe mean of the control group (95.4 6 5.23 mm2 [range45.60–172.50 mm2 ]) (t ¼ �5.57, P < .001) (Fig. 3).
An overview of PFTs in the study group is given inTable II. Patients showed varying degrees of obstructivepathology. The vital capacity of patients was within nor-mal range of their expected height and age. Flow rates(PEF and FEV1) were significantly lower than expectedvalues (P < .001). The value of the FEV1/FVC rate was81.5% of expected mean and was significantly correlatedwith PEF rates (r ¼ 0.59; P ¼ .017). No significant corre-lation was found between PFTs and GAs in this series.
CFD AnalysesCross-sectional average values of velocity magni-
TABLE III.Overview of Patient Characteristics and Previous Interventions.
Subject Age, yr Etiology Tracheotomy PTLC Revision
1 76 Thyroidectomy � Right Yes
2 65 Thyroidectomy þ Bilateral No
3 43 Thyroidectomy � Bilateral No
4 38 Thyroidectomy þ Left No
5 54 Thyroidectomy � Right No
6 58 Unknown � Bilateral No
7 47 Thyroidectomy � Bilateral No
8 63 Thyroidectomy þ Right No
9 67 Thyroidectomy � Bilateral Yes
10 35 Thyroidectomy � Left No
11 56 Thyroidectomy � Bilateral Yes, twice
12 60 Thyroidectomy � Bilateral Yes
13 48 Thyroidectomy þ Left No
14 42 Postintubation ankylosis � Bilateral No
15 51 Thyroidectomy þ Left No
PTLC ¼ posterior transverse laser cordotomy.
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI
1812
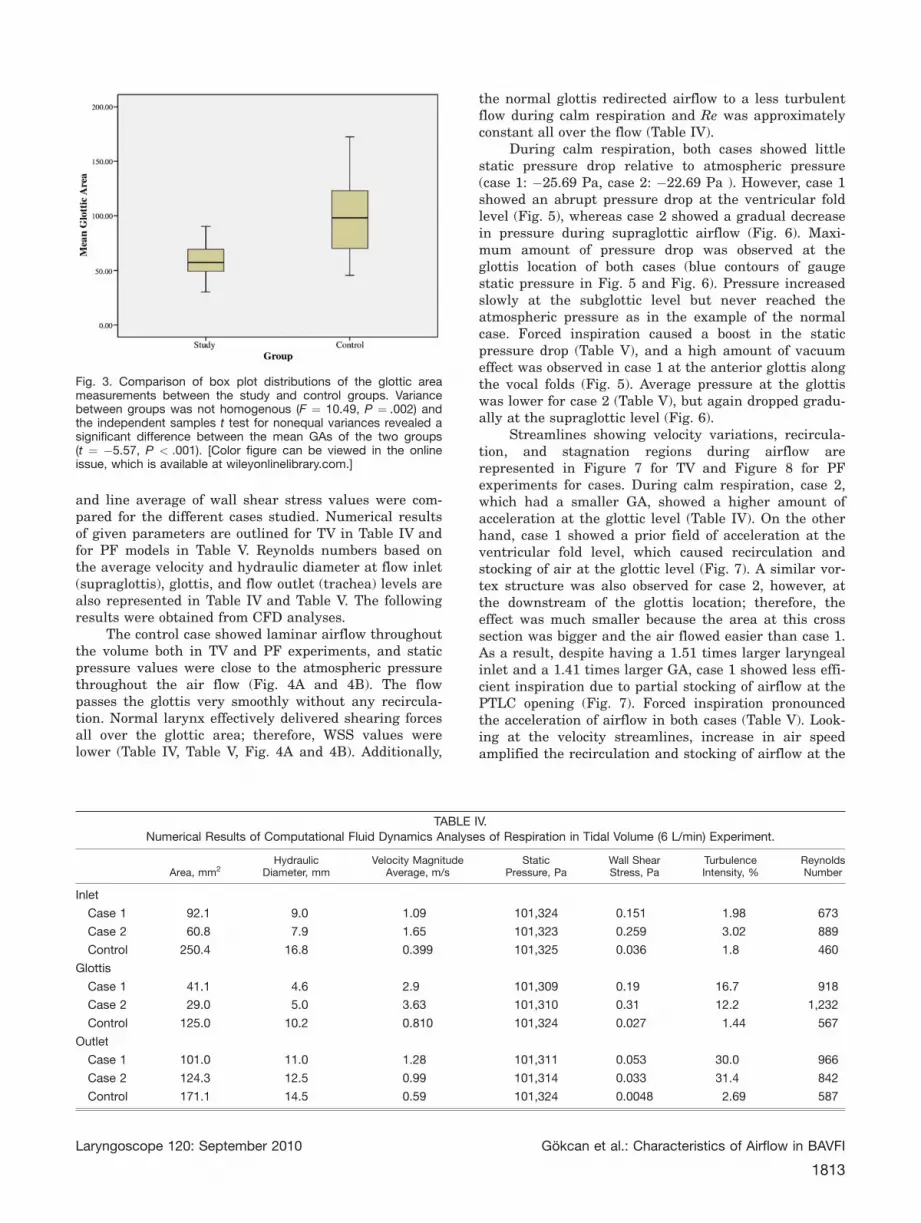
and line average of wall shear stress values were com-pared for the different cases studied. Numerical resultsof given parameters are outlined for TV in Table IV andfor PF models in Table V. Reynolds numbers based onthe average velocity and hydraulic diameter at flow inlet(supraglottis), glottis, and flow outlet (trachea) levels arealso represented in Table IV and Table V. The followingresults were obtained from CFD analyses.
