Originally, carcinoid tumours denoted all gastroente-ropancreatic endocrine tumours which were subdividedaccording to their embryological origin into foregut carci-noids (stomach, duodenum, upper jejunum, pancreas),midgut carcinoids (lower jejunum, ileum, appendix andcaecum) and hindgut carcinoids (colon, rectum) [1]. How-ever, this classification does not accurately describe thenatural history and clinical behaviour of all gut endocrinetumours. A revised classification of endocrine tumourshas been proposed which takes into account tumour loca-tion, tumour size, angioinvasion, hormone production,histological grade and proliferative index [2]. Using this
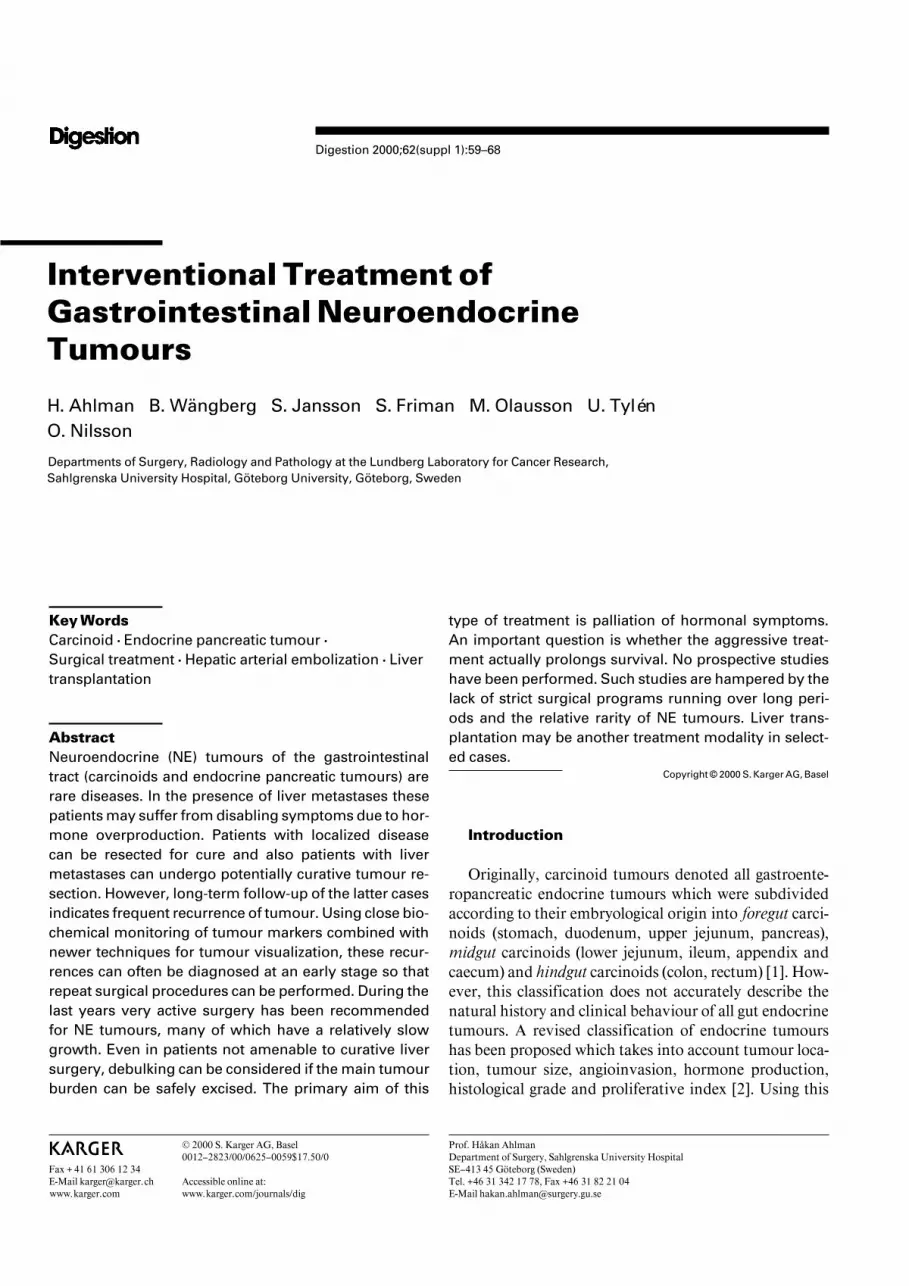
Fig. 1. Characteristic morphological fea-tures of well-differentiated endocrine tu-mours (midgut carcinoid, MC) and aggres-sive neuroendocrine carcinomas (NEC). Inthe well-differentiated tumours, there arenests, or trabeculae, of tumour cells whichare uniform in size and shape with low mi-totic activity. In the NEC, tumour cells growin solid sheets with frequent necrosis. Thereis considerable variation in the size of tu-mour cells, which display high mitotic activi-ty. Immunocytochemical staining for endo-crine markers such as chromogranin A (CgA)is strongly positive in both well-differen-tiated endocrine tumours and NEC. Theproliferative activity, assessed by Ki67 im-munostaining, is low in the well-differen-tiated endocrine tumours but high in theNEC.
