LEKAN JOHN OYEFARA* Female genital mutilation (FGM) and theory of promiscuity: myths, realities and prospects for change in Oworonshoki Community, Lagos State, Nigeria 1. INTRODUCTION Female Genital Mutilation (FGM) or Female Circumcision (FC) has been defined as a traditional practice in which a person, who may be unskilled, or a health worker cuts off parts or whole organs of the female gen- itals usually with knife or razor blade which for most part is unsteriled as a cutting instrument (Adebayo, 1992). In another dimension, World Health Organization (WHO) conceptualized it as all procedures which involve par- tial or total removal of the external female genitalia and/or injury to the female genital organs whether for cultural or any non-therapeutic reasons (WHO, 1994; 2008). In Nigeria, FGM is widespread among the various eth- nic groups, socio-economic groups and classes and it is usually practiced for cultural, religious, and ritual purposes, often as part of initiation rite into womanhood. It is one of the cultural and traditional practices that persist in contemporary Nigeria society despite significant increase in levels of literacy and other modernization values. Research findings over the years in the coun- try (Adebayo, 1992; Centre for Gender and Social Policy Studies, 1998; Odimegwu and Okemgbo, 2000; National Population Commission (NPC) [Nigeria] and ICF Macro (NPC and ICF Macro), 2009) revealed that many Nigerians still practice FGM on a daily basis. In fact, millions of young girls in the country have been circumcised and many more thousands are still wait- ing to be circumcised. Worrisome national data from two recent Nigeria Demographic and Health Survey (NDHS) revealed an increase in the practice of FGM in the country from 19 percent in 2003 to 30 percent in 2008 (NPC and ICF Macro, 2004; 2009). This reality calls for deeper reflections and fur- ther studies into FGM practice in Nigeria considering various campaigns, intervention programmes and legislations that had been put in place by vari- ous development partners, state and non-state actors against FGM in the past two decades in the country. It is imperative to note that FGM is a harmful traditional practice which is inimical to the wellbeing of a woman and it has been described in the liter- ature as an act of violence against women (United Nations Children’s Fund 7 GENUS, LXX (No. 2-3), 7-33 * Department of Sociology, Faculty of Social Sciences, University of Lagos, Akoka, Yaba, Lagos, Nigeria, e-mail: [email protected].
Transcript
LEKAN JOHN OYEFARA*
Female genital mutilation (FGM) and theory of promiscuity: myths, realities and prospects for change
in Oworonshoki Community, Lagos State, Nigeria
1. INTRODUCTION
Female Genital Mutilation (FGM) or Female Circumcision (FC) hasbeen defined as a traditional practice in which a person, who may beunskilled, or a health worker cuts off parts or whole organs of the female gen-itals usually with knife or razor blade which for most part is unsteriled as acutting instrument (Adebayo, 1992). In another dimension, World HealthOrganization (WHO) conceptualized it as all procedures which involve par-tial or total removal of the external female genitalia and/or injury to thefemale genital organs whether for cultural or any non-therapeutic reasons(WHO, 1994; 2008). In Nigeria, FGM is widespread among the various eth-nic groups, socio-economic groups and classes and it is usually practiced forcultural, religious, and ritual purposes, often as part of initiation rite intowomanhood. It is one of the cultural and traditional practices that persist incontemporary Nigeria society despite significant increase in levels of literacyand other modernization values. Research findings over the years in the coun-try (Adebayo, 1992; Centre for Gender and Social Policy Studies, 1998;Odimegwu and Okemgbo, 2000; National Population Commission (NPC)[Nigeria] and ICF Macro (NPC and ICF Macro), 2009) revealed that manyNigerians still practice FGM on a daily basis. In fact, millions of young girlsin the country have been circumcised and many more thousands are still wait-ing to be circumcised. Worrisome national data from two recent NigeriaDemographic and Health Survey (NDHS) revealed an increase in the practiceof FGM in the country from 19 percent in 2003 to 30 percent in 2008 (NPCand ICF Macro, 2004; 2009). This reality calls for deeper reflections and fur-ther studies into FGM practice in Nigeria considering various campaigns,intervention programmes and legislations that had been put in place by vari-ous development partners, state and non-state actors against FGM in the pasttwo decades in the country.
It is imperative to note that FGM is a harmful traditional practice whichis inimical to the wellbeing of a woman and it has been described in the liter-ature as an act of violence against women (United Nations Children’s Fund
7
GENUS, LXX (No. 2-3), 7-33
* Department of Sociology, Faculty of Social Sciences, University of Lagos, Akoka, Yaba, Lagos,Nigeria, e-mail: [email protected].
OYEFARA
8
(UNICEF, 2013). According to Sai (1995) and UNICEF (2013), FGM is anact of violence that is committed against a woman or a girl, simply becauseshe was born female. It usually leads to physical, sexual, mental or emotion-al suffering to the woman with concomitant grievous negative effects on herhealth. In addition, FGM has been identified to be one of the leading culturalpractices responsible for high maternal and infant mortality in Nigeria (NPCand ICF Macro, 2004; 2009). Basically, there are three major conventionalforms of FGM identified by scholars in the literature. The first one is calledclitoridectomy, which is the least severe form of the practice. It involves thesurgical removal of the prepuce or the hook of the clitoris, leaving the clitorisitself and the posterior larger part of the minora. The second type is referredto as excision which consists of the removal of clitoris along with parts of thelabia minora or all of it. The third type is called infibulation and is consideredthe most severe form of the practice. It involves the removal of the clitoris,the labia minora and the adjacent medial part of labia majora in their anteriortwo-third. What makes it infibulation is that the two sides of the vulva arethen stitched together (generally using thorns, catcuts or a paste of egg, sugarand gum Arabic) leaving an opening the size of a pin head to allow for theflow of urine and menstrual blood (Toubia, 1993; Dawit, 1994; Centre forGender and Social Policy Studies, 1998; Rahman and Toubia, 2000; Odimeg-wu and Okemgbo, 2000; Shell-Duncan, 2008; UNFPA, 2011). The degree ofcutting is much extensive and often impairs a woman’s sexual and reproduc-tive function (Rahman and Toubia, 2000; Berg and Underland, 2013). Thethree forms of FGM still exist in the six-geopolitical zones of Nigeria, butthere is a variation in the nature, pattern and prevalence of each of themacross the regions (NPC and ICF Macro, 2004; 2009).
Different reasons had been adduced for the practice and continuation ofFGM in Nigeria. The reasons include: socio-cultural, psychological, hygien-ic, aesthetic/beautification and even religious values. For some communities,it is a component of a rite of passage to socially acceptable adulthood; whilefor others, it is a nuptial necessity. It is perceived as a way to curtail premar-ital sex and preserve virginity. It also reduces the female sexual demands onher husband and thus men can guaranty the paternity of their children mostespecially from their wives. As argued by Carr (1997), the cutting is believedto impart chastity and virtue. It safeguards the women against pre-and extra-marital sexual activities. Clitoridectomy diminishes sexual sensation whileinfibulation impedes sexual intercourse. Therefore, it is often posited thatFGM reduces sexual urge of a girl/woman and uncircumcised girls arebelieved to be promiscuous, will initiate sex early and will have high rate ofsexual activity (Odimegwu and Okemgbo, 2000; NPC, 2008).
In the past two decades, international organizations, development part-ners, United Nations (UN) agencies, state and non-state actors in Nigeria havebeen working vigorously through initiation, development and implementation
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
9
of various intervention programmes in the country in order to eradicate thisharmful traditional practice. In fact, various international conventions recog-nized FGM as violation of women’s basic right. Worthy of note is that the UNprinciples on women’s development are derived from human rights lawswhich are set out in various conventions, and include the principles of oppor-tunity for women as for men, and for girls as for boys. Women and girls areequally entitled to all fundamental human rights such as rights to life andreproductive health. Specifically, the preamble of Convention on the Elimina-tion of All Forms of Discrimination against Women (CEDAW) recalls that thebasic principles of the UN include faith in fundamental human rights, in thedignity of the human person, and the equal rights of men and women. Theseprinciples on human rights, quite apart from practical programme interest, aresufficient in themselves to justify an overriding programme interest in genderequality. Considering the central hypothesis of prevention of promiscuity andother social context of FGM in contemporary Nigerian society, this articleseeks answers to the following three research questions: first, what are theeffects of FGM on sexual behavior of women in the study location? Second,what are the relationships between women’s socio-demographic backgroundand FGM status of their daughters? Third, do socio-economic status of thewomen influence their plan to circumcise their daughters in the future? It isimperative to note that question two is referred to the current status of thedaughters, while question three is referred to the future (prospective orplanned) status of the daughters. These questions among other things wereanswered in this article.
