http://vaw.sagepub.com/ Violence Against Women http://vaw.sagepub.com/content/15/2/148 The online version of this article can be found at: DOI: 10.1177/1077801208329386 2009 15: 148 Violence Against Women Heather Littleton and Craig E. Henderson Victims Evaluation of Predictors of PTSD Symptomatology Among College Rape If She Is Not a Victim, Does That Mean She Was Not Traumatized? : Published by: http://www.sagepublications.com can be found at: Violence Against Women Additional services and information for http://vaw.sagepub.com/cgi/alerts Email Alerts: http://vaw.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://vaw.sagepub.com/content/15/2/148.refs.html Citations: at UNIV OF MIAMI on December 13, 2010 vaw.sagepub.com Downloaded from
Transcript
http://vaw.sagepub.com/Violence Against Women
http://vaw.sagepub.com/content/15/2/148The online version of this article can be found at:
DOI: 10.1177/1077801208329386
2009 15: 148Violence Against WomenHeather Littleton and Craig E. Henderson
VictimsEvaluation of Predictors of PTSD Symptomatology Among College Rape
If She Is Not a Victim, Does That Mean She Was Not Traumatized? :
Published by:
http://www.sagepublications.com
can be found at:Violence Against WomenAdditional services and information for
Authors’ Note: This study was supported in part by a grant-in-aid from the Society for the PsychologicalStudy of Social Issues (H. Littleton). We gratefully acknowledge FredAnthony Miller, who developed theonline data-collection program.
If She Is Not a Victim, DoesThat Mean She Was NotTraumatized?Evaluation of Predictors of PTSDSymptomatology Among CollegeRape VictimsHeather LittletonEast Carolina UniversityCraig E. HendersonSam Houston State University
The issue of whether individuals can be traumatized by the experience of rape if theydo not label the experience a victimization remains controversial. Indeed, there are con-flicting findings with regard to the extent to which such unacknowledged victims expe-rience posttraumatic symptoms. The goal of the current study was to evaluateacknowledgment status as a predictor of posttraumatic stress disorder symptomatologyusing structural equation modeling among a sample of 346 college rape victims.Results showed that whereas acknowledged victims reported more symptoms of post-traumatic stress disorder, acknowledgment status did not add to the prediction of post-traumatic stress disorder symptoms in a model including assault violence and otherimportant predictors of these symptoms.
Keywords: PTSD; rape acknowledgment; sexual assault; structural equation modeling
Rape is unfortunately an all-too-common experience in the lives of youngwomen. Although definitions vary somewhat from state to state, most
researchers define rape as unwanted sex obtained by threat, force, or the assault of avictim who is incapable of consenting (e.g., as a result of drinking alcohol or usingsubstances; Abbey, BeShears, Clinton-Sherrod, & McAuslan, 2004). Indeed, allstates now include a provision in their statutes that victims may be unable to consentto sex as a result of drinking alcohol or using other drugs (Cole, 2006). Recent preva-lence estimates for rape among women using these criteria have ranged from 14% to
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
22% in college, community, and medically recruited samples (Abbey et al., 2004;Arata, 1999; Brener, McMahon, Warren, & Douglas, 1999; Cloutier, Martin, &Poole, 2002; Kahn, Jackson, Kully, Badger, & Halvorsen, 2003; Littleton, RadeckiBreitkopf, & Berenson, 2008; Masho, Odor, & Adera, 2005).The experience of rape is frequently associated with the development of significant
and persistent psychological distress. This distress often takes the form of posttraumaticstress disorder (PTSD), which includes reexperiencing the trauma in the form ofunwanted thoughts, images, and dreams; avoidance of reminders of the trauma, such ascertain situations or people; and increased arousal, such as the development of insomniaor a heightened startle response (American PsychiatricAssociation, 1994). Between onehalf and nearly two thirds of rape victims develop PTSD following this trauma (Breslauet al., 1998; Rothbaum, Foa, Riggs, Murdock, &Walsh, 1992), including chronic PTSD.For example, one community sample found that the median duration of PTSD followinginterpersonal trauma was 4 years (Breslau et al., 1998). In another example, Kilpatrick,Saunders, Veronen, Best, and Von (1987), using a random community sample of rapevictims, found that 16% met criteria for current PTSD, even though the rape hadoccurred on average 17 years earlier. Rape victims also often experience other forms ofpsychological distress. For example, in a community sample of women, 39% of rapevictims met current criteria for either an anxiety disorder other than PTSD or majordepression (Boudreaux, Kilpatrick, Resnick, Best, & Saunders, 1998).Many women who report experiences that meet a legal definition of rape do not
label their experience as such or even as a victimization. Studies of college rapevictims have found that between 47% and 73% do not label their experience a rapeor a victimization; these victims are referred to as unacknowledged victims(Bondurant, 2001; Botta & Pingree, 1997; Fisher, Daigle, Cullen, & Turner, 2003;Frazier & Seales, 1997; Layman, Gidycz, & Lynn, 1996; Littleton, Axsom, RadeckiBreitkopf, & Berenson, 2006; McMullin &White, 2006). Research with noncollegevictim samples similarly suggests that a sizable percentage of rape victims do notacknowledge these unwanted sexual experiences as rapes (Conoscenti & McNally,2006; Koss, Figueredo, Bell, Tharan, & Tromp, 1996; Littleton et al., 2008; Russell,1982). Instead, they give their experience a much more benign label, such as a mis-communication or bad sex, or state that they are unsure how to label their experience(Littleton et al., 2006; Littleton et al., 2008).A number of differences have been found in the assault experiences of unacknowl-
edged and acknowledged rape victims. The most consistent finding is that the assaultsof unacknowledged victims are less violent, involving less force by the assailant, resis-tance by the victim, and injury to the victim (Bondurant, 2001; Botta & Pingree, 1997;Fisher et al., 2003; Kahn, Andreoli Mathie, & Torgler, 1994; Layman et al., 1996;Littleton et al., 2006; Littleton et al., 2008). Some studies have also found that unac-knowledged rapes are more likely than acknowledged rapes to involve alcohol use bythe victim and the perpetrator (Bondurant, 2001; Botta & Pingree, 1997; Layman et al.,1996; Littleton et al., 2008; McMullin & White, 2006). In addition, unacknowledged
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
victims are more likely than acknowledged victims to report that they were romanticallyinvolved with the perpetrator (Frazier & Seales, 1997; Kahn et al., 2003; Koss, 1985;Koss, Dinero, Seibel, & Cox, 1988; Littleton et al., 2008) and that they engaged in con-sensual sexual activity with the perpetrator prior to the assault (Koss, 1985).The fact that many unacknowledged assaults resemble a normative sexual interac-
