ENDOVASCULAR THERAPY AND NEUROCRITICAL CARE 0749-0704/99 $8.00 + .OO ENDOVASCULAR THERAPY OF TRAUMATIC INJURIES OF THE INTRACRANIAL CEREBRAL ARTERIES J. Claude Hemphill 111, MD, Daryl R. Gress, MD, and Van V. Halbach, MD Traumatic injury to the intracranial arteries is an uncommon event but may have sudden and catastrophic consequences. These injuries may occur in a variety of clinical circumstances, including closed-head trauma, penetrating skull injury, inadvertent vascular injury during an extravascular operative procedure, and intravascular injury during angi- ography. Although catastrophic vascular injury such as carotid artery transection may result in early death at the time of severe head trauma, many traumatic intracranial arterial injuries present in a delayed fashion, making diagnosis and anticipation of treatment challenging. For a vari- ety of reasons, including inaccessibility, urgency, and comorbid condi- tions, direct surgical treatment of these lesions may be difficult. As endovascular techniques have advanced over the past three decades, therapeutic intravascular embolization and occlusion have come to play an increasing role in the management of intracranial arterial injuries. Concurrently, advances in neurologic critical care have focused attention on monitoring and intervention in the prevention of secondary brain injury in these patients. From the Departments of Neurology UCH, DRG), Neurosurgery (DRG, VVH), and Radiol- ogy (WH); the Neurovascular Service (JCH, DRG), and the Division of Interventional Neurovascular Radiology (WH), University of California, San Francisco; and Neuro Critical Care, San Francisco General Hospital UCH), San Francisco, California CRITICAL CARE CLINICS VOLUME 15 * NUMl3ER 4 OCTOBER 1999 811
Transcript
ENDOVASCULAR THERAPY AND NEUROCRITICAL CARE 0749-0704/99 $8.00 + .OO
ENDOVASCULAR THERAPY OF TRAUMATIC INJURIES OF THE
INTRACRANIAL CEREBRAL ARTERIES
J. Claude Hemphill 111, MD, Daryl R. Gress, MD, and Van V. Halbach, MD
Traumatic injury to the intracranial arteries is an uncommon event but may have sudden and catastrophic consequences. These injuries may occur in a variety of clinical circumstances, including closed-head trauma, penetrating skull injury, inadvertent vascular injury during an extravascular operative procedure, and intravascular injury during angi- ography. Although catastrophic vascular injury such as carotid artery transection may result in early death at the time of severe head trauma, many traumatic intracranial arterial injuries present in a delayed fashion, making diagnosis and anticipation of treatment challenging. For a vari- ety of reasons, including inaccessibility, urgency, and comorbid condi- tions, direct surgical treatment of these lesions may be difficult. As endovascular techniques have advanced over the past three decades, therapeutic intravascular embolization and occlusion have come to play an increasing role in the management of intracranial arterial injuries. Concurrently, advances in neurologic critical care have focused attention on monitoring and intervention in the prevention of secondary brain injury in these patients.
From the Departments of Neurology UCH, DRG), Neurosurgery (DRG, VVH), and Radiol- ogy (WH); the Neurovascular Service (JCH, DRG), and the Division of Interventional Neurovascular Radiology (WH), University of California, San Francisco; and Neuro Critical Care, San Francisco General Hospital UCH), San Francisco, California
CRITICAL CARE CLINICS
VOLUME 15 * NUMl3ER 4 OCTOBER 1999 811
812 HEMPHILL et a1
PATHOLOGY AND EPIDEMIOLOGY OF TRAUMATIC INTRACRANIAL ARTERIAL INJURIES
Traumatic injuries of the intracranial arteries can be divided into three main categories: dissections, aneurysms, and fistulas. Although there may be overlap between these categories regarding specific lesions, this is a useful distinction in terms of pathologic understanding and treatment planning.
Dissections
A dissection, sometimes known by the misleading term dissecting aneurysm, occurs when injury to one or more arterial layers allows blood to force its way between vessel layers along a dissection ~ lane .4~ Intracranial arteries differ from extracranial arteries in that they lack an external elastic lamina and have a thinner ad~entit ia.~ Although systemic vascular dissection has been attributed to a defect in the arterial media from a rupture in the vasa vasorum, intracranial dissection may manifest variably, depending on the plane of dissection. Most intracranial dissec- tions result from a defect in the internal elastic lamina (intimal tear).61 Blood that accumulates below the internal elastic lamina may push this layer toward the arterial lumen, thereby creating an intimal flap that acts as a nidus for embolic material or may even occlude the arterial lumen.61 Less commonly, intracranial arterial dissections may originate within the media or adventitia. In this case, the intima may be spared, but subarachnoid hemorrhage may result from rupture through the adventitia.62 This type of dissection may result in the formation of a pseudoaneurysm.
The cause of most intracranial dissections remains obscure. Al- though some case series have not implicated severe trauma as a direct cause, others have suggested that trauma is an important contributor.", 38* 55 When catheter-related trauma during angiography causes a dissec- tion, it is usually of the intimal tear type. When severe head injury results in a tear in the adventitia, then the distinction between pseudoan- eurysm and dissection may be arbitrary.
The actual incidence of traumatic intracranial dissection is difficult to assess because angiography is no longer performed routinely in patients who have traumatic brain injury. It is likely higher than appreci- ated because many lesions either remain asymptomatic or not identified in patients who succumb from the incident trauma. Of note, M ~ a r ~ ~ found a 30% incidence of intimal disruption of the cervical carotid artery in autopsies of 200 consecutive patients who died in motor vehicle accidents. Although conventional angiography has been required for definitive diagnosis in the past, magnetic resonance (MR) imaging or MR angiography may show pr~mise.~, l8 With intracranial dissections, the middle cerebral artery is most commonly involved, followed by the basilar artery, but any intracranial artery may be impli~ated.~~ Because of their rarity and the difficulty in asymptomatic diagnosis, the natural
TRAUMATIC INJURIES OF THE INTRACRANIAL CEREBRAL ARTERIES 813
history of intracranial dissections is unknown. Surgical exploration and repair, especially of posterior circulation intracranial dissections, has been advocated and anticoagulation has often been eschewed for fear of extension and possible r~pture .~ , Endovascular therapy offers new alternatives such as angioplasty and stent deployment to restore vessel patency. Currently, however, the technology for intracranial stenting is still in evolution.