2. PREVIOUS STUDIES
2.1 Introduction
In recent times, FGM has attracted a lot of interests among scholars,human right activists, and feminists for obvious reasons; some of which areinterconnected and have compelled many researchers and human right activiststo conduct studies on possible effects of female circumcision on sexual pleas-ure of married women and their spouses, as well as the long term health impli-cations of such an act (Shell-Duncan and Hernlund, 2000; Weil-Curiel andTemmerman, 2007; Berg et al., 2010). Many scholars (Weil-Curiel and Tem-merman, 2007; Berg and Underland, 2013) are of the opinion that FGM is aform of discrimination directed at the female gender. The main aim of this sec-tion is to document the state of knowledge on FGM in the literature in order toidentify the essential lacuna in knowledge for this study to fill. Thus, this liter-ature review has been grouped under three thematic sub-sections namely: inci-dence and prevalence of FGM, Causes of FGM and consequences of FGM.
2.2 Incidence and prevalence of FGM
It has been noted that FGM now exists in many countries of the world, notonly because of ethnic background or religious affiliation, but it cuts acrossinternational boundaries (Hedley and Dockenoo, 1992). Emmanuel (1998)described FGM as an extreme example of the general subjugation of women inAfrica because it is one, in which the health and welfare of women suffer a long-term adverse effect. FGM is seen as one of the manifestations of gender-basedhuman rights violations, which aims to control women’s sexuality and autono-my (Adebayo, 1992). This practice dates back to the era of the pharaohs ofancient Egypt and although it is deeply field to cultural and traditional beliefs, ithas no regard for the dangers and sufferings posed to the health of its victims(Heise, 1993). The nature of the ‘operation’ varies from one country to anotherand from one ethnic group to another. In Nigeria, it may be performed on neona-tal, infant, pubertal, pregnant or post-partum women. Considering the culturalcontext of the practice, Adebayo (1992) argued that even though there is no the-ological basis for the practice of FGM, it will be hard to eradicate until we havea better understanding of the cultural beliefs. Omolade (1992) argues that FGMis widespread among the various ethnic groups in Nigeria. It is one cultural ortraditional practice which has not been significantly influenced either by theincrease in the level of literacy or of growing modern Muslim and Christian val-ues. According to this scholar, of the six largest ethnic groups in Nigeria - theYoruba, Hausa, Fulani, Ibo, Ijaw, and Kanuri - only the Fulani do not practiceFGM. In other words, it is a practice that is still prevailing in the country.
2.3 Causes of FGM
Different reasons have been advanced for the prevalence of the culturaltradition of FGM in the various studies that have been carried out on the sub-ject across Nigeria (Apena, 1980; Emmanuel, 1998; Odimegwu and Okemg-bo, 2000; NPC, 2008). For some communities, it is a component of a rite ofpassage to socially acceptable standard of adulthood while for others it is anuptial necessity. Yet for others, it is a mark of courage, especially where it iscarried out on older people. Whatever reasons are preferred for this practice,it has been medically and scientifically proven that there is no immediate andremote benefit or advantage to the victims of FGM (Ibhawoh, 1999). Thisauthor further noted that FGM is a major human rights issue, not just a healthconcern. This is because reducing FGM to a health issue only would be like“treating symptoms”; victims only suffer health complications as a conse-quence of the mutilation. Culturally, it is believed that the act of mutilation ofthe girl child is performed for some beliefs and reasons which are to reducethe female libido in order to prevent promiscuity, enhance sexual pleasure of
OYEFARA
10
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
11
man, cultural ritual that females should undergo before marriage, it couldhave an esthetic/beautification value on the girl and prevent pain during inter-course, it could have cause death of a child if the clitoris is allowed to touchthe baby’s head during childbirth and a man can become impotent if the penistouches the head of the clitoris. These reasons revealed that FGM is beenpracticed because of the need to control women’s sexuality.
2.4 Consequences of FGM
FGM is an act that invariably results in physical, sexual or emotional suf-fering to the woman (United Nations General Assembly, 1981). It is an oldharmful traditional practice in Nigeria that affects the reproductive health ofgirls and women. Toubia (1993) believes that female circumcision raisesnumerous human right issues, including reproductive rights, the protectionfrom violence, women’s rights and especially children’s rights since most cir-cumcisions take place on girls who are four to ten years of age who have nosay in the matter. Centre for Gender and Social Policy Studies (1998) in a sur-vey report showed that “lack of interest in sex” was the top sexual problem ofcouples especially on the part of women. There are a variety of myths sur-rounding female genital mutilation in Nigeria, among the proverbs which areused to underscore the myths are “the clitoris is the cap of prostitution whichthe vagina wears from heaven. If we do not clip the clitoris young, it is goingto be asking for great sacrifice from the penis when it grows up”. However,other reports argue that lack of sexual interest and sexual orgasm or climaxare parts of the major aftermaths of female genital mutilation and that lack ofsexual interest specifically makes it almost impossible for the women affect-ed to climax or attain sexual orgasm (Apena, 1980, Emmanuel, 1998; Rah-man and Toubia, 2000, Idomu, 2009; Mohammed and Ahmed, 2000; Osi-nowo and Taiwo, 2003; Huston, 2006; Olurode and Oyefara, 2010).
It should be noted that with FGM, complications are common and canlead to death. According to Hosken (1993), the highest maternal and infantmortality rates in the globe are in FGM-practicing regions of the world. Inareas of the Sudan, for example, where antibiotics are not available, it wasestimated that one-third of the girls undergoing FGM die (Women’s PolicyInc., 1996). Conservative estimates suggest that, more than one millionwomen in Central African Republic (CAR), Egypt, and Eritrea, the only coun-tries where such are available, experienced adverse health effects from FGM(Shell-Duncan and Hernlund, 2000). One quarter of women in CAR and 1/5of women in Eritrea reported FGM-related complications and in an areawhere medical facilities are ill-equipped; emergencies arising from the prac-tice cannot be treated. Thus, a child who develops uncontrolled bleeding orinfection after FGM may die within hours (Koso-Thomas, 1987; WHO,
OYEFARA
12
2001). According to Koso-Thomas (1987), women who have undergoneFGM are twice as likely to die during childbirth and are more likely to givebirth to a still born child than other women. He argues further that obstructedlabour can also cause brain damage to the infant and complications for themother (including fistula formation, an abnormal opening between the vagi-na and the bladder or the vagina and the rectum, which can lead to inconti-nence. Shell-Duncan (2008) and UNAIDS & WHO (2013) had argued that inaddition to the direct consequences of bleeding, there is the ever present riskof infection, especially tetanus or HIV/AIDS. This is because most times, thesame knives used on a girl are used on as many as are brought for the ritualon a particular day or occasion, often without proper or no sterilization ofsuch knives. In the event of infection which sometimes leads to death or dis-ability, the operators explain the disaster away as judgment from the gods forsome imaginary wrong or offense that the female or one of the parents mighthave committed (Omolade, 1992).
Omolade argues further that besides these, there is also the grave danger ofdamage to other organs of the female system. It has also been established thatFGM can also cause infertility in women. Mohammed (1989) reported that inSudan, 20-25 per cent of female infertility has been attributed to FGM compli-cations. Some researchers describe the psychological effects of FGM as rang-ing from anxiety to severe depression and psychosomatic illness (Toubia,1993). Many children exhibit behavioural changes after FGM, but problemsmay not be evident until the child reaches adulthood. It is imperative to note thatthere is paucity of studies on the possibility of intergenerational continuation ofthe practice and rigorous test of the theory of FGM and prevention of promis-cuity among women in Nigeria. This article examines these areas among otherintricacies that surround FGM in the study location.
3. RESEARCH METHODS
3.1 Research design and study setting
The study location is Oworonshoki community in Kosofe Local Govern-ment Area (LGA) of Lagos State, Southwestern Nigeria. Oworonshoki is locat-ed within the mainland part of Lagos State. Up north, the study location shareboundaries with Bariga Local Council Development Area. The lagoon is situat-ed at the western part of Oworonshoki community while it shares boundarieswith Ifako and Ogudu at the east and south respectively. Oworonshoki can belinked through land and water transport systems. The lagoon connects Oworon-shoki and Lagos Island together. The study location has as its inhabitants peoplefrom various ethnic and religious groups which include Yoruba, Ibo, Hausa, andother ethnic minorities in Nigeria. The community also comprises Muslims,
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
13
Christians and Traditional worshippers as there are mosques, churches, andshrines in the area. It is important to note that Oworonshoki is owned and pre-dominantly occupied by the Yoruba. The traditional ruler - Oloworo ofOworonshoki - upholds and maintains the Yoruba traditions. Oworonshoki ismainly a residential area with highly educated people, averagely educated,and illiterates living in the community. The economic activities of the peopleinclude fishing, sand extraction, petty trading, craftsmen, artisans and thosewho engage in the civil service. As a result of this, Oworonshoki is a hetero-geneous population with diverse views and beliefs on the subject matter. Asat 2013, Oworonshoki community has an estimated population of about202,972 with 111 streets and two geographical distribution spanning intoareas/wards A and B as divided by a major road named Oworo road. A non-experimental research design was employed to elicit data on the objectives ofthe study from the respondents. In the design, cross-sectional survey researchmethod was adopted to generate quantitative data.