classification, digestive neuroendocrine (NE) tumours aredivided into well-differentiated tumours comprising car-cinoid tumours of the gastrointestinal tract and endocrinepancreatic tumours (EPT) and poorly differentated (neu-ro)endocrine carcinomas (NEC or PDEC). NE tumoursare usually diagnosed at a late stage when the disease isdisseminated and causes hormonal symptoms. The work-up of the patient includes CT, octreotide scintigraphy,biochemical screening and analysis of biopsy material.The histopathological examination aims at classifying thetumour regarding origin, biological behaviour and prog-nosis. While immunohistochemical staining for amineand peptide hormones may help to define the origin of thetumour, its biological behaviour has been notoriously dif-ficult to assess. However, systematic histopathologicalanalysis of NE tumours regarding growth pattern, degreeof neuroendocrine differentiation and proliferative capac-
ity may provide some information regarding prognosis[3]. Analysis of growth patterns includes evaluation oftumour cell growth, degree of cellular and nuclear atypiaas well as presence, or absence, of necrosis. All factors arethen summarized in a histological grade (G1–G3) scale.Neuroendocrine differentiation is evaluated by immuno-cytochemistry using antibodies against granule proteins(chromogranin A, synaptophysin) or cytosolic markers(NSE, PGP 9.5). Well-differentiated tumours are positivefor all markers in a vast majority of tumour cells, whilepoorly differentiated endocrine tumours often lack, orhave scant labeling for granule markers, while the cyto-solic markers are retained. Proliferative capacity can beassessed by counting mitoses, but is more reliably esti-mated by analysing the number of tumour cells expressingthe Ki67 antigen (fig. 1). Following a systematic histo-pathological analysis, NE tumours can be broadly divided
Intervention of Neuroendocrine Tumours Digestion 2000;62(suppl 1):59–68 61
into well-differentiated tumours (comprising the majorityof carcinoid tumours and EPT) with good or intermediateprognosis and neuroendocrine carcinomas (NEC), orpoorly differentiated endocrine carcinomas (PDEC),which have a sinister prognosis. In the future, other fac-tors such as angiogenic capacity of tumour cells and spe-cific genetic changes may prove to be valuable tools indetermining prognosis, biological behaviour and responseto therapy.
Anaesthesiological Considerations
Prior to all interventional treatment of NE tumours thetumour type and hormone production must be assessed.Patients with midgut carcinoids are pretreated with long-acting somatostatin analogues, e.g. octreotide (100 Ìg ! 4s.c.), to prevent carcinoid crises during intervention. Incase of a crisis reaction with bronchoconstriction andhypotension, adrenergic drugs should be avoided, sincecarcinoids may express adrenoceptors. Instead the surgi-cal manipulation should be interrupted, volume substi-tuted according to haemodynamic parameters and iter-ated doses of octreotide and cortisone given. Spinal anaes-thesia with markedly reduced blood pressure may elicitcarcinoid crises due to compensatory release of catechol-amines from the adrenals in turn causing release of sero-tonin from the tumour [4]. For postoperative pain, epidu-ral analgesia is preferred. Foregut carcinoids with excessproduction of histamine may cause an atypical carcinoidsyndrome (generalized flushing, lacrimation, hypoten-sion, cutaneous oedema, bronchoconstriction). Emboliza-tion therapy of liver metastases in these patients may becontraindicated due to noncontrollable release reactions.The cornerstone to correct diagnosis of these tumours isanalysis of the main histamine metabolite, methylimida-zole acetic acid (MelmAA) in urine [5]. Patients withhistamine-producing tumours are optimally pretreatedwith a combination of somatostatin analogues, blockadeof histamine receptors and cortisone. Histamine-liber-ating agents, e.g. morphine and tubocurarine, should beavoided. For glucagonoma and VIPoma, preoperativetreatment with octreotide is usually adequate. Patientswith gastrinoma maintain their medication with omepra-zole for a period after removal of the tumour, since theyhave elevated gastric acid secretion due to hypertrophicgastric mucosa. Patients with large insulinomas may re-quire hypertonic glucose after tumour removal and closeglucose monitoring is necessary.
Surgical Treatment of Locoregional Disease
Surgery is the only option for curative treatment of NEtumours of the gastrointestinal tract. There is an evidentcorrelation between the size of the primary tumour andpresence of metastatic disease for lesions in certain re-gions, e.g. appendix and rectum [6]. Tumours !1 cm arecured by simple excision, or appendectomy, while largeror locally invasive tumours may require more extensivesurgery [7]. In case of small intestinal midgut carcinoids,tumour size does not influence prognosis [8]. Two-thirdsof small midgut carcinoids (!1 cm) have microscopicspread to lymph nodes and almost half of the patientshave liver metastases [9]. Midgut carcinoids may be mul-tiple and require resection of involved intestine and mes-entery. The tumours are often accompanied by retroperi-toneal fibrosis, or fibrotic mesenteric reaction, leading toconstriction of the bowel lumen and intestinal ischaemia.The primary surgical treatment should therefore attemptsharp dissection of the high mesenteric lymph nodes tomobilize the small intestine for adequate resection inorder to prevent local complications.
Gastric carcinoids are divided into four subtypes: Hy-pergastrinemia induces hyperplasia of enterochromaffin-like (ECL) cells with subsequent progression into smallmultiple carcinoids in the corpus-fundus region. This con-dition can be associated with chronic atrophic gastritis(type I) or MEN-1 gastrinoma (type II). Type III tumoursare larger solitary lesions, not associated with hypergastri-nemia, and type IV tumours comprise very rare tumours,e.g. NEC. Type I lesions are fairly benign and probablybest managed by endoscopic excision and follow-up. TypeII lesions may require wider excision, or gastric resection.The role of antrectomy to reduce gastrin levels in order toreverse ECL cell carcinoidosis has not been fully evaluat-ed. Type III tumours and NEC require cancer surgerywhen resectable [10].