Traumatic Aneurysms
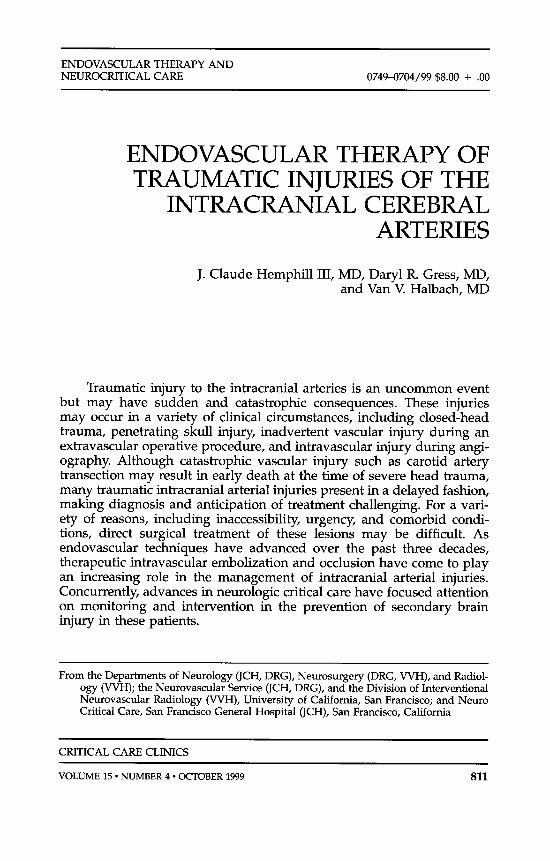
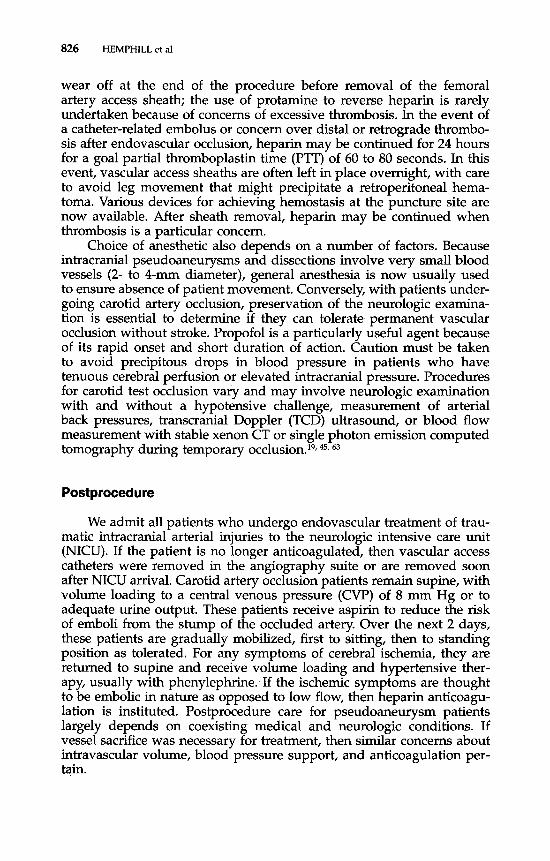
A traumatic intracranial aneurysm occurs when there is disruption of the arterial wall resulting in an outpouching or enlargement of the involved arterial lumen.35 In saccular aneurysms, which are much more common, the media and internal elastic lamina are attenuated. The saccular aneurysm wall, although composed of primarily intima and adventitia, represents a competent wall without disruption, unless, of course, the aneurysm has previously 56 Traumatic intracranial aneurysms may be divided into true and false traumatic aneurysms. True traumatic aneurysms result when there is disruption of intima, internal elastic lamina, and media, leaving only ad~entitia.4~ False traumatic aneurysms are much more common than true traumatic aneurysms and result when there is disruption of all vessel layers. A false aneurysm is actually just a hematoma that is contained by surrounding tissue with the medial portion of the hematoma excavated by turbulent arterial blood at the site of the arterial defect.l, 6n Over time, the wall of the false aneurysm is formed from collagenous organization of the periphery of the original hemat0ma.4~ Because the distinction between true and false traumatic intracranial aneurysms is histologic, it may not be possible to distinguish between them, based solely on angiography. The term pseudoaneurysm is more inclusive and encompasses both true and false aneurysms (Fig. 1).=
Traumatic aneurysms are uncommon and compose less than 1% of all intracranial aneurysms in large series.', However, in children they make up a higher percentage, because of the relative rarity of saccular aneurysms.", 58, 6n Traumatic intracranial aneurysms are thought to arise more commonly in penetrating skull injuries, especially from sharp 0bje~ts.l~ Kieck and de Villiers4'I found a 10% incidence of traumatic aneurysms in 109 patients who had penetrating head injuries, mostly stab wounds. Conversely, Ferry and Kempe15 found only 2 cases of traumatic intracranial aneurysms in 2187 patients who had penetrating head trauma, primarily gunshot wounds, sustained in Vietnam. Inadver- tent arterial puncture or injury during a surgical procedure has also been implicated as a cause of pseudoaneurysm.16 Despite this predilection for penetrating injuries, reports of severe closed-head injury resulting in traumatic intracranial aneurysms are not uncommon, and this is the likely cause of most traumatic intracranial aneurysms in civilian circum- s tance~.~~, 52, 57 Penetrating injuries may result in pseudoaneurysm forma-
814 HEMPHILL et a1
Figure 1. Dissections and pseudoaneurysrns. A, lntimal flap type dissection. B, Adventitial tear type of dissection with formation of a true traumatic aneurysm. C, False traumatic aneurysm with disruption of all vessel layers. Hatches indicate surrounding tissue that comprises the wall of false aneurysm. B and C are considered pseudoaneurysms. Heavy solid line = Adventitia; heavy shaded line = media; narrow black line = intima.
tion in whichever vessel is involved. Traumatic aneurysms from severe closed-head injury have a predilection for distal cerebral arteries, espe- cially the middle cerebral artery, from trauma against the falx or the tentorium or from overlying skull fractures.37
Traumatic intracranial aneurysms, as pseudoaneurysms, most often become symptomatic 2 to 8 weeks after the incident t ra~ma.4~ Sudden intracranial hemorrhage is the most common presenting event. In a minority of cases, symptoms of mass effect may be the presenting sign of an enlarging, unruptured pseudoaneurysm. This is especially true in children, who may present with enlarging sutures or skull fractures.'* Other symptoms of pseudoaneurysm mass effect include progressive visual loss or cranial neuropathies, especially when the pseudoaneurysm is located in the cavernous sinus. When intracranial hemorrhage is the presenting symptom, the type of hemorrhage is determined by the location of the aneurysm. Because traumatic pseudoaneurysms may occur on proximal or distal intracranial arteries, subdural, intraparenchy- mal, intraventricular, or subarachnoid hemorrhage may result. Of partic- ular concern is the possibility of life-threatening epistaxis from rupture of a supraclinoid internal carotid artery pseudoaneurysm with associ- ated skull and facial fracture^.^, 30, 41 In this circumstance, there may be one or more episodes of mild epistaxis before a massive bleeding episode from which death by exsanguination may occur.