tion to a certain extent (e.g., they are not highly violent, they occur within the contextof a relationship wherein sexual activity would be considered normative), combinedwith the fact that the victims themselves do not view the experience as a victimization,has led some social critics to dismiss the notion that these individuals are traumatizedby this experience or that they should be considered victims (see Gavey, 1999, for areview). Supporting the possibility that unacknowledged victims are less traumatizedby the experience, Kahn and Andreoli Mathie (2000) found that unacknowledgedvictims reported feeling less victimized and less negative affect during the rape thanacknowledged victims. In a subsequent study, Kahn and colleagues (2003) found thatunacknowledged victims reported less negative affect following the assault thanacknowledged victims. Studies that have directly assessed whether unacknowledged oracknowledged victims differ in postvictimization psychological distress have hadequivocal findings. Several studies found no differences in general distress (e.g., neg-ative affect) between unacknowledged and acknowledged victims (Frazier & Seales,1997; Koss, 1985; Layman et al., 1996; Littleton et al., 2006). In contrast, Botta andPingree (1997) found in a sample of 62 acknowledged and 34 unacknowledged victimsthat unacknowledged victims were more poorly adjusted than acknowledged victimsin several domains, including current negative affect, interference in activities due toemotional problems, and alcohol use. Concerning PTSD symptomatology, three stud-ies found that acknowledged victims reported more PTSD symptomatology than unac-knowledged victims (Koss et al., 1996; Layman et al., 1996; Littleton et al., 2006),whereas one study found no difference in PTSD symptomatology between unac-knowledged and acknowledged victims in a sample of 26 unacknowledged and 19acknowledged victims (Marx & Soler-Baillo, 2005).Although it is difficult to interpretthese equivocal findings, one possible explanation is that a number of studies in thisarea have been limited by low power to detect all but large differences in distressbetween unacknowledged and acknowledged victims (Littleton, Rhatigan, & Axsom,2007). For example, Koss (1985) evaluated distress among a sample of 36 acknowl-edged and 26 unacknowledged victims, and Layman and colleagues (1996) evaluateddistress among a sample of 40 unacknowledged and 20 acknowledged victims. In addi-tion, these studies did not control for potential confounding variables (e.g., assault vio-lence) that may account for differences in distress between acknowledged andunacknowledged victims rather than the acknowledgment itself. Overall, however,these studies suggest the possibility that at least some unacknowledged victims can bedistressed and potentially traumatized by their experience.The most comprehensive study specifically evaluating whether the experience
of sexual victimization produces distress, regardless of acknowledgment status, was
150 Violence Against Women
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
conducted by Harned (2004). Using path analysis, she examined two competing mod-els. In the first, the experience of unwanted sex predicted participants’ labeling the expe-rience a victimization, and in turn, labeling predicted greater distress. In the second,unwanted sexual experiences predicted both participants’ labeling the experience a vic-timization and distress, and there was no direct relationship between labeling and dis-tress. She found stronger support for the latter model. Although the findings fromHarned’s study are intriguing, it is important to note some limitations of the study. Theseinclude restricting analyses only to victims of assaults in dating relationships and inclu-sion of victims of multiple types of unwanted sexual experiences, in addition to rape. Inaddition, Harned did not specifically evaluate the role of acknowledgment status in pre-dicting victims’ symptoms of PTSD, despite some evidence that unacknowledgedvictims may experience fewer PTSD symptoms than acknowledged victims, even if thetwo groups do not differ in general distress (Koss et al., 1996; Layman et al., 1996;Littleton et al., 2006). Such comparisons are also necessary to conclusively state thatunacknowledged victims do not experience trauma symptoms following the assault.To summarize, there is moderately strong evidence that unacknowledged sexual
assault can be a distressing experience, and the fact that the victim does not acknowledgethe rape does not necessarily mean that she is not distressed by the experience. However,the evidence suggesting that unacknowledged victims’ distress is expressed as traumasymptoms is equivocal. Thus, the primary goal of the current investigation was to evalu-ate through structural equation modeling (SEM) the role of acknowledgment status as apredictor of PTSD symptomatology among rape victims. We accomplished this goal byevaluating the extent to which (a) acknowledgment status predicted PTSD symptoma-tology and (b) whether inclusion versus exclusion of the relationship between acknowl-edgment and PTSD symptoms affected overall model fit. In the latter case, if model fitwas unaffected by including versus excluding the path between acknowledgment andPTSD symptoms, we would reject the model including this path for the more parsimo-nious model in which it was excluded. On the basis of this evidence, we would concludethat victims’ unwanted sexual experiences are related to PTSD symptoms regardless ofwhether the victims acknowledge that these experiences were indeed victimizations.Given previous work suggesting that experiencing a more violent assault is asso-
ciated with acknowledging the rape (e.g., Bondurant, 2001; Botta & Pingree, 1997;Kahn et al., 1994; Layman et al., 1996; Littleton et al., 2006) and that experiencinga more violent assault is associated with greater PTSD symptomatology (e.g.,Ullman, Townsend, Filipas, & Starzynski, 2007), we included assault violence in themodel as a predictor of acknowledgment and PTSD symptomatology. In addition,greater reliance on maladaptive coping, such as avoidant and ruminative strategies,has been related to experiencing more PTSD symptomatology among rape victims(Dunmore, Clark, & Ehlers, 2001; Ullman & Filipas, 2001; Ullman et al., 2007) aswell as victims of other forms of interpersonal violence (Dunmore et al., 2001;Johnson, Sheahan, & Chard, 2003). Greater assault violence has also been associ-ated with more reliance on maladaptive coping (Littleton & Radecki Breitkopf,
Littleton, Henderson / College Rape Victims 151
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
2006). Thus, maladaptive coping was included in the model as a predictor of PTSDsymptomatology, and assault violence was included as a predictor of maladaptivecoping. Finally, social support has been found to act as a protective factor withregard to victims’ use of maladaptive coping following rape, such that victims withstronger support networks engage in less maladaptive coping (Ullman et al., 2007).Thus, social support was included in the model as a predictor of maladaptive coping.
Method
Participants
A total of 1,744 women, recruited from the psychology department participantpools of three southern universities, participated for course credit during two acade-mic semesters (fall 2006 and spring 2007). A total of 353 women, 20.2% of the sam-ple, responded positively to a screening questionnaire assessing sexual assaultexperiences in adolescence or adulthood. Because we were interested in evaluatingacknowledgment status as a predictor of PTSD symptoms, 7 (1.9%) participants whodid not indicate their acknowledgment status were eliminated from further analyses.Unfortunately, these individuals generally had extensive missing data, precludinganalyses comparing characteristics of included and excluded participants. The aver-age age of the 346 included women was 21.7 years (SD = 5.6, range 18-54 years).Seventy-three percent characterized their ethnicity as European American, 8.1% asLatina, 6.4% as Black or Caribbean Islander, 5.8% asAsian or Pacific Islander, 2.3%as multiethnic, and 0.6% as Native American, and 4.3% did not indicate their eth-nicity. Participants from the three universities differed in the percentage of womenwho self-identified as ethnic minorities, χ2(2) = 33.10, p < .001 (24.2%, 45.2%,14.0%). Participants also differed in their mean age, F(2, 333) = 34.14, p < .001(23.39 years, 24.33 years, 19.41 years). However, there were no significant differ-ences in the percentage of women at each university reporting a sexual assault expe-rience, χ2(2) = 2.95, p = .229 (18.7%, 22.3%, 18.6%).
Procedures
Data were collected using an online survey. Potential participants were recruitedusing posted fliers and announcements on psychology department research partici-pant management Web sites at the three universities. Posted information stated thatparticipants would be asked to complete a confidential survey about their negativesexual experiences, coping, and psychological health. Participants were excluded ifthey were male or younger than 18 years of age. Some form of student identificationwas collected to award course credit and to prevent duplicate participation (studentidentification information was removed from the data files prior to data processing).