The surgical management of EPT also varies withtumour type, e.g. simple enucleation of small benign insu-linomas or pancreatic resection of larger, more aggressivetumours like gastrinoma, glucagonoma, VIPoma, or non-functional tumours. The MEN-1 pancreas is a surgicalenigma, which may lead to repeat resection of successive-ly diagnosed tumours eventually ending up with subtotalor completion pancreatectomy [11].
The surgical treatment of primary NE tumours andlocoregional disease is not controversial. Treatment ofpatients with liver metastases is more demanding andmay involve several interventional modalities. For futurerandomized studies of medical treatment in advanced
disease, primary surgery is of importance to prevent localcomplications and correctly stage the tumour disease.
Interventional Treatment of Liver Metastases
The surgical/interventional treatment for liver metas-tases can be divided into four modalities: liver resection,vascular interventions, other peroperative procedures andliver transplantation.
Liver ResectionAnatomical liver resection can be performed for le-
sions situated within any of the 8 liver segments, eachindependently supplied by branches of the hepatic arter-ies and portal vein draining into one hepatic duct. Forcurative resections a good clearance margin is required,but for NE tumours resected for palliative reasons thismargin can be narrowed and local tumour deposits can beremoved by atypical resections. The extent of tumour dis-ease is assessed by inspection, palpation and intraopera-tive ultrasound. The latter technique allows a good defini-tion of liver anatomy and the relation between the tumourand the portal and hepatic venous pedicles. This is of spe-cial importance if techniques like cryo- or laser therapyare used.
The most common variant in arterial anatomy isreplacement of the right hepatic artery by a branch of thesuperior mesenteric artery. For right-sided liver tumours,preoperative angiography is therefore often valuable. Forright hepatectomy it may be easy to control the righthepatic vein outside the liver rather than within theparenchyma during resection. Inflow control of the lesseromentum is usually applied by clamping. The safe dura-tion of hepatic ischemia may exceed 1 h but can bereduced in hepatic dysfunction. Therefore the shortestpossible clamping should be used, since it is associatedwith intestinal congestion and accumulation of toxic me-tabolites.
For left hepatectomy the left and middle hepatic veinshave their junction at variable levels, which means thatthey cannot always be controlled separately outside theliver. Division of the liver parenchyma most often in-cludes the use of an ultrasonic surgical aspirator, whichdestroys liver cells leaving the more resistant biliary andvascular structures intact allowing exact placement ofligatures and clips.
Metastasectomy of multiple deposits usually requiresintermittent clamping of inflow vessels, diathermic inci-sion around the individual lesions and blunt dissection.
To obtain a good debulking effect, the principles of ana-tomical resection, wedge resection and metastasectomyare often combined. The operative mortality for electiveliver surgery must be low. In most series, figures less than5% are reported [12]. Prophylactic use of antibiotics hasdecreased infectious complications, but morbidity is stillmore frequently associated with sepsis than bleeding dur-ing surgery.
For patients with multiple liver tumours, Farges andBelghiti [13] recently described the two-stage liver resec-tion strategy. As the first step the primary tumour and theleft lateral segment of the metastatic liver are removedand the right branch of the portal vein ligated. The latterprocedure induces hypertrophy of the residual left liver inabout 6 weeks. Thereafter, extended right-sided hepatec-tomy can be performed.
ResultsOver the last decade, very active surgery has become
increasingly more common as primary treatment of low-grade NE tumours and their metastases. Curative liversurgery (= no gross residual tumour) must be consideredfor all patients with resectable disease. Palliative liver sur-gery can be considered for some patients with slowtumour growth and severe hormonal symptoms. Pallia-tive liver resections are generally performed in patients inwhom more than 90% of the tumour volume can be safelyexcised [14, 15]. In a series of patients with NE tumours10 years ago, the liver resection rate with curative intentwas about 10% [16, 17]. In our own consecutive series of64 patients with the midgut carcinoid syndrome and livermetastases, 14 patients (22%) with unilateral liver lesionunderwent intentionally curative liver surgery and nor-malized their tumour markers [18]. In recent Americanand French series [19–21], curative, or palliative, liverresections were performed in 40–50% of patients with NEtumours. In all referred series the mortality was low(!5%) and the complication rate below 30%.
One evident problem with an active liver surgery pro-gram is that many resections are considered curative atthe time of surgery but later proven not to be. With accessto sensitive diagnostic tools (specific tumour markers,octreotide scintigraphy, spiral CT and MR) and carefulfollow-up, subclinical disease can be discovered and lim-ited lesions re-resected [22]. If multiple metastases recur,vascular interventions, or other treatments, are at hand.In case there is no extrahepatic disease these patients maybe candidates for liver transplantation.
More than 10 years ago, Norton et al. [23] reportedvery active surgery in selected patients with advanced gas-
Intervention of Neuroendocrine Tumours Digestion 2000;62(suppl 1):59–68 63
trinoma, who all underwent major liver resections com-bined with other debulking procedures at tumour progres-sion, followed by chemotherapy. On a short-term basis,good symptomatic relief and markedly reduced tumourmarkers were seen with this strategy. Of 42 consecutivepatients with EPT treated over a 10-year period at theNIH, 17 were resected and 25 were deemed inoperableand medically treated [19]. There seemed to be a 5-yearsurvival advantage in the surgically treated group (79%)versus the medically treated (28%) in this selected series.There was no operative mortality, but the tumour diseaserecurred in all surgically treated patients within 8 years.Such a delay of the tumour disease with a long medica-tion-free interval, as also observed for midgut carcinoids[18], is a major therapeutic advantage in itself.