3.2 Study population and sample size determination
The study population comprised of ever-married women from ages 20years and above in the study location. In order to have a representative sam-ple size for the cross-sectional survey, a statistical formula was used and 345participants came out to be representative of the estimated population. How-ever, a total of 360 questionnaires were administered considering expectedcases of invalid questionnaires due to incomplete response, inconsistency inthe responses or a total no response from the respondents. At the end of thequestionnaire administration, a total of 350 questionnaires were found usablefor the study. Thus, the non-responses and incomplete responses constituteabout 2.8 percent of the total questionnaires administered.
3.3 Sampling method
To select respondents for the cross-sectional survey, a multi-stage ran-dom sampling technique was adopted. It is imperative to note that Oworon-shoki community consists of two wards (i.e. ward A and B) and 111 streets.The multi-stage random sampling technique adopted involves a total of fourstages before eligible respondents were selected for the study. Stage 1involves strategic sub-division of the community into two existing geo-polit-ical wards A and B. The two wards were included in the study and formed twostrata from where the sample was drawn. In the second stage, a systematicrandom sampling method was used to select 14 streets from the two wards forthe study. Specifically, 6 streets were randomly sampled from ward A, and 8streets were also randomly sampled from ward B. The number of streets sam-
OYEFARA
14
pled per ward was made to be proportional to the estimated population andstreets per ward. The third stage consisted of numbering and sampling ofhouses and households in the selected streets. Considering total number ofhouses and household per street and average of 25 respondents to be sampledper street, a sampling interval was developed for each street to guide the ran-dom sampling of eligible respondents in each of the streets. The fourth andfinal stage of the multistage sampling method was the sampling of the respon-dent in each of the identified houses and households at stage three. In case ofplural eligible respondents per household, simple random method was used toselect one respondent per household. In all, for the valid returned question-naires used in the analysis, a total of 150 ever-married women were sampledfrom ward A, while another 200 were sampled from ward B. it is imperativeto note that the women were interview alone without the presence of theirhusbands. Thus, 350 questionnaires were found to valid returned instrumentsfor further analysis.
3.4 Research instrument and data collection
A questionnaire was developed to elicit data from respondents. The ques-tionnaire was designed in such a way that adequate information was collect-ed on the research questions with a view to actualizing the purpose and objec-tives of the study. Specifically, the questionnaire consists of 68 questions thatwere sub-divided into eight subsections. Section one consists of questions onsocio-demographic background of the participants. In section two were ques-tions on marital history; while in the third section questions on issues aroundfemale genital mutilation were asked. Section four consists of questions onsexual initiation. Questions on sexual activity and sexual satisfaction wereasked in section five and six respectively. Section seven and eight consist ofquestions on fertility history and marital harmony of the respondents respec-tively. The fieldwork activities of the study were carried out between July andSeptember in the year 2012. Eight female research assistants were recruitedand trained in addition to the principal researcher to conduct the study.
3.5 Dependent and independent variables
There are three major outcome variables in this study. These are: 1)mother’s sexual behaviour, 2) daughters’ circumcision status and 3) mother’splan to circumcise daughters in the future. Sexual behaviour was measuredwith other five sub-indicators which are: having sexual desire, ever had extra-marital sexual affair, frequency of sexual initiation, number of sexual inter-course in the last 30 days and ever reach orgasm during sexual intercourse.The synthesis of these sub-indicators was used to measure the sexual behav-
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
15
iour of the respondents in the study location. The second outcome variable isthe daughters’ circumcision status. This was assessed by maternal history ofher daughters’ circumcision status; a daughter was said to be circumcised ifshe had experienced any of the three forms of FGM (i.e. clitoridectomy, exci-sion or infibulation). The third outcome variable is whether the mother plansto circumcise her daughters in the future. It was measured as a dichotomousvariable where a respondent can either answer yes or no. The main explana-tory variables of this study are women’s socio-demographic characteristicsand their FGM status. In all, a total of 6 variables were used as explanatoryvariables for both bivariate and multivariate analysis. The variables are: agegroup, education, religion, ethnic background, form of marriage and FGMstatus of the respondent.
3.6 Study limitations and ethical issues
The major constraint of the study was the fact that many of the womenwere not ready to be interviewed due to their claims that they were very busywith their economic activities. In addition, the women had poor memoryabout the exact time they were circumcised. It is important to note that humanhistory is prone to certain level of error. In spite of these constraints and lim-itations, efforts were made to generate both reliable and valid data for thestudy. Considering the medical and social implications of the topic of thestudy on the respondents, some ethical factors were considered and imple-mented during the period of data collection. The first ethical issue is the factthat all respondents were promised total confidentiality of the informationprovided. In addition, there was an “informed consent” form which each ofthe respondents read through (and interpreted to the illiterate ones) in order tounderstand the purpose and objectives of the study and finally signed beforethe commencement of each interview. Furthermore, respondents were com-pletely anonymous in relation to their responses.
3.7 Data processing and analysis
The adopted research design and method produced mainly quantitativedata for the study. Consequently, quantitative methods of data analysis wereused in the study. The returned questionnaires were screened and edited forpossible errors, while open-ended questions were coded. After the coding, thereturned questionnaires were entered into computer for further analysisthrough Statistical Package for Social Sciences (SPSS) version 16.0. It isimperative to note that quantitative research method seeks to statisticallyappraise observable behaviour with a view to providing a coherent explana-tion to its findings. Thus, the analysis of the collected data was done at three
OYEFARA
16
levels: i) univariate analysis, ii) bivariate analysis, and iii) multivariate analysis.The univariate analysis consists of frequency distributions, percentages andmodes; bivariate analysis involves the use of chi-square (�2) to examine rela-tionships between outcome variable and various explanatory variables, whilemultivariate analysis consist of one logistic regression model on outcome andexplanatory variables. Furthermore, the 95% confidence interval (CI) wasadded to the Odds ratios in the interpretation of the logistic regression model. Itis important to note that the bivariate analysis examines relationship betweenthe outcome variable and the explanatory variables taken one at a time, where-as multivariate analysis examines relationship between the outcome variableand the explanatory variables taken all the variables at a time.
4. RESEARCH FINDINGS
This section deals with the organization, presentation, analysis and inter-pretation of data collected from the field. As stated earlier, quantitative datawere analyzed at univariate, bivariate and multivariate levels. The univariateanalysis involved data on socio-demographic profile, marital history anddynamics, and FGM knowledge, incidence and prevalence; while bivariateanalysis consists of women FGM status and sexual behavior, women socio-demographic background and their daughters’ circumcision status, andwomen socio-economic status and their plan to circumcise their daughters inthe future. At the multivariate level, various socio-demographic status of themothers were regressed against their daughters FGM status in order to see ifthose factors that were significant at bivariate level will also be significant atmultivariate level after controlling for other exigency factors. These sub-sec-tions are presented below accordingly:
4.1 Socio-demographic profile of respondents
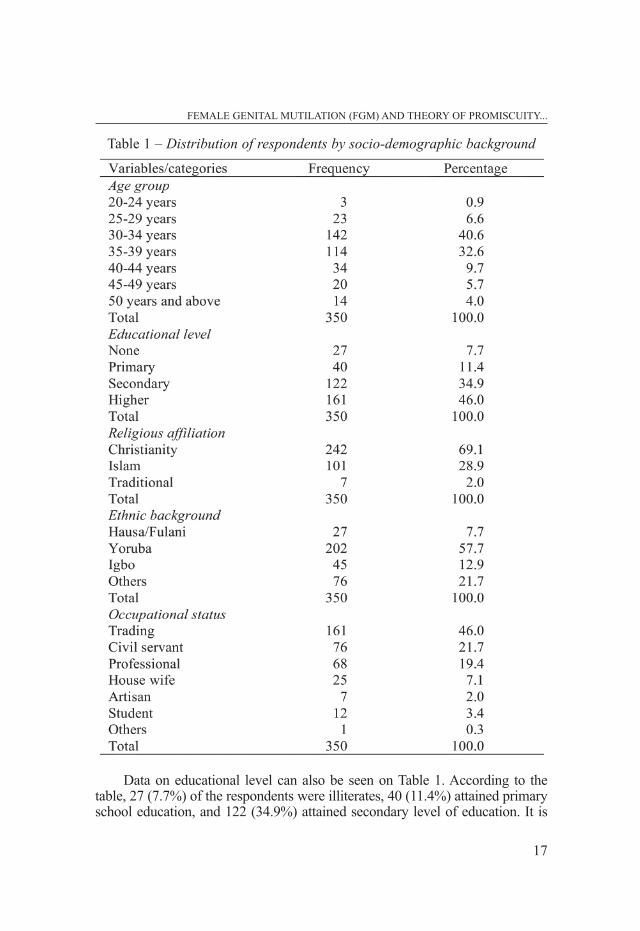
Data on socio-demographic profile of the respondents can be seen onTable 1 below. As presented on the table, 3 (0.9%) of the respondents werebetween the age group of 20-24 years, 23 (6.6%) were between age group 25-29 years, 34 (9.7%) of the respondents fell within the age bracket 40-44 years,while 20 (5.7%) were in age group 45-49 years. Furthermore, 14 (4%) were50 years and above. It is imperative to note that 257 (73.2%) were betweenage 30 and 39 years. Specifically, the dominant age group was age group 30-34 years with 142 respondents constituting 40.6 percent of the total respon-dents. This was followed by age group 35-39 years with 114 respondents con-stituting 32.6 percent of the respondents. Thus, it can be adduced that major-ity (73.2%) of the respondents were in the mid-period of their reproductiveyears with the expected high reproductive activities.
