P214 Un unexplained syncope: usefulness of right parasternal approach Comunello A.; Rossi A.; Ribichini FL. University of Verona, AOUI VR, Verona, Italy An 87-year-old male patient was referred to our ER in March 2017 after a brief syncopal episode at home (witnessed by patient’s son) while sitting, in the absence of prodromes and associated with a short sphincter release, without consequent trauma. Medical history was: hyper- tensive heart disease, previous TIA, chronic vascular encephalopathy. Home therapy was: Aspirin 100 mg/day, Dutasteride 0.5 mg/day, Lan- soprazole 15 mg/day. At the physical examination in the ER patient was totally asymptomatic, haemodynamically stable (GCS was 15). At the cardiac auscultation a high grade systolic aortic murmur was detected. The remaining physical examination was negative: no peripheral edema, no jugular distension, normal peripheral pulses. The ECG at admission was: sinus tachycardia with 1st degree AV block and left anterior hemiblock. Troponin I was repeatedly negative. The chest X-ray showed a mild increased cardiac shadow. The brain CT was nega- tive for focal lesions and intracranial hemorrhage. Given the persistent and unexplained sinus tachycardia at the ECG monitoring (mean HR 130-140 bpm) associated with the relevant systolic murmur, a cardiac evaluation and an echocardiogram were requested. The prevalent di- agnostic hypothesis was a severe aortic stenosis as responsible for the syncope. The left parasternal and the apical approach were charac- terized by a very poor technical quality, however the subcostal approach showed a mild global systolic dysfunction of the left hypertrophic ventricle and a mild circumferential pericardial effusion. Because of the poor acoustic window of the left parasternal approach, which couldn’t allow a good examination of the aorta, a right parasternal approach (in this case of good technical quality) was performed. This revealed the presence of an ascending dilated aorta (55 mm) with associated circumferential mobile intimal dissection flap extended through all the visible ascending aorta. A subsequent thoracic-abdominal CT scan confirmed the presence of a dilated ascending aorta with a type A aortic dissec- tion, starting from the valvular plane up to the renal arteries. In this patient aortic dissection manifested without the characteristical clinical features, with syncope as the only symptom. The right parasternal approach allowed the correct diagnosis in this patient and, therefore, it should be performed in selected cases whenever the classical transthoracic approaches are impracticable to guide diagnosis and manage- ment. Abstract P214 Figure. Right parasternal approach Abstracts -- Poster Session -- Clinical case poster session 1 Downloaded from https://academic.oup.com/ehjcimaging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
Transcript
P214
Un unexplained syncope: usefulness of right parasternal approachComunello A.; Rossi A.; Ribichini FL.
University of Verona, AOUI VR, Verona, Italy
An 87-year-old male patient was referred to our ER in March 2017 after a brief syncopal episode at home (witnessed by patient’s son) whilesitting, in the absence of prodromes and associated with a short sphincter release, without consequent trauma. Medical history was: hyper-tensive heart disease, previous TIA, chronic vascular encephalopathy. Home therapy was: Aspirin 100 mg/day, Dutasteride 0.5 mg/day, Lan-soprazole 15 mg/day. At the physical examination in the ER patient was totally asymptomatic, haemodynamically stable (GCS was 15). Atthe cardiac auscultation a high grade systolic aortic murmur was detected. The remaining physical examination was negative: no peripheraledema, no jugular distension, normal peripheral pulses. The ECG at admission was: sinus tachycardia with 1st degree AV block and leftanterior hemiblock. Troponin I was repeatedly negative. The chest X-ray showed a mild increased cardiac shadow. The brain CT was nega-tive for focal lesions and intracranial hemorrhage. Given the persistent and unexplained sinus tachycardia at the ECG monitoring (mean HR130-140 bpm) associated with the relevant systolic murmur, a cardiac evaluation and an echocardiogram were requested. The prevalent di-agnostic hypothesis was a severe aortic stenosis as responsible for the syncope. The left parasternal and the apical approach were charac-terized by a very poor technical quality, however the subcostal approach showed a mild global systolic dysfunction of the left hypertrophicventricle and a mild circumferential pericardial effusion. Because of the poor acoustic window of the left parasternal approach, which couldn’tallow a good examination of the aorta, a right parasternal approach (in this case of good technical quality) was performed. This revealed thepresence of an ascending dilated aorta (55 mm) with associated circumferential mobile intimal dissection flap extended through all the visibleascending aorta. A subsequent thoracic-abdominal CT scan confirmed the presence of a dilated ascending aorta with a type A aortic dissec-tion, starting from the valvular plane up to the renal arteries. In this patient aortic dissection manifested without the characteristical clinicalfeatures, with syncope as the only symptom. The right parasternal approach allowed the correct diagnosis in this patient and, therefore, itshould be performed in selected cases whenever the classical transthoracic approaches are impracticable to guide diagnosis and manage-ment.
Abstract P214 Figure. Right parasternal approach
Abstracts -- Poster Session -- Clinical case poster session 1
Dow
nloaded from https://academ
ic.oup.com/ehjcim
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P215
Successful management of myocardial infarction complicated with ventricular septalrupture and cardiogenic shock
1Medical Research Institute, Alexandria University, Cardiology and Angiology Unit, Clinical and Experimental Internal Medicine Department,Alexandria, Egypt2Alexandria University, Department of Cardiology, Alexandria, Egypt
Introduction: Ventricular septal rupture (VSR) is a complication seen in approximately 0.2-0.4% of acute myocardial infarction (AMI) cases.While the incidence of this complication has reduced significantly at the percutaneous coronary intervention (PCI) era, the mortality remainsquite high. VSR often results in cardiogenic shock, right ventricular dysfunction and requires immediate surgical repair.
case presentation: we hereby report a case of 60-year-old female patient with past medical history of type II diabetes mellitus and hyper-tension presented with acute left-sided weakness and aphasia. She was diagnosed as acute cerebrovascular stroke and referred to a speci-alized neuropsychiatry hospital. On clinical examination, she was hemodynamically stable with a loud pansystolic murmur heard over the leftlower sternal border. ECG showed deep Q waves at anterior chest leads. TTE showed reduced left ventricular systolic function with apicalcap akinesia, anterior and anteroseptal wall akinesia with an accidentally discovered small restrictive VSR located at the apicoseptal seg-ment measuring 0.6 cm. Coronary angiography revealed multi-vessel coronary artery disease (CAD). She underwent coronary artery bypassgrafting (CABG) with VSR repair using a Dacron patch. The patient recovered and discharged safely.
Conclusion: VSR after AMI is exceedingly rare in the PCI era but mortality rates remain high. VSR is associated with cardiogenic shock andright-sided heart failure and it is more likely to occur in patients who are elderly, females, hypertensives and non-smokers. It occurs in thesetting of the first myocardial infarction (MI) with delayed or absent reperfusion. The defect occurs at the myocardial infarct border zone,located in the apical septum in the anterior MI and in the basal inferior septum with inferior MI. A high index of clinical suspicion with promptdiagnosis by a multidisciplinary approach using different imaging modalities is required. Definitive repair, though challenging and associatedwith high surgical mortality, remains the treatment of choice. Alternatively, delaying surgery in stable patients may provide better results. Pro-longed medical management is usually futile, but includes afterload reduction and intra-aortic balloon pump placement. Using full mechani-cal support to delay surgery is an attractive option, but data on success is limited to case reports. Finally, percutaneous VSR closure may beused as a temporizing measure to reduce shunt, or for patients in the sub-acute to chronic period whose comorbidities preclude surgicalrepair.
1Medical Research Institute, Alexandria University, Cardiology and Angiology Unit, Clinical and Experimental Internal Medicine Department,Alexandria, Egypt2Alexandria University, Department of Cardiology, Alexandria, Egypt
Intro
Giant right atrial aneurysm is an extremely rare cardiac condition that can be seen anytime in human life from childhood to elderly.
Many cases have no symptoms, others may develop arrhythmias such as atrial fibrillation, and sometimes thrombi may develop inside theright atrium with risk of pulmonary embolism as well as paradoxical embolism through a patent foramen ovale.
This condition can be caused by causes of cor-pulmonale, right ventricular disease, tricuspid valve diseases and -in extremely rare cases- ifall these causes are excluded, it is considered idiopathic.
Body Page
A 62-year-old-male patient was referred for a pre-operative echocardiography before cataract surgery. He had a history of hypertension andchronic atrial fibrillation for which he was receiving digoxin and warfarin and he was totally asymptomatic.
Transthoracic echocardiography revealed a giant right atrial aneurysm that measures 160X140 mm in its dimensions with an estimated vol-ume of 1450 ml, the giant right atrium was compressing the left atrium, left ventricle and the right pulmonary artery. The left ventricular systol-ic function was normal, the tricuspid valve was normal in morphology, the pulmonary valve and pulmonary artery were also normal in struc-ture and dimensions.
Further multi-slice computed tomography (MSCT) confirmed the diagnosis.
As the patient was asymptomatic, the decision was to continue rate control of the atrial fibrillation and proper anti-coagulation.
Conclusion: Giant right atrial aneurysms are very rarely diagnosed, they may be asymptomatic or may present by arrhythmias.
Echocardiography is the main tool for the diagnosis and detection of the etiology of this condition.
Management usually depends on the patients’ symptoms as well as their clinical condition and it varies from conservative management tosurgical resection.
1Aswan Heart Centre, Adult Cardiology Department, Aswan, Egypt2Ain Shams University, Radiology department, Cairo, Egypt3Aswan Heart Centre, Aswan, Egypt
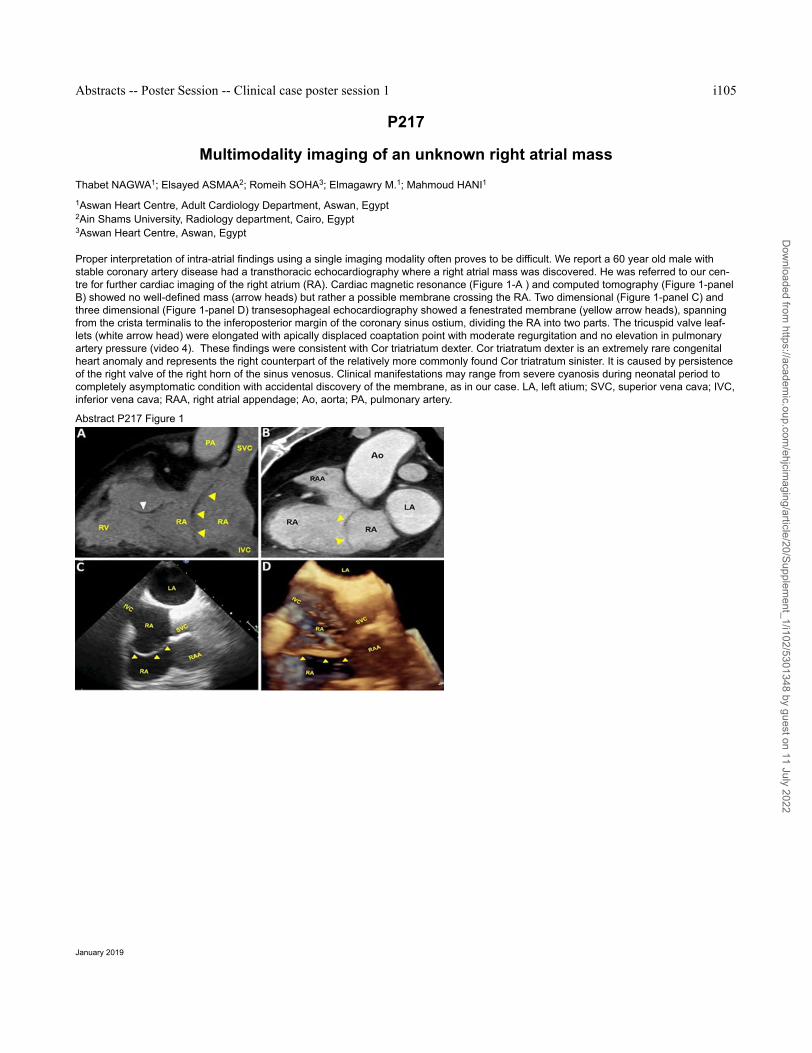
Proper interpretation of intra-atrial findings using a single imaging modality often proves to be difficult. We report a 60 year old male withstable coronary artery disease had a transthoracic echocardiography where a right atrial mass was discovered. He was referred to our cen-tre for further cardiac imaging of the right atrium (RA). Cardiac magnetic resonance (Figure 1-A ) and computed tomography (Figure 1-panelB) showed no well-defined mass (arrow heads) but rather a possible membrane crossing the RA. Two dimensional (Figure 1-panel C) andthree dimensional (Figure 1-panel D) transesophageal echocardiography showed a fenestrated membrane (yellow arrow heads), spanningfrom the crista terminalis to the inferoposterior margin of the coronary sinus ostium, dividing the RA into two parts. The tricuspid valve leaf-lets (white arrow head) were elongated with apically displaced coaptation point with moderate regurgitation and no elevation in pulmonaryartery pressure (video 4). These findings were consistent with Cor triatriatum dexter. Cor triatratum dexter is an extremely rare congenitalheart anomaly and represents the right counterpart of the relatively more commonly found Cor triatratum sinister. It is caused by persistenceof the right valve of the right horn of the sinus venosus. Clinical manifestations may range from severe cyanosis during neonatal period tocompletely asymptomatic condition with accidental discovery of the membrane, as in our case. LA, left atium; SVC, superior vena cava; IVC,inferior vena cava; RAA, right atrial appendage; Ao, aorta; PA, pulmonary artery.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P218
Large left ventricular non-infectious vegetation in patient with eosinophilic granuloma-tosis with polyangiitis
Seol SH.; Song YJ.; Kim S.; Kim DK.; Kim KH.; Kim DI.