TRAUMATIC INJURIES OF THE INTRACRANIAL CEREBRAL ARTERIES 815
In general, traumatic pseudoaneurysms, especially false aneurysms, do not spontaneously resolve. If they are not identified before rupture, then the approach to treatment must also involve management of the new event, such as intraparenchymal or subarachnoid hemorrhage. If identified before rupture, these traumatic aneurysms should be treated, as their natural history is unlikely to remain benign? Surgical treatment may involve clipping or resection if the lesion is amenable. Occasionally, a vascular bypass is necessary, especially if the aneurysm occurs as part of a proximal artery that cannot be preserved. Historically, surgical ligation of the carotid artery in the neck was used for intracranial internal carotid artery traumatic aneurysms.8 Presently, endovascular occlusive therapy, such as with detachable balloons, is preferable and may be lifesaving in patients who have the threat of exsanguination from epi~taxis.~, 30 Endovascular coil embolization has also been demonstrated successful in cases of pseudo aneurysm^.^^
Fistulas
Abnormal connections between intracranial arterial and venous cir- culations (arteriovenous fistulas) may occur after severe or even rela- tively mild head trauma? Intracranial arteriovenous fistulas may be divided into direct and indirect fistulas.26* 27, 34 Direct fistulas occur when there is complete disruption of the wall of an artery, with connection directly into the venous circulation. Almost all direct intracranial fistulas are direct carotid-cavernous fistulas (CCF), an acquired connection be- tween the intracranial carotid artery and the cavernous sinus. Trauma is a common, but not exclusive, cause of direct CCEB A direct CCF may occur at the time of closed-head trauma from the tearing of a small carotid artery branch in the cavernous sinus or in a delayed fashion after rupture of an intracavernous traumatic pseudoaneurysm. Penetrat- ing head trauma may also be implicated.22 Indirect arteriovenous fistulas (AVF), also known as dural AVF, are acquired arteriovenous connections located within the dura. The arterial supply may be from dural branches of the external carotid artery but also from dural branches of the internal carotid artery.29 Indirect CCF may occur, as may dural AVF involving other venous structures, including the transverse and the sigmoid si- nuses.25, 28, 29 Indirect AVF may be engendered by trauma and tend to present in a delayed fashion, months to weeks later.14
Direct CCF are the most common type of posttraumatic intracranial fistula. They may present with bruit, chemosis, exophthalmos, visual loss, and cranial neuropathies referable to the cavernous sinus.2o How- ever, the severity of clinical symptoms depends on factors such as the size of arterial injury and the adequacy of venous drainage. Also, if a cavernous carotid aneurysm extends outside the cavernous sinus, such as into the sphenoid sinus or subarachnoid space, then a direct CCF may be associated with more catastrophic symptoms such as massive epistaxis or subarachnoid hemorrhage. Indirect AVF may present with
816 HEMPHILL et a1
relatively benign symptoms such as pulsatile tinnitus or headache, but can also present with focal cerebral dysfunction or intracerebral hemor- rhage if there is involved cortical venous drainage and venous outflow obstruction?
Approaches to treatment for traumatic AVF vary depending on the nature of the lesion. Low-flow direct CCF may on occasion be cured with intermittent external cervical carotid artery and jugular vein manual compre~sion.~~ Surgical approaches such as cervical carotid artery liga- tion or, rarely, intracavernous carotid artery microsurgical repair have been used in the past.1° Currently, endovascular intervention has as- sumed a dominant role in the treatment of direct CCE9 Detachable balloon occlusion or endovascular embolization via the transarterial or, occasionally, the transvenous route have demonstrated great success.2, 23,
24, 27, 39 Indirect AVF are usually first considered for endovascular therapy but may be resected surgically as well.25, 26, 28, 29 The endovascular ap- proach can be transarterial or transvenous, depending upon the precise anatomy of the lesion and venous outflow.
ENDOVASCULAR INTERVENTION
History
Before the advent of CT and MR imaging, diagnostic angiography, usually via a cervical carotid artery puncture, was routinely used for neurodiagnostic purposes in the management of stroke and traumatic brain injury. The ability to treat lesions at the time of angiography has been considered advantageous since catheter-based techniques began to evolve in the 1970s. In fact, some of the earliest considerations of endovascular treatment involved traumatic intracranial arterial injuries. In 1971, Prolo and Hanberysl described intraluminal nondetachable bal- loon catheter occlusion of a traumatic direct CCF followed by carotid artery ligation. Serbinenk0,5~ in 1974, described over 300 cases of balloon catheterization and temporary occlusion of cerebral vessels as a method of determining tolerance to permanent vascular ligation and adequacy of collateral circulation; he anticipated the future role of permanent endovascular occlusion by proposing that a balloon be left in place and the catheter be cut at the angiographic puncture site. Subsequent to this, Hieshima and colleague^^^ demonstrated the feasibility of detachable balloon occlusion in the endovascular treatment of extracranial and intracranial injuries. Much of the early evolution of endovascular treat- ment involved the embolization of traumatic fistulas, direct CCF, and arterial transections in which emergency occlusive techniques were used.
Materials
To date, endovascular treatment of traumatic intracranial arterial injuries has almost exclusively involved the use of embolic materials (Table 1) to occlude pseudoaneurysms, fistulas, or large arteries. Cur-
TRAUMATIC INJURIES OF THE INTRACRANIAL CEREBRAL ARTERIES 817
Small terminal artery lacerations (e.g., ethmoidal) Distal vessels 50.5-mm diameter
impregnated)
Direct carotid-cavernous fistulas Large artery parent vessel (e.g., internal carotid) Aneurysms and pseudoaneurysms Indirect (dural) AVF Direct carotid-cavernous fistulas Parent vessel occlusion (various sizes)
Electrolytically detachable coils
rently, there is interest in the use of angioplasty and stenting in the treatment of dissections, but this research remains preliminary. Polyvinyl alcohol foam (PVA) particles were among the first embolic materials used.59 These particles range in size from 250 to 1000 micrometers and are suitable for embolization of small arterial lacerations in terminal vessels such as ethmoidal arteries. PVA particles may be delivered via 3F catheters passed through a 5F more proximal delivery catheter. Barium- impregnated Silastic spheres have also been used in the past for occlu- sion of distal vessels of 0.5-mm diameter or less.59 Detachable balloon catheters include a silicone balloon that is delivered at the tip of a catheter to the appropriate site; an internal miter valve prevents deflation after balloon deployment.% Newer detachable balloon devices have al- lowed the injection of a liquid polymerizing material, 2-hydroxyethyl methacrylate (HEMA), into the balloon after placement has been deemed satisfactory via fluoroscopy. The HEMA then solidifies over 40 to 60 minutes, providing permanent embolic material within the aneurysm or vessel lumen to be 0ccluded.3~ Electrolytically detachable platinum coils are now used as embolic material preferentially over detachable balloons in cases of pseudoaneurysms, dural AVF, and many direct CCEZ4, 42, 57
Catheter delivery systems have evolved profoundly over the past two decades. Most endovascular procedures are now performed with the femoral artery for access. Only rarely is the brachial artery used. Direct carotid puncture is no longer used for routine angiographic or endovascular access. Improvements in catheter technology allow steer- able superselective catheters to be directed into distal vessels or aneu- rysms, allowing precise embolization of small distal lesions as desired.
