Acta Neurochirurgica 55, 85--97 (1980) ACTA NEUROCHIRURGICA by Springer-Verlag 1980 Departments of Neurosurgery and Neuroradiology, Ciudad Sanitaria "1o de Octubre" and Faculty of Medicine, Madrid, Spain Chronic Adult Hydrocephalus Due to Uncommon Causes By R. D. Lobato, E. Lamas, F. Cordob~s, M. J. Mufioz, and R. Roger With 7 Figures Summary The authors report on four unusual cases of chronic adult hydrocephalus extracted from a large personal series of patients with hydrocephalic dementia. A syndrome resembling that of normal pressure hydrocephalus was due to the following aetiologies in these patients: Paget's disease of the skull, unruptured cerebral arteriovenous malformation, colloid cyst of the third ventricle, and cerebromeningeal cysticercosis. All these patients exhibited disturbances in cerebro- spinal fluid dynamics at the time of study, and were considerably improved by CSF shunting. The value of the continuous CSF pressure monitoring and the constant infusion test in selecting patients with chronic hydrocephalus for shunt therapy is emphasized. Keywords: Hydrocephalus; Paget's disease; colloid cyst; arteriovenous mal- formation; cysticercosis; intracranial pressure; computed tomography. The symptomatic triad of dementia, gait disturbance, and urinary incontinence occurring in patients with chronic hydrocephalus, i.e., the so-called normal pressure hydrocephalus (NPH) is now a well- accepted clinical entity. The most frequently recognized causes of this syndrome are subarachnoid haemorrhage 4, 5, 7, 12, 16, 19, 21, 27, 28, 32, 33, h e a d t r a u m a 4, 7, 14, 16, 19, 21, 22, 27, 28, a n d m e n i n g e a l i n f e c - t i o n 16, 19, 27, 30 Apart from the cases of unknown aetiology which account for approximately 35 per cent in different series 1.4, 7, li, ~6, 19, 21, 27, other rare causes such as aqueduct stenosis 21, 21, 28, 35, tumours obstructing the foramina of Monro 2, 17, 23, and ectasia of the basilar artery 9 have been reported. All the above mentioned aetiologies except the last were represented in a group of 84 patients with chronic 0001-6268/80/0055/0085/$ 02.60
Departments of Neurosurgery and Neuroradiology, Ciudad Sanitaria "1o de Octubre" and Faculty of Medicine, Madrid, Spain
Chronic A d u l t H y d r o c e p h a l u s D u e to U n c o m m o n Causes
By
R. D. Loba to , E. L a m a s , F. Cordob~s , M. J . Mufioz, and R. R o g e r
With 7 Figures
Summary
The authors report on four unusual cases of chronic adult hydrocephalus extracted from a large personal series of patients with hydrocephalic dementia. A syndrome resembling that of normal pressure hydrocephalus was due to the following aetiologies in these patients: Paget's disease of the skull, unruptured cerebral arteriovenous malformation, colloid cyst of the third ventricle, and cerebromeningeal cysticercosis. All these patients exhibited disturbances in cerebro- spinal fluid dynamics at the time of study, and were considerably improved by CSF shunting. The value of the continuous CSF pressure monitoring and the constant infusion test in selecting patients with chronic hydrocephalus for shunt therapy is emphasized.
The symptomat ic tr iad of dementia, gait disturbance, and ur inary incontinence occurring in patients wi th chronic hydrocephalus, i.e., the so-called normal pressure hydrocephalus ( N P H ) is now a well- accepted clinical entity. The most frequently recognized causes of this syndrome are subarachnoid haemorrhage 4, 5, 7, 12, 16, 19, 21, 27, 28, 32, 33, head t rauma 4, 7, 14, 16, 19, 21, 22, 27, 28, and meningeal infec- tion 16, 19, 27, 30 Apa r t f rom the cases of unknown aetiology which account for approximate ly 35 per cent in different series 1.4, 7, li, ~6, 19, 21, 27, other rare causes such as aqueduct stenosis 21, 21, 28, 35, tumours obstructing the foramina of Monro 2, 17, 23, and ectasia of the basilar ar tery 9 have been reported. All the above mentioned aetiologies except the last were represented in a group of 84 patients wi th chronic
0001-6268/80/0055/0085/$ 02.60
86 R.D. Lobato et al.: Chronic Adult Hydrocephalus Due to Causes
hydrocepha lus s tudied in our D e p a r t m e n t dur ing the last seven years. H e r e we r epor t in detail on four cases which have been ex t rac ted f r o m the to ta l series because of their unusual aetiologies. These four pat ients d isp layed identical features to others wi th N P H of com- mone r aetiologies, and were submi t ted to shunt t h e r a p y on the basis o f bo th the c l inicoradiological p resenta t ion and the changes shown in CSF hydrodynamics .
The a im of this p a p e r is twofo ld , f i rs t ly to br ing fur ther evidence t ha t N P H is a synd rome wi th mul t ip le diverse aetiologies, and secondly to emphas ize the va l i d i t y of CSF studies in selecting adul t pa t ients wi th chronic hydrocepha lus for shunt the rapy .