Inje University College of Medicine, Haeundae Paik Hospital, Busan, Korea Republic of
Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare form of systemic vasculitis in which cardiac involvement is relatively commonand accounts for half of EGPA-related deaths. The cardiac involvement is more frequent in patients with absence of ANCA and those withhigher eosionophil counts. Clinical manifestations are various include myocarditis, pericarditis, pericardial effusion, heart failure, arrhythmias,valvular insufficiencies, intra-cardiac thrombus formation. The pathology of cardiac involvement in EGPA is usually endomyocardial and peri-cardial eosinophilic infiltration. Considering the potential adverse outcomes associated with cardiac involvement in EGPA, early detection isimportant. A 27-year-old man presented fever, skin rash, both ankle pain with numbness for about 10 days. The patient had a history ofbronchial asthma and chronic rhinitis which had been managed for 2 years. On admission, his body temperature was 38.1˚C, blood pressurewas 120/80mmHg, heart rate was 80/ min, and respiration rate was 20/min. Breath sounds were slightly decreased on the left lower lungfield, heart murmur was not audible. Petechial rash was found on his whole body. The electrocardiography was normal sinus rhythm. A chestradiograph showed cardiomegaly and blunted left costopleural angle. The pleural effusion study revealed neutrophil-predominat exudate, PHwas 7.0, ADA was 25IU/L, Glucose was 51mg/dL, Gram’s and AFB staining were negative. Bacterial and fungal cultures showed no growth.The laboratory test showed mild leukocytosis (9.14 × 109/L) with marked eosinophilia(39.0%). C-reactive protein was 11.5mg/dL, P-ANCAand C-ANCA were negative, parasite specific antibodies were all negative as well. Total IgE level was high at 2154.0 IU/mL. Pro-BNP(3548.0pg/mL), CK-MB(20.9ng/mL) and Troponin-I(2.92ng/mL) were elevated. Blood cultures were all negative. The absence of plate-let-derived growth factor receptor-α and β (PDGRFA, PDGFRB) gene fusion made a diagnosis of idiopathic hypereosinophilic syndrome un-likely. The transthoracic echocardiography showed oscillating mass like lesions at the mid anteroseptal wall of left ventricle (LV) (Figure 1)Coronary angiographic CT revealed normal conorary artery. Nerve conduction study showed decreased sensory nerve action potential am-plitude in both sural nerves. The patient had an operation for resection of the mass lesions in LV. Pathological gross finding showed frag-ments of pinkish gray soft tissue, measuring 3.0 x 1.0 cm. 2.5 x 1.0 cm (Figure 2). Microscopic finding revealed non infective vegetations thatcomposed of thrombus, granulation tissues, eosinophils, lymphoplasma cells, neutrophils and histiocytes infiltrations (Figure 3). The patientwas discharged and is on oral methylprednisolone treatment at outpatient department.
1University of L"Aquila, L"Aquila, Italy2Sandro Pertini Hospital, Rome, Italy
Cystic echinococcosis is a rare zoonotic parasitic disease which is caused by the larval form of E. Granulosus. The disease is endemic inEuropean, Middle Eastern, South American and African countries [1]. Carnivores represent their definitive hosts, while humans are their in-termediate hosts. E. Granulosus eggs, which are the infectious agents for human beings, may contaminate vegetables and water via thefeces of carnivores.
Clinic case
A 31-year-old woman from Romania presented to our hospital with abdominal pain from three weeks. Her past medical history was unre-markable. Electrocardiogram was normal. At abdominal echography, an 8.7 x 7.3 x 7.2 cm lesion was observed in liver. A total body compu-ted tomography (CT) detected other lesions in heart, lungs and right kidney. An urgent 2D and 3D echocardiography confirmed a very largemulti-lobular echo-density occupying the right ventricle without haemodynamic obstruction. It was located on the right ventricle free wall andhad a rounded shape and thin wall. Further evaluation with chest magnetic resonance imaging displayed a cystic mass (3.9 x 3.4 x 4.6 cm)in the lower-right part of pericardium sac. The patient was treated with Albendazole 400 mg BID. She rejected a radical resection of echino-coccosis cardiac lesion. From the current literature, a prognosis estimation of patients that received alternative non-surgical treatment regi-mens is not possible.[3]
Discussion
Echinococcosis is a chronic disease which is characterized by growing of cysts in various organs, especially in liver and lungs. However,there is a cardiac involvement in less than 2% of cases. [1,2] A first diagnostic hint is provided by patient"s travel, origin and social histo-ry. The variability of cardiac E. signs and symptoms depend on localization and dimension of the cyst. [2] Echocardiography is both highlysensible and specific. Serology can confirm the diagnosis but its specificity and sensitivity are low. The CT resolution is excellent, especiallyin the evaluation of cyst wall calcification. However, the multiplanar and multiparameter imaging facilities and the non-invasiveness of cMRIallow a comprehensive evaluation of the disease.[2] Cardiac echinococcosis cysts should always be surgically removed in symptomatic andasymptomatic patients, since cardiac cysts bear high risk of a spontaneous rupture. From the current known cases, most showed an uncom-plicated course after surgery. [2,3]
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P221
A rare huge ascending aortic aneurysmKandil AA.; Ayaz M.; Salih A.; Aslan A.
Queen Elizabeth Hospital NHS Trust, King"s Lynn, United Kingdom
Introduction: Aortic aneurysm is the second most common in the spectrum of aortic diseases after atherosclerosis. Thoracic aortic aneur-ysms (TAA) are usually silent until acute and often lethal complication occurs.The aetiology of ascending aortic aneurysms is probably multi-factorial. Risk factors include smoking, chronic obstructive pulmonary disease, hypertension, atherosclerosis, male gender, older age, bicus-pid aortic valves, and family history whereas 15% of first-degree relatives of patients with aortic aneurysms have an aneurysm.
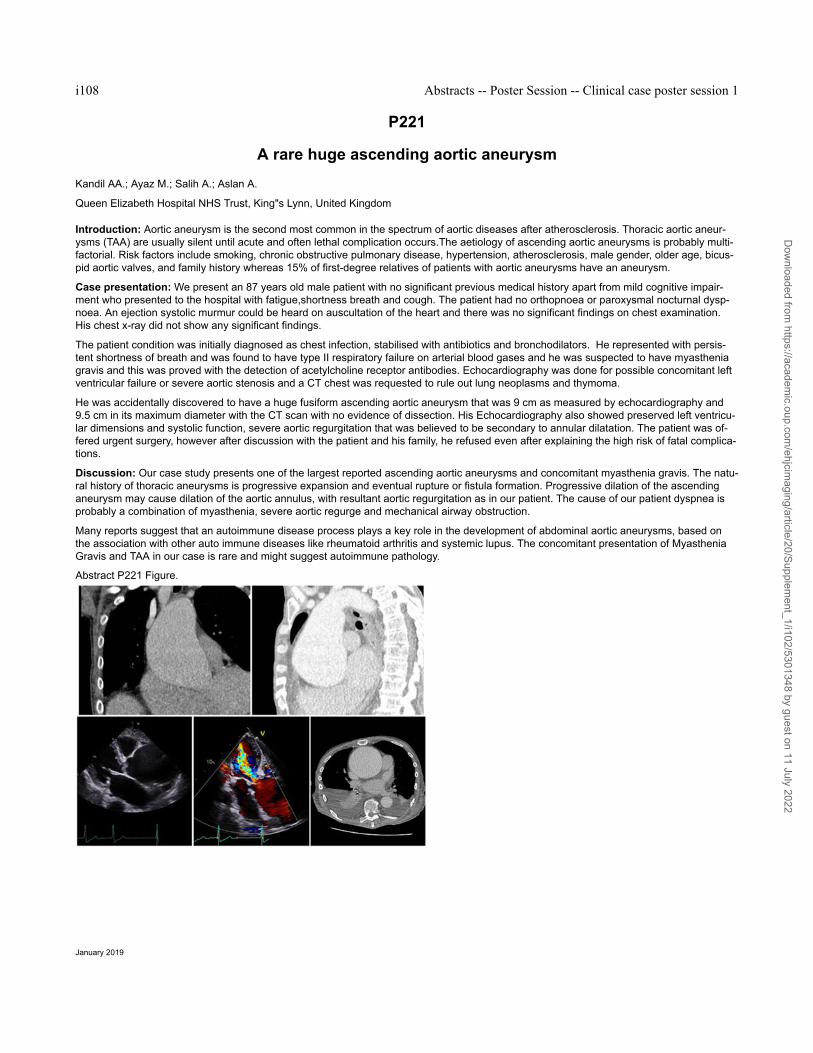
Case presentation: We present an 87 years old male patient with no significant previous medical history apart from mild cognitive impair-ment who presented to the hospital with fatigue,shortness breath and cough. The patient had no orthopnoea or paroxysmal nocturnal dysp-noea. An ejection systolic murmur could be heard on auscultation of the heart and there was no significant findings on chest examination.His chest x-ray did not show any significant findings.
The patient condition was initially diagnosed as chest infection, stabilised with antibiotics and bronchodilators. He represented with persis-tent shortness of breath and was found to have type II respiratory failure on arterial blood gases and he was suspected to have myastheniagravis and this was proved with the detection of acetylcholine receptor antibodies. Echocardiography was done for possible concomitant leftventricular failure or severe aortic stenosis and a CT chest was requested to rule out lung neoplasms and thymoma.
He was accidentally discovered to have a huge fusiform ascending aortic aneurysm that was 9 cm as measured by echocardiography and9.5 cm in its maximum diameter with the CT scan with no evidence of dissection. His Echocardiography also showed preserved left ventricu-lar dimensions and systolic function, severe aortic regurgitation that was believed to be secondary to annular dilatation. The patient was of-fered urgent surgery, however after discussion with the patient and his family, he refused even after explaining the high risk of fatal complica-tions.
Discussion: Our case study presents one of the largest reported ascending aortic aneurysms and concomitant myasthenia gravis. The natu-ral history of thoracic aneurysms is progressive expansion and eventual rupture or fistula formation. Progressive dilation of the ascendinganeurysm may cause dilation of the aortic annulus, with resultant aortic regurgitation as in our patient. The cause of our patient dyspnea isprobably a combination of myasthenia, severe aortic regurge and mechanical airway obstruction.
Many reports suggest that an autoimmune disease process plays a key role in the development of abdominal aortic aneurysms, based onthe association with other auto immune diseases like rheumatoid arthritis and systemic lupus. The concomitant presentation of MyastheniaGravis and TAA in our case is rare and might suggest autoimmune pathology.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P222
A rare case of severe coronary disease
Nunes A.1; Margarida Lebreiro A.1; Lopes R.1; Nascimento H.1; Almeida R.1; Pires Rosa G.2; Pinho T.1; Campelo M.1; Jose Madureira A.3;Pinho P.4; Julia Maciel M.1
1Sao Joao Hospital, Cardiology Service, Porto, Portugal2Sao Joao Hospital, Internal Medicine Service, Porto, Portugal3Sao Joao Hospital, Radiology Service, Porto, Portugal4Sao Joao Hospital, Cardiothoracic Surgery Service, Porto, Portugal
Introduction: Takayaso Arteritis is a rare and chronic granulomatous vasculitis of large vessels with preferential involvement of the aortaand its major branches and tipically affects the female sex. It is a progressive disease with relapses and remissions, with associated sub-stantial morbidity, and often requires long-term immunosuppression.
Clinical Case: A 43-year-old woman with arterial hypertension, granulomatous tenosynovitis and erythema nodosum, started angina andclaudication of the upper limbs. She was admitted to the emergency room for an acute coronary syndrome without ST segment eleva-tion. On physical examination, she had high blood pressure with differential > 10 mmHg in the upper limbs, decreased brachial and radialpulses with anisophigmia and normal cardiopulmonary auscultation. It was performed an electrocardiogram that showed sinusal rythm. Ana-lytically she had raised troponin I, BNP, SR and RCP. Then it was performed a echocardiogram that showed normal left and right ventricularfunction without changes in segmental motility, and mild dilatation of the ascending aorta with mild to moderate aortic regurgitation. Becauseof refractory thoracic pain, it was performed an emergent cardiac catheterization (attempt of access right radial artery without success be-cause it was occluded): 80-90% ostial CT, proximal RC 100%, right subclavian artery occluded after right IMA origin (stenosis at its origin),left subclavian artery occluded at its origin. Four days after, it was performed a coronary artery bypass grafting (SV-AD, SV-PD). To betterunderstand the case, during surgery it was performed an aortic biopsy that showed mild and non-specific changes, and myocardial biopsythat was compatible with ischemic heart disease, without lesions of vasculitis or recoverable inflammatory infiltrate. It was also performeda Angio-MRI that showed diffuse thickening of the aortic wall, supra-aortic trunks and common iliac arteries, with a maximum thickness of 3mm in the ascending and lower abdominal aorta; severe stenosis of the left subclavian artery at 10 mm from its origin and occlusion of thevessel after the origin of the left vertebral artery; distal re-permeability through collaterals; occlusion of the right subclavian artery with distalrepermeabilization. The hospital stay was uneventful. Hospital discharge was at day 10, oriented for Internal Medicine Autoimmune Disea-ses and Cardiology Consultations and for Family Doctor, and it was considered to start steroid therapy.
Conclusion: Our patient meets criteria to establish a diagnosis of Takayaso Arteritis. In order to guarantee good revascularization outcomesit is essential to control disease activity with steroid therapy whitch is first line treatment.