McEntee et al. [15] from the Mayo Clinic also reportedencouraging results in 37 patients treated with liver resec-tion, including both carcinoids and EPT. They reported17 curative resections (9 with hormonal symptoms). Eightwere completely relieved of symptoms and 5 of these werealive after 2 years with no signs of residual disease. Twen-ty patients had palliative resection (16 with hormonalsymptoms). Eight experienced symptom relief and 5 werealive after 1 year. In a review from the Mayo Clinic [20],74 patients with metastatic NE tumours underwent liverresection including 41 patients with midgut carcinoids.The 4-year survival was 73%, even though nearly two-thirds of the procedures were palliative. Symptomaticresponse to liver resection was seen in 90% with a meanduration of response of almost 20 months. Resection oflarge (110 cm) dominant lesions was clearly related tosymptom relief and reduction of tumour markers. Therole of resection for enhanced survival is still not provenin randomized studies.
Vascular InterventionsMarkowitz [24] in 1952 first proposed hepatic vascular
interventions as therapeutic procedures. The backgroundfor ischaemic treatment of NE tumours of the liver is theirmain blood supply from the hepatic artery [25, 26] of thetumour with maintained portal perfusion of the normalliver parenchyma. Ischaemia can be achieved by severaltechniques directed against the hepatic artery: ligation,selective embolization or temporary occlusion. The meth-ods differ in completeness, distribution and duration ofischemia [27].
Ligation of the hepatic artery was clinically introducedmore than 30 years ago [28]. It has largely been aban-doned due to difficulties to obtain adequate ischaemiawith the rich collateral blood supply to the liver, signifi-
cant mortality in end-stage patients and restricted possi-bilities for repeat vascular interventions.
Selective embolization of the hepatic arteries causes atemporary, but complete ischaemia, since the arterial treedistal to the point of injection is filled with embolizationmaterial [29]. Contraindications are tumour burden ex-ceeding 50% of the liver volume, occlusion of the portalvein, hyperbilirubinaemia and persistently elevated liverenzymes. Relative contraindications are contrast allergy,coagulopathies, extrahepatic tumour dominance or poorperformance status of the patient [30]. In our experience,patients with tumour volumes exceeding 50% can alsosafely undergo this type of treatment using iterated super-selective embolizations well separated in time. A similarstrategy can also be followed for patients with previoushemihepatectomy and recurrent tumours in the residualliver. Immediately before embolization an arteriogram isperformed to demonstrate the arterial anatomy, tumourblood flow and patency of the portal vein [31, 32]. Bothabsorbable and nonabsorbable embolization materialshave been used, e.g. gelfoam powder and alcohol-Ivalonparticles [30, 33]. The need to maintain an open route forrepeat procedures excludes the choice of steel coils in theproximal arterial segment. Aiming at complete ischaemiaof long duration, efforts have been directed toward small-er permanent emboli to obtain a good peripheral isch-aemia without reaching the liver sinusoids [29, 34].
Chemoembolization is embolization combined withliver-targeted intra-arterial administration of chemother-apy. Hajarizadeh et al. [35] found symptomatic improve-ment to 5-FU in carcinoid patients with a mean durationof 2 years associated with significant tumour regression inhalf of the patients. Similar response rates were reportedfor several types of NE tumours using doxorubicin, mito-mycin C and cisplatinum [36–38]; these authors reportedtumour regression in one-third of their patients with amodified embolization procedure using iodized oil, doxo-rubicin and gelfoam particles.
Some centres have reported good symptom palliationrelated to biochemical and clinical tumour responses inpatients with the midgut carcinoid syndrome using tem-porary occlusion of the hepatic artery via external vesselloops (positioned during surgery) and repeat periods ofapplied ischaemia [39]. For long-term treatment, tempo-rary occlusion can be applied via a port-operated tourni-quet around the hepatic artery. A combination of periph-eral embolization and temporary proximal occlusion canhave additive effects in therapy-resistant cases.
The embolization procedure is accompanied by liverpain, transient elevation of liver enzymes, nausea and late
fever reaction. Embolization may lead to serious compli-cations in individual patients (gallbladder ischaemia,pancreatitis, liver abscess, vascular damage and aneurysmformation, hepatorenal syndrome and hormonal crises).The mortality in the major series is less than 5% [30]. Tominimize adverse reactions, several precautions can beundertaken, which include first of all an experiencedinterventional radiologist, but also the use of coaxial cath-eter systems for superselective catheterization with lowrisk of vascular damage, prophylactic use of octreotide,cholecystectomy at the time of primary surgery to elimi-nate the risk for gallbladder perforation, intravenous hy-dration and haemodynamic monitoring to reduce the riskfor the hepatorenal syndrome [4, 27].