Patients and Methods
This series includes four pat ients whose basic diseases were: Paget ' s disease of the skull, un rup tu red giant cerebral a r te r iovenous m a l f o r m a t i o n , colloid cyst of the th i rd ventr icle, and cerebro- meningeal infes ta t ion by cysticercus cellulosae. Pat ients were studied wi th compu ted t o m o g r a p h y (CT) , and had p reope ra t ive cont inuous in t r aven t r i cu la r pressure ( IVP) recordings p e r f o r m e d b y a me thod described b y us elsewhere 19. Cons tan t infusion tests wi th 2 ml /minu te of saline solution at r oom t empera tu r e 1~, as well as est imations of the CSF pressure /vo lume relat ionship were also p e r f o r m e d in three c a s e s .
Cases Report
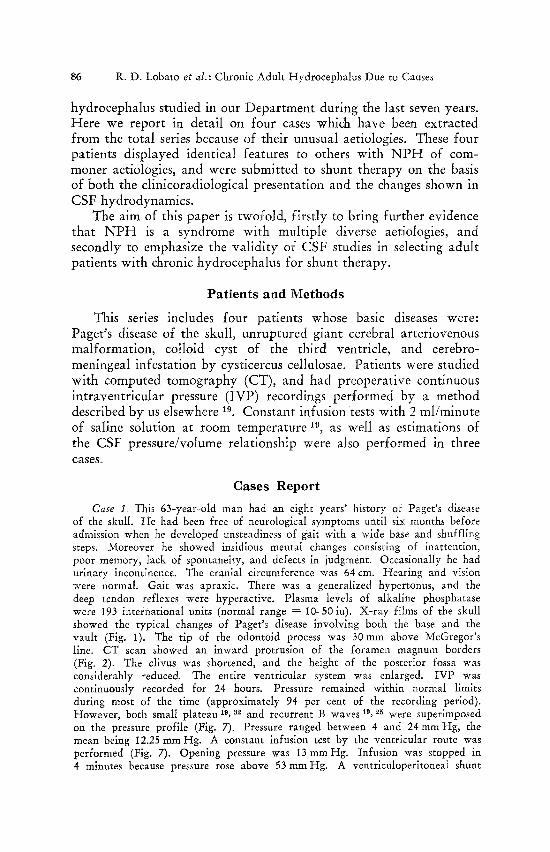
Case 1. This 63-year-old man had an eight years" history of Paget's disease of the skull. He had been free of neurological symptoms until six months before admission when he developed unsteadiness of gait with a wide base and shuffling steps. Moreover he showed insidious mental changes consisting of inattention, poor memory, lack of spontaneity, and defects in judgment. Occasionally he had urinary incontinence. The cranial circumference was 64 cm. Hearing and vision were normal. Gait was apraxic. There was a generalized hypertonus, and the deep tendon reflexes were hyperactive. Plasma levels of alkaline phosphatase were 193 international units (normal range = 10-50iu). X-ray films of the skull showed the typical changes of Paget's disease involving both the base and the vault (Fig. 1). The tip of the odontoid process was 30 mm above McGregor's line. CT scan showed an inward protrusion of the foramen magnum borders (Fig. 2). The clivus was shortened, and the height of the posterior fossa was considerably reduced. The entire ventricular system was enlarged. IVP was continuously recorded for 24 hours. Pressure remained within normal limits during most of the time (approximately 94 per cent of the recording period). However, both small plateau 19, ~ and recurrent B waves 19, ~5 were superimposed on the pressure profile (Fig. 7). Pressure ranged between 4 and 24mm Hg, the mean being 12.25 mm Hg. A constant infusion test by the ventricular route was performed (Fig. 7). Opening pressure was 13 mm Hg. Infusion was stopped in 4 minutes because pressure rose above 53 mm Hg. A ventriculoperitoneal shunt
Fig. 1. Case 1. X-ray film of the skull shows the typical changes of Paget's disease involving the base and the vault
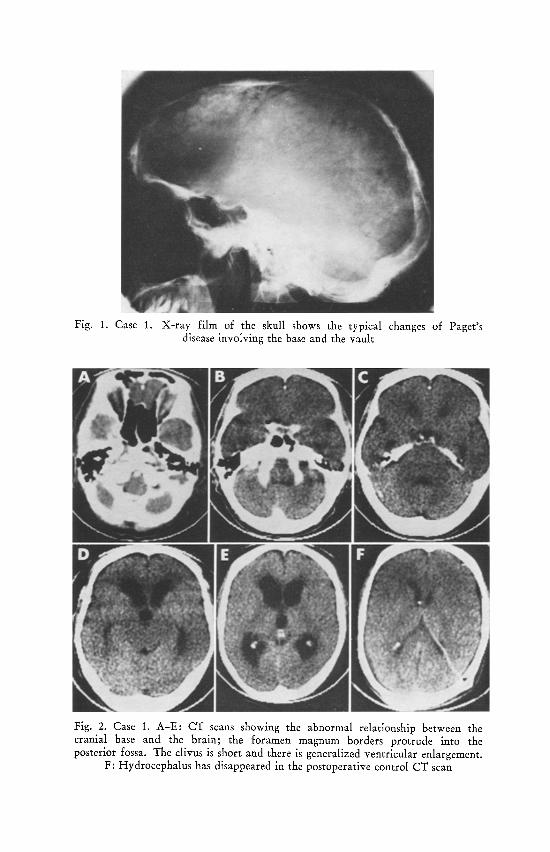
Fig. 2. Case 1. A-E" CT scans showing the abnormal relationship between the cranial base and the brain; the foramen magnum borders protrude into the posterior fossa. The clivus is short and there is generalized ventricular enlargement.