Abstract P222 Figure. Stenosis of the left subclavian artery
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P223
Severe aortic regurgitation of new onset during postoperative aortic dissectionRamirez-Escudero Ugalde G.; Asla Ormaza C.; Codina Prat M.; Mendoza Cuartero P.; Garcia Ibarrondo N.; Bravo Martinez I.; Manzanal ReyA.; Aurrekoetxea Bajeneta G.; Ruiz Gomez L.; Martinez De Bourio R.
Hospital de Basurto, Cardiology, Bilbao, Spain
Aortic dissection (AD) is a disruption of the medial layer provoked by intramural bleeding, resulting in separation of the aortic wall layers andsubsequent formation of a true and a false lumen, with/without communication. Complications are cardiac tamponade, aortic valve regurgita-tion (AR), and proximal/distal bad perfusion syndromes. AR in AD can be originated by dilatation of the aortic root/annulus, tearing of theannulus/valve cusps, downward displacement of one cusp below the line of the valve closure, loss of support of the cusp, and physical inter-ference in the closure of the aortic valve by an intimal flap.
Computed tomography (CT), magnetic resonance (MRI), and transthoracic/transoesophageal echocardiography (TTE/TOE) are equally relia-ble for confirming/excluding the diagnosis of AD. CT and MRI are superior for the assessment of AD extension and branch involvement, aswell as for the diagnosis of intramural haematoma, penetrating aortic ulcer, and traumatic aortic lesions. TOE is superior for imaging flowacross tears and identifying their locations.
We report a case of 62-year-old man who was admitted at hospital because of abrupt chest pain. He had personal history of hypertension,atrial fibrillation, and aortic root enlargement of 45 mm, without other significant findings in TTE. He had no cardiological family history.
At his admission he was sweaty, pale and poorly perfused. Blood pressure: 70/40mmHg. An ECG was performed, observing atrial fibrillationat 50 bpm. An urgent TTE was performed, observing a moderate AR and a suspicious image in the aortic root, suggestive of an intimal flapdue to aortic dissection, without pericardial effusion. The CT confirmed the diagnosis of type A aortic dissection, extended from the aorticroot to external iliac arteries. All the main arteries were originated in the true lumen, without signs of visceral ischemia.
An emergent cardiac surgery was carried out, performing a replacement of the ascending aorta by a supracoronary tube. In the immediatepostoperative TEE there was only a mild AR.
On the third day of stay in the intensive care unit, an abrupt pulmonary oedema came over. A new TTE was performed, observing a newsevere AR. The TEE confirmed the progression of the aortic dissection to the non-coronary cusp as well as to the left main coronary ostium.The patient had to be intervened again, for implantation of a valvulated tube and double aortocoronary bypass grafting.
After that, in the context of great hemodynamic instability, cardiac tamponade was diagnosed, so a third reoperation was necessary. A tearwas observed on the anastomosis from the right coronary artery to the valvulated tube. A 3º aortocoronary graft and a ligature of the rightcoronary ostium were performed.
The patient presented a favorable evolution, so he could be transferred to a hospital ward. However, he disgracefully presented a cardiores-piratory arrest at the 35º day of admission, and finally died.
Abstract P223 Figure. New severe aortic regurgitation
1Institute of Cardiology, Jagiellonian University, John Paul 2 Hospital,Dept.of Cardiovascular Diseas, Krakow, Poland2Center of Diagnosis,Prevention and Telemedicine, John Paul 2 Hospital, Krakow, Poland
Background: Hypoplasia of the thoracic and abdominal aorta is an extremly rare cardiovascular anomaly. Congenital or acquired (inflam-matory/infectious) etiology has been implicated. Symptoms occur within the first three decades of life. Chief complaints are hypertension(upper extremities), lower extremity claudication, and mesenteric ischemia. Surgical bypass grafting is considered the optimal method oftreatment. Aortic hypoplasia has been described in all portions of the thoracic and abdominal aorta. Aortic hypoplasia is frequently associ-ated with narrowing or hypoplasia of renal arteries (33–81%) and less frequently of celiac trunk (CT, 9%), superior mesenteric artery (SMA,4%) and inferior mesenteric arteries (IMA, 1.3%).
Case report: A 35-year- old woman with congenital hypoplastic thoracic and abdominal aorta (treated surgically) and asymptomatic criticalceliac trunk stenosis, was admitted to our department for cardiovascular evaluation in the 27th week of her first pregnancy. Her past medicalhistory was positive for hypertension, first noted during childhood, and for Reclinghausen disease. At the age of 27 years she underwent asurgical repair with thoracic to abdominal aorta bypass, and then blood pressure was normalized. On admission physical examination re-vealed no hypertension or cyanosis, BMI 22.4 kg/m2, BP 110/70 mmHg, HR 75 bpm. She didn’t complain about chest or abdominal pain, nointestinal angina. An electrocardiogram showed a sinus rhythm with a heart rate of 75 bpm. ABPM was in normal limit, with mean BP 118/65mmHg during a day and 99/53 mmHg at night. Transthoracic echocardiography showed normal cardiac chamber dimensions, preservedbiventricular systolic function, no evidence of thrombus, and no signs of pulmonary hypertension. No abnormality was detected in the as-cending aorta, aortic arch, or supracervical branches.
A 24-hour ECG Holter monitoring showed a sinus rhythm, mean 84 bpm, max.118 bpm and min.68 bpm, supraventricular premature beats13, ventricular premature beats 8. The condition of the fetus, assessed by gynecological examination with fetal ultrasonography was normal.The course of pregnancy was uneventful, she was monitored systematically by the cardiologist, obstetrician and angiologist. In the 37thweek a cesarean section in epidural anaesthesia was performed and a healthy baby girl, 2700g/52 cm was delivered. APGAR was 10 at 1and at 5 min. There were no congenital heart diseases or other congenital defects in newborn. One year after delivery the patient and herbaby remained asymptomatic. Control echocardiography was performed and showed no deterioration of cardiac function; MRI revealed agood function of the aortic graft. Conclusion: In a patient after surgical correction of the thoracic and abdominal aorta hypoplasia pregnancywas uncomplicated with an excellent maternal and fetal outcome.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P225
"Troponinitis" - a rare phenomenon to take into account after inconclusive multi-mo-dality imaging
Graca Santos L.; Ribeiro Carvalho R.; Ruivo C.; Montenegro Sa F.; Saraiva F.; Soares F.; Guardado J.; Correia J.; Pernencar S.; Morais J.
Hospital Santo Andre, Cardiology, Leiria, Portugal
Heterophile antibodies (HAb), present in 0.1-3% of the general population, can usually develop after a viral infection and exhibit weak multi-specific activity against poorly defined antigens. They represent a rare yet possible source of false positives in troponin tests, binding notspecifically to the Fc portions of the assay antibodies.
We present the case of a 57-year-old woman brought to the Emergency Room complaining of a recent episode of prolonged chest painradiating to the left upper limb, absent on admission. She reported personal history of fibromyalgia and hypothyroidism under levothyroxine,denying other toxicological habits. On admission, she was conscious and oriented, afebrile, and eupneic without supplemental oxygen.She presented with hypertension (167/54mmHg) but heart rate was normal and no changes in cardiopulmonar auscultation or signs of pe-ripheral congestion were evident. The electrocardiogram (ECG) revealed sinus rhythm with ST depression and V1-4 biphasic T wave. Bloodtests showed C-reactive protein 35.4mg/L (N <5.0), creatine kinase 380U/L (10-145) and troponin (Tn) I 6.29ng/mL (<0.04), with no otherchanges. The diagnosis of non-ST elevation myocardial infarction (NSTEMI) was assumed. However, coronary angiogram did not reveal epi-cardial coronary disease. Transthoracic echocardiography (TTE) showed preserved biventricular systolic function with normal segmental wallmotion and no other changes. She remained asymptomatic, with normalization of the ST-T changes and decrease of myocardial necrosisbiomarkers, and was discharged with the presumptive diagnosis of acute myocarditis, awaiting the completion of cardiac magnetic reso-nance imaging (CMR).
A month later, she returns complaining of another chest pain episode associated with no relevant changes on the ECG. Isolated Tn I eleva-tion (10.46ng/mL) was present and remained despite serial normal ECG, and absence of changes on both TTE and CMR (Figure 1). Afterconsulting her history on the national health data platform, we found a hospital admission in 2011, not reported by the patient, due to NSTE-MI with normal coronary arteries and persistence of elevated Tn I after discharge. Given this discovery, we considered the possibility of false-ly elevated serum Tn results from the routine assay used in our hospital. Normal values were determined using a point-of-care Tn I assay. Asample was sent to the laboratory of the supplier and it was treated with a reagent containing interference blocking proteins, concluding forthe presence of HAb causing abnormally high TnI values.
The present case draws attention to the association between circulating serum HAb and the possibility of Tn false positives by the immuno-assays commonly used. Although it is a rare phenomenon with about 40 cases reported, the cardiologist must be aware of it, specially whendiagnostic investigation is inconclusive, in order to avoid false diagnosis, iatrogeny, absenteeism and increased costs.
Abstract P225 Figure. Normal cardiac imaging evaluation
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P226
The lethal hug: a giant but barely symptomatic mediastinal mass encircling the heartCannata F.; Pellegrino M.; Lavanco V.; Fazzari F.; Curzi M.; Bragato RM.; Monti L.
Clinical Institute Humanitas IRCCS, Cardio Center, Rozzano, Italy
Synovial sarcomas are rare malignant tumours of mesenchymal origin, with a histologic resemblance to synovial cells. The most commonpresentation is a soft tissue tumour of the extremities in young adults. Synovial sarcomas tend to grow slowly, are associated with a high riskof late metastases and are the more-chemotherapy sensitive subtype. The diagnosis is often late due to the painless nature of the tumourand the symptoms, when present, usually suggest a neurovascular compromise. A multimodality imaging is essential in the diagnostic andprognostic assessment, both assisting in the biopsy plan and execution and defining the extent of the primary tumour and the presence ofmetastatic disease. Even the treatment usually requires a multimodality approach, combining surgery, radiotherapy and chemotherapy andindividualizing the therapeutic protocol.
Hereby, we present the case and the unbelievable images of a 39-year-old man whose dyspnoea on moderate exertion turned out to be theisolate symptom of a giant mediastinal synovial sarcoma encircling the heart (length 14 cm, width 10 cm and height 13 cm). This mass andits complex relationships within the mediastinum were evaluated with chest computerized tomography, cardiac magnetic resonance andtrans-thoracic echocardiography. This sarcoma infiltrated the antero-lateral wall of the right atrium and the right anonymous vein, com-pressed the right ventricle, the superior vena cava and the right pulmonary veins and encircled the ascending thoracic aorta. Every imagingtechnique added some useful information resulting necessary for a correct all-comprehensive evaluation of the tumour: the computerizedtomography provided us detailed information regarding the size, the tissue characteristics and the relationships with the lungs, the trans-thoracic echocardiography permitted us to focus on the effects on cardiac function in an easily reproducible way and the cardiac gated mag-netic resonance helped us to distinguish vessel compression versus vessel invasion.
The patient underwent a computerized tomography guided needle biopsy which revealed a biphasic synovial sarcoma. The treatment strat-egy began with chemotherapy (Adriamycin and Ifosfamide) followed by high-dose radiotherapy and then a wide local surgical resection. Thepatient is alive after almost one year since the diagnosis and is now beginning a new cycle of radiation therapy.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P227
A hybrid approach to a giant left atrial massCardoso Torres S.; Vasconcelos M.; Dias P.; Sousa C.; Almeida PB.; Araujo P.; Silva JC.; Sousa AR.; Macedo F.; Maciel MJ.
Sao Joao Hospital, Porto, Portugal
Introduction: Primary cardiac tumors are an extremely rare entity with a wide variety of clinical presentations. The vast majority are benigntumors.
Case report: We report a case of a 51-year-old woman with light smoking habits who presented with complaints of occasional palpitations.As requested by her family doctor, she underwent an electrocardiogram that showed sinus rhythm with right bundle branch block and leftanterior hemiblock, and a transthoracic echocardiogram which revealed the presence of a large (78x70mm) mass in the left atrium, whichwas severely dilated. The mass was apparently attached to the interatrial septum and protruded trough the mitral valve causing severe flowobstruction. A giant atrial myxoma was suspected. Based on this finding, she was referred to our tertiary care center for surgical excision ofthe mass.
For better characterization of the mass we performed a transesophageal echocardiography, which revealed a heterogeneous vacuolizedmass with regular contours adherent to the fossa ovalis region, corroborating the diagnosis of atrial myxoma.
As part of her preoperative assessment, the patient underwent a coronary angiography which showed a richly vascularized atrial mass main-ly supplied by a right coronary branch and, to a lesser extent, by a circumflex artery branch. There was no obstructive coronary artery dis-ease.
For further elucidation of the tumor characteristics a cardiac MRI was conducted, which showed features and a contrast enhancement pat-tern compatible with the diagnosis of cardiac myxoma.
After a Heart Team discussion involving interventional and clinical cardiologists and cardiac surgeons, it was decided to perform a preopera-tive polyvinyl alcohol embolization of the tumor main afferent artery (a branch of the right coronary artery), which occurred without complica-tions. The main goal was to minimize the risk of excessive surgical blood loss. In the next day she was submitted to surgical resection of themass, followed by interatrial septum and left atrium base reconstruction with a bovine pericardial patch. The postoperative period was un-eventful, and she was discharged 5 days later.
The anatomopathological examination of the resected tissue confirmed the diagnosis of cardiac myxoma.