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
17
Data on educational level can also be seen on Table 1. According to thetable, 27 (7.7%) of the respondents were illiterates, 40 (11.4%) attained primaryschool education, and 122 (34.9%) attained secondary level of education. It is
Table 1 – Distribution of respondents by socio-demographic background
OYEFARA
18
instructive to note that a total of 161 (46 %) of the respondents acquired high-er level of education. Elicited data therefore reveal that more of the respon-dents were people with higher level of education. The percentage distributionof respondents by religion reveals that majority of the sampled populationwere Christians. Specifically, 242 (69.1%) of the respondents were Chris-tians. This was closely followed by the Muslims with 101 respondents consti-tuting 28.9 percent of the respondents. It is also important to note that tradi-tional worshippers constituted just 7 respondents which was about 2.0 percentof the total respondents. This suggests dominancy of Christianity and Islam inthe study location.
The distribution of respondents by ethnic group reveals that majority of therespondents were Yoruba with 57.7 percent, followed by the Ibos with 12.9 per-cent, and the Hausas with 7.7 percent, while 21.7 percent of the respondentswere from other ethnic minority groups in the country. This shows that signifi-cant number of the population in the study area were Yoruba. This is not unex-pected since the study was carried out in a Yoruba settlement. Occupational datareveal that majority of the respondents (46%) were traders. This was closely fol-lowed by civil servants with 21.7 percent. Professionals were 19.4 percent andhousewives 7.1 percent. In addition, a total of 2 percent of the respondents wereartisans, while 3.4 percent were students. It can be deduced from the occupa-tional data that high number of the sample were gainfully employed. Thisreflects the reality of financial requirements in family upkeep in contemporaryNigerian society since the introduction of structural adjustment programmes(SAP) on the 26th September, 1986. This reality requires men as well as womento work possibly outside home in order to make ends meet in family financialmaintenance and upkeep. Thus, women being full housewives and home keep-ers are gradually becoming unpopular and unacceptable in the country.
4.2 Marriage history and dynamics
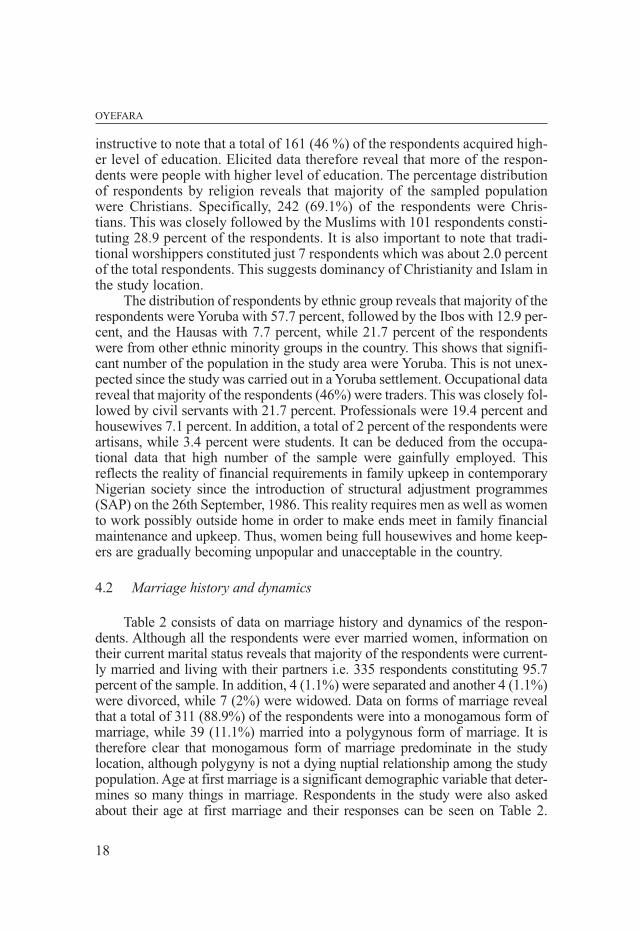
Table 2 consists of data on marriage history and dynamics of the respon-dents. Although all the respondents were ever married women, information ontheir current marital status reveals that majority of the respondents were current-ly married and living with their partners i.e. 335 respondents constituting 95.7percent of the sample. In addition, 4 (1.1%) were separated and another 4 (1.1%)were divorced, while 7 (2%) were widowed. Data on forms of marriage revealthat a total of 311 (88.9%) of the respondents were into a monogamous form ofmarriage, while 39 (11.1%) married into a polygynous form of marriage. It istherefore clear that monogamous form of marriage predominate in the studylocation, although polygyny is not a dying nuptial relationship among the studypopulation. Age at first marriage is a significant demographic variable that deter-mines so many things in marriage. Respondents in the study were also askedabout their age at first marriage and their responses can be seen on Table 2.
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
19
As presented in the table, marriage rarely comes before age 25 yearsamong women in the study location. Specifically, about 10.0 percent of therespondents got married between ages 15 and 19 years, 12.9 percent betweenages 20 and 24 years, while 71.1 percent between ages 25 and 29 years. Inaddition, what can be term as late marriage is minimal among women in thestudy location as only 21 (6.0%) got married between ages 30 and 34 years. Itis imperative to note that marital dissolution was minimal in the study location,and in case of dissolution, there seems to be a quick re-marriage leaving sig-nificant number of ever married women in conjugal union in most aspect oftheir reproductive life-span. Specifically, only 38 (10.9%) had married morethan once and only 8 (2.2%) were out of marital union as a result of either sep-
Table 2 – Distribution of respondents by nuptial/marital history
OYEFARA
20
aration or divorce as at the time of the study. In addition, significant number,i.e. 31 (81.6%) of the dissolution of first marriage was due to death of spouseand many of the widows had re-married since only 7 (2.0%) claimed to bewidow as at the time of the survey.
4.3 FGM knowledge, incidence and prevalence
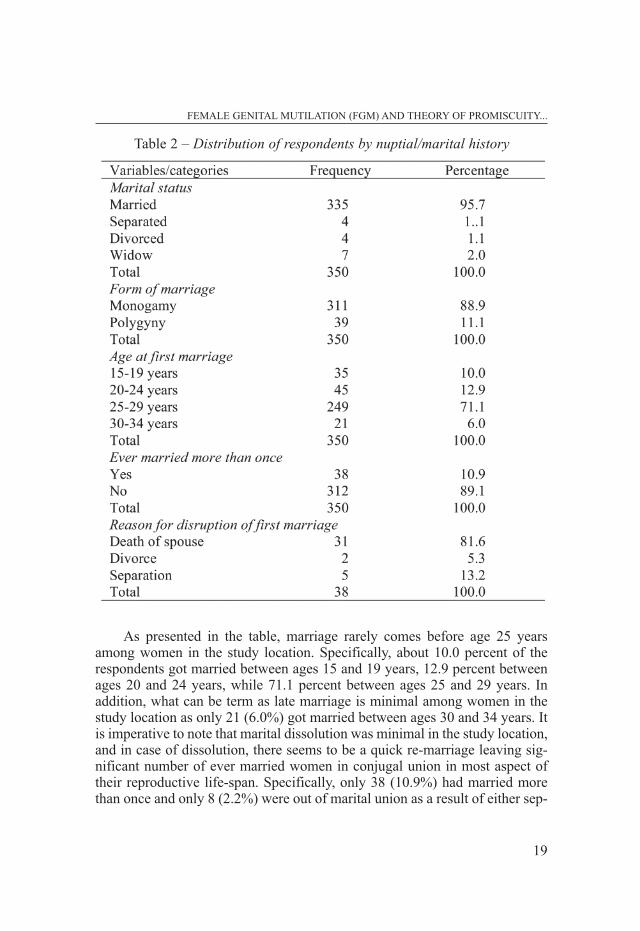
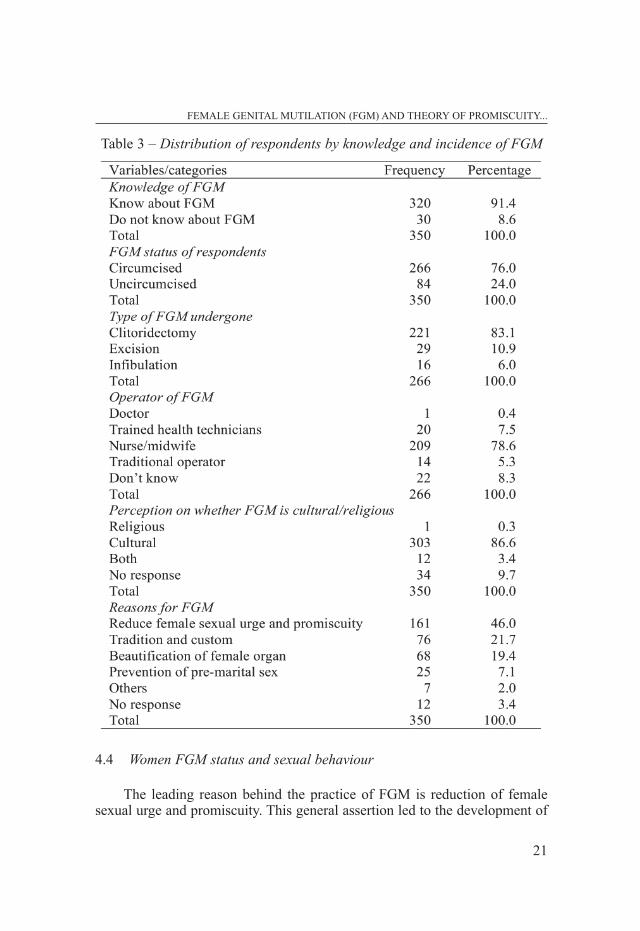
Data on Table 3 involve information on knowledge, prevalence andforms of FGM among women in the study location. As presented in thetable, the knowledge of FGM is widespread in the study location as 320(91.4%) of the respondent acknowledged that they know that FGM exist intheir community, while only 30 (8.6%) stated that they did not know aboutthe existence of FGM. Respondents were further asked about their FGMstatus, 266 (76.0%) claimed that they were circumcised, while 84 (24%)stated that they were not circumcised. This suggests high prevalence ofFGM among the generation of women in the study location. Other probequestion was to document the nature of FGM undergone by each of thewomen that were circumcised. Responses to this question reveal that cli-toridectomy predominates among women in the study location. Particular-ly, 221 (83.1%) of ever circumcised women had clitoridectomy, 29 (10.9%)had excision, while 16 (6.0%) had infibulation. The operators of FGM in thestudy location range from medical doctors, to trained health technicians,nurses/midwives, and traditional operators. Specifically, 209 (78.6%) of theFGM were performed by nurses/midwives, 20 (7.5%) by trained healthtechnicians, 14 (5.3%) by traditional operators, 1 (0.4%) by medical doctor,while 22 (8.3%) of ever circumcised women did not know who actually per-formed FGM for them.