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
Participants were given a brief description of the study and information aboutavailable counseling resources and were asked to provide their electronic consent.Behaviorally specific screening questions were used to determine if participants had anexperience in adolescence or adulthood that would meet a legal definition of rape or sex-ual assault. Participants who confirmed having had a sexual assault experience wereasked several questions about the circumstances of their “experience with unwanted sex-ual contact” (or the most serious experience if they had multiple experiences). They werealso given eight potential labels for the assault: rape, attempted rape, some other type ofcrime, miscommunication, seduction, hook-up, bad sex, and not sure. Those who did notlabel the assault a victimization (i.e., rape, attempted rape, or another crime) were clas-sified as unacknowledged. Participants also completed measures assessing their assault-related coping strategies and posttraumatic stress symptoms. The study was approved bythe institutional review boards of the three universities and followed the guidelines forensuring the confidentiality of online data outlined by Reips (2002).
Measures
Victimization items. Two behaviorally specific screening items to assess experi-ences of rape since the age of 14 were derived from the Sexual Experiences Survey(Koss & Gidycz, 1985). The items were developed to be consistent with the defini-tions of rape and sexual assault in the Commonwealth of Virginia and the state ofTexas, the commonwealth and state in which the research was conducted. The itemsassessed experiences of unwanted sex (vaginal, oral, or anal intercourse or objectpenetration) that was obtained by force or by threat of force or that occurred whenthe individual was incapacitated or unconscious, such as from alcohol or drugs.
Assault characteristics questionnaire. Victims completed a questionnaireregarding the circumstances of their rape experience (or the one they regarded asmost serious, if they had multiple experiences). The questionnaire was based on onedeveloped previously (Littleton & Radecki Breitkopf, 2006). The questionnaireincluded several items assessing the violence of the assault. Two variables were con-structed regarding the types of force that the victim reported the assailant used froma list provided: moderate physical force (using his superior body weight, twistingyour arm or holding you down) and severe physical force (hitting or slapping you,choking or beating you, showing or using a weapon). Victims were also asked if theassailant had engaged in verbal threats to harm them or others. Three resistance vari-ables were constructed regarding the types of resistance strategies victims reportedusing during their assault from a list provided: nonverbal resistance (turned cold,cried), verbal resistance (reasoned or pleaded with him, screamed for help), andphysical resistance (ran away, physically struggled). Specifically, we coded whetherthe participant reported each assault element as present or absent.
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
Victims were asked to indicate their relationship with the assailant at the time ofthe experience of unwanted sexual contact from a list provided. The relationshipwith the assailant was then coded as unknown/minimal (stranger, just met), acquain-tance (friend, acquaintance), romantic (dating casually, steady date, romantic part-ner), or relative. The victim also estimated the number of standard drinks both sheand the assailant had consumed prior to the assault. Victim and assailant drinkinglevel was then coded as binge or nonbinge (four standard drinks by the participant,five standard drinks by the assailant; National Institute on Alcohol Abuse andAlcoholism, 2006). Victims also indicated whether they had disclosed the assaultand the number of individuals to whom they had disclosed the experience.Participants indicated their relationship with the individuals to whom they had dis-closed from a list provided. Participants’ disclosure was coded as being to informalsources (e.g., relative, sibling, boyfriend/partner, friend) and to formal sources (e.g.,police, doctor/nurse/health care provider, counselor). Finally, victims reported thenumber of months that had elapsed since the assault occurred.
Coping Strategies Inventory. The 32-item short form of the Coping StrategiesInventory (Tobin, Holroyd, Reynolds, & Wigal, 1989) was administered to assessvictims’ strategies in coping with the assault. This measure assesses two main types ofcoping: engagement and disengagement. The entire measure was administered, however,because use of avoidance and ruminative strategies have predicted PTSD symptomatol-ogy (Branscombe, Wohl, Owen, Allison, & N’gbala, 2003; Littleton, Horsley, John, &Nelson, 2007); we examined only scores on the disengagement coping scales. The dis-engagement coping scales are problem avoidance (I avoided thinking or doing anythingabout the situation), wishful thinking (I hoped a miracle would happen), social with-drawal (I spent more time alone), and self-criticism (I criticized myself for what hap-pened). Both the problem avoidance and the social withdrawal scales appear to measureavoidance coping strategies. The wishful thinking and self-criticism scales appear tomeasure ruminative coping and unproductive counterfactual thinking (e.g., blaming one-self for the sexual assault, wishing the assault had not occurred). For each item, individ-uals rated how often they used the coping strategy with the experience of unwantedsexual contact identified on a 5-point Likert-type scale anchored by 1 (not at all) and 5(very much).Alpha coefficients of the scales have averaged .70 (Tobin, 2001). In the cur-rent study, alpha coefficients ranged from .67 (problem avoidance) to .90 (self-criticism).
PTSD Symptom Scale. The PTSD Symptom Scale (Foa, Riggs, Dancu, &Rothbaum, 1993) is a brief measure designed to assess symptoms of posttraumaticstress. The measure contains three scales assessing the three types of PTSD symptoms:reexperiencing, avoidance, and arousal. A sample item is, “Having bad dreams ornightmares about the event.” In the current study, for each item, individuals rated howoften they have had the symptom in the past week in connection to their experience ofunwanted sexual contact on a 4-point Likert-type scale anchored by 0 (not at all or
154 Violence Against Women
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
only one time) and 3 (five or more times per week/almost always). Cronbach’s alphafor the scales in a previous study of rape victims ranged from .78 to .82 (Foa et al.,1993) and in the current study ranged from .84 to .86. In addition, the PTSD SymptomScale was found to have a sensitivity of 62% and specificity of 100% for the diagno-sis of PTSD when compared with a structured clinical interview (Foa et al., 1993).
Multidimensional Scale of Perceived Social Support. The MultidimensionalScale of Perceived Social Support (Zimet, Dahlem, Zimet, & Farley, 1988) is a 12-item measure of perceived social support adequacy. The Multidimensional Scale ofPerceived Social Support has three subscales: support from family (I can talk aboutmy problems with my family), support from friends (my friends really try to helpme), and support from a significant other (I have a special person who is a realsource of comfort to me). For each item, individuals indicated the extent to whichthey agreed with the statement on a 7-point Likert-type scale bounded by 1 (verystrongly disagree) and 7 (very strongly agree). Cronbach’s alpha of the scales in acollege student sample ranged from .85 to .91 (Zimet et al., 1988) and in the currentsample ranged from .93 to .96. Factor analysis with a college sample supported thethree-factor structure of the measure (Zimet et al., 1988).