F: Hydrocephalus has disappeared in the postoperative control CT scan
O
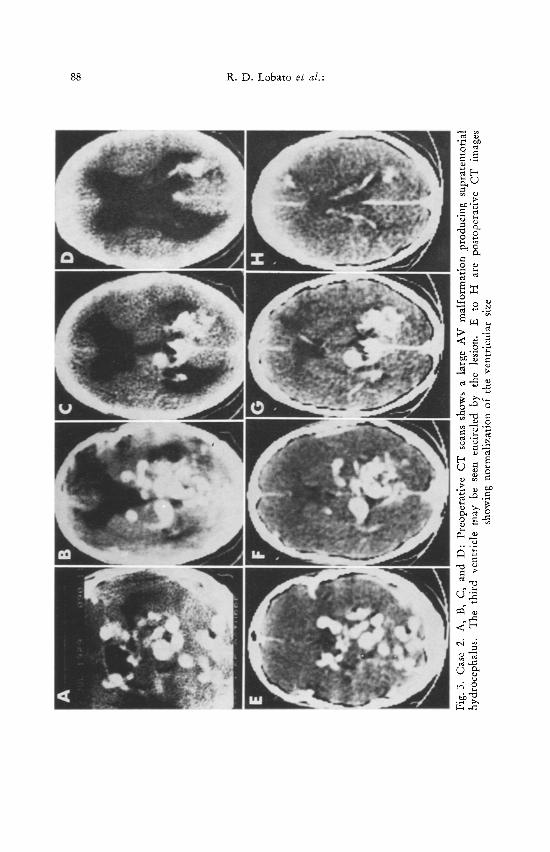
Fig.
3.
Cas
e 2.
A,
B,
C,
and
D:
Pre
oper
ativ
e C
T
scan
s sh
ows
a la
rge
AV
mal
form
atio
n pr
oduc
ing
supr
aten
tori
al
hydr
ocep
halu
s.
The
th
ird
vent
ricl
e m
ay
be s
een
enci
rcle
d by
th
e le
sion
. E
to
H
ar
e po
stop
erat
ive
CT
im
ages
sh
owin
g no
rmal
izat
ion
of t
he v
entr
icul
ar s
ize
Chronic Adult Hydrocephalus to Uncommon Causes 89
was implanted, and the patient's mentation gradualiy improved during the first postoperative week. Both mental and motor performances further improved until he reached a normal state despite the occurrence of subdural hygromas.
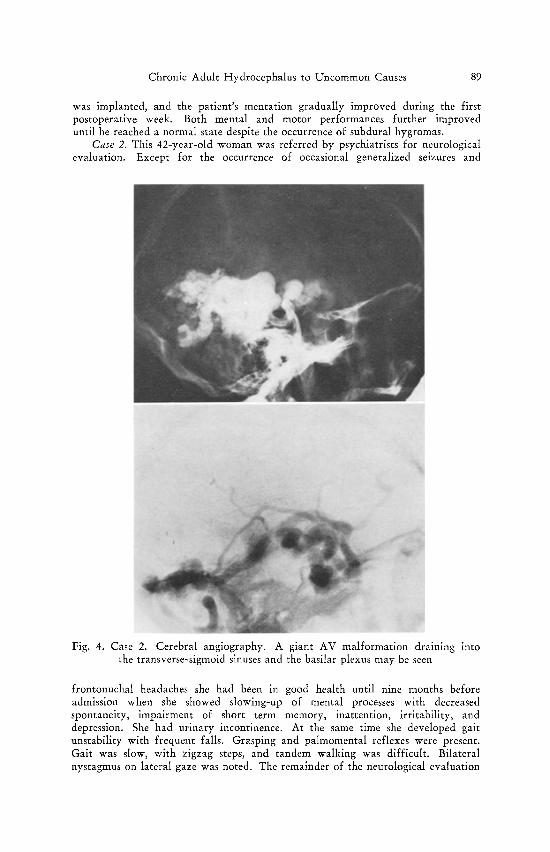
Case 2. This 42-year-old woman was referred by psychiatrists for neurological evaluation. Except for the occurrence of occasional generalized seizures and
Fig. 4. Case 2. Cerebral angiography. A giant AV malformation draining into the transverse-sigmoid sinuses and the basilar plexus may be seen
frontonuchal headaches she had been in good health until nine months before admission when she showed slowing-up of mental processes with decreased spontaneity, impairment of short term memory, inattention, irritability, and depression. She had urinary incontinence. At the same time she developed gait unstability with frequent falls. Grasping and paimomental reflexes were present. Gait was slow, with zigzag steps, and tandem walking was difficult. Bilateral nystagmus on lateral gaze was noted. The remainder of the neurological evaluation
90 R . D . Lobato et al.:
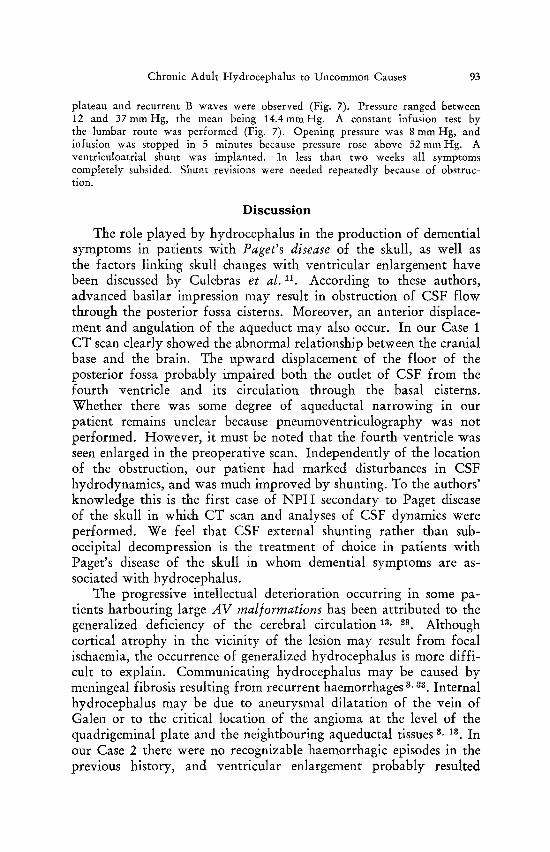