Respondents were asked about their opinion on whether FGM is cultur-al or religious practice, responses to the question on Table 3 revealed that 303(86.6%) of the women believed that FGM was a cultural practice, 1 (0.3%)stated that it was a religious practice, while 12 (3.4%) claimed that the prac-tice was both religious and cultural. Respondents adduced various reasons forthe practice of FGM in the study location. As presented in the table, 215(61.4%) mentioned reduction of female sexual urge and promiscuity, 52(14.9%) mentioned beautification of female sexual organ, 35 (10.0%) men-tioned avoidance of pre-marital sex, 13 (3.7%) mentioned tradition and cus-tom, while 3 (0.9%) mentioned other reasons such as prevention of still birthand keeping women pure. It is important to note that 32 (9.1%) of the respon-dents did not respond to the question.
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
21
4.4 Women FGM status and sexual behaviour
The leading reason behind the practice of FGM is reduction of femalesexual urge and promiscuity. This general assertion led to the development of
Table 3 – Distribution of respondents by knowledge and incidence of FGM
OYEFARA
22
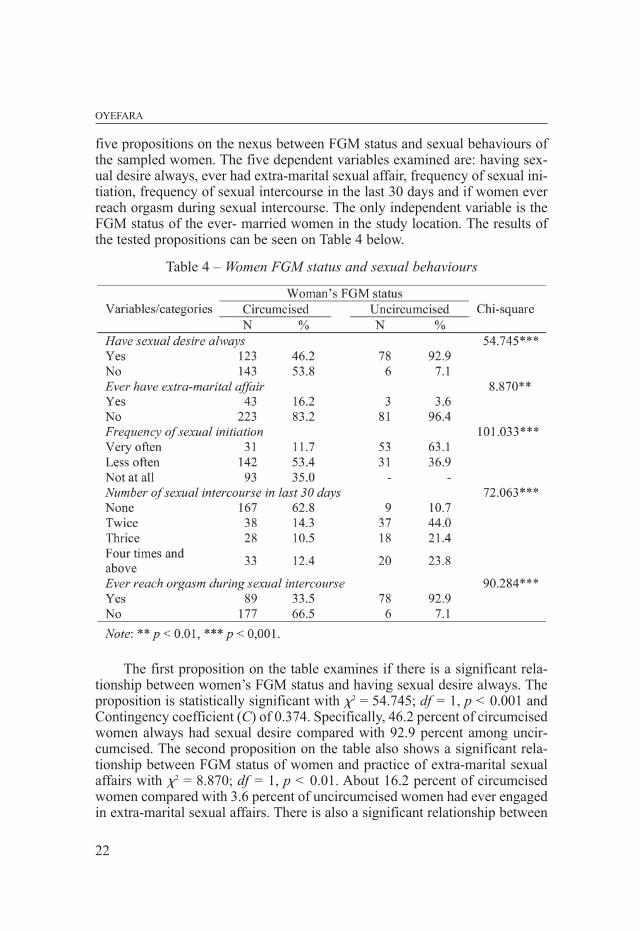
five propositions on the nexus between FGM status and sexual behaviours ofthe sampled women. The five dependent variables examined are: having sex-ual desire always, ever had extra-marital sexual affair, frequency of sexual ini-tiation, frequency of sexual intercourse in the last 30 days and if women everreach orgasm during sexual intercourse. The only independent variable is theFGM status of the ever- married women in the study location. The results ofthe tested propositions can be seen on Table 4 below.
The first proposition on the table examines if there is a significant rela-tionship between women’s FGM status and having sexual desire always. Theproposition is statistically significant with �2 = 54.745; df = 1, p < 0.001 andContingency coefficient (C) of 0.374. Specifically, 46.2 percent of circumcisedwomen always had sexual desire compared with 92.9 percent among uncir-cumcised. The second proposition on the table also shows a significant rela-tionship between FGM status of women and practice of extra-marital sexualaffairs with �2 = 8.870; df = 1, p < 0.01. About 16.2 percent of circumcisedwomen compared with 3.6 percent of uncircumcised women had ever engagedin extra-marital sexual affairs. There is also a significant relationship between
Table 4 – Women FGM status and sexual behaviours
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
23
women FGM status and frequency of sexual initiation by the women with �2
= 101.033; df = 2, p < 0.001. Data on the table show that only 11.7 percent ofcircumcised women as against 63.1 percent of uncircumcised women veryoften initiate sexual intercourse with their husbands in the study location. FGMstatus of the respondents has significant relationship with frequency of sexualintercourse in last 30 days before the survey with �2 = 72.063; df = 3, p <0.001. Specifically, about 62.8 percent of circumcised women compared with10.7 percent of uncircumcised women did not have sexual intercourse withtheir husbands in the last 30 days before the survey. There is also a significantrelationship between FGM status and women reaching orgasm during sexualintercourse with �2 = 90.284; df = 1, p < 0.001. As presented in the table, 33.5percent of circumcised women compared with 92.9 percent of uncircumcisedwomen used to reach orgasm during sexual intercourse in the study location.
4.5 Women socio-demographic background and their daughters’circumcisionstatus
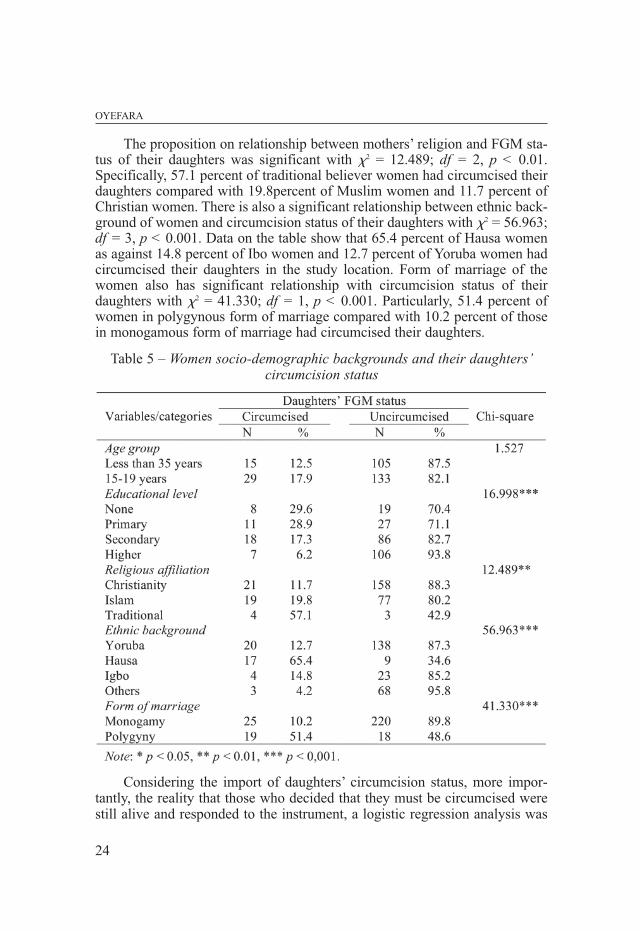
This section and the next examine possible intergenerational change in theprevalence of FGM between mothers and their daughters on one hand, and theinfluence of mothers’ socio-demographic factors on their daughters’ FGM statusin the study location, on the other hand. On Table 5 below, five propositions weretested on the relationship between maternal socio-demographic factors and cir-cumcision status of their daughters in the study location. The five maternal inde-pendent variables are: mothers’ age group, level of education, religious affilia-tion, ethnic background and form of marriage. The only dependent variable is theFGM status of their daughters. The results of the tested propositions can be seenon Table 5. The first proposition examines if there is a significant relationshipbetween women’s age group and FGM status of their daughters. The propositionis not statistically significant with �2 = 1.527; df = 1, p > 0.05 after the age groupwas recorded into two groups. The data suggest that irrespective of age group ofthe mother (young or old), daughters’ circumcision cuts across all the age groupsin the study location. A critical examination of the data reveals a pocket of FGMamong daughters of women across age groups, even among young women intheir early twenties. There is a significant relationship between mothers’ level ofeducation and circumcision of their daughters with �2 = 16.998; df = 3, p <0.001. The percentage distribution reveals a negative relationship between levelof education and daughters’ female circumcision. That is, the higher the level ofeducation of the women, the lower the probability of daughters circumcision.Specifically, 29.6 percent of women without any formal education had circum-cised their daughters compared with 28.9 percent among women with primaryeducation, 17.3 percent among women with secondary education and 6.2 percentamong women with higher education.