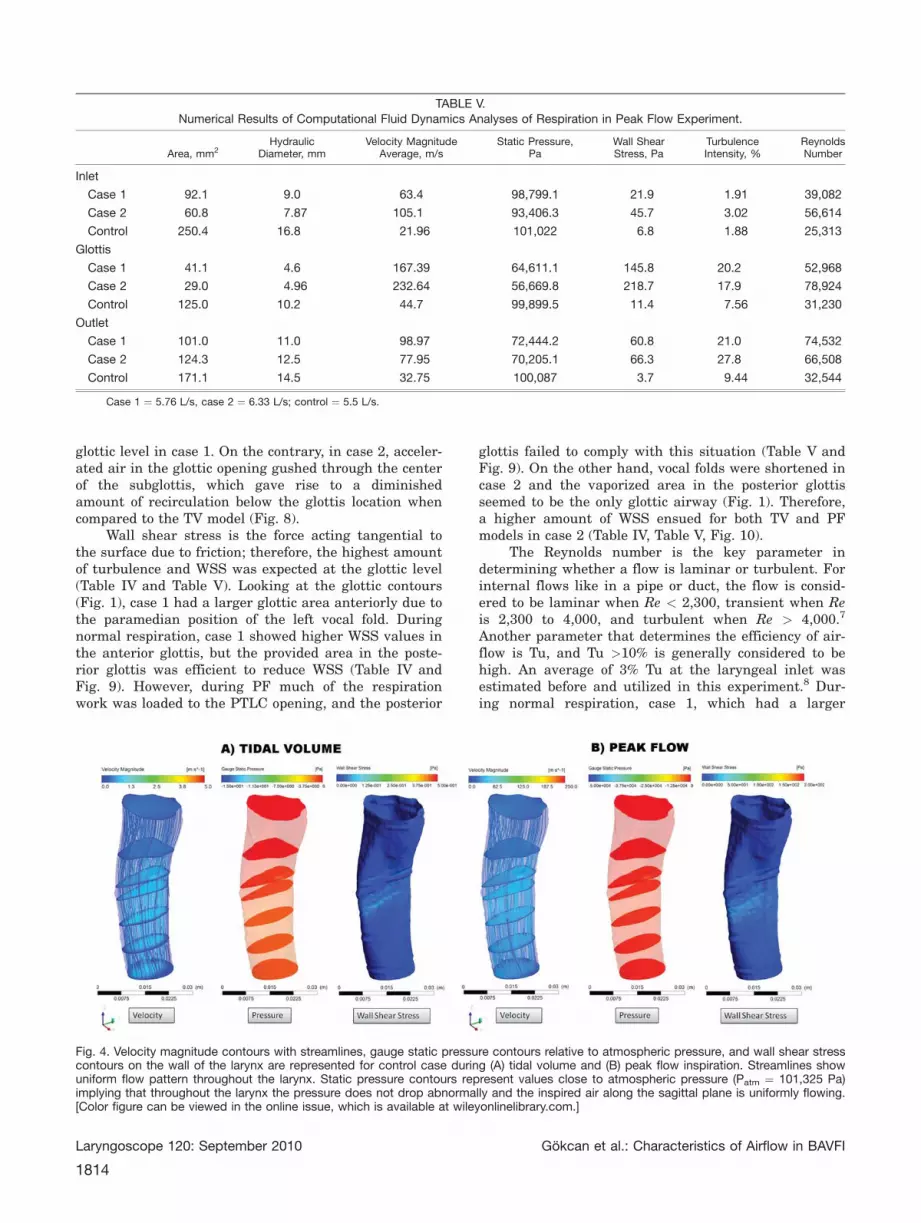
The control case showed laminar airflow throughoutthe volume both in TV and PF experiments, and staticpressure values were close to the atmospheric pressurethroughout the air flow (Fig. 4A and 4B). The flowpasses the glottis very smoothly without any recircula-tion. Normal larynx effectively delivered shearing forcesall over the glottic area; therefore, WSS values werelower (Table IV, Table V, Fig. 4A and 4B). Additionally,
the normal glottis redirected airflow to a less turbulentflow during calm respiration and Re was approximatelyconstant all over the flow (Table IV).