Analysis Plan
The main hypotheses in this study were tested with a series of latent variable (LV)structural equation models fitting the hypothesized model to the sample covariancematrix using the Mplus program (Version 4.21; Muthén & Muthén, 1998-2007). Toassess model fit, in addition to the model χ2, we also examined three fit indices, theroot-mean-square error of approximation (RMSEA), the comparative fit index (CFI),and the Tucker-Lewis Index (TLI). The RMSEA assesses model misfit per degree offreedom, and previous research has indicated that values of approximately .06 or lessare indicative of good fit (Hu & Bentler, 1999). The CFI and TLI measure improve-ment in fit when the model tested is compared to an independence model in which thevariables are uncorrelated with one another. Previous research has indicated thatCFI/TLI values close to .95 are indicative of good fit (Hu & Bentler, 1999). It shouldbe noted that in moderately sized samples (N > 200), the chi-square test tends to beinflated and may reach significance even with adequately fitting models (Kline,2005). Therefore, when discrepancies between the chi-square test and other fit indicesarose, we relied more heavily on the supplemental fit indices.The order of analyses was as follows. First, we used confirmatory factor analysis
to evaluate three LV measurement models created from the subscales of the CopingStrategies Inventory, PTSD Symptom Scale, and Multidimensional Scale ofPerceived Social Support. In addition, we created an LV measurement model fromfive assault violence indicators (verbal resistance, nonverbal resistance, physicalresistance, moderate physical force, severe physical force). Finally, we modeled
Littleton, Henderson / College Rape Victims 155
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
assault acknowledgment as an observed manifest dichotomous item in the structuralequation models described more fully below. Because the assault violence itemswere specified as categorical indicators in the structural equation models, means,variances, and covariances are not sufficient statistics under maximum likelihoodestimation, and thus Mplus does not produce either the chi-square test of absolute fitor other model fit indices (Linda Muthén, personal communication, April 14, 2007).Therefore, we used the weighted least squares estimator to examine all LV models.1
Modification indices (Lagrange Multiplier and Wald tests) were examined to deter-mine if model fit could be improved by either constraining or freeing parameters.Next, we tested the two structural equation models, the only difference between
them being whether acknowledgment status was included in the model as a predic-tor of PTSD symptomatology. We used a chi-square difference test to determinewhether including assault acknowledgment in the model produced superior fit com-pared to when it was removed. A nonsignificant chi-square difference test wouldindicate that the two models did an equally good job of reproducing the observeddata. However, in most SEM applications, the original model is retained when thechi-square difference test is not significant because retaining the nested model is tan-tamount to rejecting a null hypothesis on the basis of nonsignificant effects, a logi-cal error that is well documented in the literature (Keppel, 1991). Therefore, we alsoused the Bayesian Information Criterion (Schwarz, 1978) to help guide our selectionof the final model, with smaller values indicating better fit.
Results
Sample Characteristics
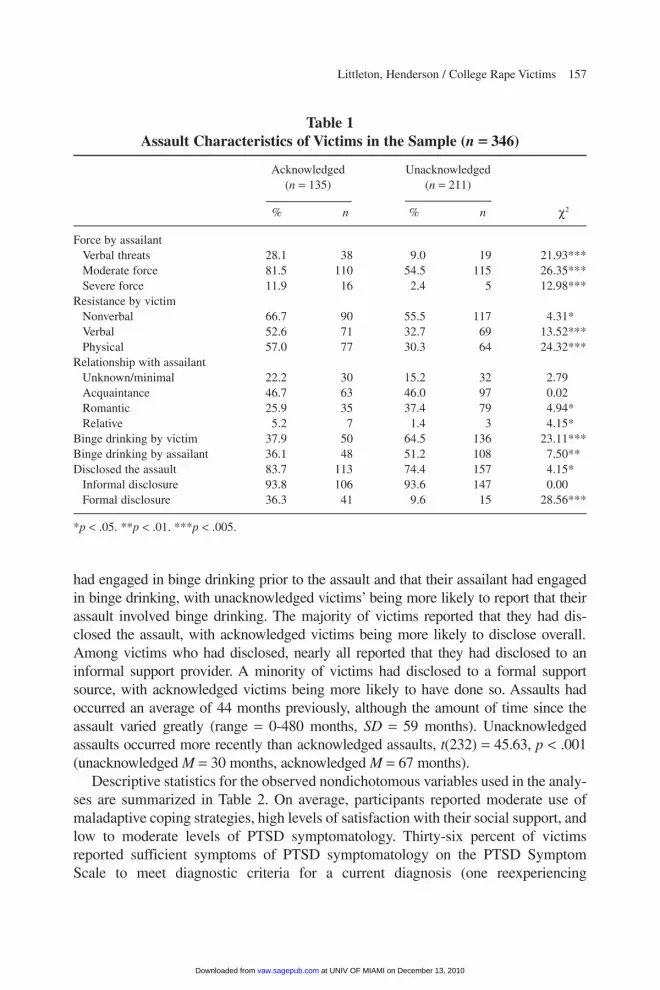
The majority of women, 61%, were unacknowledged rape victims, whereas 39%were acknowledged. Of unacknowledged victims, 46% were unsure how to labeltheir experience, 38% labeled it a miscommunication, 9% a hook-up, 4% bad sex,and 3% a seduction. Of acknowledged victims, 66% labeled their experience a rape,24% an attempted rape, and 10% some other type of crime. Characteristics of par-ticipants’ assaults, broken down by acknowledgment status, are summarized in Table1. The majority of assaults involved the use of physical force by the assailant, andthe majority of victims engaged in some form of resistance, although the assaults ofacknowledged victims were more likely to involve both force by the assailant andresistance by the victim. However, it should be noted that few participants reportedthat their assault involved the use of severe force.Consistent with prior research, the vast majority of participants knew their assailants,
althoughmost reported fairly casual relationships with them (e.g., acquaintance, friend).Unacknowledged victims were more likely to report a romantic relationship with theassailant than acknowledged victims.A sizable percentage of victims reported that they
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
had engaged in binge drinking prior to the assault and that their assailant had engagedin binge drinking, with unacknowledged victims’ being more likely to report that theirassault involved binge drinking. The majority of victims reported that they had dis-closed the assault, with acknowledged victims being more likely to disclose overall.Among victims who had disclosed, nearly all reported that they had disclosed to aninformal support provider. A minority of victims had disclosed to a formal supportsource, with acknowledged victims being more likely to have done so. Assaults hadoccurred an average of 44 months previously, although the amount of time since theassault varied greatly (range = 0-480 months, SD = 59 months). Unacknowledgedassaults occurred more recently than acknowledged assaults, t(232) = 45.63, p < .001(unacknowledged M = 30 months, acknowledged M = 67 months).Descriptive statistics for the observed nondichotomous variables used in the analy-
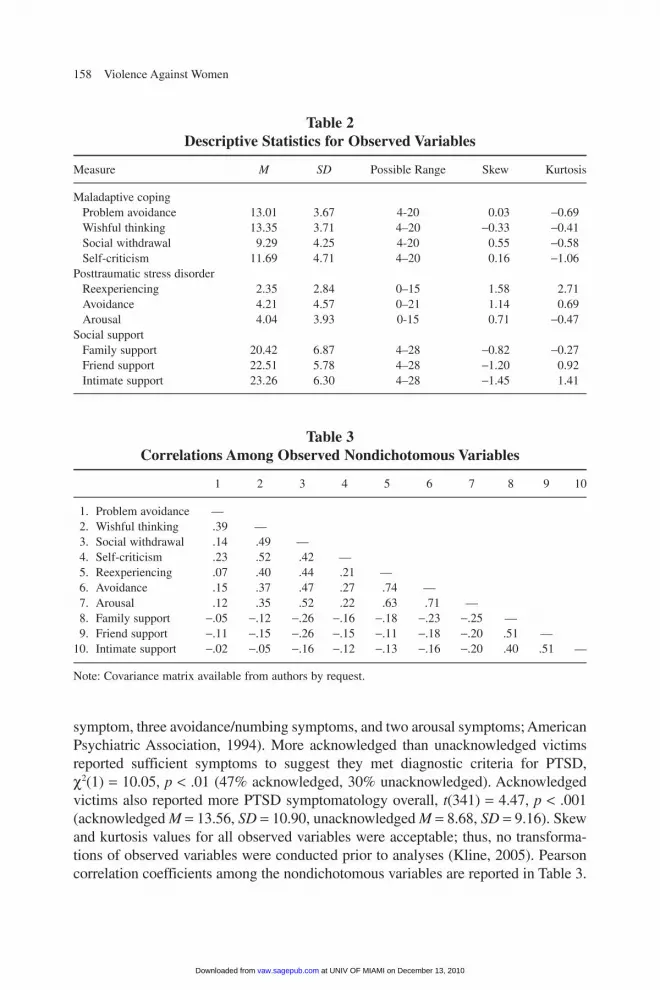
ses are summarized in Table 2. On average, participants reported moderate use ofmaladaptive coping strategies, high levels of satisfaction with their social support, andlow to moderate levels of PTSD symptomatology. Thirty-six percent of victimsreported sufficient symptoms of PTSD symptomatology on the PTSD SymptomScale to meet diagnostic criteria for a current diagnosis (one reexperiencing
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
Note: Covariance matrix available from authors by request.