The proposition on relationship between mothers’ religion and FGM sta-tus of their daughters was significant with �2 = 12.489; df = 2, p < 0.01.Specifically, 57.1 percent of traditional believer women had circumcised theirdaughters compared with 19.8percent of Muslim women and 11.7 percent ofChristian women. There is also a significant relationship between ethnic back-ground of women and circumcision status of their daughters with �2 = 56.963;df = 3, p < 0.001. Data on the table show that 65.4 percent of Hausa womenas against 14.8 percent of Ibo women and 12.7 percent of Yoruba women hadcircumcised their daughters in the study location. Form of marriage of thewomen also has significant relationship with circumcision status of theirdaughters with �2 = 41.330; df = 1, p < 0.001. Particularly, 51.4 percent ofwomen in polygynous form of marriage compared with 10.2 percent of thosein monogamous form of marriage had circumcised their daughters.
Considering the import of daughters’ circumcision status, more impor-tantly, the reality that those who decided that they must be circumcised werestill alive and responded to the instrument, a logistic regression analysis was
OYEFARA
24
Table 5 – Women socio-demographic backgrounds and their daughters’circumcision status
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
25
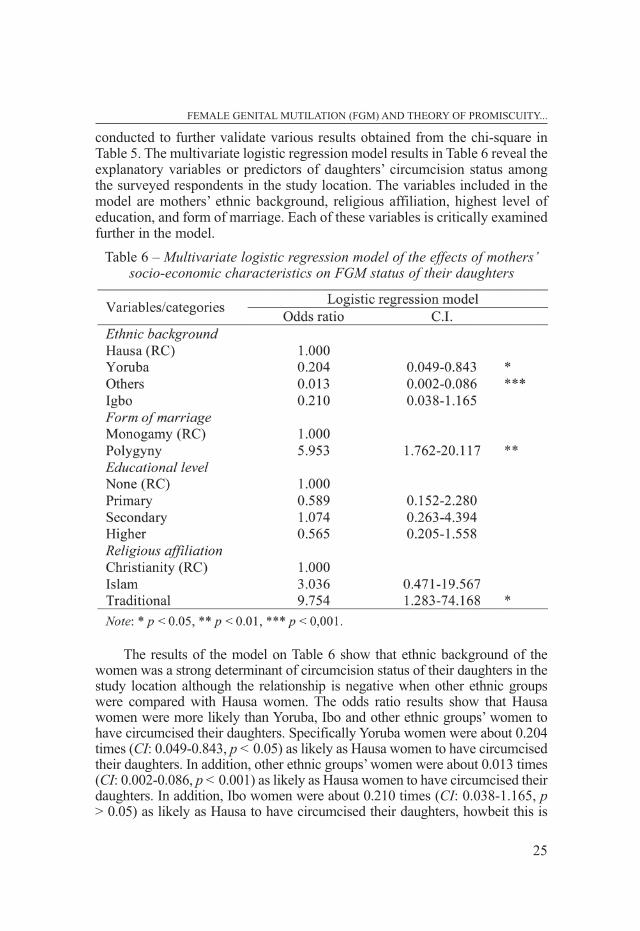
conducted to further validate various results obtained from the chi-square inTable 5. The multivariate logistic regression model results in Table 6 reveal theexplanatory variables or predictors of daughters’ circumcision status amongthe surveyed respondents in the study location. The variables included in themodel are mothers’ ethnic background, religious affiliation, highest level ofeducation, and form of marriage. Each of these variables is critically examinedfurther in the model.
The results of the model on Table 6 show that ethnic background of thewomen was a strong determinant of circumcision status of their daughters in thestudy location although the relationship is negative when other ethnic groupswere compared with Hausa women. The odds ratio results show that Hausawomen were more likely than Yoruba, Ibo and other ethnic groups’ women tohave circumcised their daughters. Specifically Yoruba women were about 0.204times (CI: 0.049-0.843, p < 0.05) as likely as Hausa women to have circumcisedtheir daughters. In addition, other ethnic groups’ women were about 0.013 times(CI: 0.002-0.086, p < 0.001) as likely as Hausa women to have circumcised theirdaughters. In addition, Ibo women were about 0.210 times (CI: 0.038-1.165, p> 0.05) as likely as Hausa to have circumcised their daughters, howbeit this is
Table 6 – Multivariate logistic regression model of the effects of mothers’socio-economic characteristics on FGM status of their daughters
not statistically significant even at p < 0.05. Respondents were asked about theirform of marriage in order to know the degree of association on daughters’ cir-cumcision status based on women’s form of marriage in the study area. The oddsratio of multivariate logistic regression show a high prevalence rate of daughters’circumcision among women in polygynous form of marriage compared withthose ones in monogamous form of marriage. In particular, the results showedthat daughters of women in polygynous form of marriage were about 5.953times (CI: 1.762-20.117, p < 0.01) as likely as daughters of women in monoga-mous form of marriage to have been circumcised. This identified relationship issignificant at 0.01 level of significance. This finding revealed the significantinfluence of women’s form of marriage on circumcision status of their daughtersin the study location.
The results of the multivariate model on Table 6 show that women withhigher level of education were less likely to circumcise their daughters comparedwith other levels of education. This relationship can be explained as follows: incomparison with women with no formal education, primary education and sec-ondary education, women with higher level of education are less likely to havetheir daughters circumcised, although this relationship is not statistically signif-icant at 0.05 level of significance in the multivariate logistic level. On the rela-tionship between religious affiliation of the women and their daughters’ circum-cision status, the multivariate logistic regression analysis shows a significant sta-tistical relationship among the variables in the study location. The odds ratiofrom the model shows that Muslim women were about 3.036 times (CI: 0.471-19.567, p > 0.05) as likely as Christian women to have circumcised their daugh-ters, while women that were affiliated into the traditional religions were about9.754 times (CI: 1.283-74.168, p < 0.05) as likely Christian women to have cir-cumcised their daughters; the later relationship was statistically significant at0.05 level of significance.