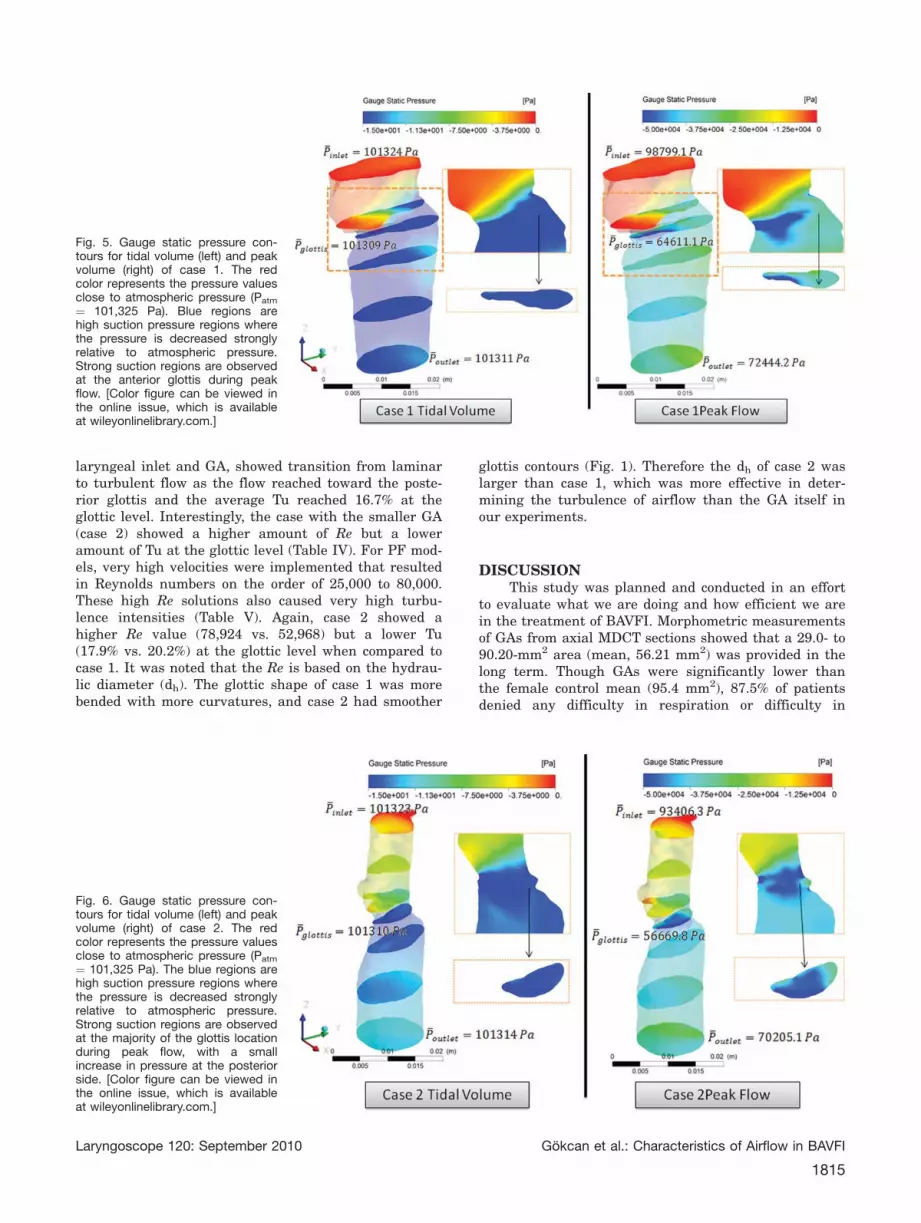
During calm respiration, both cases showed littlestatic pressure drop relative to atmospheric pressure(case 1: �25.69 Pa, case 2: �22.69 Pa ). However, case 1showed an abrupt pressure drop at the ventricular foldlevel (Fig. 5), whereas case 2 showed a gradual decreasein pressure during supraglottic airflow (Fig. 6). Maxi-mum amount of pressure drop was observed at theglottis location of both cases (blue contours of gaugestatic pressure in Fig. 5 and Fig. 6). Pressure increasedslowly at the subglottic level but never reached theatmospheric pressure as in the example of the normalcase. Forced inspiration caused a boost in the staticpressure drop (Table V), and a high amount of vacuumeffect was observed in case 1 at the anterior glottis alongthe vocal folds (Fig. 5). Average pressure at the glottiswas lower for case 2 (Table V), but again dropped gradu-ally at the supraglottic level (Fig. 6).