To monitor the outcome of ischaemic therapy, CT scanand biochemical tumour markers are used. According toour follow-up schedule these investigations are comparedwith preoperative results in the outpatient clinic 1 monthafter completion of embolization therapy [18]. It would bea therapeutic advantage if the response to ischaemia couldbe followed closer to embolization. For this purpose, wehave tried to develop better monitoring systems. Weobserved bilateral tumour regression in individual pa-tients only subjected to unilateral embolization indicatingactivation of systemic antitumour effects, e.g. activationof natural killer (NK) cells [40]. In one series, responsivepatients developed rapid lymphocytosis with predomi-nance of NK cells; in vitro the cytotoxic activity of iso-lated lymphocytes from these patients increased shortlyafter embolization. The observed early immunologic re-sponses were closely correlated with late markers of thetherapeutic effect [41]. MR spectroscopy of liver tumoursbefore and after embolization with regard to energy-richphosphates may also give information on the degree ofischaemia achieved.
ResultsThe result of ischaemic treatment of liver metastases is
obviously dependent on stage of the disease. Coupe et al.[42] reported a series of 63 consecutive patients withadvanced stage, of whom 30 were embolized for pallia-tion. The survival after angiography, or angiography +embolization, was similar in both groups. Mitty et al. [43]reported long-term follow-up of 18 patients treated withembolization with prolongation of the expected survivalby 2 years. Carrasco et al. [34] treated 25 patients with thecarcinoid syndrome. The vast majority of patientsshowed both biochemical responses and tumour regres-sion with an average duration of 1 year. Marlink et al. [44]introduced a different time schedule for embolization in
patients with severe symptoms. Two successive emboliza-tions were performed within 1 week leading to rapidsymptom palliation. In our own study, patients with mid-gut carcinoids were embolized in two settings 1 monthapart after primary surgery [18]. Our 40 patients could bedivided into two equally large groups: responders withmore than 50% tumour reduction and pronounced reduc-tion of 5-HIAA excretion (80%) and nonresponders withless than 50% tumour reduction, and a moderate 5-HIAAreduction (30%) with clear survival advantage in theformer group. In a Norwegian study the response rate tointerferon (IFN) was twice as high in patients subjected toprior embolization indicating additive effects. It shouldbe noted that IFN is a potent enhancer of NK cell cytotox-icity [45].
Reviewing our first 94 embolizations in patients withthe midgut carcinoid syndrome, we met the followingcomplications: Three patients occluded the main hepaticartery (one hepatic abscess), but had excellent symptomrelief. One patient developed an aneurysm of the hepaticartery after the first embolization and a fatal hepatorenalsyndrome after the second embolization. These complica-tions together with 1 case of pancreatitis were all seenamong the initial 11 embolizations before introduction ofa coaxial catheter system. At the subsequent 83 emboliza-tions only two minor complications were seen (transientrenal insufficiency and cardiac arrhythmia).
Peroperative ProceduresTaking advantage of the high expression of somatosta-
tin receptors by several NE tumours, attempts to developradioguided surgery using a hand-held scintillation detec-tor after preoperative injection of radiolabelled somatos-tatin analogues have been evaluated. The indications forradioguided surgery would be recurrent tumours in re-gions not easily investigated by other methods (e.g. neckmetastases of medullary thyroid carcinoma, carcinoidsand EPT), small EPT (e.g. in the MEN-1 syndrome) andas control of adequate tumour removal (e.g. carcinoidmetastases in the mesenteric root after lymph node dissec-tion). Promising results have been reported, but scintilla-tion detection is clearly not sensitive enough to detectmicroscopic tumour growth or microadenomas [46].
At an advanced stage of histamine-producing tumours,ischemic liver treatment is potentially dangerous due tononcontrollable release of tumour products. In individualpatients we have used cytotoxic drugs (melphalan and cis-platinum) delivered by regional hyperthermic liver perfu-sion. During perfusion the venous effluent from the liverwith vasoactive substances was shunted from the systemic
Intervention of Neuroendocrine Tumours Digestion 2000;62(suppl 1):59–68 65
circulation avoiding vasomotor effects. Cytostatic perfu-sion of the isolated liver with simultaneous filtration ofportal vein blood and a maintained systemic circulationwere made possible by a special perfusion catheter in-serted in the caval vein. The surgical technique involvesisolation of the hepatic artery, portal vein and caval veininferior and superior to the liver together with a tempora-ry portocaval shunt that allows blood flow rates to bemaintained in both the hepatic artery and portal lines[47]. Repeat hyperthermic perfusion can be very difficultto perform due to intense fibrotic reaction of the vesselsused for perfusion.
In elderly patients, or patients with progressive diseaseafter previous treatment, percutaneous alcohol injectionsinto isolated liver lesions can be performed under phar-macological blockade [48]. The volume of individual me-tastases is estimated ultrasonographically and the lesionsare injected with equal volumes of absolute alcohol. Dur-ing injection the lesions develop high echogenicity. Withrepeat injections marked symptom palliation related toreduced tumour markers and proven tumour necrosis canbe achieved. Alternatively, the tumour can be destroyedby cryosurgical techniques, which also have the advantagethat multiple lesions can be treated at a single session.Cryoprobes can also be equipped with intraoperativeultrasound for tumour localization. Modern cryoprobescan destroy tumours deep in the liver without damagingthe normal overlying parenchyma [49]. Metastatic livertumours can also be treated by interstitial laser [50] orradiofrequency therapy [51, 52] causing selective thermo-coagulation. These techniques can be used intraoperative-ly or percutaneously. Ultrasound is usually the imagingguidance, but open thermosensitive MR systems for mon-itoring of coagulative effects are being developed [53].