Conclusion: Although benign in the majority of cases, cardiac tumors frequently represent a challenge to cardiac surgeons due to their loca-tion and size. This case illustrates the importance of multimodality cardiac imaging for the characterization of cardiac tumors and also showsthe benefits of a hybrid approach, with percutaneous and surgical techniques combined, to provide a safer and successful surgical resectionof cardiac masses, even in the case of benign entities such as myxomas.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P228
Malignant lymphoma, pulmonary arteriovenous malformation: uncommon diseaseswith common presentation
Khalifa EA.; Abushahba G.; Ghareep AN.; Helmy S.; Alkuwari M.
Hamad Medical Corporation Heart Hospital, cardiology, Doha, Qatar
Cardiac involvement of a malignant lymphoma is usually a late manifestation of the disease. Therefore, heart failure as the initial presenta-tion of the disease is extremely rare. We present a case of malignant lymphoma with diffuse cardiac involvement whose first presentationwas congestive heart failure with an incidental finding of pulmonary arteriovenous malformation that worsened due to cardiac decompensa-tion.
Case report: A 29- years old male patient with no past medical history, was admitted with dyspnea of 1-month duration, orthopnea, intermit-tent fever, night sweating and weight loss. Oxygen saturation was 85 % on room air with peripheral cyanosis. Peripheral lymphadenopathyand hepatosplenomegaly were absent.
Echocardiogram showed diffuse symmetrical biventricular myocardial hypertrophy with sever systolic dysfunction and grade III diastolic dys-function. There was diffuse thickening of aortic and pulmonary arteries walls. Also, marked thickening of involved right ventricular outflowtract (RVOT) causing significant narrowing and obstruction was noted. The patient was hypoxemic with peripheral cyanosis. Agitated salinewas performed to exclude any shunt which resulted in opacification of the left atrium (LA) through the upper right pulmonary vein after > 6beats, which indicated extra cardiac shunt.
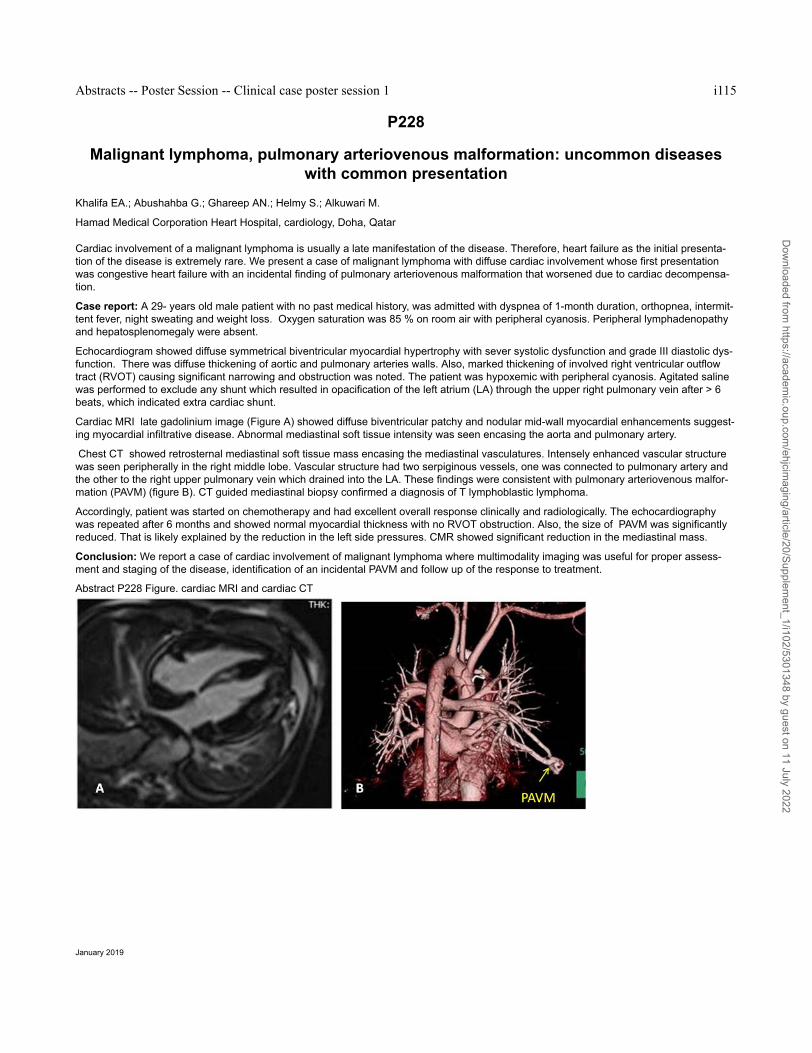
Cardiac MRI late gadolinium image (Figure A) showed diffuse biventricular patchy and nodular mid-wall myocardial enhancements suggest-ing myocardial infiltrative disease. Abnormal mediastinal soft tissue intensity was seen encasing the aorta and pulmonary artery.
Chest CT showed retrosternal mediastinal soft tissue mass encasing the mediastinal vasculatures. Intensely enhanced vascular structurewas seen peripherally in the right middle lobe. Vascular structure had two serpiginous vessels, one was connected to pulmonary artery andthe other to the right upper pulmonary vein which drained into the LA. These findings were consistent with pulmonary arteriovenous malfor-mation (PAVM) (figure B). CT guided mediastinal biopsy confirmed a diagnosis of T lymphoblastic lymphoma.
Accordingly, patient was started on chemotherapy and had excellent overall response clinically and radiologically. The echocardiographywas repeated after 6 months and showed normal myocardial thickness with no RVOT obstruction. Also, the size of PAVM was significantlyreduced. That is likely explained by the reduction in the left side pressures. CMR showed significant reduction in the mediastinal mass.
Conclusion: We report a case of cardiac involvement of malignant lymphoma where multimodality imaging was useful for proper assess-ment and staging of the disease, identification of an incidental PAVM and follow up of the response to treatment.
Introduction: Human infection caused by Borterella hinzii is rare. The main risk factor is inmunosuppression. Intracardiac abscess with nor-mal function of valve prosthesis is even less common than endocarditis associated with valve prosthesis dysfunction.
Case description: A 79 year old male who underwent an aortic valve biological prosthetics for severe valve aortic stenosis in 2013. He suf-fered from chronic liver disease, chronic kidney disease, diabetes type 2 and arterial hypertension. There were no cardiovascular incidents inthe follow-up. In 2018 he was admitted to the hospital because of fever and cough, accompanied by dysarthria and alterations in his behav-iour. Any significant abnormalities were found in neither cranial scan nor chest x-ray nor abdominal US. Urine, sputum and blood cultureswere drawn and ceftriaxone was prescribed. But 72 hours later, Borterella hinzii was isolated in blood cultures. Antibiotic therapy was scaledto meropenem because of in vitro antibacterial susceptibilities. The symptoms improved. However, 7 days later, both fever and persistentbacteremia were still present. Several tests were performed. Firstly, a chest abdominal pelvis CT scan did not show any pathological finding.Secondly, transthoracic and transesophageal echocardiograms were performed, which showed a large periaortic cavity (41x29x14mm) be-tween prosthesis and interatrial septum - Fig. A and B. Its aspect was non homogeneous, without any connection between cavity and aorticprosthesis. Moreover, aortic valve prosthesis worked properly. These findings indicated a high diagnosis suspicion of periaortic abscess.Thus, a PET-CT scan (18-F-FDG) was done. It showed an increase in the pathological metabolism of the periaortic valve prosthesis, consis-tent with a perivascular infectious pathology - Fig. C and D. Given the diagnosis of an extensive infective periaortic abscess by B. hinzii withadverse clinical progress, the patient was sent for intervention. It was a very complicated surgery because of a huge abscess located in thefibrous tissue annulus of the heart. It was performed a hard draining of the abscess in combination with left atrial, aortic and left ventricularoutflow reconstruction and both aortic and mitral replacement. In the postoperative period the patient had a favorable evolution. Collectedsamples during the operation confirmed the insulation of Borterella hinzii.
Conclusion: On the one hand, this is a rare case of endocarditis located in fibrosis annulus and periaortic tissue near aortic valve biologicalprosthetics. Chronic liver and kidney disease in this diabetic patient could be predisposing factors for this Borterella’s infection. On the otherhand, multi-modalitity heart imaging techniques are essential in the definitive diagnosis of this unusual endocarditis at a very late stage afteraortic valve replacement.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P230
Multimodality imaging in a rare case of paravalvular endocarditis around the stent of apercutaneus lotus valve
Di Giannuario G.; Candiottti N.; Grosseto D.; Carigi S.; Venturi P.; Santarelli A.; Amati S.; Farneti L.; Mainardi A.; Testa P.; Ruffini M.; Piovac-cari G.
Infermi Hospital of Rimini, Cardiovascular, Rimini, Italy
Funding Acknowledgements: none
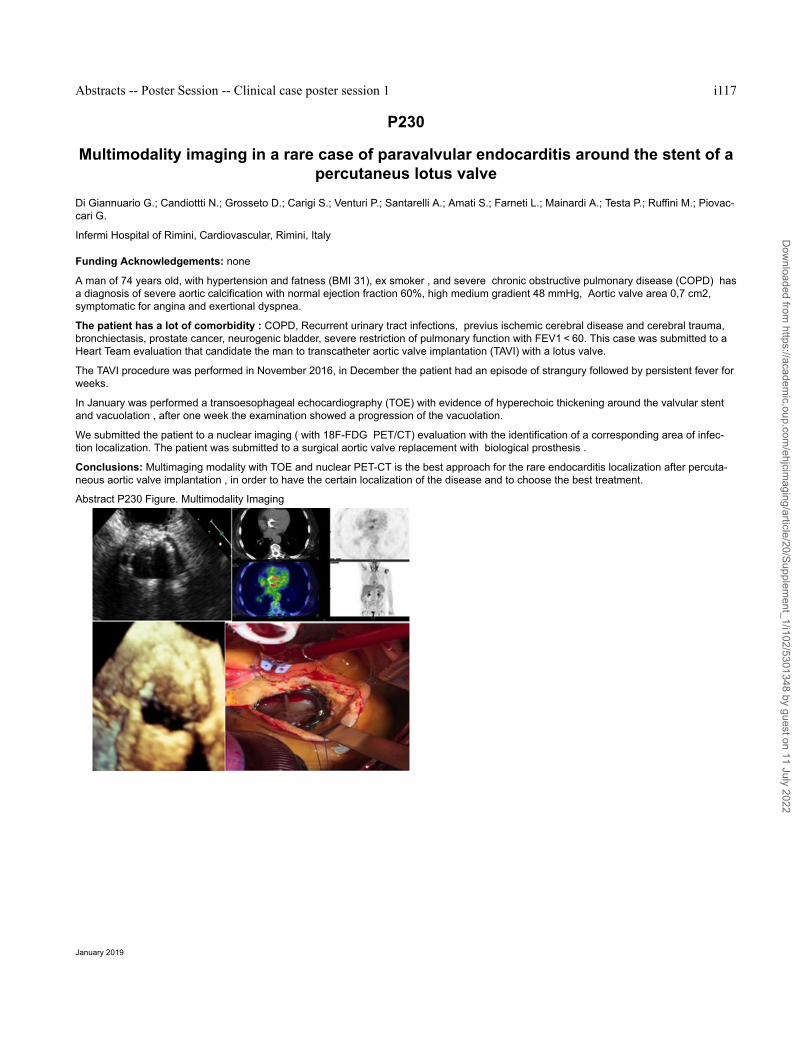
A man of 74 years old, with hypertension and fatness (BMI 31), ex smoker , and severe chronic obstructive pulmonary disease (COPD) hasa diagnosis of severe aortic calcification with normal ejection fraction 60%, high medium gradient 48 mmHg, Aortic valve area 0,7 cm2,symptomatic for angina and exertional dyspnea.
The patient has a lot of comorbidity : COPD, Recurrent urinary tract infections, previus ischemic cerebral disease and cerebral trauma,bronchiectasis, prostate cancer, neurogenic bladder, severe restriction of pulmonary function with FEV1 < 60. This case was submitted to aHeart Team evaluation that candidate the man to transcatheter aortic valve implantation (TAVI) with a lotus valve.
The TAVI procedure was performed in November 2016, in December the patient had an episode of strangury followed by persistent fever forweeks.
In January was performed a transoesophageal echocardiography (TOE) with evidence of hyperechoic thickening around the valvular stentand vacuolation , after one week the examination showed a progression of the vacuolation.
We submitted the patient to a nuclear imaging ( with 18F-FDG PET/CT) evaluation with the identification of a corresponding area of infec-tion localization. The patient was submitted to a surgical aortic valve replacement with biological prosthesis .
Conclusions: Multimaging modality with TOE and nuclear PET-CT is the best approach for the rare endocarditis localization after percuta-neous aortic valve implantation , in order to have the certain localization of the disease and to choose the best treatment.
Background: The mitral-aortic intervalvular fibrosa (MAIVF) is an avascular fibrous structure connecting the anterior mitral leaflet to the aort-ic annulus, susceptible to infection, surgery and trauma which may lead to formation of pseudoaneurysm at the MAIVF level. We diagnoseda PMAIVF in an asymptomatic neonate by a TTE with both 2D and 3D acquisitions and we followed her up for 5 years.
Purposes: Report a case of an asymptomatic 5 years old girl incidentally diagnosed at one month of age, by transthoracic echocardiogram(TTE), to have a pseudoaneurysm of the mitral-aortic intervalvular fibrosa (PMAIVF), and present a review of the literature.