symptom, three avoidance/numbing symptoms, and two arousal symptoms; AmericanPsychiatric Association, 1994). More acknowledged than unacknowledged victimsreported sufficient symptoms to suggest they met diagnostic criteria for PTSD,χ2(1) = 10.05, p < .01 (47% acknowledged, 30% unacknowledged). Acknowledgedvictims also reported more PTSD symptomatology overall, t(341) = 4.47, p < .001(acknowledged M = 13.56, SD = 10.90, unacknowledged M = 8.68, SD = 9.16). Skewand kurtosis values for all observed variables were acceptable; thus, no transforma-tions of observed variables were conducted prior to analyses (Kline, 2005). Pearsoncorrelation coefficients among the nondichotomous variables are reported in Table 3.
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
Initial confirmatory factor analyses suggested that the indicator representingproblem avoidance was not strongly related to the maladaptive coping LV (β = .37).Thus, problem avoidance was removed from the model. Each of the remaining man-ifest variables was moderately to strongly associated with the LV (wishful thinking:β = .78, self-criticism: β = .67, social withdrawal: β = .63). For PTSD symptoma-tology, each of the manifest variables was strongly associated with the LV (reexpe-riencing: β = .81, avoidance: β = .91, arousal: β = .78). For the social support LV,each of the manifest variables was moderately to strongly associated with the LV(family support: β = .64, friend support: β = .80, intimate support: β = .63). A mea-surement model including each of the three LVs with nondichotomous indicatorsand the covariances between them also demonstrated adequate model fit, χ2(24) =62.30, p < .001, CFI = .96, TLI = .94, RMSEA = .07.Initial confirmatory factor analysis of the assault violence LV suggested that the
indicator representing nonverbal resistance was not strongly related to the LV (β =.12). Thus, nonverbal resistance was removed from the model. Because the assaultviolence indicators consisted of dichotomous items reflecting the presence orabsence of assault characteristics, traditional fit indices were not available to judgemodel fit. However, the likelihood ratio χ2 test of the confirmatory factor analysisafter removing the nonverbal resistance indicator was not significant, χ2(2) = 3.66,p = .16, and each of the indicators showed moderate to strong associations with theLV (moderate physical force: β = .94, severe physical force: β = .53, verbal resis-tance: β = .60, physical resistance: β = .78).
Structural Equation Models
The first structural model (see Figure 1) tested the effects of maladaptive coping,assault violence, and assault acknowledgment on PTSD symptoms. In addition, useof maladaptive coping was predicted by assault violence and social support. Finally,assault acknowledgment was predicted by assault violence. The model test revealedthat although the χ2 test of exact fit was significant, χ2(30) = 71.76, p < .001, the othermodel fit indices generally indicated that the data fit the model adequately (CFI = .90,TLI = .93, RMSEA = .06).2 As shown in Figure 1, a significant direct effect on PTSDsymptoms was found with maladaptive coping (β = .64, p < .001), such that greaterreliance on maladaptive coping was associated with greater PTSD symptomatology.In contrast, both assault violence (β = .06, p = .27) and acknowledgment status(β = –.11, p = .06) did not significantly predict PTSD symptoms. The model overallaccounted for 50% of the variance in PTSD symptoms. Assault violence (β = .31,p < .001) and social support (β = –.33, p < .001) significantly predicted maladaptivecoping and accounted for 25% of the variance in maladaptive coping. Specifically,greater assault violence was associated with greater reliance on maladaptive coping,
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
Figure 1Results of Latent Variable Structural Equation Modeling
Including Acknowledgment Status as a Predictor of Posttraumatic Stress Disorder (PTSD) Symptoms
AssaultViolenceVerbal
resistance
Severeforce
Moderateforce
.63.87
.44
.89
.69
.56
.74 –.11
.31
SocialSupport
Familysupport
Friendshipsupport
Intimatesupport
.06
–.33
.78
.73
.56
Wishfulthinking
PTSDSymptomatology
Socialwithdrawal
Physicalresistance
Avoidance
Arousal
.78
.85
.87
.64
AcknowledgmentStatus
-.61
Self-criticism
MaladaptiveCoping
Re-experiencing
and less social support satisfaction was associated with greater reliance on maladap-tive coping. In addition, assault violence predicted acknowledgment (β = –.61,p < .001), such that greater assault violence was associated with greater likelihood ofbeing an acknowledged victim. Assault violence was indirectly associated with PTSDsymptomatology through maladaptive coping (β = .20, p < .001) and nonsignificantlyassociated with PTSD symptomatology through acknowledgment status (β = .06,p = .27). Social support was also significantly indirectly associated with PTSD symp-tomatology through maladaptive coping (β = –.21, p < .001). In addition, all themodel modification indices values were less than 15.0.In the model shown in Figure 2, PTSD symptoms are not predicted from assault
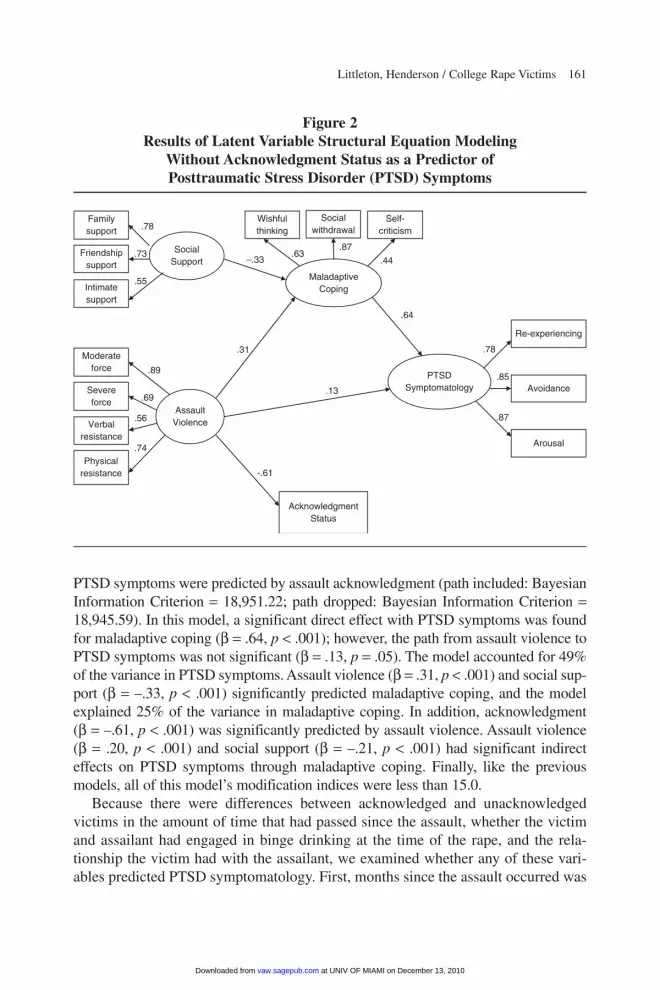
acknowledgment. As with the previous model, the χ2 test for exact fit was significant,χ2(30) = 71.76, p < .001; however, the model fit indices generally suggested that thedata fit this model adequately (CFI = .90, TLI = .93, RMSEA = .06). The likelihoodratio difference test indicated that the model fits for the two competing models werevirtually indistinguishable, ∆χ2(1) = 0.18, ns. The Bayesian Information Criterion forthe hypothesized model was also smaller than that for the previous model in which
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
Figure 2Results of Latent Variable Structural Equation Modeling
Without Acknowledgment Status as a Predictor of Posttraumatic Stress Disorder (PTSD) Symptoms
AssaultViolenceVerbal
resistance
Severeforce
Moderateforce
.63.87
.44
.89
.69
.56
.74
.31
SocialSupport
Familysupport
Friendshipsupport
Intimatesupport
.13
–.33
.78
.73
.55
Wishfulthinking
PTSDSymptomatology
Socialwithdrawal
Physicalresistance
Avoidance
Arousal
.78
.85
.87
.64
AcknowledgmentStatus
-.61
Self-criticism
MaladaptiveCoping
Re-experiencing
PTSD symptoms were predicted by assault acknowledgment (path included: BayesianInformation Criterion = 18,951.22; path dropped: Bayesian Information Criterion =18,945.59). In this model, a significant direct effect with PTSD symptoms was foundfor maladaptive coping (β = .64, p < .001); however, the path from assault violence toPTSD symptoms was not significant (β = .13, p = .05). The model accounted for 49%of the variance in PTSD symptoms. Assault violence (β = .31, p < .001) and social sup-port (β = –.33, p < .001) significantly predicted maladaptive coping, and the modelexplained 25% of the variance in maladaptive coping. In addition, acknowledgment(β = –.61, p < .001) was significantly predicted by assault violence. Assault violence(β = .20, p < .001) and social support (β = –.21, p < .001) had significant indirecteffects on PTSD symptoms through maladaptive coping. Finally, like the previousmodels, all of this model’s modification indices were less than 15.0.Because there were differences between acknowledged and unacknowledged