was within normal limits. CT scan showed a giant AV malformation involving temporooccipital lobes, mesencephalon, and cerebellum (Fig. 3). The lateral and third ventricles were considerably enlarged. This latter cavity was surrounded by the lesion so that the passage of CSF was probably compromised. Cerebral panangiography showed that the AV malformation was fed by the posterior cerebral and superior cerebellar arteries bilaterally (Fig. 4). Venous drainage was through the vein of Galen, the transverse and sigmoid sinuses, the cavernous sinus, and the basilar plexus. Surgical excision of the angioma was rejected, and it was questioned whether the hydrocephalus was active or "ex vacuo". IVP was
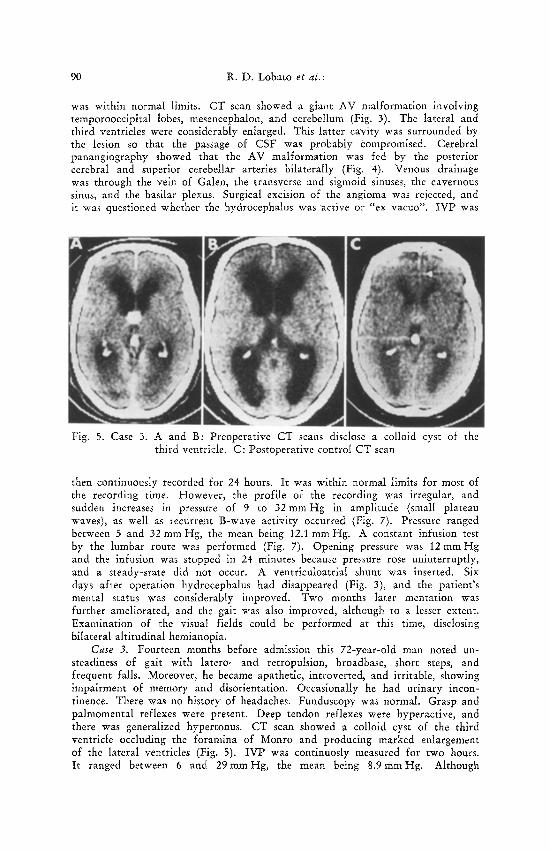
Fig. 5. Case 3. A and B: Preoperative CT scans disclose a colloid cyst of the third ventricle. C: Postoperative control CT scan
then continuously recorded for 24 hours. It was within normal limits for most of the recording time. However, the profile of the recording was irregular, and sudden increases in pressure of 9 to 32 m m H g in amplitude (small plateau waves), as well as recurrent B-wave activity occurred (Fig. 7). Pressure ranged between 5 and 32 mm Hg, the mean being 12.1 mm Hg. A constant infusion test by the lumbar route was performed (Fig. 7). Opening pressure was 12 mm Hg and the infusion was stopped in 24 minutes because pressure rose uninterruptly, and a steady-state did not occur. A ventriculoatrial shunt was inserted. Six days after operation hydrocephalus had disappeared (Fig. 3), and the patient's mental status was considerably improved. Two months later mentation was further ameliorated, and the gait was also improved, although to a lesser extent. Examination of the visual fields could be performed at this time, disclosing bilateral altitudinal hemianopia.