Methods: The baby was referred at one month of age to our institution for a heart murmur which turned to be innocent. Clinical examinationand EKG were normal. No history of infection or trauma or intervention was recorded. Echocardiogram was completely normal with no valvu-lar malformations nor other cardiac anomalies except for the congenital/idiopathic PMAIVF. We performed a 2D and 3D TTE (Fig. 1)with aPhilips iE33 and in parasternal long and short axis views we obtained very clear images of the sac behind the aortic root and posterior andsuperior to the anterior mitral leaflet, with a typical systolic expansion and diastolic collapsing At the age of 4, she underwent CT examina-tion, confirming echo data. Now the girl is 5 yrs old and is undergoing 6 months‘ follow up with 2D and 3D TTE and no variations in sizeand/or shape of the PMAIVF were detected in this 5 years‘ follow up. She is still completely asymptomatic and on aspirin therapy.
Conclusion: Recent published data confirmed that PMAIVF has two prevalent causes: infective endocarditis or surgical trauma. Rare repor-ted cases due to blunt chest trauma or congenital isolated PMAIVF exist. Since clinical evolution of PMAIVF is hard to predict, in the litera-ture dissimilar suggestions about PMAIVF management exist: conservative with close clinical and echocardiographic follow up versus inva-sive surgical approach. All considered we now opted for a conservative approach.
1Sacred Heart Hospital of Negrar, Cardiology, Negrar-Verona, Italy2Sacred Heart Hospital of Negrar, Radiology, Negrar-Verona, Italy
Funding Acknowledgements: No financial support
Background: Among possible anatomical variants, agenesia of the left atrial appendage (LAA) is very rare and differential diagnosis for novisualization of the LAA during transesophageal echocardiogram (TEE) includes complete occlusion by thrombus, poor echocardiographicwindows, prior surgical ligation or percutaneous closure.
Clinical case: A 69 years old man, with persistent atrial fibrillation (AF) was referred to our centre for cryoablation procedure. His work upincluded two dimensional (2D)/ three dimensional (3D) TEE to exclude intracardiac thrombus and contrast-enhanced multidetector compu-ted tomography (CT) for anatomical details of the left atrium (LA). Despite 2D TEE imaging at multiple angles, LAA could not be visualized(arrows, Figures 1A) and colour Doppler imaging characteristic flow of LAA could not be demonstrated (Figure 1B). 3D TEE "en face" viewdemonstrated the absence of LAA anatomic orifice, below left upper pulmonary vein and lateral ridge with uniformity appearance of LA later-al wall (Figure 1C). Cropping 3D data sets, no LAA body was identified, only a small residue (Figure 1D). Multidetector CT scan confirmedthe suspicion of LAA absence with optimal spatial resolution (Figures 1E, 1F). Anatomical reconstruction of LA during cryoablation proce-dure led to the same conclusion, showing pulmonary veins in the usual anatomic pattern and LAA body absence on LA outer surface (Fig-ures 1G).
Conclusion: In conclusion, 3D TEE and multidetector CT could be performed to confirm the presence or absence of LAA and to excludethrombotic occlusion especially in the era of LA intervention. No conflicts of interest.
1University of Medicine and Pharmacy Carol Davila, Cardiology Elias Hospital, Bucharest, Romania2University of Medicine and Pharmacy of Cluj Napoca, 2nd department of Internal Medicine, Cluj Napoca, Romania3Spitalul Monza, Bucharest, Romania4University of Medicine and Pharmacy Carol Davila, Oncology, Elias Emergency University Hospital, Bucharest, Romania
A 69 y/o man was referred to our department for coronary angiography. He complained for at least one month of jaw pain and fatigue onexertion. Six month before he had been operated for right bronchopulmonary adenocarcinoma (right inferior lobectomy and mediastinal lym-phadenectomy) undergoing chemotherapy afterwards. A cardiologic exam performed one month before diagnosed myocardial infarction andechocardiography at that time described wall motion abnormality and apical thrombus attached to the akinetic apical segments of lateral andinferior walls. ECG (fig 1) showed sinus rhythm, tall R waves V1-V2, ST segment elevation I, II, III, aVF, V3-V6, horizontal ST segment de-pression V1-V2, aVR. Echocardiography (fig 2) performed in our institution showed normal LVEDD, LVESD, normal LVEF, thick LV walls,especially in the apical segments of lateral and inferior walls, and small pericardial effusion (5 mm adjacent to the lateral wall), raising thesuspicion of a LV wall tumor. Coronary angiography showed normal coronary arteries and ventriculography suggested apical hypertrophiccardiomyopathy. We referred the patient to another unit for cardiac MRI. The MRI diagnosis intramyocardial hematoma involving apical seg-ments of the inferior and lateral walls, apical pseudoaneurysm of inferolateral wall, infero-lateral myocardial infarction, normal size LV, LVEF56%, normal size and function RV and small pericardial effusion. Thoracic CT (fig 3A) performed for neoplasia surveillance showed a diffuseregion of myocardial edema 6/4cm and suggested ischemia. Cardiac surgery was indicated for the LV pseudoaneurysm. The surgeon founda thick but spongious aspect of the apical segments of the LV heavily adherent to the pericardium that could not be excised but severalbiopsies were taken. The result was mesothelioma or atypical carcinomatous tumour. Imunohistologic examination of the biopsies confirmedscuamous carcinoma. The evolution was poor despite chemotherapy (gemcitabine + carboplatin). The follow-up CT (fig 3B) performed afterthree months showed marked increase in LV tumour size and mediastinal adenopathies. Meanwhile the etiology of temporomandibular painwas determined. An initial negative CT of the region was followed by CT showing a mass invading the bone, progressing in the third CTexam. The amplitude of ST segment elevation increased during follow-up. The patient died 3 months after the first presentation to our de-partment.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P234
Left ventricular ejection fraction in patients with heart failure with reduced ejectionfraction and small left ventricle is not a good predictor of mortality
1Medical University of Silesia, SMDZ in Zabrze, 3rd Department of Cardiology, Silesian Centre for Heart Disease in Zabrze, Katowice, Po-land2Medical University of Silesia, Department of Social Medicine and Prevention, School of Public Health in Bytom, Katowice, Poland
Introduction: Left ventricular ejection fraction (LVEF) is an independent prognostic factor in patients with heart failure with reduced LVEF(HFrEF).
Purpose: The purpose of our study was to verify the hyposthesis whether LVEF in patients with HFrEF and small left ventricular end diastol-ic volume (LVEDV) has the same predictive value than in patients with HFrEF and normal or large LVEDV.
Methods: There were 1505 patients with optimally treated stable HFrEF included in the study. Repeated Cox proportional hazard regressionanalyses were performed to determine the LVEDV threshold below which LVEF loses its predictive value for 12-month mortality. In the nextstep, baseline characteristics and 12-month mortality between groups with LVEDV below and over the threshold were compared.
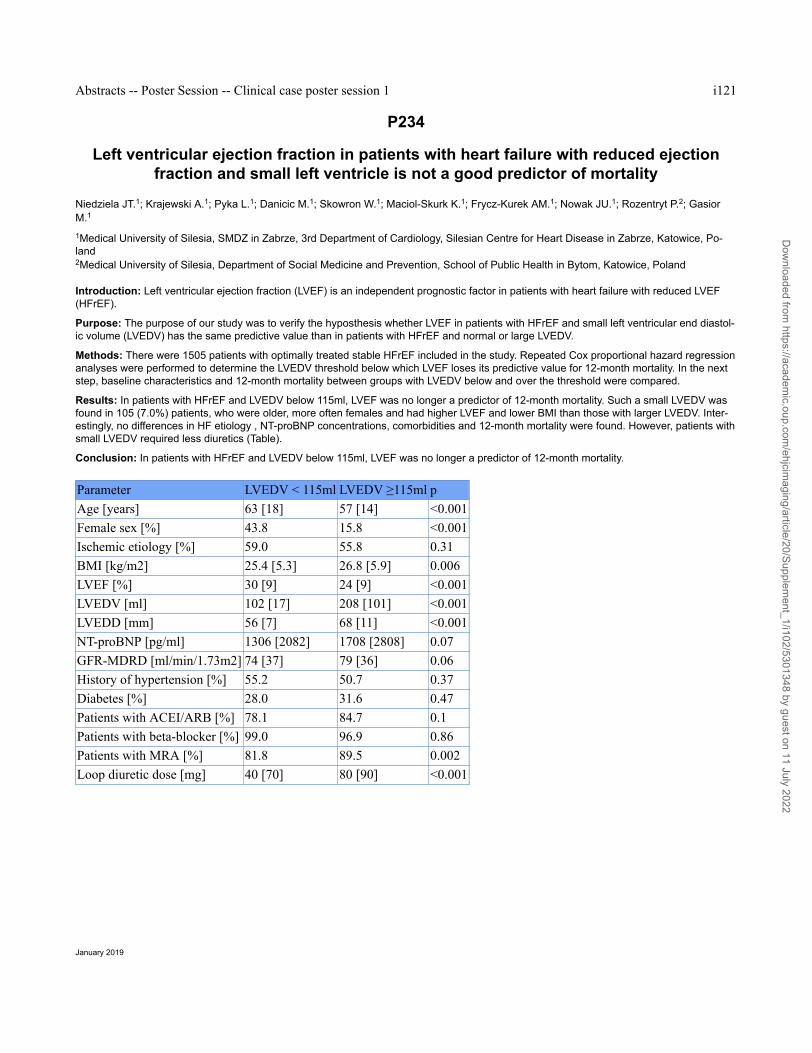
Results: In patients with HFrEF and LVEDV below 115ml, LVEF was no longer a predictor of 12-month mortality. Such a small LVEDV wasfound in 105 (7.0%) patients, who were older, more often females and had higher LVEF and lower BMI than those with larger LVEDV. Inter-estingly, no differences in HF etiology , NT-proBNP concentrations, comorbidities and 12-month mortality were found. However, patients withsmall LVEDV required less diuretics (Table).
Conclusion: In patients with HFrEF and LVEDV below 115ml, LVEF was no longer a predictor of 12-month mortality.
1Northwest state medical university by I.I. Mechnikov, Functional Diagnostic Department, St. Petersburg, Russian Federation2State hospital ?40, Functional diagnostic, Saint-Petersburg, Russian Federation
Patient K., 66 years old, was hospitalized by emergency with sustained anginal pains irradiating to the interscapular space on February 27,2018. Taking into account the clinical symptoms, ECG changes, increase of myocardial necrosis markers, inferior myocardial infarction (MI)was verified. At coronary angiography: left anterior descending artery (LAD) stenosis in the middle third 80%, diagonal artery orifice stenosis50%, circumflex artery stenosis 70%, right coronary artery (RCA) thrombotic occlusion. Simultaneously, angioplasty and stenting of RCA bytwo no drug-eluting stents were performed with a good angiographic result. Coronary bypass surgery further had been planned.
On the 3rd day of hospitalization negative dynamics consisted in increase of heart failure (HF) signs. By echocardiography (Echo) postin-farction interventricular septal (IVS) rupture 21 mm with a significant left-to-right shunt, basal left ventricular (LV) aneurysm were found. LVejection fraction was 76%.
Сontrol echo data revealed the expansion of the defect with the separation of the IVS dissection from basal part to LV apex.
Taking into account the early terms of myocardial infarction, the stability of hemodynamics the emergency correction of the IVS rupture wasconsidered inadvisable. Conservative treatment of MI and preparation for surgery (myocardial revascularization + IVS rupture correction)was recommended.
Later the HF symtoms progressed: lower extremities edema, ascites, bilateral hydrothorax, hydropericard and bilateral pneumonia. Com-plex conservative therapy allowed stabilize the patient"s status, manifestations of the infectious-inflammatory syndrome were stopped. Re-current worsening was noted 13.04.2018 with appearance of anginal pain at rest, which was stopped by short-acting nitrates. Coronary inter-vention due to unstable angina was performed on 13.04.2018.
Sternotomy, endoventriculoplasty of IVS by xenopericardial patch, LAD angioplasty, autovenous marginal brances and posterior descendingartery bypass grafting were performed.
In the early postoperative period signs of HF persisted. Treatment of patient in the intensive care department consisted of inotropic and vaso-pressor support. Intra-aortic balloon pump was stopped on April 17, 2018. As a result of pleural drainage procedure 1,500 ml serous-hemor-rhagic liquid from the right and 1200 ml from the left pleural cavity were evacuated. Haemotransfusion therapy was also performed. No angi-na symtoms were noted at the early postoperative period.
On 19.04.2018. the patient was successfully discharged in satisfactory state for further cardiac rehabilitation.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P237
Challenging pregnancy counselling in a case with systemic RV dysfunction - multimo-dality imaging
Castro Verdes MB.1; Ilagan L.2; Surkova E.2; Flick C.2; West C.2; Babu-Narayan S.3; Li W.3
1Royal Brompton Hospital, Cardiology, London, United Kingdom2Royal Brompton Hospital, Echocardiography, London, United Kingdom3Royal Brompton Hospital, Adult congenital heart disease, London, United Kingdom
In patients with Transposition of the Great Arteries (TGA) and Mustard, systemic right ventricle (RV) systolic function (RVSF) is a predictor ofoutcome. Pregnancy represents an additional stress for haemodynamic decompensation that can be fatal. We present a case of systemicRV dysfunction with difficult risk stratification due to discrepant imaging modalities.
A 30 year-old lady with TGA repaired with Mustard aged 4 and ventricular septal defect closed percutaneously in 2006, was asymptomaticand physically active, with a recent excellent exercise test. Her RV was known to be severely dilated and moderately dysfunctional despiteheart failure medication. She manifested desire for pregnancy, and counselling work-up including a stress echocardiogram (SE) off medica-tion and right heart catheterisation (Rcath) was started.