4.6 Women socio-economic status and plan to circumcise their daughters in future
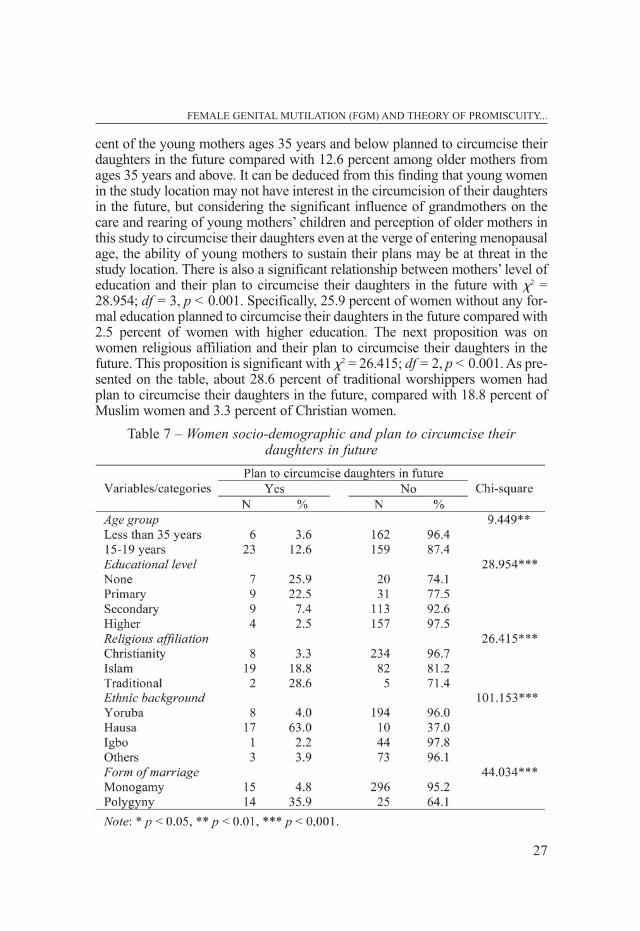
The relationship between women socio-economic status and their plan tocircumcise their daughters in future was examined in this section. Like preced-ing section, five propositions were tested on maternal socio-economic factorsand their plan to circumcise their daughters in future. The five maternal inde-pendent variables are: mothers’ age group, level of education, religious affilia-tion, ethnic background and form of marriage. The only dependent variable is theplan of the mothers to circumcise their daughters in the future. The findings ofthese relationships can be seen on Table 7. Data on Table 7 show a significantrelationship between women’s age group and their plan to circumcise theirdaughters in the future. The hypothesis is statistically significant with �2 = 9.449;df = 1, p < 0.01 and Contingency coefficient (C) of 0.162. Particularly, 3.6 per-
OYEFARA
26
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
27
cent of the young mothers ages 35 years and below planned to circumcise theirdaughters in the future compared with 12.6 percent among older mothers fromages 35 years and above. It can be deduced from this finding that young womenin the study location may not have interest in the circumcision of their daughtersin the future, but considering the significant influence of grandmothers on thecare and rearing of young mothers’ children and perception of older mothers inthis study to circumcise their daughters even at the verge of entering menopausalage, the ability of young mothers to sustain their plans may be at threat in thestudy location. There is also a significant relationship between mothers’ level ofeducation and their plan to circumcise their daughters in the future with �2 =28.954; df = 3, p < 0.001. Specifically, 25.9 percent of women without any for-mal education planned to circumcise their daughters in the future compared with2.5 percent of women with higher education. The next proposition was onwomen religious affiliation and their plan to circumcise their daughters in thefuture. This proposition is significant with �2 = 26.415; df = 2, p < 0.001. As pre-sented on the table, about 28.6 percent of traditional worshippers women hadplan to circumcise their daughters in the future, compared with 18.8 percent ofMuslim women and 3.3 percent of Christian women.
Table 7 – Women socio-demographic and plan to circumcise their daughters in future
There is also a significant relationship between ethnic background ofwomen and their plan to circumcise their daughters in the future with �2 =101.153; df = 3, p < 0.001. Data on the table show that 63.0 percent of Hausawomen as against 4.0 percent of Yoruba women and 2.2 percent of Ibowomen had plan to circumcise their daughters in the future in the study loca-tion. Form of marriage of the respondents has significant relationship withtheir plan to circumcise their daughters in the future with �2 = 44.034; df = 1,p < 0.001. About 35.9 percent of women in polygynous union, compared with4.8 percent of women in monogamous union, had intension to circumcisetheir daughters in the future.
5. DISCUSSION OF FINDINGS AND CONCLUSION
In summary, the knowledge of FGM is widespread in the study locationand high proportion of the respondents claimed that they were circumcised.This suggests high prevalence of FGM among the generation of women in thestudy location. Data on types of FGD in the location reveal that clitoridectomypredominates among women in the study location followed by excision, andinfibulation respectively. The operators of FGM in the study location rangefrom medical doctors, to trained health technicians, nurses/midwives, and tra-ditional operators. The general believe of the women in the study location wasthat FGM is a cultural practice and they adduced various reasons for the prac-tice of FGM in the study location as: reduction of female sexual urge andpromiscuity, beautification of female sexual organ, avoidance of pre-maritalsex, tradition/custom, and other reasons such as prevention of still birth andkeeping women pure. Bivariate analysis reveals that a significant negativerelationship between women’s FGM status and various sexual indicators vari-ables such as having sexual desire always, practice of extra-marital sexualaffairs, frequency of sexual initiation, frequency of sexual intercourse in last30 days before the survey, and probability that a woman will reach orgasm dur-ing sexual intercourse. The second bivariate analysis reveals a significant rela-tionship between women’s level of education, ethnic background, form of mar-riage and FGM status of their daughters. The third bivariate analysis also showa significant relationship between women’s age group, level of education, reli-gious affiliation, ethnic background, form of marriage and their plan to circum-cise their daughters in the future.
The central argument behind the practice of FGM in Nigeria is the pre-vention of sexual immorality among women. This explanation predominateother reasons behind the practice of FGM as over 70.0 percent of the respon-dents in this study linked FGM practice to reduction and prevention of sexualurge, promiscuity and pre-marital sexual initiation. Findings of this studyrevealed both myths and realities about the theory of promiscuity and the prac-tice of FGM in the study location. The realities are that FGM suppresses
OYEFARA
28
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
29
women’s sexual desire, sexual initiation, sexual practice and sexual enjoymentas measured by reaching orgasm during sexual intercourse. Specifically, cir-cumcised women compared with uncircumcised ones are less likely to havesexual desire in marriage, initiate sexual intercourse with their partners,engage in sexual intercourse in a month and reaching orgasm during sexualintercourse. The reality of FGM is that it distorted the sexual programming andwiring of a woman leaving them at the mercy of their male sexual partners toinitiate and ultimately enjoy sexual intercourse/relationship which corrobo-rates previous studies by other scholars (Owumi, 1993; 1994; Von der Osten-Sacken and Uwer, 2007; Idomu, 2009). The major myth discovered in thestudy about FGM is the fact that it does not prevent sexual promiscuity butrather promote it. Significant proportion of circumcised women in the studyreported extra-marital sexual relationships compared with uncircumcisedwomen in the study location. This paradox can be explained within the contextof anomie theory. The theory emphasized that human beings are more likely todesire and delve into or indulge in those things which seem to be their legiti-mate rights but they had been deprived of it. Thus, they develop differentmechanisms, which are sometime illegitimate, for their aspirations and desiresto be met. It is imperative to note that contrary to the expectation, it seems asif FGM practice increases promiscuity and may even be a cause for prostitu-tion because a circumcised woman being frigid or near frigid may require mul-tiple sex encounters with many men before she can be sexually satisfied.
Prospects for change in the practice of FGM was examined using propor-tion of mothers who have circumcised their daughters and those who planned todo so in the future after controlling for their socio-demographic status. Criticalexamination of the nexus between age of the women and prospect for changerevealed that circumcision of daughters cuts across all age groups of womenincluded in the study, including both the young and the elderly. However, signif-icant higher proportion of the young mothers (i.e. those ones that were less than35 years) had no plan to circumcise their daughters in the future, whereas the eld-erly (i.e. those that were 35 years and above) among them do. A very importantepistemological question that needs to be asked is about whether the youngmothers will be able to sustain their plans considering the significant influenceof the elderly and grandmothers on the care and rearing of young mothers’ chil-dren, decision of older mothers in this study to circumcise their daughters in thefuture and the fact that some of the young mothers had already circumcised theirdaughters. Young mothers may have to contend and prevail over older genera-tion for their plans not to circumcise their daughters in the future to come true.Educational status of the women plays significant role in their daughters’ cir-cumcision status as well as plan to circumcise their daughters in the future,although FGM practice cuts across all levels of educational categories in thecountry. Women with no formal education are more likely to circumcise theirdaughters in the future compared with those with some forms of education.
OYEFARA
30
Other socio-demographic factors examined include ethnic background, religiousaffiliation and form of marriage. It is imperative to note that the practice of FGMcuts across all existing categories in each of these factors, however, more thanother ethnic group, Hausa women are more likely to circumcise their daughtersin the future. In addition, women who were traditional worshippers and those inpolygynous union are more likely to circumcise their daughters in the future. Insummary, young women that are educationally empowered are more likely todecline any request or pressure to circumcise their daughters in the future. Thisfinding is similar to the conclusion of Afifi (2009); using the 2000 Egypt Demo-graphic and Health Survey data, he contended that those women with high lev-els of empowerment and education were 8.06 times more likely not intending toperpetuate female genital cutting for their daughters than those women that werelow-empowered and low level of education.