Liver TransplantationLiver transplantation was first regarded as an optimal
mode of treatment for all hepatobiliary malignancies, butthe long-term results for advanced primary liver tumourswere dismal with early tumour recurrence. Today there isa narrow indication for transplantation in small hepato-cellular carcinomas and more unusual tumour types, e.g.fibrolamellar carcinoma and hepatoblastoma. Patientswith secondary liver tumours had a very low survival rate:12% 1 year after transplantation [54]. Better results mightbe expected in patients with secondary NE tumours, sincemetastatic disease of gastrointestinal carcinoids, or EPT,can be limited to the liver for long periods and thesetumours may have slow growth potential. Many of thebiogenic amines and peptides, which are produced by the
primary tumour, are metabolized by the liver. In patientswith liver metastases these products are secreted directlyinto systemic circulation causing invalidating symptoms.When considering liver transplantation for NE tumours,the expected results with conventional treatment strate-gies must be weighed versus the risks with liver transplan-tation and subsequent immunosuppression. This is not aneasy task, since a 5-year survival of 70% can be achievedin patients with midgut carcinoids and liver metastasesusing multimodal therapy and a 10-year survival wellexceeding 50% (fig. 2) [55]. The following indications forliver transplantation in patients with NE tumours may beconsidered:
(1) Metastatic disease limited to the liver, not accessi-ble for curative liver surgery, including recurrent tumoursin patients earlier subjected to curative liver resection andpatients with severe hormonal symptoms due to livertumours not possible to treat with other interventions, e.g.histamine-producing carcinoids.
(2) Tumour progression after embolization and medi-cal therapy in patients with no proven disease outside theliver.
An upper age limit of 55 years has been suggested forliver transplantation. Some centres will not accept atumour mass exceeding 50% of the liver volume, althoughno studies on NE tumour volume and outcome of trans-plantation are available. The overall prognosis for malig-nant EPT is worse than for midgut carcinoids. In our ownseries of EPT patients with liver metastases, the sametreatment program was followed as for carcinoid tumourswith much less favourable results (fig. 2). One reason forthis difference was that patients with high-grade malig-nant tumours (NEC) were included in our series of EPT incontrast to others. NEC have a very poor prognosis andare seldom diagnosed at a resectable stage. For thistumour type, liver transplantation is contraindicated.
A careful assessment of the outcome of primary sur-gery has been emphasized, since growth of residual tu-mour may accelerate during immunosuppression. Usingbiochemical markers, CT/MR and octreotide scintigra-phy residual extrahepatic tumour was revealed in a highproportion of patients worked up for liver transplantation[56]. It therefore seems reasonable to follow a two-stepstrategy with histology-proven radical removal of the pri-mary carcinoid, or EPT with tail location, followed bycareful investigation of extrahepatic metastases prior toliver transplantation. EPT with head location are proba-bly best managed with cluster transplantation (en-blocresection of liver, pancreas and stomach). A careful work-up of extrahepatic disease in these cases may include stag-
Fig. 2. Kaplan-Meier survival analysis in our consecutive series of patients with midgut carcinoids (MC, n = 64) andendocrine pancreatic tumours (EPT, n = 14) and liver metastases from the same time period treated with an activesurgical program (resection of locoregional disease, liver surgery of unilateral liver lesions or embolization of bilateralliver lesions). The series of EPT also include NEC – left panel. Survival analysis of patients with NE tumours (n = 31)after liver transplantation in a French multicenter study – right panel. The similarities between treatment resultsindicate that EPT tumours are more aggressive than MC tumours. (Reproduced by permission of Br J Cancer [55]).
ing laparotomy to verify that the tumour mass can beradically removed by the cluster procedure.
ResultsTen years ago, Starzl’s group [57] introduced liver
transplantation as treatment of NE tumours. Of the first 5patients, 3 survived 7–34 months after surgery. Two yearslater another group reported upon 11 patients, of whommore than half were alive after 6 months [58]. In 1994,Bechstein and Neuhaus [59] reviewed the world litera-ture, which at that time consisted of 30 patients with NEtumour that had undergone liver transplantation (15 EPTand 13 gastrointestinal carcinoids, 1 lung carcinoid and 1nondefined primary carcinoid). The 1-year survival was52%. Transplant-associated deaths occurred in half ofthese patients soon after transplantation; the other deathswere due to recurrent tumour. More strict criteria forselection of patients and concentration of liver transplan-tation to centres of excellence will probably improve thesefigures. Promising long-term results in selected patientseries have recently been reported. The actuarial 5-yearsurvival in a series from Hannover was almost 80% [60].This series was dominated by patients with carcinoid dis-ease; only 1 out of 12 patients died of tumour recurrence.Similar survival figures for carcinoid patients were recent-
ly reported in a French multicentre study of 31 patients.In this series the 5-year survival was considerably worsefor patients with EPT (!10%) (fig. 2) [61]. In both theGerman and French series there were several patientswith correct tumour diagnoses first after transplantation,which was performed on suspicion of hepatocellular can-cer. These patients underwent resection of the primaryNE tumour at a second operation. For cluster proceduresthe prognosis for NE tumours widely surpassed othertumour diagnoses, e.g. sarcoma, hepatocellular carcinomaor cholangiocarcinoma, and reached a 5-year survivalabove 60% [62]. Thus, available studies indicate thatpatients with metastatic NE tumours confined to the livercan be offered long periods of symptom palliation by livertransplantation. In individual cases, transplantation mayeven offer cure.
Acknowledgements
This work was supported by grants from the Swedish MRC(5220) and the Swedish Cancer Society (3911).