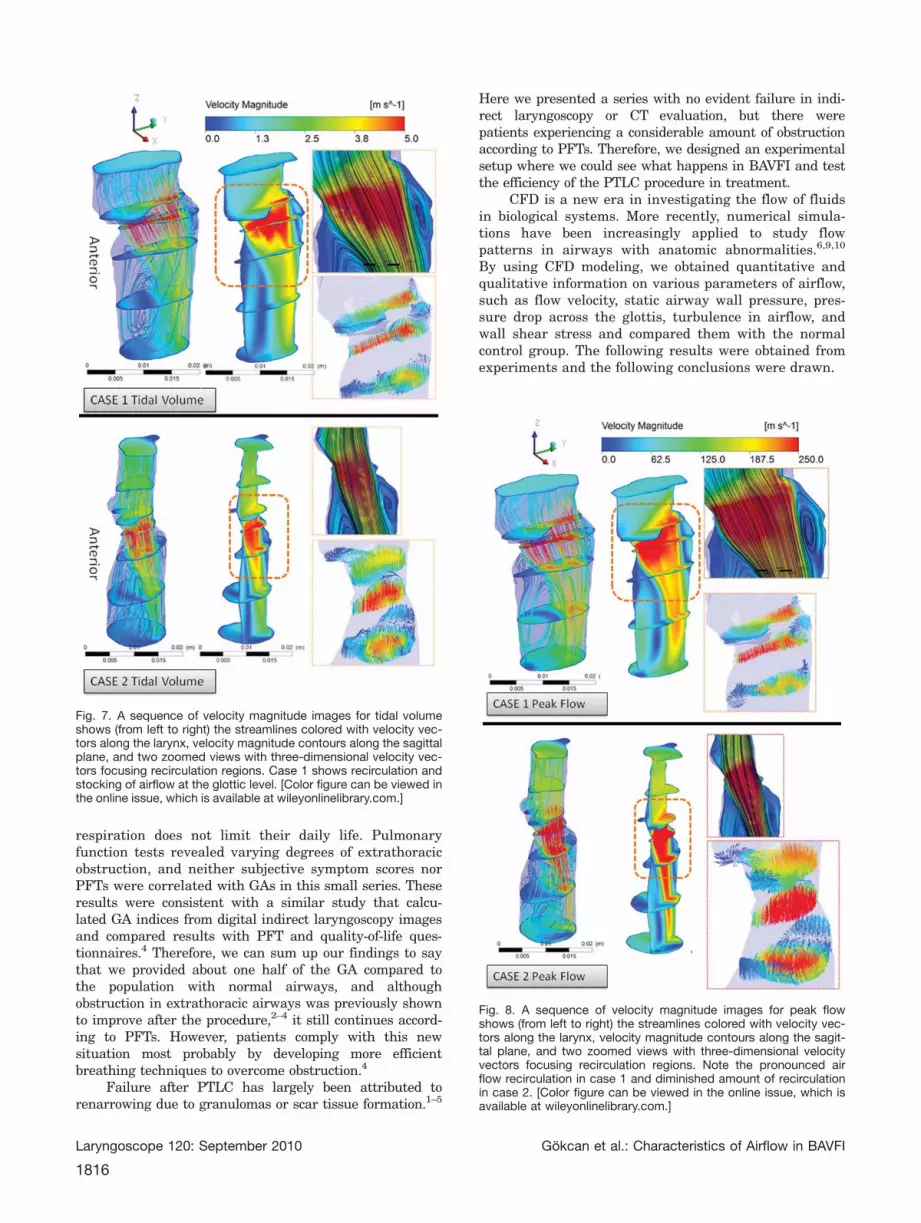
Streamlines showing velocity variations, recircula-tion, and stagnation regions during airflow arerepresented in Figure 7 for TV and Figure 8 for PFexperiments for cases. During calm respiration, case 2,which had a smaller GA, showed a higher amount ofacceleration at the glottic level (Table IV). On the otherhand, case 1 showed a prior field of acceleration at theventricular fold level, which caused recirculation andstocking of air at the glottic level (Fig. 7). A similar vor-tex structure was also observed for case 2, however, atthe downstream of the glottis location; therefore, theeffect was much smaller because the area at this crosssection was bigger and the air flowed easier than case 1.As a result, despite having a 1.51 times larger laryngealinlet and a 1.41 times larger GA, case 1 showed less effi-cient inspiration due to partial stocking of airflow at thePTLC opening (Fig. 7). Forced inspiration pronouncedthe acceleration of airflow in both cases (Table V). Look-ing at the velocity streamlines, increase in air speedamplified the recirculation and stocking of airflow at the
Fig. 3. Comparison of box plot distributions of the glottic areameasurements between the study and control groups. Variancebetween groups was not homogenous (F ¼ 10.49, P ¼ .002) andthe independent samples t test for nonequal variances revealed asignificant difference between the mean GAs of the two groups(t ¼ �5.57, P < .001). [Color figure can be viewed in the onlineissue, which is available at wileyonlinelibrary.com.]
TABLE IV.Numerical Results of Computational Fluid Dynamics Analyses of Respiration in Tidal Volume (6 L/min) Experiment.