Case 3. Fourteen months before admission this 72-year-old man noted un- steadiness of gait with latero- and retropulsion, broadbase, short steps, and frequent falls. Moreover, he became apathetic, introverted, and irritable, showing impairment of memory and disorientation. Occasionally he had urinary incon- tinence. There was no history of headaches. Funduscopy was normal. Grasp and palmomental reflexes were present. Deep tendon reflexes were hyperactive, and there was generalized hypertonus. CT scan showed a colloid cyst of the third ventricle occluding the foramina of Monro and producing marked enlargement of the lateral ventricles (Fig. 5). IVP was continuosly measured for two hours. It ranged between 6 and 29mmHg, the mean being 8 .9mmHg. Although
Chronic Adult Hydrocephalus to Uncommon Causes 91
pressure level was normal most of the time, recurrent B wave activity was observed. A stereotactic puncture of the cyst was performed according to the technique reported by Bosch et al. s. However, no more than 0.4 ml of the cyst's content could be aspirated, because of its viscous consistency. Such a reduction in cyst volume was considered insufficient to relieve hydrocephalus, so a ventriculo-
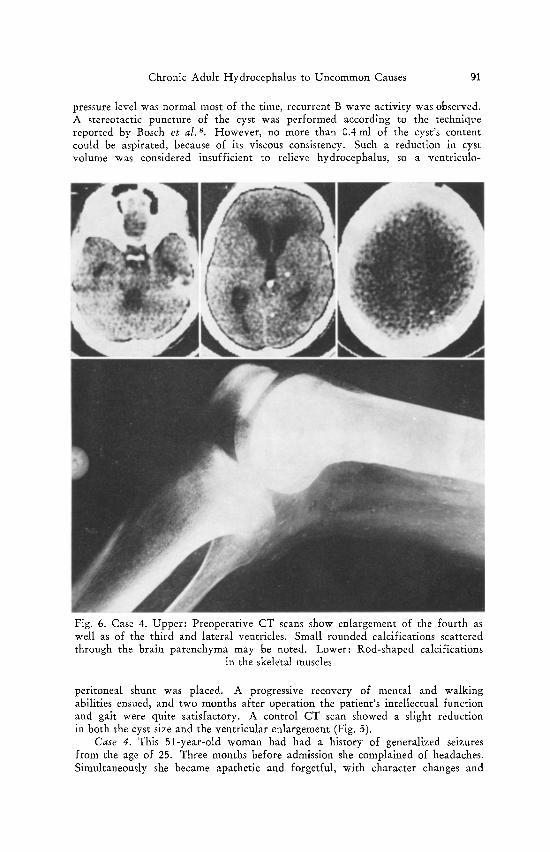
Fig. 6. Case 4. Upper: Preoperative CT scans show enlargement of the fourth as well as of the third and lateral ventricles. Small rounded calcifications scattered through the brain parenchyma may be noted. Lower: Rod-shaped calcifications
in the skeletal muscles
peritoneal shunt was placed. A progressive recovery of mental and walking abilities ensued, and two months after operation the patient's intellectual function and gait were quite satisfactory. A control CT scan showed a slight reduction in both the cyst size and the ventricular enlargement (Fig. 5).