A SE on a bicycle was performed. At rest, RV appeared severely impaired. Fractional area change was negative due to reversed septalmotion and TAPSE was 12mm. There was moderate functional tricuspid regurgitation (TR), mild pulmonary veins baffle obstruction, mild leftventricle (LV) outflow tract obstruction (LVOT), and severe pulmonary regurgitation. The LV was normal. The patient exercised for 08:35minwith adequate chronotropic response, reaching 90% of maximum heart rate. She remained asymptomatic, with no drop in blood pressure orarrhythmias. At peak stress, RVSF and TR improved visually. The LV became hyperdymanic and LVOT gradient increased to 77mmHg. 3dimensional (3D) RV ejection fraction (RVEF) at rest was estimated in 11%, and Global longitudinal strain at -3.6%. A MRI revealed RV enddiastolic volume of 275ml and RVEF of 40%. Late gadolinium enhancement suggested mild fibrosis of the anterior RV wall. Rcath showednormal pulmonary artery pressure (26/8/16) and normal RV end-diastolic pressure (5).
The accurate estimation of systemic RVSF is crucial, because severe impairment heightens maternal risk for complications such as arrhyth-mias or sudden death. Multimodality imaging in this case illustrates the inherent challenges of RV functional assessment and the conse-quent clinical implications. 3D has the advantage to overcome the biplane limitations of 2D. However, normal values for systemic RVEF ordimensions are not currently available. In addition, MRI remains the gold standard for quantification of RV volumes and function, but theagreement between 3D and MRI in congenital heart disease has not been stablished. Indirect signs suggested maintained RV contractilereserve (visual improvement in RVSF and TR on exercise, lack of symptoms, good blood pressure response), and MRI RVSF was not se-verely impaired. In this regard, a pregnancy would be considered high risk but not contraindicated. However potential RVSF deteriora-tion during pregnancy may ensue, often unpredictably, and patients need to be counselled accordingly.
1Sao Joao Hospital, Porto, Portugal2Hospital Centre do Tamega e Sousa, Cardiology, Penafiel, Portugal
INTRODUCTION: Blunt chest trauma is a rare, but potentially catastrophic, cause of aortic regurgitation (AR). Trauma occurring during theventricular diastole could lead to the rise of aortic pressure against the closed aortic valve, which may result in the rupture or detachment ofone or more cusps.
CLINICAL CASE: The authors report the case of a 36-year-old woman, victim of motor vehicle accident (run over). Major right limbs bonefractures and chest trauma with a pneumothorax lead to a prolonged hospitalization in an intensive care unit with the need for several ortho-paedic interventions. There was no reference to cardiac complications during this period. After physical rehabilitation, the pt recovered welland returned to daily life without major limitations. About a year after the event, the patient was observed at primary care for worsening fati-gue; a de novo decrescendo diastolic murmur, audible at the level of the sternum left border was found. Transthoracic echocardiogram (TTE)revealed moderate to severe aortic regurgitation (AR), with a very eccentric jet (making it difficult to understand its mechanism and aetiolo-gy), a non-dilated left ventricle and with preserved systolic function and a non-dilated ascending aorta (AA). The patient was the referred toour center for additional stud. Transesophageal echocardiogram (TEE) confirmed the presence of severe AR, in a tricuspid aortic valve withthin cusps. The 3D evaluation od the aortic valve revealed an oval and irregular cleft (11x4mm) at base of the non-coronary cusp (NCC) asthe cause of this severe eccentric AR (3D VC 4x11mm; RVol 71mL; EROA 0.36cm2; diastolic reversed flow in ascending aorta). No otherrelevant findings were documented (normal dimension of AA and cardiac cavities; no signs of pulmonary hypertension; preserved biventricu-lar systolic function). The patient was referred for surgery with confirmed the presence of a tricuspid aortic valve with a single perforation ofthe NCC, near the annulus. Aortic valve repair was possible - closure of the cusp tear with autologous pericardium. After an unremarkable 5-day hospital stay, the pt was discharged and remains clinically well at 1-month follow up.
CONCLUSION: Traumatic AR clinical presentation is very heterogeneous. Because of its dismal prognosis, prompt surgical correctionshould be considered in all cases. This clinical case illustrates the unquestionable role of 3D TEE in the study of valve morphology and forsurgical planning, specially when a valve repair is being considered.
Abstract P238 Figure. 3D TEE en-face view of the aortic valve
Background:The echocardiographic appearance of residual floating masses in the right atrium after removal of permanent pacemakers andimplantable cardioverter-defibrillators was recently described. However, the significance of these ghosts and their relationship with CDRIEare unknown.
Case presentation
We report a case of 18 years old male patient with past history of dual chamber pacemaker implantation (DDD) on top of complete heartblock 4 years ago.He reported persistent fever for 3 months. On examination, temperature was 39˚c.No audible murmurs could be heard.Routine laboratory investigations showed high white cell count and CRP values. Blood cultures revealed no bacterial growth. 2D Transthora-cic echocardiography (TTE) showed a floating right atrial (RA) mass near the IVC orifice. No vegetations could be seen over the tricuspidvalve.2D Tranesophageal echocardiography (TEE) showed 2 large mobile masses attached to one of the pacemaker leads. 3D TEE re-vealed clearly the attachment of the vegetations to the RA lead .Percutaneous extraction of both leads was done and antibiotics were initi-ated immediately. Follow up TTE and TEE revealed 2 residual small vegetations seen attached to a fibrous sheath along the RA lead. An-other new two elongated and highly mobile structures were seen coming from SVC orifce.3D TTE revealed 2 long mobile masses seen at-tached to the ventricular perspective of the tricuspid valve with mild valve regurgitation. At the end of antimicrobial course, no residual mass-es were seen at the SVC nor on the tricuspid valve yet, the RA masses were still there but smaller in size.His resting heart rate was 55 bpmwith no related resting nor exertional symptoms.The patient was discharged and scheduled for follow up visits.
Conclusion: Ghosts are observed in 8% of patients after percutaneous device extraction. Their presence is suggestive of device infectionand seems to be associated with the diagnosis of CDRIE. The prognostic significance of such findings needs further investigation.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P240
Persistent left atrial appendage formation despite prolonged oral anticoagulation: it"snot always a clot. 3D transesophageal ecocardiography diagnosis of cardiac fibroelas-
toma
Bernardini A.1; Taborchi G.1; Colella A.2; Berteotti M.1; Del Bene R.1; Barletta GA.1
1Careggi University Hospital (AOUC), Diagnostic Cardiology, Florence, Italy2Careggi University Hospital (AOUC), Electrophysiology Department, Florence, Italy
The prevalence of transesophageal echocardiography–detected thrombi in the left atrial appendage (LAA) during oral anticoagulation variesbetween 0.5 and 7%. This event, although less frequent than during the treatment with Vitamin K Antagonists (VKA), was reported also withNovel Oral Anticoagulants (NOACs).
We present the case of a patient affected by atrial fibrillation (AF) who received a previous diagnosis of mobile thrombus in LAA despitecorrect anticoagulation, but with echocardiographic characteristics that suggested a different and rarer etiology than clot.
A 69 year old man affected by persistent AF, hypertension and obstructive sleep apnea syndrome underwent transesophageal echo evalua-tion (TEE) for a catheter ablation procedure to improve AF-related symptoms; the patient was on VKA (Warfarin) because his CHA2DS2-VASc score was 2. TEE showed a mobile and pedunculated formation with a diameter of 5 millimeters in the proximal part of the LAA, whichwas suspicious for a clot. As under dosage of oral anticoagulant was guessed, the ablation procedure was postponed and a new anticoagu-lation therapy with Dabigatran 300 milligrams per day was started.
Four weeks after strict NOAC therapy, a second TEE was performed. Being the pedunculated formation still present, the coagulation assetwas reevaluated. Diluted thrombin time and ecarin clotting assay confirmed Dabigatran levels in therapeutic range.
Six weeks after additional anticoagulant therapy, the patient was referred to our Hospital Center for a second opinion evaluation. As 2D-TEEcould only confirm the persistence of the mobile formation, 3D-TEE was performed. It showed absence of slow flow in the LAA and presenceof the mobile and pedunculated structure attached to the superior and proximal part of the LAA with some kind presence of multiple papillaryfronds. Another analogue smaller lesion (2 millimeters in diameter) was found in the left coronary cusp of the aortic valve. Given the stabilityof the lesion despite correct oral anticoagulation, its morphology, the unusual position, the coexistence of a similar lesion on the aortic valve,the diagnosis of cardiac fibroelastoma was supposed.
Taking into account the absence of embolic complications, the small dimension of the lesions and the lack of specific recommendations fromthe literature, the consensus was to not proceed with surgical excision of the suspected fibroelastoma.
An informed consent about the risks of the procedure was obtained and catheter ablation of the pulmonary veins was performed; no emboliccomplications occurred and sinus rhythm was restored. After 4 months follow-up the patient had remained in sinus rhythm, asymptomatic,anticoagulation with Dabigatran was continued.
Two lessons may be learned from this clinical case: 1. not all the mobile masses in left atrium are clot formations; 2. a fibroelastoma inLAA do not contraindicate ablative procedure for AF.
Abstract P240 Figure. 3D-TEE view of the fibroelastoma in LAA
1Hospital of Santarem, Cardiology, Santarem, Portugal2Hospital de Santa Marta, Cardiothoracic Surgery Department, Lisbon, Portugal
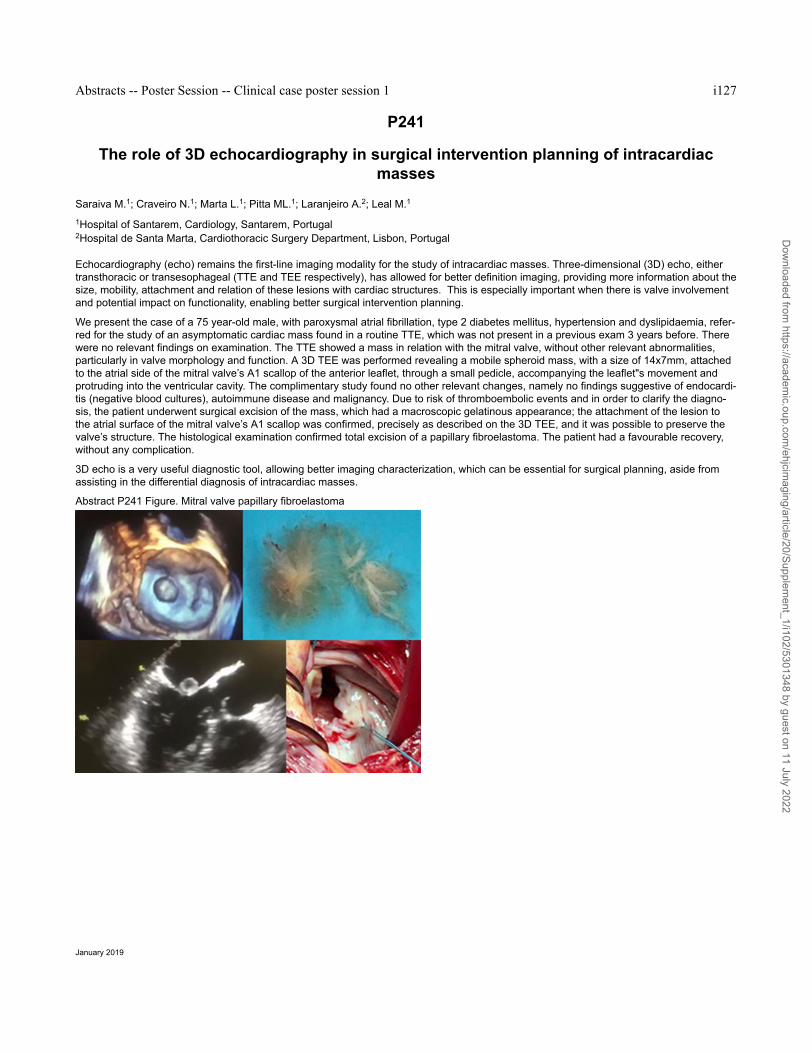
Echocardiography (echo) remains the first-line imaging modality for the study of intracardiac masses. Three-dimensional (3D) echo, eithertransthoracic or transesophageal (TTE and TEE respectively), has allowed for better definition imaging, providing more information about thesize, mobility, attachment and relation of these lesions with cardiac structures. This is especially important when there is valve involvementand potential impact on functionality, enabling better surgical intervention planning.
We present the case of a 75 year-old male, with paroxysmal atrial fibrillation, type 2 diabetes mellitus, hypertension and dyslipidaemia, refer-red for the study of an asymptomatic cardiac mass found in a routine TTE, which was not present in a previous exam 3 years before. Therewere no relevant findings on examination. The TTE showed a mass in relation with the mitral valve, without other relevant abnormalities,particularly in valve morphology and function. A 3D TEE was performed revealing a mobile spheroid mass, with a size of 14x7mm, attachedto the atrial side of the mitral valve’s A1 scallop of the anterior leaflet, through a small pedicle, accompanying the leaflet"s movement andprotruding into the ventricular cavity. The complimentary study found no other relevant changes, namely no findings suggestive of endocardi-tis (negative blood cultures), autoimmune disease and malignancy. Due to risk of thromboembolic events and in order to clarify the diagno-sis, the patient underwent surgical excision of the mass, which had a macroscopic gelatinous appearance; the attachment of the lesion tothe atrial surface of the mitral valve’s A1 scallop was confirmed, precisely as described on the 3D TEE, and it was possible to preserve thevalve’s structure. The histological examination confirmed total excision of a papillary fibroelastoma. The patient had a favourable recovery,without any complication.