victims in the amount of time that had passed since the assault, whether the victimand assailant had engaged in binge drinking at the time of the rape, and the rela-tionship the victim had with the assailant, we examined whether any of these vari-ables predicted PTSD symptomatology. First, months since the assault occurred was
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
added to the model (depicted in Figure 2) as a predictor of PTSD symptomatology.Because months since assault did not significantly predict PTSD symptoms (β = –.05,p = .25), we removed it from the model. Next, binge drinking by the victim andassailant were added to the model as predictors of PTSD symptoms. However, thismodel showed poor fit to the data, χ2(38) = 98.69, p < .001, CFI = .86, TLI = .88,RMSEA = .07, and likewise these variables were removed from the model. Finally, thevictim’s relationship with the assailant (romantic/nonromantic) did not significantlypredict PTSD symptoms (β = .01, p = .43) and thus was removed from the model.
Discussion
As in some previous studies, unacknowledged victims reported fewer symptomsof PTSD than acknowledged victims and were less likely to report sufficient currentsymptoms of PTSD to suggest they met diagnostic criteria for this disorder. However,it is notable that despite the fact that unacknowledged assaults were significantly lessviolent than acknowledged assaults, and the victims themselves did not characterizethe experience as a victimization, a sizable percentage (30%) of unacknowledgedvictims’ responses suggested they met current diagnostic criteria for PTSD. In thestructural equation model, acknowledgment status did not emerge as a significant pre-dictor of PTSD symptomatology, and the addition of a path from acknowledgmentstatus to PTSD did not result in improvement in model fit. In addition, removal of thepath from acknowledgment to PTSD symptomatology did not affect the amount ofvariance in PTSD symptomatology explained. The structural equation model alsosuggested that assault violence may be a potential mechanism to explain differencesin PTSD symptomatology. As predicted, less violence in the assault was associatedwith being an unacknowledged victim. In addition, greater assault violence was asso-ciated with greater PTSD symptomatology, primarily through the relation betweenassault violence and reliance on maladaptive coping. It is also worth noting that othervariables in which unacknowledged and acknowledged victims differed (monthssince assault, binge drinking during the assault, being romantically involved with theassailant) did not improve the prediction of PTSD symptoms or overall model fit.The results also provide some intriguing findings regarding the roles of assault vio-
lence, maladaptive coping, and social support in predicting PTSD symptomatology.Unlike in some prior research (e.g., Bownes, O’Gorman, & Sayers, 1991; Kilpatricket al., 1989), assault violence was not directly associated with PTSD symptomatol-ogy. However, greater assault violence was associated with greater reliance on mal-adaptive coping strategies with respect to the rape and indirectly predicted PTSDsymptomatology through coping. Thus, one possibility is that victims of more violentassaults are more likely to turn to maladaptive avoidant and ruminative strategies incoping with the rape, perhaps because they are more likely to experience negativecognitions during the assault and high levels of trauma symptoms immediately
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
afterward (Dunmore, Clark, & Ehlers, 1999, 2001). Reliance on these maladaptivestrategies could then lead to a perpetuation and exacerbation of PTSD symptomatol-ogy through several processes including avoidance attempts leading to paradoxicalhyperattention to trauma-related thoughts (Snyder & Pulvers, 2001) and perpetuationof symptomatology by maladaptive ruminative strategies such as self-criticism andunproductive counterfactual thinking (Branscombe et al., 2003). Similarly, social sup-port was not a direct predictor of PTSD symptomatology but instead was indirectlyassociated with PTSD symptomatology through its relationship with maladaptivecoping. There are a number of potential ways in which social support could influencevictims’ coping strategies. For example, individuals with a strong support networkmay be more likely to use it to assisting them in implementing adaptive coping strate-gies (Folkman & Lazarus, 1990; Littleton & Radecki Breitkopf, 2006; Silver &Wortman, 1980). Individuals with supportive relationships may also feel more confi-dent in their ability to actively cope with the trauma (Littleton & Radecki Breitkopf,2006; Silver & Wortman, 1980). In addition, survivors’ support networks may chal-lenge their use of maladaptive strategies, reducing reliance on such strategies(Littleton & Radecki Breitkopf, 2006; Silver & Wortman, 1980).Limitations of the current study should be noted. The study involved a sample of
college rape victims and thus may not generalize to other populations of victims,although it should be noted that the sample was fairly diverse with regard to age andethnicity. In addition, the results represent cross-sectional data, limiting our ability todraw causal inferences. Indeed, it seems possible that there exist reciprocal relation-ships among some of the variables in the model. For example, experiencing posttrau-matic symptoms may lead to greater reliance on maladaptive strategies in coping withthe rape. In another example, unacknowledged victims who experience significantand persistent distress may reconceptualize their experience as a victimization.3 Also,although it is not a limitation per se, it should be noted that we used a broader con-ceptualization of unacknowledged rape (those victims who did not conceptualizetheir experience as a victimization) than did some prior research (i.e., victims who didnot label the experience a rape). We felt that what was key in defining acknowledg-ment was whether women conceptualized their experience as a victimization ratherthan whether they chose the specific label “rape” for their experience. Finally, we didnot examine a number of potential factors that could influence PTSD symptomatol-ogy, such as previous trauma history, peritraumatic reactions, disclosure reactions,resource loss, and trauma-related cognitions (e.g., the world is a dangerous place).Despite these limitations, the results have important implications for future work.