Case 4. This 51-year-old woman had had a history of generalized seizures from the age of 25. Three months before admission she complained of headaches. Simultaneously she became apathetic and forgetful, with character changes and
92 R .D. Lobato et al.:
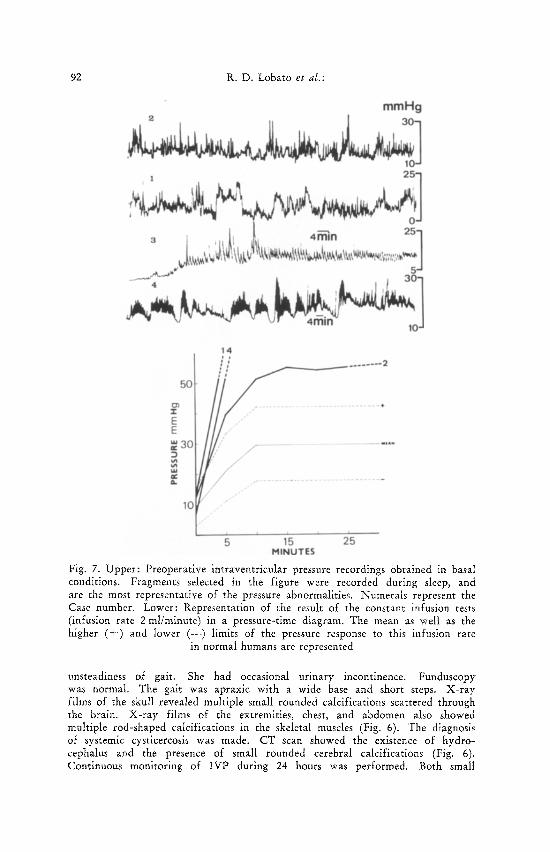
Fig. 7. Upper: Preoperative intraventricular pressure recordings obtained in basal conditions. Fragments selected in the figure were recorded during sleep, and are the most representative of the pressure abnormalities. Numerals represent the Case number. Lower: Representation of the result of the constant infusion tests (infusion rate 2 ml/minute) in a pressure-time diagram. The mean as well as the higher (+ ) and lower (--) limits of the pressure response to this infusion rate
in normal humans are represented
unsteadiness of gait. She had occasional urinary incontinence. Funduscopy was normal. The gait was apraxic with a wide base and short steps. X-ray films of the skull revealed multiple small rounded calcifications scattered through the brain. X-ray films of the extremities, chest, and abdomen also showed multiple r0d-shaped calcifications in the skeletal muscles (Fig. 6). The diagnosis of systemic cysticercosis was made. CT scan showed the existence of hydro- cephalus and the presence of small rounded cerebral calcifications (Fig. 6). Continuous monitoring of IVP during 24 hours was performed. Both small
Chronic Adult Hydrocephalus to Uncommon Causes 93
plateau and recurrent B waves were observed (Fig. 7). Pressure ranged between 12 and 3 7 m m H g , the mean being 14 .4mmHg. A constant infusion test by the lumbar route was performed (Fig. 7). Opening pressure was 8 mm Hg, and infusion was stopped in 5 minutes because pressure rose above 52ram Hg. A ventriculoatrial shunt was implanted. In less than two weeks all symptoms completely subsided. Shunt revisions were needed repeatedly because of obstruc- tion.
D i s c u s s i o n
The role played by hydrocephalus in the production of demential symptoms in patients with Paget's disease of the skull, as well as the factors linking skull changes with ventricular enlargement have been discussed by Culebras et al. 11. According to these authors, advanced basilar impression may result in obstruction of CSF flow through the posterior fossa cisterns. Moreover, an anterior displace- ment and angulation of the aqueduct may also occur. In our Case 1 CT scan clearly showed the abnormal relationship between the cranial base and the brain. The upward displacement of the floor of the posterior fossa probably impaired both the outlet of CSF from the fourth ventricle and its circulation through the basal cisterns. Whether there was some degree of aqueductal narrowing in our patient remains unclear because pneumoventriculography was not performed. However, it must be noted that the fourth ventricle was seen enlarged in the preoperative scan. Independently of the location of the obstruction, our patient had marked disturbances in CSF hydrodynamics, and was much improved by shunting. To the authors' knowledge this is the first case of NPH secondary to Paget disease of the skull in which CT scan and analyses of CSF dynamics were performed. We feel that CSF external shunting rather than sub- occipital decompression is the treatment of choice in patients with Paget's disease of the skull in whom demential symptoms are as- sociated with hydrocephalus.
The progressive intellectual deterioration occurring in some pa- tients harbouring large A V malformations has been attributed to the generalized deficiency of the cerebral circulation lz, 2~. Although cortical atrophy in the vicinity of the lesion may result from focal ischaemia, the occurrence of generalized hydrocephalus is more diffi- cult to explain. Communicating hydrocephalus may be caused by meningeal fibrosis resulting from recurrent haemorrhages 3, z~. Internal hydrocephalus may be due to aneurysmal dilatation of the vein of Galen or to the critical location of the angioma at the level of the quadrigeminal plate and the neightbouring aqueductal tissues 3, 13. In our Case 2 there were no recognizable haemorrhagic episodes in the previous history, and ventricular enlargement probably resulted
94 R . D . Lobato et aL:
because the malformation encroached upon the posterior part of the third ventricle and the upper part of the aqueduct resulting in an incomplete obstruction. The normal mean CSF pressure suggested that our patient had a compensated or even an ex vacuo hydro- cephalus. However, the presence of abnormal waves in the pressure recording as well as the abnormal infusion test, indicate the active nature of the ventricular enlargement in our case, which represents an exceptional example of internal hydrocephalus presenting with the syndrome of NPH. Although large cerebral AV malformations may increase venous pressure within the dural sinuses and impede CSF reabsorption, we discard the possibility that this mechanism could have played some role in the production of hydrocephalus in our case. Raised sagittal sinus pressure is prone to cause hydro- cephalus in infants, but in adults it most often produces pseudo- tumour-like states 20.