3D echo is a very useful diagnostic tool, allowing better imaging characterization, which can be essential for surgical planning, aside fromassisting in the differential diagnosis of intracardiac masses.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P242
The case of the vanishing cardiac massImran T.; Manning P.; Bernard S.
Boston University, Boston Medical Center, Cardiology Section , Boston, United States of America
Introduction: Immune checkpoint inhibitors such as Ipilimumab and Nivolumab have significantly improved the prognosis of patients withmetastatic melanoma. However, their effects on cardiac metastases have not been elucidated.
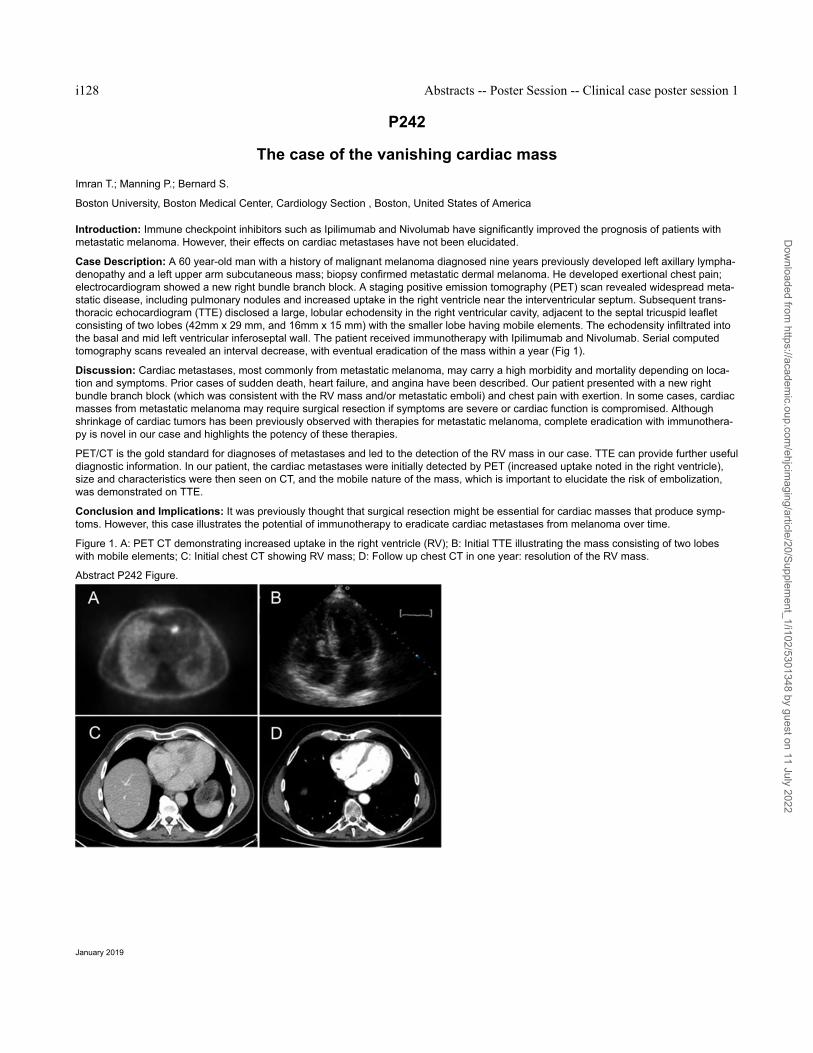
Case Description: A 60 year-old man with a history of malignant melanoma diagnosed nine years previously developed left axillary lympha-denopathy and a left upper arm subcutaneous mass; biopsy confirmed metastatic dermal melanoma. He developed exertional chest pain;electrocardiogram showed a new right bundle branch block. A staging positive emission tomography (PET) scan revealed widespread meta-static disease, including pulmonary nodules and increased uptake in the right ventricle near the interventricular septum. Subsequent trans-thoracic echocardiogram (TTE) disclosed a large, lobular echodensity in the right ventricular cavity, adjacent to the septal tricuspid leafletconsisting of two lobes (42mm x 29 mm, and 16mm x 15 mm) with the smaller lobe having mobile elements. The echodensity infiltrated intothe basal and mid left ventricular inferoseptal wall. The patient received immunotherapy with Ipilimumab and Nivolumab. Serial computedtomography scans revealed an interval decrease, with eventual eradication of the mass within a year (Fig 1).
Discussion: Cardiac metastases, most commonly from metastatic melanoma, may carry a high morbidity and mortality depending on loca-tion and symptoms. Prior cases of sudden death, heart failure, and angina have been described. Our patient presented with a new rightbundle branch block (which was consistent with the RV mass and/or metastatic emboli) and chest pain with exertion. In some cases, cardiacmasses from metastatic melanoma may require surgical resection if symptoms are severe or cardiac function is compromised. Althoughshrinkage of cardiac tumors has been previously observed with therapies for metastatic melanoma, complete eradication with immunothera-py is novel in our case and highlights the potency of these therapies.
PET/CT is the gold standard for diagnoses of metastases and led to the detection of the RV mass in our case. TTE can provide further usefuldiagnostic information. In our patient, the cardiac metastases were initially detected by PET (increased uptake noted in the right ventricle),size and characteristics were then seen on CT, and the mobile nature of the mass, which is important to elucidate the risk of embolization,was demonstrated on TTE.
Conclusion and Implications: It was previously thought that surgical resection might be essential for cardiac masses that produce symp-toms. However, this case illustrates the potential of immunotherapy to eradicate cardiac metastases from melanoma over time.
Figure 1. A: PET CT demonstrating increased uptake in the right ventricle (RV); B: Initial TTE illustrating the mass consisting of two lobeswith mobile elements; C: Initial chest CT showing RV mass; D: Follow up chest CT in one year: resolution of the RV mass.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P243
Radionuclide ventriculography phase analysis for risk stratification of patients under-going cardiotoxic cancer therapy
Jones KA.1; Small AD.1; Paterson CA.1; Robinson J.1; Hamilton DJ.2; Goodfield N E R1
1Glasgow Royal Infirmary, Nuclear Cardiology, Glasgow, United Kingdom2University of Glasgow, Glasgow, United Kingdom
Background/Introduction
Accurate diagnostic tools to identify patients at risk of cancer therapy related cardiac dysfunction (CTRCD) are critical.
Serial Radionuclide ventriculography (RNVG) is often used to assess LVEF (as well as left ventricular wall motion) in patients receiving car-diotoxic cancer therapy to monitor cardiac function. There has been interest within the field in further measures, including entropy, fromRNVG studies to provide additional prognostic information and characterise dyssynchrony.
Approximate Entropy (ApEn) is a regularity statistic that quantifies unpredictability of fluctuations in a series or data and, unlike simple entro-py, takes into account regional phase similarity of adjacent pixels. ApEn calculates the probability that a series of length m remains similarwithin a tolerance r at the next point in the data series. It is well established in other fields. e.g. gait analysis and heart rate variability but hasnot previously been widely investigated for assessing ventricular contraction.
Echocardiography derived measures of myocardial mechanics such as speckle tracking derived myocardial longitudinal strain, which arerelated to dyssynchrony, have demonstrated predictive utility for left ventricular ejection fraction (LVEF) decline and / or symptomatic heartfailure. This suggests that RNVG measures of dyssynchrony, such as ApEn, may also have predictive value in assessing cardiotoxicity.
Purpose: The aim of this work is to determine if ApEn can predict which patients are at a higher risk of CTRCD.
Methods: Phase analysis was retrospectively carried out on sequentially acquired baseline RNVG studies of 195 breast cancer patientsbefore they received Trastuzumab therapy. All patients had multiple studies and a baseline ejection fraction of > 55%. 24 frame gated RNVGimages were acquired and ApEn was calculated from phase information extracted from the first order Fourier harmonic of the RNVG.
Serial RNVG images were acquired for each patient at intervals of approximately 3 months for up to 2 years following the baseline study.Patients had between 2 and 9 RNVGs from which LVEF was measured and compared to baseline.
The maximum change in LVEF between baseline and subsequent scans was determined and compared with ApEn.
Results: Patients were split into 3 groups based on the maximum change in LVEF. Group 1 (102 patients) showed no significant drop (<10%) in LVEF, Group 2 (75 patients) showed a drop of more than 10% while maintaining a normal LVEF (> 50%), Group 3 (12 patients) werefound to have a drop in LVEF of more than 10% to below 50%.
A significant difference (p <0.01) in ApEn was found between Groups 1 (mean ApEn: 0.70 ) & 3 (mean ApEn: 0.80 ) and Groups 2 (meanApEn: 0.72) & 3. There was no significant difference between Groups 1 & 2.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P244
Concealed cardiac amyloidosis in a patient with biventricular takotsubo cardiomyop-athy
Okura H.; Keshi A.; Nakada Y.; Ishihara S.; Nogi M.; Okayama S.; Kawakami R.; Saito Y.
Nara Medical University, Kashihara, Japan
Case presentation: A 85-year-old woman was transferred to our hospital because of dyspnea. She had been medicated for chronic heartfailure (HF) of unknown origin and chronic kidney disease for one year. Physical examination revealed that jugular vein was distended andthird heart sound was audible. A chest X-ray showed cardiomegaly and pulmonary congestion. An ECG showed poor r wave progression onV1-4 and ST elevation in V2-4. Imaging Findings: Echocardiography showed LVH, diffuse mild hypokinesis of LV and severely reduced bi-ventricular apical wall motion (Figure A, arrows). Her HF improved with vasodilator and diuretics. Echocardiography showed improved biven-tricular apical wall motion. Coronary angiography showed that her coronary artery was normal. 99mTc-pyrophosphate scintigraphy revealeddiffuse left ventricular uptake confirming the diagnosed of ATTR cardiac amyloidosis (Figure B). Serial echocardiography demonstrating tran-sient biventricular apical wall motion abnormalitiestrongly suggested the diagnosis of biventricular Takotsubo cardiomyopathy (TC). On theother hand, presence the diffuse LV hypokinesis with LVH and a granular sparkling pattern suggested the diagnosis of cardiac amyloidosis.
Discussion: TC is characterized as a transient mid-ventricular wall motion abnormality with or without apical involvement. Although emotion-al or physical stress such as infection, stroke and cancer are known triggers of TC, cardiac disease could be a trigger or co-existing conditionof TC. Careful interpretation of the echocardiographic images and multimodality image assessments are needed to correctly diagnose pa-tients with multiple cardiac diseases.
1Medical Research Institute, Alexandria University, Cardiology and Angiology Unit, Clinical and Experimental Internal Medicine Department,Alexandria, Egypt2Alexandria University, Department of Cardiology, Alexandria, Egypt3Alexandria University, Department of Radiology, Medical Research Institute, Alexandria, Egypt
Introduction: Pulmonary capillary hemangiomatosis (PCH) is a rare devastating disease characterized by dysregulated pulmonary capillaryangiogenesis infiltrating peribronchial, perivascular interstitium, and lung parenchyma. According to the Fifth World Symposium on Pulmona-ry Hypertension held in Nice, PCH, together with pulmonary veno-occlusive disease (PVOD), is classified as a subcategory of group 1 pul-monary arterial hypertension (PAH). Patients with PCH typically present with pulmonary hypertension and the condition usually progressesrapidly until severe pulmonary hypertension and resulting right cardiac failure develop.
Case Presentation: We report a case of 37 years old male patient presented to our medical facility complaining of long-standing bilaterallower limb oedema and abdominal swelling for years. On examination, bilateral congested non-pulsating neck veins with marked ascites,hepatomegaly and lower limb oedema were encountered. Routine laboratory investigations including virology were unremarkable, chest xray revealed marked cardiomegaly. Abdominal ultrasonography revealed congested hepatomegaly with dilated hepatic veins and inferiorvena cava (IVC). 2D and 3D Transthoracic echocardiography (TTE) revealed dilated right side with hugely dilated right atrium with overlyingright atrial thrombus with severe tricuspid regurgitation, dilated pulmonary artery and branches and a moderate amount of pericardial effu-sion. Chest Multislice computed tomography (MSCT) with pulmonary angiography showed diffuse small ground glass centrilobular pulmo-nary nodules seen in both longs with no lobar predominance such features are highly suggestive of PCH as the cause of severe pulmonaryhypertension.
So, long-standing right-sided heart failure of the patient was finally explained by PCH. The patient was discharged on anti-failure measuresand anticoagulation with close follow-up.
Conclusion: PCH is a subgroup of PAH characterized by uncontrolled capillary proliferation in the lung. Clinically, PCH can be asymptomat-ic at 1st resulting in irreversible PAH with subsequent right-sided heart failure. Medications used for PAH were applied in PCH treatment butare relatively ineffective. Vasodilators should be used cautiously due to the risk of pulmonary oedema, respiratory distress, and death. Medi-cations targeting pathogenesis of PCH, such as imatinib, doxycycline, and interferon alpha-2a, are reported to be effective in some cases.
Abstract P245 Figure. TTE,MSCT of PCH with RAA thrombus
1Medical Research Institute, Alexandria University, Cardiology and Angiology Unit, Clinical and Experimental Internal Medicine Department,Alexandria, Egypt2Alexandria University, Department of Cardiology, Alexandria, Egypt3Alexandria University, Department of Radiology, Medical Research Institute, Alexandria, Egypt4Ain Shams University, Department of Cardiology, Cairo, Egypt
Introduction: Pulmonary capillary hemangiomatosis (PCH) is a very rare fatal disease characterized by dysregulation of pulmonary capillaryangiogenesis infiltrating peribronchial, perivascular interstitium, and lung parenchyma. According to pulmonary hypertension classification,PCH, together with pulmonary veno-occlusive disease (PVOD), is classified as a subcategory of group 1 pulmonary arterial hypertension(PAH). Patients with PCH may be asymptomatic for a longtime then typically present with pulmonary hypertension and it progresses rapidlyuntil severe pulmonary hypertension and consequently right-sided heart failure develop.