Results indicate that unacknowledged victims can be traumatized by their experi-ence, even though they do not conceptualize their experience as a victimization.Results also suggest that differences in trauma symptoms between unacknowledgedand acknowledged victims may be accounted for in part by differences in assaultviolence between these two groups. We believe that the results of this study suggestthat focusing on victims’ distress and trauma symptoms following rape should
Littleton, Henderson / College Rape Victims 163
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
include both unacknowledged and acknowledged victims. Results also highlight thepotential role of coping in producing and perhaps maintaining PTSD symptoms fol-lowing rape. In contrast, social support may act as a resiliency-promoting factor fol-lowing rape, perhaps through its influence on victims’ coping. Thus, future workshould continue to focus on victims’ postassault experiences in evaluating predictorsof distress rather than focusing exclusively on characteristics of the assault. There isalso a clear need for longitudinal research evaluating the likely complex relation-ships among assault factors, acknowledgment status, postassault experiences, anddistress among victims. Finally, there is a continued need for research focusing onthe experiences of diverse samples of rape victims.
Notes
1. Because likelihood ratio difference tests are not valid using the weighted least squares estimator,we reran the models using robust maximum likelihood estimation to conduct the likelihood ratio differ-ence tests.
2. It should be noted that although the weighted least squares estimator will produce correct estimatesusing categorical data, it does sacrifice some information with respect to the continuous indicators.Therefore, model fit will be worse with weighted least squares estimation than it would be under robustmaximum likelihood estimation.
3. Although procedures have been developed to test reciprocal relationships using structural equationmodeling, these models are notoriously difficult to estimate. Furthermore, the models we have presentedhere provide a more direct test of our hypotheses and are consistent with previous research in the area.Therefore, we decided not to report the results of such nonrecursive structural equation models.
References
Abbey, A., BeShears, R., Clinton-Sherrod, A. M., & McAuslan, P. (2004). Similarities and differences inwomen’s sexual assault experiences based on tactics used by the perpetrator. Psychology of WomenQuarterly, 28, 323-332.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders(4th ed.). Washington, DC: Author.
Arata, C. M. (1999). Coping with rape: The roles of prior sexual abuse and attributions of blame. Journalof Interpersonal Violence, 14, 62-78.
Bondurant, B. (2001). University women’s acknowledgment of rape: Individual, situational, and socialfactors. Violence Against Women, 7, 294-314.
Botta, R. A., & Pingree, S. (1997). Interpersonal communication and rape: Women acknowledge theirassaults. Journal of Health Communication, 2, 197-212.
Boudreaux, E., Kilpatrick, D. G., Resnick, H. S., Best, C. L., & Saunders, B. E. (1998). Criminal victim-ization, posttraumatic stress disorder, and comorbid psychopathology among a community sample ofwomen. Journal of Traumatic Stress, 11, 665-678.
Bownes, I. T., O’Gorman, E. C., & Sayers, A. (1991). Assault characteristics and posttraumatic stress dis-order in rape victims. Acta Psychiatrica Scandinavica, 83, 27-30.
Branscombe, N. R., Wohl, M. J. A., Owen, S., Allison, J. A., & N’gbala, A. (2003). Counterfactual thinking,blame assignment, and well-being in rape victims. Basic and Applied Social Psychology, 25, 265-273.
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
Brener, N. D., McMahon, P. M., Warren, C. W., & Douglas, K. A. (1999). Forced sexual intercourse andassociated health-risk behaviors among female college students in the United States. Journal ofConsulting and Clinical Psychology, 67, 252-259.
Breslau, N., Kessler, R. C., Chilcoat, H. D., Schultz, L. R., Davis, G. D., & Andreski, P. (1998). Traumaand posttraumatic stress disorder in the community: The 1996 Detroit area survey of trauma. Archivesof General Psychiatry, 55, 626-632.
Cloutier, S., Martin, S. L., & Poole, C. (2002). Sexual assault among North Carolina women: Prevalenceand health risk factors. Journal of Epidemiology and Community Health, 56, 265-271.
Cole, T. B. (2006). Rape at U.S. colleges often fueled by alcohol. Journal of the American MedicalAssociation, 296, 504-505.
Conoscenti, L. M., & McNally, R. J. (2006). Health complaints in acknowledged and unacknowledgedrape victims. Anxiety Disorders, 20, 372-379.
Dunmore, E., Clark, D. M., & Ehlers, A. (1999). Cognitive factors involved in the onset and maintenanceof posttraumatic stress disorder (PTSD) after physical or sexual assault. Behaviour Research andTherapy, 37, 809-829.
Dunmore, E., Clark, D. M., & Ehlers, A. (2001). A prospective investigation of the role of cognitive fac-tors in persistent posttraumatic stress disorder (PTSD) after physical or sexual assault. BehaviourResearch and Therapy, 39, 1063-1084.
Fisher, B. S., Daigle, L. E., Cullen, F. T., & Turner, M. G. (2003). Acknowledging sexual victimization asrape: Results from a national-level study. Justice Quarterly, 20, 535-574.
Foa, E. B., Riggs, D. S., Dancu, C. V., & Rothbaum, B. O. (1993). Reliability and validity of a brief instru-ment for assessing post-traumatic stress disorder. Journal of Traumatic Stress, 6, 459-473.
Folkman, S., & Lazarus, R. S. (1990). Coping and emotion. In N. L. Stein, B. Leventhal, & T. Trabasso (Eds.),Psychological and biological approaches to emotion (pp. 313-332). Hillsdale, NJ: Lawrence Erlbaum.
Frazier, P. A., & Seales, L. M. (1997). Acquaintance rape is real rape. In M. D. Schwartz (Ed.),Researching sexual violence against women: Methodological and personal perspectives (pp. 54-64).Thousand Oaks, CA: Sage.
Gavey, N. (1999). “I wasn’t raped, but . . .” In S. Lamb (Ed.), New versions of victims: Feminists strug-gle with the concept (pp. 57-81). New York: New York University Press.
Harned, M. S. (2004). Does it matter what you call it? The relationship between labeling unwanted sex-ual experiences and distress. Journal of Consulting and Clinical Psychology, 72, 1090-1099.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis:Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1-55.