It is well-known that colloid cysts produce symptoms by obstruct- ing CSF flow, and the paroxysmal nature of the headaches, often associated with vomiting, has been considered to be a suggestive feature of this lesion 6. s, ~7, .2~. However, the clinical manifestations of colloid cysts are diverse 6, and occasionally patients present with the syndrome of N P H iv, ~a. Our patient had never had headaches, and before the CT scan was performed we thought he suffered from idiopathic NPH. He is one of the oldest patients with a colloid cyst reported in the literature and the first presenting the syndrome of N P H in whom CT scan and analysis of CSF pressure have been performed. As the volume of the cyst was only partially reduced by means of the stereotactic aspiration, it remains uncertain whether improvement must be attributed to the opening of the foramina of Monro or to the action of the implanted shunt.
Infestation of the brain by the larvae (Cysticercus cellulosae) of the Taenia Solium may occur at parenchymai, intraventricular, lepto- meningeal level, or all these levels simultaneously 25, 26, 82, 34 Par- enchymal infestation usually produces seizures. Colonization of the ventricular system may produce internal hydrocephalus 1~, ~, Sub- arachnoid and cisternal infestation may provoke inflammatory re- actions liable to cause arachnoid-expanding cysts or communicating hydrocephalus 18. We have had the opportunity to treat three patients with internal hypertensive hydrocephalus and five with chronic "normotensive" communicating hydrocephalus secondary to infesta- tion by cysticereosis, and the case reported here is representative of the features in the last group. These five patients had mixed par- enchymal and cisternal infestation so they presented with a history of seizures and later developed the syndrome of NPH.
Chronic Adult Hydrocephalus to Uncommon Causes 95
Despite their quite different aetiologies (dysplasic, vascular, tumoural, and infective-parasitic) and the distinct levels of obstruc- tion to CSF flow (fourth ventricle-basal cisterns, aqueduct, foramina of Monro, and subarachnoid space) hydrocephalus caused the same symptomatic triad of gait disturbance, progressing dementia, and urinary incontinence in our cases. By convention, the syndrome of N P H consists of the aforementioned symptomatic triad associated with "normal" lumbar CSF pressure .'v. However, according to our experience 19, 24 and that of other authors 7, 10, 1~, 3.', patients with NPH, idiopathic or not, have episodically raised pressure. This parameter is indeed normal most of the time (80-97 per cent of the recording period) but not all the time as in normal individuals or in patients with global atrophy. This was also true in the present series because we have shown that no patient had symptoms of raised intracranial pressure, and IVP remained within normal limits most of the recording time. However, abnormal increases in pressure above the base line were episodically recorded in every case. On the other hand, the reserve in CSF reabsorptive capacity estimated by means of the constant infusion tests was found to be reduced in three cases. These changes in CSF dynamics, which are absent in patients with global atrophy (hydrocephalus ex vacuo), were con- sidered as convincing evidence that ventricular enlargement was an active process requiring shunt therapy rather than a passive event. To us the abnormal pressure waves in the preoperative recordings, which seem to occur when there is a reduction in the intracranial volumetric buffering capacity 19, .,5, 3~, are the best predictor of the result of CSF shunting in patients with chronic hydrocephalus.
R e f e r e n c e s
1. Adams, R. D., Fisher, C. M., Hakim, S., Ojemann, R. G., Sweet, W. H., Symptomatic occult hydrocephalus with "normal" cerebrospinal fluid pressure. A treatable syndrome. N. Engl. J. Med. 273 (1965), 117--126.
2. Aleksic, S. N., George, A. E., Dementia and low-pressure hydrocephalus in a patient with pituitary adenoma. J. Neurol. Sci. 19 (1973), 341--345.
3. Aronson, S. M., Vascular malformations, in: Pathology of the Nervous System, Vol. 2 (Minckler, ed.). New York: McGraw-Hill, Inc. 1972.
4. Bannister, R., Gilford, E., Kocen, R., Isotope encephalography in the diagnosis of dementia due to communicating hydrocephalus. Lancet 2 (1967), 1014--1017.
5. Barnett, H. J. M., Some clinical features of intracranial aneurysms. Clin. Neurosurg. 16 (1969), 43--71.
6. Batnitzky, S., Sarwar, M., Leeds, N. E., Colloid cysts of the third ventricle. Radiology I12 (1974), 327--341.
7. Belloni, G., di Rocco, C., Focacci, C., Gally, G., Maira, G., Rossi, G. F., Surgical indications in normotensive hydrocephalus. A retrospective analysis of the relations of some diagnostic findings to the results of surgical treatment. Acta Neurochir. (Wien) 33 (1976), 1--21.
96 R.D. Lobato et al.:
8. Bosch, D. A., R~ihn, T., Backlund, E. O., Treatment of Colloid cysts of the third ventricle by stereotactic aspiration. Surg. N eurol. 9 (1978), 15--18.
9. Brelg, A., Ekbom, K., Greitz, T., Kugelberg, E., Hydrocephalus due to elongated basilar artery--a new clinicoradiologicai syndrome. Lancet 1 (1967), 874--~75.
10. Chawla, J. C, Hulme, A., Cooper, R., IntracraniaI pressure in patients with dementia and communicating hydrocephalus. J. Neurosurg. 40 (1974), 376--380.