Procedures
Specific procedures vary depending on the nature of the lesion to be embolized and the medical condition of the patient (Table 2). In general, the goal of therapy is to occlude the pseudoaneurysm or fistula
818 HEMPHILL et a1
Table 2. ENDOVASCULAR TREATMENTS FOR INTRACRANIAL ARTERIAL INJURIES
Traumatic Injury Endovascular Treatment Options
Dissections Intimal flap type Adventitial tear type
Coil embolization (transarterial or transvenous) Balloon occlusion Coil embolization (transarterial) Glue embolization of fistula site (rarely)
with the desired embolic material, most likely balloons or coils, while preserving the parent artery? An important exception is the patient who has life-threatening epistaxis from a ruptured supraclinoid internal carotid artery aneurysm in the setting of facial fractures. In this circum- stance, the only option may involve emergent carotid artery occlusion with detachable balloon^.^, 30 Also, many intracranial dissections with pseudoaneurysm formation lead to fusiform lesions, requiring vessel sacrifice for treatment.
Higashida and colleaguesM described the endovascular treatment of 234 cases of traumatic carotid and vertebral artery lesions; of these 206 were direct CCF. Transarterial embolization with detachable balloons was the initial treatment of choice. With a transfemoral approach, a delivery catheter was placed into the internal carotid or vertebral artery, depending on the location of the lesion. To avoid catheter-related throm- boembolic complications, intravenous heparin was given. Balloons were then guided into place and an arteriogram was obtained to ensure proper placement of the balloon. At this point, the balloon was detached. Occasionally, transarterial embolization was performed with other mate- rials, including PVA and coils, especially in the setting of traumatic dural AVF with multiple arterial supplies. Under circumstances in which fistulas could not be successfully treated via the transarterial route, a transfemoral transvenous approach was used to deliver embolic material for fistula occlusion. Other reports have confirmed the use of the transar- terial approach as the method of choice for direct CCF with the transve- nous approach as a practical alternative for direct CCF as well as other posttraumatic fistulas.24, 25, 39
In contrast, treatment options are limited in patients presenting with massive epistaxis from a ruptured traumatic pseudoaneurysm. Because the site of bleeding may not be known, diagnostic angiography is neces- sary prior to consideration of surgical ligation or endovascular occlusion of the parent artery. Balloon occlusion of the parent vessel, usually
TRAUMATIC INJURIES OF THE INTRACRANIAL CEREBRAL ARTERIES 819
internal carotid artery, with the transfemoral approach, may be per- formed at the time of diagnostic angiography and usually represents the best option. Although Han and reported the use of a test occlusion to ensure that permanent internal carotid artery occlusion would be tolerated, we have encountered cases in which the epistaxis was so severe that carotid sacrifice was ine~itable.~ Analogous to surgical trapping, balloon deployment is usually necessary above and below the pseudoaneurysm so that bleeding does not continue from collateral filling of the pseudoaneurysm. If technically feasible, balloon deploy- ment at the actual site of the pseudoaneurysm may also be desirable.
Endovascular coil embolization is successfully used in the treatment of certain saccular intracranial aneur~sms.2~,~~ The use of these electrolyt- ically detachable coils has also been reported for the treatment of trau- matic pseudoaneurysms as well.", 57 This technique involves angiogra- phy via a transfemoral route, with heparin given to maintain an activated clotting time of greater than 200 seconds. Digital road mapping with a 6F or 7F guide catheter is used then to allow a microcatheter to be navigated into the origin of the aneurysm. After a small injection of contrast material into the aneurysm has confirmed proper positioning, platinum coils are advanced into the aneurysm. When placement of an individual coil is confirmed, it then is electrolytically detached. Several coils may be necessary to achieve complete filling of the pseudoaneu- rysm. Subsequent clotting and fibrous organization of the pseudoaneu- rysm proceed, with preservation of the parent artery." Both true and false traumatic intracranial aneurysms have been successfully treated with this technique, and it appears that it is not necessary to make this distinction prior to undertaking endovascular intervention.
Traumatic intracranial arterial dissections that are not associated with pseudoaneurysm formation may cause neurologic symptoms sec- ondary to decreased arterial flow or from distal embolization. There is interest in the use of angioplasty balloons and arterial wall stents to tack back an intimal flap, thereby restoring full vessel patency. Currently, endovascular approaches to the treatment of these lesions have been limited by considerations related to catheter, stent, and inflatable balloon technology. In fact, there is presently no stent made specifically for the cerebral circulation. Despite these limitations, endovascular intervention remains a potential option in refractory cases. For example, we have successfully used a coronary stent to treat a complex catheter-related vertebrobasilar dissection. As technology and experience evolve, endo- vascular treatment of these lesions may become more common.