Johnson, D. M., Sheahan, T. C., & Chard, K. M. (2003). Personality disorders, coping strategies, and post-traumatic stress disorder in women with histories of childhood sexual abuse. Journal of Child SexualAbuse, 12, 19-39.
Kahn, A. S., & Andreoli Mathie, V. (2000). Understanding the unacknowledged rape victim. In C. BrownTravis & J. W. White (Eds.), Sexuality, society, and feminism (pp. 377-403). Washington, DC:American Psychological Association.
Kahn, A. S., Andreoli Mathie, V., & Torgler, C. (1994). Rape scripts and rape acknowledgment.Psychology of Women Quarterly, 18, 53-66.
Kahn, A. S., Jackson, J., Kully, C., Badger, K., & Halvorsen, J. (2003). Calling it rape: Differences inexperiences of women who do or do not label their sexual assault as rape. Psychology of WomenQuarterly, 27, 233-242.
Keppel, G., (1991). Design and analysis: A researcher’s handbook (3rd ed.). Englewood Cliffs, NJ:Prentice Hall.
Kilpatrick, D. G., Saunders, B. E., Amick-McMullan, A., Best, C. L., Veronen, L. J., & Resnick, H. S.(1989). Victim and crime factors associated with the development of crime-related post-traumaticstress disorder (PTSD). Behavior Therapy, 20, 199-214.
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
Kilpatrick, D. G., Saunders, B. E., Veronen, L. J., Best, C. L., & Von, J. M. (1987). Criminal victimiza-tion: Lifetime prevalence, reporting to the police, and psychological impact. Crime & Delinquency,33, 479-489.
Kline, R. B. (2005). Principles and practice of structural equation modeling (2nd ed.). New York: Guilford.Koss, M. P. (1985). The hidden rape victim: Personality, attitudinal, and situational characteristics.
Psychology of Women Quarterly, 9, 193-212.Koss, M. P., Dinero, T. E., Seibel, C. A., & Cox, S. L. (1988). Stranger and acquaintance rape: Are there
differences in the victim’s experience? Psychology of Women Quarterly, 12, 1-24.Koss, M. P., Figueredo, A. J., Bell, I., Tharan, M., & Tromp, S. (1996). Traumatic memory characteris-
tics: A cross-validated mediational model of response to rape among employed women. Journal ofAbnormal Psychology, 105, 421-432.
Koss, M. P., & Gidycz, C. A. (1985). Sexual Experiences Survey: Reliability and validity. Journal ofConsulting and Clinical Psychology, 53, 422-423.
Layman, M. J., Gidycz, C. A., & Lynn, S. J. (1996). Unacknowledged versus acknowledged rape victims:Situational factors and posttraumatic stress. Journal of Abnormal Psychology, 105, 124-131.
Littleton, H. L., Axsom, D., Radecki Breitkopf, C., & Berenson, A. B. (2006). Rape acknowledgment andpostassault experiences: How acknowledgment status relates to disclosure, coping, worldview, andreactions received from others. Violence and Victims, 21, 761-778.
Littleton, H. L., Horsley, S., John, S., & Nelson, D. V. (2007). Trauma coping strategies and psychologi-cal distress: A meta-analysis. Journal of Traumatic Stress, 20, 977-988.
Littleton, H. L., & Radecki Breitkopf, C. (2006). Coping with the experience of rape. Psychology ofWomen Quarterly, 30, 106-116.
Littleton, H. L., Radecki Breitkopf, C., & Berenson, A. B. (2008). Beyond the campus: Unacknowledgedrape among low income women. Violence Against Women, 14, 269-286.
Littleton, H. L., Rhatigan, D., & Axsom, D. (2007). Unacknowledged rape: How much do we know aboutthe hidden sexual assault victim? Journal of Aggression, Maltreatment, and Trauma, 14(4), 57-74.
Marx, B. P., & Soler-Baillo, J. M. (2005). The relationships among risk recognition, autonomic and self-reported arousal, and posttraumatic stress symptomatology in acknowledged and unacknowledgedvictims of sexual assault. Psychosomatic Medicine, 67, 618-624.
Masho, S. W., Odor, R. K., & Adera, T. (2005). Sexual assault in Virginia: A population-based study.Women’s Health Issues, 15, 157-166.
McMullin, D., & White, J. W. (2006). Long-term effects of labeling a rape experience. Psychology ofWomen Quarterly, 30, 96-105.
Muthén, L. K., & Muthén, B. O. (1998-2007). Mplus user’s guide (4th ed.). Los Angeles: Author.National Institute on Alcohol Abuse and Alcoholism (2006, January). Underage drinking: Why do ado-
lescents drink, what are the risks, and how can underage drinking be prevented? Alcohol Alert, 67.Retrieved April 3, 2007, from www.niaaa.nih.gov/Publications/AlcoholAlerts/default.htm.
Reips, U.-D. (2002). Internet-based psychological experimenting: Five dos and five don’ts. Social ScienceComputer Review, 20, 241-249.
Rothbaum, B. O., Foa, E. B., Riggs, D. S., Murdock, T., & Walsh, W. (1992). A prospective examinationof post-traumatic stress disorder in rape victims. Journal of Traumatic Stress, 5, 455-475.
Russell, D. E. H. (1982). The prevalence and incidence of forcible rape and attempted rape of females.Victimology, 7, 81-93.
Schwarz, G. (1978). Estimating the dimension of a model. Annals of Statistics, 6, 461-464.Silver, R. L., & Wortman, C. B. (1980). Coping with undesirable life events. In J. Garber & M. E. P. Seligman
(Eds.), Human helplessness: Theory and applications (pp. 279-339). New York: Academic Press.Snyder, C. R., & Pulvers, K. M. (2001). Dr. Seuss, the coping machine, and “Oh, the Places You’ll Go.”
In C. R. Snyder (Ed.), Coping with stress: Effective people and processes (pp. 3-29). Oxford, UK:Oxford University Press.
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from
Tobin, D. L. (2001). User manual for the Coping Strategies Inventory. Unpublished manuscript.Tobin, D. L., Holroyd, K. A., Reynolds, R. V., & Wigal, J. K. (1989). The hierarchical factor structure of
the Coping Strategies Inventory. Cognitive Therapy and Research, 13, 343-361.Ullman, S. E., & Filipas, H. H. (2001). Predictors of PTSD symptom severity and social reactions in sex-
ual assault victims. Journal of Traumatic Stress, 14, 369-389.Ullman, S. E., Townsend, S. M., Filipas, H. H., & Starzynski, L. L. (2007). Structural models of the rela-
tions of assault severity, social support, avoidance coping, self-blame, and PTSD among sexual assaultsurvivors. Psychology of Women Quarterly, 31, 23-37.
Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The Multidimensional Scale ofPerceived Social Support. Journal of Personality Assessment, 52, 30-41.
Heather Littleton is an assistant professor in the Department of Psychology at East Carolina University.Her research interests span several areas related to women’s health including sexual victimization amongwomen, rape acknowledgment, coping and recovery following traumatic events, and body image.
Craig E. Henderson is an assistant professor in the Department of Psychology and Philosophy at SamHouston State University. His research interests encompass a broad range of topics, including family psy-chology, substance abuse, and advanced data analytic methods.
Littleton, Henderson / College Rape Victims 167
at UNIV OF MIAMI on December 13, 2010vaw.sagepub.comDownloaded from