11. Culebras, A., Feldman, R., Fager, C., Hydrocephalus and dementia in Paget's disease of the skull. J. Neurol. Sci. 23 (1974), 307--321.
12. Gruss, P., Kroiss, A., Gaab, M., Fuhrmeister, U., Long-term measurement of intraventricular pressure in patients with normal pressure hydrocephalus, in: Advances in Neurosurgery 4, pp. 168--175 (W~illenweber, R., Brock, M., t-lamer, J., Klinger, M., Spoerri, O., eds.). Berlin-Heidelberg-New York: 1977.
13. French, L. A., Seljeskog, E. L,, Arteriovenous malformations of the brain, in: Neurological Surgery, pp. 827--836 (Youmans, J. R., ed.). Philadelphia: Saunders Co. 1973.
14. Hakim, S., Adams, R. D., The special clinical problem of symptomatic hydro- cephalus with normal cerebrospinal fluid pressure: Observations on cerebro- spinal fluid hydrodynamics. J. Neurol. Sci. 2 (1965), 307--327.
15. Isamat, F., Cisticercosis cerebral. Barcelona: Vergara S. A. 1957. 16. Katman, R., Normal pressure hydrocephalus, in: Dementia, pp. 69--92
(Wells, E., ed.). Philadelphia: FA Davis Co. 1977. 17. Kelly, R., Colloid cysts of the third ventricle. Analysis of 29 cases. Brain 74
(1951), 23--65. 18. Lamas, E., Estevez, J., Soto, M., Obrador, S., Computerized axial tomography
for the diagnosis of cerebral cysticercosis. Acta Neurochir. (Wien) 44 (1978), 197--205.
19. Lamas, E., Lobato, R. D., Intraventricular pressure and CSF dynamics in chronic adult hydrocephalus. Surg. Neurol. 12 (1979), 287--295.
20. Lamas, E., Lobato, R. D., Esparza, J., Escudero, L., Dural posterior fossa AV malformation producing raised sagittal sinus pressure. Case report. J. Neurosurg. 46 (1977), 804--810.
21. LeMay, M., New, P. F. J., Radiological diagnosis of occult normal pressure hydrocephalus. Radiology .96 (1970), 347--358.
22. Lewin, W., Preliminary observations on external hydrocephalus after severe head injury. Brit. J. Surg. 55 (1968), 747--751.
23. Little, J. R., MacCarty, C. S., Colloid cysts of the third ventricle. J. Neuro- surg. 40 (1974), 230--235.
24. Lobato, R. D., Lamas, E., Esparza, J., Portillo, J. M., Rivas, J. J., Intra- ventricular pressure monitoring and CSF dynamics in non-tumor aqueductal stenosis, in: Intracranial Pressure IV, pp. 511--514 (Shulman, K., Marmarou, A., Miller, J. D., Becket, D. P., eds.). Berlin-Heidelberg-New York: Springer. 1980.
25. Lundberg, N, Continuous recording and control of ventricular fluid pressure in neurosurgical practice. Acta Psycbiat. Scand., Suppl. 149 (1960), 1--193.
337--370. 28. Ojemann, R. G., Fisher, C. M., Adams, R. D., Sweet, W. H., New, P. F. J.,
Further experience with the syndrome of "normal" pressure hydrocephalus. J. Neurosurg. 31 (1969), 279--294.
Chronic Adult Hydrocephalus to Uncommon Causes 97
29. Olivecrona, H., Riives, J., Arteriovenous malformations of the brain. Their diagnosis and treatment. Arch. Neurol. Psychiat. 59 (1948), 567--602.
30. Pedersen, K. K., Sorensen, P. S., Ankerhuss, J., Danielsen, U. T., Syphilitic normal pressure hydrocephalus. Acta Neurochir. (Wien) 48 (1979), 35--39.
31. Simms, N. M., Maxwell, R. E., Christenson, P. C., French, L. A., Internal hydrocephalus secondary to cysticercosis cerebri: Treatment with a ventriculo- atrial shunt. J. Neurosurg. 30 (1969), 305--309.
32. Symon, L., Dorsch, N. W. C., Use of long-term intracranial pressure measure- ment to asses hydrocephalic patients prior to shunt surgery. J. Neurosurg. 42 (1975), 258--273.
33. Theander, S., Granholm, L., Sequelae after spontaneous subarachnoid hemor- rhage with special reference to hydrocephalus and Korsakoff's syndrome. Acta Neurol. Scand. 43 (1967), 479--488.
34. Tolosa, E., Cysticercose c~r~bral. Aspects cliniques et possibilit~s th~rapeutique. Rev. Neurol. 90 (1954), 187--208.
35. Wilkinson, H. A., LeMay, M., Drew, J. H., Adult aqueductal stenosis. Arch. Neurol. 15 (1966), 643--648.
Authors' address: R. D. Lobato, M.D., Servicio de Neurocirugla, Ciudad Sanitaria "1o de Octubre", C/Anda!ucla Km 5,400, Madrid, Spa'n.