CASE EXAMPLES
Case Study 1
Subarachnoid hemorrhage from traumatic intracranial dissection. A 42- year-old kickboxer was struck in the left temple during a practice match. He had malaise and headache until 1 week later when he developed sudden, severe
820 HEMPHILL et a1
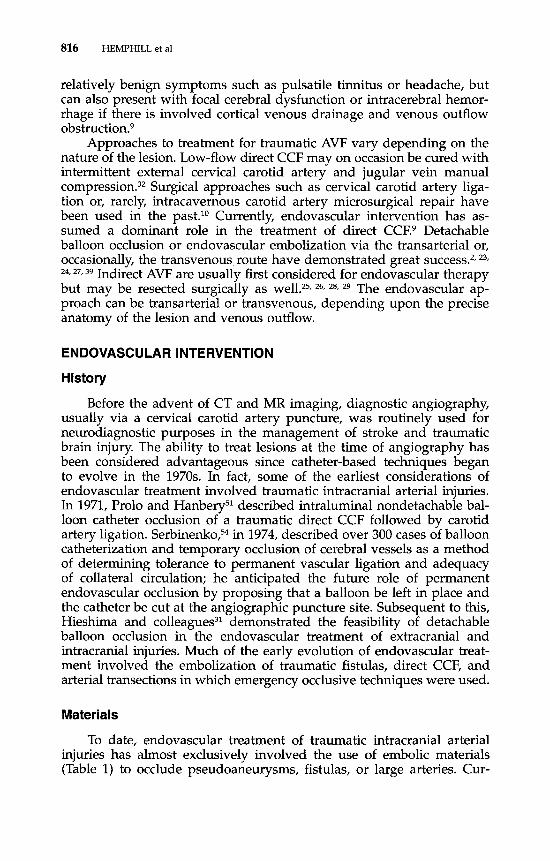
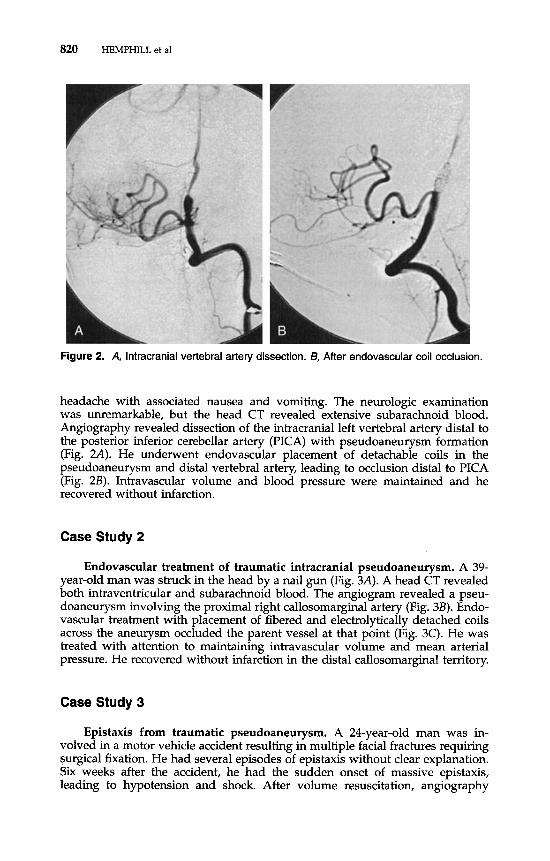
Figure 2. A, lntracranial vertebral artery dissection. B, After endovascular coil occlusion.
headache with associated nausea and vomiting. The neurologic examination was unremarkable, but the head CT revealed extensive subarachnoid blood. Angiography revealed dissection of the intracranial left vertebral artery distal to the posterior inferior cerebellar artery (PICA) with pseudoaneurysm formation (Fig. 2A). He underwent endovascular placement of detachable coils in the pseudoaneurysm and distal vertebral artery, leading to occlusion distal to PICA (Fig. 2B). Intravascular volume and blood pressure were maintained and he recovered without infarction.
Case Study 2
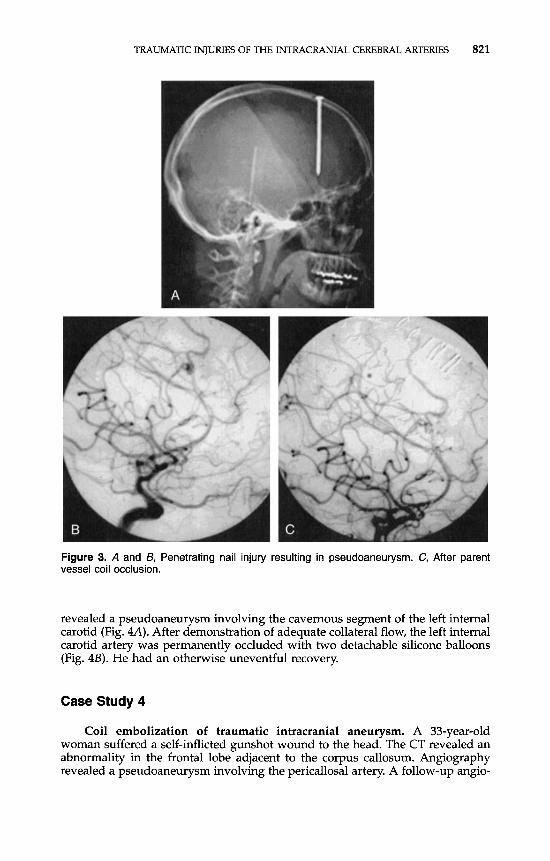
Endovascular treatment of traumatic intracranial pseudoaneurysm. A 39- year-old man was struck in the head by a nail gun (Fig. 3A). A head CT revealed both intraventricular and subarachnoid blood. The angiogram revealed a pseu- doaneurysm involving the proximal right callosomarginal artery (Fig. 3B). Endo- vascular treatment with placement of fibered and electrolytically detached coils across the aneurysm occluded the parent vessel at that point (Fig. 3C). He was treated with attention to maintaining intravascular volume and mean arterial pressure. He recovered without infarction in the distal callosomarginal territory.
Case Study 3
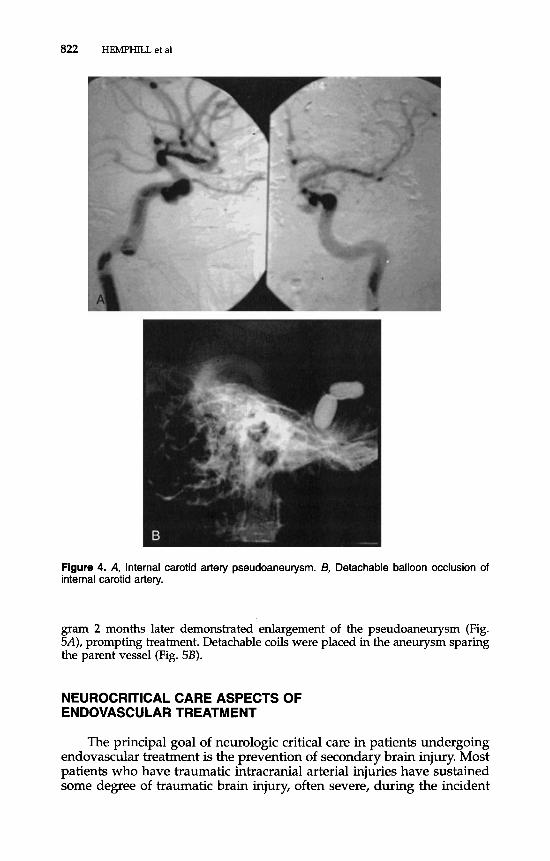
Epistaxis from traumatic pseudoaneurysm. A 24-year-old man was in- volved in a motor vehicle accident resulting in multiple facial fractures requiring surgical fixation. He had several episodes of epistaxis without clear explanation. Six weeks after the accident, he had the sudden onset of massive epistaxis, leading to hypotension and shock. After volume resuscitation, angiography
TRAUMATIC INJURIES OF THE INTRACRANIAL CEREBRAL ARTERIES 821
Figure 3. A and 13, Penetrating nail injury resulting in pseudoaneurysm. C, After parent vessel coil occlusion.
revealed a pseudoaneurysm involving the cavernous segment of the left internal carotid (Fig. 4A). After demonstration of adequate collateral flow, the left internal carotid artery was permanently occluded with two detachable silicone balloons (Fig. 4B). He had an otherwise uneventful recovery.