Area, mm2Hydraulic
Diameter, mmVelocity Magnitude
Average, m/sStatic
Pressure, PaWall ShearStress, Pa
TurbulenceIntensity, %
ReynoldsNumber
Inlet
Case 1 92.1 9.0 1.09 101,324 0.151 1.98 673
Case 2 60.8 7.9 1.65 101,323 0.259 3.02 889
Control 250.4 16.8 0.399 101,325 0.036 1.8 460
Glottis
Case 1 41.1 4.6 2.9 101,309 0.19 16.7 918
Case 2 29.0 5.0 3.63 101,310 0.31 12.2 1,232
Control 125.0 10.2 0.810 101,324 0.027 1.44 567
Outlet
Case 1 101.0 11.0 1.28 101,311 0.053 30.0 966
Case 2 124.3 12.5 0.99 101,314 0.033 31.4 842
Control 171.1 14.5 0.59 101,324 0.0048 2.69 587
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI
1813
glottic level in case 1. On the contrary, in case 2, acceler-ated air in the glottic opening gushed through the centerof the subglottis, which gave rise to a diminishedamount of recirculation below the glottis location whencompared to the TV model (Fig. 8).
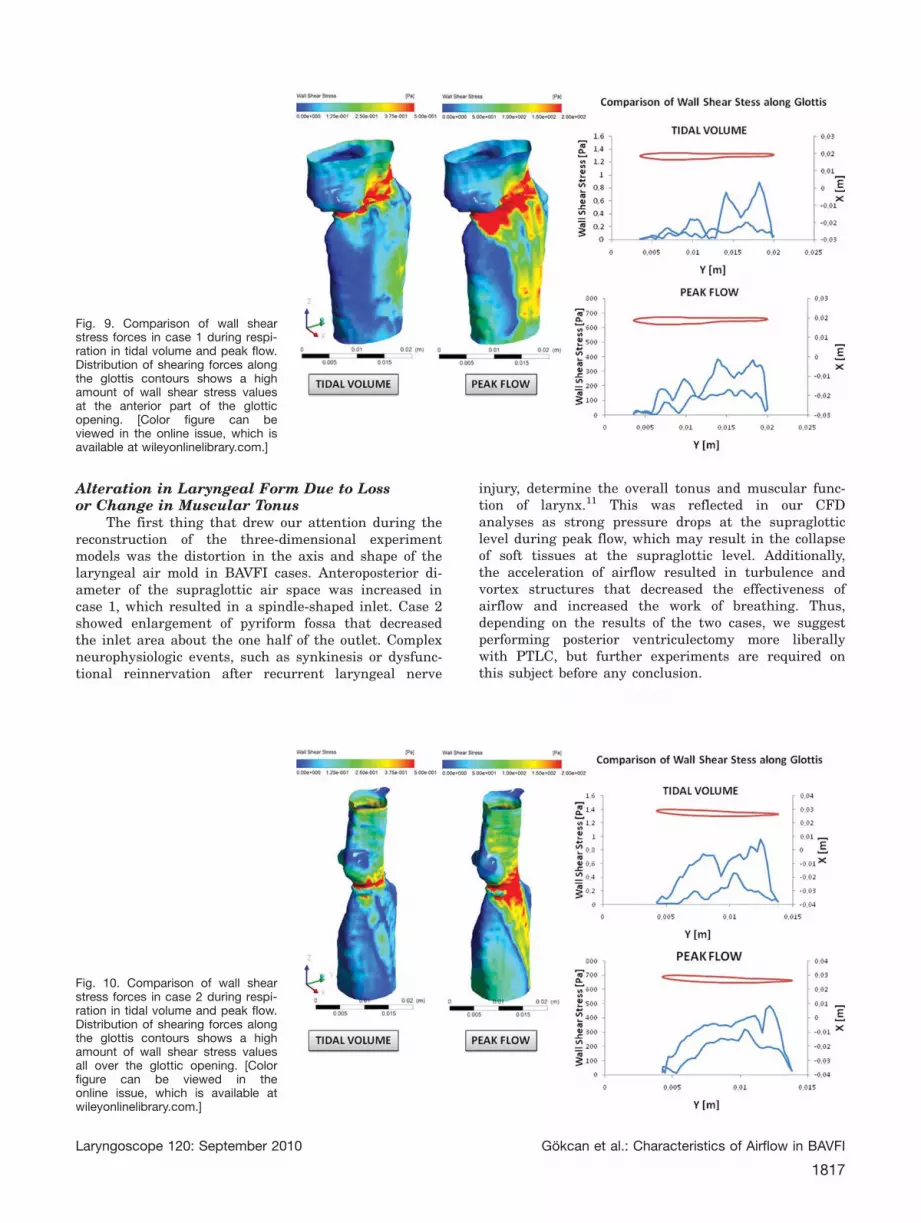
Wall shear stress is the force acting tangential tothe surface due to friction; therefore, the highest amountof turbulence and WSS was expected at the glottic level(Table IV and Table V). Looking at the glottic contours(Fig. 1), case 1 had a larger glottic area anteriorly due tothe paramedian position of the left vocal fold. Duringnormal respiration, case 1 showed higher WSS values inthe anterior glottis, but the provided area in the poste-rior glottis was efficient to reduce WSS (Table IV andFig. 9). However, during PF much of the respirationwork was loaded to the PTLC opening, and the posterior
glottis failed to comply with this situation (Table V andFig. 9). On the other hand, vocal folds were shortened incase 2 and the vaporized area in the posterior glottisseemed to be the only glottic airway (Fig. 1). Therefore,a higher amount of WSS ensued for both TV and PFmodels in case 2 (Table IV, Table V, Fig. 10).