Case presentation: We report a case of 19 years old male patient with no past medical or surgical history presented to our medical facilitycomplaining of dyspnea and effort intolerance since 5 months. On examination pansystolic murmur was best heard on the tricuspid area andpropagated over the whole pericardium with accentuated P2 over the pulmonary area. Routine laboratory investigations including virologywere unremarkable. Chest x ray revealed marked cardiomegaly. Electrocardiogram (ECG) demonstrated signs of right ventricular (RV) hy-pertrophy with tall right precordial R waves, right axis deviation and right ventricular strain. 2D Transthoracic echocardiography (TTE) re-vealed marked RV hypertrophy with evident dilatation with severe tricuspid regurgitation with marked delay in contrast study. Zoomed mode3D TTE of the tricuspid valve from RV perspective revealed a quadricuspid tricuspid valve with marked leaflet thickening.
Chest Multislice computed tomography (MSCT) with pulmonary angiography showed diffuse small ground glass centrilobular pulmonary nod-ules seen in both longs with no lobar predominance such features are highly suggestive of PCH as the cause of severe pulmonary hyperten-sion. The patient refused to proceed for further invasive techniques to confirm the diagnosis with lung biopsy and he was discharged onmedical treatment and close follow-up
Conclusion: PCH is a subgroup of PAH characterized by uncontrolled capillary proliferation in the lung. Clinically, PCH can be asymptomaticat 1st resulting in progressive irreversible PAH with subsequent end-stage right-sided heart failure. Usual medications used for treatment ofPAH are usually ineffective. Vasodilators should be avoided due to the risk of pulmonary oedema, respiratory distress, and death. Medica-tions targeting pathogenesis of PCH, such as imatinib, doxycycline, and interferon alpha-2a, are reported to be effective in some cases.
Abstract P246 Figure. CT, 2D, 3D TTE OF PCH with severe PAH
1Medical Research Institute, Alexandria University, Cardiology and Angiology Unit, Clinical and Experimental Internal Medicine Department,Alexandria, Egypt2Alexandria University, Department of Cardiology, Alexandria, Egypt3Alexandria University, Department of Radiology, Alexandria, Egypt
introduction: Endomyocardial fibrosis (EMF) is a form of restrictive cardiomyopathy common in the tropics and subtropics. The aetiology ofEMF is unknown but parastitic infections such as schistosomiasis have been implicated.
Case presentation: A 45-years old female patient with past history of treated Schistosomiasis since 25 years presented to our healthcarefacility complaining of a gradual onset of dyspnea grade III which was not associated with orthopnea or paroxysmal nocturnal dyspnea. Onclinical examination she was distressed with congested non-pulsating neck veins with icteric tinge, distant heart sounds, hypotension andbilateral lower limb oedema. Echocardiography revealed large tamponading pericardial effusion and dilated right atrium and collapsed rightside. Pericardiocentesis was done through a subcostal view with a tapping of 2000 cc of hemorrhagic effusion. Transthoracic echocardiogra-phy after tapping revealed obliterated right ventricular apex with hugely dilated right atrium measuring 130 mm in maximum dimension. CTchest with IV contrast showed marked dilatation of right atrium compressing the left cardiac chambers & displacing the pulmonary trunk tothe left side with marked distension of superior & inferior vena cavae with moderate pericardial effusion and bilateral mild pleural effusion.Cardiac MRI (CMR) revealed relatively smaller right ventricle with marked obliteration of its apex. Moderate tricuspid regurgitation and mildmitral regurgitation are noted with markedly dilated right atrium as well as congested IVC and hepatic veins. in the late Gadolinium enhance-ment sequence, apical RV diffuse sub-endocardial enhancement was noted (V–sign) yet no LV enhancement could be noted. No evidenceof ventricular thrombi with a Mild pericardial collection, and moderate bilateral pleural effusion. Recurrent tapping due to rapid reaccumula-tion of pericardial effusion with further pleuropericardial window was done with follow-up echo revealing mild pericardial effusion. She wasdischarged safely on anticoagulation for atrial fibrillation and diuresis and follow-up.
conclusion:
So, we report a case of right-sided endomyocardial fibrosis (EMF) in a patient with schistosomiasis, however, the relation between both re-mains to be clarified. We believe that fibrosis plays a crucial role in the pathogenesis of liver and cardiac disease in those patients.2D/3DTTE allows early detection of cardiac fibrosis and associated complications commonly pericardial effusion.
Abstract P247 Figure. 2D, 3D TTE and CMR of bilharzial EMF
Introduction. Pulmonary embolism (PE) is the third most frequent cardiovascular disease with an estimated annual incidence of 100-200per 100000 inhabitants. Computed tomographic pulmonary angiography (CTPA) is the method of choice according the current guidelines toevaluate a patient with suspected PE. In the majority of cases PE originates from deep vein thrombosis (DVT). The CUS (Compression Ve-nous Ultrasonography), by showing incomplete compressibility of the vein, is the diagnostic criteria for DVT and an important tool in patientswith suspected PE. According to ESC Guidelines, simplified CUS only examines four anatomical focus (groin and popliteal fossa).
Case report. An 84-year-old man was admitted to the emergency department with chest pain and dyspnoea and a reported episode of syn-cope about two-three hours before. History of hypertension under pharmacological treatment was the only cardiovascular risk factor recor-ded. At admission he presented tachycardia and tachypnea. Blood pressure was 105/70 mmHg. Electrocardiogram was suggestive for pul-monary embolism (showing a S1Q3T3 pattern). Arterial blood gas test revealed hypoxaemia with hypercapnia and respiratory alkalosis.Blood exams reported high levels of I-troponin and D-Dimer. Echocardiography showed a dilated right ventricle, a Mac Connell sign, D-shapeof the left ventricle. Wells score was 6. CTPA was performed, showing a large thrombus on the pulmonary artery bifurcation extended to thecentral part of the lumen of both branches. Patient was then admitted to our intensive care unit. Anticoagulant treatment was started asstandard care and a possible source of the thrombus was investigated by performing a lower limb venous ultrasound examination. Accordingto the current guidelines of PE, a simplified CUS test was used with negative results at the groin as well as in the popliteal fossa. Because ofthe massive embolism poplitea we also evaluated veins below poplitea fossa (infra-popliteal tract). Surprisingly, a positive CUS was foundwith bilateral deep vein thrombosis and large thrombi extending from the popliteal vein until their bifurcation. No thrombophilic state was de-tected to explain this unusual event.
Discussion. Bilateral DVT is less common than unilateral DVT and is often associated with the exposure to well known risk factors. Thiscase is an unprovoked bilateral DVT. Moreover, the simplified CUS test at the popliteal fossa was negative with a thrombus unusually detec-ted in the infra-popliteal tract of popliteal vein of both sides. .
Conclusion. Simplified CUS not always allows to identify the source of embolism in case of PE and sometimes it could give false negativeresults. Based on this case, unusual sites should be also investigated for unexplained PE. In case of intermediate-high suspicious of PE, orin case of certain PE, the CUS test should be extended as lower as possible along the limb to avoid false negative results in the usual sitesof thrombus formation.
1Military Hospital Mohammed V, cardiac intinsif care and rhythmology, Rabat, Morocco2Ibn Sina University Hospital, CARDIOLOGY B, Rabat, Morocco
Introduction :
Dyslipidemias are a disorder of the lipids metabolism which precipitates the occurrence of atherosclerosis and cardiovascular attack (coro-nary artery disease, stroke...).
They are of multifactorial idiopathic causes, except for familial hypercholesterolemia.
This genetic pathology is a disorder transmitted by the autosomal dominant mode.
Purpose :
The homozygous form is rarer and more severe than the heterozygous form because it accelerates the atherogenesis. It’s a provider, at avery young age, of cardiovascular complications and significantly reduces life expectancy to less than 30 years.
Methods and résults:
We report the case of a 12-year-old woman with hypertension and homozygous familial hypercholesterolemia who has had interdigital-pal-mar cutaneous xanthomas and tendinous xanthomas since the age of four.
The lipid profile showed hypercholesterolemia at 44.33 mmol / l; LDL at 39.39 mmol / l, TG at 5.44 mmol / l. Lipid electrophoresis revealedhypercholesterolemia type IIA. The genetic study is in favor of a mutation of the LDL gene receptor. She is admitted for stress angina andtransient ischemic stroke.
CT angiography of the Supra-aortic trunks revealed stenosis of the left internal carotid artery and coronary angiography found significantlesions of the right coronary artery: 70% tight lesion at the ostial level and very tight lesion of the middle segment at 90%. Doppler ultraso-nography of the legs finds diffuse atheromatous overload with no effect on the flow.
An angioplasty with placement of two drug-eluting stents at the ostium of the right coronary and at her middle segment was performed withuneventful postoperative. Optimal medical treatment is conducted in the absence of LDL-apheresis, PCSK9 inhibitors and other new thera-pies in our context.
Conclusions :
The main interests of this clinical case are to make the medical profession aware of early childhood screening, the early treatment of familialhypercholesterolemia especially in its homozygous form, in order to curb the development of atheroma, as well as to search for new thera-peutics hoping to improve their life expectancy. This is a rare, serious pathology whose prognosis remains very dark.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P251
A rare cause of dyspnoea
Craveiro N.1; Costa C.1; Abouwda Y.2; Pitta ML.1; Peres M.1; Santos C.2; Cabrita M.2
1Hospital of Santarem, Cardiology, Santarem, Portugal2Hospital of Santarem, Medicine, Santarem, Portugal
Background: Platypnea–orthodeoxia syndrome (POS) is a rare clinical condition, associated with normal oxygen saturation in supine posi-tion and arterial hypoxemia on upright posture. It can be secondary to an intracardiac shunt, most commonly through a patent foramen ovale(PFO), a pulmonary vascular shunt or a ventilation–perfusion mismatch.
Clinical Case: We report the case of an 84 year-old woman with complaints of progressive dyspnea that developed a POS due to a right-to-left intracardiac shunt, through a PFO. Transesophageal echocardiography performed with agitated saline contrast confirmed the diagnosis.It revealed an aneurysmal interatrial septum with passage of a significant eccentric jet of bubbles through the PFO, from right-to-left atrium,with patient sited. This condition was potentiated, from a pathophysiological point of view, by a dilated thoracic ascendant aorta, a frequentfinding in the hypertensive elderly population. PFO closure was planned and a septal occluder device was implanted with remarkable im-provement in patient symptoms.
Conclusion: POS is an underdiagnosed pathology that should be investigated in the presence of a position-dependent hypoxemia. In car-diac etiology, the percutaneous PFO closure is an effective procedure that immediately relieves hypoxemia and patient symptoms.
aging/article/20/Supplement_1/i102/5301348 by guest on 11 July 2022
P252
Dressler syndrome - truth or dare?Duraes Campos I.; Quina-Rodrigues C.; Oliveira C.; Salgado A.; Azevedo P.; Marques J.; Vieira C.
Hospital de Braga, Cardiology, Braga, Portugal
INTRODUCTION: Dressler’s syndrome, also called postcardiac injury syndrome, was first described by William Dressler at MaimonidesMedical Center in 1956, and its incidence has been declining in recent years. Dressler syndrome is a secondary form of pericarditis thatcould occurs after acute myocardial infarction, cardiac surgery, traumatic injury or routine endovascular procedures. The aetiology is not wellunderstood, but it is believed that an initial injury to mesothelial pericardial cells combined with blood in the pericardial space triggers animmune response and results in immune complex deposition in the pericardium, pleura, and lungs which cause an inflammatory response.
SUMMARY: A 46-year-old male was admitted to the emergency department due to a fever associated a pleuritic chest pain in the last fourdays ago. Six weeks before this admission, he underwent ascending aorta replacement and aortic valve repair because he had a history of abicuspid aortic valve with aortic regurgitation. The patient’s electrocardiogram showed diffuse ST segment elevation and PR segment de-pression (signs of acute pericarditis), and his blood tests showed increased inflammation markers and negative myocardial necrosis mark-ers. Pericardial and left-sided pleural effusion were noted. Sterile blood cultures are negative. The patient"s clinical presentation (pleuriticchest pain and fever), the recent cardiac injury, the increase in the inflammatory markers, the electrocardiogram signs compatible with acutepericarditis and the alterations found in the thoracic images (small left-sided pleural and pericardial effusion, a thickening and hypercaptationof the pericardial leaflets) support the diagnosis of Dressler"s syndrome. The patient improved clinically and analytically with a short courseof anti-inflammatory therapy and was discharged on colchicine. A chest X-ray performed after 2 months showed a complete remission ofpleural effusion. DISCUSSION: Although not a common condition, Dressler’s syndrome should be considered in all patients with persistentfever and pleuritic chest pain, especially if symptoms begin two weeks after cardiac injury. After advances in treatments for heart lesions thiscondition is less frequent, however, the fast diagnosis of Dressler"s syndrome is crucial since the favourable prognosis depends on howquickly the condition is treated. The goal of treatment is to reduce inflammation through anti-inflammatory therapy with NSAIDs (aspirin, ibu-profen or naproxen) and colchicine. Corticosteroids can be used in resistant cases.