Case Study 4
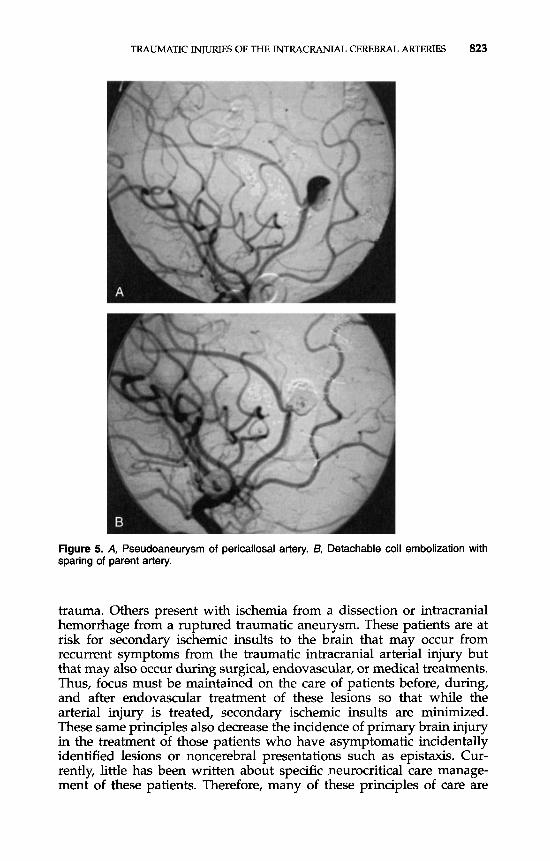
Coil embolization of traumatic intracranial aneurysm. A 33-year-old woman suffered a self-inflicted gunshot wound to the head. The CT revealed an abnormality in the frontal lobe adjacent to the corpus callosum. Angiography revealed a pseudoaneurysm involving the pericallosal artery. A follow-up angio-
822 HEMPHILL et a1
Figure 4. A, Internal carotid artery pseudoaneurysm. B, Detachable balloon occlusion of internal carotid artery.
gram 2 months later demonstrated enlargement of the pseudoaneurysm (Fig. 5A), prompting treatment. Detachable coils were placed in the aneurysm sparing the parent vessel (Fig. 5B).
NEUROCRITICAL CARE ASPECTS OF ENDOVASCULAR TREATMENT
The principal goal of neurologic critical care in patients undergoing endovascular treatment is the prevention of secondary brain injury. Most patients who have traumatic intracranial arterial injuries have sustained some degree of traumatic brain injury, often severe, during the incident
TRAUMATIC INJURIES OF THE INTRACRANIAL CEREBRAL ARTERIES 823
Figure 5. A, Pseudoaneurysm of pericallosal artery. B, Detachable coil ernbolization with sparing of parent artery.
trauma. Others present with ischemia from a dissection or intracranial hemorrhage from a ruptured traumatic aneurysm. These patients are at risk for secondary ischemic insults to the brain that may occur from recurrent symptoms from the traumatic intracranial arterial injury but that may also occur during surgical, endovascular, or medical treatments. Thus, focus must be maintained on the care of patients before, during, and after endovascular treatment of these lesions so that while the arterial injury is treated, secondary ischemic insults are minimized. These same principles also decrease the incidence of primary brain injury in the treatment of those patients who have asymptomatic incidentally identified lesions or noncerebral presentations such as epistaxis. Cur- rently, little has been written about specific neurocritical care manage- ment of these patients. Therefore, many of these principles of care are
824 HEMPHILL et a1
modified from those directed at severe head trauma and stroke," 36 with institutional experience playing an important role (Table 3).
Preprocedu re
Because most traumatic intracranial arterial injuries have a delayed presentation, specific issues related to the acute management of severe closed-head injury may take precedence. However, because of the risks associated with acutely symptomatic intracranial arterial injuries, endo- vascular treatment may need to be undertaken in the setting of recent head trauma, ischemic stroke, or intracranial hemorrhage. Preprocedure issues involve stabilization of acute medical and neurologic issues in these patients and placement of necessary monitoring tools for hemody- namic, ventilatory, and neurologic management. In one of the few de- tailed descriptions of medical management for endovascular procedures, Polin and colleagues50 discussed their approach in 39 patients undergo- ing endovascular treatment of carotid-cavernous aneurysms, none of which were described as traumatic. They admitted patients to the neuro- logic intensive care unit the night before the planned procedure, placed a pulmonary artery catheter and a radial arterial line, and initiated volume loading to a wedge pressure of 10 cm H,O. We do not currently follow this aggressive approach, believing that pulmonary artery cathe- ter monitoring is unnecessary in routine patients who lack cardiac com- promise or other unique circumstances. For patients who are acutely ill with other neurologic problems such as closed-head injury, ischemic stroke, or intracranial hemorrhage, we place a triple-lumen central ve- nous catheter. For carotid circulation lesions, the contralateral subclavian vein is chosen to minimize the untoward consequences of an inadvertent arterial puncture; for vertebrobasilar circulation lesions, either subcla- vian vein is acceptable. Internal jugular catheters are avoided unless the presence of systemic anticoagulation, severe lung injury, or anatomic concerns make this preferable. A radial arterial catheter is placed, with the recognition that the angiographic arterial sheath will also allow blood pressure transduction. A ventriculostomy is placed for hydroceph- alus or in patients who have a depressed level of consciousness from head injury or intracranial hemorrhage. If mechanical ventilation is required, then normoventilation is the goal. In patients who have a hyperacute presentation, such as life-threatening epistaxis, these prepa- rations may not be able to be undertaken.