After all considerations and analysis of this empirical study, a clear con-clusion can be drawn that FGM has a significant strong negative influence onsexual activity, satisfaction and health of women. In addition, there seems tobe a slight inter-generational shift among women in their perception about itseradication, although the practice is deeply rooted and intertwined in the cul-tural milieu of the people. More importantly, young and educated women aremore likely to discontinue the practice of FGM among their daughters in thenearest future. Based on the findings of this study, the following recommenda-tions have been put forward as a way of addressing the harmful effects offemale genital mutilation on girl child and women in the study location: First,gender advocates and various ministries responsible for gender mainstreamingin the country need to redesign their advocacy, enlightenment and sensitizationprogrammes to provide adequate education on the myths and realities of FGMpractice on sexuality and overall health of women. This invariably will reducehighly esteemed erroneous believe about FGM in the study location. Second,there seems to be a window of opportunity for intergenerational change amongeducated young mothers against the practice of FGM in the study location, thisgroup of women needs to be targeted with appropriate behavioural changecommunication materials in order to improve their self-esteem and decisionmaking capability toward possible eradication of the practice in the study loca-tion. Third, international human right bodies and organizations had declaredFGM as a violation of rights of women and girl child. There is a need for col-laboration between local human rights organizations with these bodies. Thiswill produce desired synergy that will give room for activation and implemen-tation of existing local laws and international conventions and treaties on therights of women in Nigeria. As noted by Rahman and Toubia (2000), it is onething to recognise FGM as a practice that violates the rights of girls/womenand another to enforce laws that bring to justice those who perpetrate this act.Government at all levels should strive to enforce all existing laws relating toFGM in the study location. In addition, the synergy between governments andother development partners should target publishing all existing laws prohibit-
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
31
ing the act. These laws should be translated into local languages for localinhabitants to internalise. This will go a long way to stem high rate of FGM inOworonshoki community of Lagos State, Nigeria.
References
ADEBAYO C.O. (1992), Female Circumcision and Other Dangerous Practicesto Women’s Health issues in Nigeria, U.K: Pearson Education Interna-tional.
AFIFI M. (2009), “Women’s empowerment and the intention to continue thepractice of female genital cutting in Egypt”, Archives of Iranian Medi-cine, 12(2): 154-160.
APENA A. (1980), Female Circumcision in Africa and Problem of Cross Cul-tural Perspectives in Africa, London, Dorling Kindersley Book.
BERG R.C., UNDERLAND V. (2013), Obstetric Consequences of Female Geni-tal Mutilation/Cutting (FGM/C), Report from Kunnskapssenteret No. 6-2013, Oslo, Norwegian Knowledge Centre for Health Services, 2013.
BERG R.C., DENISON E., FRETHEIM A. (2010), Psychological, social and sexualconsequences of female genital mutilation/cutting (FGM/C): a systemat-ic review of quantitative studies. Report from Kunnskapssenteret nr 13-2010, Oslo, Nasjonalt kunnskapssenter for helsetjenesten, 2010.
CARR D. (1997), Female Genital Cutting: Findings from the Demographic andHealth Survey Programme, Calverton, Maryland: Macro International.
CENTRE FOR GENDER AND SOCIAL POLICY STUDIES (1998), Report of BaselineSurvey of Positive and Harmful Traditional Practices Affecting Womenand Girls in Nigeria, Obafemi Awolowo University, Ile-Ife.
DAWIT S. (1994), “African Women in the Diaspora and the Problem of FemaleGenital Mutilation”, ASA Women’s Caucus Newsletter.
EMMANUEL B. (1998), Women’s Rites versus Women’s Rights: A Study of Cir-cumcision among the Ketu Yoruba of South-Western Nigeria, New York,Africa World Press.
HEDLEY R., DOCKENOO E. (1992), Child Protection and Female Genital Muti-lation, New York, Africa World Press.
HEISE L.L. (1993), “Reproductive Freedom and Violence against Women:Where are the Intersections?”, Journals of Law, Medicine, and Ethics21(2): 206-216.
HOSKEN F.P. (1993), The Hosken Report: Genital and Sexual Mutilation ofFemales, Fourth Edition, Lexington, Massachusetts: Woman’s Interna-tional Network News.
HUSTON D. (2006), Viagra for Women to Increase Female Libido: Eliminat-ing Female Sexual Health Problems. Retrieved from http://www.wom-ens_health_fitness.com/female_sexual_health.html
IBHAWOH B. (1999), Between Culture and Constitution, the Cultural Legiti-macy of Human Rights in Nigeria, The Danish Centre for Human Rights.
IDOMU I.A. (2009), Female Genital Mutilation among Women in TertiaryInstitutions in Delta State, Nigeria, in NWAGWU H.O., MORONKLA O.A.,AKINTUNDE D.O. (eds.), Women Issues in Nigeria, Ibadan, Royal People(Nigeria) Ltd.
JOINT UNITED NATIONS PROGRAMME ON HIV/AIDS (UNAIDS) AND WORLDHEALTH ORGANIZATION (WHO), (2013), AIDS Epidemic Update, May,Geneva, pp. 13-18.
KOSO-THOMAS O. (1987). The Circumcision of Women: A Strategy for Eradi-cation, London, Dotesios Ltd.
MOHAMMED W. (1989), “Medical and Social Aspects of Female Circumcisionin Somalia”, in Female Circumcision: Strategies to Bring Change by theItalian Association for Woman in Development and the Somali Women’sDemocratic Organization, Rome, The Italian Association for Women inDevelopment.
MOHAMMED T., AHMED S.M.A. (2000), Defective Sexuality and Female Cir-cumcision: The Cause and the Possible Management, Faculty of Medi-cine, Cairo University, Cairo University, Cairo, Egypt.
NATIONAL POPULATION COMMISSION (NPC) [NIGERIA] AND ORC MACRO(2004), Nigeria Demographic and Health Survey 2003, Calverton, Mary-land, National Population Commission and ORC Macro.
NATIONAL POPULATION COMMISSION (NPC) [NIGERIA] AND ICF MACRO(2009), Nigeria Demographic and Health Survey 2008. Abuja, Nigeria:National Population Commission and ICF Macro.
ODIMEGWU C.O., OKEMGBO C.N. (2000), “Female Circumcision and SexualActivity: Any Relationship?”, UNILAG Sociological Review, 1, 159-176.
OLURODE L., OYEFARA J.L. (2010), Issues in Sexual Harassment in Nigeria’sTertiary Institutions, Conspiracy, Compromises, and Challenges, Lagos,Rebonik Publications.
OMOLADE O. (1992), Unending Harmful Tradition Shrouded in Secrecy:Female Genital Mutilation, Ibadan, Royal People Publishers.
OSINOWO H.O., TAIWO A.O. (2003), “Impact of Female Genital Mutilation onSexual Functioning, Self-esteem and Marital Instability of Women inAjegunle”, Ife Psychologia, 11(1): 123-130.
OWUMI B.E. (1993). A social–cultural analysis of female circumcision amongthe Urhobo. A study of the Okpe people of Delta state. A project submit-ted to the Inter African Committee (IAC Nigeria), Lagos.
OYEFARA
32
FEMALE GENITAL MUTILATION (FGM) AND THEORY OF PROMISCUITY...
33
OWUMI B.E. (1994), “Forms and age at circumcision: some psychologicalimplications for women’s fertility”, Women’s Behavioural Issues 1(1):10-16.
Rahman A., Toubia N. (2000), Female Genital Mutilation: A Guide to Lawsand Policies Worldwide, London and New York, Zed Books, p. 4.
SAI F. (1995), Socio-Cultural and Legal Practices and Gender Equity, Adamand Eve and the Serpent, Accra, The Ghana University Press.
SHELL-DUNCAN B. (2008), “From Health to Human Rights: Female GenitalCutting and the Politics of Intervention”, American Anthropologist,110(2): 225-236.
SHELL-DUNCAN B., HERNLUND Y. (eds.) (2000), Female “Circumcision” inAfrica: Culture, Controversy and Change, Lynne: Riener Publishers.
TOUBIA N. (1993), Female Genital Mutilation: A Call for Global Action, 2nd
edition, New York, Women Ink.UNFPA (2011), Project Embera-wera: An Experience of Culture Change to
Eradicate Female Genital Mutilation in Colombia-Latin America, NewYork, UNFPA.
UNITED NATIONS CHILDREN’S FUND (UNICEF) (2005), Female Genital Mutila-tion/Cutting, A Statistical Exploration, New York, UNICEF.
UNITED NATIONS CHILDREN’S FUND (UNICEF) (2013), Female Genital Mutila-tion/Cutting: A Statistical Overview and Exploration of the Dynamics ofChange, New York, UNICEF.
UNITED NATIONS GENERAL ASSEMBLY (1981), Convention on the Eliminationof all Forms of Discrimination against Women (CEDAW), New York,United Nations.
VON der OSTEN-SACKEN T., Uwer T. (2007), “Is Female Genital Mutilation anIslamic Problem?”, Middle East Quarterly, Winter, 29-36.
WEIL-CURIEL L., TEMMERMAN M. (2007), “An analysis of the implementationof laws with regard to female genital mutilation in Europe”, Crime, Lawand Social Change, 47(1): 1-31.
WOMEN’S POLICY INC. (1996), Female Genital Mutilation in Women’s HealthEquity Act of 1996, Legislature Summary and Overview, Women’s Pol-icy Inc. pp. 48.
WORLD HEALTH ORGANIZATION (1994), Female Genital Mutilation Informa-tion Kit, Geneva, Switzerland.
WORLD HEALTH ORGANIZATION (2001), A Systematic Review on HealthComplications of Female Genital Mutilation including Squealed inChildbirth, Geneva, Switzerland.
WORLD HEALTH ORGANIZATION (2008), Eliminating Female GenitalMutilation, An Interagency Statement, Geneva, Switzerland.