Intervention of Neuroendocrine Tumours Digestion 2000;62(suppl 1):59–68 67
References
1 Williams E, Sandler M: The classification ofcarcinoid tumours. Lancet 1963;i:238.
2 Capella C, Heitz P, Höfler H, Solcia E, KlöppelG: Revised classification of neuroendocrine tu-mors of the lung, pancreas and gut. Digestion1994;55:11–23.
3 Rindi G, Azzoni C, La Rosa S, Klersy S, Pao-lotti D, Rappel S, Stolte M, Capella C, Bordi C,Solcia E: ECL cell tumor and poorly differen-tiated endocrine carcinoma of the stomach:Prognostic evaluation by pathological analysis.Gastroenterology 1999;116:532–542.
4 Ahlman H, Åhlund L, Dahlström A, Martner J,Stenqvist O, Tylén U: The use of SMS 201-995and provocation tests in carcinoid patients inpreparation for surgery and hepatic arterial em-bolisation. Anesth Analg 1988;67:1142–1148.
5 Ahlman H, Wängberg B, Nilsson O, GrimeliusL, Granérus G, Modlin IM, Stenqvist O,Scherstén T: Aspects of diagnosis and treat-ment of the foregut carcinoid syndrome. ScandJ Gastroenterol 1992;27:459–471.
6 Moertel CG: An odyssey in the land of smallintestinal tumors. J Clin Oncol 1987;5:1502–1522.
7 Rothmund M, Kisker O: Surgical treatment ofcarcinoid tumours of the small bowel, ap-pendix, colon and rectum. Digestion 1994;55(suppl 3):86–91.
8 Norton JA: Surgical management of carcinoidtumors: Role of debulking and surgery for pa-tients with advanced disease. Digestion 1994;55(suppl 3):98–103.
11 Tisell LE, Ahlman H, Jansson S, Grimelius L:Total pancreatectomy in the MEN-1 syn-drome. Br J Surg 1988;75:154–157.
12 Benjamin IS: Management of secondary endo-crine tumours of the liver; in Lynn J, Bloom SR(eds): Surgical Endocrinology. Oxford, Butter-worth-Heinemann, 1993, pp 538–547.
13 Farges O, Belghiti J: Options in the resection ofendocrine liver metastases; in Mignon M, Co-lombel JF (eds): Recent Advances in the Patho-physiology and Management of InflammatoryBowel Diseases and Digestive Endocrine Tu-mours. Paris, Libbey Eurotext, 1999, pp 335–337.
24 Markowitz JC: The hepatic artery. Surg Gyne-col Obstet 1952;95:644–646.
25 Gelin LE, Lewis D, Nilsson L: Liver blood flowin man during abdominal surgery. II. The effectof hepatic artery occlusion on the blood flowthrough metastatic tumor nodules. Acta Hepa-tosplenol 1968;15:21–24.
26 Cho KJ, Reuter SR, Schmidt R: Effects ofexperimental hepatic artery embolization onhepatic function. Am J Roentgenol 1976;127:563–567.
27 Geterud K, Tylén U, Jansson S, Stenqvist O,Tisell LE, Ahlman H: Hepatic arterial emboli-zation in the treatment of the midgut carcinoidsyndrome and other advanced endocrine tu-mours metastatic to the liver. J Intervent Ra-diol 1990;5:69–76.
28 Almersjö O, Bengmark S, Engevik L, HafströmLO, Nilsson LA: Hepatic artery ligation as pre-treatment for liver resection of metastatic can-cer. Rev Surg 1966;23:377–380.
29 Chuang VP, Wallace S: Hepatic artery emboli-zation in the treatment of hepatic neoplasms.Radiology 1981;140:51–58.
30 Ajani JA, Carrasco CH, Wallace S: Neuroendo-crine tumors metastatic to the liver vascularocclusion therapy. Ann NY Acad Sci 1994;733:479–487.
31 Allison DJ, Modlin IM, Jenkins WJ: Treat-ment of carcinoid liver metastases by hepaticartery embolization. Lancet 1977;ii:1323–1325.
32 Pueyo I, Jimenez JR, Hernandez J, BrugarolasA, Garcia-Moran M, Garcia-Muniz JI, ArroyoF: Carcinoid syndrome treated by hepatic em-bolization. Am J Roentgenol 1978;131:511–513.
33 Lunderquist A, Ericsson M, Nobin A, SandinG: Gelfoam powder embolization of the hepat-ic artery in liver metastases of carcinoid tumor.Radiologe 1982;22:65–70.
37 Perry LJ, Stuart K, Stokes KR, Clouse ME:Hepatic arterial chemoembolization for meta-static neuroendocrine tumours. Surgery 1994;116:1111–1116.
38 Ruszniewski P, Rougier P, Roche A, LegmannP, Sibert A, Hochlaf S, Ychou M, Mignon M:Hepatic arterial chemoembolisation in patientswith liver metastases of endocrine tumors.Cancer 1993;71:2624–2630.
39 Nobin A, Månsson H, Lunderquist A: Evalua-tion of temporary liver dearterialization andembolization in patients with metastatic carci-noid tumor. Acta Oncol 1989;28:419–424.
40 Wängberg B, Geterud K, Nilsson O, Jansson S,Dahlström A, Tylén U, Ahlman H: Embolisa-tion therapy in the midgut carcinoid syndrome– Just tumour ischemia? Acta Oncol 1993;32:251–256.