The Reynolds number is the key parameter indetermining whether a flow is laminar or turbulent. Forinternal flows like in a pipe or duct, the flow is consid-ered to be laminar when Re < 2,300, transient when Reis 2,300 to 4,000, and turbulent when Re > 4,000.7
Another parameter that determines the efficiency of air-flow is Tu, and Tu >10% is generally considered to behigh. An average of 3% Tu at the laryngeal inlet wasestimated before and utilized in this experiment.8 Dur-ing normal respiration, case 1, which had a larger
TABLE V.Numerical Results of Computational Fluid Dynamics Analyses of Respiration in Peak Flow Experiment.
Area, mm2Hydraulic
Diameter, mmVelocity Magnitude
Average, m/sStatic Pressure,
PaWall ShearStress, Pa
TurbulenceIntensity, %
ReynoldsNumber
Inlet
Case 1 92.1 9.0 63.4 98,799.1 21.9 1.91 39,082
Case 2 60.8 7.87 105.1 93,406.3 45.7 3.02 56,614
Control 250.4 16.8 21.96 101,022 6.8 1.88 25,313
Glottis
Case 1 41.1 4.6 167.39 64,611.1 145.8 20.2 52,968
Case 2 29.0 4.96 232.64 56,669.8 218.7 17.9 78,924
Control 125.0 10.2 44.7 99,899.5 11.4 7.56 31,230
Outlet
Case 1 101.0 11.0 98.97 72,444.2 60.8 21.0 74,532
Case 2 124.3 12.5 77.95 70,205.1 66.3 27.8 66,508
Control 171.1 14.5 32.75 100,087 3.7 9.44 32,544
Case 1 ¼ 5.76 L/s, case 2 ¼ 6.33 L/s; control ¼ 5.5 L/s.
Fig. 4. Velocity magnitude contours with streamlines, gauge static pressure contours relative to atmospheric pressure, and wall shear stresscontours on the wall of the larynx are represented for control case during (A) tidal volume and (B) peak flow inspiration. Streamlines showuniform flow pattern throughout the larynx. Static pressure contours represent values close to atmospheric pressure (Patm ¼ 101,325 Pa)implying that throughout the larynx the pressure does not drop abnormally and the inspired air along the sagittal plane is uniformly flowing.[Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI
1814
laryngeal inlet and GA, showed transition from laminarto turbulent flow as the flow reached toward the poste-rior glottis and the average Tu reached 16.7% at theglottic level. Interestingly, the case with the smaller GA(case 2) showed a higher amount of Re but a loweramount of Tu at the glottic level (Table IV). For PF mod-els, very high velocities were implemented that resultedin Reynolds numbers on the order of 25,000 to 80,000.These high Re solutions also caused very high turbu-lence intensities (Table V). Again, case 2 showed ahigher Re value (78,924 vs. 52,968) but a lower Tu(17.9% vs. 20.2%) at the glottic level when compared tocase 1. It was noted that the Re is based on the hydrau-lic diameter (dh). The glottic shape of case 1 was morebended with more curvatures, and case 2 had smoother
glottis contours (Fig. 1). Therefore the dh of case 2 waslarger than case 1, which was more effective in deter-mining the turbulence of airflow than the GA itself inour experiments.
DISCUSSIONThis study was planned and conducted in an effort
to evaluate what we are doing and how efficient we arein the treatment of BAVFI. Morphometric measurementsof GAs from axial MDCT sections showed that a 29.0- to90.20-mm2 area (mean, 56.21 mm2) was provided in thelong term. Though GAs were significantly lower thanthe female control mean (95.4 mm2), 87.5% of patientsdenied any difficulty in respiration or difficulty in
Fig. 5. Gauge static pressure con-tours for tidal volume (left) and peakvolume (right) of case 1. The redcolor represents the pressure valuesclose to atmospheric pressure (Patm
¼ 101,325 Pa). Blue regions arehigh suction pressure regions wherethe pressure is decreased stronglyrelative to atmospheric pressure.Strong suction regions are observedat the anterior glottis during peakflow. [Color figure can be viewed inthe online issue, which is availableat wileyonlinelibrary.com.]
Fig. 6. Gauge static pressure con-tours for tidal volume (left) and peakvolume (right) of case 2. The redcolor represents the pressure valuesclose to atmospheric pressure (Patm
¼ 101,325 Pa). The blue regions arehigh suction pressure regions wherethe pressure is decreased stronglyrelative to atmospheric pressure.Strong suction regions are observedat the majority of the glottis locationduring peak flow, with a smallincrease in pressure at the posteriorside. [Color figure can be viewed inthe online issue, which is availableat wileyonlinelibrary.com.]