lntraprocedure
Once again, specific management issues may vary depending on the nature of the lesion undergoing endovascular treatment and the condition of the patient. However, there are common issues involved in all patients undergoing endovascular treatment. Systemic anticoagula-
TRAUMATIC INJURIES OF THE INTRACRANIAL CEREBRAL ARTERIES 825
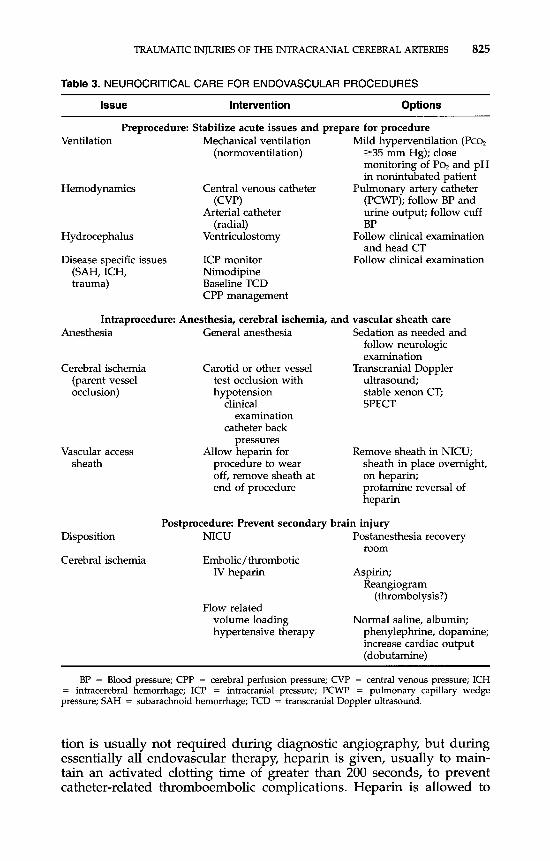
Table 3. NEUROCRITICAL CARE FOR ENDOVASCULAR PROCEDURES
Issue Intervention Options
Preprocedure: Stabilize acute issues and prepare for procedure Ventilation Mechanical ventilation Mild hyperventilation (Pco,
monitoring of PO, and pH in nonintubated patient
Hemodynamics Central venous catheter Pulmonary artery catheter (PCWP); follow BP and urine output; follow cuff
tion is usually not required during diagnostic angiography, but during essentially all endovascular therapy, heparin is given, usually to main- tain an activated clotting time of greater than 200 seconds, to prevent catheter-related thromboembolic complications. Heparin is allowed to
wear off at the end of the procedure before removal of the femoral artery access sheath; the use of protamine to reverse heparin is rarely undertaken because of concerns of excessive thrombosis. In the event of a catheter-related embolus or concern over distal or retrograde thrombo- sis after endovascular occlusion, heparin may be continued for 24 hours for a goal partial thromboplastin time (PTT) of 60 to 80 seconds. In this event, vascular access sheaths are often left in place overnight, with care to avoid leg movement that might precipitate a retroperitoneal hema- toma. Various devices for achieving hemostasis at the puncture site are now available. After sheath removal, heparin may be continued when thrombosis is a particular concern.
Choice of anesthetic also depends on a number of factors. Because intracranial pseudoaneurysms and dissections involve very small blood vessels (2- to 4-mm diameter), general anesthesia is now usually used to ensure absence of patient movement. Conversely, with patients under- going carotid artery occlusion, preservation of the neurologic examina- tion is essential to determine if they can tolerate permanent vascular occlusion without stroke. Propofol is a particularly useful agent because of its rapid onset and short duration of action. Caution must be taken to avoid precipitous drops in blood pressure in patients who have tenuous cerebral perfusion or elevated intracranial pressure. Procedures for carotid test occlusion vary and may involve neurologic examination with and without a hypotensive challenge, measurement of arterial back pressures, transcranial Doppler (TCD) ultrasound, or blood flow measurement with stable xenon CT or single photon emission computed tomography during temporary occ l~s ion .~~~ 45,
Postprocedure
We admit all patients who undergo endovascular treatment of trau- matic intracranial arterial injuries to the neurologic intensive care unit (NICU). If the patient is no longer anticoagulated, then vascular access catheters were removed in the angiography suite or are removed soon after NICU arrival. Carotid artery occlusion patients remain supine, with volume loading to a central venous pressure (CVP) of 8 mm Hg or to adequate urine output. These patients receive aspirin to reduce the risk of emboli from the stump of the occluded artery. Over the next 2 days, these patients are gradually mobilized, first to sitting, then to standing position as tolerated. For any symptoms of cerebral ischemia, they are returned to supine and receive volume loading and hypertensive ther- apy, usually with phenylephrine. If the ischemic symptoms are thought to be embolic in nature as opposed to low flow, then heparin anticoagu- lation is instituted. Postprocedure care for pseudoaneurysm patients largely depends on coexisting medical and neurologic conditions. If vessel sacrifice was necessary for treatment, then similar concerns about intravascular volume, blood pressure support, and anticoagulation per- tain.
TRAUMATIC INJURIES OF THE INTRACRANIAL CEREBRAL ARTERIES 827
SUMMARY
Traumatic intracranial arterial injuries represent uncommon compli- cations of both closed-head injury and penetrating head trauma. These injuries include arterial dissections, pseudoaneurysms, and fistulas, both direct and indirect. Although these lesions may be identified while still asymptomatic, they usually present in a delayed fashion with intracran- ial hemorrhage, focal cerebral ischemia, or, occasionally, severe epistaxis. Endovascular therapy has assumed a major role in the management of this diverse group of lesions. Embolization of pseudoaneurysms with balloons or detachable coils, the use of embolic particles for small arterial injuries, and large vessel occlusion with detachable balloons represent current treatment strategies that have evolved over the past three de- cades. Angioplasty and stent deployment may have a future role to play in the management of arterial dissection. Principles of neurologic critical care that minimize secondary brain injury are essential adjuncts in the management of these patients before, during, and after endovascular treatment.