41 Wängberg B, Ahlman H, Tylén U, Nilsson O,Hermodsson S, Hellstrand K: Accumulation ofnatural killer cells after hepatic artery emboli-sation in the midgut carcinoid syndrome. Br JCancer 1995;71:617–618.
42 Coupe MO, Hodgson HJF, Hemingway A, Al-lison DJ: The effect of hepatic artery emboliza-tion on survival in the carcinoid syndrome. JIntervent Radiol 1989;4:179.
43 Mitty HA, Warner RRP, Neuman LH, TrainJS, Parnes IH: Control of carcinoid syndromewith hepatic artery embolization. Radiology1985;155:1623–1626.
44 Marlink RG, Lokich T, Robins SR, Clouse ME:Hepatic arterial embolization for metastatichormone-secreting tumors: Technique, effec-tiveness and complications. Cancer 1990;65:2227–2232.
45 Hanssen LE, Schrumpf E, Kolbenstvedt AN,Tausjö J, Dolva LO: Treatment of malignantmetastatic midgut carcinoid tumours with re-combinant human ·-2b-interferon with orwithout prior hepatic artery embolization.Scand J Gastroenterol 1989;24:787–795.
46 Wängberg B, Forssell-Aronsson E, Tisell LE,Nilsson O, Fjälling M, Ahlman H: Intraopera-tive detection of somatostatin-receptor-posi-tive neuroendocrine tumours using indium-III-labelled-DTPA-D-Phe1-octreotide. Br J Cancer1996;73:770–775.
47 Scherstén T, Ahlman H, Wängberg B, Grané-rus G, Grimelius L: Hyperthermic liver perfu-sion chemotherapy in the treatment of the fore-gut carcinoid syndrome. Lancet 1991;338:568–569.
48 Kölby L, Wängberg B, Ahlman H, Jansson S,Forssell-Aronsson E, Erickson JD, Nilsson O:Gastric carcinoid with histamine production,histamine transporter and expression of soma-tostatin receptors. Digestion 1998;59:160–166.
49 Charnley RM, Doran J, Morris DL: Cryothera-py for liver metastases; a new approach. Br JSurg 1989;76:1040–1041.
50 Dowlatshahi K, Bhattacharya AK, Silver B,Motalen T, Williams JW: Percutaneous inter-stitial laser therapy of a patient with recurrenthepatoma in a transplanted liver. Surgery1992;112:603–606.
51 Bilchik AJ, Rose DM, Allegra DP, Bostick PJ,Hsueh E, Morton DL: Radio-frequency abla-tion: A minimally invasive technique with mul-tiple applications. Cancer J Sci Am 1999;6:356–361.
52 Matsui Y, Nakagawa A, Kamiyama Y, Yama-moto K, Kubo N, Nakase Y: Selective thermo-coagulation of unresectable pancreatic cancersby using radiofrequency capacitive heating.Pankreas 2000;1:14–20.
53 Kettenbach J, Silverman SG, Hata N, KurodaK, Saiviroonpurn P, Zientara GP, MorrisonPR, Hushek SG, Black PM, Kikinis R, JoleszFA: Monitoring and visualization techniquesfor MR-guided laser ablations in an open MRsystem. J Magn Reson Imaging 1998;8:933–943.
54 Pichlmayr R: Is there a place for liver graftingfor malignancy? Transplant Proc 1988;20:478–482.
55 Johanson V, Tisell LE, Olbe L, Wängberg B,Nilsson O, Ahlman H: Comparison of survivalbetween malignant neuroendocrine tumours ofmidgut and pancreatic origin. Br J Cancer1999;80:1259–1261.
56 Frilling A, Rogiers X, Knöfel WT, Broelsch CE:Liver transplantation for metastatic carcinoidtumours. Digestion 1994;55(suppl 3):104–106.
57 Makowka L, Tzakis AG, Mazzaferro V, Teper-man L, Demetris AJ, Iwatsuki S, Starzl TE:Transplantation of the liver for metastatic en-docrine tumours of the intestine and pancreas.Surg Gynecol Obstet 1989;168:107–111.
58 Gulanikar AC, Kotylak G, Bitter-Suermann H:Does immunosuppression alter the growth ofmetastatic liver carcinoid after orthotopic livertransplantation? Transplant Proc 1991;23:2197–2198.
59 Bechstein W, Neuhaus P: Liver transplantationfor hepatic metastases of neuroendocrine tu-mours. Ann NY Acad Sci 1994;733:507–514.
60 Lang H, Oldhafer KJ, Weimann A, Schlitt HJ,Scheumann GFW, Flemming P, Ringe B,Pichlmayr R: Liver transplantation for meta-static neuroendocrine tumors. Ann Surg 1997;225:347–354.
61 Le Treut YP, Delpero JR, Dousset B, CherquiD, Segol P, Mantion G, Hannoun L, Benha-mou G, Launois B, Boillot O, Domergue J, Bis-muth H: Results of liver transplantation in thetreatment of metastatic tumors: A 31-caseFrench multicentric report. Ann Surg 1997;225:355–364.
62 Allessiani M, Tzakis A, Todo S, Demetris AJ,Fung JJ, Starzl TE:. Assessment of 5-year expe-rience with abdominal cluster transplantation.J Am Coll Surg 1995;180:1–9.




















![[Tumours of testis]](https://static.documents.pub/doc/80x56/635022e42630aed50008c845/tumours-of-testis.jpg)