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI
1815
respiration does not limit their daily life. Pulmonaryfunction tests revealed varying degrees of extrathoracicobstruction, and neither subjective symptom scores norPFTs were correlated with GAs in this small series. Theseresults were consistent with a similar study that calcu-lated GA indices from digital indirect laryngoscopy imagesand compared results with PFT and quality-of-life ques-tionnaires.4 Therefore, we can sum up our findings to saythat we provided about one half of the GA compared tothe population with normal airways, and althoughobstruction in extrathoracic airways was previously shownto improve after the procedure,2–4 it still continues accord-ing to PFTs. However, patients comply with this newsituation most probably by developing more efficientbreathing techniques to overcome obstruction.4
Failure after PTLC has largely been attributed torenarrowing due to granulomas or scar tissue formation.1–5
Here we presented a series with no evident failure in indi-rect laryngoscopy or CT evaluation, but there werepatients experiencing a considerable amount of obstructionaccording to PFTs. Therefore, we designed an experimentalsetup where we could see what happens in BAVFI and testthe efficiency of the PTLC procedure in treatment.
CFD is a new era in investigating the flow of fluidsin biological systems. More recently, numerical simula-tions have been increasingly applied to study flowpatterns in airways with anatomic abnormalities.6,9,10
By using CFD modeling, we obtained quantitative andqualitative information on various parameters of airflow,such as flow velocity, static airway wall pressure, pres-sure drop across the glottis, turbulence in airflow, andwall shear stress and compared them with the normalcontrol group. The following results were obtained fromexperiments and the following conclusions were drawn.
Fig. 7. A sequence of velocity magnitude images for tidal volumeshows (from left to right) the streamlines colored with velocity vec-tors along the larynx, velocity magnitude contours along the sagittalplane, and two zoomed views with three-dimensional velocity vec-tors focusing recirculation regions. Case 1 shows recirculation andstocking of airflow at the glottic level. [Color figure can be viewed inthe online issue, which is available at wileyonlinelibrary.com.]
Fig. 8. A sequence of velocity magnitude images for peak flowshows (from left to right) the streamlines colored with velocity vec-tors along the larynx, velocity magnitude contours along the sagit-tal plane, and two zoomed views with three-dimensional velocityvectors focusing recirculation regions. Note the pronounced airflow recirculation in case 1 and diminished amount of recirculationin case 2. [Color figure can be viewed in the online issue, which isavailable at wileyonlinelibrary.com.]
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI
1816
Alteration in Laryngeal Form Due to Lossor Change in Muscular Tonus
The first thing that drew our attention during thereconstruction of the three-dimensional experimentmodels was the distortion in the axis and shape of thelaryngeal air mold in BAVFI cases. Anteroposterior di-ameter of the supraglottic air space was increased incase 1, which resulted in a spindle-shaped inlet. Case 2showed enlargement of pyriform fossa that decreasedthe inlet area about the one half of the outlet. Complexneurophysiologic events, such as synkinesis or dysfunc-tional reinnervation after recurrent laryngeal nerve
injury, determine the overall tonus and muscular func-tion of larynx.11 This was reflected in our CFDanalyses as strong pressure drops at the supraglotticlevel during peak flow, which may result in the collapseof soft tissues at the supraglottic level. Additionally,the acceleration of airflow resulted in turbulence andvortex structures that decreased the effectiveness ofairflow and increased the work of breathing. Thus,depending on the results of the two cases, we suggestperforming posterior ventriculectomy more liberallywith PTLC, but further experiments are required onthis subject before any conclusion.
Fig. 9. Comparison of wall shearstress forces in case 1 during respi-ration in tidal volume and peak flow.Distribution of shearing forces alongthe glottis contours shows a highamount of wall shear stress valuesat the anterior part of the glotticopening. [Color figure can beviewed in the online issue, which isavailable at wileyonlinelibrary.com.]
Fig. 10. Comparison of wall shearstress forces in case 2 during respi-ration in tidal volume and peak flow.Distribution of shearing forces alongthe glottis contours shows a highamount of wall shear stress valuesall over the glottic opening. [Colorfigure can be viewed in theonline issue, which is available atwileyonlinelibrary.com.]