References
1. Acosta C, Williams P, Clark K Traumatic aneurysms of the cerebral vessels. J Neuro- surg 36531,1972
2. Bavinzski G, Killer M, Gruber A, et al: Treatment of post-traumatic carotico-cavernous fistulae using electrolytically detachable coils: Technical aspects and preliminary expe- rience. Neuroradiology 39:81, 1997
4. Berger M, Wilson C: Intracranial dissecting aneurysms of the posterior circulation. J Neurosurg 61:882, 1984
5. Brugieres P, Castrec-Carpo A, Heran F, et al: Magnetic resonance imaging in the exploration of dissection of the internal carotid artery. J Neuroradiol 16:1, 1989
6. Bullock R, Chestnut R, Clifton G, et a1 Guidelines for the Management of Severe Head Injury. New York, Brain Trauma Foundation, 1995
7. Chen D, Concus AP, Halbach W, et al: Epistaxis originating from traumatic pseudoan- eurysm of the internal carotid artery: Diagnosis and endovascular therapy. Laryngo- scope 108326, 1998
8. Cooper A Account of the first successful operation performed on the common carotid artery for aneurysm in the year 1808: With the post-mortem examination, in 1821. Guys Hosp Rep (Lond) 1:53, 1836
9. DAlise M, Coimbra C, Batjer H Vascular complications of head injury. In Batjer H, Caplan L, Friberg L, et a1 (eds): Cerebrovascular Disease. Philadelphia, Lippincott- Raven, 1997, p 1169
10. Dolenc V k c t microsurgical repair of intracavernous vascular lesions. J Neurosurg 58:824, 1983
11. Dratz H, Woodhall B Traumatic dissecting aneurysm of left internal carotid, anterior
12. Endo S, Takaku A, Aihara H, et a1 Traumatic cerebral aneurysm associated with
13. Feldges A, Nau H-E, Reinhardt V Two cases of sudden death by rupture of traumatic
cerebral and middle cerebral arteries. J Neuropathol Exp Neurol6:286, 1947
widening skull fracture. Childs Brain 6131, 1980
and bacterial aneurysms. Intensive Care Med 15:400, 1989
828 HEMPHILL et a1
supplied by scalp, meningeal, and cortical arteries: Case report. Neurosurgery 6670, 1980
15. Ferry D, Kempe L: False aneurysm secondary to penetration of the brain through orbitofacial wounds: Report of two cases. J Neurosurg 36503, 1972
16. Feuerman TF, Hieshima GB, Bentson JR, et a1 Carotid-cavernous fistula following nasopharyngeal biopsy. Arch Otolaryngol 110412,1984
17. Fleischer A, Patton J, Tindall G: Cerebral aneurysms of traumatic origin. Surg Neurol 4233, 1975
18. Gelbert F, Assouline E, Hodes J, et al: MRI in spontaneous dissection of vertebral and carotid arteries. Neuroradiology 33111, 1991
19. Giller CA, Mathews D, Walker B, et al: Prediction of tolerance to carotid artery occlusion using transcranial Doppler ultrasound. J Neurosurg 81:15, 1994
20. Goto K, Hieshima GB, Higashida RT, et a1 Treatment of direct carotid cavernous sinus fistulae. Various therapeutic approaches and results in 148 cases. Acta Radiol Suppl 369:576, 1986
21. Graves V, Strother C, Duff T, et al: Early treatment of ruptured aneurysms with Guglielmi detachable coils: Effect of subsequent bleeding. Neurosurgery 37640,1995
22. Greatz KW, Imhof HG, Valavanis A: Traumatic carotid cavernous sinus fistula due to a gun shot injury. Int J Oral Maxillofac Surg 20280, 1991
23. Halbach W, Hieshima GB, Higashida RT, et al: Carotid cavernous fistulae: indications for urgent treatment. AJR 149:587, 1987
24. Halbach W, Higashida RT, Bamwell SL, et a1 Transarterial platinum coil embolization of carotid-cavernous fistulas. AJNR 12429, 1991
25. Halbach W, Higashida RT, Hieshima GB, et al: Dural fistulas involving the transverse and sigmoid sinuses: Results of treatment in 28 patients. Radiology 163443, 1987
26. Halbach W, Higashida RT, Hieshima GB, et a1 Transvenous embolization of dural fistulas involving the cavernous sinus. AJRN 10:377, 1989
27. Halbach W, Higashida RT, Hieshima GB, et al: Transvenous embolization of direct carotid cavernous fistulas. AJNR 9:741, 1988
28. Halbach W, Higashida RT, Hieshima GB, et al: Transvenous embolization of dural fistulas involving the transverse and sigmoid sinuses. AJNR 10:385, 1989
29. Halbach W, Higashida RT, Hieshima GB, et a1 Dural fistulas involving the cavernous sinus: Results of treatment in 30 patients. Radiology 163:437, 1987
30. Han MH, Sung MW, Chang KH, et a1 Traumatic pseudoaneurysm of the intracaver- nous ICA presenting with massive epistaxis: Imaging diagnosis and endovascular treatment. Laryngoscope 104370,1994
31. Hieshima GB, Mehringer CM, Grinnell VS, et al: Emergency occlusive techniques. Surg Neurol 9:293, 1978
32. Higashida R, Hieshima G, Halbach V, et a1 Closure of carotid cavernous sinus fistulae by external compression of the carotid artery and jugular vein. Acta Radiol Suppl 369:580, 1986
33. Higashida RT, Halbach W, Dowd C, et a1 Endovascular detachable balloon emboliza- tion therapy of cavernous carotid artery aneurysms: Results in 87 cases. J Neurosurg 72857, 1990
34. Higashida RT, Halbach W, Tsai FY, et al: Interventional neurovascular treatment of traumatic carotid and vertebral artery lesions: Results in 234 cases. AJR 153577, 1989
35. Holmes B, Harbaugh R Traumatic intracranial aneurysms: A contemporary review. J Trauma 35:855, 1993
36. Hund E, Grau A, Hacke W Neurocritical care for acute ischemic stroke. Neurol Clin 13:511, 1995
37. Jackson F, Gleave J, Janon E The traumatic cranial and intracranial aneurysms. In Vinken P, Bruyn G (eds): Handbook of Clinical Neurology. New York, Elsevier, 1976, D 381 r ~~~
38. Johnson A, Graves V, Pfaff J: Dissecting aneurysm of intracranial arteries. Surg Neurol 749, 1977
39. Joseph S, Rao V, Ravimandalam K, et a1 Endovascular management of carotid cavern- ous fistulae: Observation on angiographic and clinical results. Acta Neurol Scand 88:320, 1983
TRAUMATIC INJURIES OF THE INTRACRANIAL CEREBRAL ARTERIES 829
40. Kieck C, devilliers J: Vascular lesion due to transcranial stab wounds. J Neurosurg
41. King MA, Barkovich AJ, Halbach VA, et al: Traumatic monocular blindness and
42. Lempert TE, Halbach VV, Higashida RT, et al: Endovascular treatment of pseudoaneu-
43. Lylyk P, Vianuela F, Campos J, et al: Diagnosis and endovascular therapy of vascular
44. Malek AM, Halbach W, Dowd CF, et al: Diagnosis and treatment of dural arteriove-
45. Mathis JM, Barr JD, Jungreis CA, et al: Temporary balloon test occlusion of the internal
46. McDougall C, Halbach V, Dowd C, et al: Endovascular treatment of basilar tip aneu-
47. Mendel R, Carter L Intracranial arterial injury. In Carter L, Spetzler R, Hamilton M
48. Moar J: Traumatic rupture of the carotid arteries: An autopsy and histopathological
49. Pate1 A, Richardson A: Ruptured intracranial aneurysms in the first two decades of
50. Polin R, Shaffrey M, Jensen M, et al: Medical management in the endovascular
51. Prolo D, Hanbery J: Intraluminal occlusion of a carotid-cavernous sinus fistula with a
52. Quintana F, Diez C, Gutierrez A, et al: Traumatic aneurysm of the basilar artery. AJNR
53. Schievink W Intracranial aneurysms. N Engl J Med 336:28, 1997 54. Serbinenko F: Balloon catheterization and occlusion of major cerebral vessels. J Neuro-
surg 41:125, 1974 55. Shaw C, Foltz E: Traumatic dissecting aneurysm of middle cerebral artery and carotid-
cavernous fistula with massive intracerebral hemorrhage. Case report. J Neurosurg 28:475, 1968