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI
1817
Providing an Opening at the Posterior GlottisHelps Maintain Tidal Volume but is Insufficientfor Meeting Increased Respiratory Demands
The rationale behind the PTLC procedure lies onthe morphologic findings that regard the posterior glottisas the respiratory glottis.12 Additionally, release of thetension of the glottic sphincter results in retraction ofthe thyroarytenoid muscle and vocal fold anteriorly, so awidening in the posterior glottic airway occurred to-gether with an increase of the vocal fold mass in theanterior glottis (better voicing).1
From an aerodynamic point of view, one can easilyforesee the acceleration of airflow and presence of pres-sure drop, as the air needs to stream from a constrictedarea in the glottis. Pressure drop is an important param-eter in airflow as it can potentially increase thesusceptibility of collapse at the site of the minimumcross-sectional area, especially when the wall of a partic-ular section is floppy as in bilateral abductor vocal foldparalysis. This point is the limitation in our study asour models assumed rigid airway walls. This approxima-tion, which is common to most experimental andnumerical models, is acceptable in normal quiet breath-ing because variations of the length and diameter of theairways remain moderate. In rapid and deep breathing,the flow might change significantly, and this assumptionmight not be appropriate.13
CFD analyses showed a higher amount of accelera-tion during peak flow in the case with narrower glotticarea (case 2). Interestingly, despite having higher levelsof acceleration in air speed, case 2 showed a loweramount of pressure drop across the glottis (Pglottis � Pinlet)in TV (�13 vs. �15 Pa) but a higher amount of pressuredrop in PF (�36,736.5 vs. �34,188 Pa) models when com-pared to case 1. These visualizations also show thatdifferent patients have considerable differences in theirflow patterns and force distributions on the airway con-duits that make patient-specific models very attractivefor evaluation and treatment planning.13
Shape of the Glottic Opening is as Important asthe Dimension of the Glottic Opening
Contour of the glottic opening was found to be veryimportant in determining the hydraulic diameter of air-way and therefore the character of airflow as laminar orturbulent. During PTLC procedure we cut a 1- to 3-mmtriangular wedge of vocal fold immediately anterior tothe vocal process until the internal perichondrium of thethyroid cartilage was reached.2 However, the position ofthe vocal folds in respect to the midline and covering ofthe vaporized area with healing tissue determined theend shape of the glottic opening in the long term. Weneglected to compare the difference between unilateraland bilateral PTLC during planning of this study, andunintentionally both cases were unilateral cordotomies,therefore aerodynamic properties of the glottis afterbilateral PTLC still remain unresolved.
As a result of CFD analyses, complex flow patternswere observed demonstrating several flow characteristics.Therefore, as a future direction, we suggest development
of physical larynx models where the consequences ofBAVFI can be more precisely evaluated and validation ofthese results in respect to soft tissues can be performed.
CONCLUSIONThe larynx is a unique organ of the upper aerodi-
gestive system having a very intricate innervationsystem that direct functions such as respiration, speech,protection of lower airways, and swallowing. Losing anyof these functions can be life threatening or debilitatingfor individuals. Various endoscopic procedures exist toalleviate obstruction in BAVFI. The success rate of theseprocedures at first attempt is generally no more than70%, a point to be remembered during decision makingin therapeutic interventions.1 Therefore, until the stud-ies in neurophysiologic level such as laryngeal pacing orreinnervation procedures become successful, we shouldkeep trying to improve our efforts in providing a morephysiologic airway while preserving other vitalfunctions.
BIBLIOGRAPHY
1. Sapundzhiev N, Lichtenberger G, Eckel HE, et al. Surgeryof adult bilateral vocal fold paralysis in adduction: his-tory and trends. Eur Arch Otorhinolaryngol 2008;265:1501–1514.
3. Dennis DP, Kashima H. Carbon dioxide laser posterior cor-dectomy for treatment of bilateral vocal cord paralysis.Ann Otol Rhinol Laryngol 1989;98:930–934.
4. Harnisch W, Brosch S, Schmidt M, Hagen R. Breathing andvoice quality after surgical treatment for bilateral vocalcord paralysis. Arch Otolaryngol Head Neck Surg 2008;134:278–284.
5. Hans S, Vaissiere J, Crevier-Buchman L, Laccourreye O,Brasnu D. Aerodynamic and acoustic parameters in CO2laser posterior transverse cordotomy for bilateral vocalfold paralysis. Acta Otolaryngol 2000;120:330–335.
6. Mihaescu M, Murugappan S, Gutmark E, Donnelly LF,Khosla S, Kalra M. Computational fluid dynamics analy-sis of upper airway reconstructed from magnetic reso-nance imaging data. Ann Otol Rhinol Laryngol 2008;117:303–309.
7. Davidson PA. Turbulence. An Introduction for Scientistsand Engineers. New York, NY: Oxford University Press;2004.
8. Suh J, Frankel SH. Comparing turbulence models for flowthrough a rigid glottal model. J Acoust Soc Am 2008;123:1237–1240.
9. Ozlugedik S, Nakiboglu G, Sert C, et al. Numerical study ofthe aerodynamic effects of septoplasty and partial lateralturbinectomy. Laryngoscope 2008;118:330–334.
10. Mihaescu M, Gutmark E, Murugappan S, Elluru R, CohenA, Willging JP. Modeling flow in a compromised pediatricairway breathing air and heliox. Laryngoscope 2009;119:145–151.
11. Zealear DL, Billante CR. Neurophysiology of vocal fold pa-ralysis. Otolaryngol Clin North Am 2004;37:1–23.
12. Hirano M, Kurita S, Kiyokawa K, Sato K. Posterior glottis.Morphological study in excised human larynges. AnnOtol Rhinol Laryngol 1986;95(6 pt 1):576–581.
13. Cebral JR, Summers RM. Tracheal and central bronchialaerodynamics using virtual bronchoscopy and computa-tional fluid dynamics. IEEE Trans Med Imaging 2004;23:1021–1033.
Laryngoscope 120: September 2010 Gokcan et al.: Characteristics of Airflow in BAVFI